Marc Sadowsky - Taos, NM Technical Draft - Writing Sample
171
XXXXXX XXXXXX XXXXXXX PRIMARY CARE SERVICES FOR TAOS, NEW MEXICO RFP # VA-258-11-RP-0001 TECHNICAL PROPOSAL Submitted To: Department of Veterans Affairs Contracting Office (501/90C) New Mexico VA Health Care System 1501 San Pedro Drive SE Albuquerque NM 87108 Submitted By: Xxxxxx Xxxxx 411 Oak St. Cincinnati, OH 45219 1 The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
-
Upload
marc-sadowsky -
Category
Documents
-
view
42 -
download
2
Transcript of Marc Sadowsky - Taos, NM Technical Draft - Writing Sample
XXXXXX XXXXXX XXXXXXX
PRIMARY CARE SERVICES FOR TAOS, NEW MEXICO
RFP # VA-258-11-RP-0001
TECHNICAL PROPOSAL
Submitted To: Department of Veterans AffairsContracting Office (501/90C)New Mexico VA Health Care System1501 San Pedro Drive SEAlbuquerque NM 87108
Submitted By: Xxxxxx Xxxxx 411 Oak St. Cincinnati, OH 45219Phone: (513) XXX-XXXX Fax: (513) XXX-XXXX
This proposal or quotation includes data that shall not be disclosed outside the Government, and shall not be duplicated, used, or disclosed - in whole or in part - for any purpose other than to evaluate this proposal or quotation. If, however, a contract is awarded to the offeror or quoter as a result of or in connection with the submission of this data, the Government shall have the right to duplicate, use or disclose the data to the extent provided in the resulting contract. This restriction does not limit the Government's right to use information contained in this data if it is obtained from another source without restriction.
1
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
TABLE OF CONTENTS
1.0 Introduction to Xxxxxx Xxxxx 5
A. Personnel Qualifications 8
A.1. Xxxxxx Xxxxx’s Experience Providing Healthcare Services to the Government 8
A.2 Relevant Experience Providing Healthcare Services to the Federal Government 9
A.3 Roster of Primary Care Staff intended to be utilized in the Performance of this Contract 11
A.3.A. Physician staff providing service under this contract 13
A.3.B. Nurse Practitioner Staff Providing Service Under this Contract 15
A.3.C. Social Worker Staff Providing Service Under this Contract 16
A.3.D. Clinic Manager Staff Providing Service Under this Contract 16
A.3.F. LPN Staff Providing Service Under this Contract 18
A.3.G. Phlebotomist/Medical Assistant Staff Providing Service Under this Contract 18
A.3.H. Medical Assistant Staff Providing service under this contract 19
A.4. Roles/Responsibilities of Proposed TAOS CBOC Personnel 20
A.5 Methods and Mechanisms Xxxxxx Xxxxx will use to Provide, Qualify, and Retain Qualified Staff for the Required Positions 25
A.5.A Xxxxxx Xxxxx’s Plan for Recruitment 26
A.5.B Xxxxxx Xxxxx’s Plan for Credentialing 29
A.5.C Xxxxxx Xxxxx’s Plan for long-term rention of employees 33
A.6. Training and Experience That Will Be Utilized to Meet Administrative Support Functions of This Contract 36
A.6.A. Xxxxxx Xxxxx’s Key Corporate and Clinical Staff Experience 36
A.6.B. Xxxxxx Xxxxx’s Training Practices 41
A.7. Organization Structure and Management Practices 44
A.8. Mechanism to Schedule Qualified VA Credentialed Physicians and Staff to Cover the Required Clinic Schedule 47
A.8.A. Contingency Plan for Covering Enrolled Patients and Appointments Due to Scheduled or Unscheduled Leave 48
A.9. Capability to Recruit Adequate Staffing 50
A.10. Operational Plan to Include Staffing for the First 90 Days of Clinic Operation 50
B. Coordination and Continuity of Care 53
B.1. Appropriateness of Care54
2
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
B.1.A. Xxxxxx Xxxxx’s Ability to Assure Appropriateness of Care 55
B.1.A.I Xxxxxx Xxxxx’s Management Response to Potential Problems 57
B.1.A.II Xxxxxx Xxxxx’s Methods to Avoid Conflict of Interest 62
B.1.B. Mechanisms Utilized to Assure Appropriateness of Care 63
B.1.B.I. VA External Peer Review Program63
B.1.B.II. Employee Performance Incentives 64
B.2. Xxxxxx Xxxxx’s Understanding of Joint Commission and Other Regulatory Requirements64
B.3 Xxxxxx Xxxxx Will Ensure Continuous Communication with VA Coordinator 65
B.4. Specialized Training and Clinical Staff Meetings at VA Hospital Level 66
B.5. Ensuring Overall Timely Delivery of Services 66
B.5.A. Xxxxxx Xxxxx Site Readiness Contingency Plan 66
B.5.B. Xxxxxx Xxxxx’s Plan to Ensure Overall Timely Delivery of Services For VA Patient Care68
B.5.C. Scheduling the Implementation Template with VAMC 68
B.5.D. Xxxxxx Xxxxx Understanding of VHA Scheduling Guidelines 68
B.5.E. Timeliness in Patient Access from Contract Outset 69
B.5.F. Additional Access Will Be Implemented for the Clinic When Needed Over the Contract Term 70
B.6. Xxxxxx Xxxxx’s Contingency Plan for Computer Downtime 71
C. Past Performance 75
D. Social Economic Consideration 78
E. Quality Assurance Plan 79
E.1. Xxxxxx Xxxxx’s Approach Towards Quality Assurance 79
E.1.A. Quality Assurance Collection and Reporting Methods 79
E.1.B. Xxxxxx Xxxxx’s Patient Advocacy Program79
E.2. Performance Measures and PIP Process Used in Ongoing Management of Staffing Program 81
E.2.B. Access to Care Reporting 83
E.2.C. Quality85
E.2.C.I. Xxxxxx Xxxxx’s Overall Approach to Quality Management/Improvement 85
E.2.C.II Taos CBOC Quality Management/Improvement Directives 86
E.2.C.III. Standard Xxxxxx Xxxxx Quality Management/ Improvement Program 86
3
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
E.2.C.IV. Xxxxxx Xxxxx’s Multi-Focused Quality Management/ Improvement Program 87
E.2.D. Timeliness of Care and Access as Important Elements of Care 87
E.2.D.I. Xxxxxx Xxxxx’s CBOC Performance Incentive Program To Promote Quality 88
E.2.D.II. Clinical Practice Guidelines and Clinical Reminder Compliance 89
E.2.D.III. Xxxxxx Xxxxx’s Ability to Measure and Improve Quality of Service 89
E.2.D.IV. Performance Metrics 90
E.2.D.V. CBOC Quality Management/Improvement Plan Reports90
E.2.D.VI. Continuous Quality Improvement 91
E.2.D.VII. Additional Methods to Include Veteran Patients in Quality Management/Improvement Plan 92
E.3. Customer Satisfaction 92
E.3.A. Maintenance and Monitoring Continuity of Care for Patients 93
E.3.A.I. Clinical Results from Patient Satisfaction Surveys 94
E.3.A.II. Xxxxxx Xxxxx’s Veteran and Patient Centered Customer Service Capabilities 95
F. Location of Offices 97
F.1. Utilization of Facility’s Geographic Location to Best Serve the Patients 97
F.2. Location of Proposed Clinic: Taos, New Mexico 104
F.3. Location of Facility In Relation to Public Transportation 105
F.4. Location of Facility to Local Highways 106
F.5. Description of Facility’s Parking Availability 107
F.6. Description of Facility’s Handicap Parking Availability 107
F.7. Description of Facility’s Proposed Hours of Operation 107
G. Listing of all External Attachments and Exhibits 108
4
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
1.0 INTRODUCTION TO XXXXXX XXXXX
Xxxxxx Xxxxxx Xxxxxxx (“Xxxxxx Xxxxx”) is pleased to submit this offer to furnish Community Based Outpatient Clinic (“CBOC”) services on behalf of the local veteran population in Taos, New Mexico.
Xxxxxx Xxxxx has delivered CBOC services on behalf of the Department of Veterans Affairs (“VA”) since 1997, when it designed and opened its first dedicated VA CBOC. Given our more than 13 years of experience providing CBOC solutions to the VA, Xxxxxx Xxxxx’s management team is extremely experienced at ensuring that continuity of care is maintained between the VA Hospital parent and the Xxxxxx Xxxxx-operated CBOC. Moreover, Xxxxxx Xxxxx possesses thorough knowledge of the management approach necessary to support a dedicated freestanding clinic to provide specialized practice and administrative services for VA beneficiaries.
Xxxxxx Xxxxx has delivered CBOC services on behalf of the Department of Veterans Affairs since 1997, when it designed and opened what we understand to be the first dedicated VA CBOC on behalf of the Department of VA Healthcare on a contracted basis nationally. Since then, Xxxxxx Xxxxx has performed CBOC services at 35 locations throughout the United States. Xxxxxx Xxxxx’s management team has developed the clinic administrative structures and supervised the delivery of such structures throughout its VA CBOC System and is extremely experienced at ensuring that continuity of care is maintained between the VA Hospital parent and the Xxxxxx Xxxxx-operated CBOC.
Xxxxxx Xxxxx will provide full appointment, provider, ancillary, nursing, administrative, managerial and billing support for the proposed clinical location in Taos, New Mexico. Xxxxxx Xxxxx will provide full physical plant and equipment/supply management for the proposed clinic. Primary Care services provided within the clinic will include preventive health management services, longitudinal detection of disease and subsequent management of medical conditions in eligible veterans. Clinic care will be accessible, continuous and coordinated. Xxxxxx Xxxxx has substantive past experience regarding the development and maintenance of free-standing primary care practices on behalf of VA Medical Centers nationwide. A detailed description of Xxxxxx Xxxxx corporate experience applicable to this service is provided throughout this proposal.
In addition to CBOC services for the Department of Veterans Affairs, Xxxxxx Xxxxx has established itself as one of the two largest providers of medical support services to federal agencies of the U.S. Government. Currently, Xxxxxx Xxxxx provides services to the Federal Government totaling approximately $140 million in annual dollar amount. The firm furnishes more than 2,000 FTEs on behalf of Federal Government agencies at more than 100 Government facilities in both the United States and overseas. Xxxxxx Xxxxx currently provides healthcare, counseling and administrative support services in more than 42 states and 13 overseas nations.
Xxxxxx Xxxxx has furnished, on a full-time basis, the following categories of physician-level providers:
Family Practice Physicians ENT PhysiciansInternal Medicine Physicians NeurologistsPediatricians PsychiatristsDevelopmental Pediatricians Occupational Medicine PhysiciansEmergency Medicine Physicians Flight Medicine PhysiciansOB/GYN Physicians
5
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
Hematology/Oncologists UrologistsDiagnostic RadiologistsRadiation Oncologists PathologistsAnesthesiologists OphthalmologistsGeneral Surgeons NeurosurgeonsOrthopedists Interventional Radiologists
Additionally, Xxxxxx Xxxxx has also provided a full range of ancillary healthcare providers. Ancillary healthcare providers furnished include the following labor categories and specialties:
Pharmacists Occupational Therapy AssistantsPsychologists OptometristsChild/Adolescent Psychologists Physician AssistantsClinical Social Workers Family Nurse PractitionersPhysical Therapists Pediatric Nurse PractitionersOccupational Therapists OB/GYN Nurse PractitionersRehabilitation Therapy Assistant Neonatal Nurse PractitionersSpeech and Language Pathologists Psychiatric Nurse PractitionersEarly Childhood Special Educators Certified Registered Nurse AnesthetistsPhysical Therapy Assistants
Xxxxxx Xxxxx is also very experienced and possesses strong capabilities in the provision of nursing and related services. Nursing and related medical support services furnished by Xxxxxx Xxxxx include the following:
ICU RN Medical Administrative TechniciansCCU RN Medical AuditorsMedSurge RN Medical CodersL&D RN Medical ClerksEmergency Room RN Medical TechniciansPsychiatric RN Medical TechnologistsOR RN Radiology TechniciansRN Case Manager Medical Instrument TechniciansUtilization Management RN Pathology TechniciansOutpatient Clinic RN Certified Nursing AssistantsInpatient LPN Psychiatric TechniciansOutpatient Clinic LPN Pharmacy TechniciansRespiratory Therapist Medical Supply TechniciansMedical Assistants Social Services Assistants
In fulfillment of its healthcare services on behalf of military facilities, Xxxxxx Xxxxx currently operates branch offices in Washington, DC; Aiken SC; Norfolk, VA; Jacksonville, NC; Dothan, AL; Killeen, TX; and Oceanside, CA.
Additionally Xxxxxx Xxxxx operates overseas branch offices in Heidelberg, Germany; Landstuhl, Germany; and Okinawa, Japan.
Xxxxxx Xxxxx possesses over 80 corporate executives, recruiters, managers, credentialers, writers and other administrative staff located at its corporate headquarters in Cincinnati, Ohio. All of these individuals are
6
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
exclusively dedicated to the successful provision of direct healthcare services to U.S. Government facilities in the United States and overseas. The Corporate Office is located at: 411 Oak Street, Cincinnati, OH 45219.
Xxxxxx Xxxxx’s mission is “To serve our clients by providing the highest quality health care service available in a reliable, timely and effective manner.”
The contact personnel possessing the authority to bind and make representations on behalf of the company for this proposal are:
Richard S. XxxxxCEO, Xxxxxx Xxxxxx Xxxxxxx 411 Oak StreetCincinnati, OH 45219Phone: 513.XXX.XXXX
Brandon A. XxxxxVice President, Xxxxxx Xxxxxx Xxxxxxx 411 Oak Street, Suite 300Cincinnati, OH 45219Phone: 513.XXX.XXXX
<THIS SPACE LEFT INTENTIONALLY BLANK>
7
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
A. PERSONNEL QUALIFICATIONS
A.1. XXXXXX XXXXX’S EXPERIENCE PROVIDING HEALTHCARE SERVICES TO THE GOVERNMENT
Since first providing healthcare, counseling and administrative support services to the Government more than 29 years ago, Xxxxxx Xxxxx has established itself as one of the two largest providers of medical support services to federal agencies of the U.S. Government. Currently, Xxxxxx Xxxxx provides services to the Federal Government totaling approximately $140 million in annual dollar amount. The firm furnishes more than 2,000 FTEs on behalf of Federal Government agencies largest providers of support services to Government agencies. The firm furnishes more than 2,000 FTEs on behalf of Federal Government agencies at more than 100 Government facilities in both the United States and overseas. Xxxxxx Xxxxx currently provides healthcare, counseling and administrative support services in more than 40 states and 12 overseas nations. The privately held company is headquartered in Cincinnati, Ohio. The following sections illustrate Xxxxxx Xxxxx’s capabilities in the provision of various healthcare services.
Community Based Outpatient Clinic (CBOC) Services. Xxxxxx Xxxxx currently manages and staffs 15 CBOC clinics on behalf of the Department of Veteran Affairs that include both primary care and mental health services. Case Management and care of veterans includes compliance with VHA Clinical Practice Guidelines and Reminders that mandate mental health screenings, referrals and treatment related to PTSD and TBI, Operation Enduring Freedom (OEF) and Operation Iraqi Freedom (OIF) post-deployment, major depressive disorder, substance use disorder, chronic pain, fatigue and psychoses. These clinics are comprised of a range of services for veteran beneficiaries, including but not limited to:
Primary Care: Xxxxxx Xxxxx provides Primary Care services, including outpatient medical care for the purpose of prevention and detection of disease and subsequent management of medical conditions in a clinic environment. The Primary Care services are directed toward health promotion and disease prevention, management of acute and chronic medical conditions, pharmacological management, referral to specialty care and continuity across the inpatient and outpatient settings.
Preventive Health Care/Chronic Disease Management: Preventive Health Care /Chronic Disease Management includes screening for: established risk factors for cardiovascular disease; breast, cervical, and colorectal cancer; hepatitis C; diabetics’ depression, nutritional deficits; patient education, weight control, physical fitness/exercise; and the identification of alcohol and substance abuse, military sexual trauma, Post Traumatic Stress Disorder, and other evidence-based health screening examinations. This service also includes annual influenza vaccination and pneumovax and other immunizations as clinically indicated; and space and administrative support for VAMC-provided complete and comprehensive mental health services.
Emergency Services: In the event of an emergency for a patient during normal clinic hours, Xxxxxx Xxxxx staff immediately calls 911 and provides emergency stabilization to the maximum possible extent for the patient. For all cases in which Xxxxxx Xxxxx is aware of a veteran’s use of any emergency medical services, Xxxxxx Xxxxx will document these encounters in the patient’s medical record with a note that summarizes the occurrence and its outcome.
Phlebotomy / Laboratory Services: Xxxxxx Xxxxx provides for the collection and handling of lab specimens through an in-house laboratory in accordance with the current up-to-date instructions listed in FILE 60 in VISTA for both routine and non-routine tests. Xxxxxx Xxxxx processes all lab specimens for shipment to the VA Medical Center according to Laboratory instruction so that specimen integrity will be maintained.
8
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
Case/Care Management: Xxxxxx Xxxxx provides for the management and continuity of health care for all enrolled patients through the following minimum functions: coordination of all health services provided to enrolled patients; provision of primary care as a point of entry into the health care system for non-emergency care; requests for specialty consultations and diagnostic work-ups; intensive case/care management on a daily basis by use of electronic data transmission from multiple patients to a care manager; provision of history and physicals required for nursing home admission.
Veteran Resources: Provide veterans with information that may benefit them, such as the announcement of the clinic itself or the provision of information regarding available veteran resources.
Provision of Community Outreach ServicesIn line with current solicitation requirements, Xxxxxx Xxxxx CBOC Outreach Program follows the following protocols on a national basis, as these as they relate to Community Outreach Services:
Contractor is prohibited from marketing its services to veterans without prior approval from NMVAHCS. NMVAHCS reserves the right, at any time, to notify Contractor to discontinue or modify a particular part of the marketing plan or materials.
Contractor shall develop l500 copies of proposed Program Materials e.g., brochures (generally describing Contractor’s Primary Care program, clinic location and hours, and program highlights.
Samples of each proposed program materials shall be forwarded, for review and approval, to the Contracting Officer and to NMVAHCS Benefits Section (04E) and COTR.
Contractor must receive approval of the materials prior to dissemination to the veteran population. Contractor shall not engage in marketing practices that mislead, confuse, defraud, are unfair or
deceptive, or otherwise violates federal or state consumer protection laws or regulations. Contractor personnel shall be available to make presentations and provide tours of Contractor’s
facility to Veteran Service Organizations. Contractor will notify COTR and Business Manager of scheduled tours in advance.
A.2 RELEVANT EXPERIENCE PROVIDING HEALTHCARE SERVICES TO THE FEDERAL GOVERNMENT
This section is a sampling of Department of Defense contracts performed by Xxxxxx Xxxxx, which are additional services we provide outside of our CBOC program. These contracts have utilized some of the same primary care and mental health services that have been identified for the proposed contract at the Taos, New Mexico CBOC. Moreover, these contracts are also examples of the various sizes of contracts that Xxxxxx Xxxxx performs, which make visible the outstanding recruitment efforts, the diverse scope of practices involved in each contract and the dedication on behalf of Xxxxxx Xxxxx towards sustaining a long-lasting professional relationship with the respective Department of Defense branch through customer satisfaction.
Early Developmental Intervention Services (“EDIS”). Among the services that it provides, Xxxxxx Xxxxx currently staffs the overseas Early Developmental Intervention Services (EDIS) Program on a worldwide basis on behalf of the Army, Navy, and Air Force. Over 150 fulltime EDIS providers perform services on behalf of Xxxxxx Xxxxx on a full-time basis in the following locations: Germany, France, Belgium, the Netherlands, the United Kingdom, Spain, Portugal, Italy, Turkey, Guam, South Korea, and Japan. For the Early Developmental Intervention Services Program overseas, Xxxxxx Xxxxx provides all
9
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.

needed Developmental Pediatricians, Physical Therapists, Occupational Therapists, Speech/Language Pathologists, Early Childhood Special Educators, Clinical Psychologists, and Social Workers on behalf of military and State Department beneficiaries in the above nations.
In addition to staffing the Early Developmental Intervention Services Program on an OCONUS basis, Xxxxxx Xxxxx provides support for the EDIS Program in the United States, through its joint venture, Magnum Medical. Under this program, Xxxxxx Xxxxx provides all required early developmental intervention professionals on behalf of the Army and Air Force nationwide. Under a related contract, Xxxxxx Xxxxx provides a number of early development intervention professionals to the Navy as well.
Post-Deployment Health Reassessment (“PDHRA”). Xxxxxx Xxxxx currently provides support for the PDHRA program for military personnel. The PDHRA program is designed to identify and address health concerns, with specific emphasis on mental health, that have emerged over time since deployment. PDHRA services are offered to all service members who have returned from operational deployment, including all active duty service members, National Guard and Reserve members, as well as those who have separated or retired since their return from deployment. In particular, attention is paid to issues of behavioral health and specific screenings for Traumatic Brain Injury (TBI). Xxxxxx Xxxxx provides PDHRA support at the following locations: OCONUS Air Force PDHRA Psychology – five (5) Psychologists at Lakenheath, England; Incirlik, Turkey; Aviano, Italy; Ramstein and Spangdahlem, Germany.
Traumatic Brain Injury (“TBI”) Services. Xxxxxx Xxxxx is experienced in providing a range of psychological support services including TBI. Most recently, for example, Xxxxxx Xxxxx was awarded a contract from the Army to provide all TBI services overseas in Germany, Italy and Belgium. The behavioral health specialties include Adult and Child Psychiatrists, Adult and Child Psychologists, Neuropsychologists, and Psychiatric Nurse Practitioners or Psychiatric Nurses and Licensed Clinical Social Workers. Other specialties for the treatment of TBI included in this Contract include Neurologists, Neurosurgeons, Master’s level RN Case Managers, Physical Therapists and PTAs, Occupational Therapists and OTAs, Speech Language Pathologists, Physicians and Physician Assistants, Clinical Nurse Specialists and Licensed Practical/Vocational Nurses. The population served includes U.S. Army Soldiers in Basic or Advanced Individual Training, U.S. Army Soldiers pending deployment, U.S. Army Soldiers redeployed, U.S. Army Soldiers being evaluated for medical discharge from the service, U.S. Army Soldiers Wounded in Action (WIA) and their families, family members of U.S. Army Soldiers Killed in Action (KIA), deployment related medically unexplainable symptoms and other beneficiaries of the MHS.
Air Force OCONUS Psychological Health Services. Xxxxxx Xxxxx was awarded a contract to provide a range of psychological support services at Air Force installations under the Overseas Psychological Health Support Services (“OPHSS”) program. This service includes nine (9) clinical psychologists, five (5) clinical social workers and one (1) Psychiatrist for 17 overseas medical treatment facilities (MTFs) in seven (7) countries for the United States Air Forces in Europe (“USAFE”) and Pacific Air Force (“PACAF”) commands.
Air Force Medical/Administrative Support Services (“MASS Program”). Xxxxxx Xxxxx currently provides, as a subcontractor, RN Case Management services to military personnel at several Air Force MTF facilities in the United States and overseas. Our RN Case Managers often work with military beneficiaries who have both medical and mental health diagnoses. They are responsible to make appropriate referrals for mental health issues to TRICARE so that an appointment for consultation can be made. Additionally, for patients assigned to our Case Managers that already receive mental health support, all relevant information
10
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
related to care and case management for the patient is exchanged and coordinated between our Case Managers and the assigned mental health provider.
Army Corps of Engineers (“ACE”) Occupational Health Service. Xxxxxx Xxxxx currently provides Occupational Health Services on behalf of ACE’s South Atlantic Division and other Federal agencies who utilize the ACE Occupational Health Clinic within each Federal building. Our nurses provide occupational health services to personnel including case management and screenings for any mental health issues, and make appropriate referrals to ACE or other Federal agency Employee Assistance Program for follow-up care and treatment.
Also among its services, Xxxxxx Xxxxx provides large-scale services on behalf of the Army, Navy, and Air Force on both a direct contract and subcontract basis. Among these, Xxxxxx Xxxxx has successfully provided services under a number of Army multi-site contracts over its history. For the last 29 years, we have reliably supplied one of the scarcest medical specialties, Diagnostic Radiologists, to the majority of Army facilities nationwide. Locations at which Xxxxxx Xxxxx has provided all required Contract-supplied Diagnostic Radiologists for at least the past 15 years include Ft. Hood, TX, Ft. Gordon, GA, Redstone Arsenal, AL, Ft. Jackson, SC, and Ft. Irwin, CA.
Originally commencing services on behalf of military healthcare facilities in 1981, Xxxxxx Xxxxx has become one of the two largest providers in the world of direct healthcare services at military hospitals and clinics
A.3 ROSTER OF PRIMARY CARE STAFF INTENDED TO BE UTILIZED IN THE PERFORMANCE OF THIS CONTRACT
Xxxxxx Xxxxx possesses strong recruiting capabilities consisting of a large scale, in-house direct mail center. This direct mail center currently sends more than 1.5 million pieces of mail per year for recruiting purposes to qualified healthcare providers. The direct mail center can issue recruitment mailings with as little as one (1) business day lead-time.
Strong telemarketing efforts for recruiting efforts are conducted by Xxxxxx Xxxxx’s large team of in-house recruiters with telemarketing and customer service experience. These recruiters are supported by a state-of-the-art network telephone system, which possesses the capability of direct dialing telephone numbers based on each recruiter “clicking” on a licensed professional’s name with their computer mouse.
Xxxxxx Xxxxx regularly sponsors and provides marketing booths at nationwide professional conferences for recruiting purposes. Xxxxxx Xxxxx, for example, sponsored a recruiting booth at the American Academy of Family Practice’s Annual Scientific Meeting held in Chicago for over four (4) days. Over the term of the upcoming Contract, Xxxxxx Xxxxx hopes to provide marketing booths at a number of national conferences held by the American College of Internal Medicine and the American Academy of Family Practice.
Classified ad campaigns are run by Xxxxxx Xxxxx’s full-time Media Marketing Manager whose corporate role is devoted to placing classified ads, professional journal advertisements and establishing Internet recruiting campaigns.
Xxxxxx Xxxxx also uses a large scale classified ad purchasing company capable of nationwide coverage.
11
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
Through weekly volume purchases with this company, the cost of classified ads for recruiting is greatly reduced. This cost reduction, in turn, allows Xxxxxx Xxxxx to obtain more advertisements for its recruiting advertising budget than would otherwise be available, enhancing its recruiting capability.
Xxxxxx Xxxxx’s Media Marketing Manager places approximately ten (10) advertisements per week in the largest professional journal utilized for Physician recruiting, the Journal of the American Medical Association (“JAMA”). Ongoing advertisements in JAMA, purchased at a bulk contract rate on a weekly basis, will further enhance Xxxxxx Xxxxx’s recruitment capability throughout the term of the upcoming Contract. Additionally, Xxxxxx Xxxxx places regular weekly ads with the Annuals of Internal Medicine. These ads are placed at a discounted rate, increasing the cost effectiveness of Xxxxxx Xxxxx’s recruiting and marketing efforts.
Integral to its Internet recruiting efforts for qualified candidates, the company possesses nationwide resume search privileges on two of the largest general recruiting sites in the country: www.Monster.com and www.careerbuilder.com. In addition to these general recruiting sites, Xxxxxx Xxxxx also possesses nationwide resume search capability on the following web sites designed specifically to recruit healthcare professionals: www.physicianwork.com, www.absolutelyhealthcare.com, www.healthecareers.com, and www.aafp.com.
Through its extensive investment regarding nationwide search capabilities in all of the above general and healthcare-specific recruiting sites, Xxxxxx Xxxxx maximizes its ability to recruit qualified healthcare professionals in fulfillment of this Contract.
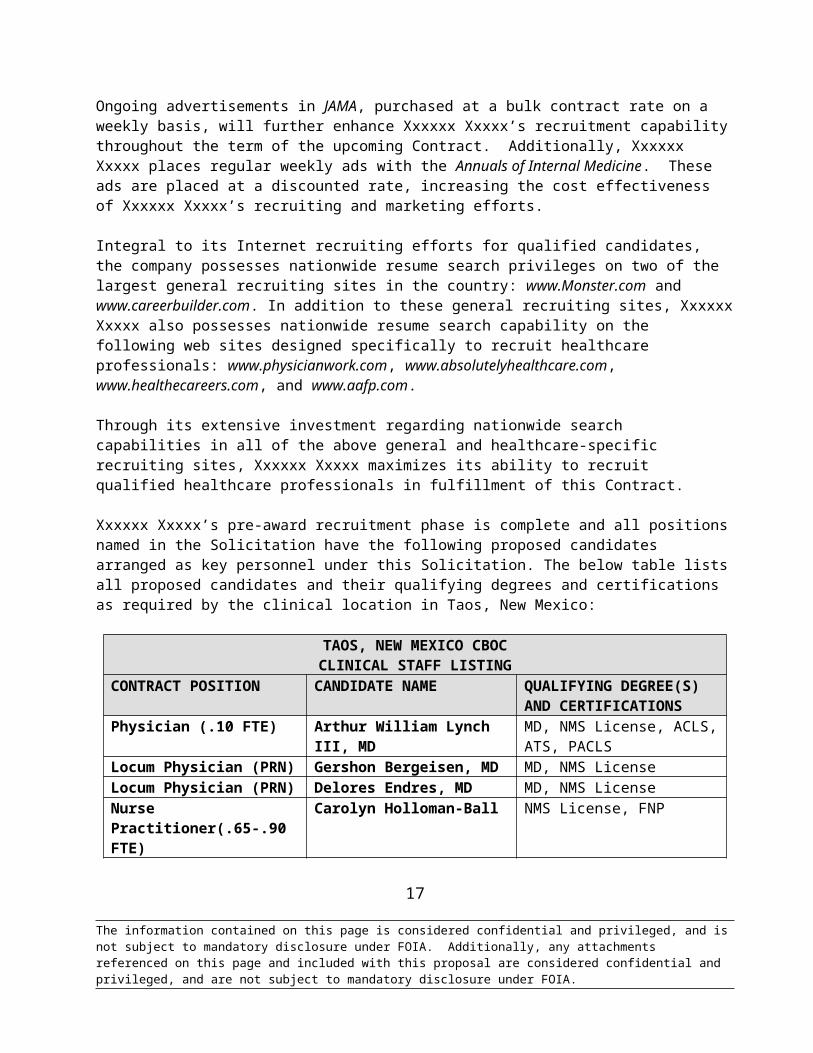
Xxxxxx Xxxxx’s pre-award recruitment phase is complete and all positions named in the Solicitation have the following proposed candidates arranged as key personnel under this Solicitation. The below table lists all proposed candidates and their qualifying degrees and certifications as required by the clinical location in Taos, New Mexico:
TAOS, NEW MEXICO CBOC CLINICAL STAFF LISTING
CONTRACT POSITION CANDIDATE NAME QUALIFYING DEGREE(S) AND CERTIFICATIONS
Physician (.10 FTE) Arthur William Lynch III, MD MD, NMS License, ACLS, ATS, PACLS
Locum Physician (PRN) Gershon Bergeisen, MD MD, NMS LicenseLocum Physician (PRN) Delores Endres, MD MD, NMS LicenseNurse Practitioner(.65-.90 FTE)
Carolyn Holloman-Ball NMS License, FNP
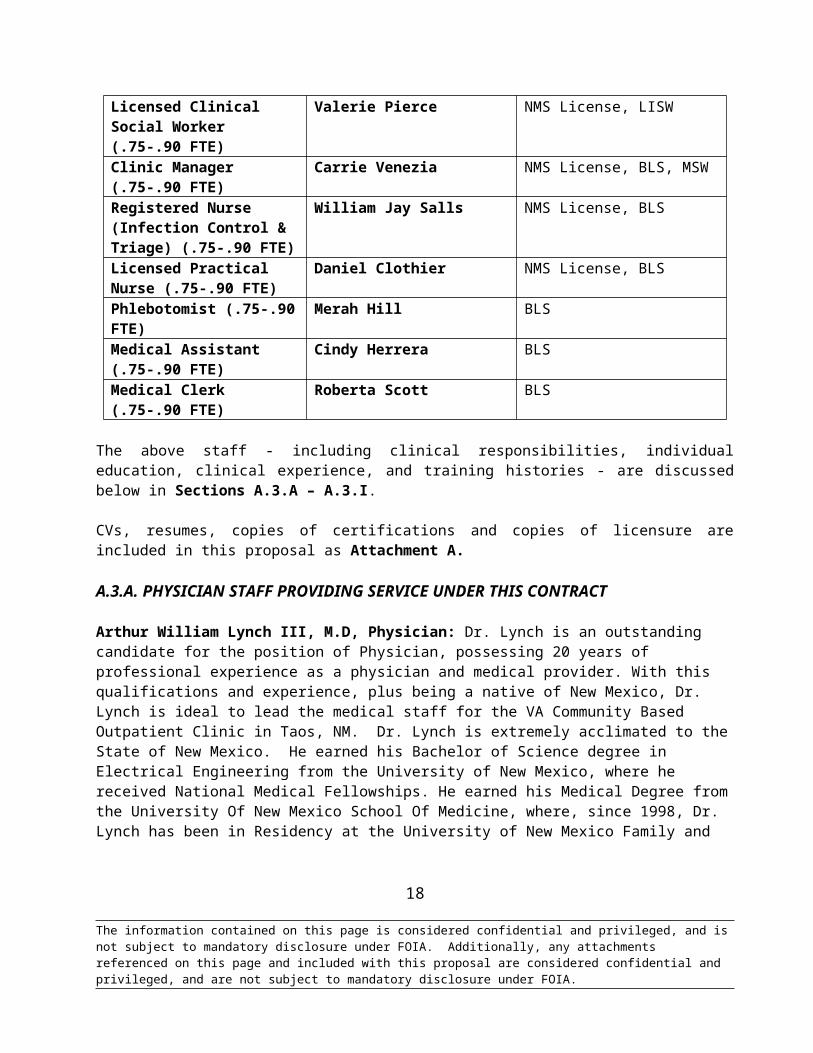
Licensed Clinical Social Worker (.75-.90 FTE)
Valerie Pierce NMS License, LISW
Clinic Manager (.75-.90 FTE) Carrie Venezia NMS License, BLS, MSWRegistered Nurse (Infection Control & Triage) (.75-.90 FTE)
William Jay Salls NMS License, BLS
Licensed Practical Nurse (.75-.90 FTE)
Daniel Clothier NMS License, BLS
Phlebotomist (.75-.90 FTE) Merah Hill BLS
12
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.

