
Massive Transfusion in the New Era JHSGR 17 Apr 2010 Dr J Leung CMC.
28
Massive Transfusion in the New Era JHSGR 17 Apr 2010 Dr J Leung CMC
-
Upload
marisa-barnish -
Category
Documents
-
view
215 -
download
0
Transcript of Massive Transfusion in the New Era JHSGR 17 Apr 2010 Dr J Leung CMC.

Massive Transfusion in the New Era
JHSGR 17 Apr 2010Dr J Leung
CMC
Outline
• Massive transfusion (MT)– Definition, conditions, outcomes– Coagulopathy
• Hemostatic resuscitation– Transfusion of FFP, Platelet and PRBC– Hypotensive resuscitation
• Massive transfusion protocol– Outcome, complications
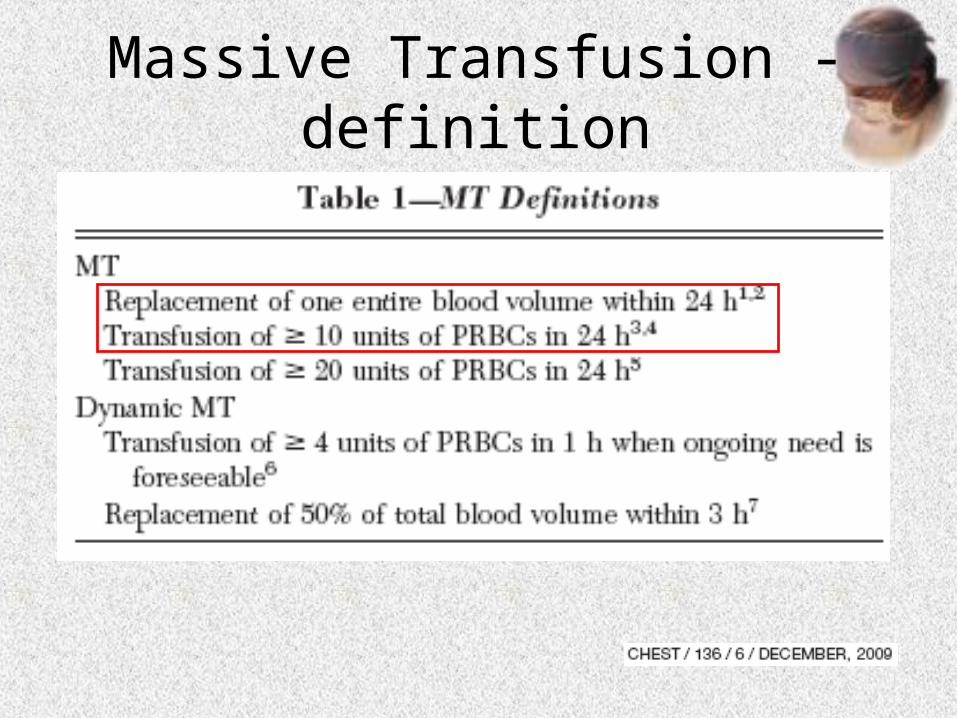
Massive Transfusion - definition
Massive Transfuion - Conditions
• Trauma– e.g Pelvic fracture, Liver lacerations
• Non Trauma– Abdominal Aortic Aneurysm repair– Gastrointestinal Hemorrhage– Liver Transplant– Obstetrics Conditions eg ectopic pregnancy,
postpartum hemorrhage

