Nutrition 526 - 2009 A Framework for Maternal & Infant Nutrition.
Maternal and Child Health & Nutrition
Dr.Santhi Sri, K.V Assistant Professor Dept. of Foods & Nutritional Sciences Acharya Nagarjuna University, Guntur

The mother’s food habits and nutritional status before conception, as well as during pregnancy, influence the outcome of the pregnancy.
Through the food a pregnant woman eats, she gives her unborn child the nourishment required to begin and sustain fetal growth and development.

Status of women and Children in Developing Countries:● Throughout the world, women and children
are the most vulnerable and the least
serviced In the less technically developed
areas of the world, disease and death take
the highest toll among mothers and children
who make up over two-thirds of the
population.5/29/2017 3

Low birth weight is a major public health problem,particularly prevalent in developing countries. It is one ofthe important causes of high infant mortality rates. Theincidence of low birth weight is high in India, despiteadoption of many health policies for bringing it down. Theestimated proportion of low birth weight in India is about 7-8%. It contributes to 60-80 % of all neonatal deaths.
World Health Organization has been defined low birthweight as a birth weight of an infant less than 2500 grams. It
is further divided in to three categories as –
1 Low birth weight- 1500gms.-2500gms.2 Very low birth weight- 1000gms-1500 gms.3 Extremely low birth weight <1000 gms.
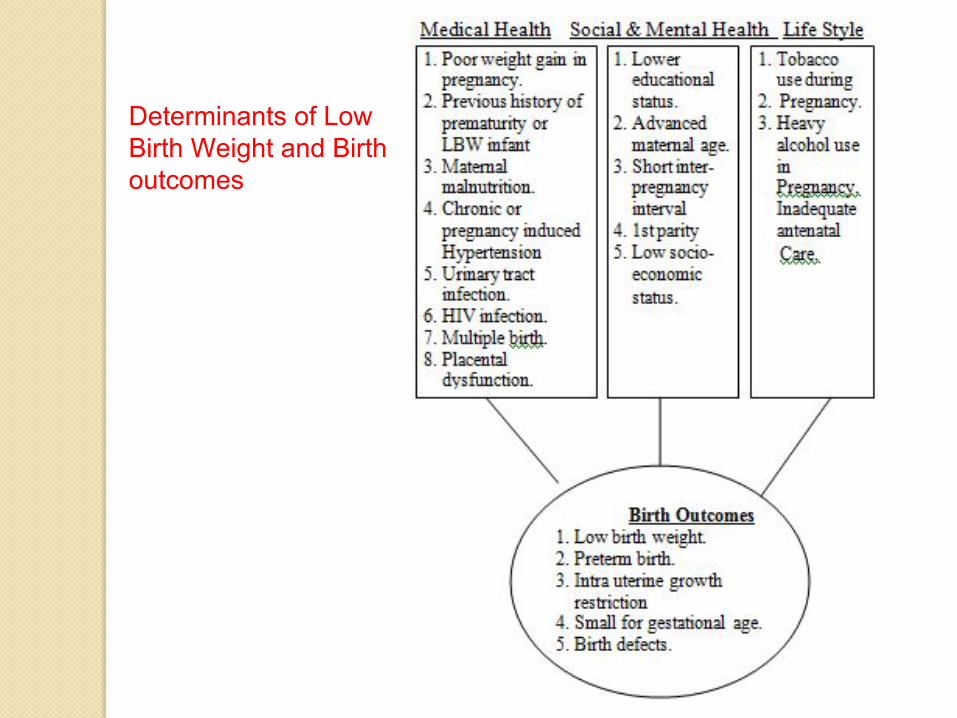
Determinants of Low Birth Weight and Birth outcomes
Maternal Health and NutritionHealth & nutritional status of mother during & beforepregnancy is considered to be strongly associated withpregnancy outcomes. Poor nutritional status & inadequateintake of food in pregnancy not only affect women’s healthbut also effect birth weight & development of infant.Nutritional status of mother is strongly related to the birthweight of infant. Energy, fatty acids and micronutrientsdeficiency, have all been implicated in causing LBW ininfants.
In many developing countries, majority of LBW is due toIUGR, Which may cause by:
� Low nutrients intake� High nutrients loss.� Placental dysfunction� Maternal infection.� Increased nutritional requirement..
Major Issuesin Maternal Nutrition
∙ Inadequate weight and height
∙Micronutrient deficiencies

