
Massive Allografts in the Treatment of Osteosarcoma and...
11
Massive Allografts in the Treatment of Osteosarcoma and Ewing Sarcoma in Children and Adolescents* BY BENJAMIN A. ALMAN. M.D.I. ANTHONY DE BARI. M.D.S. AND J, IVAN KRAJBICH. M.D.. F.R.C.S.(C)I. TORONTO. ONTARIO. CANADA Investigatior~ perfonned at The Hospital for Sick Chilrirrn. Toronro ABSTRACT: A retrospective review was performed of the results of all allograft reconstructions that had been done after the resection of an osteosarcoma or an Ewing sarcoma in a skeletally immature patient between 1982 and 1989 at The Hospital for Sick Chil- dren in Toronto. There were twenty-six patients. Six reconstructions were intercalary, sixteen were resec- tion arthrodeses, three followed resection of a bone segment including the epiphysis (osteoarticular recon- struction), and one was a replacement of the entire humerus. Resection arthrodesis about the knee was performed with a smooth intramedullary rod and with one growth plate left intact. Six procedures were per- formed in the upper extremity. Excluding the patients who died, the average duration of follow-up was five years and three months. Twenty-one of the twenty-six patients had reached skeletal maturity at the time of follow-up. Eighteen (69 per cent) of the patients had a good or excellent result, four (15 per cent) had a fair result, and four had a failure. Twenty patients (77 per cent) had at least one complication (other than a limb-length discrepancy), and fourteen (54 per cent) sustained at least one fracture of the allograft. Fifteen patients who had had a reconstruction in the lower extremity had survived with survival of the allograft at the time of the latest follow-up. A limb-length discrepancy of at least two centimeters developed in nine of the fifteen pa- tients. Five were managed with a contralateral epiphy- seodesis, and one of them had an unsuccessful attempt at limb-lengthening as well. The patients who had a limb-length discrepancy of more than three centi- meters at the time of follow-up had been significantly younger (p < 0.05) at the time of the reconstruction than those who had a smaller discrepancy. Three allografts (12 per cent), two of which were implanted early in the series, became infected. Soft- *No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article. No funds were received in support of this study. tDepartment of Orthopaedics. New England Medical Center and Tufts University School of Medicine, Box 306, 750 Washington Street. Boston. Massachusetts 021 11. tissue coverage is of paramount importance for the prevention of infection, and we now routinely perform primary muscle (gastrocnemius or latissimus dorsi) transfers when dealing with an inadequate muscle envelope. Twelve patients were followed for more than four years (average, six years and seven months); they had no complications other than increased limb-length dis- crepancy and one subluxation of the shoulder after the first four years following the reconstruction. Although the rate of complications is higher than in adults, allograft reconstruction remains a useful op- tion for the management of skeletally immature indi- viduals. Its use in the lower extremity should be reserved for patients in whom limb-length inequality can be treated easily. Advances in adjuvant therapy and operative tech- nique have made limb-sparing operations an attractive option for the treatment of musculoskeletal sarcomas. The use of a massive allograft is one technique for the reconstruction of massive skeletal defects after opera- tive resection".'".", and there have been several reviews of the te~hnique'.'"~'"."'. complications'."". and rate of suc- CeSS~.~7-~~ of this procedure after resection of tumors. Primary malignant musculoskeletal tumors often develop in children and adolescents. In a series from the Mayo Clinic, approximately 25 per cent of 1274 osteo- sarcomas and 40 per cent of 402 Ewing sarcomas oc- curred in patients who were less than sixteen years old?. Massive allografts have been used in children at least since the early 1980's. Despite this, we know of only a few studies dealing with their use in skeletally immature individuals".". Massive allografts have been used at The Hospital for Sick Children in Toronto for reconstruction after resection of selected osteosarcomas and Ewing sarco- mas since 1982. The purpose of this study was to review the results of this procedure. with specific regard to the rate of complications and of survival of the graft in skeletally immature individuals. Materials and Methods $St. Luke's Hospital, 4884 Berl Drive, Saginaw. Michigan 48604. 9Shriner.s Hospital for Crippled Children, 3101 S.W. Sam Jack- patients had been managed with a massive son Park Road. Portland. Oregon 97201. allograft after the resection of a high-grade osteosar- 54 THE JOURNAL OF BONE AND JOINT SURGERY
Transcript of Massive Allografts in the Treatment of Osteosarcoma and...

Massive Allografts in the Treatment of Osteosarcoma and Ewing Sarcoma in Children and Adolescents*
BY BENJAMIN A. ALMAN. M.D.I. ANTHONY D E BARI. M.D.S.
A N D J , IVAN KRAJBICH. M.D.. F.R.C.S.(C)I. TORONTO. ONTARIO. C A N A D A
Investigatior~ perfonned at The Hospital for Sick Chilrirrn. Toronro
ABSTRACT: A retrospective review was performed of the results of all allograft reconstructions that had been done after the resection of an osteosarcoma or an Ewing sarcoma in a skeletally immature patient between 1982 and 1989 at The Hospital for Sick Chil- dren in Toronto. There were twenty-six patients. Six reconstructions were intercalary, sixteen were resec- tion arthrodeses, three followed resection of a bone segment including the epiphysis (osteoarticular recon- struction), and one was a replacement of the entire humerus. Resection arthrodesis about the knee was performed with a smooth intramedullary rod and with one growth plate left intact. Six procedures were per- formed in the upper extremity. Excluding the patients who died, the average duration of follow-up was five years and three months. Twenty-one of the twenty-six patients had reached skeletal maturity at the time of follow-up.
Eighteen (69 per cent) of the patients had a good or excellent result, four (15 per cent) had a fair result, and four had a failure. Twenty patients (77 per cent) had at least one complication (other than a limb-length discrepancy), and fourteen (54 per cent) sustained at least one fracture of the allograft. Fifteen patients who had had a reconstruction in the lower extremity had survived with survival of the allograft at the time of the latest follow-up. A limb-length discrepancy of at least two centimeters developed in nine of the fifteen pa- tients. Five were managed with a contralateral epiphy- seodesis, and one of them had an unsuccessful attempt at limb-lengthening as well. The patients who had a limb-length discrepancy of more than three centi- meters at the time of follow-up had been significantly younger (p < 0.05) at the time of the reconstruction than those who had a smaller discrepancy.
Three allografts (12 per cent), two of which were implanted early in the series, became infected. Soft-
*No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article. No funds were received in support of this study.
tDepartment of Orthopaedics. New England Medical Center and Tufts University School of Medicine, Box 306, 750 Washington Street. Boston. Massachusetts 021 11.
tissue coverage is of paramount importance for the prevention of infection, and we now routinely perform primary muscle (gastrocnemius or latissimus dorsi) transfers when dealing with an inadequate muscle envelope.
Twelve patients were followed for more than four years (average, six years and seven months); they had no complications other than increased limb-length dis- crepancy and one subluxation of the shoulder after the first four years following the reconstruction.
Although the rate of complications is higher than in adults, allograft reconstruction remains a useful op- tion for the management of skeletally immature indi- viduals. Its use in the lower extremity should be reserved for patients in whom limb-length inequality can be treated easily.
Advances in adjuvant therapy and operative tech- nique have made limb-sparing operations an attractive option for the treatment of musculoskeletal sarcomas. The use of a massive allograft is one technique for the reconstruction of massive skeletal defects after opera- tive resection".'".", and there have been several reviews of the te~hnique'.'"~'"."'. complications'."". and rate of suc- C e S S ~ . ~ 7 - ~ ~ of this procedure after resection of tumors.
