
Mat Maurer, MD Columbia University Medical Center
60
Cardiovascular Syndromes in Older Adults Greater New York Geriatric Cardiology Consortium October 18 and 19, 2011 Mat Maurer, MD Columbia University Medical Center
description
Cardiovascular Syndromes in Older Adults Greater New York Geriatric Cardiology Consortium October 18 and 19, 2011. Mat Maurer, MD Columbia University Medical Center. Disclosures. None. Goals of GNYGCC. AIM #1. AIM # 2. Research Innovative Investigator Initiated Multi-center - PowerPoint PPT Presentation
Transcript of Mat Maurer, MD Columbia University Medical Center

Cardiovascular Syndromes in Older Adults
Greater New York Geriatric Cardiology Consortium
October 18 and 19, 2011
Mat Maurer, MD
Columbia University Medical Center

Disclosures
None
Goals of GNYGCC
AIM #1
Seminar Series
Develop membership
Build enthusiasm
Educate
Build Camaraderie
Brainstorm Ideas
AIM # 2
Research
Innovative
Investigator Initiated
Multi-center
Multi-disciplinary
Leads to
GNYGCC Participating Sites
• New York University
• St. Luke’s Hospital
• Roosevelt Hospital
• SUNY Downstate
• Vanderbilt
• Yale University
• Woodhull
• Allen Hospital
• Columbia
• Weil Cornell
• Einstein/Montefiore
• Mount Sinai
• Maimonides
• University of Michigan

Objectives1. Define disability, frailty and co-morbidity
2. Enumerate criteria for defining “geriatric syndromes”
3. Understand the added value added for Geriatric Cardiology in moving away from a “disease based model” to a more complex paradigm involving syndromes.
4. Delineate common “geriatric cardiovascular syndromes” and identify shared risk factors among “geriatric syndromes”
5. Highlight the prevalence of “geriatric syndromes” in older adults with cardiovascular disease and their independent association with outcomes.

An Aging Society:Important Tenants for Clinical Care
Aging:1. A process of gradual and
spontaneous change, resulting in maturation.
2. To acquire a desirable quality by standing undisturbed for some time
3. To bring to a state fit for use or to maturity
Heterogeneous
Selective
Homeostenosis

Co-Morbidity, Frailty and Disability• Co-morbidity
– Concurrent presence of two or more medically diagnosed diseases in the same individual
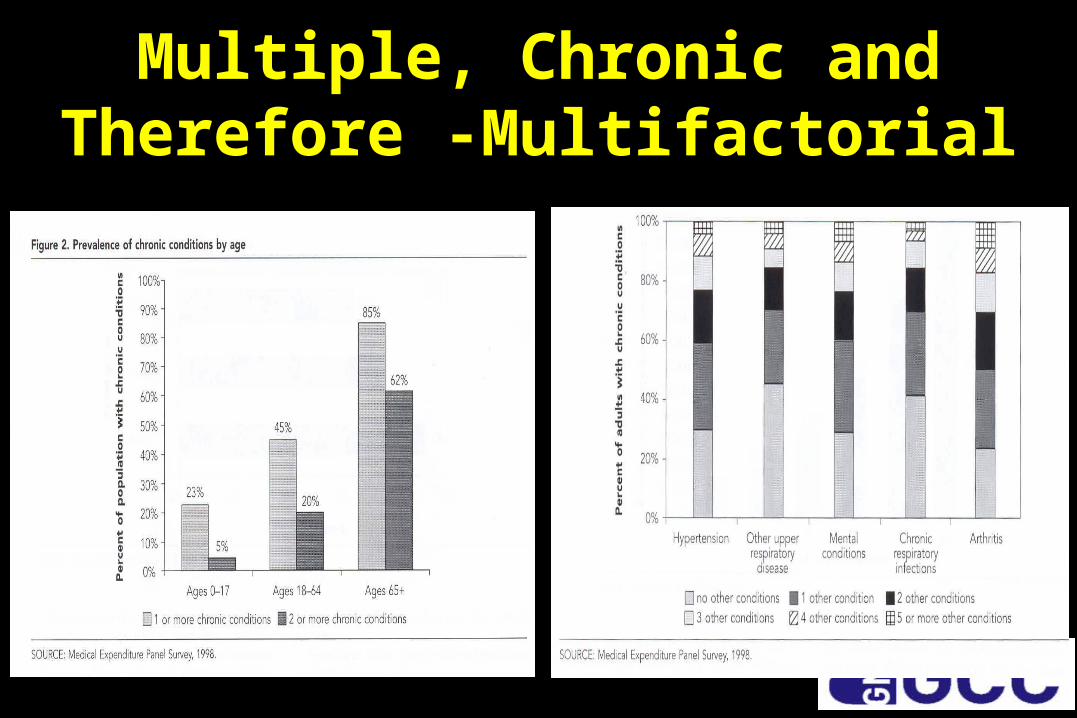
Multiple, Chronic and Therefore -Multifactorial