Medical Assistant (.75-.90 FTE)
Cindy Herrera BLS
Medical Clerk (.75-.90 FTE) Roberta Scott BLS
The above staff - including clinical responsibilities, individual education, clinical experience, and training histories - are discussed below in Sections A.3.A – A.3.I.
CVs, resumes, copies of certifications and copies of licensure are included in this proposal as Attachment A.
A.3.A. PHYSICIAN STAFF PROVIDING SERVICE UNDER THIS CONTRACT
Arthur William Lynch III, M.D, Physician: Dr. Lynch is an outstanding candidate for the position of Physician, possessing 20 years of professional experience as a physician and medical provider. With this qualifications and experience, plus being a native of New Mexico, Dr. Lynch is ideal to lead the medical staff for the VA Community Based Outpatient Clinic in Taos, NM. Dr. Lynch is extremely acclimated to the State of New Mexico. He earned his Bachelor of Science degree in Electrical Engineering from the University of New Mexico, where he received National Medical Fellowships. He earned his Medical Degree from the University Of New Mexico School Of Medicine, where, since 1998, Dr. Lynch has been in Residency at the University of New Mexico Family and Community Medical Center. He is a professional member of the Academy of Pain Management; Physicians for Social Responsibility; American Academy of Family Physicians; and the New Mexico Medical Society. Dr. Lynch Board certified in Family Practice, Advanced Cardiac Life Support, Advanced Trauma Support, and Pediatric Advanced Life Support. He is married to an Emergency Medicine Physician and is fluent in Spanish.
For the last decade, Dr. Lynch has been Physician at Taos/Picuris Indian Health Service, where his chief responsibilities are implementing treatments for pain care and being an urgent care provider. Concurrent with his work at Taos/Picuris Indian Health Service, Dr. Lynch has additionally worked since 2001 at the Colonias Chiropractic Center, a multi-disciplinary pain clinic. He utilizes his services primarily applying various pain management modalities including Trigger Point therapy and general medical management. In addition, Dr. Lynch has lent his services as a Physician for Mogul Medical Urgent Care since 2001. He provides primary and emergency care, training of Emergency Medical Technicians (EMTs), medical students, and resident physicians.
From 2001 to 2003, Dr. Lynch has worked tirelessly for the Health Centers of New Mexico, establishing Primary Care clinics in the rural locations of Penasco and Embudo. From 1991 to 1994, Dr. Lynch volunteered with the Albuquerque Mountain Rescue and Placitas Fire Brigade. Working as an Emergency Medical Technicians (EMT) and professional climbing guide and instructor, he organized and taught rescue classes. In addition to his many accomplishments, Dr. Lynch he was published in Crisis medical journal for his article, ‘Guns, Alcohol, and Intimate Partner Violence: The Epidemiology of Female Suicide in New Mexico’.
Dr. Lynch has lived and practiced medicine in the State of New Mexico his entire life. He has exemplary qualifications and two (2) decades of professional medical experience. His addition to the medical staff as Physician would be remarkably invaluable for the VA CBOC located in Taos, New Mexico.
13
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
Gershon Bergeisen, MD, Locum Tenens Physician: Dr. Bergeisen has extensive education and experience to be the Locum Tenens Physician for the Taos CBOC location in New Mexico. After completing her Bachelor’s and her medical degree at the University of California at Los Angeles, Dr. Bergeisen graduated from the Uniformed Services if Health Sciences (USUHS) in Epidemiology and then became a Distinguished Graduate from the School of Aerospace Medicine at Brooks Air Force Base, in San Antonio, Texas as a Flight Surgeon.
In addition, Dr. Bergeisen has remarkable knowledge from an educational perspective. From 1982-1984 he was an assistant professor at the University of Kentucky in the Department of Family & Community Medicine. From 1992 to 2003 he served as adjunct professor at the Uniformed Services if Health Sciences (USUHS) in Bethesda, Maryland in the Department of Preventative Medicine. Dr. Bergeisen has had numerous supervisory positions as well. From 2002-2005, he was Director of Employee Health Services and Attending Physician in Family Medicine at St. Joseph Regional Medical Center in Paterson, New Jersey. In 1987 and 1988 Dr. Bergeisen was Medical Director of the Health Centers of Northern New Mexico located in Espanola, New Mexico and served on the medical staff at Northeastern Hospital in Las Vegas, New Mexico. Dr. Bergeisen has served the health community in locations as far reaching as Alaska, South Dakota, Montana and Minnesota.
Dr. Bergeisen is a member of such professional and scientific societies such as; The American College of Occupational & Environmental Medicine; The American College of Preventative Medicine; The American Academy of Family Physicians; and The American Medical Association. He has been published a dozen times appearing in such venerable publications as, The Journal of the American Medical Association, American Journal of Public Health, and The Journal of Occupational Medicine. Dr. Bergeisen is fluent in four languages (English, Spanish, French and Dutch), and has working conversation in both German and Hebrew.
For the past two years, Dr. Bergeisen has been employed by Xxxxxx Xxxxx as a Family Practice Locum Tenens Physician at various locations. His most recent positions have placed him at United Health Centers in Parlier, California and Health Centers for Northern New Mexico. Given the vast range of experience and education, we contend that Gershon Henoch Bergeisen, MD., is an excellent candidate for providing Locum Tenens services for the Taos, New Mexico location.
Delores Endres, MD, Locum Tenens Physician: Dr. Endres is an excellent candidate for the position of Locum Tenens Physician. Possessing more than 30 years of professional experience as a physician, Dr. Endres will be an integral addition to the medical staff for the VA Community Based Outpatient Clinic in Taos, NM. Dr. Endres earned two Bachelor of Science degrees in Biology and Chemistry from St. Norbert College, and her Medical degree from the University of Wisconsin. She is fully licensed to practice medicine in the State of New Mexico, and is Board Certified by the American Board of Family Practice and the Fellow of American Academy of Family Physicians. Dr. Endres is a member of many professional medical societies; American Academy of Family Practice; Federal Physicians Association; Physicians for Social Responsibility; and The Professional Association of the Commissioned Corps of the U.S. Public Health. She is currently a resident of Taos, NM, and an active member of Taos Search and Rescue.
Dr. Endres possesses significant Locum experience in New Mexico. Since 2009, she has been Locum Tenens Physician at El Centro Health Centers and Pine Hill Health Center. Dr. Endres has additionally been Locum Tenens Physician at Isleta Health Center since 2010, and lent her services as a Locum for Family Practice Associates in Taos, New Mexico since 2005. Prior to her years of work as a Locum Tenens
14
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
Physician, Dr. Endres was Commissioned Officer in the Public Health Service, Indian Health Service branch. She retired from the position in 2005. From 1993 to 2005, Dr, Endres was the Clinical Specialty Consultant Physician for Taos/Picuris Indian Health Center. She was Medical Director for the Taos Indian Health Clinic from 1989 to 1993, and was General Medical Officer for Albuquerque Indian Hospital from 1984 to 1989.
Dr. Endres has additionally proven herself for her services on an ‘as needed’ basis. In 1992, she took a temporary duty assignment (TDY) for the Santa Clara Health Center in California, and 1982, Dr. Endres was a TDY Physician for the Peach Springs Service Unit in Arizona. Dr. Endres has demonstrated her abilities by volunteering in very isolated areas of world with limited resources. Working on behalf of various organizations, Dr. Endres has provided medical services in remote areas such as, Haiti, Peru, Belize, Honduras, Bolivia, Nicaragua, and Zimbabwe.
Dr. Endres possesses more than there (3) decades of professional medical experience as a physician. Notably, she is extremely familiar to the region and native cultures of Northern New Mexico. Given her exemplary qualifications and her past experience as a Locum, Dr. Endres is ideal for the position of Locum Tenens Physician for the VA CBOC located in Taos, New Mexico.
A.3.B. NURSE PRACTITIONER STAFF PROVIDING SERVICE UNDER THIS CONTRACT
Carolyn Holloway-Ball, FNP, Nurse Practitioner: Ms. Ball is an ideal candidate for the position of Nurse Practitioner for the VA CBOC in Taos, NM. She possesses more than 25 years of professional experience in the field of nursing. Ms. Ball has an impressive array of education. She earned her Associates Degree in Nursing in 1985, and her Bachelor of Science in Nursing in 1993 from the University of Mary Hardin Baylor. In 1996, Ms. Ball earned her Master’s of Science in Nursing Administration, and completed the Family Nurse Practitioner Program from Texas A&M University. In addition, Ms. Ball completed the Acute Care PNP certification program from the University of Texas. She fully licensed in the State of New Mexico, and is certified as a Neonatal Nurse Practitioner (NNP) and as a Family Nurse Practitioner (FNP). Ms. Ball is additionally certified in BLS and PALS.
Since 2005, Ms. Ball has been the Neonatal Nurse Practitioner (NNP), Family Nurse Practitioner (FNP), and Acute Care PNP for Holy Cross Hospital in Taos, NM. She manages newborns, attends high-risk deliveries, teaches Basic Life Support (BLS) to the staff. She additionally assists with administration, hospital management, and aids with the discharge of pediatric patients. Ms. Ball also lends her services as a Family Nurse Practitioner at Penasco Family Health Clinic. From 2003 to 2005, Ms. Ball was a Neonatal Nurse Practitioner for Allina Health Care (on behalf of Unity and Mercy Hospitals) in Minnesota. Her primary responsibilities comprised of basic NNP duties, medical management of newborns, attending deliveries and stabilizing sick newborns for transport.
Prior to her work in Minnesota, Ms. Ball was the Instructor of Maternal Neonatal Nursing at the University of Mary Hardin Taylor in Belton, TX. From 2003 to 2003, she taught classes and oversaw clinicals in OB-GYN (obstetric-gynecologic), neonatal and postpartum, and was elected by students to Student Nursing Association Faculty Advisor. From 1986 to 2004, Ms. Ball was employed as a Neonatal Nurse Practitioner for Scott & White Hospital in Temple, TX. She originally functioned as a charge nurse, transport nurse, and clinician. After becoming certified as a NNP, Ms. Ball performed the requisite duties associated with caring for newborns. Additionally while at Scott & White, Ms. Ball became a certified instructor and taught BLS,
15
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
CPR, and NRP. She also assisted in the updating of the computerized nursing charting system for the hospital.
With her education combined with years of professional nursing experience, Ms. Ball is more than qualified for the position of Nurse Practitioner. She will be an exceptional addition to the medical staff for the VA Community Based Outpatient Clinic located in Taos, New Mexico.
A.3.C. SOCIAL WORKER STAFF PROVIDING SERVICE UNDER THIS CONTRACT
Valerie Pierce, LICSW, Licensed Clinical Social Worker: Ms. Pierce has over 20 years of experience in her field of clinical social work and would make an excellent candidate for the position of Licensed Clinical Social Worker for the Taos, NM CBOC. Currently, Ms. Pierce is working as a private practitioner, providing outpatient behavioral health services to all ages. During the 2 years at her private practice, Ms. Pierce has performed social work services for Questa Independent Schools, providing social service and support to staff in K-12 multi-school settings. Prior to her starting her own practice, Ms. Pierce was a Behavioral Health Specialist for Presbyterian Medical Services, providing contract clinical social work services for Hospice/Home Health sites, outgoing assessment/treatment services for all ages, populations and most diagnoses.
Ms. Pierce received her Master of Social Work from Barry University in Miami, FL and began working as a Clinical Social Worker for the Northeastern Mental Health Center in Aberdeen, South Dakota, where she provided outpatient assessment/treatment services for all ages, populations and most diagnoses, consultation services, marketing & community outreach/assistance, court testimony in an outpatient clinic, home-based and nursing home setting. She worked as the Director of Behavioral Health for Hannahville Indiana Community in Wilson Michigan as well as for Heritage Health Services, where her combined responsibilities included staff supervision, program maintenance/development, marketing and quality assurance & risk management functions. We strongly believe that Ms. Pierce’s vast experience in her field would make her an excellent candidate for the Licensed Clinical Social Worker position at the Taos, NM CBOC.
A.3.D. CLINIC MANAGER STAFF PROVIDING SERVICE UNDER THIS CONTRACT
Carrie E. Venezia, Clinic Manager: Ms. Venezia is an outstanding candidate for the position of Clinic Manager. Possessing 18 years of professional experience, she will be a welcomed addition to the staff for the VA Community Based Outpatient Clinic in Taos, NM. Ms. Venezia is an experienced project support and operational manager will proven success in a variety of venues. She earned her degree in Business Administration from Hutchinson Community College, and is additionally a Certified Nursing Assistant (CNA). Ms. Venezia is proficient in MS Office (Word, Excel, PowerPoint, Access and Outlook), Citrix, Allscripts, Photoshop, and Adobe Acrobat. She has won numerous awards for her philanthropy and volunteerism.
Since 2010, Ms. Venezia has been the Director of Chamber Services for the Red River Chamber of Commerce in New Mexico. Her primary duties dealt with maintaining membership relations, preparing quarterly newsletters, soliciting new business, and fundraising through the Economic Development Committee. In addition, Ms. Venezia is the leader of staff management, and is responsible for the effective operation of the Visitor’s Center. From 2000 to 2010, Ms. Venezia was the Program Coordinator for the University of Arizona Cancer Center and the College of Pharmacy. As Program Director, she was the chief
16
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
liaison between administration and departments, especially assisting with the University Cancer Center, to ensure all offices were running at optimum efficiency. In addition, Ms. Venezia established budgets and analyzed prior year expenditures to forecast annual spending, presenting findings to key administrators for the purpose of recommending effective strategies. Her devotion to the University of Arizona earned Ms. Venezia the 2005 Staff Award for Excellence.
From 1998 to 2000, Ms. Venezia was the Division Coordinator for PCS Health Systems in Scottsdale, AZ. She was responsible for providing project and administrative support to key level decision makers, including Vice Presidents, Product Managers, and Development staff. Moreover, Ms. Venezia scheduled and coordinated meetings, interviews, appointments, events and other similar activities to improve overall operational efficiency. From 1993 to 1998, Ms. Venezia was employed by Shawnee Mission Medical Center as Private Duty Office Manager. She acted as lead strategist to develop plans in the opening of the Shawnee Mission Medical Center. Ms. Venezia was responsible for identifying the needs of the staff’s education and training. In addition, she managed inventory control, working with suppliers and service providers ensuring equipment was ready and available for both patients and staff.
Possessing nearly two (2) decades of experience, combined with a superb track record of efficiency. Ms. Venezia is more than qualified for the position of Clinic Manager. She will be an invaluable addition to the staff for the VA CBOC located in Taos, New Mexico.
A.3.E. REGISTERED NURSE STAFF PROVIDING SERVICE UNDER THIS CONTRACT
William Jay Salls, RN, Registered Nurse (Infection Control and Triage): Mr. Salls is an outstanding choice for the position of Registered Nurse (RN). Possessing more than seventeen years in the professional field of nursing, Mr. Salls will be an invaluable addition to the medical staff for the VA CBOC in Taos, NM. Mr. Salls earned his degree in Nursing from the New England Baptist Hospital School of Nursing in Boston, MA. He is certified in BLS, ACLS, PALS, TNCC, ENCP, and NRP. In addition, Mr. Salls is certified by the New Mexico Board of Nursing.
From 2010 to the present, Mr. Salls has been employed as a Registered Nurse for SDPI Healthy Heart, IHS, TPHS in Taos, NM. His responsibilities are quite comprehensive. He educates patients with Diabetes Type II, and at risk for and or diagnosed with CVD, refers patients to appropriate team members of Health Heart Project and Clinic. He maintains constant updating and monitoring of educational tools in reaching patients and prevention of furthering disease process, collaborates with Medical, Healthy Heart and Behavior Health staff for best results for patients to understand and cope with Diabetes and prevent further disease process. And he additionally assists with development of methods and protocols for educating pts as required by SDPI Healthy Heart Grant and Tribal and Cultural requirements. In 2009, Mr. Salls was an RN for Correctional Medical Services in Santa Fe, NM. He performed emergency care and triage, Assessments, medical decision making for inmates in maximum security prison setting, and provided care for patients.
From 2006 to 2009, Mr. Salls was employed in the Emergency Department as a Registered Nurse at Spanish Peaks Regional Hospital, Walsenburg, CO and at Holy Cross Hospital, Taos NM. His duties dealt with all aspects of Emergency Services
17
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
including triage, trauma care, and providing care for ground/air transport of critically ill patients. In addition, Mr. Salls was responsible for training new nursing graduates.
Mr. Salls possesses nearly two (2) decades of professional experience combined with an excellent education. Mr. Salls additionally has years of expertise in both triage and emergency services. He is an ideal candidate for the position of Registered Nurse with a concentration In Infection Control and Triage. Mr. Salls will be a welcomed asset to the medical staff for the VA CBOC located In Taos, New Mexico.
A.3.F. LPN STAFF PROVIDING SERVICE UNDER THIS CONTRACT
Daniel K. Clothier, LPN, Licensed Practical Nurse: Mr. Clothier is an excellent candidate for the position of Licensed Practical Nurse. Possessing over 15 years of professional experience in the field of nursing, he will be a valued asset to the medical staff for the VA Community Based Outpatient Clinic in Taos, NM. Mr. Clothier has an impressive education with several degrees. He holds Associate’s degrees in Nursing, Addictionology, Law Enforcement and General Studies. Mr. Clothier is fully licensed to practice nursing in the State of New Mexico and is BLS, CPR, AED and Paramedicine certified. He is an honorably discharged veteran of the US Army National Guard.
Since 2008, Mr. Clothier has worked as both a nurse and therapist for the residential alcohol and drug rehabilitation Vista Taos Renewal Center. His therapist duties include, but are not limited to, treating patients suffering from codependence, eating disorders, and substance abuse. He additionally provides vocational advisements for patients, creating patient care plans, and medical histories. Mr. Clothier’s nursing responsibilities comprise of emergency care, patient assessments, taking phone orders, and communicating medical advisement to the clinical staff. Moreover, Mr. Clothier actively facilitates patient transport, and providing staff training as the primary BLS and First Aid Instructor.
Prior to his work at Vista Taos Renewal Center, Mr. Clothier was a Licensed Practical Nurse at San Cristobal Ranch Academy. His primary responsibilities included oversight of the clinical staff, patient counseling, nursing, and basic medical education. Mr. Clothier additionally created a Search and Rescue Team officially recognized by the State of New Mexico. From 2006 to 2010, and concurrent to his work at both Vista Taos Renewal Center and San Cristobal Ranch Academy, Mr. Clothier was employed as a Licensed Practical Nurse for Holy Cross Hospital. Working primarily in the Medical/Surgical unit, Mr. Clothier was a member of the Impaired Employee Support Team. His basic duties involved providing patient assessments, wound care, performing transfusions, and administering medication. From 1977 to 1988, Mr. Clothier was a Paramedic for the City of San Diego.
Mr. Clothier is an extremely accomplished individual, possessing years of professional experience in the field of nursing. He will be an invaluable addition to the staff as a Licensed Practical Nurse for the VA CBOC located in Taos, New Mexico.
A.3.G. PHLEBOTOMIST/MEDICAL ASSISTANT STAFF PROVIDING SERVICE UNDER THIS CONTRACT
Merah Hill, Phlebotomist: Ms. Hill is an excellent candidate for the position of Phlebotomist. With over three (3) years of professional experience, she will be a valuable addition to the support staff for the VA Community Based Outpatient Clinic in Taos, NM. Ms. Hill earned her degree in Applied Science in
18
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
Medical Technology from Tulsa Community College. She is a professional member of The American Society for Clinical Pathology (ASCP) and the American Society for Clinical Laboratory Science (ASCLS). Ms. Hill is BLS certified.
In 2010, Ms. Hill was employed as a Medical Laboratory Technician for Utica Park Clinic in Tulsa, OK. She was responsible for reporting of diagnostic laboratory procedures, processing specimens, plus the maintenance and validation of laboratory instruments. In addition, Ms. Hill monitored quality control programs in order to provide superior patient care. In 2009, Ms. Hill was a Client Specialist for St. Johns Medical Center in Tulsa, OK. She received, ordered and processed clinical laboratory specimens as well as assuring that tested specimens met all necessary requirements. Prior to her work at St. Johns Medical Center, Ms. Hill was employed by the Diagnostic Laboratory of Oklahoma. From 2007 to 2008, she processed specimens, performed data entry in QLS, and maintained the preparation of all specimens.
With years of professional experience in the field of medicine, coupled with her education, Ms. Hill is exemplary choice for the position of Phlebotomist for the VA CBOC located in Taos, New Mexico.
A.3.H. MEDICAL ASSISTANT STAFF PROVIDING SERVICE UNDER THIS CONTRACT
Cindy Herrera, Medical Assistant: Ms. Herrera is an excellent choice for the position of Medical Assistant. Possessing more than 13 years of providing patient safety and care, she will be a welcomed addition to the support staff for the VA Community Based Outpatient Clinic in Taos, NM. Ms. Herrera has proven expertise in infection control, bone density screening, orthopedics, and machine calibration. She is a strong leader with success directing highly skilled professionals in supporting and achieving operational objectives, and is able to train peers and rapidly gain proficiency in new techniques and advancements. She is fully proficient in MS Windows, Office, PACS, and RIS Systems. Ms. Herrera received her Associate of Applied Science Degree in Radiologic Technology from Northern New Mexico Community College. She is fully licensed in the State of New Mexico and is AART, BLS/CPR certified.
Since 2010, Ms. Herrera has been employed as a Medical Assistant and X-Ray Technologist at Taos Urgent Care Center-Taos, NM. Her duties comprise of assisting physicians with patient care, procuring lab cultures, drawing blood, and administering injections. Prior to her work at Taos Urgent Care Center, Ms. Herrera was an X-Ray Technologist at Physicians Medical Center of Santa Fe, NM. From 2009 to 2010, she performed extended patient care from registration through post-op for the clinic employing up to 100 staff. She additionally assisted healthcare providers in a broad variety of radiology-related assignments. From 2006 to 2009, Ms. Herrera was employed by Santa Fe Imaging as an X-Ray Technologist. Working with a staff of 80 providers, her responsibilities included performing radiology imaging, greeting patients, performing office duties, collecting pathological information, and serving as bone densitometrist. From 1997 to 2006, Ms. Herrera served as X-Ray Technologist for Orthopedic Associates of Northern New Mexico. She provided patient care, operated advanced radiological technology, and assisted orthopedic technicians in day-to-day assignments. In addition, Ms. Herrera ordered and tracked supplies, filed patient charts and films, and assisted physicians with basic medical procedures.
Ms. Herrera has personally contributed to multiple achievements in many highly respected departments, and is open to any modality training available in order to contribute to the VA. She has suburb qualifications and sound experience in the field of medical care. Ms. Herrera will be an extremely valued asset as a Medical Assistant for the VA CBOC located in Taos, New Mexico.
19
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
A.3.I. MEDICAL CLERK STAFF PROVIDING SERVICE UNCER THIS CONTRACT
Roberta Scott, Medical Clerk: Ms. Scott is an exceptional candidate for the position of Medical Clerk for the VA CBOC located in Taos, NM. She possesses fifteen years of professional experience within the field of medical care, working specifically in medical recording, billing and coding. Ms. Scott earned her degree from Northern New Mexico Community College, is both certified as a Certified Nursing Assistant (CNA) and Medical Transcriptionist, and is fluent in English and Spanish.
Since 2004, Ms. Scott has been Medical Record/Referral Specialist for El Centro Family Health in Embudo, NM. Her responsibilities comprise of copying and maintaining records for patients, attorneys, and staff, assisting Veteran patients, completing insurance and Medicaid forms, preparing medical charts, performing office/secretarial duties, and training staff with new software. Prior to her work at El Centro, Ms. Scott was employed at the Women’s Health Institute in Taos, NM. She was supervisor for all medical records, assisted with appointments and scheduling, copied records for all patients and staff, and authorized referrals for specialty services when necessary. From 2003 to 2004, Ms. Scott was Medical Record/Referral Specialist for Los Alamos Medical Center, and from 1999 to 2002, she was Medical Record/Referral Specialist for the Health Centers of Northern New Mexico. Her duties at both facilities included, but were not limited to, maintaining medical records, assisting Veteran patients, performing front desk tasks, and assisting the Clinic Manager with all remaining responsibilities.
Ms. Scott is extremely well versed in all present medical terminology and procedures. With her years of experience and dedication, she is more than qualified for the position of Medical Clerk. Ms. Scott will be an essential and welcomed addition to the support staff to the VA Community Based Outpatient Clinic in Taos, New Mexico.
A.4. ROLES/RESPONSIBILITIES OF PROPOSED TAOS CBOC PERSONNEL
Physician - The Physician is responsible for providing a comprehensive range of outpatient medical services on behalf of the veteran population served by the clinic.
The Physician provides medical care which may be complex in nature in order to provide overall professional diagnostic assessment, treatment, and referral, as applicable on behalf of veteran beneficiaries. Clinical specialty areas impacting the patient population include: cardiovascular disease/hypertension, oncology, obesity/geriatric medicine, diabetes, infectious disease, and gerontology/neuropsychiatric disease, as well as common medical conditions such as URI, lower back pain, skin lesions, flu syndrome, strep throat, migraine headaches, and the like.
A high incidence of chronic diseases with multiple risk factors in the patient population must be recognized in determining the appropriate work schedules for the Physician and selecting appropriate continuing education.
The Physician will be required to perform and/or oversee the administration of vaccines and supplements, including: influenza vaccines, pneumovax vaccines, vitamin B-12, tetanus vaccines, and hepatitis B treatments. The Physician will ensure that all prescriptions are appropriate to treat the affecting condition in accordance with all VA regulations. The Physician will perform women’s health services, including, but not limited to: annual PAP and pelvic exams per VA clinical standards, annual clinical breast exams and
20
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
mammogram referrals if appropriate, family planning services, management of conditions related to menopause, osteoporosis screening, and other services as they pertain to care of the female patient.
The Physician will provide clinical services that meet the needs required by the management of complex cases in order to ensure both high quality care and continuity of service.
The Physician will complete timely documentation of all incidents of patient encounter, including patient history, diagnosis, treatment, and any consultation or referrals indicated.
All care will be provided in accordance with all applicable care standards established by the American Medical Association and the American College of Internal Medicine, as applicable.
Locum Physician - The duties of the Locum Physician are identical to the Physician and are performed by the Locum Physician at the clinic when the full-time Physician is unavailable to work. One active Primary Care Locum will be experienced at all times under the Contract in provision of VA CBOC services at alternate VA CBOC locations on behalf of Xxxxxx Xxxxx and will maintain VETPRO currency by performance of services within the VA system of care somewhere within Xxxxxx Xxxxx’s national CBOC system every 30.
Nurse Practitioner - The Nurse Practitioner will provide medical care in order to provide professional medical treatment as applicable on behalf of veteran beneficiaries. Clinical specialty areas impacting the patient population include: cardiovascular disease/hypertension, oncology, obesity/geriatric medicine, diabetes, infectious disease, and gerontology/neuropsychiatric disease as well as common medical conditions such as URI, lower back pain, skin lesion, flu syndrome, strep throat, migraine headaches, and the like.
The Nurse Practitioner will be responsible for a regularly appointed clinic that in compatible with the workload and, further, able to provide immediate evaluation and management of emergent problems as they arise. The Nurse Practitioner will have the capability to collect and record, in proper format, medical and social historical data appropriate to the patient’s condition. The Nurse Practitioner will also have the capability to perform general physical examinations, record their findings in the proper format and determine medical qualifications for a variety of purposes.
It is the responsibility of the Nurse Practitioner/Physician Assistant to provide a full range of services on an outpatient basis including supervising and providing general screening and medical care and examinations of patients for routine, acute, and chronic conditions involving any and all organ systems; as well as providing diagnosis, treatment, and patient counseling as indicated. The Nurse Practitioner will promote preventative and health-maintenance care, including annual physicals, positive health behaviors, and self-care skills through education and counseling. She/he will coordinate patient care through a continuum and facilitate the achievement of optimal outcomes in relation to care for VA beneficiaries.
The Nurse Practitioner will collaborate with a Physician in the healthcare of patients with chronic illnesses. In other appropriate situations, it is the responsibility of the Nurse Practitioner/Physician Assistant to request patient consultation or referrals with a Physician, clinic, or other health resource as indicated.
The Nurse Practitioner will prescribe and dispense medications authorized under Mississippi State law. The Nurse Practitioner/Physician Assistant will order diagnostic tests as applicable.
21
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
The Nurse Practitioner will be responsible for ensuring that VA guidelines are met in regards to preventative care, clinical practice guidelines, adverse event reporting and any other issues that logically pertain to the provision of quality outpatient care.
The Nurse Practitioner will also be required to clearly communicate to other health personnel orally or in writing, the finding, diagnosis and planned treatment in accordance with VA and VHA guidelines. All patient records will be kept in CPRS in accordance with all applicable VA policies. All patient care activities will be documented in the electronic record.
The Nurse Practitioner: (1) Must be a graduate of an accredited Nurse Practitioner and be certified by the American Nursing Association in either Adult Health or Family Practice. (2) Must hold an active, current, full and unrestricted state license and operate only within scope of that license and acceptable community standards of practice.
Licensed Clinical Social Worker - The Social Worker staff will provide, evaluate, assess, diagnose, treat, and follow-up by utilizing the therapeutic modalities of individual, marital, family, and group therapy to address family and marital problems and adjustment difficulties. Social Worker will coordinate comprehensive treatment needs as a member of a multi-disciplinary team.
The Social Worker staff shall counsel individuals/families as referred, to explore basic personality structures and behavior patterns in relationships, the mechanisms and symptoms of the specific adjustment problem and its underlying causes and consequences to the individual/family. In the course of individual/family counseling, Social Worker shall discuss behavioral responsibility, motivation and attitudes in achieving redirected behavior.
Social Worker staff shall provide crisis intervention and therapy to referred clients, maintain a therapeutic relationship with the patient/family during treatment and rehabilitation, and collaborate with civilian agencies in case follow-up and closure.
Conduct psychosocial evaluations and provide therapeutic interventions including medical management.
Social Worker staff will display tact and courtesy to all persons, either in person or on the telephone, regardless of circumstances.
The licensed social worker: (1) Must have a Masters or Doctorate of Social Work from a graduate school of Social Work accredited by the Council on Social Work Education (CSWE). (2) Must be capable of practicing independently with a current, active, full and unrestricted New Mexico License as a Licensed Clinical Social Worker (LCSW) for a reimbursable practice.
Clinic Manager - The person in this position is responsible for providing a comprehensive range of management duties. This person is responsible for supervising the entire staff of the clinic. It is the policy of Xxxxxx Xxxxx that supervision is done with fairness and no discrimination of any kind. Any problems that occur with staff should be brought to the immediate attention of the Program director. This person is responsible, in clinics where we are charged with the enrollment process, when necessary, to assist entering 10-10’s into the CPRS to ensure that new patients are appointed in a timely manner.
22
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
It is the clinic coordinator’s responsibility to schedule staff to cover during lunch hours as well as scheduled time off and sick time. Coverage for providers will be provided by the corporate office. Staff, including providers, must complete a request for scheduled time off. Provider requests should be forwarded to the National Program Director.
The Clinic Coordinator will keep personnel files on his/her staff. These will include all demographic information on the employee along with a copy of the employee’s signed position description, copies of pertinent licenses, requests for leave, absence reports, and any actions of discipline.
She/he will also, in OSHA compliance, keep a medical file on each employee. These will include, copy of OSHA required medical record, immunization record, and hepatitis B vaccine or declination of.
It is of extreme importance that the Clinic Coordinator take very seriously OSHA> ALL compliance measures must be met in your clinic.
This person is responsible for insuring that all quality measures are met in the clinic. She/he will provide, at the end of each month, all necessary materials for the QA process to the Program Office.
She/he will also conduct, upon return of the providers QA, meetings with the provider and lead Nurse to discuss the results of the QA and ways in which quality measures may be better met.
She will also aid the VA Medical Center in any QA they require.
Staff meetings are to be conducted on a regular basis by the Clinic Coordinator. These should occur at least once a month, more if there are concerns to discuss. The Clinic Coordinator may invite the National Program director for a teleconference staffing if she would like assistance.
This person is responsible for all reporting that the National Program Director requires. These include, but are not limited to, daily stats, weekly payroll, and monthly QA.
The Clinic Coordinator is responsible to document all incidents of employee discipline.
This person will complete timely documentation for all activities as required by clinic procedure and supervisory instructions.
Prompt response to communications and messages is considered imperative, including the routing of any necessary information to persons who need to be aware of it.
Discussions with the medical center with regard to Sterling policy or concerns with the clinic should be discussed promptly with the National Program Director.
In the event concerns arise on the Clinic Coordinator’s part regarding our collaboration with the medical center, they too should be promptly brought to the Program Director’s Attention.
It is essential that this person develop relationships with other team members and supervisors that facilitate two-way communication and discussion of working relationships.
23
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.

