
Marine toxins
70
Jeevan Jacob Junior Resdient Dept. of Pharmacology
-
Upload
jeevan-jacob -
Category
Health & Medicine
-
view
276 -
download
2
Transcript of Marine toxins
Jeevan Jacob
Junior Resdient
Dept. of Pharmacology

Marine envenomation
Sea Food Poisoning
Drugs from marine Toxins

Important species causing Marine Envenomation are:
1. CNIDARIA
2. MOLLUSCA
3. ECHINODERMATA
4. CHORDATA
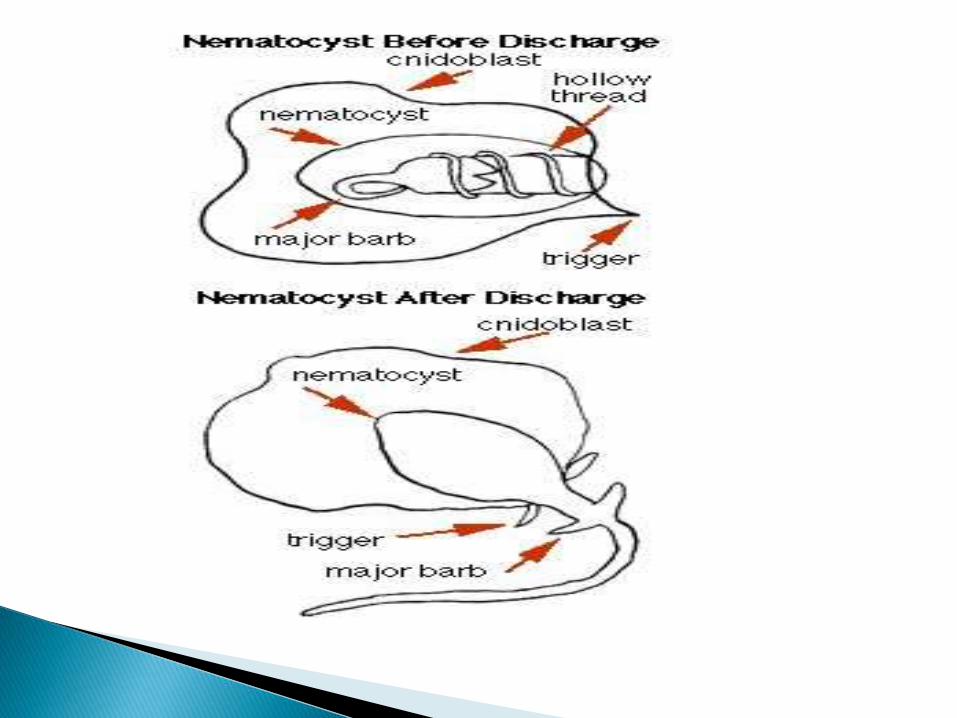
They have tentacles equipped with nematocysts that discharge toxins on contact
Nematocysts are cell organelles in specialized epithelial cells.
They consist of a capsule wall enclosing a tightly coiled hollow tube that bursts forth like a dart on contact.