Primary malignant musculoskeletal tumors often develop in children and adolescents. In a series from the Mayo Clinic, approximately 25 per cent of 1274 osteo- sarcomas and 40 per cent of 402 Ewing sarcomas oc- curred in patients who were less than sixteen years old?. Massive allografts have been used in children at least since the early 1980's. Despite this, we know of only a few studies dealing with their use in skeletally immature individuals".".
Massive allografts have been used at The Hospital for Sick Children in Toronto for reconstruction after resection of selected osteosarcomas and Ewing sarco- mas since 1982. The purpose of this study was to review the results of this procedure. with specific regard to the rate of complications and of survival of the graft in skeletally immature individuals.
Materials and Methods $St. Luke's Hospital, 4884 Berl Drive, Saginaw. Michigan 48604. 9Shriner.s Hospital for Crippled Children, 3101 S.W. Sam Jack- patients had been managed with a massive
son Park Road. Portland. Oregon 97201. allograft after the resection of a high-grade osteosar-
54 THE J O U R N A L O F B O N E A N D J O I N T S U R G E R Y
MASSIVE ALLOGRAFTS I N THE TREATMENT OF OSTEOSARCOMA AND EWING SARCOMA
coma (stage IIB or 111, according to the classification of Enneking et al.') or an Ewing sarcoma of a long bone at The Hospital for Sick Children in Toronto between 1982 and 1989 were identified and their records were re- viewed. The minimum duration of follow-up was thus three years. except when a patient had died. Two patients were skeletally mature at the time of the reconstruction and were excluded from this investigation. This left twenty-six patients for the study (Table I). Before 1985.
therapy consisted of methotrexate with leucovorin res- cue, cisplatin, and Adriamycin (doxorubicin). Beginning in 1985, cisplatin and Adriamycin were given before the operation and ifosfamide and etoposide were added postoperatively if the rate of tumor necrosis in the re- sected specimen was less than 80 per cent. Bone scans, computed tomography scans, and, later in the study pe- riod, magnetic resonance imaging scans were performed to stage the lesion and to plan the resection.
FIG. I-A FIG. I-B FIG. I-C
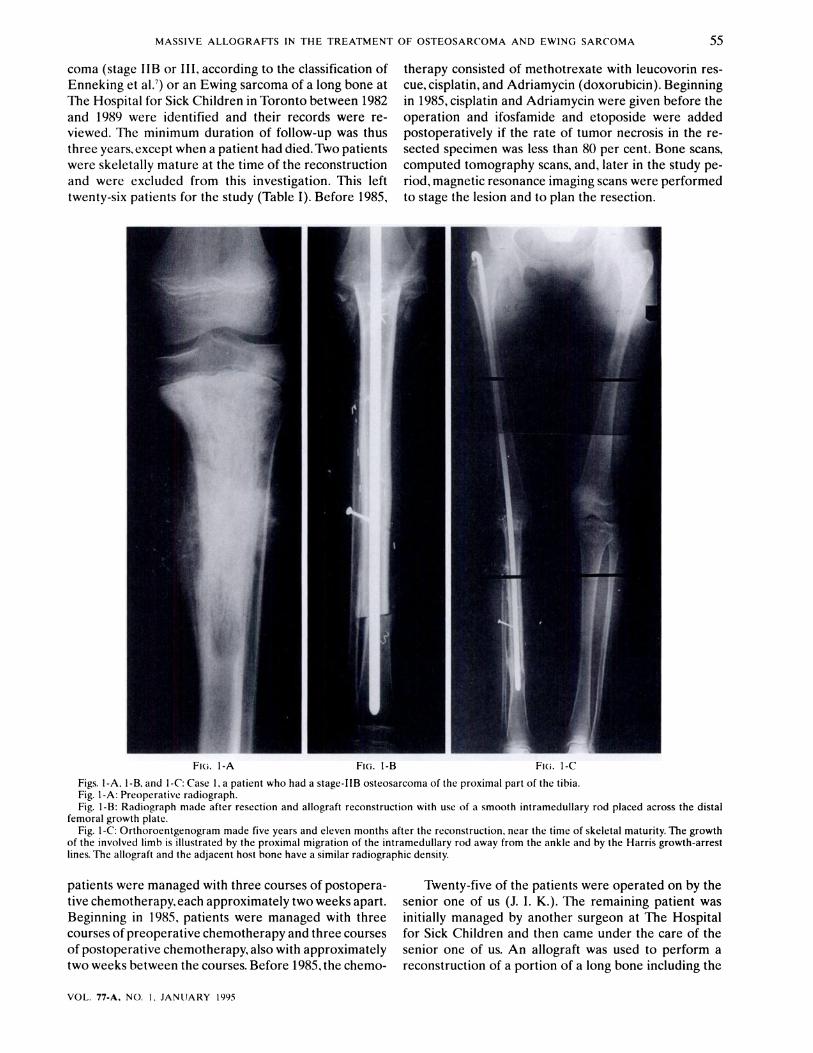
Figs. I-A. 1-B. and I-C: Case I . a patient who had a stage-IIB osteosarcoma of the proximal part of the tibia. Fig. I-A: Preoperative radiograph. Fig. I-B: Radiograph made after resection and allograft reconstruction with use of a smooth intramedullary rod placed across the distal
femoral growth plate. Fig. I-C: Orthoroentgenogram made five years and eleven months after the reconstruction. near the time of skeletal maturity. The growth
of the involved limb is illustrated by the proximal migration of the intramedullary rod away from the ankle and by the Harris growth-arrest lines. The allograft and the adjacent host bone have a similar radiographic density.
patients were managed with three courses of postopera- Twenty-five of the patients were operated on by the tivechemotherapy,each approximately two weeks apart. senior one of us (J. I. K.). The remaining patient was Beginning in 1985, patients were managed with three initially managed by another surgeon at The Hospital courses of preoperative chemotherapy and three courses for Sick Children and then came under the care of the of postoperative chemotherapy,also with approximately senior one of us. An allograft was used to perform a two weeks between the courses. Before 1985, the chemo- reconstruction of a portion of a long bone including the
VOL. 77-A. NO. I , JANIJARY 1995
56 B. A. ALMAN. ANTHONY DE BARI. A N D J. I . K R A J B I C H
TABLE I CHARAC~EKISTICS. COMPLICATIONS. AND FOLLOW-UP OF PA TI EN^ MANAGED WITH ALLOGRAF~ RECONSIRI ' (~~IOK
Age Grade7 and Site of Type of Duration of Complications Status at Follow-up
Case at Op. Type of Tumor Tumor Reconstruction Follow-up and Treatment* Disease Functiont4? (Yrs. + Mos.) (Yrs. + Mos.)
4 12 + 11 IIB osteosarcoma Humerus Complete bone replacement
5 13 + 7 IIB osteosarcoma Tibia Arthrodesis
6 11 + 10 IIB osteosarcoma Tibia Intercalary
7 12 + 1 IIB osteosarcoma Tibia Intercalary
8 10 + 3 IIB osteosarcoma Tibia Arthrodesis
9 9 + 5 IIB osteosarcoma Femur Intercalary
10 10 + 7 IIB osteosarcoma Femur Arthrodesis
11 11 + 8 IIB osteosarcoma Femur Arthrodesis
12 14 + 11 IIB osteosarcoma Tibia Arthrodesis
13 12 + 9 IIB osteosarcoma Xbia Intercalary
14 17 + 2 IIB osteosarcoma Humerus Arthrodesis
15 15 + 7 IIB osteosarcoma Humerus Osteoarticular
16 1 1 + 9 IIB osteosarcoma Humerus Arthrodesis
17 17 + 2 IIB osteosarcoma Tibia Arthrodesis
18 10 + 3 IIB osteosarcoma Femur Arthrodesis
1 9 + 6 IIB osteosarcoma Tibia Arthrodesis 5 + 11 IM rod backed out. Disease-free revised: limb-length discrep.. 2 cm: epiphyseod.