Co-Morbidity, Frailty and Disability• Co-morbidity
– Concurrent presence of two or more medically diagnosed diseases in the same individual
• Frailty– A physiologic state of increased vulnerability to stressors that
results from decreased physiologic reserves causing homeostenosis.
• Disability– Difficulty or dependency in carrying out activities essential to
independent living (e.g. Loss of ADLs and IADLs).
60%8%
7%

Embracing Complexity
…at best out of date and at worst harmful
…lead to under-treatment, overtreatment or mistreatment
Am J Med. 2004 Feb 1;116(3):179-85.

Geriatric Cardiology: A delicate balance
Commission
Omission

What is a Syndrome?
• Syndrome derives from the Greek roots – "syn“ = meaning "together“– "dromos" = meaning "a
running“
• Refers to "a concurrence or running together of constant patterns of abnormal signs or symptoms."

What constitutes a Geriatric Syndrome?
1. High Frequency (e.g.>10%)– Particularly frail older adults
2. Chronic/intermittent conditions– Not isolated episodes
3. Triggered by acute insults
4. Associated with functional decline
Geriatric Syndromes: Clinical Perspective
• Chief Concern/Complaint– Expressed by patient or caregiver– Does not represent the specific pathological
condition underlying the change in health status.
• Result from impairments in multiple systems– Not from a discrete disease
• Develop from accumulated effects of impairments in multiple domains that ultimately compromise compensatory ability

Common Geriatric Syndromes
• Falls/Syncope
• Delirium
• Dizziness
• Urinary Incontinence
• Pressure Ulcers
• Dementia
• Weak Bones
• Visual difficulties
• Auditory difficulties
• Weight loss
• Sleep disorders