Subphyla
1. HYDROZOA
2. CUBOZOA
3. SCYPHOZOA
4. ANTHOZOA

Physalia physalis aka the Atlantic Portuguese man-of-war
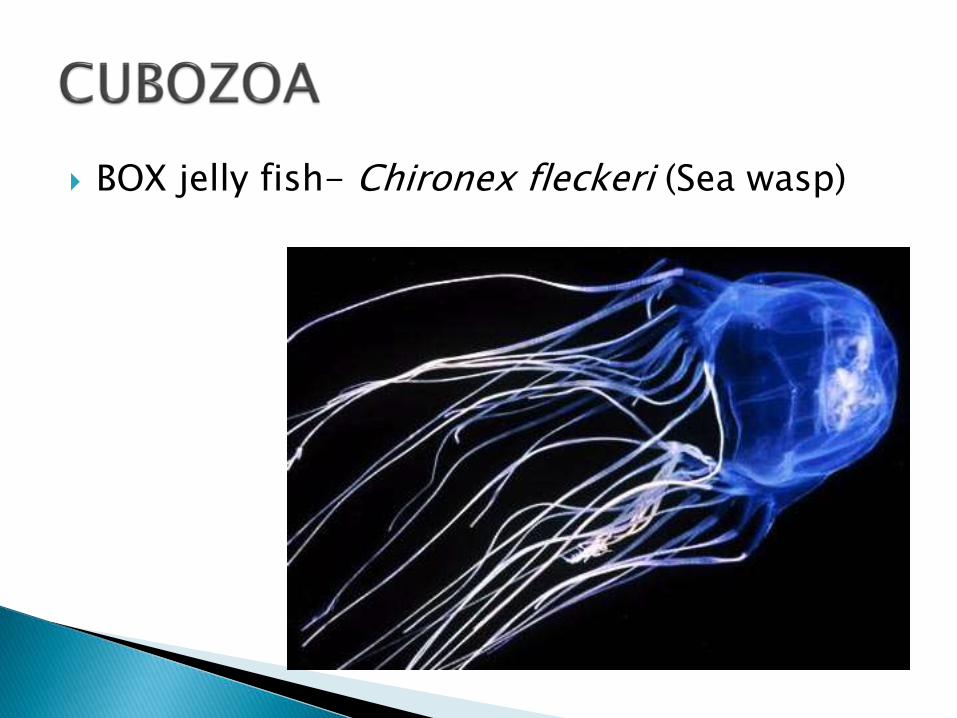
BOX jelly fish- Chironex fleckeri (Sea wasp)
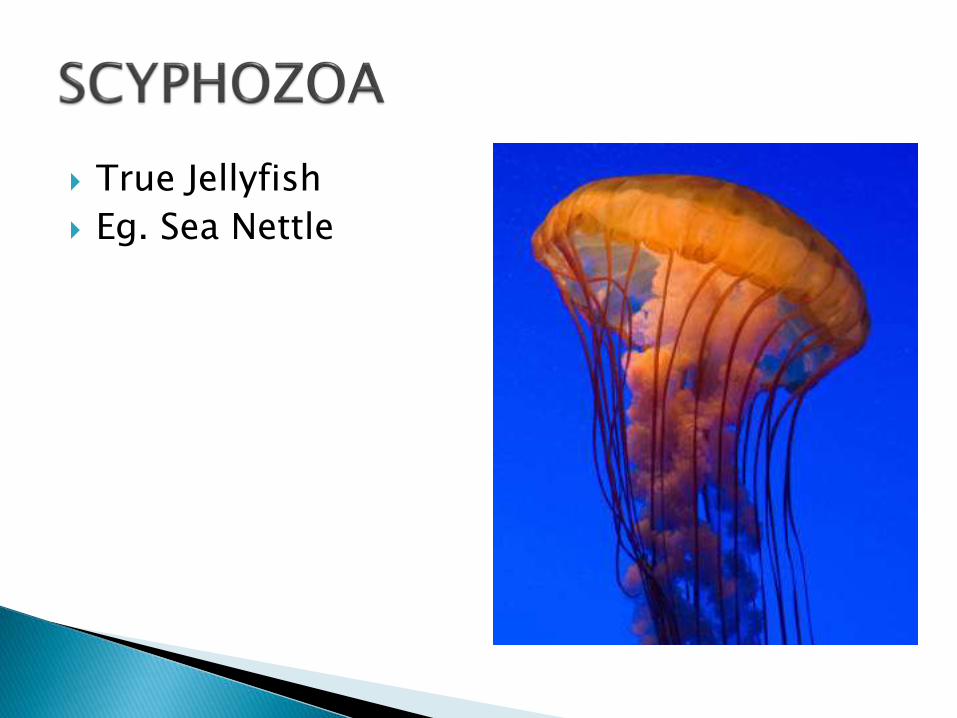
True Jellyfish
Eg. Sea Nettle

Corals and Sea anemones

OCTOPUS – Blue ringed octopus ( Haplochlaenamaculosa)
CONE SHELLS

STARFISH – Crown of thorn star fish
SEA URCHINS
Subphylum Vertebrata
Fishes (eg. Weever fish, Scorpion fish and stonefish)
Sting Ray
Sea snake
JELLY FISH ( Hydrozoa, Cubozoa, Scyphozoa)
Potential toxins include vasoactive amines (histamine, serotonin, and dopamine), elastase, hemagglutinin, protease, collagenase, and palytoxin.
Anemone venoms contain neurotoxins,cardiotoxins, hemolysins, and protease inhibitors.
Injurious effects resulting from an encounter with coelenterate nematocysts range from mild dermatitis to rapid death
Generalised symptoms such as headache, urticaria, muscle cramps, nausea, and vomiting may occur.