2 15 + 10 IIB osteosarcoma Tibia Arthrodesis 3 + 7 None Disease-free
3 1 2 + 4 IIB osteosarcoma Tibia Arthrodesis 3 + 5$ Non-union at 1 yr.: Metast.. died bone graft. ORIF: infect. at 3 yrs. + 4 mos.: resect. of graft. no reconstr.
0 + lo$ Skin slough at 2 wks.: Metast.. died skin graft
3 + 10 IM rod backed out. Metast. revised: limb-length (pulmon.). discrep.. 1.9 cm: resect. no op.
6 + 0 Fract. at 1 yr. + 8 mos.: Disease-free bone graft. ORIF: limb-length discrep.. 4.8 cm: epiphyseod.
6 + 3 Fract. at 1 yr. + 5 mos.: Metast. bone graft, ORIF: (spine). infect. at 2 yrs.: amput. resect.
8 + 2 Non-union at 1 yr.: Disease-free bone graft. ORIF: fract. at 2 yrs.: bone graft, ORIF: limb-length discrep.. 6 cm: attempted Wagner length. and contralat. epiphyseod.
3 + 8 Fract. at 1 mo.: ORIF. Disease-free revis. of IM rod: fract. at 1 yr. + 5 mos.: bone graft. ORIF: limb-length discrep.. 7 cm: no op.
7 + 2 Fract. at 3 yrs. + 10 mos.: Disease-free bone graft. ORIF: limb-length discrep.. 3 em: epiphyseod.
5 + 9 Limb-length discrep.. Metast. 4 cm: no op. (pulmon.).
resect. 1 + 7$ None Metast.. died 3 + 10 Limb-length discrep.. Disease-free
1.5 cm: no op. 4 + 1 Fract. at 1 yr. + 4 Disease-free
rnos.: bone graft. ORIF: fract. at 2 yrs. + 8 mos.: bone graft. ORIF
3 + 9 None Metast. (pulmon.). resect.
3 + 4 None Disease-free 6 + 2 Non-union at 1 yr.: Disease-free
bone graft. ORIF 6 + 11 Fract. at 2 yrs.: bone Disease-free
graft. ORIF: limb- length discrep.. 5 cm: epiphyseod.
19 1 0 + 2 IIB osteosarcoma Femur Arthrodesis 0 + l l $ Infect. at 6 mos.: amput. Metast.. died
Exc
Exc. Failure
Fair
Good
Exc
Failure
Good
Fair
Good
Exc.
Fair Exc.
Good
Good
Exc.
Exc.
Good
Failure
T H E J O U R N A L OF BONE A N D JOINT SIJRGEKY
MASSIVE ALLOGRAFTS I N THE TREATMENT OF OSTEOSARCOMA AND E W l N G SARCOlMA
TABLE I (cot l f in~ted) CH,IRAC-I.L;HIS'I'I(.S. COMPLICATIONS. AND FOLLOW-UP OF PATIENTS MANAGED WITH ALL.O(;RAR RECONSTRI~CI'ION
Age Grade: and Site of Type of Duration of Complications Status at Follow-up
Case at Op. Type of Tumor Tumor Reconstruction Follow-up and Treatment* Disease FunctionIJt (Yrs . + Mos J (Yrs. + Mo.7.)
20 13 + 10 IIB osteosarcoma Humerus Osteoarticular 3 + 3 Fract. at 6 mos.: bone Local recur.. Failure graft amput.:
metast. (spine). resect.
2 1 12 + l l Ewing sarcoma Tibia Arthrodesis 4 + 1 1 Fract. at 6 yrs. + 6 mos.: Disease-free Exc. immobil.
22 10 + 2 IIB osteosarcoma Humerus Osteoarticular 6 + 6 Fract. at 1 yr.: bone Disease-free Good converted to graft. ORIF: painful arthrodesis shoulder sublux. at
5 yrs. + 4 mos.: shoulder arthrodesis
23 5 + 3 Ewing sarcoma Femur Intercalary 3 + 1 1 Non-union at I yr. + 6 Disease-free Exc. mos.: bone graft. ORIF: fract. at 2 yrs. + 4 mos.: bone graft. ORIF: limb-length discrep.. 3.5 cm: no op.
24 1 1 + 11 111 osteosarcoma Femur Arthrodesis 1 1 + 2 Fract. at 1 yr. + 6 mos.: Metast. bone graft. ORIF: (pulmon.). limb-length discrep., resect. 5.6 cm: no op.
25 16 + 3 IIB osteosarcoma Tibia Arthrodesis 3 + 1 Fract. at 1 yr. + 10 mos.: Metast. Fairs bone graft. O R l F (pulmon.).
resect. 26 15 + 2 IIB ostcosarcoma Femur Intercalary 3 + 9 Fract. at 5 mos.: bone Disease-free Exc.
graft. ORIF: fract. at 1 yr. + I mo.: bone graft. ORIF; fract. at 2 yrs. + 4 mos.: bone graft. O R I F
*IM = intramedullary and O R I F = open reduction and internal fixation. tFor thc patients who died. the functional rating was based on the last evaluation before death. $Interval between the reconstruction and death. $The arthrodesis was converted to a knee arthroplasty.
Good
epiphysis (an osteoarticular reconstruction), an inter- calary reconstruction, or a resection-arthrodesis recon- struction. A common osteoarticular reconstruction was the replacement of the proximal half of the humerus including the humeral articular portion of the shoulder joint. A common intercalary reconstruction was the re- placement of the middle half of the tibial shaft. Fixation was achieved with an intramedullary rod in the resec- tion arthrodeses of the lower extremity and with a single plate in the intercalary reconstructions and in the re- constructions of the upper extremity. When a resection arthrodesis was performed around the knee, either the distal femoral or the proximal tibial growth plate was left intact and the smooth intramedullary rod was placed across the growth plate (Figs. 1-A through 2-H). A smooth intramedullary rod was used in an attempt to allow continued growth from the remaining physis in patients in whom a limb-length discrepancy would oth- erwise be expected. The length of the allograft was cho- sen to achieve an appropriate limb length at the end of growth. Lengthening, however, usually was limited to two centimeters by the neurovascular structures. Autol-
ogous bone graft from the iliac crest was placed around the host-allograft junction and around as much of the allograft as possible.
Chemotherapy was continued after the patient had recovered from the operative procedure. with the first postoperative course usually given two weeks after the operation. The patients were then followed at least every six weeks for the first six months, every three months for the next year and a half. and every six months thereafter. Medical oncologists evaluated the patients for evidence of metastatic disease at regular intervals. Standard radiographs were made at every follow-up visit, and they were supplemented by ortho- roentgenograms, computed tomography scans, bone scans, and magnetic resonance imaging scans as needed. Data from orthoroentgenograms were plotted on the straight-line graph described by Moseley in an attempt to determine relative growth of the treated extremity.