Anergia: A Neglected Geriatric Syndrome• Anergia (an·er·gia) (an-ər´je-ə):
– 1. characterized by abnormal inactivity; inactive. – 2. marked by lack of energy. – 3. lack of mental energy, debility; passivity
• Analogous to fatigue (~20% of the population) but not strictly a post-exertional construct.
• The prevalence and clinical significance is not well characterized in the elderly population.
The Journals of Gerontology; Medical Sciences: 2008; 63A, 707-714
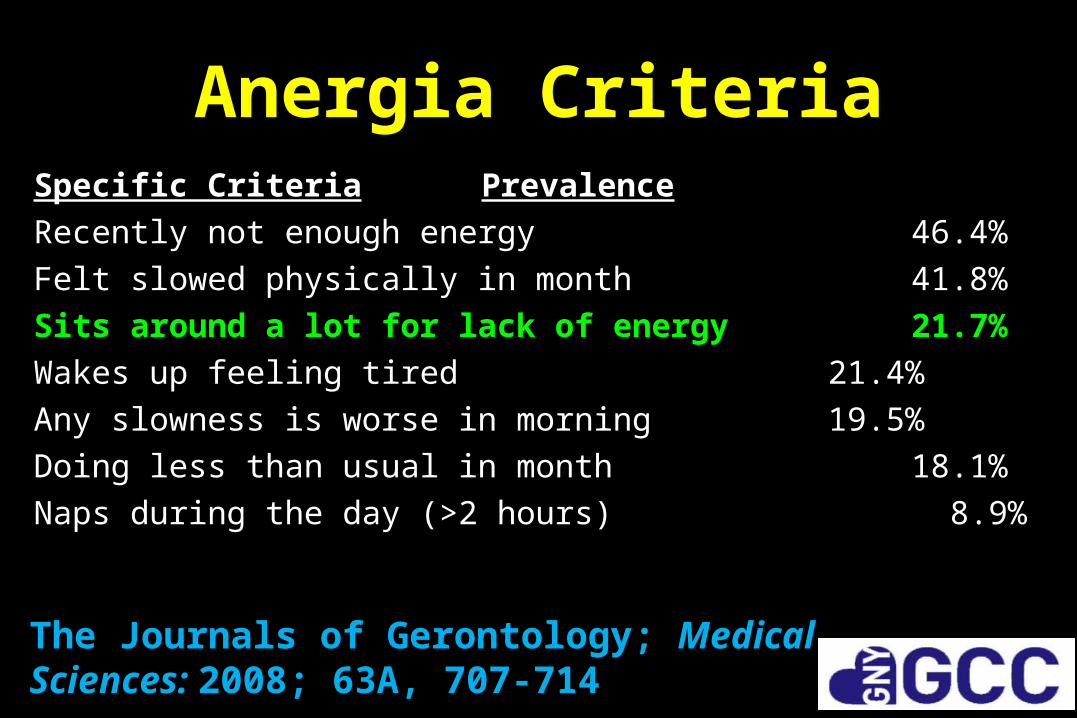
Anergia CriteriaSpecific Criteria Prevalence
Recently not enough energy 46.4%
Felt slowed physically in month 41.8%
Sits around a lot for lack of energy 21.7%
Wakes up feeling tired 21.4%
Any slowness is worse in morning 19.5%
Doing less than usual in month 18.1%
Naps during the day (>2 hours) 8.9%
The Journals of Gerontology; Medical Sciences: 2008; 63A, 707-714
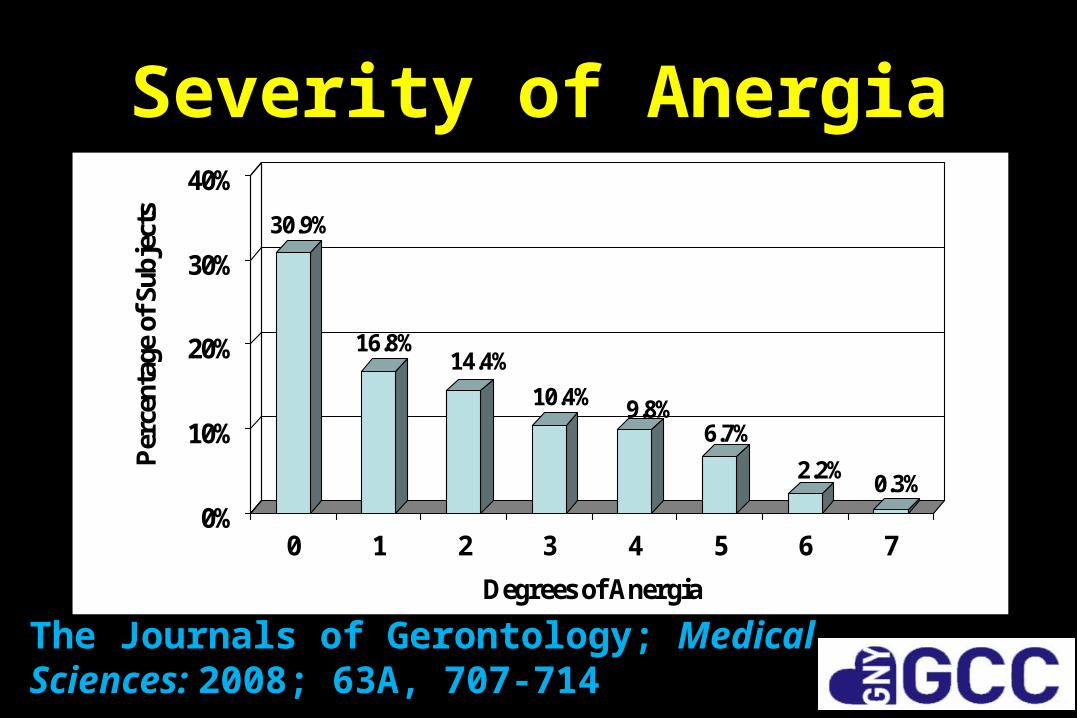
Severity of Anergia
30.9%
16.8%14.4%
10.4% 9.8%6.7%
2.2%0.3%
0%
10%
20%
30%
40%P
erce
ntag
e of
Sub
ject
s
0 1 2 3 4 5 6 7
Degrees of Anergia
The Journals of Gerontology; Medical Sciences: 2008; 63A, 707-714
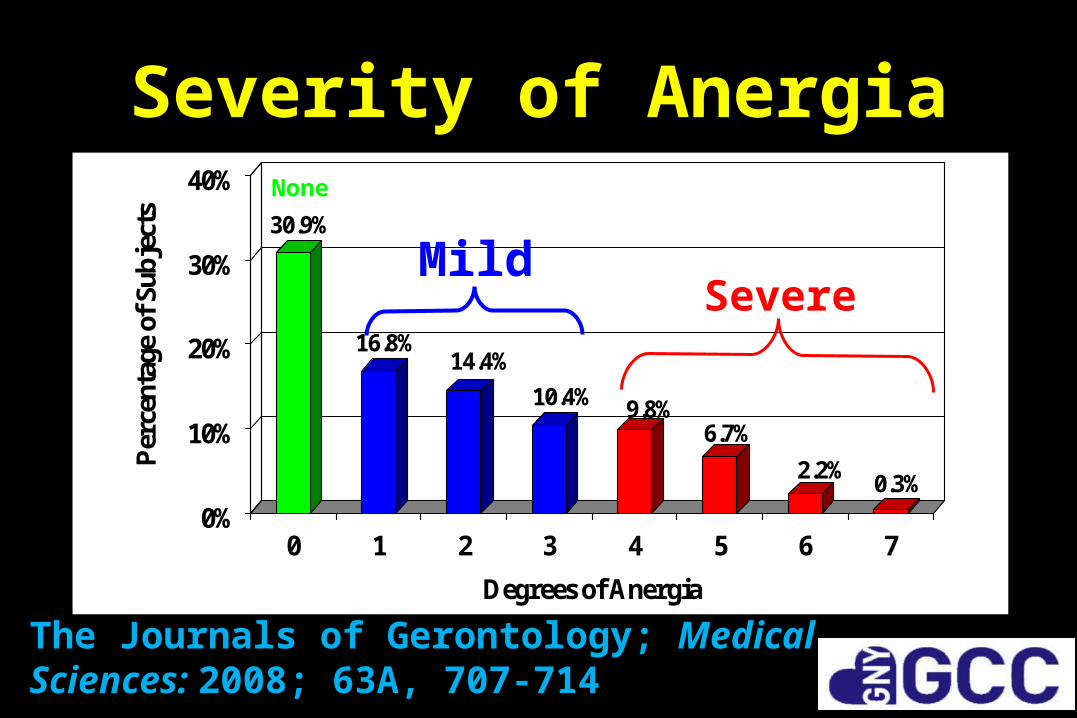
Severity of Anergia
30.9%
16.8%14.4%
10.4% 9.8%6.7%
2.2%0.3%
0%
10%
20%
30%
40%P
erce
ntag
e of
Sub
ject
s
0 1 2 3 4 5 6 7
Degrees of Anergia
Mild
None
Severe
The Journals of Gerontology; Medical Sciences: 2008; 63A, 707-714