Stings by Chironex fleckeri is potentially dangerous.
The effects usually consist of extremely painful localized areas of wheal, edema, and vesiculation, which later result in necrosis involving the full thickness of the skin.
Irukandji venom causes a release of catecholamines.
Painful muscle spasms, shock, cardiomyopathy and pulmonary edema can occur rapidly.
The presentation of Irukandji syndrome may be misdiagnosed as a MI.
When occurring in divers it may be difficult to distinguish from decompression illness.

Treatment of coelenterate stings is symptomatic and supportive.
ACLS may be necessary for patients who sustain cardiac arrest, either from toxic effects of the venom (e.g., C. fleckeri) or from anaphylaxis
Symptoms of Irukandji syndrome have responded to the administration of intravenous magnesium.
The mechanism may be by antagonism of epinephrine

Portuguese man-of-war stings can be removed by applying a slurry of paste of sodium bicarbonate (baking soda) to the wound.
After an hour the baking soda should be moistened with water and scraped off with a dull object, such as a spoon, to remove any remaining nematocysts.
The application of baking soda is notrecommended for box jellyfish, which should be scraped off the skin after pouring 5% acetic acid(vinegar) for a minimum of 30 seconds.
Anemone venoms contain neurotoxins,cardiotoxins, hemolysins, and protease inhibitors.
Causes burning pain initially, later vesicles are formed which forms ulcers and even necrosis can occur.
There are no clear first aid recommendations for
treatment of sea anemone stings; one suggestion is to remove adherent tentacles with forceps or gloved fingers, blot dry, and apply cold packs.
Simple analgesia may be effective. Systemic antihistamines and steroids may be needed to treat local allergic reactions. Topical agents are ineffective.
Produces toxin called asterotoxin, a saponinand possibly hemorrhagic toxins.
Saponins are related to steroids
Destroys cell by forming pores in the membrane
Sharp spines can penetrate skin. Spines can also break off and remain embedded
Stings from the crown-of-thorns starfish cause severe pain and the wounds become inflamed and may bleed excessively.
The affected limb may become swollen, and infection is common

Sea urchin venom is thought to contain proteins, steroid glycosides, and inflammatory mediators
Sea urchin stings are extremely painful, and the spines often become embedded in the patient.
Multiple stings by the black sea urchin has been followed by a delayed severe bulbar polyneuritis.
Sea urchin (and starfish) toxin is remarkably heat labile, and hot water immersion therapy is indicated for pain relief and deactivation of the venom.
Surgical removal, especially of the thick calcium-containing spines, is indicated.

The Australian blue-ringed octopus rarely exceeds 8 inches in full extension and can fit in the palm of the hand.
The octopus bites with its beak and secretes tetrodotoxin from its posterior salivary gland.
Tetrodotoxin, which, like saxitoxin, inhibits fast sodium channels during depolarization, but at a separate site.
Conduction of peripheral motor, sensory, and autonomic nerves is reduced.

Envenomation by the blue-ringed octopus is described as painless, but the patient rapidly succumbs, becoming weak and unconscious, and develops respiratory arrest often within 15 minutes.
Cardiac arrest and death follow. Because the toxin has a short duration of action, patients may survive with prompt resuscitation.
Pain following cone shell envenomation is variable, and the skin blanches or has a bluish discoloration.
This is followed by numbness and swelling.
In severe poisoning nausea, pruritus and muscle weakness occur; vision and hearing may be affected.
Death results from respiratory paralysis.

The immediate treatment for cone shell and blue ringed octopus envenomation is the application of pressure immobilization by wrapping the limb in a crepe bandage using the same tension as if bandaging a sprained ankle—not sufficient to obstruct blood flow.
The limb is then splinted. The bandage can be left on until the patient stabilizes. Treatment is otherwise supportive. Assisted ventilation, if required, may only be necessary for a few hours.
CAT FISH
STONE FISH
STING RAY
SEA SNAKE

Catfish stings are common, painful, and often become secondarily infected.
A patient often has a painful, swollen, and infected wound days after the initial result.
Intense pain results from stings by stonefish.
Systemic symptoms, including headache, seizures, paralysis, abdominal pain, and hypotension, generally result only from envenomation by stonefishes.