Four patients died during the course of the study, and the information on these patients was obtained from their medical records. The remainder of the pa- tients were seen by us. They were examined clinically
V O L . 77-A. N O . I. J A N U A R Y 199.5
B. A. ALMAN. ANTHONY D BARI. AND J. I . KRAJBICH
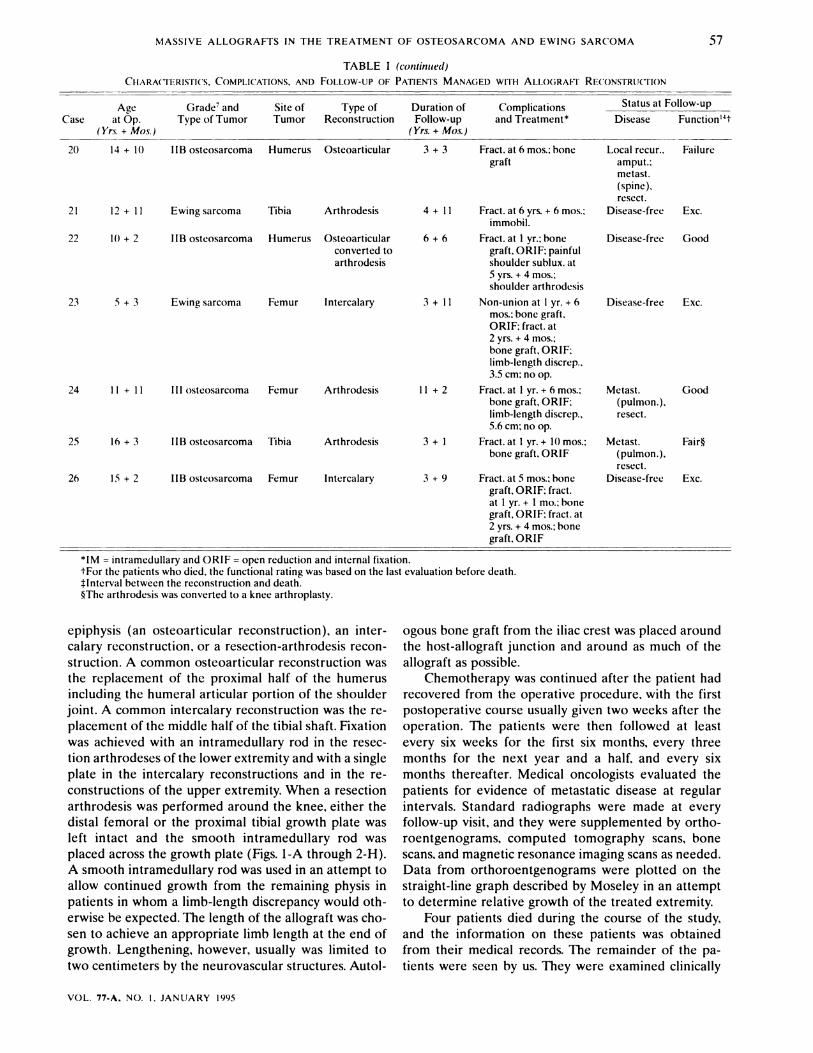
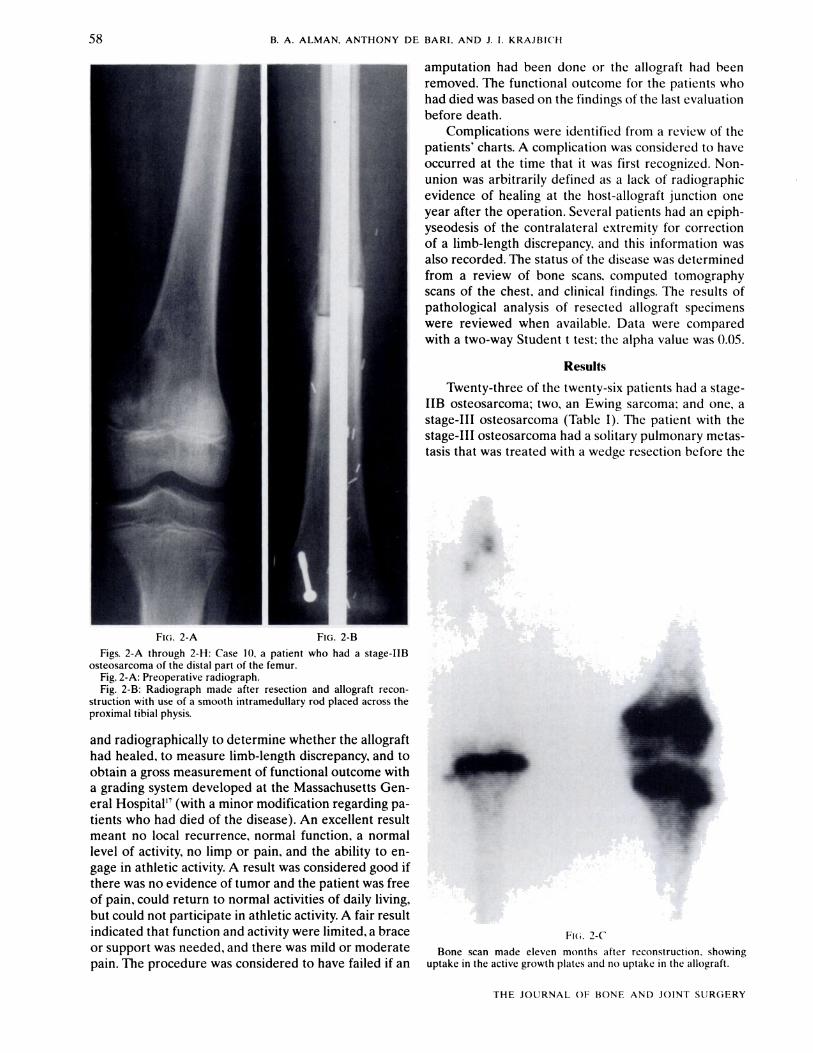
Figs. 2-A through 2-H: Case 10. a patient who had a stage-IIB osteosarcoma of the distal part of the femur.
Fig. 2-A: Preoperative radiograph. Fig. 2-B: Radiograph made after resection and allograft recon-
struction with use of a smooth intramedullary rod placed across the proximal tibia1 physis.
and radiographically to determine whether the allograft had healed, to measure limb-length discrepancy, and to obtain a gross measurement of functional outcome with a grading system developed at the Massachusetts Gen- eral Hospital" (with a minor modification regarding pa- tients who had died of the disease). An excellent result meant no local recurrence, normal function, a normal level of activity, no limp or pain. and the ability to en- gage in athletic activity. A result was considered good if there was no evidence of tumor and the patient was free of pain, could return to normal activities of daily living, but could not participate in athletic activity. A fair result indicated that function and activity were limited. a brace or support was needed, and there was mild or moderate pain. The procedure was considered to have failed if an
amputation had been done or the allograft had been removed. The functional outcome for the patients who had died was based on the findings of the last evaluation before death.
Complications were identified from a review of the patients' charts. A complication was considered to have occurred at the time that it was first recognized. Non- union was arbitrarily defined as a lack of radiographic evidence of healing at the host-allograft junction one year after the operation. Several patients had an epiph- yseodesis of the contralateral extremity for correction of a limb-length discrepancy. and this information was also recorded. The status of the disease was determined from a review of bone scans. computed tomography scans of the chest, and clinical findings. The results of pathological analysis of resected allograft specimens were reviewed when available. Data were compared with a two-way Student t test: the alpha value was 0.05.
Results
Twenty-three of the twenty-six patients had a stage- IIB osteosarcoma; two, an Ewing sarcoma: and one. a stage-111 osteosarcoma (Table I). The patient with the stage-111 osteosarcoma had a solitary pulmonary metas- tasis that was treated with a wedge resection before the
FKi. 2-C
Bone scan made eleven months after reconstruction. showing uptake in the active growth plates and no uptake in the allograft.
