Marian Jalos ( ARDS )
21
7/29/2019 Marian Jalos ( ARDS ) http://slidepdf.com/reader/full/marian-jalos-ards- 1/21
Transcript of Marian Jalos ( ARDS )

7/29/2019 Marian Jalos ( ARDS )
http://slidepdf.com/reader/full/marian-jalos-ards- 1/21

7/29/2019 Marian Jalos ( ARDS )
http://slidepdf.com/reader/full/marian-jalos-ards- 2/21
It was first identified in 1967, ARDShas been known in various name
such as:
shock lung
wet lung
Vietnam lung
Adult hyaline membrane disease
adult respiratory distress
syndrome

7/29/2019 Marian Jalos ( ARDS )
http://slidepdf.com/reader/full/marian-jalos-ards- 3/21
This clinical syndrome is characterized
by a sudden and progressive pulmonaryedema.
is a condition in which the lungs
suffer severe widespread injury,interfering with their ability to take up
oxygen.
HALLMARK OF ARDS
A low blood oxygen level and the inability to
get oxygen to normal levels.

7/29/2019 Marian Jalos ( ARDS )
http://slidepdf.com/reader/full/marian-jalos-ards- 4/21
Etiologic Factors Related to Acute Respiratory
Distress Syndrome
•inhalation (aspiration of gastric contents, smoke, neardrowning )
•Drug ingestion and overdose ( aspirin ,
methadone)•Hematologic disorders ( DIC )
•Localized infection ( Viral pneumonia )
•Metabolic disorders ( pancreatitis, uremia )•Shock ( hemorrhagic shock , septic shock)
• Trauma ( lung contusion,fat emboli )

7/29/2019 Marian Jalos ( ARDS )
http://slidepdf.com/reader/full/marian-jalos-ards- 5/21
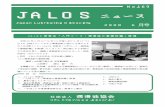
Primary Insult
Damage surfactant –
producing cells
Damage to alveolar –
capillary membrane
Alveolar EdemaInterstitial
Edema
Dilution of
surfactant
Decreased surfactant
production
Decreased lung compliance, atelectasis,
hyaline membrane formation
Impaired gas exchangeIncreased work of breathing
Respiratory failure
Chemical Mediators Released

7/29/2019 Marian Jalos ( ARDS )
http://slidepdf.com/reader/full/marian-jalos-ards- 6/21

7/29/2019 Marian Jalos ( ARDS )
http://slidepdf.com/reader/full/marian-jalos-ards- 7/21
Manifestations dyspnea
tachypnea
AnxietyIncreasing respiratory rate
Intercostal retraction
Use of accessory muscles of respirationCyanosis
As respiratory failure progress mental status
changes occur:
Agitation
Confusion
lethargy

7/29/2019 Marian Jalos ( ARDS )
http://slidepdf.com/reader/full/marian-jalos-ards- 8/21
Complications
Barotrauma
Paralytic ileusRenal failure
Dysrhythmias
Infectionmalnutrition
Death

7/29/2019 Marian Jalos ( ARDS )
http://slidepdf.com/reader/full/marian-jalos-ards- 9/21
Nursing Diagnoses
impaired gas exchange
ineffective breathing pattern risk for infection
Alteration in comfort
ineffective coping

7/29/2019 Marian Jalos ( ARDS )
http://slidepdf.com/reader/full/marian-jalos-ards- 10/21
DIAGNOSTIC TEST
ABG – initially show hypoxemia withPO2 of less than 60mmHg and
respiratory alkalosis.
Chest X-ray – Diffuse infiltrates are
seen initially , progressing to a “white
outˮ pattern
Pulmonary function testing – shows
decreased lung compliance withreduced vital capacity , minute volume
and functional vital capacity

7/29/2019 Marian Jalos ( ARDS )
http://slidepdf.com/reader/full/marian-jalos-ards- 11/21
Pulmonary artery pressure monitoring –
shows normal pressures in ARDS , helping
distinguish ARDS from cardiogenicpulmonary edema.

7/29/2019 Marian Jalos ( ARDS )
http://slidepdf.com/reader/full/marian-jalos-ards- 12/21
Management
Medical Management
primary focus in the management
includes identification and treatment of the
underlying condition . Aggressive ,
supportive care must be provided tocompensate for the severe respiratory
dysfunction.
there is no definitive drug therapy for ARDS , a number of medications may be
used.

7/29/2019 Marian Jalos ( ARDS )
http://slidepdf.com/reader/full/marian-jalos-ards- 13/21
inhaled nitric oxide – reduces intrapulmonary
shunting and improves oxygenation by dilating
blood vessels in better ventilated areas of the
lungs.
Surfactant therapy – helps maintain openalveoli , decreasing the work of breathing ,
improving compliance and gas exchange.
Corticosteroid – may be used late in thecourse of ARDS to improve oxygenation and
lung mechanics when fibrotic changes occur.