It will also be demonstrated that she conveys a willingness to extend self to meet the needs of the team. She can accept constructive criticism, consider it, and act upon it.
Licensed Practical Nurse - The person in this position is responsible for providing a comprehensive range of nursing services within the scope of practice for a LPN. This person will also be responsible to keep exam rooms stocked. This person will maintain appropriate CEU’s as required by the State of New Mexico Board of Nursing, and will maintain current CPR.
In assisting the provider this person will prepare patients to be seen, i.e. vitals, review of medications, reason for visit, and follow all diagnostic protocol.
This person will also perform other procedures such as; EKG’s, ear irrigation’s, injections, dressings, throat cultures, Accu checks, breathing treatments, and patient teaching.
This person will complete timely documentation for all activities as required by clinic procedure and supervisory instructions. This LPN is also responsible or other timely written reports as indicated by the needs of the patient and/or clinic procedures.
Prompt response to communications and messages is considered imperative, including the routing of any necessary information to persons who need to be aware of it.
The LPN will also assist in filing and answering the phones as needed.
Employee will ensure all mandated trainings be completed in appropriate time frames. It is essential that this person develop relationships with other team members and supervisor that facilitates two-way communication and discussion of working relationships.
Phlebotomist - The person in this position is responsible for providing a comprehensive range of phlebotomy services. This person is responsible for venipuncture as requested by the providers. This person will assure that all specimens are marked accurately and prepared for transfer to the lab. They will also need to do the encounter forms for all labs drawn and schedule all lab appointments. Any on line information required by the hospital will also be the responsibility of this individual. They will order any supplies needed by completing a PO and forwarding it to the Program Office.
This person will complete timely documentation for all activities as required by clinic procedure and supervisory instructions. This Technician is also responsible for other timely written reports as indicated by the needs of the patient and/or clinic procedures.
Prompt response to communications and messages is considered imperative, including the routing of any necessary information to persons who need to be aware of it.
This position may require repetitive bending.
This Technician will also assist in filing and answering the phone as needed.
It is essential that this person develop relationships with other team members and supervisor that facilitates two-way communication and discussion of working relationships.
24
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
Medical Clerk - The person in this position is responsible for providing a comprehensive range of enrollment and data entry duties.
All 10-10's completed and turned into clinic will be entered within 24 hours. 10-10's that are received as a result of a marketing promotion will be entered within one week of receipt.
The person in this position will at times have to travel to areas where there is a health fair or convention to discuss the enrollment process and the benefits that the VA has to offer.
This person will schedule all appointments for enrollments in VistA, following the designated template. Each individual will be contacted by phone once the 10-10 has been entered to be offered an appointment. If the patient is not reachable by phone a letter will be sent advising the patient that they have been enrolled in the clinic and asking them to contact the clinic to schedule an appointment. Any individual not eligible for benefits will receive a letter informing them of the decision and all original paperwork will be kept on file at the clinic.
This person will send all eligible veterans a letter of acceptance.
This person is responsible to answer all calls coming into clinic in regards to enrollment and benefits. This person is also responsible to help all individuals who require additional help filling out enrollments forms or means tests either in person or on the telephone.
The person in this position is responsible to report all new patients, add backs, and deaths on designated spreadsheet. At the end of every month this person is responsible to fax all enrollment logs to the corporate office in Cincinnati.
The person in this position is responsible to clarify any eligibility in computer that is showing "IN PROCESS". Which includes but not limited to if the person needs a means test, or proof of Active Duty. Once clarification has been made then this person is responsible to send clarification to Health Eligibility Center in Albuquerque, New Mexico or as directed by the parent VA Hospital.
This person is responsible for taking the pictures and processing the Veteran Identification Cards for the veteran.
A.5 METHODS AND MECHANISMS XXXXXX XXXXX WILL USE TO PROVIDE, QUALIFY, AND RETAIN QUALIFIED STAFF FOR THE REQUIRED POSITIONS
Xxxxxx Xxxxx’s mechanism used to provide qualified physicians, physician assistants, nurse practitioners, and primary care provider staff to perform the Contract work is divided into three (3) primary sections:
1. Our plan for recruitment2. Our plan for credentialing3. Our plan for long-term retention of employees
Accordingly, these mechanisms are delineated further below.
25
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
A.5.A XXXXXX XXXXX’S PLAN FOR RECRUITMENT
Based upon 30 years of experience in staffing medical programs, Xxxxxx Xxxxx has developed and continuously refined a time-tested process to recruit and credential highly qualified staff, retain the staff and provide training for staff.
Xxxxxx Xxxxx possesses the documented recruiting capability for ongoing staff recruitment, in order to assure effective fulfillment of any replacement provider or staff needs or new provider or staff expansion.Throughout its recruiting efforts, Xxxxxx Xxxxx will draw upon its 30 years of experience in healthcare provider and staff recruiting in support of VA and military staff requirements. Since it commenced service under its first federal contract for provision of health care, Xxxxxx Xxxxx has recruited the full range of healthcare provider and staff specialties for service at Government-sponsored medical centers, hospitals and clinics.
For the proposed Contract, recruitment of new providers will be centralized at Xxxxxx Xxxxx’s corporate office where 21 full-time healthcare recruiters, with extensive experience in recruiting the full range of healthcare specialties on behalf of government healthcare facilities, are based.
Additionally, a specifically assigned Lead Recruiter will oversee recruitment efforts for this project, based at the corporate office, will provide service. The Lead Recruiter possesses extensive experience in recruiting healthcare and counseling professionals, including providers providing service on behalf of VA beneficiaries. In performance of duties, the Lead Recruiter will be assisted by at least two (2) full-time Staff Recruiters. These Staff Recruiters will also possess extensive experience recruiting healthcare professionals on behalf of the VA and military professionals.
The Lead Recruiter and Staff Recruiters have and will continue to utilize Xxxxxx Xxxxx's established and proven methods for recruitment of providers, including the following:
Large scale direct mail campaigns to qualified licensed providers Targeted nationwide telemarketing Classified ad campaigns in regional news media Extensive professional journal advertisements Extensive Internet searches for qualified candidates Utilization of E-mail blasts Utilization of Xxxxxx Xxxxx's existing internal database of qualified professional counselor
candidates
These methods are described in greater detail below:
Direct Mail Campaigns – Xxxxxx Xxxxx regularly utilizes direct mail campaigns as a recruitment method. Direct mail flyers, properly targeted and sent on a large-scale basis, are an extremely effective means of recruiting for professional positions. Direct mail campaigns are a very powerful tool in the recruiting organization’s toolbox, and are particularly effective for recruiting over a wide area for a number of professional positions. Xxxxxx Xxxxx presently sends out over 1.5 million direct mail pieces a year, both on a computerized and manual, handwritten basis. Xxxxxx Xxxxx sends out a variety of correspondence via traditional mail, including personalized letters and glossy, high resolution postcards.
26
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
Nationwide Telemarketing Campaigns – Telemarketing or cold calling potential candidates is a very resource-intensive, proactive, and productive form of recruiting and is essential to any highly successful recruitment effort. For targeted recruiting of a particular geographic area, telemarketing by several experienced recruiters is extremely effective in identifying candidates who would not be reached through less proactive methods. For telemarketing purposes, Xxxxxx Xxxxx utilizes customized lists, obtained from a number of different proprietary sources, to conduct its telemarketing campaigns.
As a key component of its telemarketing campaign, Xxxxxx Xxxxx employs a sophisticated, software-based autodialer program that enables highly targeted recruitment of qualified professionals. Each corporate recruiter has a PC-based autodialer program which automatically loads candidate phone numbers into an onscreen dialog box. Recruiters can view the name of each candidate, the location of each candidate, and each candidate’s phone number. Additionally, a notes column enables recruiters to add annotations and comments. After calling individual candidates via the autodialer, recruiters are instructed to either annotate the events of each conversation or mark the candidate as unavailable/uninterested. Subsequently, uninterested candidates are removed from the autodialer database.
Throughout and at the end of each day, recruiters can print out a summary report of their telephonic recruitment efforts. Notably, this report features all details related to contacted candidates, including any pertinent notes resulting from discussions between recruiter and candidate (e.g. a recruiter might note a particular candidate’s desired start date or a candidate’s desire to relocate to certain area). This report can be used by senior management to note recruitment productivity and recruitment trends and, subsequently, more efficiently tailor extant telephonic recruitment efforts to individual requirements. Since implementing the above described autodialer system, Xxxxxx Xxxxx has noted recruitment efficiency increases of approximately 50%.
Classified Advertisement Campaigns in Regional News Media – Classified advertisements in general publications, particularly Sunday newspapers, can be an effective method of recruiting qualified candidates. Such advertisements have short lead times, as short as 48 hours for ads placed on Friday, and may reach significant numbers of candidates. Xxxxxx Xxxxx regularly places classified advertisements in local and regional news media sources throughout the United States and abroad.
Classified Advertisements in Professional Journals – In addition to classified newspaper advertisements, Xxxxxx Xxxxx regularly places classified advertisements in a wide variety of national professional publications. Classified advertisements in professional journals are a very effective way of recruiting qualified, specialized professionals. By utilizing professional journals, Xxxxxx Xxxxx specifically targets specialized professionals that may be otherwise difficult reach using more traditional methods of advertising.
Examples of Professional Journals in which Xxxxxx Xxxxx places classified advertisements include – but are not limited to – journals published by the following organizations:
The American Case Management Association The Case Management Society of North America The American Society of Radiologic Technologists The American Optometric Association The American Nurses Association The American Academy of Physician Assistants
27
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.

The Physician Assistant Foundation The American Occupational Therapy Association The American Physical Therapy Association The American Psychiatric Association The American Journal of Speech Language Pathology The American Psychological Association The American Association of Neurological Surgeons The American Academy of Neurology The American Neurological Association The American Academy of Family Physician The International Association of Physicians The American College of Physicians The American Medical Group Association The American Medical Association
An example of a professional publication which we will utilize in support of the current requirement is The Journal of the American Medical Association (“JAMA”). Notably, JAMA has the largest circulation of any medical journal in the world and is received each week by physicians in virtually every practice and setting. In fact, JAMA generates advertising exposure among more medical specialties than any other single title.
Extensive Internet Searches for Qualified Candidates – Xxxxxx Xxxxx regularly uses the internet, in a variety of capacities, to develop an ongoing pool of potential candidates. Due to the fact that Internet advertisements possess short lead times, internet advertisements can be used, like the general classified ads, for immediate openings. For this Solicitation, Xxxxxx Xxxxx has utilized and will continue to utilize search keys and posting capabilities for the following websites:
SITE NAME URLAbsolutely Healthcare Job Bank www.healthjobsusa.comHealthECareers www.healthecareers.comADVANCE for Nurse Practitioners www.nurse-practitioners.advanceweb.comAmerican Academy of Family Physicians www.aafp.orgPSYRIS: Psychology Resource Information Network http://psyris.comPA World http://www.paworld.netNP World http://www.npworld.netThe American Nurses Association http://www.nursingworld.orgHospital Jobs Online http://www.hospitaljobsonline.comMonster.com www.monster.comCareerBuilder.com www.careerbuilder.com
Xxxxxx Xxxxx employs the above sites to contact and recruit qualified personnel. Additionally, if the successful offeror under a particular procurement effort, Xxxxxx Xxxxx continues to utilize Internet employment sources throughout the life of this contract to ensure continuity of service. Internet advertising is an effective method of recruitment, because candidates who respond to advertisements posted on the Internet are generally computer literate, and possess skills important for successful employment. However, Xxxxxx Xxxxx never substitutes Internet advertisement campaigns for more resource intensive forms of recruitment such as telemarketing.
28
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
Utilization of E-Mail Blasts – E-mail blasts are an effective way of electronically reaching a large number of qualified providers. Using data collected from Monster.com, Careerbuilder.com, and proprietary lists constructed from Xxxxxx Xxxxx’s extant databases, Xxxxxx Xxxxx recruiters can send a form e-mail (with personalized salutation reflecting individual candidate names) to a number of qualified candidates. Responses to e-mail blasts are directed towards specific recruiters, thus enabling an efficient, effective mechanism to quickly reach a number of candidates.
In order to effectively reach candidates via e-mail blasts, Xxxxxx Xxxxx utilizes the Mach5 Mailer software program. The Mach5 is a powerful, scriptable permission e-mail marketing software program which enables Xxxxxx Xxxxx to efficiently send mass-customized messages to potential candidates. The Mach5 enables connectivity to any data source, including both Native sources and ODBC data sources (e.g. MS Access, MS Excel, and Oracle). Additionally, the Mach5 software program features integrated PHP, Javascript, and VBScript scripting and list maintenance and management features that include automated "bounce" address removal.
Of course, Sterling Medial takes necessary precautions to only contact, via e-mail, candidates who have expressed an interest in receiving such e-mails. In fact, Xxxxxx Xxxxx’s usage of e-mail is refined in order to only reach those qualified candidates who have placed their contact information on credible and confidential job-seeking sites or other legitimate job placement services. In more conceptual terms, Xxxxxx Xxxxx sees e-mail blasts as e-mail oriented marketing campaigns that serve as one-on-one communications between itself and each individual candidate.
Utilization of Internal Databases – As the result of its prior pre-recruiting efforts in support of previous healthcare, administrative, and professional initiatives, Xxxxxx Xxxxx possesses extensive in-house databases of candidates, especially those in the healthcare service delivery. Accessing these internal resources will accelerate performance under the current requirement, and enable Xxxxxx Xxxxx to deliver services within the required start-up time frame. Currently, Xxxxxx Xxxxx maintains a robust database that has the names and contact information – categorized by occupation, experience levels, and current/desired location – for qualified personnel in all 50 states and will continue to augment that list throughout the life of the instant Contract.
Through its extensive investment regarding nationwide search capabilities in all of the above general and healthcare-specific recruiting sites, Xxxxxx Xxxxx maximizes its ability to recruit qualified healthcare professionals in fulfillment of this Contract.
A.5.B XXXXXX XXXXX’S PLAN FOR CREDENTIALING
Xxxxxx Xxxxx possesses a large credentialing department, staffed with eight (8) experienced credentialers, who have successfully credentialed staff members and providers in the past in support of Xxxxxx Xxxxx's VA CBOC program nationwide. Xxxxxx Xxxxx's experienced Credentialing Department thus provides a very tangible advantage to an organization of our size and scope, and will allow the NMVAHCS to rely confidently on Xxxxxx Xxxxx's credentialing abilities. Our credentialing strategies involve both an initial screening phase and a more complete primary source verification phase.
In the initial phase, our credentialers and recruiters review the stated qualifications of candidates (from their application (SFI 0-2850), resume, etc.), and compare these to the qualifications required by the contract, and
29
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
by the VAMC’s Professional Affairs Office (in the post-award period). Our staff members make preliminary decisions regarding whether candidates are qualified to provide service.
During the initial, screening phase, online media are used to check the qualifications of candidates. This includes websites such as the American Board of Internal Medicine website and the American Medical Association “AMA” web site, both of which allow for fast and efficient preliminary review of candidates, to determine their prima facie qualification for service. These steps allow our credentialing department to quickly identify potential problems with a credentialing packet, prior to the expending large quantities of time obtaining primary source verifications, and importantly, prior to any reliance by the firm upon a candidate who will ultimately not be successful in the credentialing process. As soon as we have determined that a candidate's qualifications meet the facility’s needs, we begin the process of obtaining primary source verifications for all necessary qualifications.
Our credentialers and recruiters are extremely experiences in the use of the VET-PRO system that has been adopted by a number of VAMCs. We would certainly use this system if it were the desire of the NMVACS.
Xxxxxx Xxxxx also possesses contract arrangements with the National Practitioner Databank, allowing us to receive online practitioner profiles within a four (4) hour period. We also use the AMA web site, which, for a fee, provides the profile of member physicians along with the record of all physician credentials previously verified by the AMA. All medical staff and credentialed and privileged ancillary staff are credentialed through the VAMC, as well through Xxxxxx Xxxxx using primary source verification procedures. Source verification for credentialing includes:
The American Medical Association Physician Masterfile - for verification of a Physician’s United States and Puerto Rican medical school graduation and residency completion.
The American Board of Medical Specialties (“ABMS”) - for verification of a Physician’s board certification.
The Educational Commission for Foreign Medical Graduates (“ECFMG”) - for verification of a Physician’s graduation from a foreign medical school.
The American Osteopathic Association (“AOA”) Physician Database - for pre-doctoral education accredited by the AOA Bureau of Professional Education; postdoctoral education approved by the AOA Council on Postdoctoral Training; and Osteopathic Specialty Board Certification.
The Federation of State Medical Boards (“FSMB”) - for all actions against a Physician’s medical license.
Monthly Peer Review and Quality Control - is conducted for all medical staff. Corrective Action Plan Development - is undertaken for all new deficiencies.
Xxxxxx Xxxxx has an established mechanism that requires two checks of all credentials packets prior to submission. This helps to ensure that complete and current credentials are submitted to the VAMC:
Step 1. After primary source verification, the assigned Credentialer for each candidate file will assemble the documents into a complete credentials application packet for submission, in the format prescribed by the COTR and the VAMC’s Professional Affairs Office ("PAO"). At this time, the Credentialer performs a review of the packet contents to determine the packet's completeness, and specifically, pays careful attention to the current status of all credentials with an expiration date.
30
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
Step 2. After the Credentialer is assured that the packet is complete and current, it will be presented to the corporate administrator assigned to the project, who then makes one final review of the packet prior to submission to the COTR.
Subsequently, Xxxxxx Xxxxx will confirm, by telephone, the receipt of the credentials package by the COTR. The assigned credentialing contact will obtain any additional information that the COTR may require or request prior to forwarding to the PAO or that may be requested by the PAO after the packet has been forwarded. The credentialing contact for each applicant is the contact whose name appears on the letter accompanying each submitted packet to the COTR and is the same contact who called the COTR to confirm receipt of the application packet.
This system of assigning each credential file to a designated Credentialer streamlines the process because the COTR or PAO always knows the name of the contact. The Credentialer has the ongoing responsibility of clarifying any questions that the VAMC may pose regarding an individual credentialing file. An additional benefit of this process is the expeditious response to requests for additional information or documentation. This is possible because the Credentialer who initially spoke with the candidate during the document collection phase, and who has an established familiarity with the candidate, remains the credential’s point of contact throughout the contract period.
Xxxxxx Xxxxx has specific techniques for assessing provider candidates for potential use within the CBOC, and on the specific credentialing documents that are assessed, kept and maintained as current, in the healthcare provider's personnel file. Integral to the process of determining qualification of provider applicants, is the verification of licensure, training and certification.
Beyond verification of education and professional documentation, Xxxxxx Xxxxx obtains three (3) to five (5) Professional references for each staff physician. These references must be primarily from professional providers in the physician's own specialty with direct observational knowledge of the physician's clinical skills and competencies, including applicable surgical skills. For those physicians who have completed residency training within the preceding three (3) years, at least one (1) of these references must be from a senior staff member in the department in which the physician completed their residency training. If any of the references contacted indicate any clinical or interpersonal problem of significance with respect to the evaluated physician, the physician will not be retained by this firm.
Each physician applicant receives a personal interview with appropriate personnel designated by Xxxxxx Xxxxx. Characteristics noted in this interview are:
Fluency of language Flexibility in dealing with people of different ages, ethnicities and backgrounds Ability to accept appropriate medical and hospital administrative authority, and to comply with
prescribed hospital rules, regulations and procedures Empathetic clinical and interpersonal skills, helping to create a positive patient-clinical
Experience
In addition to credentialing forms, prospective applicants must also respond to an additional credentials history questionnaire in which physician applicants provide attestations to:
31
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
Professional training Work experience Malpractice history State medical licensures Physical and mental impairments which could limit clinical practice Current medications usage Potentially communicable diseases Hospitalizations in the last five (5) years History as a defendant in a felony or misdemeanor case Instances of state medical licensure (including DEA) revocation, suspension or denial History of denials, limitations, suspensions and/or revocations of hospital privileges by any
institution to which the physician has applied Requests for resignation of physician by a medical institution to prevent an adverse
credentialing action History of treatment or referral for treatment for alcoholism, drug abuse or psychiatric
problems
While a single alleged malpractice incident may not necessarily disqualify any evaluated physician, any significant malpractice judgment or settlement is carefully considered for indication of actual negligence on the part of the physician and may preclude contractual employment with Xxxxxx Xxxxx. Provider and attorney statements of fact concerning any such claim are obtained. All information furnished by providers concerning any malpractice claims is crosschecked against applicable National Provider Database to verify accuracy.
Before finalizing retention of any prospective provider, or the submission of any provider credentialing material to the VAMC, primary source verifications are performed regarding professional licensures/certifications possessed by the provider. Such verifications take the form of either: (1) response on original letterhead from primary issuing agency; or (2) telephone verification from primary issuing agency plus a copy of outgoing letter to primary issuing agency requesting written verification. In the case of telephone verification, the physicians file is double-checked to ensure that return response on original letterhead from issuing agency has been received within thirty days.
For each healthcare provider, copies of the following documentation is obtained from the candidate as applicable: (a) curriculum vitae; (b) medical school diploma; (c) internship certificate; (d) residency certificate; (e) fellowship certificate; (f) board certification; (g) ECFMG certification; (h) FMGEMS (Foreign Medical Graduate Examination In The Medical Sciences); (i) ACLS, BLS and NRP certification; and (j) state medical licensures held within the last ten years. All of the certificates and certifications are confirmed, under the procedures discussed above, with the appropriate accrediting or issuing institution.
In order to document and verify experience and clinical competence, a listing of all practice experience that accounts for all periods of time following graduation from medical school will be accompanied by written verifications for each position.
Since no corporate organization possesses comparable professional skills and resources for monitoring physician competency possessed by the applicable professional colleges (e.g., American Academy of Family Practice), Xxxxxx Xxxxx attempts to retain wherever possible physicians who are board-
32
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
certified in their applicable subspecialties. Such physicians possess demonstrated competency and clinical abilities, as attested to by the educational and clinical evaluations of their respective boards. In fact, more than 80% of the physicians currently retained on staff by Xxxxxx Xxxxx possess board certification in their particular fields.
Where a physician does not possess board certification, or has recently completed post-graduate training, Xxxxxx Xxxxx makes an extra effort to contact additional educational/professional references not included within the physician's designated five (5) initial references, with the goal of further assessing the physician's clinical competency and expertise.
Xxxxxx Xxxxx has a standard procedure to ensure that all licensures and certifications remain current. A designated credentials staff member at Xxxxxx Xxxxx reviews all physicians' files on a cyclical basis. The review is directed at ensuring that all required credentialing material, together with any applicable physician insurance endorsements, is actually maintained in the appropriate physician's file. The credentials staff member checks all physicians' license and certification expiration dates to determine which are scheduled for imminent expiration. Each physician receives a form letter notifying them that their license or certification is to expire. The physician's file is tagged for follow-up to determine that appropriate renewals are obtained in timely fashion. Renewal certifications are verified using the procedures discussed above.
All of Xxxxxx Xxxxx's physicians are responsible for maintaining Continuing Medical Education (“CME”) requirements in at least the minimum annual quantities necessary for maintaining state medical licensure and hospital privileging. Attendance at professional CME meetings and courses during contractually provided CME/vacation time is expected of all providers. A record of all CME obtained is included in the physician's credentialing file to satisfy required credit quantities.
A.5.C XXXXXX XXXXX’S PLAN FOR LONG-TERM RENTION OF EMPLOYEES
In order to facilitate staff retention, Xxxxxx Xxxxx has instituted a number of initiatives designed to retain employees on a long-term basis:
Written Provider Agreements. To facilitate provider retention, all full-time providers are retained under written, multi-year contracts which extend for the full duration of the underlying client contract, inclusive of all relevant option periods. Providers are required to give a minimum notice period of ninety days to terminate their contract. Through use of such multi-year contract agreements, providers are able to visualize the full term of their possible service. This facilitates provider-retention on a long-term basis. Written provider contracts are highly detailed, and clearly set forth the work to be performed, giving providers the specific requirements for their position. Long-term retention is facilitated by clearly setting forth, in advance, the requirements of each position and ensuring provider awareness of such position requirements.
Nationally Competitive Salary Structure. Provider retention is further facilitated by competitive compensation totals furnished to each provider. All compensation totals furnished to providers are verified as competitive using national and regional compensation surveys as well as extensive market research conducted by Xxxxxx Xxxxx in the provider's specialty. This ensures that compensation is adequate for both recruitment and retention.
Regular Salary Increases. In addition, providers receive regular annual increases, retroactive to each anniversary of their initial employment date with Xxxxxx Xxxxx. Annual salary increases facilitate provider
33
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.

retention, as providers are aware that they will receive such increases on a regular basis, unrelated to collection percentages or any particular form of financial performance incentives on the part of the company. Regular annual increases, based on merit factors that recognize and reward excellent performance, along with cost of living, are another element of the compensation program used for retention. Variable retention bonuses are offered at certain locations and for certain employees. These bonuses are structured to encourage retention at particular locations, such as geographically challenging locations, and for long-term employees who may require an additional bonus to facilitate their retention.
Competitive Paid Time Off Packages. Provider retention is also facilitated by the availability of adequate leave under each provider contract. At a minimum, each provider receives a minimum of ten federal holidays and three (3) weeks of vacation, totaling a full twenty-five days of leave from regular duties.
Competitive Benefits Program. Xxxxxx Xxxxx offers both provider and support staff a comprehensive and flexible benefit program that includes robust plans for health, dental, and vision coverage. These benefits are employee-funded and are made available under a Section 125 "Cafeteria-Style" plan. The benefits include: 401(k) Plans, Health Insurance, Dental Insurance, Prescription Coverage, Vision Coverage and Life Insurance. Xxxxxx Xxxxx has received pre-authorization to provide incumbent staff with health insurance without a waiting period and newly-hired staff is eligible for benefits after thirty days of employment. Additionally, the 401(k) Plan provides for 25% tax deferment, compared to the 8-11% industry average. A full delineation of our benefits package is included below:
BENEFIT TYPE
BENEFIT(S)DESCRIPTION
COMPREHENSIVE MEDICAL BENEFITS
Administered by United Medical Resources PPO, a wholly owned subsidiary of UnitedHealthcare Network, the largest healthcare network in the U.S. Features include a deductible of $500 per person ($1000 per family) with co-pays of $20 for primary care, $25 for specialty care, and $35 for urgent care. Features of our medical benefits plan include co-pays of only $20 for primary care physician visits and $25 for specialty care physician visits, both available without satisfaction of the deductible, and a deductible of $500 per person, or $1000 for a family, for health care expenses including hospitalization rather than physician visits. Also included in our Comprehensive Medical Benefits Program is a prescription card providing $10 co-pay for any generic prescription and$35 co-pay for name brand prescriptions.
DENTAL BENEFITS
Administered by United Medical Resources PPO, employees can use this plan to access any dental provider. Deductibles are $50 per person per family. Dental insurance applies to preventative, restorative and, after 12 months, reconstructive dental care. The policy covers dental care obtained from any licensed dental provider in any of the 50 states, and in overseas U.S. territories and possessions.
VISION BENEFITS
Administered by United Medical Resources PPO, employees can use this plan to access any vision provider. Notable highlights include: Vision coverage available to all HCPs working at least 20 hours per week; Vision coverage for eye examinations with any provider (no network restrictions); Reimbursed expenses for glasses with any type of lenses, and options such as solid or gradient tinting, scratch resistance coating, UV protecting coating and anti-reflective/glare coating; Reimbursed expenses for contact lenses whether elective or medically necessary, including exam, fit, follow-up care, and materials.
SUPPLEMENTAL TERM LIFE
Notable highlights include: Life Insurance coverage is available in $25,000 units from a minimum of $25,000 to a maximum of $100,000. Furthermore, our Life
34
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
INSURANCE
Coverage is unique in that a policy of $100,000 can be obtained based only on the employee’s signature, with no need for a medical examination. Employees can purchase coverage for dependents in the amount of $10,000 for spouse and $5,000 for children. One (1) premium covers all eligible dependents; The Guarantee Issue Amount, the amount of coverage that can be purchased without answering proof of good health questions, for a HCP is $100,000; a spouse is $10,000; a child is $5,000.
ACCIDENTAL DEATH AND DISMEMBERMENT
The AD&D benefit equals the employee Life Insurance amount to a maximum of $100,000; AD&D provides 24-hour coverage and a benefit in the event of loss of life, limb or eyesight as a direct result of an accident, provided the loss occurs within 365 days of the accident.
LONG AND SHORT-TERM DISABILITY
Notable highlights include: Monthly benefit levels may be selected in units of $100, from a minimum of $500 to the lesser of $5,000 or 80% of basic covered monthly pay, rounded to the next lower $100; Any amount of coverage selected is available on a Guarantee Issue basis; Benefits are not subject to federal income tax when premiums are paid with after-tax dollars; Coverage extends 24-hours a day, seven days a week, on or off the job; No qualifying period for benefits. Benefits are available immediately when the definition of disability is met. Notably, our Long-Term Disability coverage requires no medical examination for enrollment.
HEALTHCARE FLEX SPENDING ACCOUNT (“HEALTHCARE FSA”)
Under the Healthcare FSA, healthcare providers can elect to contribute up to $5,000 per year on a pre-tax basis in order to fund any eligible healthcare expense, including medical insurance co-pays, dental insurance co-pays, orthodontist expenses, vision care expenses, prescription eyewear, contact lenses, over-the-counter medications, and other eligible healthcare expenses.
DEPENDENT CARE FLEX SPENDING ACCOUNT (“DEPENDENT CARE FSA”)
Xxxxxx Xxxxx offers a Dependent Care FSA, in which HCPs can elect to contribute up to $5,000 per year on a pre-tax basis in order to fund any eligible dependent care expense, including Day Care expense, employed au pair expense, and other eligible dependent care expenses.
401(K) PLAN WITH EMPLOYER MATCH
The 401(k) plan offered, and matched up to 2% by Xxxxxx Xxxxx, is administered by Huntington National Bank, a $36 billion regional bank holding company. HCPs can make special elective salary deferrals of up to 100% of any bonuses. Notably, staff may elect a 401(k) with a choice of up to 20 mutual funds to invest their portfolios, including a wide range of domestic stocks, international stocks, domestic bonds, money market and mutual funds.
VETERINARY CARE INSURANCE
Banfield Comprehensive Pet Healthcare Plans provide owners with different levels of its Optimum Wellness Plans, which are intended to prevent illness and lengthen an animal’s life. The Plans are designed to save 50% on the routine medical needs of covered pets.
CREDIT UNION MEMBERSHIP
Xxxxxx Xxxxx employees can obtain interest-free checking and savings accounts, as well as automobile loans in most states through CINCO’s Family Financial Center.
EMPLOYEE DISCOUNT PROGRAMS
Employees match benefit from a 20% discount program for cell phone equipment and service plans with Sprint.
Employees also receive discounts for purchases made online on Overstock.com.
Employees also receive discounts on automobile rentals with Avis.
35
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.

EMPLOYER SPONSORED AUTO, RENTERS, AND HOME OWNER’S INSURANCE
Employees may choose to benefit from a discount offered on auto, renter’s, and home owner’s insurance offered by Met Life. The group discount is typically 15%. In most cases, insurance can be 100% funded through payroll deduction only, without the need for a large down payment, as is typically required under individual auto insurance policies. Superior driver discounts are available in most states for Auto Insurance.
In conclusion, staff retention is facilitated through a number of initiatives comparable to the provider initiatives including competitive and adequate compensation, regular annual increases, and competitive and adequate leave packages which typically cover ten (10) federal holidays and three (3) weeks paid time-off. Milestone awards are also offered to staff members on numerous occasions, providing plaques and cash awards commemorating service milestones with the company, including awards at five (5) year, seven (7) year, and ten (10) year anniversaries. Finally, we offer a competitive and diverse benefits package.
A.6. TRAINING AND EXPERIENCE THAT WILL BE UTILIZED TO MEET ADMINISTRATIVE SUPPORT FUNCTIONS OF THIS CONTRACT
This Section A.6 provides discussion of the training and experience that will be utilized to meet the administrative support functions of this contract. To that end, this section is divided in the following manner:
Discussion of the experience held by Xxxxxx Xxxxx’s key corporate staff as it relates to the administration of CBOC Contracts on behalf of the VA
Discussion of the training practices employed by Xxxxxx Xxxxx to ensure that all on-site personnel perform duties within the professional standards of clinical administration as established by the Joint Commission on Accreditation of Healthcare Organizations (“JCAHO”)
Accordingly, the above topical issues are delineated in-depth below.
A.6.A. XXXXXX XXXXX’S KEY CORPORATE AND CLINICAL STAFF EXPERIENCE
The following chart identifies the key personnel in Xxxxxx Xxxxx’s management structure who will contribute to the successful accomplishment of services at the proposed Taos location:
POSITION TITLE NAME PROFESSIONAL EXPERIENCE/TRAININGVA CBOC Program Project Manager
Brandon Xxxxx, Xxxxxx Xxxxx Vice President
13 years experience as CBOC Program Manager
More than 20 years experience with CBOC start-ups on behalf of the VA
VA CBOC HR Liaison
Karen Xxxxx, Xxxxxx Xxxxx Senior CBOC Human Resources Liaison
Ten (10) years experience as Senior Xxxxxx Xxxxx VA Program HR Liaison
VA CBOC Clinical Liaison
Charlene Xxxxx, Xxxxxx Xxxxx
11 years of experience as Xxxxxx Xxxxx’s CBOC Clinical Senior Administrator
36
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.

Clinical Liaison Administrator
More than 15 years experience with CBOC start-ups on behalf of the VA
VA CBOC Physician Consultants
Barry Kaler, DODonald Courts, MDEthan Loeb, MD
9 years of experience with Xxxxxx Xxxxx’s CBOC Program (combined)
More than 5 years experience with CBOC start-ups on behalf of the VA
Facilities Director Tim Fordyce, Xxxxxx Xxxxx Director of Construction
10 years of experience with Xxxxxx Xxxxx’s CBOC Program
More than 10 years experience with CBOC start-ups on behalf of the VA
Physician Arthur William Lynch III, MD
20 years of experience
Locum Physician Gerson Bergeisen, MD 24 years of experienceLocum Physician Delores Endres, MD 31 years of experienceNurse Practitioner Carolyn Holloway-Ball,
FNP 25 years of experience
Licensed Independent Social Worker
Valerie Pierce 20 years of experience
Clinic Manager Carrie Venezia 18 years of experience Registered Nurse – Infection Control & Triage
William Jay Salls 32 years of experience
Licensed Practical Nurse
Daniel Clothier 15 years of experience
Phlebotomist Merah Hill 3 years of experience Medical Assistant Cindy Herrera 13 years of experience Medical Clerk Roberta Scott 15 years of experience
Additionally, Xxxxxx Xxxxx’s ability to fully administer all elements of contractual performance is aided by extremely experienced corporate departments. Delineation of Xxxxxx Xxxxx’s corporate departments is included below.
Xxxxxx Xxxxx’s Physician Recruitment Department - Xxxxxx Xxxxx’s Physician Recruitment Department includes experienced Physician Recruiters who specialize in recruiting and placing well qualified physicians in professional positions on behalf of Government agencies. Xxxxxx Xxxxx’s Physician Recruiters place physicians at VA Army, Air Force and Navy healthcare facilities.
Xxxxxx Xxxxx’s Physician Recruiters possess extensive experience in recruiting a wide range of physician specialists, including Neurosurgeons, Radiologists, Family Practice Physicians, Internal Medicine Physicians, Pediatricians, OB/GYN Physicians, General Surgeons, Urologists, Neurologists, and Psychiatrists.
Xxxxxx Xxxxx’s Physician Recruitment Department possesses ten (10) full-time physician recruiters.
Xxxxxx Xxxxx’s Staff Recruitment Department - Xxxxxx Xxxxx’s Staff Recruitment Department consists of experienced professional Staff Recruiters who exclusively recruit and place professional
37
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
healthcare staff members, exclusive of physicians, at professional positions on behalf of Government agencies. Our experienced Staff Recruiters place the full range of professional healthcare staff at VA Army, Air Force and Navy healthcare facilities.
Xxxxxx Xxxxx’s Staff Recruiters possess current experience in recruiting for a wide range of professional healthcare specialties. Our Staff Recruitment Department currently recruits and places the following professional mid-level providers: Pharmacists, Optometrists, Chiropractors, Family Nurse Practitioners, Pediatric Nurse Practitioners, OB/GYN Nurse Practitioners, Speech Language Pathologists, Physical Therapists, Occupational Therapists, Clinical Psychologist, Child and Adolescent Psychologist, Licensed Clinical Social Workers, Physician Assistant, and Medical Supply Technician.
Among the various professional healthcare specialties, Xxxxxx Xxxxx’s Staff Recruitment Department currently recruits the following full range of nursing specialists: RN Case Managers, Med-Surg RNs, ICU RNs, Emergency Room RNs, Labor and Delivery RNs, Family Practice Clinic RNs, Pediatrics Clinic RNs, and Licensed Practical Nurses.
Additionally, our Staff Recruitment Department currently recruits the following ancillary healthcare specialties: Medical Laboratory Technicians, Audiology Technicians, Medical Assistants, Certified Nursing Assistants, Medical Records Clerks, Phlebotomists, Audiologists, Pharmacy Technicians, Radiology Technicians, Laboratory Technicians, Bio Medical Equipment Technologists, and Behavioral Health Technicians.
Xxxxxx Xxxxx currently possesses eleven (11) full-time recruiters in its Staff Recruitment Department. These individuals are highly trained and experienced in recruiting and placing the full range of professional healthcare staff members, as indicated above. They possess extensive skills in Internet recruiting, telephonic recruiting, recruiting through personal presentations, and recruiting through attendance at professional job fairs. They are also highly experienced in negotiating with, and where necessary relocating, professional healthcare staff to fulfill opportunities in other states and other nations.
Xxxxxx Xxxxx’s Credentialing Department - Over the past 30 years, all of our Credentialers have provided complete credentials information on behalf of services provided by Xxxxxx Xxxxx at almost every military healthcare facility in the United States, over 20 CBOC facilities, and 13 OCONUS nations, including: the United Kingdom, Germany, Iceland, Italy, Japan, Portugal, South Korea, Spain, Netherlands, Belgium, Turkey, and Canada.
Xxxxxx Xxxxx’s Credentialing Department is responsible for obtaining primary source verification of all potential candidates and is organized to conduct appropriate verifications of credentials prior to candidate submission. Xxxxxx Xxxxx’s Credentialing Department is organized to verify all professional licensures, board certifications, professional residencies, professional degrees, and all periods of post graduate employment. Xxxxxx Xxxxx’s Credentialing Department is organized to obtain all such verifications based on original sources verification, (i.e. verification of licensures, certifications, residencies, professional education, and professional employment with the issuing institution or employer, as applicable).
By ensuring that all Xxxxxx Xxxxx staff posses the education, certification, and employment history that they have claimed, Xxxxxx Xxxxx’s Credentialing Department can guarantee the Government, on a national and international basis, that all its employees posses the education, certification, and employment history necessary for high quality healthcare and administrative service provision.
38
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.