THE JOURNAL OF B O N E AND J O I N T SIJRGERY
MASSIVE ALLOGRAFTS I N THE TREATMENT OF OSTEOSARCOMA AND EWlNG SARCOMA
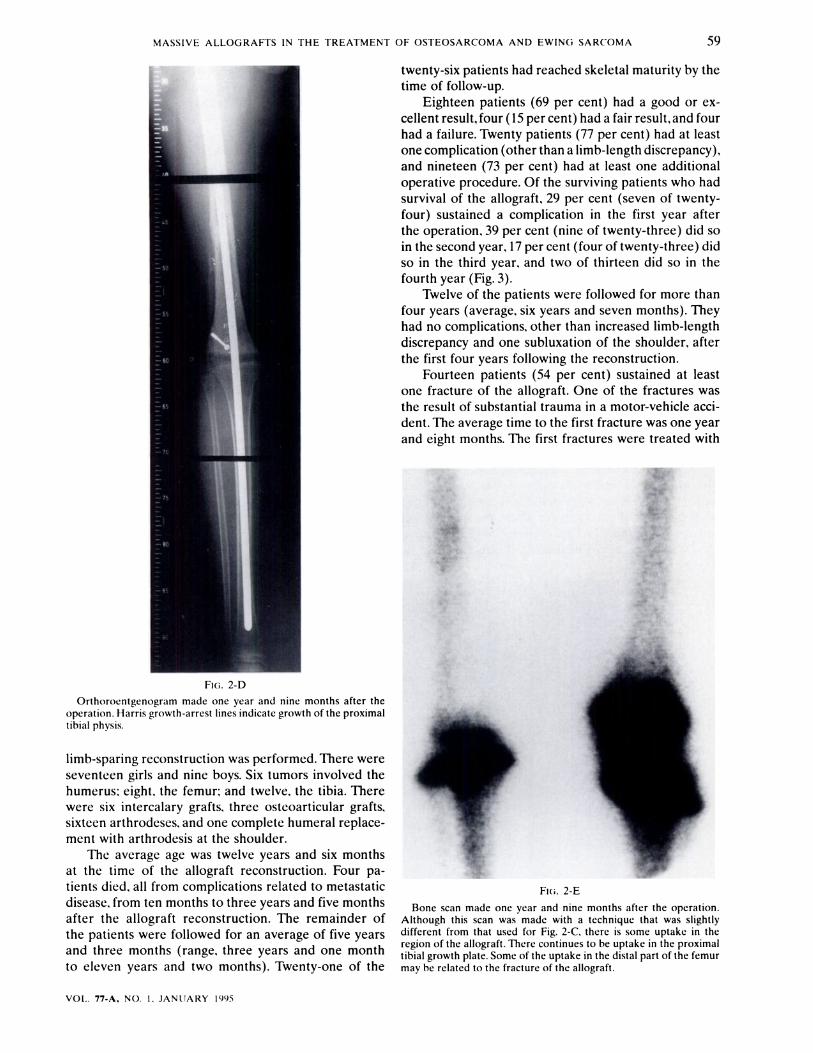
FIG. 2-D Orthoroentgenogram made one year and nine months after the
operation. Harris growth-arrest lines indicate growth of the proximal tibial physis.
limb-sparing reconstruction was performed. There were seventeen girls and nine boys. Six tumors involved the humerus: eight. the femur; and twelve. the tibia. There were six intercalary grafts, three osteoarticular grafts, sixteen arthrodeses, and one complete humeral replace- ment with arthrodesis at the shoulder.
The average age was twelve years and six months at the time of the allograft reconstruction. Four pa- tients died, all from complications related to metastatic disease, from ten months to three years and five months after the allograft reconstruction. The remainder of the patients were followed for an average of five years and three months (range, three years and one month to eleven years and two months). Twenty-one of the
twenty-six patients had reached skeletal maturity by the time of follow-up.
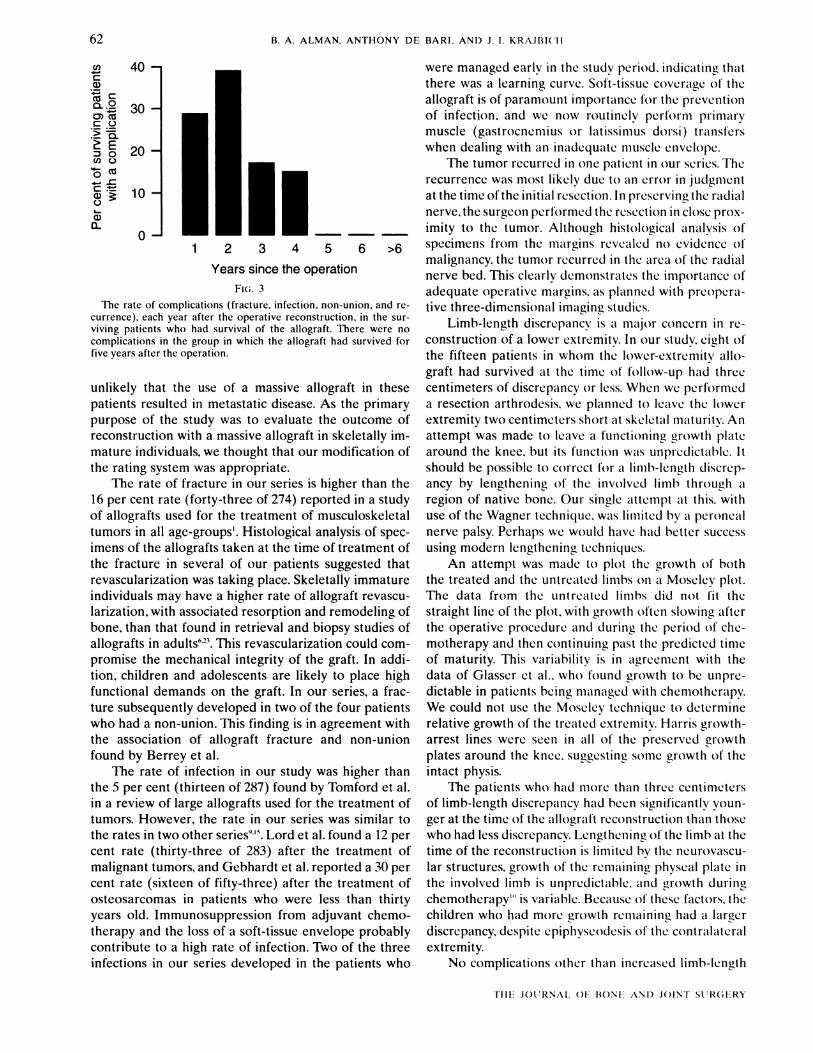
Eighteen patients (69 per cent) had a good or ex- cellent result, four (15 per cent) had a fair result, and four had a failure. Twenty patients (77 per cent) had at least one complication (other than a limb-length discrepancy), and nineteen (73 per cent) had at least one additional operative procedure. Of the surviving patients who had survival of the allograft. 29 per cent (seven of twenty- four) sustained a complication in the first year after the operation, 39 per cent (nine of twenty-three) did so in the second year, 17 per cent (four of twenty-three) did so in the third year, and two of thirteen did so in the fourth year (Fig. 3).
Twelve of the patients were followed for more than four years (average, six years and seven months). They had no complications, other than increased limb-length discrepancy and one subluxation of the shoulder, after the first four years following the reconstruction.
Fourteen patients (54 per cent) sustained at least one fracture of the allograft. One of the fractures was the result of substantial trauma in a motor-vehicle acci- dent. The average time to the first fracture was one year and eight months. The first fractures were treated with
Bone scan made one year and nine months after the operation. Although this scan was made with a technique that was slightly different from that used for Fig. 2-C. there is some uptake in the region of the allograft. There continues to be uptake in the proximal tibial growth plate. Some of the uptake in the distal part of the femur may be related to the fracture of the allograft.
VOL.. 77-A. NO. I. JANLJARY 199.5
B. A . ALMAN. ANTHONY D E BARI. A N D J. I . KRAJBICH
an autologous bone graft and supplemental internal fix- ation in all but one patient, in whom a fracture of a tibial graft healed after immobilization.
Two patients sustained two fractures and one, three fractures. Histological specimens, consisting of curetted material from the allograft, were available from a site distant from the fracture in five of the patients who had had an operation because of the fracture. Four of the specimens showed living bone within a framework of necrotic bone. In the fifth specimen, only necrotic bone was seen.