7/29/2019 Marian Jalos ( ARDS )
http://slidepdf.com/reader/full/marian-jalos-ards- 14/21
Mechanical Ventilation
The mainstay of ARDS management is
endotracheal intubation and mechanicalventilation . With ARDS , it is rarely possible
to maintain adequate tissue oxygenation
with oxygen therapy alone.
Often it is necessary to add continuous
positive airway pressure (CPAP) or positive
end-expiratory pressure (PEEP) to
mechanical ventilation setting to maintain
blood and tissue oxygenation

7/29/2019 Marian Jalos ( ARDS )
http://slidepdf.com/reader/full/marian-jalos-ards- 15/21
Nutritional Therapy
Adequate nutritional support is vital
in the treatment of ARDS. Patients
require 35 to 45 kcal/kg per day to
meet caloric requirements . Enteral
feeding is the first consideration
however, parenteral nutrition also
may be required.

7/29/2019 Marian Jalos ( ARDS )
http://slidepdf.com/reader/full/marian-jalos-ards- 16/21
Nursing Care
nursing care needs of the client with
ARDS are very similar to those of any client
with acute respiratory failure.
Maintaining adequate ventilation and
respiration are of highest priority , along with
preventing injury and managing anxiety. Additional high priority nursing care
concerns for the client are related to the
effects of PEEP on cardiac output and potential problems of weaning ventilatory support.

7/29/2019 Marian Jalos ( ARDS )
http://slidepdf.com/reader/full/marian-jalos-ards- 17/21
Decreased Cardiac Output
Manifestations of decreased cardiac output include hypotension
and compensatory tachycardia as the hearts attempt to maintain
CO despite decreased stroke vol. In the client who is already
hypoxic because of ARDS this drop in CO can increase tissue
damage . Urine output falls , and dysrhythmias may develop.
Nursing Interventions
Monitor and record vital signs , including apical pulse, at leastevery 2hours;more frequently immediately following initiation of
mechanical ventilation or addition of PEEP.
Frequent assessment is vital to detect early signs of
decreased cardiac output.PRACTICE ALERT:
Record urine output hourly . Because a significant portion of the
cardiac output goes directly to the kidneys ,a fall in urine output to
less than 30ml/hr is often the first sign of decreased cardiac output.

7/29/2019 Marian Jalos ( ARDS )
http://slidepdf.com/reader/full/marian-jalos-ards- 18/21
Assess level of consciousness at least every 4 hours.
Altered level of consciousness ,confusion, and
restlessness are early signs of cerebral hypoxia due to
decreased CO. Monitor pulmonary artery pressure , central venous
pressure and CO every 1 to 4 hours.
Changes in these measurement may indicate
worsening cardiac status. Assess heart and lung sound sounds frequently.
increasingly crackles or abnormal heart sounds may
indicate heart failure.
Weight daily at the same time . Accurate daily weightsare the best indicators of fluid vol. status.
Maintain intravenous fluids as ordered. intravenous
fluids are given to maintain vascular volume and prevent
deh dration.
D f i l i

7/29/2019 Marian Jalos ( ARDS )
http://slidepdf.com/reader/full/marian-jalos-ards- 19/21
Dysfunctional weaning assess vital signs every 15 to 30 mins. Following
changes in ventilator setting and during T-piece trials.
Vital signs , heart and respiratory rates in particular ,can provide early signs of hypoxemia and poor tolerance
of the weaning process.
place in Fowler’s or high fowlers position . Fowlers
position facilitates lung expansion and reduces the workof breathing.
fully explain all weaning procedures , along with
expected changes in breathing. Adequate explanations
help reduce anxiety and improve ability to cooperate.Limit procedures and activities during weaning periods.
reducing energy expenditures and cardiac work
facilitates the weaning process.
P id di i h t l i i di

7/29/2019 Marian Jalos ( ARDS )
http://slidepdf.com/reader/full/marian-jalos-ards- 20/21
Provide diversion, such as television or radio.
Diversion helps distract the focus from breathing.
begin weaning procedures in the morning, when the
client is well rested and alert; weaning may bediscontinued overnight to provide rest. The work of
breathing increases during the weaning process ;
adequate rest is important.
Avoid administering drugs that may depressrespirations during the weaning process ( except as
ordered at night to facilitate rest when ventilator support
is provided ). Sedatives or analgesics that depress
respirations can impair the weaning process.
PRACTICE ALERT: frequently assess respiratory status following weaning
and extubation.keep an intubation kit readily available following extubation;be
prepared for emergency reintubation.laryngeal spasm or laryngeal edema may
develpo following extubation,necessitating reintubation to maintain respirations.

7/29/2019 Marian Jalos ( ARDS )
http://slidepdf.com/reader/full/marian-jalos-ards- 21/21