The stingrays spine is very sharp, and by virtue of the mechanism of injury, it is common for a patient to receive a laceration rather than a puncture wound.
The usual presenting symptom is severe shooting pain that increases in intensity during the first hour.
Systemic symptoms, such as chest pain, syncope, and other neurologic sequelae, have been described.
Death has been reported but is uncommon and is usually related to chest or abdominal injuries
Most cases of marine stings and spine envenomation can be treated in a standard fashion.
The key to therapy involves care of the wound, relief of pain, hot water immersion, observation, and hospitalization in severe cases.
The affected part should then be immersed continuously in comfortably hot water for at least 60 minutes; this deactivates the heat-labile venom and relieves the pain.
Hot water immersion alone often provides pain relief, and pain medication may not be necessary.
After an hour of continuous hot water immersion, the patient should take the affected part out of the water.
If he or she suffers no pain, hot water treatment may stop.

Wounds should then be irrigated, cleansed, debrided, and explored if necessary to remove any foreign body.
Lacerations may then be surgically closed, although leaving the wound open with follow-up may be preferable, depending on the clinical situation.
Patients who suffer a wound on the chest or abdomen may require surgical exploration.
In the case of stingray injuries, all wounds must be surgically explored to exclude injury to deeper tissues and to remove foreign material that is usually left behind when the barb breaks off.
Treatment of scorpion fish injury is similar to that for stingray injury.
Hot water immersion, wound debridement, and supportive care are indicated.
Tetanus prophylaxis should be given if indicated.
Despite the potential for marine wounds to become infected, prophylactic antibiotics are not recommended for healthy people, but a course of doxycycline should be considered for patients who are immunosuppressed, have chronic renal or liver illness, or are diabetic.
Sea snake bites are often painless. The fangs are often small thus, bites are often difficult to detect.
Symptoms occur within 3.5 hours of the bite. The first symptoms are usually muscle pain; this may be preceded by headache and vomiting.
After some hours, a flaccid paralysis may develop and can progress to respiratory paralysis.
Rhabdomyolysis, myoglobinuria, and subsequent renal failure may occur.

Commonwealth Serum Laboratories produce antivenom for sea snake, stone fish and box jelly fish poison.
Sea snake antivenom should be given to any patient with signs of rhabdomyolysis or neuropathy.
One vial should be given intravenously, up to three if severely poisoned, and can be repeated, up to a totally of 10 vials if signs are progressing.

Common poisonings are paralytic shellfish poisoning (PSP), scombroid fish poisoning, tetrodotoxin poisoning, and ciguatera.
With the exception of tetrodotoxin and scombroid poisoning, the causative toxins originate in dinoflagellates.
Scombroid poisoning and possibly tetrodotoxin have a bacterial origin. The affected fish and shellfish are usually unaffected by the toxins.
Scombroid-affected fish are often reported to taste metallic or peppery, but other toxins are tasteless. All toxins are heat stable.
Red tides result from excessive growth of algae species, including those that cause PSP.
Pigments contained within the algae give the water a red-brown appearance.
Red tides are a coastal phenomenon that occur sporadically.
Poisonings related to red tides of oceans have been described for thousands of years. Because of a red tide in 208 BC, the name Red Sea was given to all the coasts of Arabia by the ancient Greeks
Paralytic shellfish poisoning is caused by saxitoxin and a number of related compounds, sometimes termed gonyautoxins.
These compounds are among some of the more potent toxins known.
They attach to fast sodium channels in nerve and muscle, blocking the initial influx of sodium during depolarization, resulting in a conduction block.
Paralytic shellfish poisoning results in progressive neurologic impairment that initially affects sensory fibers, bulbar nerves, peripheral motor neurons, and the central nervous system.
Scombroid fish poisoning results from the activity of bacteria, such as Proteus morganii, utilizing the enzyme histidine decarboxylase to metabolize histidine to histamine.
Scombroid fish poisoning resembles immunoglobulin E–mediated food allergies, replicating the typical features of endogenous histamine production.
Patients who have eaten scombroid-affected fish often present with signs and symptoms of histamine intoxication, often within 30 minutes.
Flushing of the upper body, urticaria, headache, chills, vomiting, diarrhea, and abdominal cramps are common. Conjunctival erythema may occur.
Severe cases that include bronchospasm and hypotension have been reported.