Four patients (15 per cent) had a non-union. The non-unions were treated with supplemental autologous bone graft, and all healed within one year after this procedure. The allograft later fractured in two of these patients.
The allograft became infected in three patients (12 per cent). and two of them had an amputation. The third patient had a resection of the allograft: a reconstruction was planned, but the patient died of metastatic disease before it could be performed. Two of these patients were operated on early in the series: in fact, an infection developed in two of the first three patients to be man- aged. In the third patient. the infection developed after operative treatment of a fracture of the allograft.
A patient who had an osteosarcoma of the humerus and who had a fracture at one year that was treated with a bone graft and internal fixation subsequently had a subluxation of the shoulder at five years and four months. This patient had an arthrodesis of the shoulder.
One tumor. a proximal humeral osteosarcoma, re-
curred locally. At the time of the initial resection, the tumor had been found to be in close proximity to the radial nerve. The decision had been made to preserve the nerve. and both analysis of a frozen section during the operative procedure and routine histological exam- ination of the resected specimen showed no evidence of tumor at the radial nerve margin. A local recurrence and a solitary spinal metastasis were discovered at the same time. The local recurrence was treated with a modified forequarter amputation. and the spinal metastasis was treated with resection. Histological examination showed the recurrent tumor to be in the radial nerve bed. The patient was free of disease three years and three months after resection of the recurred and metastatic tumors.
Fifteen patients who had had a reconstruction of the lower extremity survived, with the allograft intact. to the time of the latest follow-up. Nine of them had at least two centimeters of limb-length discrepancy, which was treated operatively in five. Operative treatment was of- fered if the discrepancy was predicted to be more than two centimeters at maturity. An epiphyseodesis of the contralateral extremity was recommended when serial orthoroentgenograms showed a progressive discrep- ancy. An epiphyseodesis of one or two growth plates of the contralateral extremity was performed in four pa- tients, and one patient was managed with a Wagner-type limb-lengthening through a region of native bone as well as with a contralateral distal femoral and proximal tibial epiphyseodesis. The lengthening was limited by a peroneal nerve palsy. and the patient was left with a residual six centimeters of discrepancy.
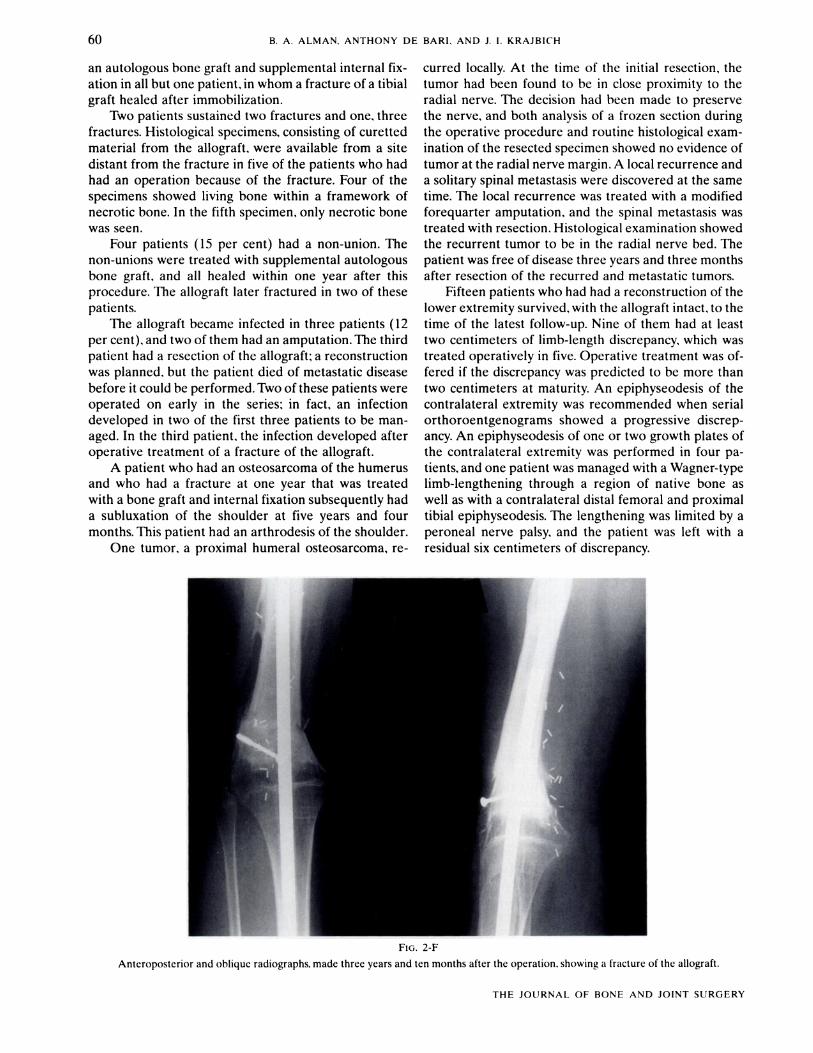
FIG. 2-F
Anteroposterior and oblique radiographs. made three years and ten months after the operation. showing a fracture of the allograft.
THE JOURNAL OF BONE A N D JOINT SURGERY
MASSIVE ALLOGRAFTS I N THE TREATMENT OF OSTEOSARCOMA AND EWlNG SARCOMA
allograft reconstruction and that the long-term perfor- mance of the graft may be inadequate in physically ac- tive individuals.
Previous studies have shown good short-term results in skeletally immature patients. Kohler et al. followed ten children for an average of twenty-two months and found the results to be satisfactory over-all. Gebhardt et al. reported that, of thirty-one patients managed with an allograft because of osteosarcoma when they were less than eighteen years old, seventeen (55 per cent) had a good or excellent result, twelve (39 per cent) had a failure, and three (10 per cent) had a fracture at an average of two years and one month after the procedure. However, the follow-up was short in both of these series; the complications that we reported often occurred sev- eral years after the allograft reconstruction. Dubousset' found late deterioration of the allograft in a group of children managed with allograft reconstruction, and his experience was one of the reasons why we reviewed the records of our patients. In our patients, the complications other than limb-length discrepancy and one subluxation of the shoulder occurred within four years after the operation.
