Massive Coronary Aneurysm After Multiple Percutaneous Interventions
2
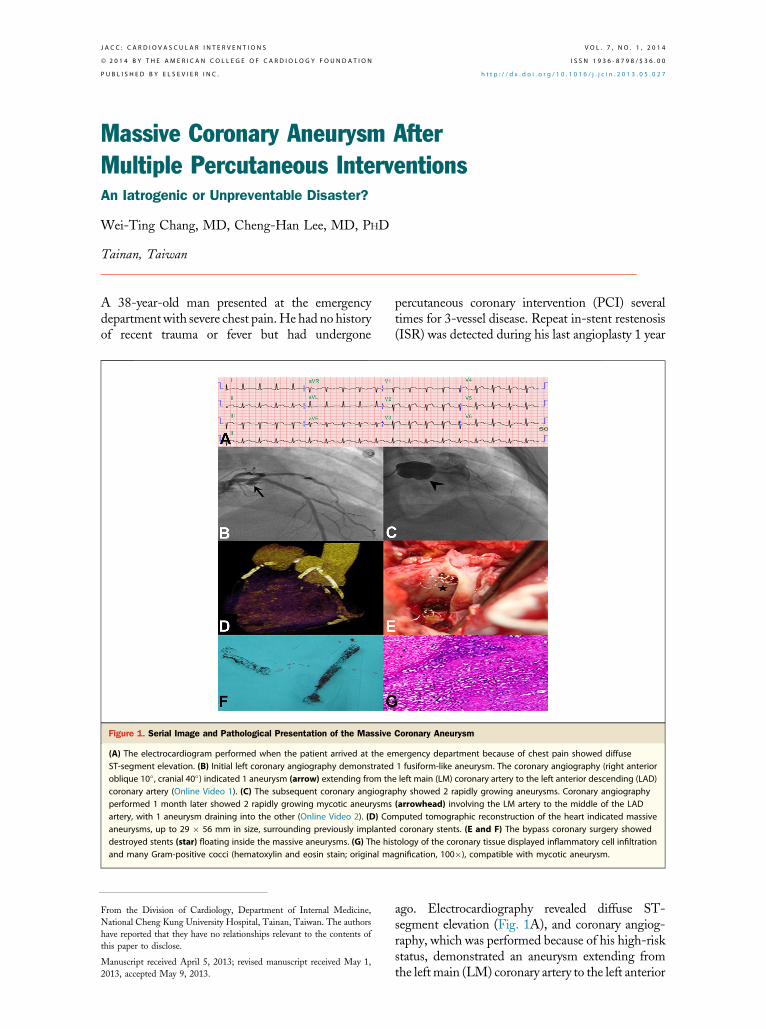
Massive Coronary Aneurysm After Multiple Percutaneous Interventions An Iatrogenic or Unpreventable Disaster? Wei-Ting Chang, MD, Cheng-Han Lee, MD, PHD Tainan, Taiwan A 38-year-old man presented at the emergency department with severe chest pain. He had no history of recent trauma or fever but had undergone percutaneous coronary intervention (PCI) several times for 3-vessel disease. Repeat in-stent restenosis (ISR) was detected during his last angioplasty 1 year ago. Electrocardiography revealed diffuse ST- segment elevation (Fig. 1A), and coronary angiog- raphy, which was performed because of his high-risk status, demonstrated an aneurysm extending from the left main (LM) coronary artery to the left anterior Figure 1. Serial Image and Pathological Presentation of the Massive Coronary Aneurysm (A) The electrocardiogram performed when the patient arrived at the emergency department because of chest pain showed diffuse ST-segment elevation. (B) Initial left coronary angiography demonstrated 1 fusiform-like aneurysm. The coronary angiography (right anterior oblique 10 , cranial 40 ) indicated 1 aneurysm (arrow) extending from the left main (LM) coronary artery to the left anterior descending (LAD) coronary artery (Online Video 1). (C) The subsequent coronary angiography showed 2 rapidly growing aneurysms. Coronary angiography performed 1 month later showed 2 rapidly growing mycotic aneurysms (arrowhead) involving the LM artery to the middle of the LAD artery, with 1 aneurysm draining into the other (Online Video 2). (D) Computed tomographic reconstruction of the heart indicated massive aneurysms, up to 29 56 mm in size, surrounding previously implanted coronary stents. (E and F) The bypass coronary surgery showed destroyed stents (star) floating inside the massive aneurysms. (G) The histology of the coronary tissue displayed inflammatory cell infiltration and many Gram-positive cocci (hematoxylin and eosin stain; original magnification, 100), compatible with mycotic aneurysm. From the Division of Cardiology, Department of Internal Medicine, National Cheng Kung University Hospital, Tainan, Taiwan. The authors have reported that they have no relationships relevant to the contents of this paper to disclose. Manuscript received April 5, 2013; revised manuscript received May 1, 2013, accepted May 9, 2013. JACC: CARDIOVASCULAR INTERVENTIONS VOL. 7, NO. 1, 2014 ª 2014 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-8798/$36.00 PUBLISHED BY ELSEVIER INC. http://dx.doi.org/10.1016/j.jcin.2013.05.027
Transcript of Massive Coronary Aneurysm After Multiple Percutaneous Interventions
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 7 , N O . 1 , 2 0 1 4
ª 2 0 1 4 B Y T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N I S S N 1 9 3 6 - 8 7 9 8 / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R I N C . h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j c i n . 2 0 1 3 . 0 5 . 0 2 7
Massive Coronary Aneurysm AfterMultiple Percutaneous Interventions
An Iatrogenic or Unpreventable Disaster?Wei-Ting Chang, MD, Cheng-Han Lee, MD, PHD
Tainan, Taiwan
A 38-year-old man presented at the emergencydepartment with severe chest pain.He had no historyof recent trauma or fever but had undergone
Figure 1. Serial Image and Pathological Presentation of the Massive
(A) The electrocardiogram performed when the patient arrived at the eST-segment elevation. (B) Initial left coronary angiography demonstratedoblique 10� , cranial 40�) indicated 1 aneurysm (arrow) extending from thcoronary artery (Online Video 1). (C) The subsequent coronary angiograperformed 1 month later showed 2 rapidly growing mycotic aneurysmsartery, with 1 aneurysm draining into the other (Online Video 2). (D) Coaneurysms, up to 29 � 56 mm in size, surrounding previously implantedestroyed stents (star) floating inside the massive aneurysms. (G) The hisand many Gram-positive cocci (hematoxylin and eosin stain; original ma
From the Division of Cardiology, Department of Internal Medicine,
National Cheng Kung University Hospital, Tainan, Taiwan. The authors
have reported that they have no relationships relevant to the contents of
this paper to disclose.