Anergia: Source of Presentation and Association with Somatic Symptoms and DiseaseParameter Odd’s RatioArthritis Arthritis/Rheumatism Joint pain, stiff or swelling Often takes meds for pain
2.38 (1.96-2.88) 3.39 (2.75-4.17)3.78 (2.83-5.05)
Respiratory Shortness of breath Breathless all the time Other lung conditions
7.10 (5.18-9.73)9.6 (1.31-70.58)2.10 (1.38-3.22)
Cardiovascular Every had heart trouble Felt dizzy or weak Exertional chest pain Ever had high blood pressure
2.04 (1.63-2.55) 6.42 (4.86-8.49) 4.94 (3.40-7.19)2.98 (1.90-4.68)
Sleep Disorder Trouble falling asleep Medication for sleep
3.67 (2.90-4.64)2.68 (1.90-3.78)
Parameter Odd’s RatioMobility Falls Assist device to ambulate Ever had a fracture
2.77 (2.20-3.49)5.42 (3.81-7.70) 1.52 (1.20-1.92)
Incontinence 3.83 (2.63-5.57)
Depression 5.80 (3.97-8.46)
Sensory Deficits Hearing Difficulty Trouble seeing
2.24 (1.78-2.82)2.52 (1.90-3.33)
Neurology Ever had stroke Dementia Parkinsons’ Disease
2.41 (1.57-3.70)1.91 (1.37-2.64)1.55 (0.61-3.92)