Trauma
• The leading cause of death for Americans under 35 years old
Hemorrhage: 40% of all trauma deaths
Hemorrhage: 40% of all trauma deaths
The most common reason for massive transfusion
The most common reason for massive transfusion
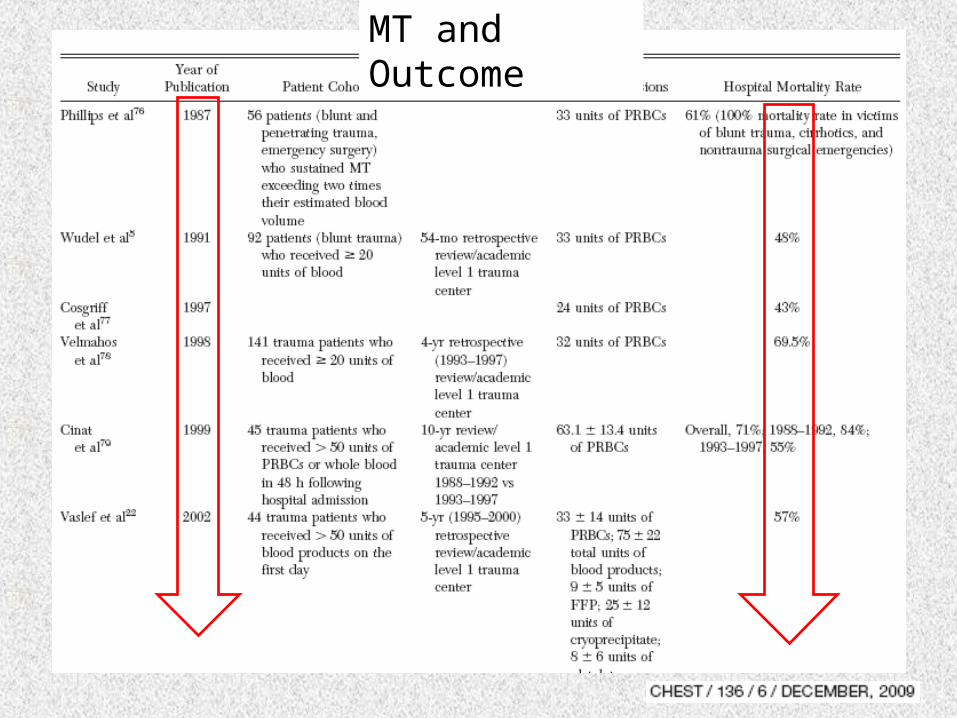
Massive Transfusion - Outcomes
• Trauma patient: 19-84% mortality
MT and Outcome
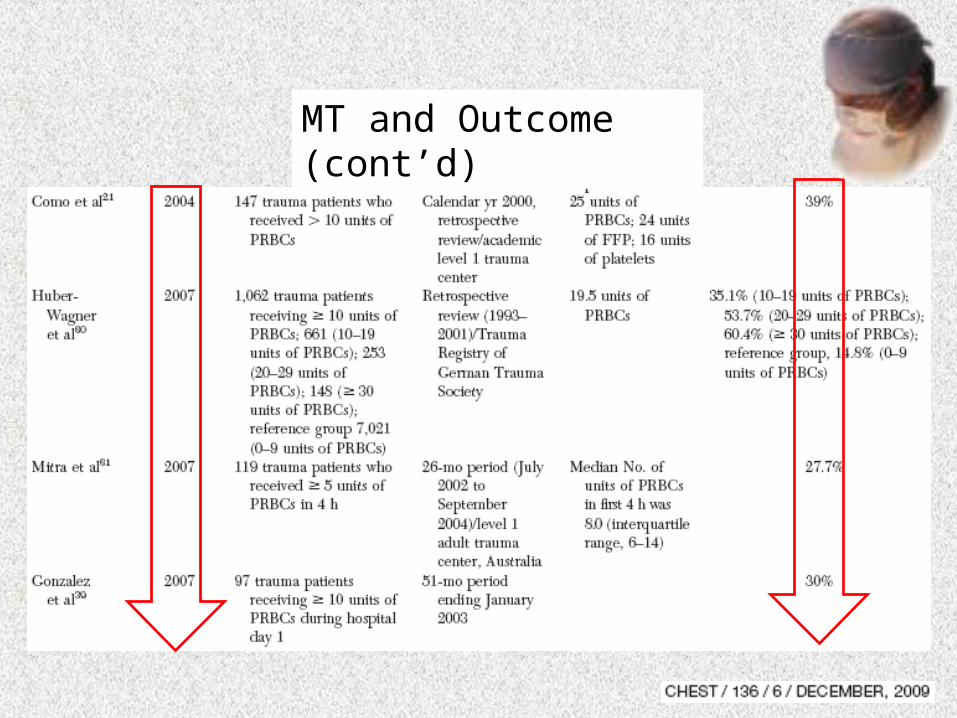
MT and Outcome (cont’d)
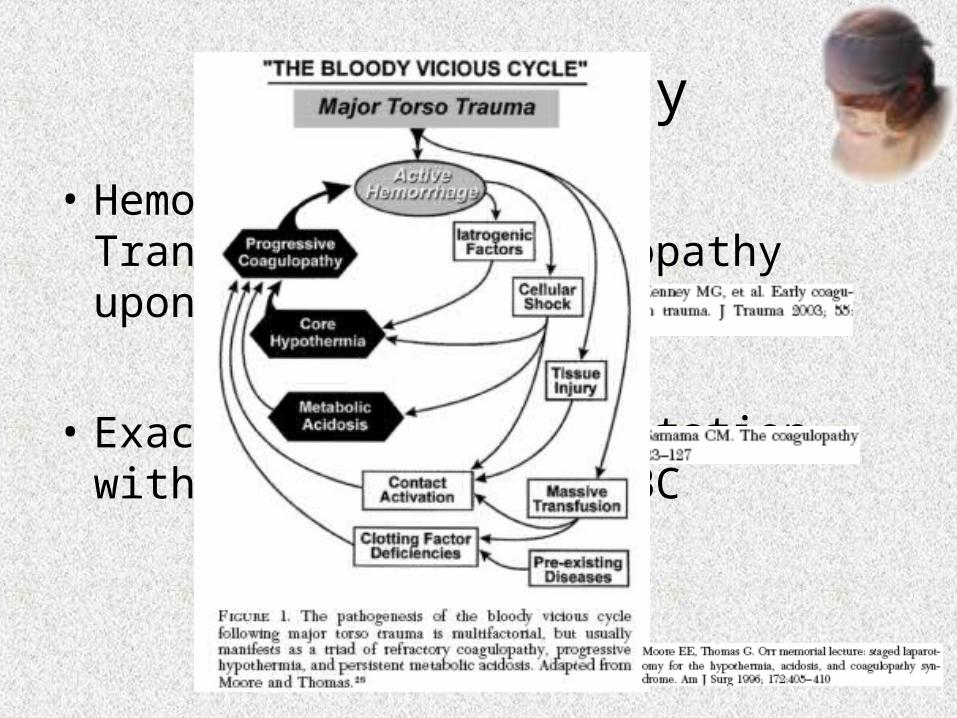
Coagulopathy
• Hemorrhage -> Massive Transfusion -> coagulopathy upon or soon after admission
• Exacerbated by resuscitation with crystalloid & PRBC

