MARMOR - Ophthalmology and Art - Simulation of Monet's Cataracts and Degas Retinal Disease
6
SPECIAL ARTICLE Ophthalmology and Art: Simulation of Monet’s Cataracts and Degas’ Retinal Disease Michael F. Marmor, MD M uch has been written about the failing vision of Edgar Degas and Claude Monet, and theore tical ar guments have be en ma de about the exte nt to whic h it wa s or wa s not a factor in their late style. 1-7 Contemporaries of both Degas and Monet noted that their late works were strangely coarse or garish and seemed out of character or even unfitting relative to the finer works that these artists had produced over the years. 8,9 To better understand what Degas and Monet were facing in these late years, it would be helpful to know how they actually saw their world and saw their canvases. This article uses medical knowl- edge and computer simulation to demonstrate their perceptions and show the relevance of their different diseases and styles of painting. METHODS To sim ula te the eff ect s of di sease, an image ofa ne ar ac ui ty te st ca rd (L ig ht ho us e fo r the Bli nd, New Yor k, NY) was mod ifi ed in Pho - toshop (Adobe Systems, San Jose, Calif). Gaussian blur was applied first to fog the char t in corre spon denc e with diff erent lev- els of visual acuity judging by the last line that remained readable. Then, brunes- cen ce was sim ula ted (fr om cli nic al ex per i- ence) by removing blue (effectively add- inga yel lowfilte r) and dar ken ingthe ima ge. Fi gure 1 shows the visual acuity chart as it might appear with a brunescent cataract wi th a vis ual acu ity of 20/20 0. Fin all y, blu r and filter settings appropriate to different stages of Degas’ and Monet’s eye disease we re app lie d to pho tog rap hs of Monet’s gar - den and to works of art. DEGAS Degas (1834-1917) probably had a pro- gress ive retinal disea se that caused cen- tral (macular) damage. 3,10,11 The primary effect of such disease is visual blur (poor vis ual acui ty). Deg as remaine d abl e to wal k aro und com for tab ly lat e in lif e, whi ch sug - gests that the damage did not involve the ret ina l pe rip her y. The re was nev er any in- dication that he had cataracts, although these would have been easily recogniz- able and operable during his lifetime. Degas first talked about “infirmity of sight” in the mid 1880s, although he was stillab le to read thenewspaper. From cli ni - ca l ex pe ri ence, on e ma y surmis e tha t hi s vi - sua l ac uit y wa s in the20/4 0 or 20/5 0 ran ge. 12 By the 1890s, Degas was making frequent ref ere nce in his le tte rs to po or ey es and di f- fic ult y in readin g and wri tin g, and his han d- writing enlarged and became less regular. His vis ual acuity had pro ba bly fal len to the range of 20/100 to 20/200. By the turn of the 20t h cen tur y, he wasquite di sab ledwith vis ual acu ity of 20/ 20 0 to 20 /40 0. Rem ark - ably, however, he continued to do pastels unti l he ha d to moveout ofhis fa mi li ar st u- dio in 1912. Cha nge s in Deg as’ sty le cor rel ate d rath er clo sel y wi th thi s pro gre ssi ve lo ss of vision. His works in the 1870s were drawn quite precisely with facial detail, careful shad- ing , andattention to thefold in g of ba ll et cos- tumes and towels. As his visual acuity be- ga n to di mini sh in the 18 80 s an d 1890s, he drewthe sam e sub jec ts, but the shad ing lines and det ail s of the fac e, hai r, and clo thi ng be- cam e pro gres siv ely less refi ned (Fi gur e 2A, B,andC). On e stud y 13 sho we d tha t thespac - ing of his shading lines increased in pro- por tio n to his fai lin g vis ual acu ity ove r nea rly 3 decades. After 1900, these effects were qui te ext rem e andmany pic tur es see m me re shadows of his customary style (eg, Figure 2C). Bodies were outlined irregu- larly, images were marred by strange blo tche s of col or, and the re was vir tual ly no detailing of faces or clothing. Nothing in Author Affiliation: Department of Ophthalmology, Stanford University, Stanford, Calif. (REPR INTED) ARCH OPHTHALMOL/ VOL 124, DEC 2006 WWW.ARCHOPHTHALMOL. COM 1764 ©2006 American Medical Association. All rights reserved. on May 27, 2008 www.archophthalmol.com Downloaded from