Xxxxxx Xxxxx’s Credentialers are also highly skilled in obtaining professional references, both initial telephonic references, and final professional references, for inclusion in the applicant’s credentials application.
Xxxxxx Xxxxx’s Human Resources Department - Xxxxxx Xxxxx’s Human Resources Department is a corporate department located at the company’s headquarters in Cincinnati, Ohio. Xxxxxx Xxxxx’s Human Resources Department has 30 years of experience working within the healthcare realm, including with VA and DoD clients. The Human Resources Department oversees both the Payroll and Benefits Departments, ensures that Xxxxxx Xxxxx’s Employee Handbook is comprehensive and accurate, and distributed to all employees and provides approval of written counseling actions, performance improvement plans (“PIPs”), written policy changes and policy distributions, approval of staff promotions, and, where necessary, staff termination actions.
Xxxxxx Xxxxx’s Human Resources Department also oversees corporate level problem resolution procedures up to and including, but not limited to, referred counseling for employees, enforcement of Xxxxxx Xxxxx’s Drug-Free Workplace Policy and Policies Against Harassment, and corporate disciplinary action. The Human Resources Department also ensures that annual reviews are accomplished, that all substantive reviews are complete, and that overall company standards are met with respect to human resources actions.
Xxxxxx Xxxxx’s Human Recourses Department works in cooperation with Xxxxxx Xxxxx’s Physician and Staff Management departments in ensuring that all counseling, policy, promotions, and termination actions are effectively accomplished in accordance with Xxxxxx Xxxxx’s policies and procedures, as well as in accordance with federal and state law.
Xxxxxx Xxxxx’s Benefits Department - Xxxxxx Xxxxx’s Benefits Department is organized to deliver high quality employee benefits to Xxxxxx Xxxxx’s healthcare providers in the United States and abroad. Xxxxxx Xxxxx’s Benefits Department has 30 years of experience working with VA and DoD clients within the healthcare realm.
Xxxxxx Xxxxx’s Benefits Department offers and delivers the following benefits on behalf of healthcare professionals furnishing service to military and Veterans Administration facilities in the United States: healthcare insurance, prescription card, dental insurance, vision insurance, supplemental life insurance, long-term disability insurance, flexible healthcare spending accounts, flexible dependent care spending accounts, and 401(k) with employer match.
For its overseas direct healthcare providers, Xxxxxx Xxxxx’s Benefits Department is organized to offer the following benefits: healthcare insurance, prescription card, dental insurance, vision insurance, life insurance, long-term disability insurance, and 401(k) with employer match.
Xxxxxx Xxxxx’s Payroll Department - Xxxxxx Xxxxx’s Payroll Department is organized to provide highly effective payroll support for Xxxxxx Xxxxx’s healthcare staffing efforts in the United States and in 13 OCONUS nations. Xxxxxx Xxxxx’s Payroll Department is comprised of five (5) fulltime payroll specialists skilled in the calculation an accurate delivery of payroll to over 2000 employees.
39
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.

Xxxxxx Xxxxx’s Payroll Department is organized to deliver payroll via direct deposit and/or overnight courier if requested by the employee, throughout the United States and in the following 12 OCONUS nations: the United Kingdom, Germany, Iceland, Italy, Japan, Portugal, South Korea, Spain, Netherlands, Belgium, Turkey, and Canada. Xxxxxx Xxxxx’s Payroll Department will also offer direct deposit to all Contract employees. Those opting out will receive payroll though overnight courier service.
Xxxxxx Xxxxx’s Payroll Department utilizes the Paycor Payroll System, which provides downloadable hours by contract/task order/CLIN numbers. The information generated by the payroll system is downloaded into Excel spreadsheets for utilization by Xxxxxx Xxxxx’s Accounts Receivable Department. By these means, totals generated by the payroll system are integrated with, and actually checked against, independent totals generated by Xxxxxx Xxxxx’s Accounts Receivable Department. Notably, Xxxxxx Xxxxx’s Accounts Receivable Department receives a copy of all timesheets, approved by the Government supervisor, and forwarded to the Xxxxxx Xxxxx Payroll Department.
Notably, Xxxxxx Xxxxx’s accounting system has been approved by the Defense Contract Audit Agency (“DCAA”) as an acceptable accounting system to track accumulation of contract costs for Government contract purposes. Xxxxxx Xxxxx currently posses a DCAA approval letter for the said accounting system on file.
Payroll is successfully delivered not only in US Dollars, but also in Pounds Sterling, Euros, Yen, and Canadian Dollars.
Xxxxxx Xxxxx’s Payroll Department has successfully delivered accurate payrolls to healthcare professionals at military facilities for the past 30 years.
Xxxxxx Xxxxx’s Finance Department. Xxxxxx Xxxxx’s Finance Department has been at the forefront of the company, managing all financial and audit compliance aspects of the corporation. Since 1998, Xxxxxx Xxxxx has increased its revenue from $13 million to $100 million, with projected sales of over $140 million for 200. During this time period, Xxxxxx Xxxxx has proven itself financially responsible to handle the tremendous growth.
Xxxxxx Xxxxx’s Finance Department has built a proven infrastructure to handle the addition of new contract awards. Xxxxxx Xxxxx currently has numerous contracts with the Department of Defense and the Department of Veterans Affairs in excess of $96 million. Xxxxxx Xxxxx has an extensive number of FTEs staffing military bases in over 42 States and in 13 Foreign Countries. Payrolls are biweekly and monthly which are processed by Paycor, a large regional payroll processing company.
Xxxxxx Xxxxx’s Finance Department has undergone and passed seven (7) DCAA audits of contracts incurred cost proposals, as well as four (4) DCAA pre-award contract audits. Recently, a financial responsibility audit was conducted with DCAA for an Army OCONUS Multiple Award Task Order (“MATO”), qualifying Xxxxxx Xxxxx and its teaming partner for potential award. Also Xxxxxx Xxxxx has been audited by the Internal Revenue Service, other State agencies, and overseas tax audits in countries such as Germany, all of which resulted in zero (0) audit adjustments.
Xxxxxx Xxxxx’s Finance Department is supported by a network of financial institutions that are willing to support Xxxxxx Xxxxx’s continued growth.
40
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
Xxxxxx Xxxxx’s Accounts Receivable Department - Xxxxxx Xxxxx’s Accounts Receivable Department is organized to deliver high quality, timely and accurate billings, for all services rendered under its client contracts, both in the United States and abroad.
Xxxxxx Xxxxx’s Accounts Receivable Department possesses six (6) fulltime accounts receivable billers. These individuals are exclusively devoted to providing timely and accurate invoices for direct healthcare services at military and VA facilities.
The Accounts Receivable Department delivers all invoices within ten (10) days after the close of each month in which services are provided. This allows adequate time for staff members furnishing service at Government facilities to provide their timesheets after the close of each month, and for Xxxxxx Xxxxx to obtain the supervisor’s signature verifying the accuracy of employee reported hours prior to timesheet submission.
Additionally, this timeframe allows for members of Xxxxxx Xxxxx’s Accounts Receivable Department to receive and check the aforementioned timesheets, for members of Xxxxxx Xxxxx’s Accounts Receivable Department to enter employee data into a calculation spreadsheet established (and Government approved) for each account, and for these calculations to be subsequently checked for accuracy. In 2008, approximately 92% of all invoices were delivered within seven calendar days after the close of each month in which services were provided. Over 99% of all invoices in 2008 were delivered within ten calendar days after the close of each month in which services were provided.
Xxxxxx Xxxxx’s Accounts Receivable Department is highly proficient in the use of the Wide Area Work Flow (“WAWF”) system. Following the aforementioned processes, all pertinent data is entered into WAWF. If WAWF is not made available by the client for a particular service, the information is then sent in the form of hard copy invoice, with appropriate supporting documentation, by overnight courier on or before the deadline date. Xxxxxx Xxxxx’s Accounts Receivable Department is highly experienced in the use of WAWF for invoicing healthcare services; in 2008, Xxxxxx Xxxxx’s Accounts Receivable Department delivered over 5,000 invoices through the WAWF system.
In addition to establishing a deadline for each account, the Xxxxxx Xxxxx’s Accounts Receivable Department Manager also establishes a target date for submission of all pertinent invoices for each account. The target date is typically the day two (2) days prior to deadline dates or three (3) business days following the close of each month. In cases where too many submission dates overlap, a slight adjustment may be made, with the approval of the Government, for a particular account.
All services to be invoiced, target dates, and deadline dates are furnished to the entire Xxxxxx Xxxxx Accounts Receivable Department by the Accounts Receivable Manager each month, approximately two (2) weeks prior to commencement of each month. Each month’s schedule is established, taking into account the way in which weekdays and holidays fall at the end of each month and the beginning of each month.
Xxxxxx Xxxxx’s Accounts Receivable Department has successfully delivered accurate invoices to healthcare professionals at military facilities for the past 28 years.
A.6.B. XXXXXX XXXXX’S TRAINING PRACTICES
41
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.

In addition to the extensive experience of Xxxxxx Xxxxx as an organization, the extensive experience of key personnel overseeing contract administration, and the extensive experience of Xxxxxx Xxxxx’s on-site healthcare staff, we also find it of paramount importance to furnish regular training to our employees to ensure complete adherence to all established JCAHO standards.
With regard to performing all work within the professional standards of clinical administration as established by the Joint Commission, Xxxxxx Xxxxx fully understands the importance of ensuring that all of its staff personnel are adequately and competently trained in accordance with all JCAHO standards. Such training, administered by Xxxxxx Xxxxx, allows for a safe, stable clinical environment wherein all Government beneficiaries receive the highest quality of service.
To that end, Xxxxxx Xxxxx requires that all Supplemental Nurse staff personnel are administered yearly training on topics related to compliance with all standards set forth by the JCAHO. This training is delivered via provider firm Medcom. Under an exclusive agreement with Medcom-Trainex, (“Medcom”), an educational service provider accredited by eight (8) national organizations, all staff providers will be provided with unlimited access to continuing education opportunities. Medcom has partnered with employers as well as organizations such as Joint Commission and the Veterans Administration to create and sustain staff development programs that promote lifelong learning and continued competence. Medcom provides high-quality, must-have education, training and clinical specialty information to healthcare professionals and support staff utilizing principles of adult learning through a variety of Web-based, video, print and CD-ROM learning technologies.
Through needs-based curriculum development, Medcom provides clients with the most up-to-date information related to regulatory requirements, clinical issues and advances, evidence-based practice findings, leadership management research breakthroughs, annual competencies, staff development, industry-specific news and more. A single-source provider, Medcom deftly couples its expert content with the software services and delivery systems necessary to construct a customized training environment, regardless of underlying technology platforms, workforce distribution or media presentation preferences. Clients can either draw coursework from Medcom's ever-expanding multimedia training library, or work with Medcom to create "custom libraries," tailored to fit the exact needs of their training environment. Such customized integration of the training components consistently yields the desired result for the client.
Specific JCAHO standards training curriculums, on a position-by-position basis, are delineated below:
LABOR CATEGORY
REQUIRED JCAHO TRAINING COURSES
MEDICAL DIRECTOR
The 2009-2010 National Patient Safety Goals; Strategic Surveillance System (S3): Using Data to Improve Patient Care; Emergency Preparedness – Collaboration, Communication, and Communication; Technological Solutions to Patient Safety; Hand-Off Communication; Steps to Success; Medication Reconciliation; Finding Solutions Through Process Mapping; Infection Control; Prevention Through Good Practice; Designing and Maintaining a Safe Environment of Care; Vital Signs; Rapid Response to Patient Condition Changes; The Joint Commission’s Standards of Improvement Initiative; Accreditation Process Update; Using Tracers to Achieve Results
PHYSICIAN STAFF The 2009-2010 National Patient Safety Goals; Strategic Surveillance System (S3): Using Data to Improve Patient Care; Emergency Preparedness – Collaboration, Communication, and Communication; Technological Solutions to
42
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
Patient Safety; Hand-Off Communication; Steps to Success; Medication Reconciliation; Finding Solutions Through Process Mapping; Infection Control; Prevention Through Good Practice; Designing and Maintaining a Safe Environment of Care; Vital Signs; Rapid Response to Patient Condition Changes; The Joint Commission’s Standards of Improvement Initiative; Accreditation Process Update; Using Tracers to Achieve Results
NURSE PRACTITIONER STAFF
The 2009-2010 National Patient Safety Goals; Strategic Surveillance System (S3): Using Data to Improve Patient Care; Emergency Preparedness – Collaboration, Communication, and Communication; Technological Solutions to Patient Safety; Hand-Off Communication; Steps to Success; Medication Reconciliation; Finding Solutions Through Process Mapping; Infection Control; Prevention Through Good Practice; Designing and Maintaining a Safe Environment of Care; Vital Signs; Rapid Response to Patient Condition Changes; The Joint Commission’s Standards of Improvement Initiative; Accreditation Process Update; Using Tracers to Achieve Results
MENTAL HEALTH STAFF
The 2009-2010 National Patient Safety Goals; Strategic Surveillance System (S3): Using Data to Improve Patient Care; Emergency Preparedness – Collaboration, Communication, and Communication; Technological Solutions to Patient Safety; Hand-Off Communication; Steps to Success; Medication Reconciliation; Finding Solutions Through Process Mapping; Infection Control; Prevention Through Good Practice; Designing and Maintaining a Safe Environment of Care; Vital Signs; Rapid Response to Patient Condition Changes; The Joint Commission’s Standards of Improvement Initiative; Accreditation Process Update; Using Tracers to Achieve Results
SITE MANAGER The 2009-2010 National Patient Safety Goals; Strategic Surveillance System (S3): Using Data to Improve Patient Care; Emergency Preparedness – Collaboration, Communication, and Communication; Technological Solutions to Patient Safety; Hand-Off Communication; Steps to Success; Medication Reconciliation; Finding Solutions Through Process Mapping; Infection Control; Prevention Through Good Practice; Designing and Maintaining a Safe Environment of Care; Vital Signs; Rapid Response to Patient Condition Changes; The Joint Commission’s Standards of Improvement Initiative; Accreditation Process Update; Using Tracers to Achieve Results
RN NURSE STAFF The 2009-2010 National Patient Safety Goals; Strategic Surveillance System (S3): Using Data to Improve Patient Care; Emergency Preparedness – Collaboration, Communication, and Communication; Technological Solutions to Patient Safety; Hand-Off Communication; Steps to Success; Medication Reconciliation; Finding Solutions Through Process Mapping; Infection Control; Prevention Through Good Practice; Designing and Maintaining a Safe Environment of Care; Vital Signs; Rapid Response to Patient Condition Changes
LPN NURSE STAFF The 2009-2010 National Patient Safety Goals; Strategic Surveillance System (S3): Using Data to Improve Patient Care; Emergency Preparedness – Collaboration, Communication, and Communication; Technological Solutions to Patient Safety; Hand-Off Communication; Steps to Success; Medication Reconciliation; Finding Solutions Through Process Mapping; Infection Control; Prevention Through Good Practice; Designing and Maintaining a Safe Environment of Care; Vital Signs; Rapid Response to Patient Condition Changes
MEDICAL ASSISTANT STAFF
The 2009-2010 National Patient Safety Goals; Strategic Surveillance System (S3): Using Data to Improve Patient Care; Emergency Preparedness – Collaboration, Communication, and Communication; Technological Solutions to Patient Safety; Hand-Off Communication; Steps to Success; Medication
43
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
Reconciliation; Finding Solutions Through Process Mapping; Infection Control; Prevention Through Good Practice; Designing and Maintaining a Safe Environment of Care; Vital Signs; Rapid Response to Patient Condition Changes
TECHNICIAN STAFF The 2009-2010 National Patient Safety Goals; Emergency Preparedness – Collaboration, Communication, and Communication; Infection Control; Prevention Through Good Practice; Designing and Maintaining a Safe Environment of Care; Rapid Response to Patient Condition Changes
Upon completion of each individual JCAHO training course, Medcom will deliver, to Xxxxxx Xxxxx, documentation demonstrating completion of the course. This information will be placed in each supplemental nurse staff employee’s employment file. Under the instant effort, Xxxxxx Xxxxx will incorporate such training on an as-needed basis. We will work closely with the VA in order to identify any areas wherein additional training could be beneficial to the overall effort. Reporting of all completed training courses will be facilitated via Medcom. Upon successful completion of any Medcom course, a certificate of completion, inclusive of all appropriate test scores, is delivered to the Program Manager and Xxxxxx Xxxxx’s corporate credentialing Department. These files will be placed in each employee’s permanent employment file.
A.7. ORGANIZATION STRUCTURE AND MANAGEMENT PRACTICES
As an experienced provider of an array of health care services worldwide, Xxxxxx Xxxxx exhibits a corporate structure that allows it to efficiently manage and implement policies and procedures in all of its Contracts. The chart below shows the corporate level organizational structure for its VA CBOC services.
Xxxxxx Xxxxx's organizational structure is comprised of experienced and professional corporate personnel in the areas of recruitment, credentialing, long term staff retention, corporate level recruiters, experienced contract and service administrators, a well-qualified Project Manager, and capable on-site management personnel. This strong organizational structure allows for responsive service provision a factor which, subsequently, ensures long term provider staff retention of staff at the provider level. Our CBOC-group specific organizational structure is depicted below:
44
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
Xxxxxx Xxxxx believes a key component of our ability to provide effective CBOC services in Taos, New Mexico lies in our past experience in the administration of such services. The company has provided primary care services to federal agencies - including the VA, the Air Force, the Navy, and the Army - for 30 years. More than 80 well qualified corporate personnel provide services in the areas of recruitment, credentialing, contract administration, payroll, and accounts receivable.
Xxxxxx Xxxxx is extremely cognizant of all local conditions and has experienced and versatile on-site management staff in place. This staff, headed by the Clinic Coordinator, has the unique knowledge of the local veteran community necessary to flexibly meet the needs of all local VA beneficiaries.
The goal of the Xxxxxx Xxxxx's Team Approach is that the clinical management staff charged with responsibility for certain facets of the Xxxxxx Xxxxx's CBOC service provision, including disposition and results in individual performance areas identified by both the Xxxxxx Xxxxx's corporate management team and administrators within the VA, will be available to ensure that desired results and milestones are achieved.
Xxxxxx Xxxxx’s corporate-wide methodology for determining span of control is based around the following factors:
Geographical Location: If service branches are widely dispersed, then the manager will find it difficult to supervise each of them, as such the span on control will be smaller.
Capability of Workers: If workers are highly capable, and do not require much supervision and can be left on their own.
Similarity of Task: If the task that subordinates are performing is similar, then the span of control can be wider, as the manager can supervise them all at the same time.
45
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.

Employing the above considerations, Xxxxxx Xxxxx’s seeks to maintain an optimal span of control ration of approximately one (1) manager to four (4) subordinates on both a corporate and clinical level. In certain cases - when geography, capability, and task similarity deem slightly larger spans of control feasible – Xxxxxx Xxxxx will employ slightly higher span of control rations (e.g. 1:5; 1:6: 1:7). Span of control will be, at all times, limited to a ratio of 1:7 (manager to subordinate).
Xxxxxx Xxxxx will utilize the following organizational management positions to ensure responsive administration of the instant effort to furnish CBOC Services on behalf of the local Veteran population:
POSITION TITLE PERFORMANCE TASKS
VA CBOC PROGRAM PROJECT MANAGER
Provides executive oversight of entire CBOC Contract initiative. Xxxxxx Xxxxx's authorized officer for contract negotiations. Conducts daily meetings with VA CBOC Hospital Liaison and recruitment staff, throughout contract term, to discuss contract performance. Provides management and executive direction to all Program personnel during clinic start-up phase.
VA CBOC HR LIAISON Provides supervision and coordination of Human Resource and Provider Relations function. Performs ongoing assessment of Provider Satisfaction.
VA CBOC HOSPITAL LIAISON
Responsible within the organization for ensuring smooth operations of VA CBOC locations. Meets on a routine basis with Hospital COTR's and local clinic managers to ensure smooth operation of CBOC locations. Provides substantial feedback to Vice President in making final hiring decisions with regard to clinic primary care providers. Provides supervision over all providers recruiting.
VA CBOC CLINICAL LIAISON
Supports the VA CBOC Hospital Liaison/Clinic Coordinator. Additionally, meets with Hospital COTR's and local clinic managers to ensure smooth operation of CBOC locations as needed. Supports VA CBOC Hospital Liaison/Clinic Coordinator by implementing procedural changes of all CBOC On-Site Managers and clinical staff. Provides supervision over hiring clinical support staff and supervision in all credentialing and access activities.
FACILITIES DIRECTORResponsible for the coordination of any necessary build-out or clinic facility reconfiguration necessary for the selected clinic location to be utilized to serve veteran beneficiaries.
DIRECTOR OF TELECOMMUNICATIONS
Responsible for installation, configuration, and maintenance of all computers, software, and networking necessary for ongoing communications between CBOC location and VA Hospital client.
ON-SITE CLINIC MANAGER
Provides day to day management and coordination of clinic services. Provides first line supervision of on-site administrative personnel. Cross trained in all administrative tasks within the clinic. Gathers necessary performance improvement data.
XXXXXX XXXXX CBOC PROGRAM MEDICAL DIRECTOR
Provides professional direction to Xxxxxx Xxxxx providers within Xxxxxx Xxxxx VA CBOC Program. Provides input within hiring and job action processes for retained Xxxxxx Xxxxx CHOC providers. Provides input on clinical initiatives and improvement plans throughout the program.
QA/JCAHO PREPAREDNESS COORDINATOR
Coordinates activities of ongoing quality assurance initiatives at the clinic. Implements safety and other plans required for JCAHO compliance. Supervises clinic personnel readiness program for JCAHO monitoring of clinic activities.
46
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
CLINIC PRIMARY CARE PROVIDER
Responsible for daily provision of primary care to enrolled veteran beneficiaries. Is largely freed from any administrative burden due to the large number of administrative support staff and program management members.
PATIENT CARE ADVOCATE Assists patients with complaints, enrollment issues and other customer service issues.
A.8. MECHANISM TO SCHEDULE QUALIFIED VA CREDENTIALED PHYSICIANS AND STAFF TO COVER THE REQUIRED CLINIC SCHEDULE
Highly qualified provider staff will be used to fulfill the requirements of this Contract. Full-time providers and staff necessary for complete contract performance are already recruited, as indicated in the previous sections.
A number of key protocols will be followed in order to achieve optimum scheduling of qualified physicians and staff and to cover the required clinic schedule in accordance with all terms of the solicitation. These protocols are as follows:
Sufficient Numbers of Qualified Providers : A sufficient number of qualified providers have been recruited and retained to furnish complete coverage at the clinic. Primary care providers will be retained as full-time staff members without other professional duties that would conflict with their duties at the clinic.
Sufficient Numbers of Qualified Support Staff : A sufficient numbers of qualified support staff members have been recruited and retained in order to support provider staff. Support staff members will be retained as full-time staff members without other work-related duties that would conflict with their duties at the clinic.
Established Clinic Schedule : A clinic schedule will be established that provides for continuing provider coverage during all hours of clinic operation. This will include a "staggered lunch" procedure that schedules clinic providers for lunch at different hours, in order to provide continuous coverage at the clinic during all hours of clinic operation. Support staff will be scheduled for lunch at the same time as their supported provider. This procedure ensures the clinic has adequate support staff for all providers throughout the clinic's hours of operation.
Administrative Breaks : In addition to the scheduled time for clinic appointments, adequate administrative breaks will be established in each provider's schedule to allow for dictating patient records and completing professional administrative tasks.
Provider and Staff Schedules : Provider and staff schedules will be issued by the clinic manager. All clinic schedules will specify the providers and staff scheduled each day and the scheduled lunch breaks and administrative breaks for both providers and staff. All clinic schedules will be issued at least 15 days in advance of the calendar month for which the schedule applies. The clinic manager will be responsible for issuing and distributing the clinic calendar to all providers and staff. Prior to distribution, the clinic manager will verify the availability of all specified providers and staff. A copy of the monthly clinic schedule will be provided to the Xxxxxx Xxxxx's Program Office, Transcription Department, and Lead Locum Recruiter.
47
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
This ensures that all organizational components which require knowledge of the physician and staff schedules will be aware of the upcoming clinic schedule in a timely fashion.
Corporate Oversight: A copy of the monthly Clinic schedule will be provided to the Xxxxxx Xxxxx’s Program Operations Department, and provider and Support Staff Recruiting Department. This ensures that all organizational components that require knowledge of the Physician and Support Staff schedules will be aware of the upcoming Clinic schedule in a timely fashion.
A.8.A. CONTINGENCY PLAN FOR COVERING ENROLLED PATIENTS AND APPOINTMENTS DUE TO SCHEDULED OR UNSCHEDULED LEAVE
Pre-recruited and pre-credentialed providers will be used to provide backup coverage when the regular providers are absent, including periods of scheduled and unscheduled leave. In the event of scheduled or unscheduled leave, the following plan will be initiated:
1. Pre-recruited and pre-credentialed providers will be utilized to provide backup coverage for relevant periods of provider absence, including periods of scheduled and unscheduled leave. Xxxxxx Xxxxx will also propose backup/replacement physicians. Throughout the performance period of this Contract, Xxxxxx Xxxxx will ensure that locum tenens staff members are fully credentialed and available to provide backup staffing at the CBOC facility for all periods of scheduled and unscheduled leave.
2. For all periods of scheduled leave by providers, providers under their employment agreements will be required to furnish at least 60 days notice of such scheduled leave periods to the Xxxxxx Xxxxx. The requirement for this extended notice period, included in each written employment agreement, will greatly facilitate the scheduling of locum tenens for periods of scheduled leave. All leave requests by providers will be made to the Clinic Manager. The Clinic Manager, in turn, will furnish requests for leave to the Lead Recruiter for the clinics. The Lead Recruiter, in turn, will schedule one of the pre-recruited and pre-credentialed backup providers for coverage of the scheduled leave period.
3. Once backup providers have been scheduled and confirmed for periods of necessary coverage by the Lead Recruiter, notice of all such backup assignments will be provided to the Clinic Manager for inclusion of the upcoming clinic schedule the upcoming month. Coverage periods will then be included in the clinic schedule, to be disseminated by the Clinic Manager to all relevant parties utilizing the procedures discussed in the previous section.
4. For periods of unscheduled provider absence, all providers will be required, under their written employment agreements, to notify the Clinic Manager as soon as possible of any unscheduled absences. The Clinic Manager, in turn, will notify the Lead Recruiter of any unscheduled provider absences, so that coverage can be arranged utilizing pre-recruited, pre-credentialed providers available to furnish coverage at the clinic. Once coverage has been confirmed for any period of unscheduled provider absence, the Lead Recruiter will notify the Clinic Manager, as soon as possible, by telephone and e-mail, so that the clinic schedule can be adjusted accordingly.
5. Similarly, for staff absences, a pre-recruited, pre-credentialed staff member will be retained for necessary coverage. At least two (2) such backup staff members will be identified and retained.
48
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
6. For scheduled absences, staff members will be required to provide advance notice of such absences at a minimum of 30 days of the calendar month in which they intend to take scheduled leave. For unscheduled leave, staff members are required to provide notice as soon as possible, concerning their unscheduled leave and its circumstances.
7. All staff member notification concerning scheduled and unscheduled leave will be furnished to the Clinic Manager at each location as soon as feasibly possible. Upon receipt of notification of scheduled or unscheduled leave by staff members, the Clinic Manager will be responsible for scheduling backup staff members for coverage, so that uninterrupted operation of the clinics is maintained and continuity of care is ensured.
8. Throughout the performance of this Contract, Xxxxxx Xxxxx will ensure that backup, locum tenens staff members are fully credentialed and available to provide backup staffing at the CBOC facility in Taos, for all periods of scheduled and unscheduled leave.
9. Under their employment agreements, providers will be required to furnish at least 60 days notice to Xxxxxx Xxxxx for scheduled leave. The requirement for this extended notice will greatly facilitate the scheduling of locum tenens for periods of scheduled leave. All leave requests by providers will be made to the Clinic Manager. The Clinic Manager, in turn, will furnish requests for leave to the Lead Recruiter for the clinic. The Lead Recruiter, in turn, will schedule one of the pre-recruited and pre-credentialed backup providers for coverage during the scheduled leave.
10. Once backup providers have been scheduled and confirmed for periods of necessary coverage by the Lead Recruiter, notice of all such backup assignments will be provided to the Clinic Manager for inclusion of the clinic schedule for the upcoming month. Coverage periods will then be included in the clinic schedule, to be disseminated by the Clinic Manager to all relevant parties utilizing the procedures discussed in the previous section.
11. Under their written employment agreements, all providers will be required to notify the Clinic Manager as soon as possible of any unscheduled absences. The Clinic Manager, in turn, will notify the Lead Recruiter of any unscheduled provider absences, so that coverage can be arranged using the pre-recruited, and pre-credentialed providers
12. Once coverage has been confirmed for an unscheduled provider absence, the Lead Recruiter will notify the Clinic Manager, as soon as possible, by telephone and e-mail, so that the clinic schedule can be adjusted.
13. A similar process will be used to cover staff absences. A pre-recruited, pre-credentialed staff member will be retained for necessary coverage. At least two (2) backup staff members will be identified and retained to cover both scheduled and unscheduled absences.
14. Staff members will be required to provide advance notice of scheduled absences at a minimum of 30 days of the calendar month in which they intend to take scheduled leave. Staff members will be required to provide notice as soon as possible for each unscheduled absence along with circumstances of the unscheduled absence. All staff member notification for scheduled and unscheduled leave will be furnished to the Clinic Manager as soon as feasibly possible.
49
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.

15. When notified of either a scheduled or unscheduled leave, the Clinic Manager will be responsible for scheduling backup staff members for coverage, thus ensuring uninterrupted operation of the clinic and continuity of care.
16. Backup staff members will consist of LPNs and medical assistants cross-trained so that they can perform administrative duties in support of medical reception and medical records.
A.9. CAPABILITY TO RECRUIT ADEQUATE STAFFING
Xxxxxx Xxxxx is fully capable of recruiting adequate staffing to meet the needs of this contract. The Xxxxxx Xxxxx recruitment team, overseen by the lead provider recruiter, possess over 20 years of combined experience. Their successful delivery of provider start-ups and continuity for over 15 CBOC locations ensure beyond adequate staffing for the Taos, NM CBOC. The aforementioned pre-recruited and pre-credentialed providers are utilized as immediate backup coverage for staffing shortfalls. We continue to recruit qualified personnel after start-up, preparing to expand services, as needed, and to maintain the VA Scheduling guidelines.
To that end, Xxxxxx Xxxxx will utilize the following recruitment techniques and methodological tools in order to ensure adequate staffing throughout the life of the Contract:
Large scale direct mail campaigns to qualified licensed providers Targeted nationwide telemarketing Classified ad campaigns in regional news media Extensive professional journal advertisements Extensive Internet searches for qualified candidates Utilization of E-mail blasts Utilization of Xxxxxx Xxxxx's existing internal database of qualified professional counselor
candidates A.10. OPERATIONAL PLAN TO INCLUDE STAFFING FOR THE FIRST 90 DAYS OF CLINIC OPERATION
To provide the full range of services in a timely manner as required in the Solicitation, Xxxxxx Xxxxx presents the following start up plan for the Taos, NM Clinic.
Xxxxxx Xxxxx has proven success in meeting critical deadlines for start-up of CBOC services. In as few as 45 days (though a 60-90 day start-up is preferred due in part to VA credentialing timelines), we are able to fully staff a range of healthcare positions, plan and manage the construction/remodel of the facility, purchase and install clinical equipment, secure subcontracts for ancillary support services, arrange for and provide training to our staff and conduct extensive outreach and marketing prior to the clinic’s opening. This carefully coordinated effort, which has resulted in timely openings for all of our clinics, clearly demonstrates our ability to manage successfully large contract start-ups within the specified time constraints.
Due to the short timeframe for transition of clinic services following award or the establishment of new clinic services, it is essential that pre-credentialing efforts are complete prior to contract award for all
50
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.