Anergia Is Associated with Mortality
Time Total No Anergia Anergia Odd’s Ratio
18 months
158 (8.1) 39 (5.9) 119 (9.2) 1.61
(1.11-2.35)
6 years
453 (23.2) 119 (18.1) 334 (25.9) 1.58
(1.25-2.00)
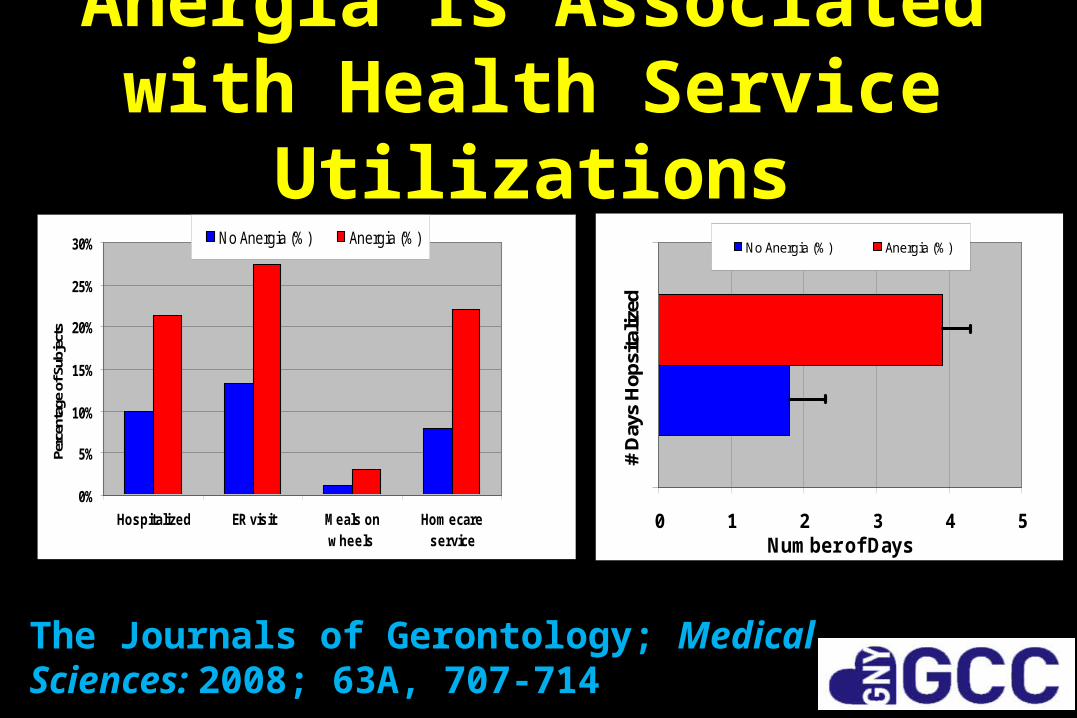
Anergia Is Associated with Health Service Utilizations
0%
5%
10%
15%
20%
25%
30%
Hospitalized ER visit Meals onwheels
Homecareservice
Perc
enta
ge o
f Sub
ject
s
No Anergia (%) Anergia (%)
0 1 2 3 4 5
# D
ays
Hop
sita
lized
Number of Days
No Anergia (%) Anergia (%)
The Journals of Gerontology; Medical Sciences: 2008; 63A, 707-714

Factors Associated with Anergia: Multivariate Analyses
Adjusted OR *
(95% CI)
Depression 2.01 (1.29-3.13)
Trouble sleep 2.01 (1.52-2.65)
Falls 1.69 (1.23-2.23)
Respiratory syndrome 1.63 (1.41-1.88)
Female 1.33 (1.01-1.74)
Isolation 1.26 (1.12-1.42)
Activity limitations 1.26 (1.15-1.38)
Pain syndrome 1.20 (1.13-1.28)
*The adjusted confounders included age, gender, married status, education, income, self-rated health, physical function, social function, somatic symptoms, medications, co-existing diseases

Anergia: A New Geriatric Syndrome?
1. Anergia may be a prevalent concern and of sufficient magnitude and duration to warrant clinical attention.
Anergia is common among multi-ethnic community-dwelling older persons.
2. Anergia may be linked to many etiologic factors and/or multiple functional, cognitive or affective disorders
Anergia is associated with many clinical symptoms and multiple co-existing diseases

Anergia: A New Geriatric Syndrome?
3. Anergia may be associated with increased health care utilization and adverse outcomes in elderly persons.
Anergia is associated with extensive health services use and poor outcomes including mortality
4. Anergia may be potentially susceptible to targeted interventions that reduce the morbidity and mortality in anergic older individuals.
Multivariate analyses suggests that several factors/diagnoses are independent of
other confounders and thus, should be investigated initially.