-
Upload
andreapinotti -
Category
Documents
-
view
219 -
download
0
Transcript of MARMOR - Ophthalmology and Art - Simulation of Monet's Cataracts and Degas Retinal Disease

8/11/2019 MARMOR - Ophthalmology and Art - Simulation of Monet's Cataracts and Degas Retinal Disease
http://slidepdf.com/reader/full/marmor-ophthalmology-and-art-simulation-of-monets-cataracts-and-degas 1/6
SPECIAL ARTICLE
Ophthalmology and Art: Simulation of Monet’sCataracts and Degas’ Retinal Disease
Michael F. Marmor, MD
Much has been written about the failing vision of Edgar Degas and Claude Monet,
and theoretical arguments have been made about the extent to which it was or was
not a factor in their late style.1-7 Contemporaries of both Degas and Monet noted
that their late works were strangely coarse or garish and seemed out of character
or even unfitting relative to the finer works that these artists had produced over the years. 8,9 To
better understand what Degas and Monet were facing in these late years, it would be helpful to
know how they actually saw their world and saw their canvases. This article uses medical knowl-
edge and computer simulation to demonstrate their perceptions and show the relevance of their
different diseases and styles of painting.
METHODS
To simulate the effects of disease,an imageofa near acuity test card(Lighthouse for theBlind,NewYork, NY)wasmodified in Pho-toshop (Adobe Systems, San Jose, Calif).Gaussian blur was applied first to fog thechart in correspondence withdifferentlev-els of visual acuity judging by the last linethat remained readable. Then, brunes-cence was simulated (from clinical experi-ence) by removing blue (effectively add-inga yellowfilter) anddarkeningthe image.Figure 1 shows the visual acuity chart asit might appear with a brunescent cataractwith a visual acuity of 20/200. Finally, blurand filter settings appropriate to differentstages of Degas’ and Monet’s eye diseasewere applied to photographs ofMonet’s gar-den and to works of art.
DEGAS
Degas (1834-1917) probably had a pro-gressive retinal disease that caused cen-tral (macular) damage.3,10,11 The primaryeffect of such disease is visual blur (poorvisual acuity).Degas remained able to walkaround comfortably late in life, which sug-gests that the damage did not involve theretinal periphery. There was never any in-dication that he had cataracts, althoughthese would have been easily recogniz-able and operable during his lifetime.
Degas first talked about “infirmity of sight” in the mid 1880s, although he wasstill able to read thenewspaper. From clini-cal experience, one may surmise that his vi-sual acuity was inthe20/40 or 20/50 range.12
By the 1890s, Degas was making frequentreferencein hisletters to poor eyes anddif-ficulty in reading andwriting, andhishand-writing enlarged and became less regular.Hisvisual acuity had probably fallen to therange of 20/100 to 20/200. By the turn of
the20th century, he wasquitedisabledwithvisual acuity of 20/200 to 20/400. Remark-ably, however, he continued to do pastelsuntil he had to moveout ofhis familiar stu-dio in 1912.
Changes in Degas’style correlated ratherclosely with this progressive loss of vision.His works in the 1870s were drawn quiteprecisely with facial detail, careful shad-ing, andattentionto thefolding ofballet cos-tumes and towels. As his visual acuity be-gan to diminish in the 1880s and 1890s, hedrewthe same subjects,buttheshadinglinesanddetails of theface, hair, andclothing be-
came progressivelylessrefined(Figure 2A,B,andC). One study13 showed that thespac-ing of his shading lines increased in pro-portion to hisfailing visualacuityover nearly3 decades. After 1900, these effects werequite extreme andmanypicturesseem mereshadows of his customary style (eg,Figure 2C). Bodies were outlined irregu-larly, images were marred by strangeblotches of color,andthere wasvirtually nodetailing of faces or clothing. Nothing in
Author Affiliation: Department of Ophthalmology, Stanford University, Stanford,Calif.