Fetal development
● Fertilization: the union of sperm and egg● Cells divide and differentiate (specialize) for 40 weeks
of gestation (pregnancy)● About a week after fertilization, the embryo implants
in the lining of the uterus● Embryo - developing human from 2 to 8 weeks after
fertilization; implantation – embedding of an embryo in the uterine lining
● After 9 weeks, an embryo becomes a fetus
Fetal nourishment
• Weeks 2–5: embryo receives nourishement from uterine lining
• After week 5 until birth: developing baby receives nourishment from placenta
• Placenta: an organ produced from maternal and embryonic tissues
• Secretes hormones• Transfers nutrients and oxygen from the mother’s blood to
the fetus, removes metabolic wastes• Transport via umbilical cord

Fetal nourishment

Maternal Nutrition● Sedentary women need to increase caloric intake
by 300 calories/day.
● Active women must make additional adjustments based upon caloric expenditure.
● Weight gain is based upon pregravid weight (weight prior to conception).
● Increases in caloric intake and weight gain should be primarily in second and third trimesters.
Protein NeedsProtein serves as the building blocks for growth of body tissues during pregnancy.◦ Rapid growth of the fetus◦ Development of the placenta◦ Growth of maternal tissues◦ Increased maternal blood volume◦ Amniotic fluid◦ Storage reserves
● Protein intake should increase 25 g per day◦ Complete protein foods ⚫ Milk, eggs, cheese, soy products, meat◦ Incomplete proteins⚫ Legumes, grains
● Protein-rich foods contribute calcium, iron, B vitamins
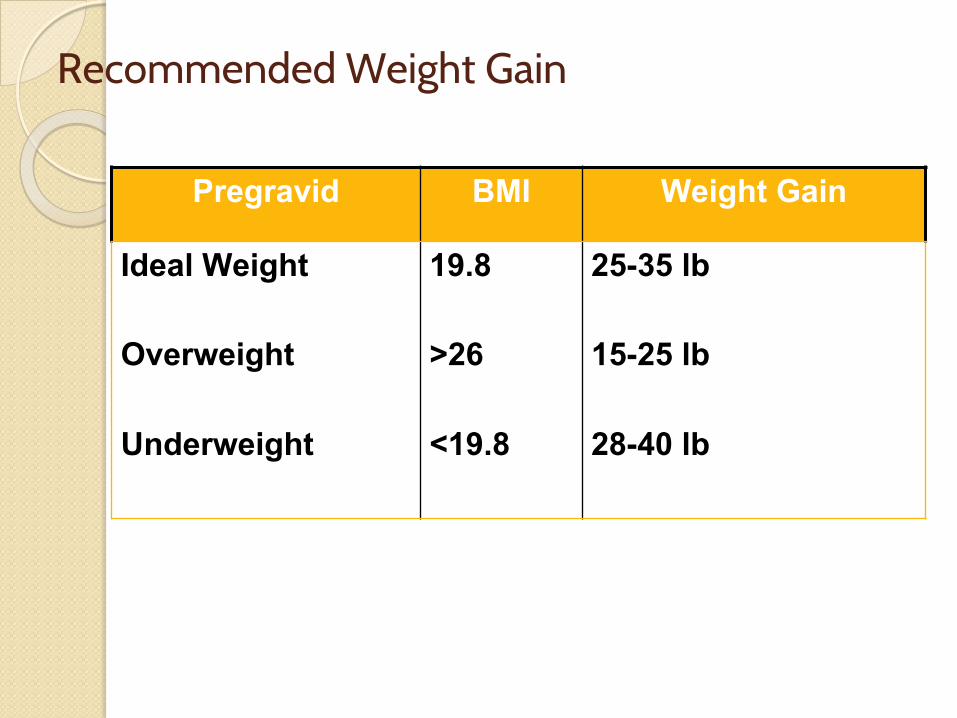
Recommended Weight Gain
Pregravid BMI Weight Gain
Ideal Weight
Overweight
Underweight
19.8
>26
<19.8
25-35 lb
15-25 lb
28-40 lb