We modified the clinical rating system of the Mas- sachusetts General Hospital", with regard to patients who had died of metastatic disease: instead of rating the results in these patients as failures, we used the rating at the last evaluation before death. There is a large body of evidence that limb-sparing operations with wide re- section of the tumor do not lead to a higher rate of metastatic disease than does amputation. It is highly
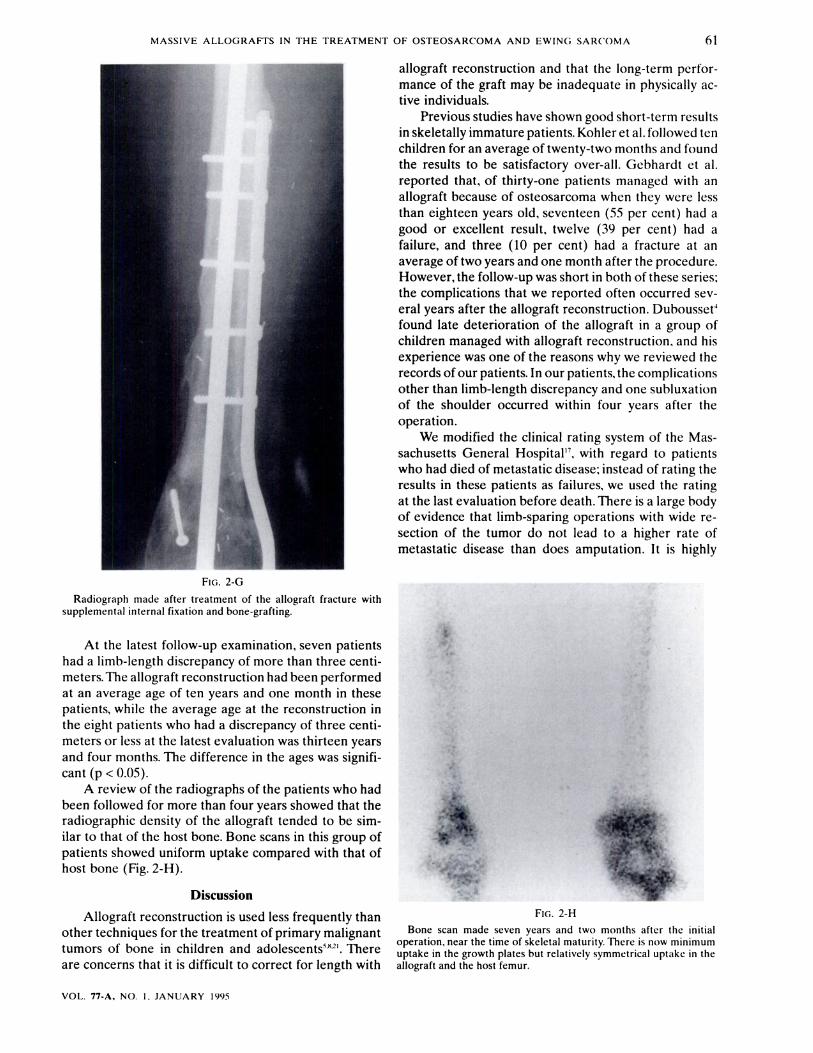
Allograft reconstruction is used less freauentlv than FIG. 2-H - other techniques for the treatment of primary malignant Bone scan made seven years and two months after the initial
operation, near the time of skeletal maturity. There is now minimum tumors of bone in and ad01escents5"21. There uptake in the growth plates but relatively symmetrical uptake in the are concerns that it is difficult to correct for length with allograft and the host femur.
VOL. 77-A, NO. I . JANUARY 1995
62 B. A . ALMAN. A N T H O N Y DE B A R I . AN11 J. I , k ; K h J I 3 I ( ' I l
Years since the operation
The rate of complications (fracture. infection, non-union, and re- currence), each year after the operative reconstruction, in the sur- viving patients who had survival of the allograft. There were no complications in the group in which the allograft had survived for five years after the operation.
unlikely that the use of a massive allograft in these patients resulted in metastatic disease. As the primary purpose of the study was to evaluate the outcome of reconstruction with a massive allograft in skeletally im- mature individuals. we thought that our modification of the rating system was appropriate.
The rate of fracture in our series is higher than the 16 per cent rate (forty-three of 274) reported in a study of allografts used for the treatment of musculoskeletal tumors in all age-groups'. Histological analysis of spec- imens of the allografts taken at the time of treatment of the fracture in several of our patients suggested that revascularization was taking place. Skeletally immature individuals may have a higher rate of allograft revascu- larization. with associated resorption and remodeling of bone, than that found in retrieval and biopsy studies of allografts in adults"". This revascularization could com- promise the mechanical integrity of the graft. In addi- tion, children and adolescents are likely to place high functional demands on the graft. In our series. a frac- ture subsequently developed in two of the four patients who had a non-union. This finding is in agreement with the association of allograft fracture and non-union found by Berrey et al.
The rate of infection in our study was higher than the 5 per cent (thirteen of 287) found by Tomford et al. in a review of large allografts used for the treatment of tumors. However, the rate in our series was similar to the rates in two other series"" Lord et al. found a 12 per cent rate (thirty-three of 283) after the treatment of malignant tumors, and Gebhardt et al. reported a 30 per cent rate (sixteen of fifty-three) after the treatment of osteosarcomas in patients who were less than thirty years old. Immunosuppression from adjuvant chemo- therapy and the loss of a soft-tissue envelope probably contribute to a high rate of infection. Two of the three infections in our series developed in the patients who
were managed early in the study period. indicating that there was a learning curve. Soft-tissue coverage of the allograft is of paramount importance for the prevention of infection. and we now routinely perform primary muscle (gastrocneniius or latissinius dol-si) transfers when dealing with an inadequate niusclc envelope.
The tumor recurred in one patient in our scrics. The recurrence was most likely due to an error in judgment at the time of the initial resection. In preserving the radial nerve. the surgeon performed the resection in close prox- imity to the tumor. Although histological analysis of specimens from the nii~rgins revealed no evidence of malignancy. the tumor recurred in the area of the radial nerve bed. This clearly denionstrates the importance of adequate operative margins. as planned with preopcra- tive three-dimensional imaging studies.
Limb-length discrepancy is a major concern in re- construction of a lower extremity. In our study. eight of the fifteen patients in whom the lower-extremity allo- graft had survived at the time of follow-up had three centimeters of discrepancy or less. When we performed a resection arthrodesis. we planned to leave the lower extremity two centimeters short at skeletal maturity. An attempt was made to leave a functioning growth plate around the knee, but its function was unpredictable. I t should be possible to correct for a limb-length discrcp- ancy by lengthening of the involved limb through a region of native bone. Our single attempt at this. with use of the Wagner technique. was limited by a pcroneal nerve palsy. Perhaps we would have had better success using modern lengthening techniques.
An attempt was made to plot the growth of both the treated and the untreated linibs o n a Moselcy plot. The data from the untreated linibs did n o t f i t the straight line of the plot. with growth often slowing after the operative procedure and during the period of clie- motherapy and then continuing past the predicted time of maturity. This variability is in agreement with the data of Glasscr et al.. who found growth to be unpre- dictable in patients being managed ~vith chemotherapy. We could not use the Moseley technique to determine relative growth of the treated extremity. Harris growth- arrest lines were seen in all of the preserved growth plates around the knee. suggesting some growth of the intact physis.
The patients who had more than three centimeters of limb-length discrep:incy had been significantly youn- ger at the time of the allograft reconstruction than those who had less discrepancy. Lengthening of the limb at the time of the reconstruction is limited by the neurovascu- lar structures. growth of the remaining physeal plate in the involved limb is unpredictable. and growth during chemotherapy'" is variable. Because of these factors. the children who had more growth remaining had a larger discrepancy. despite epipliyseodesis o f the contralateral extremity.
No complications othcr than increased limb-length

MASSIVE ALLOGRAFTS I N THE TREATMENT OF OSTEOSARCOMA A N D EWlNG SARCOMA 63
discrepancy and one subluxation of the shoulder devel- reported on thirty-one patients who had been man- oped more than five years after the operation. By this aged with an expandable prosthesis; five subsequently time, the radiographic appearance of the allograft bone had a revision because of loosening and two had one had become indistinguishable from that of the host bone because of infection. Only seven of the thirty-one pa- and uptake on the bone scan had become more uni- tients needed lengthening of the prosthesis. Of the nine- form. We have not seen late deterioration of an allo- teen patients who had a reconstruction of the lower graft. Histological analysis of specimens taken from extremity and had been followed for at least two years. allografts at operations for fractures suggested that the twelve had a good or excellent result. A major concern allograft undergoes early revascularization, which is as- with the use of prostheses in young individuals is the sociated with a higher prevalence of fracture. Clinical high potential for failure of the implant. Longer follow- findings suggested that this revascularization is followed up is required to assess the risk of failure. by achievement of a steady state, without deterioration Radiation therapy increases the risk of secondary of the allograft. ~arcoma?~.