(REPRINTED) ARCH OPHTHALMOL/ VOL 124, DEC 2006 WWW.ARCHOPHTHALMOL.COM1764
©2006 American Medical Association. All rights reserved. on May 27, 2008www.archophthalmol.comDownloaded from

8/11/2019 MARMOR - Ophthalmology and Art - Simulation of Monet's Cataracts and Degas Retinal Disease
http://slidepdf.com/reader/full/marmor-ophthalmology-and-art-simulation-of-monets-cataracts-and-degas 2/6
Figure 1. Visual acuity chart showing the blurringand color effects of a disabling brunescent cataractwith a visual acuity of 20/200.
B
D
A C
FE
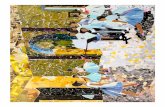
Figure 2. Degas’ paintings of nude bathers, showing the change in style (less refinement) over the years from approximately 1885 to 1910. A, Woman Combing Her Hair (1886; pastel, 5552 cm); Hermitage Museum, St Petersburg, Russia/Bridgeman Art Library. B, After the Bath, Woman Drying Herself (1889-1900;pastel, 6859 cm); Samuel Courtauld Trust, Courtauld Institute of Art Gallery, London, England/Bridgeman Art Library. C, Woman Drying Her Hair (1905; pastelon paper, 71.462.9 cm); Norton Simon Art Foundation, Pasadena. The same paintings were then blurred to the level of Degas’ eyesight at the time of thepainting. D, Woman Combing Her Hair blurred to a visual acuity of 20/50. E, After the Bath, Woman Drying Herself blurred to a visual acuity of 20/100. F, Woman Drying Her Hair blurred to a visual acuity of 20/300. Note that the shading appears more graded and natural in the blurred images than in the original works.
(REPRINTED) ARCH OPHTHALMOL/ VOL 124, DEC 2006 WWW.ARCHOPHTHALMOL.COM1765
©2006 American Medical Association. All rights reserved. on May 27, 2008www.archophthalmol.comDownloaded from

8/11/2019 MARMOR - Ophthalmology and Art - Simulation of Monet's Cataracts and Degas Retinal Disease
http://slidepdf.com/reader/full/marmor-ophthalmology-and-art-simulation-of-monets-cataracts-and-degas 3/6
Degas’ correspondenceindicatedthat
he was consciously tryingto be moreexpressionistic or abstract; in fact, hispastels were drawn on larger andlarger expanses of paper as hestruggled to work. One critic wrotethat “thesesketches arethetragicwit-nesses ofthis battle oftheartistagainsthis infirmity.”14 One may reason-ably ask whether Degas intendedthese images to appear to us the waythey do and why he continued toworkwhentheproduct seemedsooutof line with histraditional style.Someanswers maylie in the recognitionof
how these works appeared to him.Figure 2D, E, and F show thesesame works adjusted (through com-puter simulation) to the level of De-gas’ visual acuity at the time that hemade them. These simulations donot alter colors since color discrimi-nation loss with maculopathy is usu-ally mild and is not consistent. Thestriking findingis thatDegas’ blurredvision smoothed out much of the
graphic coarseness of his shading
and outlines. One might even saythat the works appear “better”through his abnormal vision thanthrough our normal vision.
How can this be? Itreflects, inlargemeasure, the particular style of De-gas’ work. He wasnot recording pre-cise landscapes or portraits as wereRembrandt or Cassatt (who stoppedpainting when cataracts blurred hervision). Degas’ main concernwastheshape andpostureof his subjectsandtheir setting in space, andthesechar-acteristics are easily discernible even
with poor vision. Although he musthave known through tactile feed-back (and perhaps by close-up ex-amination) that he wasusingcoarserlines, when he stood back to look atthe works,he saw well-shadednudesand dancers. I suggest that this cu-riously beneficial effect of visual loss,relative to Degas’ style, helps to ex-plain why he continued to work. Tohim, these late works looked simi-
lar to his earlier ones, and he could
not effectively judge or understandthe impression these works wouldmake on viewers with normalvision.