Geriatric Syndromes: Shared Risk Factors
JAMA. 1995;273:1348-1353
Falli
ng
Incontinence
Functional Dependence
Physical performance(arm and leg
strength)
Sensory Impairments
Affective Impairments
(Anxiety)

Geriatric Cardiovascular Syndromes
• Systolic Hypertension– 70% NHANES1, 90% Liftetime2
– Load lability – Hypertensive urgency and orthostasis
– Trigger: salt, NSAIDs, stress, etc
• HFPEF (aka DHF) – >Half of all heart failure– APE/AHDF/CHF - presentations– Multiple mechanisms
• Syncope/Falls– 33-50% fall/year, syncope ↑
with age.– Multiple triggers– OR 3.1 for NH placement3
• Atrial Fibrillation– >10% of octogenarians– PAF leads to chronic afib– ↑ risk for stroke/disability
1 MMWR Surveill Summ. 2011;60 Suppl:94-7, 2 Circulation. 2011 Feb 1;123(4):e18, 3 N Engl J Med. 1997;337(18):1279-84.
Added Value?Syndromes over Diseases
• Under-treatment:– Treating only the biological rather than addressing all
contributing factors results in lost opportunities to maximize health outcomes.
• Overtreatment– Get Away from the Guidelines (GAFTG)
• Mistreatment– Clinical decision making based on disease-specific
outcomes rather than on patient preferences
Am J Med. 2004;116:179 –185

Changes in Models of Care
Am J Med. 2004;116:179 –185

A New Model of Care for Older Adults with Cardiovascular Disease
Traditional Cardiology Geriatric Cardiology
Treatment focused on the heart Treatment considers the host
Few comorbidities Multiple comorbidities
Treatment yields expected outcomes Treatment may result in complex effects
Large simple trials apply Large simple trials have limited generalizability
Evidence-based medicine Patient-centered evidence-based medicine
Cardiovascular reserve usually preserved
Cardiovascular reserve usually compromised
Outcomes: death, MI, revascularization
Outcomes: morbidity, function, independence, cognition
J Am Coll Cardiol. 2011;57(18):1801-10.

HFPEF: Disease or Syndrome?
Disease Syndrome
Prevalence Variable High
Organ Focused Often Rarely
Mechanism(s) Single Multiple
Heterogeneity No Yes
Chief Complaint Represents Specific Pathologic Condition
Disconnect between Chief complaint and underlying pathology

Heart Failure: Is there a better model for care?
• HF is principally a disease of older adults.
• HF in the setting of a preserved EF (HFPEF) is increasing in prevalence/incidence.
• Disease model argued a single pathophysiologic mechanism “diastolic dysfunction”
• Outcomes in HFPEF have not improved.
• Multiple “under-appreciated” targets for therapy that confound outcomes
Heart Failure Epidemic• 6 million patients diagnosed with symptomatic HF• Annually there are
– 600,000 new cases of symptomatic HF diagnosed– 15 million visits for heart failure – 1 million hospitalizations and 6.5 million hospital days for heart
failure – 2.6 million patients hospitalized with heart failure as a 2° diagnosis
• ~33-50% of patients with heart failure as a discharge diagnosis readmitted within 90 days
• $39.2 billion annually on heart failure in the US
AHA. Heart Disease and Stroke Statistics—2010 Update.

Heart Failure and Aging
• Heart failure is the most common Medicare DRG.
• 10% of patients older than 65 years have heart failure
• 80% of hospitalized patients with heart failure are older than 65 years.

Trends in Heart Failure
N Engl J Med. 2006 Jul 20;355(3):251-9

Re-hospitalization:Heart Failure Leading the List
Conditionat Index Discharge
30 day Re-hospitalization Rate (%)
Heart Failure 26.9
Pneumonia 20.1
COPD 22.6
Psychosis 24.6
GI Problems 19.2
N Engl J Med 2009;360:1418-28.

HFPEF: Effective therapy?
J Am Coll Cardiol 2011;57:1676–86

HFPEF: Effective therapy?
J Am Coll Cardiol 2011;57:1676–86

HFPEF: Effective therapy?
J Am Coll Cardiol 2011;57:1676–86

HFPEFHeterogeneous Disorder with a Single
Pathophysiologic Mechanism?
• Although heart failure with a preserved ejection fraction (HFPEF) is a heterogeneous clinical entity, a single mechanism, diastolic dysfunction, is ascribed to explain the pathophysiology of this condition.

HFPEF: Embrace Complexity

Heart Failure and Geriatrics:More Common than Different
Heart Failure GeriatricsPatient population Generally older
adultsExclusively older adults
Disease vs. syndrome Syndrome Syndrome(s)
Multidisciplinary Yes Yes
Integrated/Tailored Management Yes Yes
Palliation Yes Yes
Complex Cases Definitely Definitely
So why don’t we collaborate anddevelop a new model of care
employing geriatric principles?