Manuscript received April 5, 2013; revised manuscript received May 1,
2013, accepted May 9, 2013.
percutaneous coronary intervention (PCI) severaltimes for 3-vessel disease. Repeat in-stent restenosis(ISR) was detected during his last angioplasty 1 year
Coronary Aneurysm
mergency department because of chest pain showed diffuse1 fusiform-like aneurysm. The coronary angiography (right anteriore left main (LM) coronary artery to the left anterior descending (LAD)phy showed 2 rapidly growing aneurysms. Coronary angiography(arrowhead) involving the LM artery to the middle of the LADmputed tomographic reconstruction of the heart indicated massived coronary stents. (E and F) The bypass coronary surgery showedtology of the coronary tissue displayed inflammatory cell infiltrationgnification, 100�), compatible with mycotic aneurysm.
ago. Electrocardiography revealed diffuse ST-segment elevation (Fig. 1A), and coronary angiog-raphy, which was performed because of his high-riskstatus, demonstrated an aneurysm extending fromthe left main (LM) coronary artery to the left anterior

J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 7 , N O . 1 , 2 0 1 4 Chang and Lee
J A N U A R Y 2 0 1 4 : 1 0 4 – 5 Massive Coronary Aneurysms After PCI
105
descending (LAD) coronary artery (Fig. 1B andOnline Video1). However, he refused surgical intervention until 1 monthlater, when he underwent treatment because of refractory chestpain and bacteremia caused by Staphylococcus aureus. Surpris-ingly, pre-operative coronary angiography and chest computedtomography revealed 2 rapidly growing mycotic aneurysmsinvolving the LM coronary artery and the mid-LAD coronaryartery. The aneurysms measured up to 29 � 56 mm, and 1 ofthem drained into the other (Figs. 1C and 1D, and OnlineVideo 2). The operation revealed destroyed stents floatinginside the massive aneurysms (Figs. 1E and 1F). Bypasssurgery was performed successfully; however, the patienteventually died of multiorgan failure. An aggressive bacterialinfection was detected in the pathological specimens(Fig. 1G).
Mycotic coronary aneurysms after PCI are rare (0.3% to0.6%) and present between 3 days and 4 years after theprocedure, mostly as fever (1). Catheter-based infectionduring repeated angioplasty is a major risk factor for stentinfection (1,2). In addition, the high pressure used to treatISR may exacerbate vessel-wall inflammation (3). Earlysurgical management is warranted because of the highmortality of mycotic coronary aneurysms (2). Thoughthe incidence of giant coronary artery aneurysm without
rupturing is low, this case indicated that coronary inter-ventions can sometimes lead to disastrous iatrogenic sepsis.
Reprint requests and correspondence: Dr. Cheng-Han Lee,Department of Internal Medicine, National Cheng Kung Univer-sity Hospital, 138 Sheng-Li Road, Tainan 704, Taiwan. E-mail:[email protected].
REFERENCES
1. Chen IC, Chao TH, Wu IH, Kan CD, Fang CC. Afebrile mycoticaneurysm with rupture in right coronary artery after bare-metal stentimplantation. Acta Cardiol Sin 2012;4:344–8.
2. Aoki J, Kirtane A, Leon MB, Dangas G. Coronary artery aneurysmsafter drug-eluting stent implantation. J Am Coll Cardiol Intv 2008;1:14–21.
3. Gautam SR, Mishra D, Goyal BK. Mechanical intervention and coro-nary artery aneurysm. J Invasive Cardiol 2010;22:E213–5.
Key Words: diffuse ST-segment elevation - in-stentrestenosis - mycotic coronary aneurysms.
APPENDIX
For accompanying videos, please see the online version of this paper.