MONET
The situation was different for Mo-net (1840-1926). We know frommedical records and correspon-dence that he had cataracts thatworsened steadily over the decadefrom 1912 to 1922.4-6,15 Slowly pro-gressive age-related cataracts
(nuclear sclerosis) manifest as yel-lowing and darkening of thelensthatare directly visible to an examiningophthalmologist and have a majoreffect on color perception as well asvisual acuity. The visual simula-tions of this study are based on es-timation of the lens discolorationthat is typically associated with dif-fering levelsof visual acuity loss fromchronic nuclear sclerotic cataracts.
B
D
A
C
Figure 3. Monet’s lily pond and the Japanese bridge at Giverny, France. A, Photograph of the bridge as it appears today (courtesy of photographer ElizabethMurray). B, Monet’s Water Lily Pond , a painting of the pond and bridge before any visual symptoms (1899; oil on canvas, 89 92 cm); National Gallery, London,England/Bridgeman Art Library. C, The same photograph of the bridge, blurred as it might appear through a moderate nuclear sclerotic cataract. D, The samephotograph of the bridge as seen through a disabling cataract with a visual acuity of 20/200.
(REPRINTED) ARCH OPHTHALMOL/ VOL 124, DEC 2006 WWW.ARCHOPHTHALMOL.COM1766
©2006 American Medical Association. All rights reserved. on May 27, 2008www.archophthalmol.comDownloaded from

8/11/2019 MARMOR - Ophthalmology and Art - Simulation of Monet's Cataracts and Degas Retinal Disease
http://slidepdf.com/reader/full/marmor-ophthalmology-and-art-simulation-of-monets-cataracts-and-degas 4/6
Monet was aware of his failing vi-sion in 1912 andconsultedseveraldif-ferent ophthalmologists, who diag-nosed cataracts.4-6,15 Surgery wasrecommendedfor the worse eye, butMonet wasvery resistant even thoughtheoperationwaswell establishedandrelatively safe at this time. Interest-ingly, he was worried that his color
perception would be altered by thesurgery (although one might arguethat it would become more normal).Since Monet only described slightlyreduced visionandwashaving noma- jor difficulties with his art or his per-sonallife, his visual acuity in1912wasprobably no worse than 20/50.
By 1914 to 1915, Monet’s visualdifficulties were becoming more se-rious.He wrote that “colors no longerhad the sameintensity for me . . . redshad begun to look muddy . . . mypainting was getting more and more
darkened.”9
He felt that he could nolonger distinguish or choose colorswell and was “on the one hand trust-ing solely to the labels on the tubesof paint and, on the other, to force of habit.”9 He could still read and writewith effort, so I would estimate thathis visual acuityin 1918 was near 20/ 100. However, the yellowing of hislenscaused greater difficultywith hisart than the blur. Figure 3A and Bcomparea photographof Monet’sgar-den and a painting of the scene from1899 (when his vision was unim-
paired). Figure 3C shows the gardenas it would have appeared to Monetaround1915.Most colors arestill dis-tinguishable, but there is an overrid-ingyellowish cast and a loss of subtlecolordiscriminations.Figure4AandB showa waterlilypainting from 1915to 1917 as it appears to us and as itwould have looked to Monet at thattime.
I must digress at thispoint tonotethat artists canrespond in severaldif-ferent ways to a yellow filter (cata-ract) in front of their world, and one
cannot predictnecessarily howit willinfluence their art. Because cata-racts are chronic, a patient may notbe aware that the world looks yel-lowish (as there are no normal col-ors with which to compare). How-ever, whether an artist recognizestheyellow bias or not, there will be achoice between painting a yellow-ish world or adding extra blue ascompensation (eg, to make the sky
appear “properly” blue). Further-more, the artist may mix these tech-niques with Monet’s approach of painting by experience and choosecolors from habit rather than obser-vation. The idea that the artist willself-correct, ie, choose colors bymatching the canvas to the scene,does not hold because certain col-ors that are different on the palettewill look the same through the cata-ract (eg, yellow and white).