How to Treat HFPEF?
JAMA. 2008 Jul 23;300(4):431-3.

Condition PrevalencePotential Consequences
Assessment Technique
Renal Dysfunction
16%- GFR < 30 mL/min
40% - GFR 30 to 59 mL/min
Worsens symptoms, prognosis; exacerbated by diuretics, ACE inhibitors and ARBs.
•Cockroft-Gault Formula
•MDRD Formula
Chronic Lung Disease
20% to 32% Worsens symptoms; prognosis; Contributes to uncertainty about diagnosis, exacerbates right heart function
•Pulmonary Function Tests
Cognitive Impairment
Dementia – 8.5%Cognitive impairment Mild – 28% Mod/Severe – 19%
Increases chance of non-adherence with meds, diet and non-pharmacologic interventions.
•MMSE•Mini-Cog
Co-Morbidities/Geriatric Syndromes in Older Adults with Heart Failure

Condition PrevalencePotential Consequences
Assessment Technique
Delirium 30-50% of hospitalized
patients36.8% (range, 0% to 73.5% in post-op
patients>70% in ICU
Prolong hospital stay, increased chance oflong term care placement, Increased mortality
•Seven digit numbering•Confusion
Assessment Methodology
Depression 8-25% Worsens prognosis; exacerbates symptoms and increases chance of non-compliance
Geriatric Depression Scale
Co-Morbidities/Geriatric Syndromes in Older Adults with Heart Failure

Condition Prevalence Potential Consequences
Assessment Technique
Diabetes 30-50% Worsens prognosis and increases risk associated with polypharmacy. Increases risk of vascular disease, dementia, chronic renal dysfunction and anemia.
•Blood glucose•Glycosylated hemoglobin
Falls, Mobility Difficulties
30-50% Exacerbated by diuretics and vasodilators, impairs community mobility and interferes with ability to follow-up routinely
•Gait speed•Timed get up and
Go•Tinnetti Gait and
Balance Scale
Co-Morbidities/Geriatric Syndromes in Older Adults with Heart Failure

Condition Prevalence Potential Consequences
Assessment Technique
Postural/Postprandial Hypotension
Postural: 10-30%Postprandial: 10-
20%
Worsened by diuretics, vasodilators
•Orthostatic/Postprandial BP measurements
•Tilt table testingAnemia Inpatient: 70%
Outpatient: 10-20%
Worsens symptoms, increases risk of hospitalization.
•Complete Blood Count
•Blood VolumeUrinary Incontinence
Women > Men35% and 22%,
respectively
Aggravated by medical therapy including diuretics, ACE (secondary to cough thereby worsening stress incontinence)
•Bladder diary
Co-Morbidities/Geriatric Syndromes
in Older Adults with Heart Failure