Three major diagnostic groupings of birth weight
Maternal Malnutrition:A Life-Cycle Issue (1)∙ Infancy and early childhood (0-24
months)● Suboptimal breastfeeding practices● Inadequate complementary foods ● Infrequent feeding ● Frequent infections
∙ Childhood (2-9 years) ● Poor diets ● Poor health care● Poor education
Maternal Malnutrition:A Life-Cycle Issue (2)∙ Adolescence (10-19 years)
● Increased nutritional demands● Greater iron needs ● Early pregnancies
∙ Pregnancy and lactation ● Higher nutritional requirements● Increased micronutrient needs ● Closely-spaced reproductive cycles
Maternal Malnutrition:A Life-Cycle Issue (3)
∙ Throughout life● Food insecurity● Inadequate diets ● Recurrent infections● Frequent parasites● Poor health care● Heavy workloads● Gender inequities
Consequences of Maternal Chronic Energy Deficiency
∙ Infections∙ Obstructed labor∙ Maternal mortality∙ Low birth weight∙ Neonatal and infant mortality
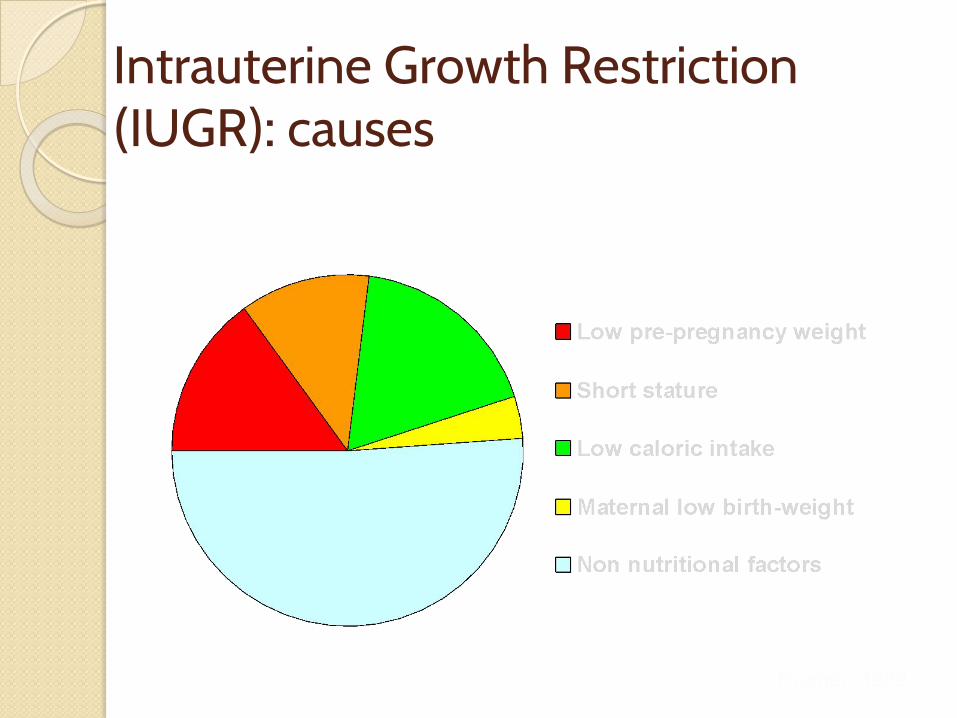
Intrauterine Growth Restriction (IUGR): causes
Kramer, 1989

