Mass Casualty Exercise: Are you Really Prepared?
21
Mass Casualty Exercise: Are You Really Prepared? Megan Coles BSN, RN Clinical Educator Emergency Department Emergency Department Observation PICC and Infusion
Transcript of Mass Casualty Exercise: Are you Really Prepared?

Mass Casualty Exercise: Are You Really Prepared?
Megan Coles BSN, RNClinical Educator Emergency Department
Emergency Department Observation
PICC and Infusion


Definitions
•HICS
•MCI
• START Triage
• Jump START Triage
• ESI
• Trauma Level Activation

MCI Process•HICS Stands up and coordinates six
critical areas:• Communication
• Resources and assets
• Safety and security
• Staffing
• Utilities
• Clinical Activates

Communication
• Confusion during a mass causality incident occurs early due to communication breakdown

What starts the communication breakdown?

Triage• Patient numbers are
doubled and tripled
RED Start Triage
ESI Level 1
Trauma Activation Level 1
Patient with chest wound
1st time patient is counted
2nd time patient is counted
3rd time patient is counted

RED Patient (Immediate)ESI Level 1 Patient that will not survive without immediate treatment but who
have a chance of survival. Requires an intervention (e.g.,
intubation) to be stable. These patient need to be seen
immediately by a physician.
ESI Level 2
T-10 Trauma
Level 1 Trauma
YELLOW Patient (Observation)ESI Level 3 Patient condition is stable for the moment and they are not in
immediate danger of death.Level 2 Trauma
GREEN Patient (Wait)
ESI Level 4 Walking wounded or stable patient that will need medical care
after more critical injuries have been treated.
WHITE Patient (Dismiss) ESI Level 5 Stable patient with minor injuries that do not require a physician care.
No test or procedures need to be done.
BLACK Patient (Expectant)Deceased and those whose injuries are so extensive that they will not be able to survive given
the care that is available

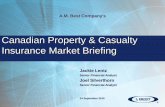
Decreasing the Confusion
•Command Structure in the Emergency Department• Specific roles were identified
• Roles are based on the HICS model
• Identifying treatment Units

HICS

ED Unit Leader
53-4130Director, Manager, ANM
Registration Supervisor
53-4137
Registration Coordinator
Resource Supervisor
53-0464
ANM, Charge Nurse, Staff
Nurse
Triage Supervisor
53-4135
ANM, Charge Nurse
Transport Supervisor
53-4127
EDO Manager, EDO ANM,
Charge Nurse, Staff Nurse
Specialty Supervisor
DECON, Evacuation,
Emerging Infectious Illness
ED Physician Leader
53-4132Medical Director, Senior ED Physician
Treatment
Supervisor
53-4207ANM, Charge Nurse
Charge Nurse Normal Operations
53-4103ANM, Charge Nurse
Charge Nurse Incident Operations
53-4115ANM, Charge Nurse
Charge Nurse, Staff Nurse
Command Structure for the Emergency Department

Job Action Sheets

ED Unit Leader
• Key position in the structure
• Over all control of the Emergency Department
• Only person that communicates to HICS
ED Manager Or Assistant Nurse Manager

Charge Normal Operations
• Hands the patients that are already in the department
• First on to get notification that incident has occurred
• Responsible to starting the process of standing up the Emergency Department Incident Command
Assistant Nurse Manager, Charge Nurse, Staff Nurse

Charge Incident Operations
• Handles all patients coming in from the incident.
• EMS Systems
• Hazardous Materials review
Assistant Nurse Manager, Charge Nurse, Staff Nurse

Transport Supervisor
• Movement of patients within the Emergency Department
• Rapid transport of patient to in house bed assignments
• Transport of patient to the ED observation unit
ED OBS Manager orED OBS Assistant Nurse Manager

Additional Supervisors
• Registration Supervisor
• Resource Supervisor
• Triage Supervisor
• Specialty Supervisor
Assistant Nurse Manager, Charge Nurse, Staff Nurse

Drill Findings
• No patient was lost in the system
• No patient was doubled or tripled.
• Able to track all the patient though the system by disaster number and name

Needs Improvement
• Registration of deceased patient
• Consideration of addition codes being called
• Code Black and Code Orange
• More training of first responders

Additional Training
• First Responders
•Ancillary Staff
•All Hazards approach• Evacuation
• Infectious Illness
• Decon
• Mass Casualty

References• MBA-HCA, C. J. (2016, October 19). Trauma centers: Prepare for mass casualty incidents by
understanding the 10 predictable stages of disruption. Retrieved October 10, 2017, from http://trauma-news.com/2016/07/trauma-centers-prepare-mass-casualty-incidents-understanding-10-predictable-stages-disruption/
• Roundtable on Hospital Communications in a Mass Casualty Radiological Event (2003). Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention.
• Halpern, P., Tsai, M., Arnold, J. L., Stok, E., & Ersoy, G. (2003). Mass-Casualty, Terrorist Bombings: Implications for Emergency Department and Hospital Emergency Response (Part II). Prehospital and Disaster Medicine, 18(03), 235-241. doi:10.1017/s1049023x00001102
• Born, C. T., MD, Briggs, S. M., MD, Ciraulo, D. L., DO, Hammond, J. S., MD, Hirshberg, A., MD, Lhowe, D. W., MD, & O'Neill, P. A., MD. (2007). Disasters and Mass Casualties: !. General Principles of Response and Management. Journal of American Academy of OrthopaedicSurgeons, 15, 388-396. Retrieved August 10, 2017.
• Hirshberg, A. (2004, March). Multiple Casualty Incidents: Lessons From the Front Line. Retrieved October 10, 2017, from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1356229
• Culley, J. M., & Svendsen, E. (2014). A review of the literature on the validity of mass casualty triage systems with a focus on chemical exposures. Retrieved October 10, 2017, from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4187211