Condition Prevalence Potential Consequences
Assessment Technique
Sensory Impairments
24% - Ocular disorders
Interferes with compliance, increases chance of medication error
•Snellen eye chart•Contrast Sensitivity
Testing•Auditory evaluation
Anergia/Fatigue Mild to mode – 70%Severe – 20%
Worsens symptoms, complicates diagnosis
•Anergia scale
Polypharmacy -Almost all. Increases risk of non-adherence, medication interaction and adverse drug reaction
•Greater than 4 medications
Co-Morbidities/Geriatric Syndromes in Older Adults with Heart Failure
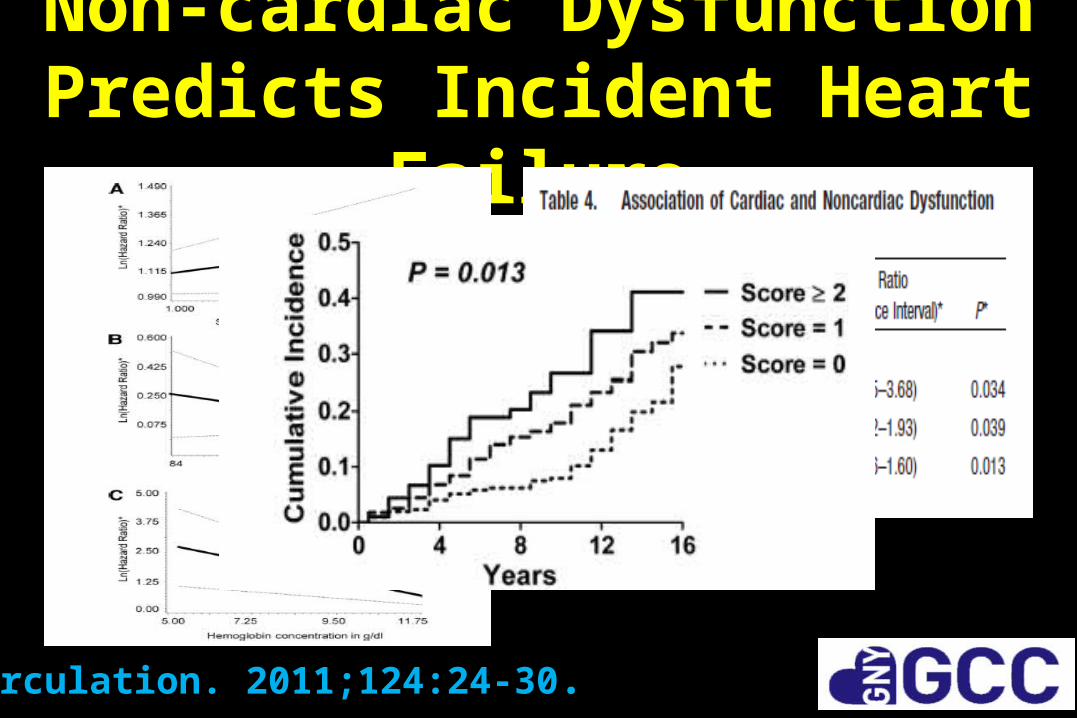
Non-cardiac Dysfunction Predicts Incident Heart Failure
Circulation. 2011;124:24-30.

Geriatric Syndromes and Outcomes in Cardiovascular Disease
Heart. 2011 Oct;97(19):1602-6.
Heart failure
46%
STEMI17%
Non-STEMI19%
Arrhythmia
11%
Syncope5%
Other 2%
Diagnosis At Admission
n=21182±5 years
Range 75-95 yearsLOS 7±4 days
Geriatric Syndromes•Functional Status/ADLs
•Cognitive Dysfunction
• Depression
• Frailty

Geriatric Syndromes and Outcomes in Cardiovascular Disease
Heart. 2011 Oct;97(19):1602-6.

Geriatric Syndromes and Outcomes in Cardiovascular Disease
J Am Coll Cardiol 2010;55:309–16

Unmet Needs: Cardiovascular Syndromes in Older Adults
• An approach to assess “homeostenosis”, frailty or vulnerability to adverse outcomes in older adults with cardiovascular disorders.
• A definition of resiliency that predicts who can tolerate invasive interventions with meaningful benefit.
• Method to identify basic mechanisms underlying geriatric cardiovascular syndromes that are targets for therapy, given underlying multifactorial complexity.
• Are there shared risk factors for geriatric cardiovascular syndromes (isolated SBP, HFPEF, syncope/falls/dizziness, atrial fibrillation)?
• Develop models that account for multiple pathways and potential synergisms between pathways that underlie geriatric cardiovascular syndromes.

Summary• Embracing the inherent complexity in caring for
older adults with cardiovascular disease may be facilitated by a move away from a “disease based model” to a more complete paradigm involving “syndromes”.
• Optimizing outcomes for older adults with cardiovascular disease will require a collaboration between disciplines capitalizing on their respective expertise.

THANK YOU!!!
• Submit your unmet needs online!!
• Join the GNYGCC!!
• Collaborate!!


Geriatric Assessment:Essential Part of Routine Clinical
Cardiovascular Care?
• “I don’t know what questions to ask.”
• “I have too little time.”
• “I am not paid to do it”
• “How do I interpret the information.”
• “What do I do if I find these problems?”
• “I am not trained to manage this.”

HFNEF: Embrace Complexity
J Am Geriatr Soc 55:780–791, 2007
Geriatric Cardiology: New Paradigm of Care
1. Emphasize patient centered approach to care
2. Screen for co-existing geriatric syndromes and co-morbidities
3. Purposefully manage pharmacologic regimen
4. Optimize care transitions

Focus of Geriatric Cardiology• Continue to emphasize:
– State-of-the-art technological and medical expertise,– Appropriate application of readily advancing technologies
• Promote skills needed to:– Assess patient preferences, – Circumvent hazards of hospitalization,– Facilitate successful transitions – Engage in useful risk-benefit discussions,– Provide care collaboratively within a care team
• Responsive to the needs of the oldest patients.


