Between 1919 and 1922, Monetwas fearful that he might have to stop
painting. He would only paint dur-ing certain hours when the lightingwas optimal, and he was well awarethat colors were lost in the yellowblur of his vision that made his gar-den appear severely monotone(Figure 3D). His visual acuity wasrecorded in 1922 to be 20/200 in thebetter eye.
As with Degas, we find strikingchanges in thestyle of Monet’s paint-
ings during the period of progres-sive visual failure. Compare paint-ings of the lily pond done in 1899(Figure 3B), in 1915 to 1917(Figure 4A), and around 1922(Figure 5A and C). These late paint-ings are almost abstract in the appli-cations of paintand show a predomi-nant red-orange or green-blue tonethat is quite different from the subtlecolor shading that characterizes Mo-net’s earlier Impressionistic work. Aswith Degas, there is nothing in Mo-net’s correspondence to suggest that
hehadany intention ofmimickingtheabstractions and distortions ex-plored by other painters in the early20th century.
However, visual failure affectedMonet differentlythanit affectedDe-gas. Monet’s mature style was not de-pendent on the outliningof figuresorthe subtle shading of figures andclothing,andhisapplicationsof paintwere larger than those of Degas.
BA
C
Figure 4. Water lily pond. A, Monet’s painting Waterlilies done with moderate cataract (1915; oil oncanvas, 130153 cm); Musee Marmottan, Paris, France/Br idgeman Art Library. B, The same imageblurred as it would have appeared to Monet through the cataract. C, Monet’s painting Morning With Weeping Willows , detail of left section, done after the cataract was removed (1915-1926; oil on canvas,200425 cm); Musee de l’Orangerie, Paris/Giraudon/Bridgeman Art Library.
(REPRINTED) ARCH OPHTHALMOL/ VOL 124, DEC 2006 WWW.ARCHOPHTHALMOL.COM1767
©2006 American Medical Association. All rights reserved. on May 27, 2008www.archophthalmol.comDownloaded from

8/11/2019 MARMOR - Ophthalmology and Art - Simulation of Monet's Cataracts and Degas Retinal Disease
http://slidepdf.com/reader/full/marmor-ophthalmology-and-art-simulation-of-monets-cataracts-and-degas 5/6
Whenwe look through Monet’s eyesat the late paintings, we see that al-thoughhe wouldhave recognized therelative coarseness of his brush-strokes, he could not recognize thetrue colors of his paintings. In 1914to 1917, his color perceptions were
dulled (Figure 4A and B), but to-ward 1922, images that are strik-ingly orange (Figure 5A) or strik-ingly blue (Figure 5C) were to himalmost indistinguishable as a murkyyellow-green (Figure5B andD).Evenif he painted these works accordingto habit, he could not judge theeffectthat he was having on theviewer, norcould he refine the works withoutrisking errors in judgment.
It is very difficult for us a cen-tury later to know whether theseworks appear to us as Monet wantedthem to appear. Monet finally ac-quiesced to cataract surgery, whichwas performed in 1923. Afterward,he destroyed many of his late can-
vases. Many of those that remain doso only because they were salvagedby family and friends. Virtually allof his paintings in this late style areundated, but there is a JapaneseBridge dated 1919 and a House andGarden dated 1922, which leads meto believe that these late-style workswere done during his period of se-verely impaired vision. Of course,wedo not know the degree to which
Monet accepted or liked these sal-vaged works, and we also do notknow whether some of these can-vases might have been reworked af-ter his cataract surgery.
Monet did very well with cataractsurgery and regainedacceptable read-
ing vision. He was acutely aware of changes in colorperception in theeyethatunderwent surgery, andhe com-plained vigorously for more than ayear that the world appeared eithertoo yellow or too blue.15 He finally re-gained confidence in his view of theworld in 1924 and worked vigor-ously to refine the great Water Lilycanvases now hanging in the Museede l’Orangerie, Paris, France. It must
B
D
A
C
Figure 5. Monet paintings of the pond and Japanese bridge done about the time of his most severe visual disability. A, The Japanese Bridge at Giverny (1918-1924;oil on canvas, 89100 cm); Musee Marmottan, Paris, France/Giraudon/Bridgeman Art Library. This version was done with a predominance of orange. B, The imageas it would have appeared to Monet through a disabling nuclear sclerotic cataract with a visual acuity of 20/200. C, The Japanese Bridge at Giverny (1918-1924; oil oncanvas, 89100 cm); Musee Marmottan, Paris/Giraudon/Bridgeman Art Library. This version was done with a predominance of blue. D, The image as it would beseen through a disabling cataract with a visual acuity of 20/200. Note the surprising color constancy of B and D despite the marked differences between A and C.