privileged healthcare providers including physicians, nurse practitioners and physician assistants, as well as any personnel that must complete the Vet-Pro credentialing. Additionally, in our experience, candidates are typically reviewed by the VAMC in meetings conducted only once per month, making our pre-recruiting and credentialing efforts even more critical to assisting timely start-up of service.
The table below illustrates the processes and methodologies of our multi-phase recruitment and credentialing efforts utilized in the management of CBOC services, from the initial phase of proposal development through post-award efforts. The below table is organized in reverse workflow manner and lists 1 day prior to commencement of clinical operations as the first delineated item:
90 Day Operational Startup Plan – From Award to Clinic Startup5 Days Prior to Commencement of Clinic Operations
Completion of all in-clinic personnel documents and OSHA declarations7 Days Prior to Commencement of Clinic Operations
One week orientation of providers and staff to begin at clinic 14 Days Prior to Commencement of Clinic Operations
One week hospital orientation begins; credentials must be complete by this date21 Days Prior to Commencement of Clinic Operations
One week orientation at alternate Offeror CBOC; provider start date 35 Days Prior to Commencement of Clinic Operations
Status update with program manager and new providers regarding changes (if any) to three-part orientation schedule
40 Days Prior to Commencement of Clinic Operations Ensure that malpractice certificates for providers and Offeror have been submitted to
hospital50 Days Prior to Commencement of Clinic Operations
Final date for submission of all required credentialing documents including contractor verification to hospital
Target date for completion of manager hire Determination of final staff candidates; telephone interviews with Program Manager
of proposed hire in each category55 Days Prior to Commencement of Clinic Operations
Final manager interviews Initial staff interviews
57 Days Prior to Commencement of Clinic Operations If credentialing to be completed through use of VET-Pro, ensure that providers have
received mailing from hospital and completed internet application Initial manager interviews; all references completed; determination of final candidates
59 Days Prior to Commencement of Clinic Operations Initial manager interviews commence Screen staff candidates and set initial interviews
60 Days Prior to Commencement of Clinic Operations
51
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
Target date for provider-signed contracts in hand Screen all staff candidates
70 Days Prior to Commencement of Clinic Operations Final provider candidates interviewed by Vice President; contract negotiations
completed75 Days Prior to Commencement of Clinic Operations
Staff advertisements to run Commitment and availability received from final provider candidates; final candidates
interviewed by medical director Determination of final provider candidates; all references completed
78 Days Prior to Commencement of Clinic Operations Screen all newly received provider candidates with sample contracts sent Manager telephone interviews with final candidates
81 Days Prior to Commencement of Clinic Operations Application for CLIA certificate completed and submitted Screen all existing candidates with sample contracts sent
<THIS SPACE INTENTIONALLY LEFT BLANK>
52
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
B. COORDINATION AND CONTINUITY OF CARE
Through operating CBOC Clinics on behalf of the VA for more than 13 years, Xxxxxx Xxxxx has both a unique awareness and attentiveness to VHA and VISN policies, regulations, and standards, as well as JCAHO and HIPAA policies. We recognize that an essential component of any successful Offeror’s ability to achieve client satisfaction is an individually formulated Quality Control Plan. Xxxxxx Xxxxx’s corporate Quality Control Plan has three (3) basic components:
Daily operational integrity: A corporate and operational culture that stresses importance in regards to all facets of daily operation.
On-site inspections that are independent of the command structure: The Contractor independently monitors the quality of service provided at the job location.
Assessment of service delivery: The Contractor collects and examines data to continually assess the quality of service provided.
Xxxxxx Xxxxx recognizes that Quality Control programs, in order to be truly effective, must be tailored to the specific needs of each client. Fundamentally, then, our Quality Control Plan is centered around an emphasis on monitoring the quality of service provided under each Key Performance Element.
Xxxxxx Xxxxx has specifically designed its Quality Control Plan to adhere to the following core principles:
Client Focus: As a primary goal, Xxxxxx Xxxxx encourages open and regular client feedback at all levels. Client satisfaction is measured through scheduled audits, program reviews, follow-up inquires, coordination with the client, and client reaction at the service level.
Corporate Philosophy: A corporate philosophy that revolves around proactively carrying out all administrative and recordkeeping tasks, maintaining the highest quality of service through corporate organization and efficiency, and the identification and correction of any problems or issues which adversely affect service delivery before such problems or issues adversely affect contract performance.
Employee Knowledge: Quality requirements and work standards are provided to all employees through training programs, orientation programs, and feedback from performance assessments. Contract-wide awareness of quality standards helps to prevent deficiencies caused by lack of awareness of contract requirements and contract goals.
Employee Empowerment: Xxxxxx Xxxxx encourages employees to take proactive ownership of their responsibilities, remain open to client feedback and report all problems to their supervisor.
Rapid Resolution: Every attempt is made to analyze and solve problems at the lowest effective level within the organization. Problems are immediately passed to the Project Manager and other appropriate Corporate Management channels as soon as it is evident that a higher level of management involvement is required.
53
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
Documentation: Every deficiency, corrective action, improvement, and change to processes or procedures is documented for full traceability. Such process allows for the expedient resolution of any issues or problems that may arise.
The above, generalized approaches to Quality Control have been formally and functionally integrated into our performance measurement process that will be implemented to monitor quality, appropriateness of care, access, and patient satisfaction. To that end, our plan for measuring and ensuring high levels of quality, appropriateness of care, access, and patient satisfaction is detailed below. The VAMC’s QASP is a direct customer service interface which will exist between the successful Offeror and the VA. Upon award to Xxxxxx Xxxxx this QASP will ensure that Xxxxxx Xxxxx performs in accordance with pre-set performance objectives, and that the VA receives the necessary service outcomes called for in the Solicitation.
For its part under this QASP requirement, Xxxxxx Xxxxx recognizes that it must not only strive to provide the Government with quality personnel, but must also demonstrate the ability to self-monitor and self-regulate furnished services.
As represented in the following sections, Xxxxxx Xxxxx acknowledges that it is absolutely crucial that the Offeror presents an understanding of the requirements as set forth in the Solicitation. For an instituted QASP to succeed, the successful Offeror must be able to demonstrate competency in the Government’s stated needs. All information, therefore, will be included in our QASP Report (Monthly Contracting Report) provided to the VA, as well as to the corporate CBOC Management Team. QASP meetings include numerous key clinic members, on-site administrative/supervisory staff and the corporate management team to ensure that all issues are identified and proposed resolutions are carried out efficiently and effectively.
The Leadership of the Taos CBOC and Xxxxxx Xxxxx’s Corporate Management Team will coordinate continual monitoring to assure that the delivery of healthcare is appropriate, timely, accessible, available, medically necessary in keeping with established guidelines and standards and reflective of the current state of medical knowledge.
The Contracting Officer (“CO”), the CBOC Medical Director, the Contracting Officer’s Technical Representative (“COTR”), the Physician Director for Performance Improvement, the CBOC Infection Control Coordinator and the Registered Nurse Clinic Coordinator comprise the key on-site personnel for the Quality Management/Improvement.
The Xxxxxx Xxxxx Corporate Management Team, which includes the corporate level Quality Improvement Program Coordinator, the corporate level Coordinator of Patient Advocacy and Xxxxxx Xxxxx Physician Consultants for CBOC Provider Training and Quality Assurance, will provide constant support to the CBOC’s on-site personnel. For further delineation of Xxxxxx Xxxxx’s Corporate Management Team, please refer to Section A.7.
B.1. APPROPRIATENESS OF CARE
Assuring the appropriateness of care at the Taos CBOC location is a key aspect necessary for contractual success. To assure our proposed CBOC’s appropriateness of care, this section will demonstrate our ability to manage appropriateness of care.
54
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
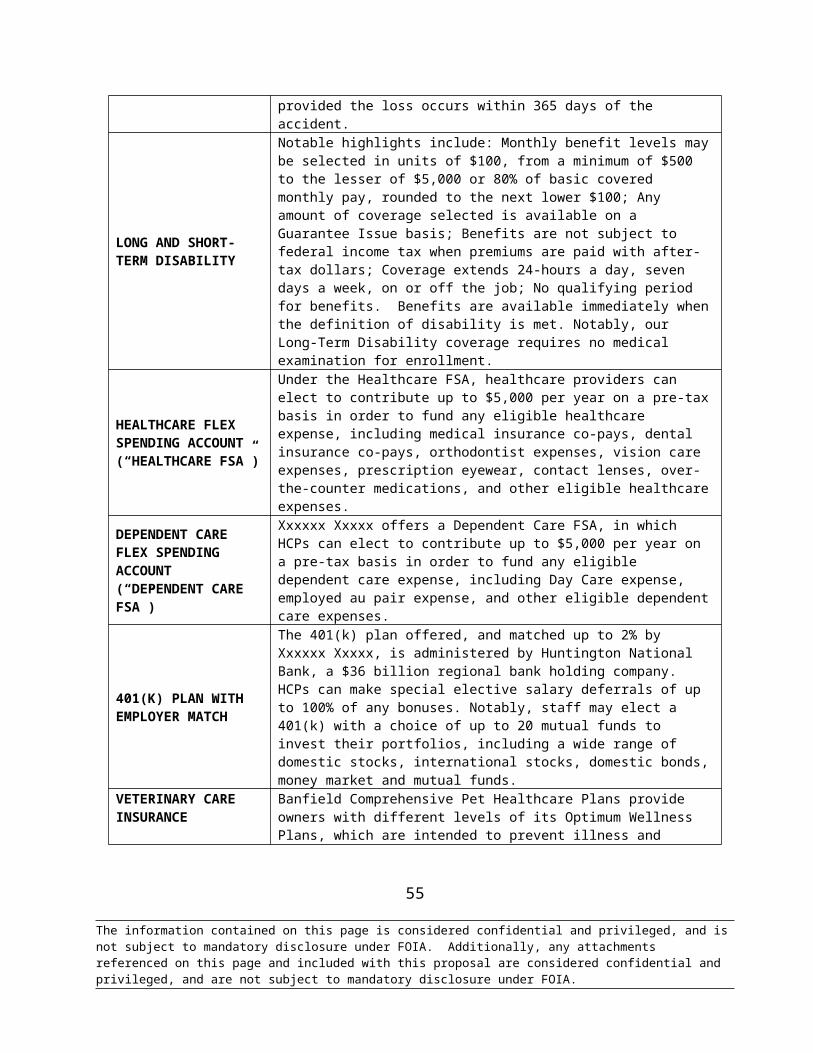
B.1.A. XXXXXX XXXXX’S ABILITY TO ASSURE APPROPRIATENESS OF CARE
Xxxxxx Xxxxx has over 13 years of nationwide CBOC management experience where we have been required to oversee all managerial aspects of CBOC contracts including recruiting, credentialing, retention, construction, orientation and training and continuing compliance and quality assurance, among others. In the execution of CBOC contracts during this span, Xxxxxx Xxxxx has placed an emphasis on establishing and maintaining effective communication among CBOC staff, Sterling management and the VA representatives. Xxxxxx Xxxxx’s corporate-level management organizational structure in its entirety is included for the VA’s review in Section B.2 of this proposal.
To ensure the coordination of services nationwide, our CBOC Management Services team members, including Xxxxxx Xxxxx Vice President for VA Services who also serves as CBOC Program Manager under this Contract, meet daily via teleconference to discuss staffing, facility or performance issues for all clinics. Furthermore, we have developed our national management program based upon years of operating CBOC clinics for the VA, as well as other services such as staffing for VA Medical Centers.These and comparable efforts have made us very knowledgeable of national VA programs and directives, as well as policies applicable to particular VA Healthcare Networks.
We have developed a Patient Advocate Program that not only informs each veteran consumer of their rights, responsibilities and contact information for the VAMC Patient Advocate applicable to that CBOC service, but also contact information for our own Patient Advocate. Patients are encouraged to share comments or suggestions with each clinic’s coordinator, but are also encouraged to contact our Patient Advocate via a toll-free 800#. The advantage of our Patient Advocacy Program is that patients are put in direct contact with our corporate management team, thus ensuring appropriateness of care. Patients are then provided with return reports, within seven (7) days of contract with Xxxxxx Xxxxx’s Patient Advocate Program, which delineates any corrective measures taken. Any issues identified by the patient are documented by our Patient Advocate who then initiates an investigation and completes a report with signed statements as applicable. This information is sent to all members of the corporate management team for follow-up, including any necessary disciplinary or corrective actions, which are also included in the report. Our Patient Advocacy Program is further discussed in Section A.1-3B. Finally, such information obtained through our Patient Advocacy Program is included in our Quality Assurance reporting to the designated VA representative.
Xxxxxx Xxxxx Vice President for VA Services – Mr. Brandon Xxxxx will perform the following duties:
Conduct daily teleconferences with all Xxxxxx Xxxxx departments applicable to CBOC services for resolution of identified areas of concern
Attends on-site meetings with the VAMC at Contract start-up phase, quarterly or monthly at the VAMC’s and Contracting Office’s preference thereafter
Participates in Provider or staff counseling Present at the Clinic on the occasion of any external audit or survey affecting the Taos Clinic
(JCAHO, SOARS, OIG, etc.) Oversees timely for launch of all new clinic initiatives Daily oversight for CBOC staff provider recruitment and continuity of service at CBOC
locations nationally
55
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
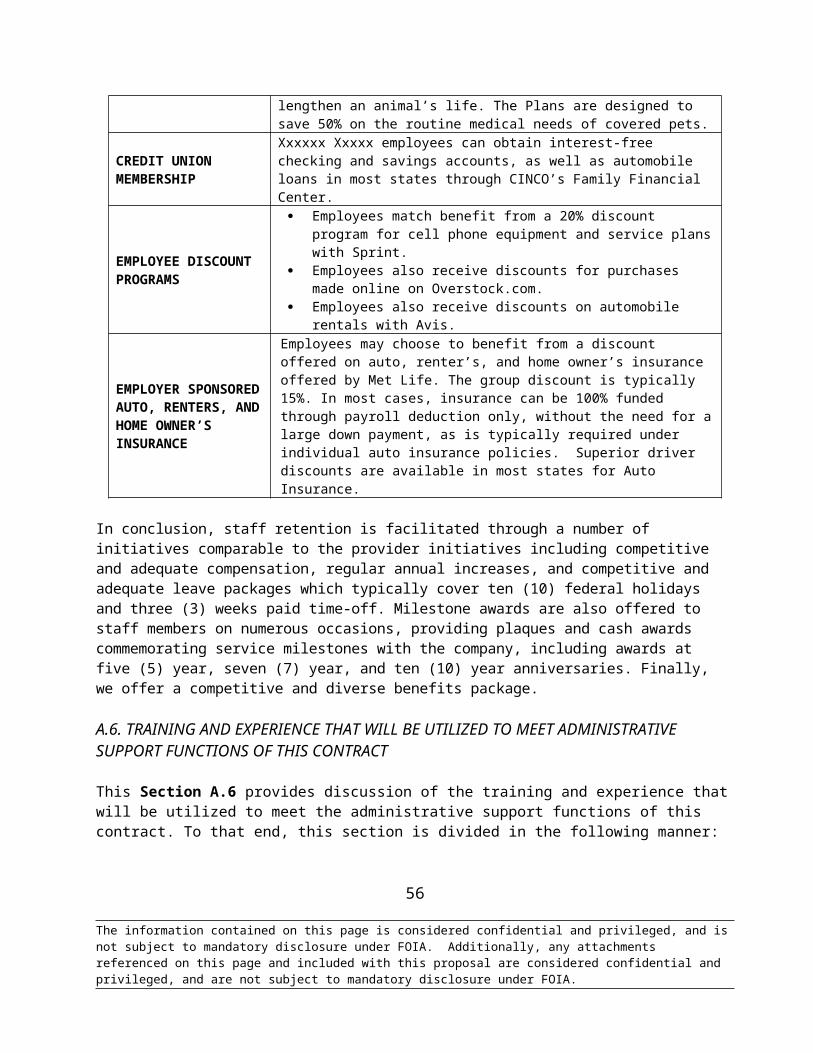
Xxxxxx Xxxxx CBOC Clinical Liaison – Ms. C. Xxxxx, LPN, will perform the following duties:
Conduct clinic walk-throughs and on-site visits, on a scheduled and unscheduled basis, on at least a quarterly basis throughout the Contract period to ensure ongoing compliance with VHA requirements
Conduct CBOC Start-Up Employee Orientation Communicate with VA representatives concerning Contract performance and other concerns
via scheduled monthly teleconference meetings, quarterly face to face meetings, and additionally as needed
Oversight of JCAHO Contract compliance for assigned clinics
Xxxxxx Xxxxx Physician Consultants for CBOC Provider Training and Quality Assurance - Dr. Ethan Loeb, MD and MPH&TM, Dr. Donald Courts, MD, and Dr. Barry Kaler, DO. Sterling’s specialized CBOC Program Physician Consultants will provide direction relating to both provider training and quality assurance at the Taos CBOC under the proposed Contract.
Notably, each of the above-listed Physician Consultants were selected and retained in this role due to extensive experience at a wide range of VA CBOC and VAMC assignments over multi-year periods while maintaining the highest QA and EPRP results. Each physician has years of experience in providing this oversight for Xxxxxx Xxxxx as follows: Dr. Courts, two (2) years; Dr. Kaler, five (5) years; and Dr. Loeb, two (2) years.
These Physician Consultants will perform the below listed responsibilities as they apply to the Taos, NM CBOC:
Provide training at the CBOC startup phase for the new Provider staff Provide peer review for Providers regarding whom non-agreement exists in peer body on
previous reviews Participate in counseling and/or annual practice reviews for Providers noting areas for
performance improvement
Xxxxxx Xxxxx CBOC Director of Operations – Ms. C. Xxxxxxx will perform the following duties:
Conduct weekly meetings with the Taos CBOC Clinic Coordinator to discuss incidents or problems
Conducts monthly meetings with the full Taos CBOC clinic staff, including providers, to resolve outstanding issues of concern
Obtains and reviews daily reports from the Taos Clinic “Snapshot” pertaining to clinic access Obtains and reviews weekly reports from Xxxxxx Xxxxx’s Patient Advocate regarding patient
satisfaction activity from the Taos Clinic Obtains and reviews daily reports pertaining to timeliness of documentation with regards to
Providers at the Taos CBOC Reviews and submits, on a monthly basis, Quality Assurance reporting data pertaining to the
Taos CBOC
Xxxxxx Xxxxx CBOC HR Liaison – Ms. K. Xxxxx will complete the following CBOC-related
56
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
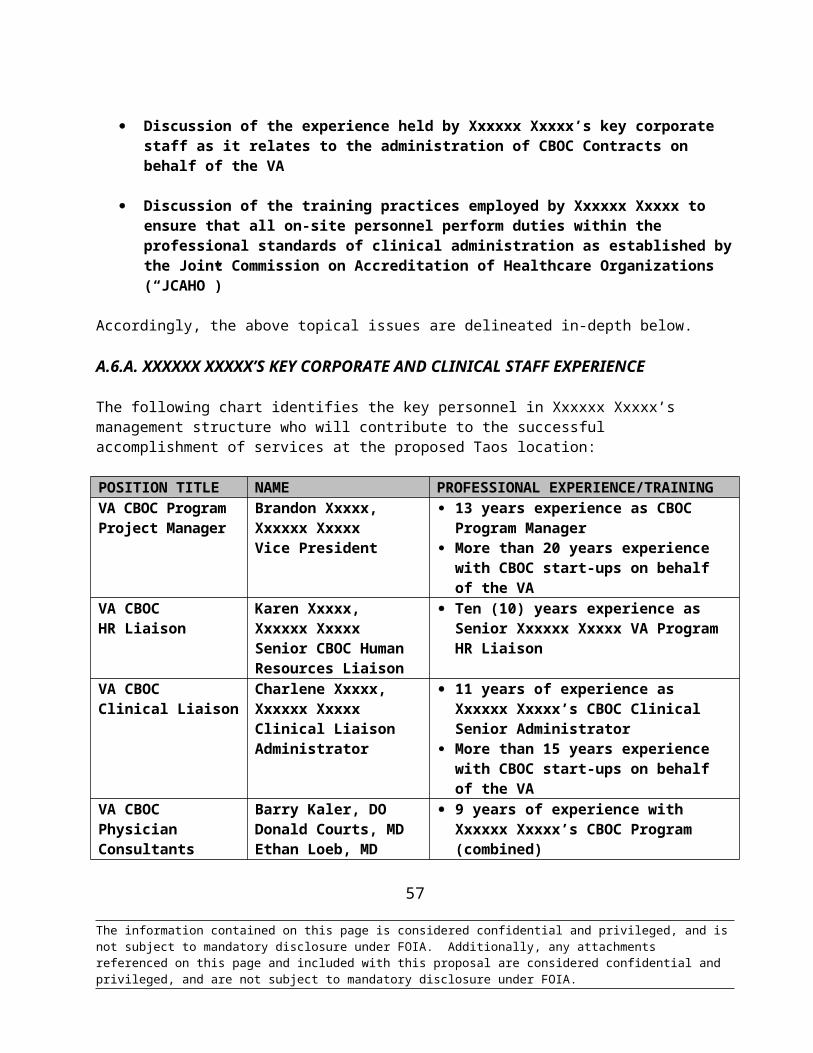
responsibilities:
Conducts weekly meetings with Xxxxxx Xxxxx’s CBOC Director of Operations to address any staff member problems or concerns
Provides written and oral counseling and commendation to CBOC staff based on both quantitative and qualitative standards from Xxxxxx Xxxxx’s monitoring and administrative programs
Ensure that Xxxxxx Xxxxx is committed to adhering to an early feedback loop to facilitate counseling and/or intervention based on quick detection and communication of issues that may have the potential to adversely affect appropriateness of care on the part of Provider or staff at the Taos CBOC prior to its occurrence
B.1.A.I XXXXXX XXXXX’S MANAGEMENT RESPONSE TO POTENTIAL PROBLEMS
Management Response to Potential Problems - Xxxxxx Xxxxx is dedicated to an ongoing effort to address any potential problems that may arise and affect the optimal operation of the CBOC facility. Xxxxxx Xxxxx’s extensive experience has afforded it the luxury of facing and overcoming such operational obstacles by developing a standard management response plan to combat any problems that may potentially disrupt operations without advance management readiness plans in place. Examples of such advance readiness planning/management handling procedures do follow:
In order to respond to human resource/staffing issues, the following procedures will be followed:
For any noted problems or deficiencies for staff members at the clinic, the On-Site Clinic Manager would provide verbal counseling to the affected staff member at the clinic. Such counseling and discussion would occur on an on-going basis to cover minor issues and problems that arise with respect to clinic staff.
In the event that more serious problems arise or problems were of a reoccurring nature, the On-Site Clinic Manager would provide written counseling to clinic staff using Xxxxxx Xxxxx written counseling forms and formats. All written counseling forms are approved in advance by the VA CBOC HR Liaison prior to dissemination to clinic staff. Once disseminated and acknowledged in writing by the affected employee, the written counseling form is maintained in the following locations: 1) locally at the clinic in the clinic employee file; 2) in the VA CBOC Program Office; and 3) in the corporate payroll file.
In cases where the same employee receives several written counseling forms, or a serious problem emerges which, although only one instance of the problem has arisen, is of such a nature that a full performance improvement plan is necessary to protect the interest of Xxxxxx Xxxxx or the Clinic, a written performance plan is written by the On-Site Clinic Manager and approved by the VA CBOC Clinic HR Liaison. The performance improvement plan is then agreed to, and signed off on by the affected employee.
In cases where the employee continues to manifest the problem that has been the subject of written counseling, or fails to follow a written performance improvement plan, or engages in actions of such a serious nature, that they themselves warrant dismissal, without counseling or use of a performance
57
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.

improvement plan, the staff member’s employment relationship with the company will be terminated. All such employee terminations are made only following guidance from Xxxxxx Xxxxx’s corporate legal counsel.
Types of behavior and employee actions which are serious enough to warrant immediate termination are set forth in the Employee Handbook. These are also the type of offenses, which, by common sense standards, would disrupt or violate the overall mission of the clinic and the reputation of Xxxxxx Xxxxx. Examples might include gambling on the job, carrying a weapon onto the workplace or other disorderly/illegal activities. None of these activities, it should be noted, has ever occurred with respect to a Xxxxxx Xxxxx employee; they are provided as examples only.
Another potential human resource issue that might arise in the course of the proposed contract might include an instance of alleged sexual harassment.
Xxxxxx Xxxxx maintains a clear written policy against sexual harassment in its Employee Handbook. The policy clearly sets forth the types of action by supervisors and by employees that might constitute sexual harassment. The Employee Handbook also clearly sets forth the reporting mechanism for individuals who feel they or others have suffered from sexual harassment in the workplace. Under this policy all individuals are requested to report any such instance to the CBOC HR Liaison for appropriate action.
All reports of sexual harassment are fully investigated, and when appropriate, prompt corrective action is taken. Investigation will be made by telephonic interviews and in-person interviews as necessary. Disposition of any sexual harassment claim is made with guidance from Xxxxxx Xxxxx’s corporate legal counsel, in all instances.
Another potential human resources problem that could conceivably arise under the CBOC or other health services Contract could be the suspicion or allegation of healthcare worker alcohol or drug abuse.
Such problems will be addressed under the guidance of Xxxxxx Xxxxx’s Drug Free Workplace Policy. Xxxxxx Xxxxx, in this context, is committed to maintaining an alcohol and drug-free workplace. Xxxxxx Xxxxx will take immediate action against any employee who, while performing service on behalf of the company, possesses, manufactures, consumes, transfers, sells or attempts to sell any form of alcohol, narcotic, depressant, stimulant, hallucinogen, or any other mind or perception-altering substances. This excludes the consumption of prescription medication as directed by a licensed physician.
Any employee who violates this policy will be subject to immediate termination. All instances of alleged alcohol or drug abuse are to be referred to Xxxxxx Xxxxx’s VA CBOC HR Liaison. The VA CBOC HR Liaison will fully investigate any allegation of substance or alcohol abuse, requesting workplace drug testing where appropriate.
Any confirmed instance of alcohol or drug abuse will result in termination of employment and further legal action where appropriate, with such action conducted by the VA CBOC HR Liaison, in consultation with corporate legal counsel.
Requests for counseling by employees who require assistance or treatment under our Drug Free
58
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
Workplace Policy are also addressed to the VA CBOC HR Liaison. Assistance and/or treatment will be arranged as needed to protect the interests of the clinic and of Xxxxxx Xxxxx.
Staffing shortfalls that might occur due to sickness, short-termed disability or other unplanned events represent another category of problems that could possibly affect the clinic. Xxxxxx Xxxxx’s plan for avoiding problems related to staffing the clinic in the event of staff absence is as follows.
First, pre-recruited and pre-credentialed providers will be utilized to provide backup coverage for relevant periods of provider absence, including periods of scheduled and unscheduled leave. Throughout this Contract, Xxxxxx Xxxxx will ensure that a minimum of four (4) backup locum tenens staff members are fully credentialed and available to provide backup staffing at the Taos CBOC facility for all periods of scheduled and unscheduled leave.
For periods of unscheduled provider absence, all providers will be required, under their written employment agreements, to notify the On-Site Clinic Manager as soon as possible of any unscheduled absences. The On-Site Clinic Manager, in turn, will notify the Lead Recruiter of any unscheduled provider absences, so that coverage can be arranged, if at all possible, utilizing one of the pre-recruited, pre-credentialed providers available to furnish coverage at the clinic. Once coverage has been confirmed for any period of unscheduled provider absence, the Lead Recruiter will notify the On-Site Clinic Manager, as soon as possible, by telephone and email, so that the clinic schedule can be adjusted accordingly. This will facilitate resolution of problems caused by unscheduled leave on the part of providers.
Similarly, for staff absences, a pre-recruited, pre-credentialed staff member will be retained for necessary coverage. For the Taos Clinic, at least two (2) such backup staff members will be identified and retained. Backup members will consist of LPNs and medical assistants, cross-trained so that they can also perform administrative duties in support of medical reception and medical records. This will facilitate resolution of problems caused unscheduled leave on the part of staff.
Another potential issue that could arise in the proposed contract would be patient complaints. Such complaints, if they arise would be dealt with as follows.
Regarding patient complaints, we note that a statement of patients’ rights will posted in each clinic. In each clinic, along with the patient rights statement, the 1-800 toll-free telephone number of Sterling’s CBOC Patient Advocate is prominently posted. The CBOC Patient Advocate notes all patient complaints in a Patient Complaint Log, which is a permanent record maintained by Xxxxxx Xxxxx.
All patient complaints will be thoroughly investigated by the CBOC Patient Advocate under the proposed Contract. Investigation will be performed telephonically, or, if necessary, on site at the Clinic. Results are reported back by the CBOC Patient Advocate to the patient or the patient’s surrogate. Such reporting is done by private telephone call reported personally by CBOC Patient Advocate. In this context, we note that all patients possess the right to be free from physical, mental, sexual, and emotional abuse. If appropriate, the proper legal authorities will be notified by the CBOC Patient Advocate. The requirement for notification of the authorities is clearly maintained for guidance of the CBOC Patient Advocate in the event of an occurrence requiring such notification. These procedures will guide resolution of any problems regarding patient complaints
59
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
under the proposed contract. Record of all reported patient complaints to the Xxxxxx Xxxxx Patient Advocacy Program along with their disposition are provided as a part of the monthly Xxxxxx Xxxxx Quality Assurance Report to the applicable VAMC, as well as any other requested reporting on a by Hospital basis.
Another potential problem that might arise under the proposed contract might conceivably be an injury of an employee at the workplace.
Procedures for immediate reporting of such an injury are posted in each clinic and will be included in the Employee Handbook, applicable to each clinic. All injuries occurring at work are to be reported to the CBOC HR Liaison under this program.
Upon communication of the injury or illness, appropriate facts are obtained including the nature of the illness or injury, the date and circumstances of the illness or injury, and the names of any individuals who witnessed the illness or injury. All illness or injury occurring as the result of any employee’s work is immediately reported to Xxxxxx Xxxxx’s workmen’s compensation carrier for follow-up-action.
The outcome of any such occurrence is also tracked by Xxxxxx Xxxxx on an on-going basis until the occurrence is fully resolved, the employee has returned to work, and all necessary financial compensations have been obtained on the employee’s behalf from the insurance carrier.
Another problem that might arise during the course of contract performance could be an alleged instance of medical malpractice.
In the event of such an occurrence, the incident or the claim would be immediately reported to the CBOC Hospital Liaison. The CBOC Hospital Liaison, in turn, would report the incident to Xxxxxx Xxxxx’s malpractice insurance carrier for investigation and/or defense as appropriate.
A potential problem area that could arise during performance of the proposed contract would be a problem involving telephone access, internet access, or power interruption.
Any such problem would be immediately reported by the On-Site Clinic Manager to the CBOC Program Manager and to the Director of Telecom, Teleconnectivity and MIS (the “Director of Telecom”). The Director of Telecom is available via both cell phone and pager on a 24 hours per day, 7-days per week basis. During any time that he is not available, his cell phone and pager duties are assumed by an alternate so that coverage of this position is always maintained.
Upon notification of any problem involving telephone access, internet access, or power interruption, the Director of Telecom will immediately contact the appropriate service provider for resolution. The Director of Telecom maintains a deep understanding of service issues that might impact connectivity or access on the part of the clinics, as well as close relationships with service providers. The Director of Telecom will continue to interface with the appropriate service provider until the connectivity issue has been resolved and service has been restored.
Another potential area of problems that might arise in the performance of the proposed contract would be problems involving the security of the clinic.
60
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
All clinics possess security alarms to secure the clinic after clinic hours. These alarms can be triggered by motion or intrusion. In such cases, the alarm monitoring company will first notify the police and will then notify the On-Site Clinic Manager. The On-Site Clinic Manager will then go to the clinic to meet the police on site. Following this direct response, an incident report will be conducted at the Clinic, and the Facilities Director will be notified for follow-up action.
Other security-related problems will be referred to the Facilities Director for follow-up action. Such issues might also conceivably be identified through the mechanism of the Quarterly Security and Safety Survey. Any such issues would be reported to the Facilities Director for appropriate resolution. Any security or safety breaches or concerns are documented on incident reports by the Facilities Director. On each incident report, the Facilities Director tracks resolution of any noted security incidents or concerns.
The above discussion is intended to illustrate the types of specific problems that could conceivably arise over the course of the proposed Taos, IN CBOC Contract, as well as Xxxxxx Xxxxx’s operational approach to resolving these specific types of problems. The above discussion certainly does not cover every type of problem that might arise over the course of the proposed contract.
Regarding general methods of problem resolution, it should be noted that a key management tool for coordinating Xxxxxx Xxxxx’s overall contract effort and its management of both problems and performance initiatives that might arise during the course of contract performance will be the mechanism of the CBOC Management Team Meeting (the “Management Team Meeting”), to be scheduled every Tuesday. The attendees for this meeting will be the VA CBOC Program Manager, the VA CBOC HR Liaison, the VA CBOC Clinical Liaison, the VA CBOC Hospital Liaison/Clinic Coordinator and the Lead Recruiter (these individuals are referred to as the “Management Team”). The attendance of other staff members may be requested according to need and relevance to issues being covered. The CBOC Management Team Meeting will provide a mechanism by which problems are brought to the attention of the Management Team, so that such problems and concerns can be acknowledged and promptly addressed in the most appropriate manner.
A management team memo will summarize the key results of each CBOC Management Team Meeting, including problems and/or issues encountered, considerations evaluated, and resolutions adopted. The Management Team Memo will be distributed prior to the next week’s Management Team Meeting to all Management Team attendees. A complete archive of Management Team Memos will be retained for the entire course of contract performance at Xxxxxx Xxxxx’s corporate office.
Through use of the Management Team meetings and the Management Team Memos, the input of key Management Team members will be brought to bear upon any major problems or issues that arise through the course of contract performance. These management tools will ensure that all management resources are brought to bear upon any problems or issues which arise during the course of contract performance, and will also ensure that all key Management Team members will have access to important information related to problems or issues that arise, with such information available to all Management Team members in a timely fashion. Through appropriate input and coordination of all Management Team members, on a regular weekly basis, the best possible resolution may be arrived at through the course of contract performance.
Another management tool, which will be utilized in the resolution of any problems that arise in the performance of the proposed contract, will be regular coordination and communication with the
61
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
Government, coordinated and conducted through the Government COR in the form of a monthly teleconference. Monthly administrative teleconference calls promote communication amongst Xxxxxx Xxxxx Contract Administrators and the RLR VAMC. This allows for the coordination of service information and administration efforts toward accomplishing Xxxxxx Xxxxx’s overall goal of providing high quality healthcare services. The frequency of the monthly teleconference calls ensures that both Xxxxxx Xxxxx Contract Administrators and the RLR VAMC are kept up-to-date on all aspects of service. Through such action, appropriate input will be obtained from the Government that will assist Xxxxxx Xxxxx’s Management Team to incorporate targeted resolution mechanisms to problems and/or new performance initiatives that arise during the course of contract performance. Xxxxxx Xxxxx fully realizes that its purpose under the proposed contract is to fully serve the needs of the VA and the VA beneficiaries, and that therefore input from the VA is essential if the best possible resolution of problems and ongoing developing performance for the clinic is to be attained.
In conclusion, resolution of problems and/or the addressing of new performance initiatives, which arise under the proposed contract, will be guided by a clear set of established policies and procedures. The individuals who can provide performance resolution on the part of Xxxxxx Xxxxx will possess clearly defined areas of responsibility, commensurate with their education and management experience. Consultation will be made with Xxxxxx Xxxxx’s corporate legal counsel for all problems where legal issues may arise. A team approach will be utilized based on regular Management Team Meetings, in order to ensure appropriate input by all key management representatives for problems, which affect the clinic as a whole. Finally, the regular input of the Government will be sought where appropriate in order to arrive at the best possible resolution for any problems, which may arise.
B.1.A.II XXXXXX XXXXX’S METHODS TO AVOID CONFLICT OF INTEREST
Organizational conflicts of interest (“OCI”) arise out of the confluence of corporate relationships and the performance of government contracts. The burden is on The Management Team to identify such conflicts and provide strategies to the contracting officer that demonstrates how conflicts of interest will be avoided and mitigated.
The Government Accountability Office (“GAO”) has long recognized that there are three major types of organizational conflicts of interest: biased ground rules, unequal access to information, and impaired objectivity.
FAR Regulation 2.101 is a subsection of Title 48 of the Federal Acquisition Regulation. The “definitions” section of FAR 2.101 states the following about organizational Conflict of Interest:
“Organizational Conflict of Interest” means that because of other activities or relationships with other persons, a person is unable or potentially unable to render impartial assistance or advice to the Government, or the person's objectivity in performing the Contract work is or might be otherwise impaired, or a person has an unfair competitive advantage.”
The general rules in 9.505-1 through 9.505-4 of the FAR prescribe limitations on contracting in order to avoid, mitigate or neutralize organizational Conflicts of Interest.
The Management Team takes seriously its obligations under this regulation, just as it recognizes the
62
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
importance of its existence in safeguarding the Government’s interests. As stated in 3.1 of the FAR, since Government Contracts are transactions involving expenditure of public funds, they require the highest degree of public trust and an impeccable standard of conduct. As the FAR OCI language illustrates, avoiding potential or actual Conflicts of Interest is essential to the proper delivery of all services required under such Government Contracts. In an effort to properly and thoroughly comply with the FAR regulations regarding Organizational Conflict of Interest, the Management Team has examined any and all potential Conflicts of Interest that may arise in the performance of this Contract, in order to identify potential areas of concern and prevent their eventual occurrence.
B.1.B. MECHANISMS UTILIZED TO ASSURE APPROPRIATENESS OF CARE
To assure appropriateness of care, Xxxxxx Xxxxx will utilize both an internal and external Peer Review Program. Nurse Practitioner and Physician Assistant notes will be evaluated using the same high standards as the Physicians. However, their notes will be reviewed specifically by their Supervising Physician. Time will be allotted for the Supervising Physician and the Nurse Practitioner/Physician Assistant to critique the notes. The Nurse Practitioner/Physician Assistant will then complete a PIP if needed. This plan will then be submitted to the QA Coordinator for Xxxxxx Xxxxx, for inclusion with the QM/I packet to the Hospital.
B.1.B.I. VA EXTERNAL PEER REVIEW PROGRAM
Xxxxxx Xxxxx will participate in the VA External Peer Review Program (“EPRP”) as an additional method to enhance Clinic quality and responsiveness, if allowed to do so. Xxxxxx Xxxxx’s participation in EPRP will be incorporated into its Quality Management/Improvement program data by reporting period. Xxxxxx Xxxxx will welcome RLR VAMC personnel to perform record reviews on electronic records and will ensure that all electronic records contain appropriate documentation required to meet all regulatory standards and national VHA, VISN 11 and RLR VAMC performance measures.
With regards to this phase, Xxxxxx Xxxxx will request the opportunity for our assigned Clinical Liaison to participate in the External Peer Review Process, as it has been our experience that doing so allows the contract clinic workload complement the opportunity to be represented at the DACS level of the survey. By doing so, at any VA Hospital where Xxxxxx Xxxxx has been invited to participate in this phase of the process, Xxxxxx Xxxxx has learned that it has been able to assist the hospital in obtaining all necessary data related to any encounters performed at the CBOC level. Additionally, such participation will allow for real time follow up by the contractor with its Provider staff.
Whether or not Xxxxxx Xxxxx is granted the opportunity to participate in the exit survey, we will include as part of the Taos, IN CBOC’s Quality Management/Improvement program:
Arranging one-on-one interviews with Managers and Providers following feedback within 7 days from the EPRP data follow-up availability to ensure that all DACS identified patient information has been addressed in the CPRS Record.
Addressing any trends identified with individual Providers in an interview format. Incorporating a corrective action plan designed to address any concerns raised from the
EPRP. Such corrective action plans will be incorporated into the QM/I Plan for that Quarter.
63
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
B.1.B.II. EMPLOYEE PERFORMANCE INCENTIVES
Xxxxxx Xxxxx will utilize performance incentives to ensure health promotion, disease prevention, and access to care, patient safety and QA reporting. These performance incentives correspond with the VA’s Performance Incentives, found on Pg. 54 of the Solicitation. These performance incentives pertain to the following items:
Acceptable levels for the Preventive Health Index and applicable clinical practice guidelines. Maintain an average waiting time of three (3) days. Achieve 100% accuracy with enrollment and test data entry.
Notably, Xxxxxx Xxxxx will pass the full amount of contract awarded positive incentives, as described in Section J of the Solicitation’s Special Contract Requirements, to individual providers on their own patient population.
Finally, Xxxxxx Xxxxx will utilize performance incentives to ensure health promotion, disease prevention, and access to care, patient safety and QA reporting. On a quarterly basis, Xxxxxx Xxxxx will provide a cash incentive of $1,500 to be split equally among clinic staff members for meeting the following performance goals:
Meeting access to care standards with no existing patients waiting more than 7 days for a scheduled primary care appointment and no new patient waiting more than 14 days for a primary care appointment.
Scoring at or above the national average for patient satisfaction (85% or higher). Demonstrated improvement in meeting or exceeding goals for clinical reminders. Maintaining “0” patient safety incidents. Maintain the Clinic’s SHEP score within a range of at least meeting the VISN 11’s average
scores in all categories. Maintaining a negative correlation between patient visits and verified patient complaints
through utilization of both the Xxxxxx Xxxxx and VA Patient Advocacy Programs.
B.2. XXXXXX XXXXX’S UNDERSTANDING OF JOINT COMMISSION AND OTHER REGULATORY REQUIREMENTS
Compliance with all Joint Commission on Accreditation of Healthcare Organizations (JCAHO) Standards are monitored through monthly questionnaires for staff, satisfaction surveys for patients, quarterly mock surveys, clinic "walk-throughs", hazard surveillance inspections and our Quality Assurance Program. We have independently listed the standards that are applicable to current CBOC locations and then presented how those standards are met. These topics, as discussed below, are intended to demonstrate Xxxxxx Xxxxx's working knowledge of JCAHO regulations. Xxxxxx Xxxxx's proposed CBOC clinic in Taos, New Mexico will be maintained in strict compliance with the current Joint Commission Comprehensive Accreditation Manual for Ambulatory Care standards (CAMAC). Specifically, the topics covered in the CAMAC that are applicable to clinic operations are listed as follows:
Xxxxxx Xxxxx currently administers primary care and mental health services at a number of VA CBOC locations throughout the United States. As such, Xxxxxx Xxxxx is experienced in providing services that meet or exceed the regulatory guidelines established by JCAHO. Xxxxxx
64
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.