Iron Deficiency∙ Most common form of malnutrition∙ Most common cause of anemia∙ Other causes of anemia:
− Parasitic infection− Malaria

Causes of DietaryIron Deficiency
∙ Low dietary iron intake
∙ Low iron bioavailability
− Non-heme iron− Inhibitors
Consequences of Vitamin A Deficiency
● Increased risk of:∙ Night blindness∙ Maternal mortality (??)∙ Miscarriage∙ Stillbirth∙ Low birth weight∙ Reduced transfer of vitamin A to fetus∙ HIV vertical transmission

Physiology of Milk Production

Consequences of MaternalVitamin A Deficiency on Lactation
UN
ICE
FC-9
2-18
/Spr
agueLow vitamin A
concentrationin breastmilk

Effects of Vitamin A deficiency on children● Contributing factor in 2.2 million deaths
each year from diarrhea and 1 million deaths from measles
● Severe deficiency can also cause irreversible corneal damage, leading to partial or total blindness
● Field trials indicate that VA supplementation of at-risk children can reduce deaths from diarrhea. Four studies showed deaths were reduced by 35-50 per cent.
● VA can reduce by half the number of deaths due to measles
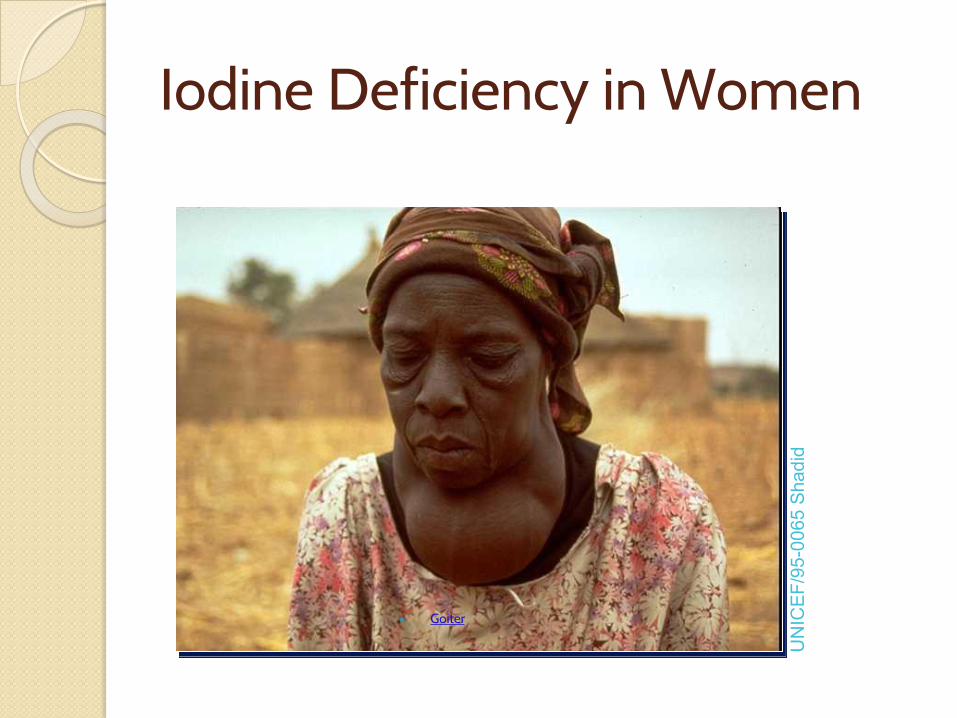
Iodine Deficiency in Women
● Goiter
UN
ICE
F/95
-006
5 S
hadi
d
Consequences of Iodine Deficiency on Intelligence
∙ 3% cretins
∙ 10% severely mentally impaired
∙ 87% mildly mentally impaired
UN
ICE
F/C
-79-
39
Consequences of Maternal Zinc Deficiency
∙ Rupture of membranes∙ Prolonged labor∙ Preterm delivery∙ Low birth weight∙ Maternal and infant
mortality