(REPRINTED) ARCH OPHTHALMOL/ VOL 124, DEC 2006 WWW.ARCHOPHTHALMOL.COM1768
©2006 American Medical Association. All rights reserved. on May 27, 2008www.archophthalmol.comDownloaded from

8/11/2019 MARMOR - Ophthalmology and Art - Simulation of Monet's Cataracts and Degas Retinal Disease
http://slidepdf.com/reader/full/marmor-ophthalmology-and-art-simulation-of-monets-cataracts-and-degas 6/6
benotedthatthe style ofthese “granddecorations” clearly harkens back tothat of his earlier paintings (com-pare Figure 4C with Figure 3B andFigure 4A). Thus, it seems unlikelythat he had adopted or espoused hisbroader style from 1919 to 1922 en-tirely byfreechoice or that he was en-tirely pleased with it.
COMMENT
Withrespect to seeing scenes or sub- jects, Degas hadfewer problems thanMonet, even though Degas’ visualacuity fell to lower levels. His mainsubject was the female form, whichwas large relative to even poor levelsof visual acuity so that his visual losswas not an impediment to planningthe organization of his pictures. Thesituation was more complicated forMonet.Theblurring ofvisionfrom his
cataract was not an impedimentto theorganizationofhispictureseither,butthe loss of color perception created amajor problem. His goal in paintingwas to highlight variations amongtimes of day, seasons, lighting, andshadows. These judgments becamenearly impossible during the severalyearsprior to his cataract surgery. Hecould use memory from 50 years of experience as a painter to choose col-ors and to try to create an impres-sionistic aura. However, weknow thathe took canvases outdoors when the
lighting was favorable, so he musthave felt that even distortedobserva-tions were still relevant.
With respect to the application of pastel or paint, both Degas and Mo-net struggled when their visual acu-ity fell to levels at which it was diffi-cult to paint details. Degas producedcoarser shading lines and less refine-ment in the outlining of his subjects,and Monet began to create his freerstyleevenbefore hewas strictlyforcedto do so. Degas had for many yearsuseda limited number ofcolorsin his
works and these were often ratherbright, so that even if his color per-ceptionwas not entirelynormal withhis maculopathy, this was not a ma- jorimpediment to histechnique. Mo-net, in contrast, must have struggledmightily as he looked out into amurky yellow-browngardenandtriedto decide what subtle impression tocreate on the canvas. He recognized
that he could not see colors well onhis palette and chose tubes by theirlabels. However, he couldnotmixcol-ors by observation or make refine-ments that had been a major part of his technique. The use of colors di-rectly from the tube may account forsome of the curiously intense colorsin his late works.
With respect to the impact of vi-sual loss on the artists’ judgment, weagain find differences between De-gas and Monet. The effect of Degas’maculopathy was to blur his ownview of the coarse shading and poordelineation in his late works so thatthey would appear smoother andmore normalto him than to us. Thisblurring of the works, given Degas’particular style, may have encour-aged him to continue to paint withfailing vision and accounted in partfor his acceptance of (or at least will-
ingness to complete)worksthat seemcuriously crude to our unblurredeyes. Monet did not have such luckwith respect to his cataracts. Theblur-ring of vision did not seriously alterhisbasic Impressionisticstyle,buthiscataracts severely changed and chal-lenged the marvelous qualities of color in his works. From his corre-spondence, we know that he wasaware of his altered color percep-tion andthat he thought he was com-pensating. However, it is very diffi-cult to know how well he achieved
this since he could not judge for him-selfthecanvaseshe created.If, infact,he was pleased with what he saw,then we with normal vision are notseeing what he intended.