Xxxxx has always taken its obligations for JCAHO compliance at its clinics extremely seriously, providing the on-site presence of National Program Office staff to ensure full preparation for these activities.
The Xxxxxx Xxxxx's JCAHO preparedness team will include a full-time JCAHO Preparedness Nurse acting exclusively to provide administrative review of the Community Based Outpatient Clinic procedures and operations to ensure JCAHO readiness and compliance of each clinic.
In order to ensure that JCAHO readiness is maintained, the organization conducts quarterly mock surveys on an unscheduled basis at each of its clinics. Such mock surveys are conducted and involve both an assessment and written checklist of JCAHO compliance, as well as quarterly training of staff members on JCAHO compliance issues.
In order to ensure JCAHO readiness, the organization has developed a series of plans designed to ensure compliance with all aspects of JCAHO standards. EOC Documentation specifically developed, tailored and updated for the clinic site proposed under the Contract has been provided for your review as part of this proposal.
Xxxxxx Xxxxx has provided for review, CBOC Management Services Compliance Plans Exhibit, included as a separate volume in a CD Rom to our technical proposal. Additionally, Xxxxxx Xxxxx has in place a corporate compliance plan that includes the following components, also detailed in our CBOC Compliance Plan CD-Rom, include: Conflict of Interest, Development and Distribution of Written Standards, Health and Safety, Competency Assessment, EOE Plan, VETS 100 Reporting & Drug-Free Workforce.
B.3 XXXXXX XXXXX WILL ENSURE CONTINUOUS COMMUNICATION WITH VA COORDINATOR
Xxxxxx Xxxxx proposes weekly telephone meetings accompanied by written reports including the following topics during the 90 day post award period and the initial 90 days of clinic operation, moved to monthly thereafter:
Credentialing Progress for all Provider and Staff Positions During Recruitment List of any or all vacancies of physicans and staff Incident reporting and problem resolution All other routine reporting mechanisms otherwise provided to the Hospital as part of Xxxxxx
Xxxxx’s regular monthly Quality Assurance, Access to Care and Workload Reporting Programs described in Section B.4 herein. Where feasible, early sampling of these monthly monitors will allow discernment of positive and/or negative trends at Clinic outset for early address in partnership with the Hospital.
Regarding general methods of problem resolution, it should be noted that a key management tool for coordinating Xxxxxx Xxxxx’s overall contract effort and its resolution of problems that might arise during the course of contract performance will be the mechanism of the CBOC management team meeting (the “Management Team Meeting”), to be scheduled at the convenience of the VA. The CBOC Management Team Meeting will provide a mechanism by which problems are brought to the attention of the Management
65
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
Team, so that such problems and concerns can be acknowledged and promptly addressed in the most appropriate manner.
A management team memo will summarize the key results of each CBOC Management Team Meeting, including problems/issues encountered, considerations evaluated, and resolutions adopted. The Management Team Memo will be distributed prior to the next week’s Management Team Meeting to all Management Team attendees. A complete archive of Management Team Memos will be retained for the entire course of contract performance at Xxxxxx Xxxxx’s corporate office.
In conclusion, resolution of problems, which arise under the proposed Contract, will be guided by a clear set of established policies and procedures. The regular input of the Government will be sought where appropriate in order to arrive at the best possible resolution for any problems, which may arise.
B.4. SPECIALIZED TRAINING AND CLINICAL STAFF MEETINGS AT VA HOSPITAL LEVEL
Xxxxxx Xxxxx will make its Providers and Staff available for specialized training opportunities and medical staff meetings as may be requested from time to time by the VA Long Beach Healthcare System. Xxxxxx Xxxxx has found that such participation by its CBOC Providers and specialty staff (e.g. RN Clinic Coordinator), as well as its Corporate Level Clinical Liaison personnel have been an invaluable coordination feature when available at the VA Medical Center level. As necessary, Xxxxxx Xxxxx will make available locum tenens and/or other backup personnel to ensure no interruption of regular clinic functions during the course of such Coordination events.
B.5. ENSURING OVERALL TIMELY DELIVERY OF SERVICES
Upon Contract award, Xxxxxx Xxxxx will establish a weekly meeting schedule with designated representatives of the VA to discuss both staffing/credentialing and facility updates. Further, there will be weekly telephonic post award meetings as well as one (1) or more in-person, with cognizant Xxxxxx Xxxxx and VA representatives at the NMVAHCS VAMC and/or proposed Taos CBOC site. Site visits are also coordinated and scheduled during these meetings to ensure that EOC and ADA requirements are met and that IT issues are addressed quickly during the rapid construction process to meet Clinic opening dates.
Prior to each weekly meeting, Xxxxxx Xxxxx constructs an update report, complete with construction progress photos to the VA team. Following the conclusion of each meeting, detailed notes and issues for the next week’s agenda are also captured. Any questions from the Xxxxxx Xxxxx or VA side are also included in this review.
B.5.A. XXXXXX XXXXX SITE READINESS CONTINGENCY PLAN
Xxxxxx Xxxxx recognizes the urgency and importance of meeting all readiness milestones in preparation for the opening day of services at the Taos facility. Because of this, Xxxxxx Xxxxx regularly utilizes construction contingency planning as part of the cost estimation process because there are unknown variables in any construction project such as the Taos facility. Xxxxxx Xxxxx’s construction management contingency (“CMC”) plan monitors and remedies any deviation from plan, stoppage or delay encountered during the buildout phase to ensure start up on the scheduled first day of services.
66
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
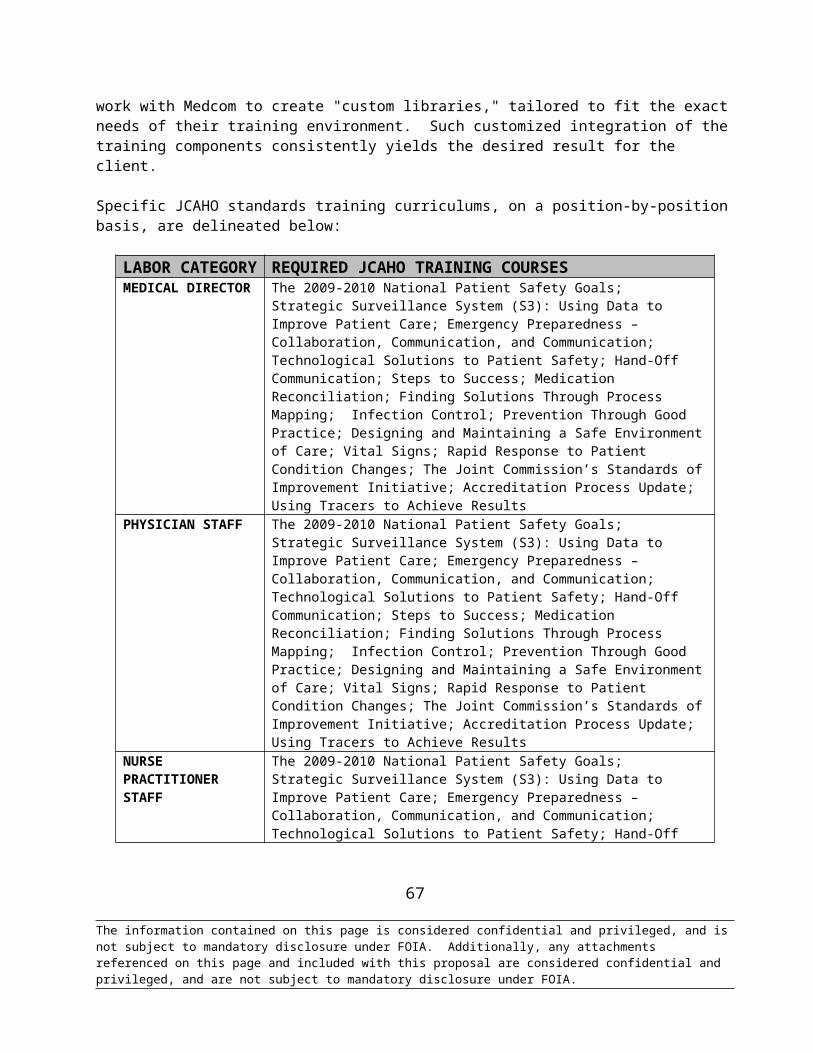
Crucial to our CMC plan is our retention of an independent construction consultant to provide construction/site readiness reports to Xxxxxx Xxxxx on a regular basis. These reports will be provided a minimum of six (6) times biweekly throughout the 90-day site readiness milestone timeline. The reports will include updates of every aspect of the ongoing project, photos of construction progress, and text including the number of days the project is on schedule (+/-).
Overtime and contingency budgets are employed with our local contractor. We will ensure that all goals and milestones are understood and agreed upon with our local contractors and what steps will be taken if failure to meet these goals becomes an issue. Reports to our independent contractor will be generated utilizing a weekly checklist system to be completed at least one day prior to each milestone event. Should any delay or interruption threaten the completion of the milestone event(s), an alternate contractor on retention will be contacted for completion of the particular entry on the timeline.
Construction Contingency Planning Steps
To avoid any delay in the 90-day milestone timeline, the following steps will be taken should there be any interruption to the established schedule:
Step Construction Contingency Action
1
On a weekly basis, the construction contractor will confirm the status of the ongoing timeline. Should there be any delay or interruption because of labor, lack of materials, permits etc. the contractor will notify the Xxxxxx Xxxxx Facility Team as soon as possible.
2A report of the delay or problem is generated and is evaluated by the team within 24 hours.
3
After ascertaining the length of delay a countdown clock begins. Facility team member will visit the site to supervise corrective actions until the timeline is restored. If not rectified or able to be rectified and back on schedule within 24 hours, an alternate or additional contractor will be brought in to bring the current section of the entire timeline back on schedule or to replace original contractor if necessary.
4The alternative contractor is contacted and work begins independent of original timeline. However, alternative has a shorter, different timeline to follow.
5Once the team ascertains project is complete and the schedule is on time, a report is generated certifying this.
6Subsequent actions may be taken to ensure there are no further delays in scheduling including updating the frequency of contractor check list reports.
7 Facility Team members resume the original timeline check procedures.
67
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
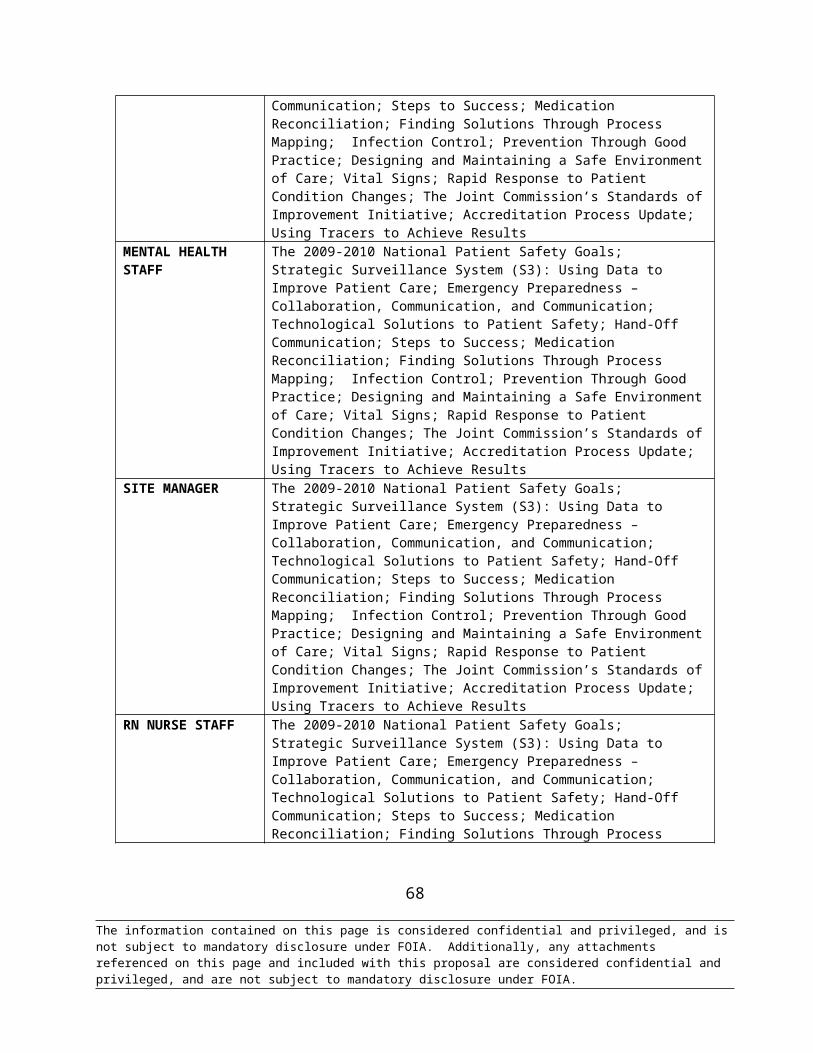
B.5.B. XXXXXX XXXXX’S PLAN TO ENSURE OVERALL TIMELY DELIVERY OF SERVICES FOR VA PATIENT CARE In order to demonstrate our capability to provide adequate, timely access for Veteran Patients’ care, we will describe our utilization of these principles: Working with the Veteran Affairs Medical Center (VAMC) to arrange initial scheduling; adherence to Veteran’s Health Administration (VHA) guidelines; and utilizing patient scheduling and tracking to ensure quality care.
B.5.C. SCHEDULING THE IMPLEMENTATION TEMPLATE WITH VAMC
Xxxxxx Xxxxx works with the parent VAMC to arrange the initial patient scheduling template. Typically, we utilize 30- or 60-minute appointments, depending on whether or not the patient is coming in as a new patient or "vesting" visit, or if the visit is for routine follow-up care.
B.5.D. XXXXXX XXXXX UNDERSTANDING OF VHA SCHEDULING GUIDELINES
Xxxxxx Xxxxx works with the parent VAMC facility to arrange the initial patient scheduling template. Typically we utilize 30 or 60 minute appointment, depending on whether or not the patient is coming in for a new patient or vesting visit, or if the visit is for routine follow-up care.
If the NMVAHCS intends to utilize ACA in the scheduling of the Taos CBOC over the coming Contract period, we are familiar and adept at the utilization of such scheduling modalities within the contractor managed VA CBOC environment.
Additionally, we recognize the Advanced Clinic Access (“ACA”) guidelines as established by the VHA. Key ACA Concepts include the following:
Shape the Demand Work Down the Backlog Reduce Demand Match Supply and Demand Understand Supply and Demand Reduce Appointment Types Optimize the Care Team Synchronize Patient, Provider, and Information Predict and Anticipate Patient Needs at Time of Appointment Optimize Rooms and Equipment Plan for Contingencies Redesign the System to Increase Supply Manage the Constraint
Clinic teams must have the knowledge and skill needed to do their work well and make changes successfully, as reflected in: seeking information and effectively using that information; using data regularly
68
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.

to design, test, and track process improvements; regularly assessing team progress; and learning from efforts of others to implement ACA.
Clinic staff members review ACA wait time performance data that is trustworthy and timely so that clinic teams providing care can assess the current level of the problem and monitor the impact of improvement efforts.
Adequate clinic resources, reflected in primary care by more exam rooms and in specialty care by greater use of consulting physicians.
Xxxxxx Xxxxx understands its obligations to comply with VHA scheduling guidelines that require maintaining an effective system of patient and staff scheduling ensuring that the clinic is properly staffed and patients are properly scheduled at all times. Particularly, Xxxxxx Xxxxx acknowledges and will meet or exceed the following standards set forth in the RFP:
To assure continuity of care for our patients, the following timelines will be adhered to when treating patients (Reference VHA Directive 2001-006, Veterans HealthCare Service Standards, dated February 7, 2001).
Patients will be seen within 20 minutes of scheduled appointment time Patients will have an appointment with a specialist, when referred from NMVAHCS within 30
days of referral New patients will be scheduled for their first primary care appointment within 30 days of the
patients’ desired date Action to make the first appointment will occur within 7 days of the appointment request Follow up appointments will occur within 30 days of the desired date. (VHA Directive 2006-
055, VHA Outpatient Scheduling Processes and Procedures)
B.5.E. TIMELINESS IN PATIENT ACCESS FROM CONTRACT OUTSET
1. Full complement of proposed staff will be hired, credentialed, oriented and trained using Xxxxxx Xxxxx’s proven practices for on-time start-up in all staff categories.
2. Beyond its careful attention to right-sizing the staff complement with timely additions to ensure patient access resources, the Taos CBOC Medical Director, Physician Director for Q1 and Xxxxxx Xxxxx Q1/QM activities performed throughout the Department will coordinate in assisting any CBOC Provider for whom the return patient utilization in excess of panel size appears to be at the root of a shortage in patient access, so that that provider may determine whether the higher utilization is for some reason patient population specific or may be appropriately curtailed through other approaches (e.g., utilization of Nurse Clinic visits for certain classes of return appointments).
3. All staff will be credentialed and processed with assistance from Xxxxxx Xxxxx to meet the rigorous 90-day timeline requirements. [Xxxxxx Xxxxx has three (3) full-time credential coordinators who work exclusively with providers entering VA CBOC programs, assisting them as they interface with the hospital’s VETPRO credentialing process in a timely manner.]
4. Beyond local VAMC provided orientation, Xxxxxx Xxxxx will provide orientation and Clinic launch
69
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
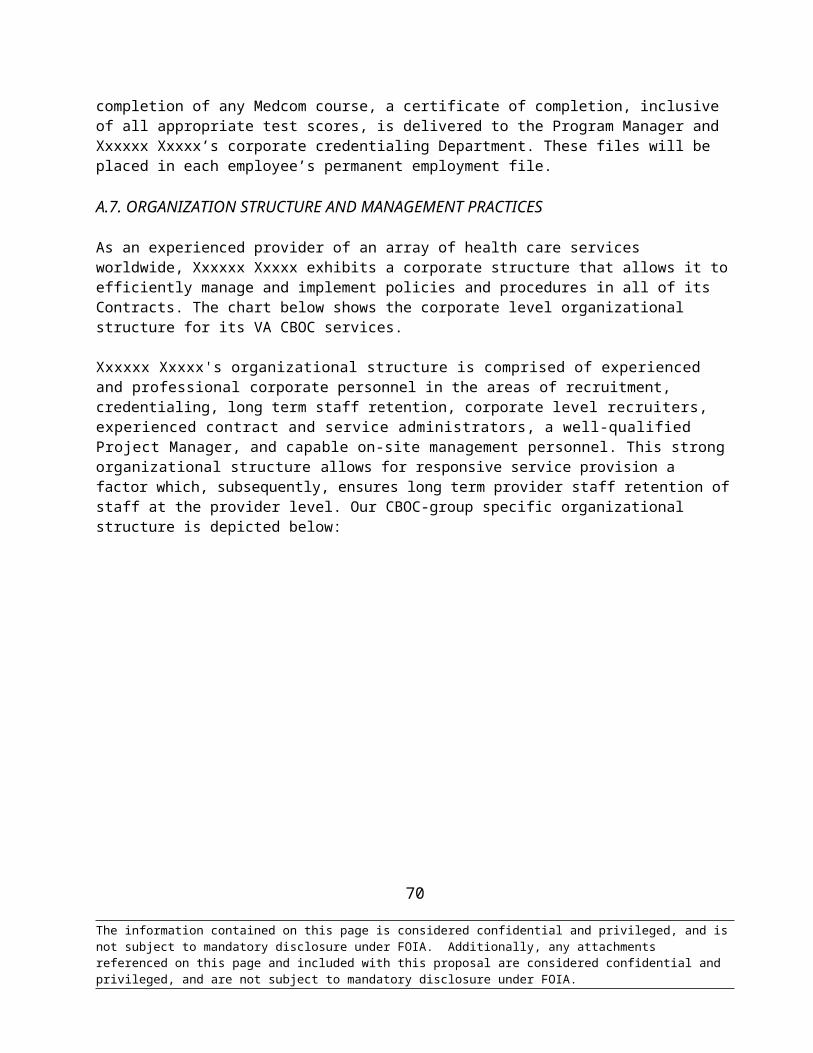
support of the Taos CBOC to include a minimum of two (2) experienced staff members in each CBOC position discipline on-site at the Taos CBOC for minimum of 30 days to assure smooth and timely ramp-up of patient appointments and corresponding access for existing and new patients over the initial 30 days of Clinic operation.
5. Xxxxxx Xxxxx will use its proven methods for timely launch, while assuring patient access, as it has for more than 35 CBOC start-ups since 1997, on behalf of the VA.
B.5.F. ADDITIONAL ACCESS WILL BE IMPLEMENTED FOR THE CLINIC WHEN NEEDED OVER THE CONTRACT TERM
The first order of business is to add additional appointment capability into the Clinic to ensure that patients can be seen.
If there is a clear, temporary only need (e.g., flu season), it may be met by existing providers adding extra shifts during extended hours or by adding a locum during the period of need.
If trends point to an ongoing need (e.g., patient numbers per provider is outgrowing appropriate panel size, or utilization is outgrowing expectation, such that expected panel size may not be obtainable) to add patient access appointment slots, recruitment for additional provider resources to be added to the Clinic will be activated.
Recommendations in the follow-up to alarm reports received at the Xxxxxx Xxxxx Management level on a weekly basis will be coupled with monthly formal reporting from the Taos CBOC Medical Director regarding access and availability of provider resources for ongoing reappraisal on a monthly basis, regarding the necessity for any new provider additions or reallocation of existing staff to better meet patient access and demands.
2. Alongside its careful attention to right-sizing the staff complement with timely additions to ensure patient access resources, the Taos CBOC Medical Director and Xxxxxx Xxxxx Q1/QM activities performed throughout the Department will coordinate in assisting any CBOC provider for whom the return patient utilization matrix in excess of panel size appears to be at root of a shortage in patient access, so that that provider may determine whether the higher utilization is for some reason patient population specific or may be appropriately curtailed through other approaches (e.g., utilization of nurse visiting the Clinic for certain classes of return appointments).
3. Attributes of Xxxxxx Xxxxx Clinic that will allow such access to be increased as necessary:
We have sized our initial CBOC Clinic foot-print so that all proposed Clinic providers can work concurrently in appropriate space efficient areas.
We will provide access during extended hours and Saturday hours as required by the VA as these appointments hours are genuinely sought by patients and will thus, in no way allow this to double as an explanation for having a Clinic facility with space limitations that counts on such extended hours in order to be right-sized to accommodate its provider panels. Xxxxxx Xxxxx’s intention in this regard is based upon the belief that a facility must be run at full capacity during the full range of permissible hours to accommodate the baseline requirement of patient quantities it has contracted
70
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
for as is in many cases rather than offering patients a choice of extended or daytime hours may actually just be asking them to fit in where an appointment is available.
Some extended hour appointments will be offered on an every week basis for the full Contract period, Monday through Friday, and Saturday hours a minimum of once per month. Patients will be given their choice of these opportunities like any other, and as Xxxxxx Xxxxx’s “alarm” resources are activated, pertinent access appointment hours in these extended hours Clinics will be responsively adjusted to be truly right-sized to patient demand rather than Xxxxxx Xxxxx or Xxxxxx Xxxxx provider preference.
Each patient will be seen by the attending provider within 20 minutes of his or her appointment time. This event is logged in a chart assigned to the provider and all entries are graphed by a Xxxxxx Xxxxx Representative as part of the monthly report presented to the VA.
Each provider who puts their own notes into CPRS and who reviews his/her alerts as well as review x-ray results will do so on a timely basis according to VA guidelines.
B.6. XXXXXX XXXXX’S CONTINGENCY PLAN FOR COMPUTER DOWNTIME
Xxxxxx Xxxxx has policies and procedures specific to the medical equipment utilized in our CBOC clinics, including steps the Clinic Manager will take to ensure that the clinic stays two (2) days ahead with paper records in the event of computer outage, paper will be utilized for notes and vital signs and that all patients will continue to be seen.
Computer system failure – As an alternative, paper version of the patients' charts will be used during any failure in the CBOC's computer system. In the event that any CBOC staff-member should experience computer difficulty, he/she will immediately notify the Clinic Manager or his/her designee for evaluation. Should the Clinic Manager or his/her designee determine that a system failure has occurred, he/she will direct all staff-members to implement the use of the paper versions of patients' charts. The use of the paper versions will continue until the Clinic Coordinator or his/her designee has officially informed the CBOC staff that the system is fully operational.
The CBOC Management Services Compliance Plans Exhibit, Part H: Medical Equipment Management Plan describes in detail the policies and procedures specific to medical equipment utilized in our CBOC clinics. This plan includes maintenance and inspection, equipment downtime, lock-out/tag-out procedures and equipment malfunctions, disruptions or failures.
The organization identifies and implements emergency procedures for responding to utility system disruptions or failures that address the following:
What to do if utility systems malfunction Identification of an alternative source of organization defined essential utilities Shutting off the malfunctioning systems and notifying staff in affected areas How and when to perform emergency clinical interventions when utility systems fail Obtaining repair services
71
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
Emergency procedures for utility systems disruptions or failures are as follows:
1. Procedures for utility systems malfunctions
a. Computer system failure — Paper versions of the patients' charts will be used during any failure of the computer system. The information recorded on paper will be entered into the computer once the system is functioning properly.
b. Power failure — Xxxxxx Xxxxx Program Office will be notified and the utility company will be contacted for timely resolution. In the event that power is unable to be restored in one (1) hour from the time of outage, the clinic will be closed, and the patients will be asked to reschedule their appointments. Should a medical emergency occur during a power outage, the patient will be referred to the VA hospital or, if necessary, the local community hospital.
* Note: Organizations may use different strategies as appropriate. For example, strategies such as predictive maintenance, interval-based inspections, corrective maintenance, or metered maintenance may be selected to ensure reliable performance.
c. Water system failure – The Clinic Coordinator or his/her designee will contact the appropriate local company for timely resolution and notify the Xxxxxx Xxxxx Program Office and the hospital.
d. Telephone system failure –In the event of a telephone system failure, the Clinic Coordinator or his/her designee will contact the appropriate local company for timely resolution.
e. Heating/air conditioning system failure – The Clinic Coordinator or his/her designee will contact the appropriate local company for timely resolution and notify the Xxxxxx Xxxxx Program Office and the hospital. If the temperature in the clinic drops below 66 degrees in the winter or rises above 80 degrees in the summer, the clinic will be closed until the problem has been resolved and the temperature in the clinic is within proper parameters.
2. Computer system failure – As an alternative, paper version of the patients' charts will be used during any failure in the CBOC's computer system.
Power failure – In the event of a power outage, emergency lighting will automatically become operational.
Water system failure – As an alternative, CBOC staff will use hand sanitizer that does not require the use of water to ensure infection control and decontamination during water system failure.
Telephone system failure –In the event of a telephone system failure, the Clinic Coordinator or his/her designee will contact the appropriate local company for timely resolution, and notify the Xxxxxx Xxxxx Program Office and the hospital.
72
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.

Heating/air conditioning system failure – In the event of a heating/air conditioning system failure, the Clinic Coordinator or his/her designee will contact the appropriate local company for timely resolution and notify the Xxxxxx Xxxxx Program Office and the hospital. If the CBOC's temperature exceeds established parameters, the clinic will be closed until the problem is resolved.
3. The Clinic Coordinator is responsible for assessing the malfunction of any utility system. If the Clinic Coordinator or his/her designee determines that an emergency has arisen and a utility system must be shut down, he/she will immediately contact the appropriate local company for direction. Once the situation is controlled, the Clinic Coordinator or his/her designee will notify the Xxxxxx Xxxxx Program Office and the hospital.
4. In the event of any utility system failure, the Clinic Coordinator or his/her designee will contact the appropriate local company for timely resolution.
a. Computer system failure – In the event that any CBOC staff-member should experience computer difficulty, he/she will immediately notify the Clinic Coordinator or his/her designee for evaluation. Should the Clinic Coordinator or his/her designee determine that a system failure has occurred, he/she will direct all staff-members to implement the use of the paper versions of patients' charts. The use of the paper versions will continue until the Clinic Coordinator or his/her designee has officially informed the CBOC staff that the system is fully operational.
b. Power failure – The failure of this utility system will be evident to all CBOC staff-members. Should this failure occur, emergency lighting would automatically become operational. If power is not restored within one (1) hour, the clinic will be closed until power is restored. In the event that there are patients in the clinic at the time of the outage, CBOC staff will, if necessary, ensure the patients' safety by escorting them to a well-lit area. If the power is not restored and the clinic must close, CBOC staff will, if necessary, ensure that patients safely exit the building.
c. Water system failure – In the event that any CBOC staff-member suspects that the water supply to the clinic has been compromised, he/she should immediately notify the Clinic Coordinator or his/her designee for evaluation. The Clinic Coordinator or his/her designee will inform the CBOC staff of any failure in the water system and take appropriate measures to ensure resolution of the problem. Upon notification of such failure, it is the responsibility of each CBOC staff-member to ensure infection control and decontamination via alternative means of sanitization (i.e., hand sanitizer that does not require the use of water).
d. Telephone system failure –In the event of a telephone system failure, the Clinic Coordinator or his/her designee will contact the appropriate local company for timely resolution, and notify the Xxxxxx Xxxxx Program Office and the hospital.
e. Heating/air conditioning system failure – In the event that any CBOC staff-member suspects the failure of the heating/air conditioning system, he/she should immediately notify the Clinic Coordinator or his/her designee for evaluation. Should the Clinic Coordinator or his/her designee determine that a failure has occurred, he/she will contact the appropriate local
73
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
company for resolution. The Clinic Coordinator or his/her designee will continue to monitor the temperature in the clinic. If the parameters are breached, the CBOC will be closed until the problem is resolved.
As part of our computer contingency plan, should the T1 connection fail, Xxxxxx Xxxxx will utilize its monthly 5 Mb internet connection with backup providers to utilize a VPN connection with VA-supplied laptops.
<THIS SPACE INTENTIONALL LEFT BLANK>
74
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.

C. PAST PERFORMANCE
Below, please find a list of representative current Community Based Outpatient Clinics (CBOC) contracts. Services at these locations are highly germane to the performance of service under the instant proposal for CBOC services at Taos, New Mexico.
Jamestown, NY CBOCVA528-P-0492
Contracting Office:
Contracting Officer: Program Manager/COTR: POP: Contract Value:
VA Western New York Healthcare System (VAWNYHS)Buffalo VA Medical Center3495 Bailey AvenueBuffalo, NY 14215Xxxxxx,Xxxxx 716-XXX-XXXXXxxxx Xxxxxx, 716-XXX-XXXX3/2/09-3/1/2014$4,997,786.25
Schenectady, NY CBOCVA-528-08-RP-0013
Contracting Office:
Contracting Officer: Program Manager/COTR: POP:
Contract Value:
Albany VA Medical Center113 Holland AvenueAlbany, NY 12208Xxxxx Xxxxx, 716-XXX-XXXXXxx Xxxxxxx, COTR, 518-XXX-XXXX10/1/03 -1/31/08 and 1/1/08-12/31/12 (+ Contract Renewal)$3,836,999
LaGrange TX CBOCVA257-P-0340
Contracting Office:
Contracting Officer: Program Manager/COTR: POP: Contract Value:
Department of Veterans Affairs, Olin E. Teague Medical Center1901 Veterans Memorial DriveTemple, TX 76504Xxxxx Xxxxxxx, 254-XXX-XXXXXxxxxx Xxxx, COTR 254-XXX-XXXX 6/2009-6/2012$1,839,912
Imperial Valley, CA CBOCVA-262-07-RP-0049
Contracting Office:
Contracting Officer: Program Manager/COTR: POP: Contract Value:
Network 22 Logistics Office5901 East 7th StreetLong Beach, CA 90822Xxxx Xxxxx, 619-XXX-XXXXXxxxx Xxxxxx, (562) XXX-XXXX6/1/2008-5/31/2013$3,836,999 (not inclusive of mental health expansion in progress)
75
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
South Sound WA CBOCVA260-P-0643
Contracting Office:
Contracting Officer: Program Manager/COTR: POP: Contract Value:
VA Puget Sound Healthcare System9600 Veterans Drive, Bldg 17Tacoma, WA 98493Xxxxxx Xxxx, 253-XXX-XXXXXxxxx Xxxxxx, 206-XXX-XXXX5/1/10 – 4/30/15$23,684,232.00
Mankato/St. James, MN CBOCVA260-P-0643
Contracting Office:
Contracting Officer: Program Manager/COTR: POP: Contract Value:
VA Midwest Healthcare System708 S. Third St., Suite 200EMinneapolis, MN 55415Xxxxxxx Xxxx, 612-XXX-XXXXXxxxx Xxxxxxx, 612-XXX-XXXX12/8/10 – 9/30/15$10,681,508.92
Washington, PA CBOCV244P-00580
Contracting Office:
Contracting Officer: Program Manager/COTR: POP:
Contract Value:
VA Pittsburgh Healthcare System University Drive Pittsburgh, PA 15240Xxxxx Xxxxxxx, 412-XXX-XXXXXxxxxx Xxxxxxxx, 412-XXX-XXXXWashington CBOC opened in 2001-(see Uniontown below)$2,059,864 (Base year value for both clinics)
Uniontown, PA CBOCV244P-00580
Contracting Office:
Contracting Officer: Program Manager/COTR: POP:
Contract Value:
VA Pittsburgh Healthcare System University Drive Pittsburgh, PA 15240Xxxxx Xxxxxx, 412-XXX-XXXXXxxxxx Xxxxxxx, 412-XXX-XXXXUniontown opened in 2005 under joint j.v. contract for Washington PA, referenced above (in current extension)$2,059,864 (Base year value for both clinics)
McKean County, PA CBOCVA244-P-0837
Contracting Office:
Contracting Officer: Program Manager/COTR: POP:
Department of Veteran Affairs, ERIE VAMC135 East 38th Street BoulevardErie, PA 16504Xxxxx Xxxx, 814-XXX-XXXXXxxxxx Xxxxxxxx, COTR 814-XXX-XXXX6/1/2009-5/31/2014
76
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
Contract Value: $3,588,345.62Bolivar TN CBOC
VA-249-P-0499Contracting Office:
Contracting Officer: Program Manager/COTR: POP: Contract Value:
Department of Veterans AffairsVISN 9; 3400 Lebanon Pike Murfreesboro TN 37129 Xxxxx Xxxxx, 616-XXX-XXXX Xxxxx Xxxxx, 615-XXX-XXXX7/1/2009-6/30/2014$6,008,081.41
<THIS SPACE INTENTIONALLY LEFT BLANK>
77
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
D. SOCIAL ECONOMIC CONSIDERATION
Xxxxxx Xxxxx plans to incorporate Service-Disabled Veteran Owned Businesses (SDVOSB), Veteran Owned Small Businesses (VOSB) and other small disadvantaged businesses into our small business subcontracting plan, which is described in greater detail in the Administrative/Costing Volume of this proposal. One example of an SDVOSB that Xxxxxx Xxxxx intends to utilize is Medical Staffing Solutions, a Service-disabled Veteran-Owned, Woman-Owned Small Disadvantaged Business that provides the medical community with a source of experienced, dedicated, high-quality medical professionals that are accessible and available for any shift.
Founded in 1999 by Teresa Xxxxxxx, a service-disabled veteran, Medical Staffing Solutions is a medical staffing firm that has received SBA 8(a), SBA Small Disadvantaged Business (SDB) and HUBZone certifications. Medical Staffing Solutions’ familiarity with the military community and its medical background give it a unique insight that facilitates the identification and procurement of highly qualified medical professionals. Medical Staffing Solutions provides medical staff members that adhere to national standards established by the Joint Commission on Accreditation of Healthcare Organization (JCAHO), American Hospital Association (AHA), American Medical Association (AMA), American Association of Nurse Anesthetist (AANA), Department of Defense (DoD), and Army Medical Department, as well as the established principles and ethics of the medical profession. Positions provided include Registered Nurses, Licensed Vocational/Practical Nurses, Advanced Practice Nurses (Nurse Anesthetists, Nurse Practitioners, Nurse Midwives), Physicians, Dentists, Podiatrists, Optometrists and ancillary staff.
For over ten years, Teresa A. Xxxxxxx has been providing nursing services to the military community. During the last four of her 10 plus years of military service, Ms. Xxxxxxx provided nurse anesthesia services for Carl R. Xxxxxx Army Medical Center (CRDAMC) in Fort Hood, Texas. In 1997, she left active duty but continued providing (CRDAMC) with obstetrical anesthesia services. Realizing the growing need for quality medical professionals, she founded Teresa A. Xxxxxxx P.C. in 1999. In June 2003, Teresa A. Xxxxxxx P.C. received the Small Business Administration 8(a) certification and began implementing plans to expand and improve the accessibility of nurses to hospitals and medical facilities. A military veteran as well as a seasoned veteran in the medical community, Ms. Xxxxxxx holds a Bachelor of Science in Nursing (BSN) and a Masters in Health Services (MHS). Certified in Critical Care Nursing and as a nurse anesthetist, Ms Xxxxxxx is also an active member of the America Association of Nurse Anesthetists.
Xxxxxx Xxxxx has incorporated into their subcontracting plan fixed percentage amount of 10% for both SDVOSB and VOSB. Xxxxxx Xxxxx anticipates Medical Staffing Solutions will perform staffing services for the positions of Medical Clerks and/or Medical Assistants at the proposed Taos CBOC under this subcontract plan on behalf of Xxxxxx Xxxxx.
<THIS SPACE INTENTIONALLY LEFT BLANK>
78
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.