Puffer fish poisoning is caused by tetrodotoxin, which, like saxitoxin, inhibits fast sodium channels during depolarization, but at a separate site.
Conduction of peripheral motor, sensory, and autonomic nerves is reduced.
In addition, tetrodotoxin also activates the CTZ and may depress the respiratory and vasomotor centers.
Effects on cardiac, VSM and skeletal muscle may occur in high doses.
Puffer fish poisoning has a predictable progression of neurologic impairment affecting peripheral sensory nerves, peripheral motor nerves, bulbar nerves, the central nervous system and respiratory muscles.
Ciguatoxin, the cause of ciguatera, also attaches to fast sodium channels but increases sodium permeability.
After an initial stimulation, prolonged refractoriness and decreased conduction velocity occurs
Ciguatera produces a complex presentation with multiple symptoms affecting many systems; the mechanisms responsible are unclear.
Saxitoxin and related toxins associated with paralytic shellfish poisoning are heat stable and water soluble.
Histamine is not normally absorbed across the gastrointestinal mucosa but metabolized by diamineoxidase. In scombroid poisoning it may be assisted by the presence of other toxins: putrescine and cadaverine.
Tetrodotoxin is heat stable and water soluble.
Ciguatoxin is heat stable and can be transferred across the placenta and by semen or breast milk.

The treatment of seafood poisoning is largely supportive.
Patients may require intubation and mechanical ventilation.
Intravenous saline should be used to replace fluid losses.
Ionotropes may be required for paralytic shellfish poisoning or severe ciguatera poisoning.
Intravenous calcium gluconate (1 g over 30 minutes, followed by 2 to 4 g/day IV) has been used to treat hypotension secondary to ciguatera.
Administration of antihistamines such as the H2 blocker and the H1 blocker is key to treatment of scombroid poisoning, as are intravenous fluids, steroids, and general supportive care.
Epinephrine may be indicated in the presence of bronchospasm, angioedema, or hypotension. The syndrome is usually self-limited, resolving within a few hours.

Intravenous mannitol has been promoted as a treatment of acute ciguatera poisoning.
However, a randomized controlled trial failed to demonstrate that it was superior to normal saline in reducing symptoms by 24 hours, and its use can no longer be recommended.
Chronic ciguatera may be bothersome, because symptoms may wax and wane.
The most success in treatment has been with the use of amitriptyline, possibly by an affect on sodium channels.
Treatment is generally begun with amitriptyline 25 mg twice a day.
Remissions and exacerbations may occur.
Alternatively, gabapentin has provided symptomatic improvement for persistent neurologic sequelae of ciguatera poisoning

High level of biodiversity in marine world
High biodiversity = high chemical diversity
Variety of molecules show unique structural features and exhibit various types of biological activity
Highly potent bioactive molecules
53

Synthetic equivalent of naturally occurring ω-conotoxin.
Became first marine-derived drug to be approved by US Food and drug Administration (FDA) in 2004.
It is considered medically necessary for the management of severe chronic pain in those individuals for whom intrathecal therapy is warranted, and who are intolerant of or refractory to other treatment, such as systemic analgesics, adjunctive therapies or IT morphine.
54
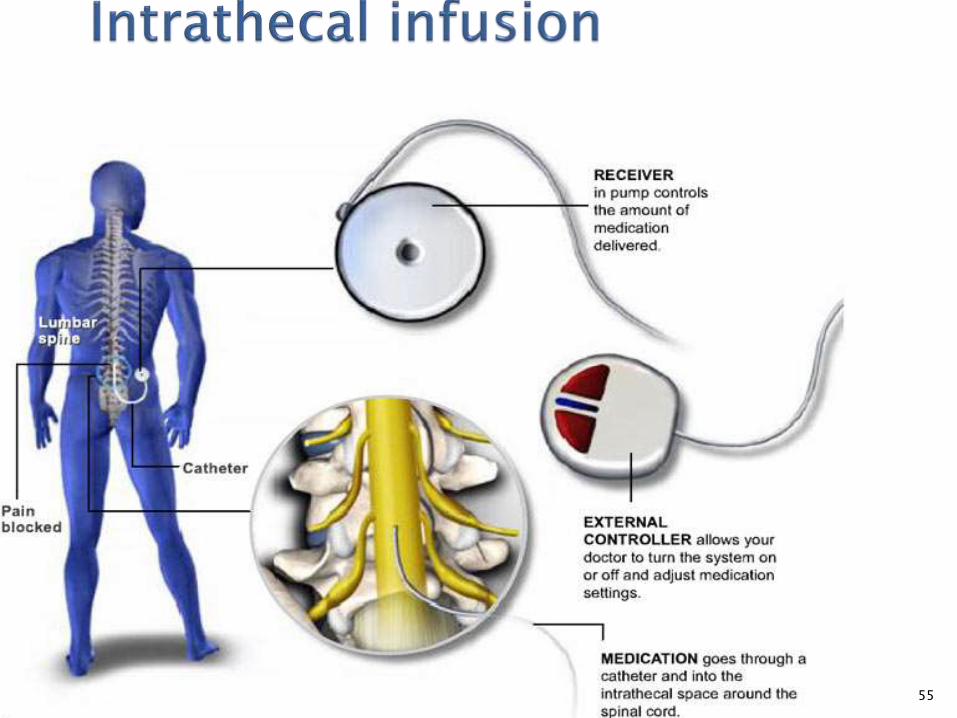
55