It is important to emphasize thatI have described the effects of retinaldamage and cataract on Degas andMonet becausewe have good histori-cal documentation of the visual lossthat afflicted these 2 great artists. If we did not have such medical rec-ords, it would be hazardous and in-appropriateto tryto recreate their di-
agnoses from the art itself. Art iscreated for many reasons, includingaesthetics, cultural conditions, andeconomics, and artists may choosedifferent colors, degrees of represen-tation, and styles. It would be pre-sumptuous, for example, to assumethatnonrepresentational paintingim-plies poor visual acuity or that paint-ing with strong colors (or a lack of
color) impliesthat theartist hascata-ract or color vision abnormalities.16
Theobservationsdescribedin this ar-ticle show how known visual disabil-ity would have altered the percep-tions of Degas and Monet. Byrecognizing how the world ap-peared to them, we can better appre-ciate their struggles and their accom-
plishments and place their late art ina proper context.
Submitted for Publication: Janu-ary 6, 2006; final revision receivedFebruary 20, 2006; accepted Febru-ary 21, 2006.Correspondence: Michael F. Mar-mor, MD, Department of Oph-thalmology, Room A-157, StanfordUniversity Medical Center, 300 Pas-teur Dr, Stanford, CA 94305-5308([email protected]).Financial Disclosure: None re-
ported.Acknowledgment: I thank DavidMarmor, AB, MFA, for assistancewith the illustrations.
REFERENCES
1. HamiltonGH. Thedyingof thelight:the lateworksof Degas, Monet and Cezanne. In: Rewald J,WeitzenhofferF, eds.Aspectsof Monet.NewYork,NY: Abrams; 1984:218-241.
2. Kendall R. Degas and the contingency of vision.Burlingt Mag . 1988;130:180-197.
3. Ravin JG, Kenyon CA. Degas’ loss of vision: evi-dence for a diagnosis of retinal disease. Surv Ophthalmol . 1994;39:57-64.
4. RavinJG. Monet’s cataracts.JAMA. 1985;254:394-399.
5. Lanthony P. Cataract and the painting of ClaudeMonet. Points de Vue . 1993;29:12-25.
6. Tucker PH. Monet in the 20th Century. New Ha-ven, Conn: Yale University Press; 1998.
7. Werner JS. Aging through the eyes of Monet. In:Backhaus WGK, Kliegl R, Werner JS, eds. Color Vision:PerspectivesFrom DifferentDisciplines.Ber-lin, Germany: Walter de Gruyter; 1998:3-41.
8. Halevy D. Edgar Degas. Le Divan . 1919;61:209.9. Thiebault-SissonF. Lesnympheas de Claude Mo-
net. La Revue de l’Art Ancien et Moderne .1927;52:41-52. Translated in:StuckeyC, ed. Mo- net: A Retrospective. New York, NY: Park Lane;1985:279-293.
10. McMullen R. Degas: HisLife, Timesand Work.Bos-ton, Mass: Houghton Mifflin; 1984.
11. BoggsJS. Degas. NewYork, NY:MetropolitanMu-seum of Art; 1988.12. Marmor MF. Degas Through His Own Eyes: Vi-
sual Disability and the Late Style of Degas. Paris,France: Somogy Editions d’Art; 2002.
13. Lanthony P. Degas et la f requence spatiale. Bull Soc Ophtalmol Fr . 1991;91:605-611.
14. Lemoisne PA. Degas et son Oeuvre. Vol 1. Paris,France: Brame & de Hauke; 1946:163.
15. WildensteinD. ClaudeMonet: CatalogRaisonne. Vol4. Paris, France: Bibliotèque des Arts; 1985:108.
16. Marmor MF, Ravin JG, eds. The Eye of the Artist.St Louis, Mo: Mosby–Year Book Inc; 1997.
(REPRINTED) ARCH OPHTHALMOL/ VOL 124, DEC 2006 WWW.ARCHOPHTHALMOL.COM1769
©2006 American Medical Association. All rights reserved. on May 27, 2008www.archophthalmol.comDownloaded from