E. QUALITY ASSURANCE PLAN
E.1. XXXXXX XXXXX’S APPROACH TOWARDS QUALITY ASSURANCE
This section describes the performance measures which Xxxxxx Xxxxx will implement in order to monitor quality, appropriateness of care, access, JCAHO/ Regulatory compliance, VA standards of documentation, workload reporting and patient satisfaction.
E.1.A. QUALITY ASSURANCE COLLECTION AND REPORTING METHODS
On-site administrative/supervisory staff will participate in corporate-wide monthly meetings, medical staff meetings for Providers (including Medical Director) and on-site manager meetings between the on-site RN Clinic Coordinator and the corporate management team. The Medical Director will also participate in monthly Provider medical staff meetings with the corporate Medical Director, coordinated by our corporate-level QA/JCAHO Preparedness Coordinator.
The RN Clinic Coordinator will participate in monthly meetings with corporate management staff represented by the QA/JCAHO Preparedness Coordinator, VA CBOC Clinical Liaison, VA CBOC Hospital Liaison and the VA CBOC services HR Liaison.
The results of meetings, including issues identified, and proposed resolutions will be addressed among members of corporate management structure. These will become the topics for the weekly management team meetings described in our Proposal.
Monthly meetings are also held if agreed to by the VA, between Xxxxxx Xxxxx’s VA CBOC Program Manager, VA Hospital Liaison and designated VAMC hospital representatives to discuss any ongoing clinical or administrative issues under this contract. Such information and outcomes from above meetings will also be reported in the monthly contracting report furnished to the VA.
A sample Quality Assurance memorandum is included as ATTACHMENT B.
E.1.B. XXXXXX XXXXX’S PATIENT ADVOCACY PROGRAM
In addition to the above patient satisfaction processes, Xxxxxx Xxxxx employs a Patient Advocacy Program.
Xxxxxx Xxxxx’s Patient Advocacy Program is a program designed to augment the Veteran Community’s patient satisfaction by directing feedback to a designated Patient Advocate. Xxxxxx Xxxxx’s Patient Advocacy Program has been developed to compliment the VA’s Patient Advocacy Program and Patient Bill of Rights. Xxxxxx Xxxxx’s corporate office employs a full-time Patient Advocate to address patient issues and concerns.
The waiting area of the Taos CBOC will prominently display a large sign providing information on this program that will include basic patient rights set forth by VHA guidelines and the toll-free number for Xxxxxx Xxxxx’s Patient Advocate. Xxxxxx Xxxxx’s corporate Patient Advocate will coordinate with the Taos CBOC staff person designated as the representative for patient advocacy in utilization of the Depart of Veterans Affairs Patient Advocate Tracking Package to log and report complaints and resolution. This two
79
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.

track portal for Taos veteran patient issues will ensure that all concerns are efficiently and effectively addressed.
Taos CBOC Patient satisfaction surveys will comply with VA standards and adhere to the principles of item consistency, survey design and sampling methods. Information obtained from surveys will be a valuable component of feedback that will be integrated into the Taos CBOC Quality Management/Improvement process. Survey results will be disseminated throughout the organization so that they can be incorporated into process improvement efforts.
Most notably, Xxxxxx Xxxxx will only institute this Patient Advocacy Program within the Taos CBOC if given specific approval from the RLR VAMC.
By adhering to the above described Patient Advocacy Program, Xxxxxx Xxxxx will be both aware and attentive to the Veteran Community’s satisfaction. Below, please find a photograph depicting Xxxxxx Xxxxx’s Patient Advocacy poster which, upon VA approval, will be displayed in the Taos, IN CBOC:
80
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
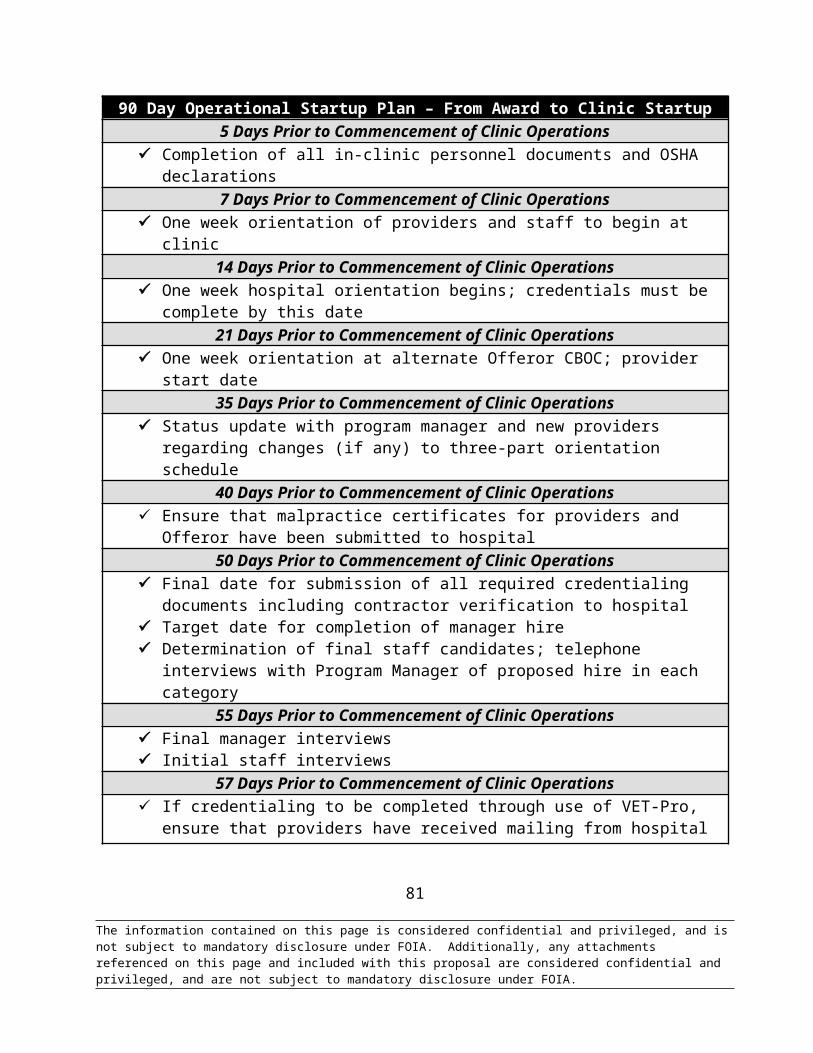
E.2. PERFORMANCE MEASURES AND PIP PROCESS USED IN ONGOING MANAGEMENT OF STAFFING PROGRAM
E.2.A. HEIDIS COMPLIANCE
HEDIS is a tool used by more than 90 percent of America's health plans to measure performance on important dimensions of care and service. Altogether, HEDIS consists of 71 measures across 8 domains of care. Because so many plans collect HEDIS data, and because the measures are so specifically defined, HEDIS makes it possible to compare the performance of health plans on an "apples-to-apples" basis. Health plans also use HEDIS results themselves to see where they need to focus their improvement efforts.
HEDIS measures address a broad range of important health issues. Among them are the following:
Asthma medication use. Persistence of beta-block use after a heart attack. Controlling high-blood pressure. Comprehensive diabetes care. Breast cancer screening. Antidepressant medication management. Advising smokers to quit.
The above measures are incorporated into our Quality Managment program, as the above are included under VHA Clinical Practice Guidelines and the VHA clinical reminders that are informed by them. Compliance with clinical reminders regarding the above, as well as all nationally directed VHA clinical reminders, as well as those that may be implemented at the RLR VAMC Director level, that will be required of Taos CBOC providers and staff are monitored ongoingly for quality improvement by our Quality Managment Department.
Xxxxxx Xxxxx is also experienced at meeting or exceeding specific requirements set forth by the parent VAMCs of each CBOC Xxxxxx Xxxxx operates. These site-specific requirements are sometimes even more stringent than VHA guidelines and they often come with penalties for non-compliance. Xxxxxx Xxxxx will incorporate the programs discussed below if the VA feels that they are necessary additions to our existing compliance policies and monitoring procedures.
The table below includes the VHA measures that Xxxxxx Xxxxx adheres to in all of its clinics as well as individual methods implemented to monitor or ensure those measures are met:
Measure or Goal: CVD - Out pt LDL-C <100 Action: Patients will be screened for elevated LDL. Patients with elevated LDL > 100 will be aggressively treated with medication, referred to Dietician for nutrition education and will have repeat labs as Provider orders (preferably every 3 months until patient is at goal).Measure or Goal: CA - Breast Screen Age 50-69 Action: All female veterans will be offered annual mammography. If the patient chooses to use outside Providers, then copies of the reports will be requested from the outside source, documented in the electronic record and scanned into the record. A log of all female veterans will be kept in the clinic to ensure records are received.
81
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
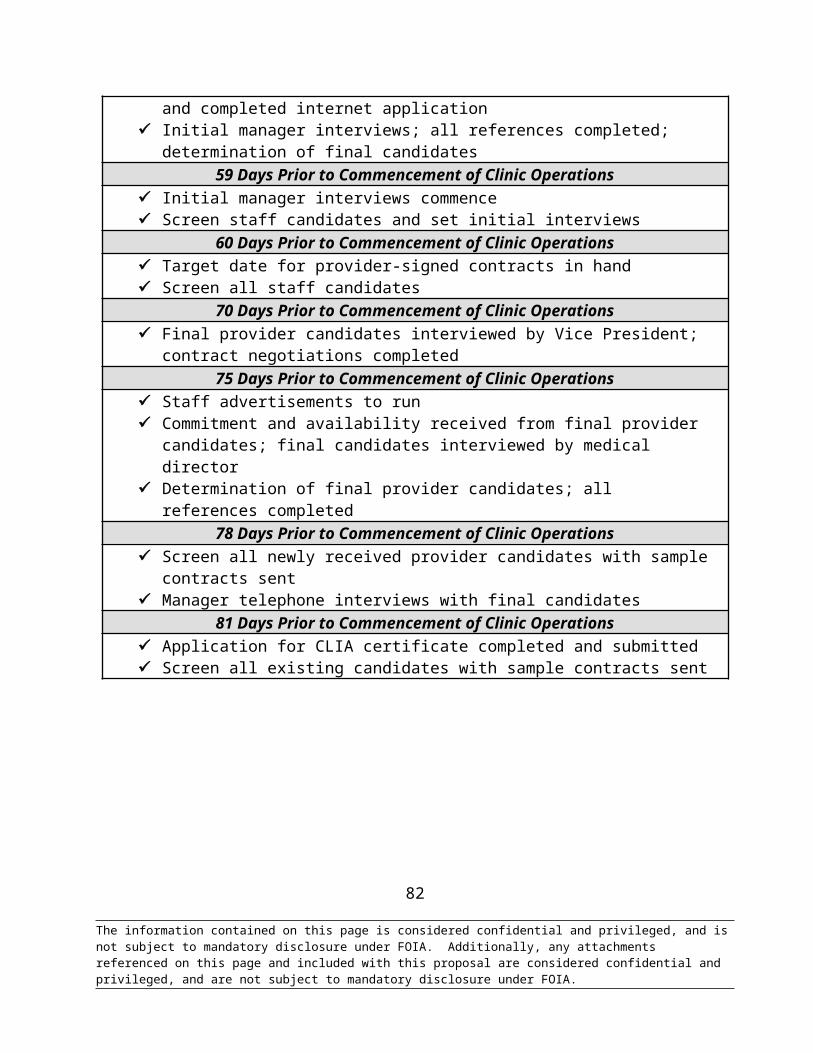
Measure or Goal: CA - Cervical Screen Action: All female veterans will be offered annual pap screening. If the veteran chooses to use outside Providers copies of the reports will be requested from the outside source, documented in the electronic record and scanned into the record. A log of all female veterans will be kept in the clinic to ensure records are received.Measure or Goal: CA - Colorectal Screen Age 50-75 Action: All veterans will asked to complete 3 FOBT cards yearly or offered screening colonoscopies. A log will be kept for all FOBT cards that are given to patients and a follow-up call will be made to the veteran until the cards are returned.Measure or Goal: DM - Outpt HbA1c Annual Action: All patients with a diagnosis of DM will have annual HgBA1c. If the patient prefers to use private outside Providers, then the patient will be asked to provide copies of the outside labs to be entered and scanned into the electronic medical record.Measure or Goal: DM Out - HbA1>9 or not done Action: All patients with a diagnosis of DM will have annual HgBA1c. If the patient prefers to use private outside Providers, then the patient will be asked to provide copies of the outside labs to be entered and scanned into the electronic medical record. Patients exhibiting A1c > 9 will be aggressively treated and referred to the Dietician for nutrition management. Labs will be followed every 3 months until A1c is controlled.Measure or Goal: DM - Outpt-LDL-C < 100 Action: Patients will be screened for elevated LDL. Patients exhibiting elevated LDL > 100 will be aggressively treated with medication; referred to a Dietician for nutrition education and will have repeat labs as Provider orders (preferably every 3 months until patient is at goal).Measure or Goal: DM - Outpt - BP <140/90 Action: CBOC nurse will take the patient’s vital signs. If the BP is above goal, the blood pressure will be repeated and documented, if the BP is still above goal prior to the patient leaving the clinic, then nurse will perform an exit interview and the BP will be repeated again. If the Provider does not change medication or if the Provider increases medication the patient will be asked to return for a nursing clinic visit for follow-up on blood pressure.Measure or Goal: Tobacco Users: Advice to Quit Action: All patients using tobacco products will receive counseling and encouragement to stop. Medication will be offered. If patient is agreeable, he/she will be referred to any applicable VA smoking cessation program available.Measure or Goal and Action: Tobacco Users: Offered Referral to Smoking Cessation - see above
To ensure these measures are met, we will utilize the VA’s electronic clinical reminder system which is used in CPRS for every patient. The clinical reminders provide prompts when applicable to provide electronic assistance to VA providers in the accomplishment of these tasks. Addition medical judgment is utilized by Xxxxxx Xxxxx providers to ensure these performance measurements are met. Electronic tabulation of data is then accessed by the offeror’s medical and administration staff utilizing the VA’s VistA reporting system in the course of its monthly quality assurance reporting process. The data in these key clinical reminders is tracked by individual Xxxxxx Xxxxx providers for performance within acceptable target range. Trending for continual improvement of all performance including performance in the ‘acceptable’ range is a goal sought of all Xxxxxx Xxxxx providers. Results of Xxxxxx Xxxxx‘s findings of performance measures as well as trending data are presented to the hospital on a monthly and/or quarterly basis at hospital preference, all as part of its quality assurance program.
82
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
Any instance of Performance outside of Acceptable Measure range will be accompanied by Performance Improvement Plan (PIP) at the Provider level. Such PIP will accompany monthly QA reporting to the Hospital. In addition to specific Performance outside of Acceptable Measure range, instances of negative trend in Performance is otherwise within the noted Acceptable Measure range will also be subject for PIP plan completion. PIP compliance will accordingly be tracked as part of ongoing QA reporting documented on a monthly basis.
Provider and Staff Performance, as measured under the QA Program, will form an important element of staff appraisal, as used for compensation review, contract incumbent retention and job advancement purposes.
Any instance of significant aberrancy from Acceptable Range in measured Performance through the Xxxxxx Xxxxx QA Program will result in counseling of Provider or Staff member. Counseling will be performed as appropriate by: Xxxxxx Xxxxx CBOC Physician Consultant(s), Xxxxxx Xxxxx HR Liaison, Xxxxxx Xxxxx CBOC Director of Operation. All such counseling will result in a formal letter to the Provider/Staff member file, and follow-up action as applicable.
E.2.B. ACCESS TO CARE REPORTING
Collection & Reporting Taos CBOC Veteran Patient Satisfaction - Xxxxxx Xxxxx will utilize a variety of tools to capture data related to customer satisfaction- both from the Government client and the patients served. The frequency of our request for this feedback from patients will be dependent in part on the performance data received from the parent VAMC hospital. On at least a quarterly basis we will send out surveys to Taos CBOC patients. The Quality Improvement Department, located at our corporate headquarters, will collect data from Taos CBOC patients via surveys, from surveys issued by the VA healthcare network and from calls made to our Patient Advocacy Program (discussed later in this section). Every patient complaint will be carefully documented and provided to a member of our CBOC Services Management Team of our corporate office for review and follow-up. Outcomes of this process will be provided in the contractor reporting to the VAMC as requested.
Xxxxxx Xxxxx also will welcome VAGLAHS staff to conduct random customer satisfaction surveys concerning appointment availability, office waiting times and other care coordination and customer service topics. Xxxxxx Xxxxx acknowledges that the VAGLAHS reserves the right to make random, unannounced visits to the Taos CBOC to review medical and other patient-related records, Clinic operations and processes. The Taos CBOC will permit the performance of a survey at the discretion of the Joint Commission.
Xxxxxx Xxxxx will have a wall-mounted suggestion box in the Taos Clinic that is accessible only by management personnel. This will allow veterans and/or their caregivers to make suggestions, provide compliments or simply offer comments with or without identifying themselves by name. These cards will be processed and reviewed only by corporate management Quality Improvement team members. One of the most critical patient issues is access to care - a large factor in patient satisfaction. In order to ensure Taos CBOC veteran patient satisfaction, timely access to care will be provided to patients in accordance with VA policy. To ensure compliance with the requirements set forth by the VHA Patient
83
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.

Advocacy Program and to further provide for timely access to care, a daily reporting form will be used to track Taos CBOC patient visits and enrollments.
The VA Clinic Daily Patient Access to Care Visit Snapshot tracks statistics such as new patient visits, annual visits, triage visits, no-shows, total patients per day, cancellations, and rescheduled appointments. It also allows for clerks or other staff members to insert comments about patient scheduling issues. Finally, and most importantly in regard to meeting access to care standards, this form automatically generates "alarms" to indicate patient wait times for scheduling with primary care providers, mental health services, dieticians or other specialty providers. This "alarm" section has been inserted below:
New Patient> 14 Days
Patient Waiting >7 days
Patient Waiting >14 MH Appt.
Patient Waiting >14 for Dietician Appt.
Patient Waiting >14 days for Podiatry Appt.
The completed VA CLINIC DAILY PATIENT VISIT SNAPSHOT, with the included "alarm" section above, is sent electronically on a daily basis to Xxxxxx Xxxxx CBOC Management Team, Xxxxxx Xxxxx Corporate QA Office and the CBOC Clinical Liaison. Data from this sheet is incorporated into our monthly QM/I tracking form utilized to track compliance with access requirements for all CBOC clinics and may be included in our monthly QM/I reporting to the hospital at its request. This allows Provider to patient ratios to be adjusted using actual access measures rather than simply relying upon straight numeric panel numbers to assess appropriate maximum workloads in terms of total patient responsibility for individual provider-staff teams.
Such access to care reporting information is provided to Xxxxxx Xxxxx CBOC VA Clients on a monthly, weekly or daily basis at the request and preference of the individual VA Hospital client. If such reporting is requested on a monthly only basis, access measures by individual provider will be included within the regular monthly quality assurance reporting to the hospital rather than a separate Access to Care report.
In order to ensure compliance with the requirements set forth by the VHA Access to Care directives and to further provide for timely access to care, a daily reporting form is used to track patient visits and enrollments at each clinic.
Data collected using this process is used to quickly identify access issues BEFORE the 7 or 14 day waiting limit is reached. Clinic managers review access data and notes weekly to determine needs and trends among all CBOC facilities managed by Xxxxxx Xxxxx. For example, temporary "surges" in patient visits (such as during flu season), can be addressed through a variety of means including an arrangement with primary care providers to move administrative time to a later hour and allow for more patient appointments during either the early morning or late afternoon/early evening time slot. Finally, it also may be used to fine tune provider panels to the individual provider staff teams.
Other trends might reveal steadily increasing clinic utilization and patient enrollment beyond the figures initially projected by the VA for option years. Our reporting mechanism allows us to identify and track such a trend and make staffing adjustments in collaboration with the VA to ensure timely access to care for all veterans. Another possibility, when permitted and approved by the VA, is the addition of extended evening Monday-Thursday hours to meet both temporary and long-term demands for primary care services.
84
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
E.2.C. QUALITY
As an experienced provider of healthcare services to the government that include CBOC management services since 1997, Xxxxxx Xxxxx is well-versed in Joint Commission (“JCAHO”) Standards, VHA and VISN Quality and Performance Measure Standards. Xxxxxx Xxxxx will follow applicable RLR VAMC policies and procedures, fully participating in the RLR VAMC’s Quality Monitoring/Performance Improvement Program. Xxxxxx Xxxxx will meet or exceed the aforementioned standards in the execution of this Contract, throughout the Contract term. Additionally, Xxxxxx Xxxxx will comply with all applicable privacy and confidentiality statutes and regulations of the HIPAA: Health Insurance Portability and Accountability Act.
The care delivered to the veterans will reflect the RLR VAMC mission, vision and core values. High priority will be given by Xxxxxx Xxxxx to the prevention of risk for the veteran. Xxxxxx Xxxxx will provide professional and compassionate care with respect for the special needs of the veteran population served at the Taos, New Mexico CBOC.
Throughout this section of our technical proposal, Xxxxxx Xxxxx will demonstrate an understanding of the Solicitation’s necessitated attention to customer service awareness and response, particularly with regards to VAMC standards and Veteran needs, and our subsequent ability to monitor the quality of service conferred upon both VA and Veteran customers. This delineation is provided below.
E.2.C.I. XXXXXX XXXXX’S OVERALL APPROACH TO QUALITY MANAGEMENT/IMPROVEMENT
Xxxxxx Xxxxx’s Quality Management/Improvement Program (“QM/I”) will be instituted and maintained throughout the period of Contract performance, including options, renewals, and extensions. Xxxxxx Xxxxx’s goal is to maintain the highest level of service personnel and delivery possible, focusing on compliance with and monitoring of VA directives/policies and JCAHO requirements and plans. Xxxxxx Xxxxx recognizes, though, that it must not only strive to provide the Government with quality personnel, it must also have the ability to self-monitor and self-regulate all that it employs. The successful offeror, then, must be able to effectively communicate with both its own employees and the Government. Clinical Coordinators will actively engage in the improvement, monitoring, and reporting of Quality Management/Improvement.
Information regarding Xxxxxx Xxxxx’s JCAHO compliance can be found in the Compliance Plan entitled “Xxxxxx Xxxxx Compliance Plan CD-ROM” with this Proposal. A summary of the Compliance Plan Components is included for convenience as ATTACHMENT C.
As represented in the following sections, Xxxxxx Xxxxx acknowledges that it is absolutely crucial that the offeror presents an understanding of the requirements as set forth in the Solicitation. For an instituted Quality Management/Improvement Program to be effective, the successful offeror must be able to demonstrate competency in the Government’s stated needs. All information, therefore, will be included in our Quality Assurance Report (monthly contracting report) provided to the VA, as well as to the corporate CBOC Management Team. Quality Management/Improvement meetings include numerous key clinic members, on-site administrative/supervisory staff and the corporate management team to ensure that all issues are identified and proposed resolutions are carried out efficiently and demonstratively.
85
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
E.2.C.II TAOS CBOC QUALITY MANAGEMENT/IMPROVEMENT DIRECTIVES
The Xxxxxx Xxxxx QM/I program, as conformed to the preferences and requirements of the particular VAMC, in this instance the RLR VAMC, will begin by tracking those measures identified as most important to that Medical Center. Accordingly, Xxxxxx Xxxxx, as directed by on Pg. 38 of the Solicitation, will conform its Taos CBOC QM/I Program to specifically track the following areas:
Patient or family complaints Referral rates Appointment availability and waiting times Panel Size or Visits per Clinician per day Formulary compliance Prescription writing patterns Volume of laboratory tests Identification of high acuity, high frequency users
Upon Contract commencement, Xxxxxx Xxxxx will hold all employees providing services at the Taos, IN CBOC to the highest possible standard. Specifically, Xxxxxx Xxxxx employees will be responsible for maintaining performance measure scores at a performance measure standard at 100% or greater of the median level of RLR VAMC Primary Care Providers for that measure.
For any measure for which the Taos, IN CBOC should falls below this Xxxxxx Xxxxx standard, Xxxxxx Xxxxx’s CBOC Management Team will conduct an internal audit, which will involve interview and counseling as appropriate at the provider level and the creation of a Performance Improvement Plan (“PIP”). The PIP will be submitted to both the VAMC and Xxxxxx Xxxxx’s corporate headquarters, regardless of whether the VAMC’s standards or targets relating to an individual measure may have still been met. This proactive approach will ensure Xxxxxx Xxxxx’s compliance with VAMC directives, thus ensuring the RLR VAMC’s satisfaction.
E.2.C.III. STANDARD XXXXXX XXXXX QUALITY MANAGEMENT/ IMPROVEMENT PROGRAM
In addition to any listed above, the Xxxxxx Xxxxx QM/I program, based on the preferences of its range of clients at Medical Centers and/or CBOC professional staff, consistently tracks:
Clinical Reminders due and trending of quantitative compliance by provider Credentialing/Re-credentialing of Providers. Availability of Veterans Rights and Responsibilities information Waits and Delays Electronic Medical Record Compliance Timely processing of Release of Information requests Patient Incidents Pharmacy Issues Laboratory errors Actions required
86
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
Next available new and follow-up appointments Consult referrals ER referrals Unique Veterans Hand Hygiene
A sample QM/I program memorandum is included as ATTACHMENT B.
E.2.C.IV. XXXXXX XXXXX’S MULTI-FOCUSED QUALITY MANAGEMENT/ IMPROVEMENT PROGRAM
Xxxxxx Xxxxx’s QM/I program is truly multi-focused, as evident in the variety of monthly reports generated throughout the performance of this program. Xxxxxx Xxxxx will provide reports on enrolled patients for monitoring quality, access, and availability of care. Patient data is accumulated in the customized Xxxxxx Xxxxx database for each patient encounter. Reports are accessed on a monthly basis to identify visit utilization by Providers, total number of patients seen by Provider and total number of patients in the cumulative panel. Additionally, monthly reports will include the number of ER and/or Urgent Care visits within 48 hours of being seen by a CBOC provider, percent of scheduled appointments that are no-shows/missed opportunities, number of enrollee grievances filed, and number of written enrollee compliments filed by letter or comment cards. This data is provided to management, Providers and VA points of contact as requested for ongoing and targeted management efforts. Management meetings are scheduled on a monthly basis between Providers and Xxxxxx Xxxxx management staff to identify and evaluate results. Meetings are also held on a monthly basis between Xxxxxx Xxxxx and VA contract administration staff where these utilization reports, as well as other issues, are reviewed.
E.2.D. TIMELINESS OF CARE AND ACCESS AS IMPORTANT ELEMENTS OF CARE
One very important focus of Xxxxxx Xxxxx’s Quality Management/Improvement Program is timeliness of care. As part of the Quality Management/Improvement Program, Xxxxxx Xxxxx reports CBOC waiting times to parent VAMCs on a monthly basis. As required by the Contract, CBOC patient waiting times will be reported monthly, as directed on Pg. 101 of the Solicitation, including:
Actual waiting time for schedule appointment (time of check-in to time seen by Provider), compiled in the following categories: 20 minutes or less; 21 to 60 minutes; and over 60 minutes.
Actual waiting time for unscheduled walk-in visit by enrolled patient from time of clinic check-in to start of triage by clinic personnel according to the following categories: 15 minutes or less; 15 to 30 minutes; and over 30 minutes.
This is in accordance with VHA guidelines’ strategic Mission and Vision (VHA Directive 2006-041, June 27, 2006) which states that “Patients must be seen by a provider within 20 minutes of their scheduled appointment.”
Regarding Collection and Reporting Clinical Indicators, Clinical Reminder Compliance - Clinical Reminders are computerized requirements for ensuring quality management regarding preventive health measures. These include items such as Immunizations, Blood Pressure control, Tobacco Use and Cessation,
87
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
CHF monitoring and ACE I Use, Diabetic eye exams, foot inspections, pedal pulse exams, Hemoglobin A1C control, Women’s Health issues and PSA for men. Reminders are based and monitored according to VA Directives and Performance Measures.
A report is received from the Hospital that indicates the clinical reminders monitored, total patients seen that month and is Provider specific. The report also indicates the total number of patients the reminder is applicable to and if there were any not completed. Once the information is tabulated, a stat sheet and graph is then provided for the Providers and nursing staff to show compliance for each reminder. Compliance is the satisfactory percentage that is provided to us by the VA Hospital; if no percentage is given then a minimum 80% compliance is used. The nursing staff and the Providers are responsible for developing a Corrective Action Plan based on non-compliance with the reminders, as well as non compliance or negative trend from the preceding reporting period.
Regarding report utilization, relevant patient data is accumulated in the customized Xxxxxx Xxxxx A.C.T. database for each patient encounter. Reports are accessed on a monthly basis to identify visit utilization by providers, total number of patients seen by provider and total number of patients in the cumulative panel with data provided to management, providers and VA points of contact as requested for ongoing and targeted management efforts. Management meetings are scheduled on a monthly basis between providers and Xxxxxx Xxxxx management staff to identify and evaluate results. Meetings are also held on a monthly basis between Xxxxxx Xxxxx and VA contract administration staff where these utilization reports, as well as other issues, are reviewed.
E.2.D.I. XXXXXX XXXXX’S CBOC PERFORMANCE INCENTIVE PROGRAM TO PROMOTE QUALITY
Xxxxxx Xxxxx will utilize performance incentives to ensure health promotion, disease prevention, access to care, patient safety and QA reporting. On a quarterly basis, Xxxxxx Xxxxx will provide a cash incentive of $1,500 to be split equally among clinic staff members for meeting the following performance goals:
Meeting access to care standards with no existing patients waiting more than 7 days for a scheduled primary care appointment and no new patient waiting more than 14 days for a primary care appointment.
Scoring at or above the national average for patient satisfaction (85% or higher). Demonstrated improvement in meeting or exceeding goals for clinical reminders. Maintaining “0” patient safety incidents.
Further, Xxxxxx Xxxxx offers disincentives to aid in the retention of Providers. In particular, there is a severe monetary disincentive (up to $5,000) should a provider cancel their contract for services within the first year. This part of the contract is a necessary component to ensure that the provider remains in place, assuring the complete training cycle required learning CPRS. It is essential that all providers put in this minimum time of one (1) year to overcome the learning curve and to become proficient with the CPRS medical records system.
E.2.D.II. CLINICAL PRACTICE GUIDELINES AND CLINICAL REMINDER COMPLIANCE
88
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
The Xxxxxx Xxxxx QM/I program is designed to encourage and monitor its Providers in following Clinical Practice Guidelines and complying with Clinical Reminders. It is Xxxxxx Xxxxx’s policy to utilize the VHA Performance Measure/Clinical Practice Guidelines Program and ORYX/Core Measures to decrease variation among practitioners and across care settings, while improving patient outcomes. VHA Performance Measures and Clinical Practice Guidelines are mandatory and based Clinical Reminder compliance in CPRS. The Clinical Practice Guidelines Program is organized by the RLR VAMC Clinical Practice Guidelines Coordinator who will analyze any indicators not meeting expected performance and implement action plans for improvement.
Clinical Practice Guidelines are recommendations for the performance or exclusion of specific procedures or services for specific disease entities. These recommendations are derived through a rigorous methodological approach that includes a systematic review of the evidence to outline recommended practice. Implementation of evidence-based Clinical Practice Guidelines is one strategy that VHA has implemented to improve care by reducing variation in practice and systematizing “best practices”. These Guidelines are tools to improve the processes of care for patient cohorts, serve to reduce errors, and provide consistent quality of care and utilization of resources throughout the system.
Data related to an individual’s performance in meeting these Clinical Practice Guidelines (through completion of Clinical Reminders, EPRP findings or results reported to the Medical Center through the Xxxxxx Xxxxx monthly QM Program), can be collected from the RLR VAMC and sent on a monthly basis to our Quality Managment office for use in monitoring performance of all HCPs for whom these performance guidelines are applicable. Additionally, analysis of such monthly reports assists with early identification of performance problems such that a Performance Improvement Plan (PIP) can be implemented for a HCP through our QA and HR processes, in coordination with the RLR VAMC Clinical Practice Guidelines Coordinator. Aditionally, Xxxxxx Xxxxx will submit biweekly the Clinical Reminders Due report to the COTR.
Individual healthcare providers will be monitored while providing PIP compliance.
The PIP can include adjustments to the HCP’s Individualized Learning Plan as the Xxxxxx Xxxxx CBOC Services Management Team, in coordination with RLR VAMC administrative members, can assign relevant CMEs/CEUs, annual basic competency courses or other training modules for completion by a specified date. Xxxxxx Xxxxx can include VHA-specific modules in our web-based curriculum as well as modules from OSHA and the CDC or other health related agencies. Improvement in performance (or lack of) can then be tracked and included in monthly reporting related to performance monitoring and trend data analysis.
The above process will assist in addressing inadequate performance early, allow for corrective action mechanisms to be implemented in a timely manner and also to allow for continuous monitoring of ongoing performance.
E.2.D.III. XXXXXX XXXXX’S ABILITY TO MEASURE AND IMPROVE QUALITY OF SERVICE
In an effort to thoroughly assure the Government of our quality of service, Xxxxxx Xxxxx will institute an established, well crafted Quality Management/Improvement Plan upon Contract commencement.
89
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
As previously mentioned, compliance with and monitoring of VA directives/policies and JCAHO requirements and plans will be incorporated into our Taos CBOC Quality Management/Improvement Plan. This will provide for continuous monitoring and improvement of compliance and performance. This information will be included in our monthly Quality Improvement Report provided to the VA, as well as to the corporate CBOC Management Team. Compliance issues will be also discussed weekly as a regular agenda item for meetings with the management team and Clinic Coordinators.
Additional information regarding Xxxxxx Xxxxx’s JCAHO Compliance Plans is included as Compliance Plan CD-ROM with this Proposal.
E.2.D.IV. PERFORMANCE METRICS
As discussed in Section II.4A.1, the Xxxxxx Xxxxx Quality Management/Improvement Plan for the Taos CBOC will include the following minimum metrics:
Performance Measures Patient Satisfaction Access Entry of Medical Data Quality Care
During the Taos CBOC contract 90 day start-up period, the contract leadership team, comprised of the Xxxxxx Xxxxx corporate level Quality Management/Improvement Program Coordinator and Patient Advocate, the Taos Contracting Officer, the CBOC Medical Director, the Contracting Officer’s Technical Representative, the Physician Director for Performance Improvement, the CBOC Infection Control Coordinator and the Registered Nurse Clinic Coordinator will hold two (2) formal meetings to ratify the Taos CBOC Quality Management/Improvement Program metrics.
Additionally, the results of the Xxxxxx Xxxxx Peer Review Program and NMVAHCS External Peer Review Program, as discussed in the following sections, will be included in the Quality Management/Improvement Plan.
E.2.D.V. CBOC QUALITY MANAGEMENT/IMPROVEMENT PLAN REPORTS
Xxxxxx Xxxxx will oversee the timely submission of the Taos CBOC minimum reporting requirements as directed as in the Solicitation. Outcomes from monitoring data, peer review and the patient compliment and complaint process will be kept on file in the COTR office, and incorporated into the re-privileging process. Beyond the daily Patient Visit Report, the COTR will receive monthly: all Licenses and Certifications that expire within 30 days, Performance Improvement Meeting Minutes, CBOC Staff Meeting Minutes, Patient Visit Reports, Patient Waiting Times Reports for both scheduled and unscheduled appointments, Staff Education Reports, Patient Grievances, and Patient Written Compliments. On the 10th workday after the end of the month the COTR shall receive the monthly New Patient Listing, the Listing of Annual Vesting Visit, the Veteran Disenrollment from the CBOC Report, and the Infection Control Committee Minutes and Quarterly Reports. The Competency Assessment Findings and Inspection Compliance Report will be submitted annually to the COTR to be kept on file. The COTR will also receive the annual Quality Management/Improvement Assessment Report including the Freedom of Information Act Requests and Privacy Act Requests.
90
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.