Hemostatic Resuscitation
• Hemorrhage control• Normalization of body temperature• Early transfusion of FFP, platelets

FFP : Plt : PRBC

• Multicentre retrospective study• 16 major Level 1 trauma centres in the US• 466 required MT trauma patient• FFP:PRBC, Platelet: PRBC & ISS • independent predictors of 30-day mortality
• 4 groups• High FFP:RBC ≥ 1:2 vs Low FFP:RBC <1:2• High Plt:RBC ≥ 1:2 vs Low Plt:RBC <1:2

Mortality
Survival is associated with increased FFP & Platelet ratio
Best ratio 1:1:1

FFP : Plt : PRBC

Survivial
Early transfusion of high ratio of
FFP:Platelet:PRBC improved survival
Hemostatic Resuscitation
• Hypotensive resuscitation:– Aggressive crystalloid fluid resuscitation in patient
with uncontrolled hemorrhage -> increase hemorrhage & coagulopathy
– Target SBP >90mmHg or Heart rate <130 bpm until hemorrhage is controlled
No consensus yetMore fluid: risk of hemodilution &
disruption of early hemostatic clotsVs
Limit fluid: prolonging shock & cellular ischemia may become
irreversible

Massive Transfusion Protocol
• In the past: – Crystalloid -> PRBC– FFP / Platelets: upon request when there is lab
evidence of coagulopathy
• Current era: – prevention of coagulopathy & thrombocytopenia– PRBC: FFP: Platelet = 1:1:1

MTP
J Am Coll Surg 2009;209: 198–205

• Retrospective review, cohorts• Stanford University Medical Center • Level I trauma Center• MTP since July 2005 – 6 PRBC: 4 FFP: 1 apheresis pack of Platelet
• 2 yrs pre (n=40), post MTP (n=37)• FFP:PRBC ratio the same: 1:1.8 (p=0.97)• Plt : PRBC ratio: 1:1.8 -> 1:1.3 (p=0.05)