Consequences of Maternal Folic Acid Deficiency
∙ Maternal anemia
∙ Neural tube defects
∙ Low birth weight
Improving Maternal Weight∙ Increase caloric intake∙ Reduce energy expenditure∙ Reduce caloric depletion (e.g.,
infections)
Improving Maternal Height
∙ Increase birth weight
∙ Enhance infant growth
∙ Improve adolescent growth

Optimal Behaviorsto Improve Women’s Nutrition
Early Infancy: Exclusive breastfeeding to about six months of age
Optimal Behaviorsto Improve Women’s Nutrition
Pregnancy:• Increase food intake• Take iron+folic acid supplements daily• Reduce workload• Management of malaria, other parasites
UN
ICE
F/C
-55-
10/W
atso
n
Optimal Behaviorsto Improve Women’s Nutrition
UN
ICE
F/C
-88-
15/G
oods
mith
Lactation:• Increase food intake• Take a high dose vitamin A at delivery• Reduce workload
Optimal Behaviorsto Improve Women’s Nutrition
UN
ICE
F90-
070/
Lem
oyne
• Delay
first pregnancy
• Increase
birth intervals
Parasite Control to Improve Women’s Micronutrient Status
Reduce parasite transmission:
∙ Improve hygiene, footwear
∙ Increase access to effective care
∙ Bednets, malaria management especially
during pregnancy
Optimal Behaviorsto Improve Women’s Nutrition
● At all times:● Increase food intake if underweight● Diversify the diet● Use iodized salt● Control parasites, including malaria● Take micronutrient supplements if
needed
Physical activity during pregnancy
• Moderate physical activity:• Improves digestion and prevents constipation• Improves mood and self image• Reduces stress• Prevents excess weight gain and low back pain• Reduces risk of diabetes and high blood pressure• Speeds recovery from childbirth

Physical activity during pregnancy
● Guidelines to maximize benefits and minimize risks of injury to mother and fetus:◦ Women physically active before pregnancy can continue a
program of about 30 minutes of carefully chosen moderate exercise per day
◦ Women who weren’t active before pregnancy should slowly add low-intensity, low-impact activities
◦ Because intense exercise can limit the delivery of oxygen and nutrients to the fetus, intense exercise should be limited
Discomforts during pregnancy
• Edema: accumulation of fluid in tissues• Morning sickness: nausea and vomiting any time of
day or night, usually in 1st trimester• Eat small, frequent snacks of dry, starchy foods
• Heartburn• Limit high-fat foods; avoid heartburn-causing substances;
eat small, frequent meals; remain upright after eating• Constipation and hemorrhoids
• Maintain moderate level of physical activity and consume plenty of fluids and high-fiber foods