Xxxxxx Xxxxx will submit to the Taos CBOC Contracting Officer a quarterly Subcontractor Report.
Should any Reportable Events occur, either catastrophic or major, the NMVAHCS QM Manager will be notified via telephone or the COTR will receive a written report within four (4) hours. The NMVAHCS CBOC Clinical Coordinator will receive reports from Xxxxxx Xxxxx regarding all cases of suspected Provider or patient abuse or fraud and a completed VA Form 10-2633 as identified using NMVAHCS policy on Identification of Abuse Victims. Xxxxxx Xxxxx will also immediately notify the Clinical Coordinator of any malpractice actions brought against any of its Providers, regardless of source or outcome.
Beyond the Taos CBOC required minimum reports, Xxxxxx Xxxxx will provide additional reports as part of our Quality Management/Improvement Plan. These will include information on enrolled patients as generated by the Taos CBOC customized database to identify visit utilization by Providers, total number of patients seen by Provider and total number of patients in the cumulative panel. This data will be shared with the Taos Clinic management, Providers and VA points of contact for ongoing and targeted quality improvement efforts.
Both a sample Quality Management/Improvement Program memorandum and a sample patient data collection chart and graph can be found in Section II.5B.4.
Graphing similar to the above-displayed graph is applied to each applicable clinical provider field, thus measuring clinic trends. By documenting positive and negative clinical movement, Xxxxxx Xxxxx is able to proactively measure and improve a Clinic’s patient access. As stated above, if the provider either fails to meet the compliance standard or has declined in their compliance standard from the preceding standard, the provider will complete a PIP. If a provider’s negative trend persists, further corrective actions will be taken, culminating in the potential termination of a provider’s services.
E.2.D.VI. CONTINUOUS QUALITY IMPROVEMENT
Continuous Quality Improvement (“CQI”) is an effort by healthcare Providers to improve the quality of service by continuously exceeding patients' expectations. Patient satisfaction with the Taos clinic will be one of the measures of the quality of care. Because QI activities will be an important part of Taos healthcare operations, patients should participate in quality improvement, which will often require direct cooperation (for example, permitting collection and use of data about their medical conditions, treatments, and outcomes). The interests of patients in receiving reliably high-quality healthcare will depend on all patients cooperating with QI activities.
Further, Xxxxxx Xxxxx, following VAMC approval, will implement an established Patient Advocacy Program at the proposed Clinic. Xxxxxx Xxxxx’s Patient Advocacy Program has been developed to compliment the VA’s patient advocacy program and patient bill of rights. Xxxxxx Xxxxx’s corporate office employs a full-time Patient Advocate to address patient issues and concerns. The waiting area of the Taos’s CBOCs will prominently display a large sign providing information on this program that will include basic patient rights set forth by VHA guidelines and the toll-free number for Xxxxxx Xxxxx’s Patient Advocate. Xxxxxx Xxxxx’s corporate Patient Advocate will coordinate with the Taos CBOC staff person designated as the representative for patient advocacy in utilization of the Department of Veterans Affairs Patient Advocate Tracking Package to log and report complaints and resolution. This two track portal for
91
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
Washington/Uniontown veteran patient issues will ensure that all concerns are efficiently and effectively address
The patient's responsibility to cooperate will be subject to standards of reasonableness, which will require that patients have access to general information about the Taos CBOC QI activities and be kept safe from harms and from violations of their rights. For example, the veteran patients should be able to count on the confidentiality of their personal health information and on the opportunity to choose whether to participate in a QI activity that will expose them to more than minimal incremental risk (measured relative to the risks of usual medical care). E.2.D.VII. ADDITIONAL METHODS TO INCLUDE VETERAN PATIENTS IN QUALITY MANAGEMENT/IMPROVEMENT PLAN
Xxxxxx Xxxxx will utilize several additional methods to incorporate Taos CBOC patients in Quality Management/Improvement efforts. At the Taos Clinic, these will include:
Establish task forces, specific to identified health issues/concerns/diseases, to explore ways to improve service and veteran care and include patients and families on site visit teams to other programs.
Work with state Quality Improvement Organization (QIO)-There are 53 QIOs (one for each state, territory and the District of Columbia). The QIOs work with consumers, physicians, hospitals, and other caregivers to improve the healthcare system. Many QIOs have consumer councils and are interested in working with consumer advocates to incorporate the patient perspective.
The customers of the Taos CBOC include the patients and their significant others, referrers (e.g., GPs and hospital specialists), the organization’s staff and other healthcare Providers. It is essential that the Taos CBOC will listen to all customers.
Hold information-gathering sessions with Taos CBOC patients and families before developing educational materials and involve them throughout the development process.
Ask patients and families to assist in adapting patient information materials to meet the literacy and language needs of patients served by the Taos Clinic.
Create volunteer or staff positions for patients and families such as clinic greeter, peer mentor/coach or peer liaison.
Solicit Taos CBOC patient and family involvement in building relationships with community programs and resources.
Utilize Xxxxxx Xxxxx’s established Patient Advocacy Program, as described in Section II.4B.3.
E.3. CUSTOMER SATISFACTION
Xxxxxx Xxxxx utilizes a variety of tools to capture data related to customer satisfaction - both from the Government client and the patients we serve. The frequency of our solicitation of this feedback from patients varies from clinic to clinic and is dependent in part on the performance data we receive from the parent VAMC hospital. Upon VAMC approval, Xxxxxx Xxxxx sends satisfaction surveys to patients on at least a quarterly basis. When there is a need for performance improvement, more focused surveys will be sent to patients to add the clinic in identifying issues
On at least a quarterly basis we send out surveys to patients, but more focused surveys will be sent out for clinics that are in need of performance improvement. These tend to be targeted for specific areas for which we have developed Performance Improvement Plans (“PIP”).
92
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
Our Quality Assurance Department, located at our corporate headquarters, collects data from patients via surveys, from surveys issued by the VA healthcare network and from calls made to our Patient Advocacy Program - discussed later in this section. Every patient complaint is carefully documented and is provided to a member of our CBOC Services Management Team of our corporate office for review and follow-up. Outcomes of this process are provided in contractor reporting to the VAMC as requested.
The following page contains a sample of patient satisfaction data compiled from surveys conducted from 2007 through 2009 for several clinics that were in operation for either a three-year period or recently began operation during 2009:
CLINIC LOCATION 2007 2008 20092010 (YTD) OVERALL
Schenectady 100.00% 99.61% 97.48% 98.75% 98.96%
Uniontown 99.50% 99.06% 96.73% 97.36% 98.16%
Washington 99.39% 99.16% 95.35% 96.60% 97.63%
Dyersburg N/A N/A 99.65% 96.84% 98.25%
Hopkinsville N/A N/A 97.77% 98.13% 97.95%
Jamestown N/A N/A 97.77% 97.38% 97.58%
McMinnville N/A N/A 97.92% 95.56% 96.74%
La Grange N/A N/A 95.78% 97.17% 96.48%
Additionally, a new program we are implementing in all clinics (including the proposed clinical locations, should Xxxxxx Xxxxx be the successful awardee under the current effort) is a wall-mounted suggestion box that is accessible only by management personnel. This allows veterans and/or their caregivers to make suggestions, provide compliments or simply offer comments with or without identifying themselves by name. These cards are processed and reviewed only by CBOC Management Team Members.
As well, one of the most critical patient issues is access to care - a large factor in patient satisfaction. In order to ensure patient satisfaction, timely access to care must be provided to CBOC patients in accordance with VA policy. To ensure compliance with the requirements set forth by the VHA Patient Advocacy Program and to further provide for timely access to care, a daily reporting form is used to track patient visits and enrollments at each clinic. This form, entitled “VA Clinic Daily Snapshot” is referenced in Section E.2.B above.
E.3.A. MAINTENANCE AND MONITORING CONTINUITY OF CARE FOR PATIENTS
Xxxxxx Xxxxx is dedicated to ensuring that VA directives regarding dual care are monitored and adhered to. Our plan for scanning, monitoring and sharing of patient information with the VA will ensure that all care for dual-care status Veterans is well coordinated, safe, documented and appropriate.
93
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
In order to ensure the quality care standards established by the VA, Xxxxxx Xxxxx will monitor the status and medical data of all dual care patients. With each patient visit, Xxxxxx Xxxxx will ensure that each Veteran’s status is updated immediately through electronic record entry. This maintenance will be monitored and executed at each level of clinic care and the process will be overseen by the CBOC provider.
First and foremost, each dual care Veteran will be assigned a single primary care provider who oversees all aspects of care including treatment, testing and recordkeeping. The patient’s information will be updated and maintained with each patient visit. Information to be gathered includes interviews with the patient, as well as physical and mental examinations and test results. All information will be entered into CPRS and will be instantly available for examination by the Salem VAMC and VHA staff.
The CBOC Provider will monitor and thoroughly update each patient’s electronic record to ensure the following criteria are met:
All patients receiving controlled substances will be managed by one designated VA provider. This provider will be responsible for monitoring the patient and maintenance of the patient’s records.
All controlled substances for designated dual care patients will be closely monitored as well as the coordination of their care with any outside community-based care.
All dual-care patients will be enrolled in VHA and are have at least one visit per year with the VA provider.
Each dual-care patient’s status will be followed and managed by a VHA primary care physician or team if the patient requests primary care health needs from the VA even if some care is community based.
Educating the patient on the risks of dual-care treatment including the responsibility of the patient to cover the costs of any treatments not provided by VA healthcare providers.
The CBOC Provider will be responsible for VA care and services that are provided to the patient. Further the CBOC Provider will document all non-VA providers supplied by the patient in the patient’s electronic health record and the coordination of care by non-VA providers as made available by the patient and non-VA provider. All laboratory tests and other necessary monitoring for high risk medications either within the VA or outside of the VA will be documented by the VA Provider in the patient’s electronic record.
VA Providers will also utilize a letter created to be mailed to community providers who care for dual care veterans. This letter requests any medical information concerning the patient be forwarded to the VA Clinic for scanning and filing in order to provide safe, effective treatment for the Veteran patient.
E.3.A.I. CLINICAL RESULTS FROM PATIENT SATISFACTION SURVEYS
Xxxxxx Xxxxx utilizes a variety of tools to capture data related to customer satisfaction - both from the Government client and the patients we serve. The frequency of our solicitation of this feedback from patients varies from clinic to clinic and is dependent in part on the performance data we receive from the parent VAMC hospital. Upon VAMC approval, Xxxxxx Xxxxx sends satisfaction surveys to patients on at least a quarterly basis. When there is a need for performance improvement, more focused surveys will be sent to patients to add the clinic in identifying issues
94
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
On at least a quarterly basis we send out surveys to patients, but more focused surveys will be sent out for clinics that are in need of performance improvement. These tend to be targeted for specific areas for which we have developed Performance Improvement Plans (“PIP”).
*SEE ABOVE SECTION C.1.10 for Patient Satisfaction Survey results.
As well, one of the most critical patient issues is access to care - a large factor in patient satisfaction. In order to ensure patient satisfaction, timely access to care must be provided to CBOC patients in accordance with VA policy. To ensure compliance with the requirements set forth by the VHA Patient Advocacy Program and to further provide for timely access to care, a daily reporting form is used to track patient visits and enrollments at each clinic.
Additionally, Xxxxxx Xxxxx will provide reports on enrolled patients for monitoring quality, access, and availability of care. Patient data is accumulated in the customized Xxxxxx Xxxxx database for each patient encounter. Reports are accessed on a monthly basis to identify visit utilization by Providers, total number of patients seen by Provider and total number of patients in the cumulative panel. Additionally, monthly reports will include the number of ER and/or Urgent Care visits within 48 hours of being seen by a CBOC provider, percent of scheduled appointments that are no-shows/missed opportunities, number of enrollee grievances filed, and number of written enrollee compliments filed by letter or comment cards. This data is provided to management, Providers and VA points of contact as requested for ongoing and targeted management efforts. Management meetings are scheduled on a monthly basis between Providers and Xxxxxx Xxxxx management staff to identify and evaluate results. Meetings are also held on a monthly basis between Xxxxxx Xxxxx and VA contract administration staff where these utilization reports, as well as other issues, are reviewed.
E.3.A.II. XXXXXX XXXXX’S VETERAN AND PATIENT CENTERED CUSTOMER SERVICE CAPABILITIES
Xxxxxx Xxxxx’s careful attention towards the veteran community’s quality of care has resulted in its ability to provide high quality of care to the veteran community for over 13 years. In order to ensure patient satisfaction within the proposed clinic, Xxxxxx Xxxxx has implemented numerous procedures designed to monitor veteran patient feedback and incorporate all applicable feedback to the clinic so that a higher quality of care can be provided.
In accordance with VHA Handbook 1050.1, Xxxxxx Xxxxx will document all patient safety related incidents, utilizing the VA-created Root Cause Analysis (“RCA”) process to identify causal factors that contribute to a patient safety related event by utilizing an interdisciplinary team for investigation of the said event. The RCA process, as prescribed in VHA Handbook 1050.1, is as follows:
In the event of an “Adverse Event” or “Close Call” occurring within a Xxxxxx Xxxxx operated CBOC, clinic personnel may use any available or locally accepted method to notify the VA Safety Officer as well as the Xxxxxx Xxxxx Safety Officer and begin the Xxxxxx Xxxxx consideration of the event. The first step taken by the Safety Officer after any required immediate action is to investigate and assign actual and potential Safety Assessment Code (“SAC”) that then define what further actions are necessary.
In the context of the proposed service, the clinic personnel will use any available accepted method to notify the VA and Xxxxxx Xxxxx’s safety officer and begin the Xxxxxx Xxxxx’s consideration of the patient
95
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.

safety related event. After the immediate reporting of this event, the Xxxxxx Xxxxx’s Safety Officer will investigate to gather the appropriate facts to assign an appropriate SAC code for the event, and will determine what further actions are necessary to prevent the same or similar events from reoccurring.
The SAC matrix for ranking incidents is described below:
SEVERITY& PROBABILITY CATASTROPHIC MAJOR MODERATE MINORFrequent 3 3 2 1Occasional 3 2 1 1Uncommon 3 2 1 1
Events receiving a score of one or two will be acted on as deemed appropriate by Clinic staff. The overall goal for the response is to eliminate, control or accept the risks associated with these events. These actions can range from performing an RCA to “no further action required.
All events receiving an SAC score of “three” will receive either a traditional RCA or an Aggregated Review, as described in VHA Handbook 1050.1, subparagraph 7a (4). Additionally, the initial report of the event will be noted in the Monthly Contractor Report, for subsequent entry by the VA, if required, into the VA’s Patient Safety Information System.
By completing an RCA, the Safety Officer will be able to determine the cause of any patient safety-related incidents, through investigation and analysis of the events leading up to the occurrence. Through identification of root causes, appropriate preventative steps may be taken to avoid patient safety-related incidents at CBOC clinics.
Through use of RCA analysis and SAC rankings, as developed in VHA Handbook 1050.1, Xxxxxx Xxxxx will possess strong tools for analyzing patient safety-related events and preventing their recurrence. For all patient safety events, the VA referral source and the COTR will be informed throughout all investigations, and all findings and conclusions will be reported to the VA referral source and the COTR.
<THIS SPACE INTENTIONALLY LEFT BLANK>
96
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.

F. LOCATION OF OFFICES
Section F delineates site accessibility for our proposed clinic in Taos, New Mexico. In support of this Contract, Xxxxxx Xxxxx proposes the following clinic location:
PROPOSED CLINIC ADDRESS123 Cruz Alta Rd, Taos, NM 87571
The proposed clinic possesses ample space for primary care as well as mental health services and also possesses 3,200 square feet of usable space.
The site will be fully accessible to veteran beneficiaries and will be fully compliant with all applicable/current National Fire Protection Association (NFPA) Occupational Health & Safety Administration (OSHA), and JCAHO specifications. In addition, the chosen Clinic will be in compliance with all relevant aspects of the Uniform Federal Accessibility Standard (UFAS) and Americans with Disabilities Act (ADA). Further, the selected Clinic will prominently feature the following attributes:
The Clinic will be a permanent structure, with permanent foundation. The Clinic will be free of hazardous materials according to applicable federal, state, and local
environmental regulations. The Clinic’s Information Technology Closets will have the appropriately secure Windows,
Doors/Door Locks, Up and Over Access, Motion Intrusion Alarm and Special Key Access. The Clinic will prominently feature a large United States flag and POW Flag The Clinic will establish an on-going quality assessment monitoring/inspection checklist to
maintain survey, address and/or correct cleanliness issues. The Clinic will feature a dedicated tele-mental health room. The Clinic will feature ample, paved parking, levelly graded and in full compliance with VA,
local, state, and national handicap accessibility laws. The Clinic will feature professionally maintained landscaping during the growing season on a
weekly cycle to keep grass and shrubs trim.
The selected CBOC option will be subject to the following site improvements:
Flagpole to display an appropriately sized U.S. Flag and POW Flag will be installed NMVAHCS acceptable exterior signage will be furnished
While already in use as an outpatient medical office facility, interior renovations will be provided to conform to the proposed clinic space to VA use in accordance with accompanying floor plan documents. In a clinical location-specific manner, the above discussed clinical attributes are further described below with the corresponding Clinic Option.
F.1. UTILIZATION OF FACILITY’S GEOGRAPHIC LOCATION TO BEST SERVE THE PATIENTS
The proposed clinical location at 123 Cruz Alta Rd., Taos, NM 87571 offers an excellent solution to the VA’s needs in Taos, New Mexico. The proposed facility is a permanent structure.
97
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
Xxxxxx Xxxxx’s proposed facility was chosen for patient convenience and ease of access. The proposed Clinic is located in a predominant location in Taos, receiving tourist and commercial traffic from a wide multitude of surrounding communities.
The proposed clinical location in Taos, New Mexico will possess the following facility features:
SPECIFICATION TYPE
DESCRIPTION
FACILITY DEDICATION
The clinic will be fully dedicated to the VA community. Veterans will never have to share the waiting room or the clinic with other non-veteran patients.
EXTERIOR AND EXTERIOR AESTHETICS
The clinic location will prominently feature signage identifying the location as a VA CBOC healthcare facility. The clinic will prominently feature a large United States flag as well as a POW flag. The clinic location will feature professionally maintained landscaping
PARKING The clinic location will feature ample, paved parking, levelly graded and in full compliance with VA, local, state, and national handicap accessibility laws
WALL COVERINGS All clinic walls will have a gloss painted surface. All clinic walls will have vinyl or rubber bases, except for ceramic tile walls, ceramic tile wainscot on painted walls.
FLOORING Vinyl composition floor covering will be tile.CEILINGS All ceilings will be fire retardantAIRFLOW AND CIRCULATION
100% exhausted air to the exterior of the Medical Clinic Space in the following areas: (1) Rest rooms; (2) Housekeeping aid closets; (3) Clinic-Designated exam rooms. Negative pressure shall be maintained in the following areas: (1) Rest rooms; and (2) Clinic-designated exam rooms. All areas within the Outpatient Clinic shall be designated to have 10 air changes per hour with the exception of the following: (1) Waiting rooms: 8 changes per hour; (2) Conference room: 8 changes per hour; (3) Office and exam rooms: 6 changes per hour.
AUDITORY PRIVACY
Auditory privacy will be ensured throughout the Clinic, including in the reception/check in area to allow for privacy upon check in of patients.
PATIENT RESTROOMS
Patient Rest Rooms shall be equipped with (1) Water closet, wall hung, flush valve; (2) Dispenser, toilet tissue, double roll with lock; (3) Grab Bar, 2 for each water closet; (4) Lavatory, wall hung 2”x18”x3 ½” apron, for 8” faucet centers; (5) Paper towel dispenser; (6) Overhead lavatory light; (7) Mirror; (8) Soap dispenser; (9) Wastebasket; (10) Ground Fault Interrupting type outlet if electrical outlet is within 6’ of a sink; (11) Changing table; (12) Sanitary product dispenser; and (13) Call system with cleanable cords.
EXAMINATION ROOMS
Examination Rooms shall be equipped with: (1) Lavatory 20”x18” x3 ½” apron, for 8” faucet centers, with wrist or foot control; (2) Outlet, telephone, wall mounted (empty conduit system), one for each wall; (3) Receptacle, electrical, hospital grade, duplex, 120 volt, 20 amps, 2 walls. A quadriplex, 120 volt, 20 amps on one wall between the two walls with the duplex receptacle. If the electrical outlet is within 6’ of a sink, then it shall be Ground Fault Interrupting type; (4) Receptacle electrical, hospital grade, quadriplex, 120 volt, 20 amps, 48” above finished floor at location for otoscope, ophthalmoscope, exam light and electrical thermometer; (5) Cabinets, wall mount, with doors sufficient to meet exam room storage needs. Cleanable surface; (6) Dispenser, paper towel: wall mounted, 40” from finished floor, 10 ¾” W x 4”D x 14 ¾”H; (7) Soap dispenser; (8) Alcohol Sanitizer dispenser; and (9) Sharps container.
98
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
SPECIFICATION TYPE
DESCRIPTION
LABORATORY The laboratory will include a specimen collection area, including a specimen pass through. Additionally, the lab will include: (1) Partitions allowing for a movable prep area; (2) Countertop sufficient for centrifuge operations with a cleanable surface; (3) Cabinets sufficient to meet the storage needs of the laboratory area, including a cleanable surface; (4) Sink for hand washing, with soap dispenser and towel dispenser; (5) Receptacle, electrical plug mold, 120 volt, and 20 amp. for centrifuge; (6) Receptacle, electrical, quadriplex, 120 volt. 20 amp (6 total) for Refrigerator. If the electrical outlet is within 6’ of a sink, then it shall be Ground Fault Interrupting type; (7) Duplex plate box with outlet for telephone system and outlet for data processing, both served by (1) ¾” empty conduit system. One set on each of two walls; (8) Dispenser, paper towel, wall mounted 40” from finished floor (at least on by each sink); Alcohol sanitizer dispenser; (10) Sharps container.
TELEMENTAL HEALTH
The clinic location features a dedicated tele-mental health room.
SECURITY A monitored security system will be provided by Xxxxxx Xxxxx, inclusive of a panic button system (number and locations of panic buttons to be agreed upon prior to operations). The Contractor shall provide a level of security that reasonably prevents unauthorized entry to the space during non-duty hours and deters loitering or disruptive acts in and around the Clinic. The Contractor shall have a perimeter Intrusion Detection System (IDS) to be operated and maintained by the Contractor. The IDS shall include silent duress alarms with lights over the doors in patient care areas, alarms at all exterior doors and windows, and motion detection sensors at interior ingress areas. A central alarm panel shall be located in the reception area. Alarms shall be tested on a monthly basis in conjunction with the Government.
UTILITIES Xxxxxx Xxxxx provide the following services and utilities: heat, electricity, sewage, water (hot & cold), trash removal, regulated medical waste removal, (sensitive material removal to be in compliance with HIPAA regulations), chilled drinking water, air conditioning, toilet supplies, janitorial services and supplies (paper towels, antimicrobial hand soap and alcohol hand-sanitizers); elevator service, window washing, carpet cleaning, initial and replacement lamps, tubes & ballasts, painting, pest control, and other appropriate services.
The proposed clinical location’s physical characteristics are described in the following physical facility figures. These included figures are indexed as follows:
FIGURE # DESCRIPTION PAGE
1The proposed clinical site in Taos, New Mexico offers a total of 3,200 sq. feet of usable space. The photograph featured in Physical Facility Figure 1 depicts the front of the proposed clinical location.
102
2The floor plan featured in Physical Facility Figure 2 depicts space allocation within the proposed clinical location’s front interior.
103
3The floor plan featured in Physical Facility Figure 3 depicts room allocation within the proposed clinical location’s middle interior.
104
4Figure 4 provides a drawing of the signage which will be displayed outside of the Taos, New Mexico location:
105
99
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
PHYSICAL FACILITY FIGURE 1 The below photograph depicts the front of the proposed Clinic Option A location in Taos:
<THIS SPACE INTENTIONALLY LEFT BLANK>
100
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
PHYSICAL FACILITY FIGURE 2 The below figure depicts space allocation within the proposed Clinic:
<THIS SPACE INTENTIONALLY LEFT BLANK>
101
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
PHYSICAL FACILITY FIGURE 3 The below figure depicts room allocation within the proposed Clinic:
<THIS SPACE INTENTIONALLY LEFT BLANK>
102
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.

PHYSICAL FACILITY FIGURE 4: The below figure represents a proposed drawing of the signage which will be displayed outside of the VA-selected Taos, New Mexico clinical location:
<THIS SPACE INTENTIONALLY LEFT BLANK>
103
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
F.2. LOCATION OF PROPOSED CLINIC: TAOS, NEW MEXICO
As noted above, the proposed Xxxxxx Xxxxx Taos, New Mexico CBOC facility will be located at 123 Cruz Alta Rd., Taos, NM 87571. This address is located firmly within the city limits of Taos, New Mexico. The below figure depicts an aerial representation of the proposed facility’s location:
<THIS SPACE INTENTONALLY LEFT BLANK>
104
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
F.3. LOCATION OF FACILITY IN RELATION TO PUBLIC TRANSPORTATION
Taos is located in Taos County, which is home to the Chile Line Public Transportation System. Since 1997, the Chile Line Public Transportation system has been operated by the Taos Transit System and is a full-featured municipal transit corporation that provides dedicated to the citizens and visitors of Taos, New Mexico. Taos Transit operates on a regular schedule throughout the weekdays from 7:30 AM to 6:30 PM Monday through Friday. The Chile Line’s Regular Fare is $.50 per one way ride and special discounts can be made for passengers who qualify as being disabled.
The Chile Line Public Transportation System maintains one (1) stop near the 123 Cruz Alta Rd. location that has been recently added to the southbound transit line at the intersection of Highway 68 and Cruz Alta Drive. The stop is 0.3 miles away from the proposed clinic’s location and is accessible via crosswalk that features ADA ramps and a painted pedestrian crosswalk.
As mentioned above, the Chile Line Public Transportation System offers special ADA Van Services known as the HANDI-VAN, which is a public transportation service offered by the Town of Taos Transit Division that provides curb to curb transportation services for persons with disabilities of all ages and who, due to disability, cannot utilize the Chile Line Fixed Route. The HANDI-VAN provides service to passengers traveling to and from any location located within three-quarters (3/4) of a mile of the fixed transit line. The HANDI-VAN uses special ADA accessible vehicles equipped with hydraulic lifts and wheel chair tie-downs. All transit drivers are specially trained in defensive driving, customer sensitivity, and ADA regulations.
Residents of the Town of Taos as well as visitor are eligible for HANDI-VAN services once they’ve completed the application, meet the eligibility criteria and once they’ve been certified as eligible by a personal physician. Once the application has been processed and the candidate has been approved, the person would call to schedule an appointment 48 to 72 hours in advance. HANDI VAN services are available at a rate of twenty-five cents ($0.25) for a one-way trip or fifty cents ($.50) for a round trip and the exact fare must be paid at the time of pick-up.
More information on the Taos Transit public transportation system can be found on their website (http:// www.taosgov.com/transportation/chile-line.php) or by calling (575) XXX-XXXX. An illustration of these aforementioned bus routes, as well as the entirety of the Chile Line Public Transportation system, including their ADA Van Services, can be found in ATTACHMENT D.
<THIS SPACE INTENTIONALLY LEFT BLANK>
105
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.
F.4. LOCATION OF FACILITY TO LOCAL HIGHWAYS
A map delineating the proposed clinical location proximity to local highways is included below:
Distances relating to the proposed CBOC location at 123 Cruz Alta Rd., Taos, NM 87571 and major local roads are provided below:
HIGHWAY NAME DISTANCE FROM CLINIC TO HIGHWAY
NM-68 0.3 milesNM-64 1.4 milesNM-240 2.3 milesNM-585 2.2 milesNM-518 5.9 milesNM-522 5.7 milesNM-285 33 milesNM-38 25.8 milesNM-434 15.7 milesNM-76 25.3 miles
106
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.

The proposed clinical location is readily accessible when traveling by vehicle and is located within the Taos city limits. To that end, we note the proposed clinical location’s proximity to of-interest destinations:
DESTINATION DISTANCE FROM CLINIC TO DESTINATIONUniversity of New Mexico - Taos 1.8 milesHoly Cross Hospital 2.1 milesTaos Regional Airport 9.7 milesAngel Fire Airport 21.8 milesDowntown Taos 1.6 miles
F.5. DESCRIPTION OF FACILITY’S PARKING AVAILABILITY
The proposed Taos, New Mexico CBOC location has a total of 28 parking spots available for the entire facility at all times of service operation. The parking lot is in good condition and is on a level, paved lot with direct access to the front entrance.
F.6. DESCRIPTION OF FACILITY’S HANDICAP PARKING AVAILABILITY
The parking area in front of the proposed facility main entrance does feature three (3) ADA parking spaces. Per ADA regulations, accessible parking spaces will be at least 108 in. wide (Ref: ANSI A117.1-502.2). Parking access aisles shall be part of an accessible route to the building or facility entrance and must be a minimum of 60 in. in width. Two accessible parking spaces may share a common access aisle (REF: ANSI A117.1-502.2). Parked vehicle overhangs shall not reduce the clear width of an accessible route (REF: ANSI A117.1-502.2). Parking spaces and access aisles shall be level with surface slopes not exceeding 1:50 (2%) in all directions (REF: ANSI A117.1-502.4 SPECIFICES 1:48).
F.7. DESCRIPTION OF FACILITY’S PROPOSED HOURS OF OPERATION
The Taos, NM CBOC will furnish services for a minimum of 30 hours a week between the hours of 7:00 AM to 7:00 PM, Monday through Friday, with ten federal holidays as established within the solicitation to support the minimum patient volume under the Contract Schedule. Upon clinic opening, Xxxxxx Xxxxx will conduct patient surveys among its enrolled patient base to determine the need for increased hour appointments during weekdays to support increased patient volumes up to maximums in the contract schedule.
Should they be determined to be a necessity, Xxxxxx Xxxxx will coordinate with the VA throughout the Contract period and if the need arises for additional hours, then Xxxxxx Xxxxx will implement extended hours (within the hours 0700 to 1900 Monday through Friday) as needed to meet the needs of the local veteran patient population. Xxxxxx Xxxxx’s leasehold arrangement provides for evening and weekend access to its proposed location for any future Primary Care or Mental Health services that may be required by the Department of New Mexico Veteran Affairs Albuquerque Healthcare System (“NMVAHCS”).
A New Mexico licensed Primary Care Provider (either a Board Certified Physician or Nurse Practitioner) will be present in the clinic during all operating hours, as would the Licensed Independent Social Worker, should the need be determined. Support staff can also be increased to support the increased hours of Primary Care and Mental Health services.
107
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.

G. LISTING OF ALL EXTERNAL ATTACHMENTS AND EXHIBITS
Please note the following attachments and exhibits which accompany this proposal:
PROPOSAL ATTACHMENTSATTACHMENT ATTACHMENT DESCRIPTIONAttachment A Copies of CVs, resumes and licensure of proposed staffAttachment B Sample QM/I Program MemorandumAttachment C Summary of Compliance Plan ComponentsAttachment D Taos, NM Public Transportation Info
CBOC Compliance Plan CD-ROMPART TOPIC
A National Patient Safety GoalsB Safety Management PlanC Fire Safety Management PlanD Security Management PlanE Emergency Management PlanF Hazardous Materials Management PlanG Medical Equipment Management PlanH Utility Management Plan I Environment Management PlanJ Performance Improvement Management PlanK Bloodborne Pathogen PlanL TB Control PlanM Infection Control PlanN HIPAA/VHA Privacy PolicyO AED Policy and InventoryP Ergonomics ProgramQ Competency AssessmentR Mock Survey
SContinuing Education, JCAHO Training, and Annual Basic Competencies
T Accident Investigation
108
The information contained on this page is considered confidential and privileged, and is not subject to mandatory disclosure under FOIA. Additionally, any attachments referenced on this page and included with this proposal are considered confidential and privileged, and are not subject to mandatory disclosure under FOIA.