Other types of limb-sparing treatment that are used Allograft reconstruction is associated with a higher in skeletally immature individuals include rotationplasty, rate of complications in children than in adults. Despite arthroplasty with an expandable prosthesis. and radia- this, it remains a useful option for the treatment of ma- tion therapy. Rotationplasty is a biological reconstruc- lignant musculoskeletal tumors in children and adoles- tion. but its disadvantage is that a prosthesis is required. cents. It is more useful in the upper extremity, the length Gottsauner-Wolf et al. reported the results of rota- of which at maturity is not as great a concern. Its use in tionplasty in seventy patients, thirty-four (49 per cent) of the lower extremity should be limited to patients in whom were less than sixteen years old at the time of the whom a limb-length inequality could be treated with a operation. and they found four pseudarthroses, six in- contralateral epiphyseodesis or perhaps with an ipsilat- stances of ischemia, and eight late fractures. Limb-length era1 limb-lengthening. Alternative techniques, such as discrepancy was not specifically addressed. but severe rotationplasty, should be used for patients who have discrepancy can be avoided by careful preoperative plan- substantial growth remaining. We currently advise chil- ning and prosthetic m~dification'~. dren who are to have an allograft reconstruction that
The advantage of expandable prostheses is that they will probably need at least one additional operative they can be lengthened as the child grows. Kenan et al. procedure.
References 1. Berrey, B. H.; Lord. C. F.; Gebhardt, M. C.: and Mankin, H. J.: Fractures of allografts. Frequency. treatment. and end-results. J. Bone and
Jortlt Srtrg.. 72-A: 825-833. July 1990. 2. Dahlin, D. C., and Unni, K. K.: Bone Tlrttror~. Gerzertll aspect.^ nnd Data on 8,542 Cases. Springfield, Illinois. Charles C Thomas. 1986. 3. Dick, H. M.; Malinin. T. I.: and Mnaymneh. W. A.: Massive allograft implantation following radical resection of high-grade tumors
requiring adjuvant chemotherapy treatment. Clitr. Ortkop.. 197: 88-95, 1985. 4. Dubousset, J.: Personal communication. 5. Dubousset, J.; Missenard, G.; and Kalifa, C.: Management of osteogenic sarcoma in children and adolescents. Clin. Orrhop.. 270: 52-
59, 1991. 6. Enneking, W. F., and Mindell, E. R.: Observations on massive retrieved human allografts. J. Bone and Joitlr Sllrg.. 73-A: 1123-1 142,
Sept. 1991. 7. Enneking, W. F.; Spanier, S. S.; and Goodman, M. A.: Current concepts review. The surgical staging of musculoskeletal sarcoma. J. Bone
c~nd Joint Slrrg.. 62-A: 1027- 1030. Sept. 1980. 8. Finn, H. A., and Simon. M. A.: Limb-salvage surgery in the treatment of osteosarcoma in skeletally immature individuals. Clin. Orthop..
262: 108-1 18. 1991. 9. Gebhardt, M. C.; Flugstad, D. I.; Springfield, D. S.: and Mankin, H. J.: The use of bone allografts for limb salvage in high-grade extremity
osteosarcoma. Clin. Orrhop.. 270: 181-196. 1991. 10. Glasser, D. B.; Duane, K.; Lane, J. M.; Healey, J. H.; and Caparros-Sison, B.: The effect of chemotherapy on growth in the skeletally
immature individual. C'liti. Orthop.. 262: 93-100. 1991. 11. Gottsauner-Wolf, F.; Katz, R.; Knahr, K.; Kristen, H.; Ritschl, P.; and Salzer, M.: Rotationplasty for limb salvage in the treatment of
malignant tumors at the knee. A follow-up study of seventy patients. J. Bone and Joint Surg., 73-A: 1365-1375. Oct. 1991. 12. Kenan, S.; Bloom, M.; and Lewis, M. M.: Limb-sparing surgery in skeletally immature patients with osteosarcoma. The use of an
expandable prosthesis. C'litr. Orrhop.. 270: 223-230. 1991. 13. Kohler, R.; Lorge, F.: Brunt-Mentigny, M.: Noyer, D.: and Patricot, L.: Massive bone allografts in children. Internat. Orrhop., 14: 249-
253. 1990. 14. Krajbich, J. I.: Modified Van Nes rotationplasty in the treatment of malignant neoplasms in the lower extremities of children. Clin.
Orrhop., 262: 74-77. 199 1. 15. Lord, C. F.; Gebhardt, M. C.; Tomford, W. W.: and Mankin, H. J.: Infection in bone allografts. Incidence, nature, and treatment. J. Bone
and Joint Sitrg., 70-A: 369-376. March 1988. 16. Malawer, M. M., and Price, W. M.: Gastrocnemius transposition flap in conjunction with limb-sparing surgery for primary bone sarco-
mas around the knee. Pltrsr. and Reconsrr. Strrg.. 73: 741-750, 1984. 17. Mankin, H. J.; Doppelt, S.; and Tomford, W.: Clinical experience with allograft implantation. The first ten years. Clin. Orthop., 174: 69-
86. 1983.
VOL. 77-A. NO. 1 , JANLIARY 1995

64 B. A. A L M A N . A N T H O N Y D E B A R I . A N D J. I . K R A J B I C ' H
18. Mankin, H. J.: Gebhardt. M. C.: and Tomford, W. W.: The use of frozen cadaveric alloprafts in the manapenlent of patients with hone tumors of the extremities. Orthop. Clitr. North Anlerictr, 18: 275-289. 1987.
19. Mankin, H. J.: Doppelt. S. H.: Sullivan. T. R.: and Tomford. W. W.: Osteoarticular and intercal;ir\ ;~llogr;~ft transplantation In the management of malignant tumors of hone. C'atrcer. 50: 613-630. 1982.
20. Mankin. H. J.: Fogelson. F. S.: Thrasher, A. Z.: and Jaffer, F.: Massive resection and allograft transpl;tnt;~tion in the treatment of malignant hone tumors. N c ~ v O ~ g l a t ~ t l J. Med.. 294: 1247-1255. 1976.
21. Mercuri. M.: Capanna, R.: Manfrini, M.; Bacci, G.: Picci. P.: Ruggieri, P.: Ferruzzi. A.: Ferraro. A.: Donati. D.: Biagini, R.: De Maio. M.: Cazzola, A.: and Campanacci. M.: The management of malignant hone tumors in children and adolescents. C'lirr. Ortllop.. 264: 156- 168. 1991.
22. Moselep C. F.: A straight-line graph for leg-length discrepancies. J. Botle t~tlt i Joitll Srrrg.. 59-A: 174-179. March 1977. 23. Muscolo, D. L.: Caletti, E.: Schajowicz, F.; Araujo, E. S.: and Makino, A.: Tissue-tvping in human nia\sive allografts of frozen hone.
J. Rorlr rtrrtl Joitrt Srtrg.. 69-A: 583-595. April 1987. 24. Parrish. F. F.: Treatment of hone tumors by total excision and replacement with massive autolopous and homolopous grafts. J Rotrr otrtl
Joint Srtrg.. 48-A: 968-990. July 1966. 25. Tomford, W. W.: Thongphasuk. 1.: Mankin, H. J.: and Ferraro. M. J.: Frozen musculoskeletal allografts. A study of the clinical incidence
and causes of infections associated with their use. J. Bone and Joit~t Srtrg.. 72-A: 1137-1 143. Sept. IYR). 26. Tucker, M. A.: D'Angio, G. J.: Boice, J. D., Jr.: Strong, L. C.: Li, F. P.: Stovall, M.: Stone. B. J.: Green, D. M.: Lombardi. F.: Newton. W.:
Hoover, R. N.: and Fraumeni, J. F.: Bone sarcomas linked to radiotherapy and chemotherapy in children. ,Yekc b.'tr,gltrt~tl J. .Urtl.. 317: 588-593. 1987.
T H E J O I ' R N A L . O F B O N E AN[> J O I N T SIJRCiERY


