Discomforts during pregnancy
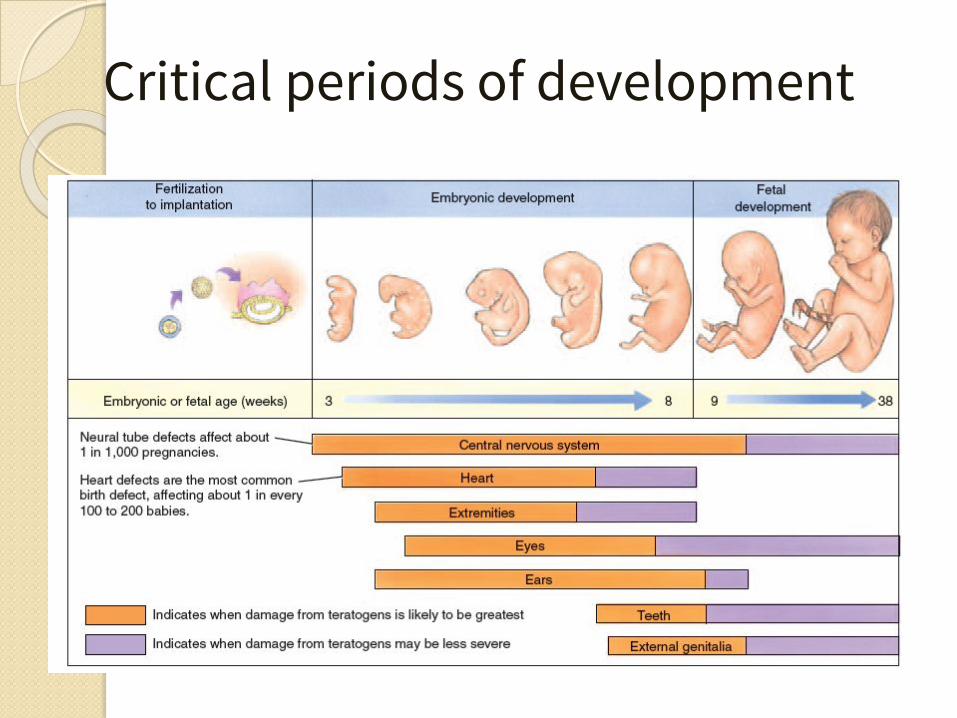
Critical periods of development
Increased risks during pregnancy
• Some women are at increased risk for complications during pregnancy due to their:
• Nutritional status• Age• Pre-existing health problems • Exposure to harmful substances
Maternal nutritional status
● Before pregnancy: ◦ Importance of proper nutrition for the maintenance of normal body
fat, hormone levels and fertility
● During pregnancy, malnutrition can lead to: ◦ growth retardation, low birth weight, birth defects, premature birth,
spontaneous abortion, stillbirth◦ increase child’s risk of developing chronic diseases such as
cardiovascular disease, high blood pressure, diabetes mellitus, obesity and osteoporosis
◦ future food preferences of an infant

Alcohol during pregnancy
• Other, less severe but more common alcohol-related problems include:
• Alcohol-related neurodevelopmental disorder (ARND) characterized by mental impairments
• Alcohol-related birth defects (ARBD) – malformations in the skeleton or major organ systems
• Complete alcohol abstinence is recommended during pregnancy!!!

Tobacco and certain drugs
• Tobacco, marijuana and cocaine should be avoided during pregnancy
• These drugs can cross placenta and lead to profound negative effects on the offspring’s development and future health

High blood pressure
• About 5% to 10% of pregnant women experience hypertension during pregnancy
• Hypertension during pregnancy are due to:• Chronic hypertension present before pregnancy• Gestational hypertension (rise in blood pressure after the 20th
week of pregnncy)• Preeclampsia: characterized by elevated blood pressure, a
rapid increase in body weight, protein in urine and edema• Dangerous to the mother and the baby
Gestational diabetes
• High glucose levels developing during pregnancy• Increased risk (20% to 50%) of diabetes within next 5
to 10 years (mother)• Babies large for their gestational age
• increased risk for difficult delivery, abnormal glucose at birth, an future diabetes
Breast milk
● Colostrum: produced by the breast for up to a week after delivery◦ Has beneficial effects on the gastrointestinal tract◦ Nutrients supplies meet the infant’s needs until mature milk
production begins◦ Contains more water, protein, immune factors, minerals, and vitamins
and less fat than mature milk
● Mature breast milk: contains an appropriate balance of nutrients in easily-digested forms
Benefits of breast milk
● Formula can never exactly duplicate human milk composition
● Immune system cells, antibodies, enzymes, and other substances pass to the child, providing immune protection
● Growth factors and hormones promote maturation of the infant’s gut and immune defenses and enhance digestion
● Physical, emotional, and financial advantages

Lactation
● Synthesis of milk components◦ Stimulated by pituitary hormone prolactin
AND● Let down: release of milk from milk-producing glands
and movement through the milk ducts to the nipple◦ Stimulated by pituitary hormone oxytocin◦ Inhibited by nervous tension, fatigue, or embarrassment

Lactation

Thank you