• 25-amino acid peptide
• Six cysteine residues linked by 3 disulfide bonds
Pharmacodynamics : • N-type voltage-sensitive calciumchannels were subsequently identified asits target site.
• It potently inhibits the conduction of nerve signals by specifically blocking the NVSCC.
56
Direct blockade of N-type channel inhibits the activity of a subset of neurons, including pain-sensing primary nociceptorswhich are controlled by the former
50 times more effective than morphine
57

Bioavailability = 50%
Half life = 1.3 hour
Excretion = <1% urine
Tmax = 5.3 hour
58
Dizziness, nausea, confusional state and nystagmus (>25%)
Meningitis, when infused with an external catheter
Side effects are to be weighed against high level of pain management, its degree and length and also lack of dependence and tolerance even after long treatment when most other drugs do not work.
59

60
The Caribbean sea-squirt Ecteinascidia turbinata
ecteinascidins
61
First marine-derived anticancer drug to reach the market – after 40 years of its discovery and 17 years after publication of its structure.
Extracts of caribbean derived tunicate Ecteinascidia turbinata
ecteinascidins were found to be cytotoxic against leukaemia cells
62
the first multistep synthesis of the compound was completed in 1996
Large scale semi synthesis developed with cynosafracin B which can be produced by fermentation of Pseudomonas fluorescens

63
A ring
C ring
Fig. Molecular-dynamics model showing the alkylation of DNA by ET-743 at N2 of guanine in the minor groove. The A Ring and C Ring represent the tetra
• Ascribed to covalent
modification of DNA by guanine-specific alkylation at the N2 position
• Selective for GC-rich sequence and forms an adduct with duplex DNA which induces a bend in the DNA helix directed towards the major groove

64
Actual mechanism is not yet known but it is believed to involve the production of superoxide near the DNA strand resulting in DNA backbone cleavage and cell apoptosis.
There is also some speculation the compound becomes 'activated' into its reactive oxazolidine form.
65
Intravenous through a fine plastic tube that is inserted
under the skin and into a vein near the collarbone (central line)
into a fine tube that is inserted into a vein in the crook of arm (PICC line).
To help prevent some of the side effects of trabectedin, you will be given an injection of a steroid drug 30 minutes before the chemotherapy

66
Protien binding : 94 to 98%
Metabolism : Hepatic (mostly CYP3A4-
mediated)
Half-life : 180 hours (mean)
Excretion : Mostly fecal
67
Varies from person to person
Risk of infection as it reduces white blood cell count
Bruising and bleeding – it reduces production of platelets
Anaemia
Loss of appetite
Marine life that is toxic to humans acts through envenomation by stinging, spinouspuncture injury, bites, ingestion etc.
Management is mainly supportive
Marine life is a promising field in Pharmaceuticals
Haddad and Winchester's Clinical Management of Poisoning and Drug Overdose, 4th ed.
Wikipedia












![4: Zootoxins (toxins of animals) [Biological-origin toxins]](https://static.fdocuments.us/doc/165x107/61cddf54f2b98d6a6b5b05e1/4-zootoxins-toxins-of-animals-biological-origin-toxins.jpg)