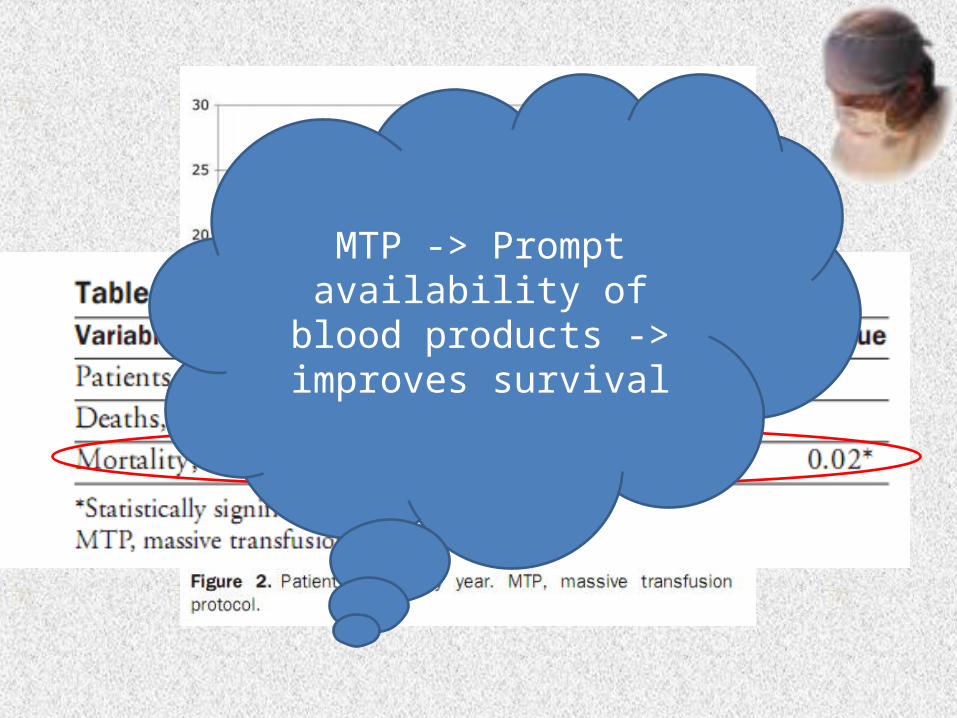
MTP -> Prompt availability of blood products -> improves
survival

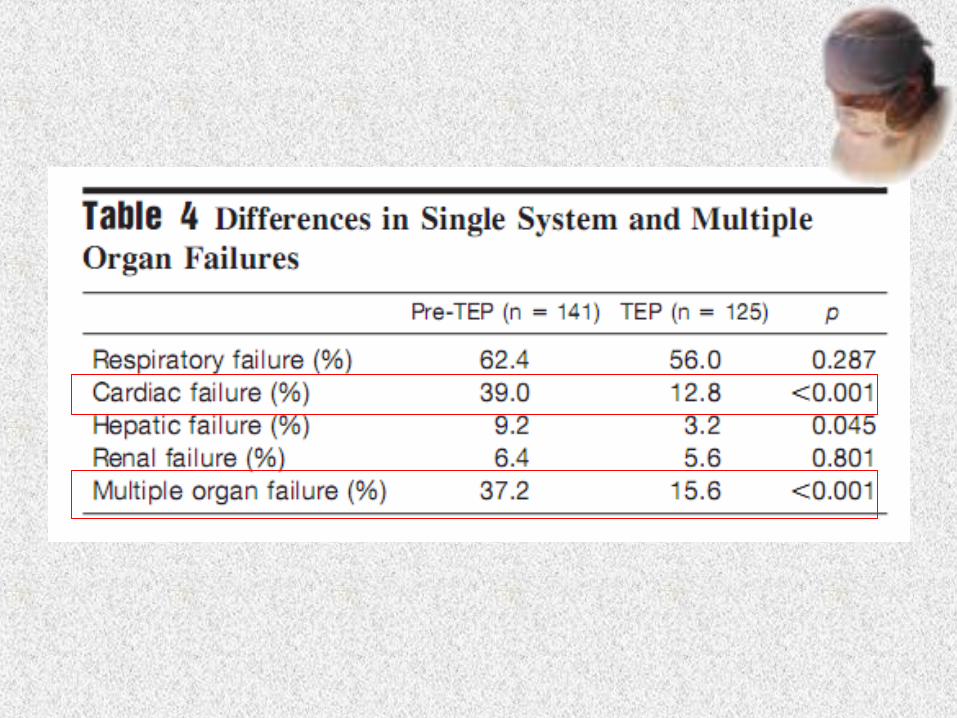
Complications from MTP?
• More multi-organ failure / ARDS?
• Retrospective Cohort• Single Level 1 trauma centre• Trauma Exsanguination Protocol in 1 Feb 2006• PRBC: FFP: Plt = 6:4:2• 2 years pre-TEP (n=141), 2 years TEP (N=125)



Conclusion
• Prevention of coagulopathy• Predefined ratio of FFP: Platelets: PRBC• Applicable to non trauma cases?• Availability of blood products

Thank You


















