Mar / April 2012
64
March/April 2012 • Volume 10 • Issue 2 EDITORIAL Scabies en and Now Lavery, Parish, and Wolf ORIGINAL CONTRIBUTIONS Erlotinib-Induced Scalp Perifolliculitis Rallis, Petronic-Rosic, and Korfitis New Findings in Delusions of Parasitosis Fellner REVIEW Wound Care in Short-Term Rehabilitation Facilities and Long-Term Care: Special Needs for a Special Population White-Chu and Reddy CORE CURRICULUM Cutaneous Tuberculosis: A Diagnostic Dilemma—Laboratory Inputs Sehgal, Verma, Bhattacharya, Sharma, Singh, and Verma DEPARTMENTS PERILS OF DERMATOPATHOLOGY Sometimes It Takes Darkness to See the Light: Pitfalls in the Interpretation of Cell Proliferation Markers (Ki-67 and PCNA) Castilla, McDonough, Tumer, Lambert, and Lambert INFECTIOUS DISEASE CAPSULES e Lion Is NOT Sleeping Tonight Carr, Bernstein, and Trevino PHOTO CAPSULES Actinomycetoma Dlova and Mosam CASE STUDIES Malignant Melanoma Arising Within Nevus Spilus Karam and Jackson Pseudocyst of the Auricle: An Uncommon Entity of the Ear Sheaffer, Sahu, and Lee Necrotic Ulcer: A Manifestation of Leukemia Cutis Aksu, Saracoglu, Sabuncu, Ciftci, Gulbas, and Isiksoy Inflammatory Linear Verrucous Epidermal Nevus With Genital Involvement Balci, Yenin, Çelik, Sarikaya, and Atik Oral Frictional Hyperkeratosis (Morsicatio Buccarum): An Entity to Be Considered in the Differential Diagnosis of White Oral Mucosal Lesions Cam, Santoro, and Lee Vesicular Palmoplantar Pityriasis Rosea Singh, Sharma, Narang, and Madan BOOK REVIEW Hall’s Manual of Skin as a Marker of Underlying Disease Reviewed by Scheinfeld
-
Upload
jo-ann-kalaka-adams -
Category
Documents
-
view
230 -
download
2
description
SKINmed Dermatology for the Clinician is a peer-reviewed, indexed bimonthly publication circulated to more than 13,000 high prescribers of dermatological products, plus many dermatologists who are members of select national and international societies. Our Journal is specifically written to be of interest to dermatologists and serve as a didactic resource of clinical content for non-dermatologists. SKINmed editorial content is succinct, practical, and focused on state-of-art contributions, enabling clinicians to maximize the quality of patient care. Editorial content includes: original contributions and review presentations, editorials, case studies, clinical trials, and roundtable discussions, as well as regular columns on cosmetic dermatology, gender dermatology and dermatologic surgery.
Transcript of Mar / April 2012

March/April 2012 • Volume 10 • Issue 2
EDITORIALScabies Then and NowLavery, Parish, and Wolf
ORIGINAL CONTRIBUTIONSErlotinib-Induced Scalp Perifolliculitis
Rallis, Petronic-Rosic, and Korfitis
New Findings in Delusions of ParasitosisFellner
REVIEWWound Care in Short-Term Rehabilitation
Facilities and Long-Term Care: Special Needs for a Special Population
White-Chu and Reddy
CORE CURRICULUMCutaneous Tuberculosis: A Diagnostic
Dilemma—Laboratory InputsSehgal, Verma, Bhattacharya, Sharma, Singh, and Verma
DEPARTMENTSPERILS OF DERMATOPATHOLOGY
Sometimes It Takes Darkness to See the Light: Pitfalls in the Interpretation of Cell Proliferation
Markers (Ki-67 and PCNA)Castilla, McDonough, Tumer, Lambert, and Lambert
INFECTIOUS DISEASE CAPSULESThe Lion Is NOT Sleeping Tonight
Carr, Bernstein, and Trevino
PHOTO CAPSULESActinomycetomaDlova and Mosam
CASE STUDIESMalignant Melanoma Arising Within Nevus Spilus
Karam and Jackson
Pseudocyst of the Auricle: An Uncommon Entity of the Ear
Sheaffer, Sahu, and Lee
Necrotic Ulcer: A Manifestation of Leukemia CutisAksu, Saracoglu, Sabuncu, Ciftci, Gulbas, and Isiksoy
Inflammatory Linear Verrucous Epidermal Nevus With Genital Involvement
Balci, Yenin, Çelik, Sarikaya, and Atik
Oral Frictional Hyperkeratosis (Morsicatio Buccarum): An Entity to Be Considered in the Differential
Diagnosis of White Oral Mucosal LesionsCam, Santoro, and Lee
Vesicular Palmoplantar Pityriasis RoseaSingh, Sharma, Narang, and Madan
BOOK REVIEWHall’s Manual of Skin as a Marker of Underlying Disease
Reviewed by Scheinfeld

Now patients can spend less time thinking about their scars and more time seeing results.
NEWDaily Scar Gel 1X
1Data on fi le. Dec. 2011. 2IMS Health. NDTI. December 2010. *Statistical significance reached on all measurements observed (P<0.01). ©/®/™ 2012 Merz Pharmaceuticals, LLC
New Mederma® Advanced Scar Gel—the fi rst and only 1X daily scar therapy.
• From the #1 doctor recommended brand in scar care2
• More convenient application, better patient compliance, better results
• Clinically shown to improve scar softness, redness, texture and overall appearance
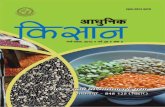
• Subjects saw a 36% greater improvement in the overall appearance of their scar
after 8 weeks vs. untreated scars (P<0.01)1
More information at mederma.com
Wear your skin proudly.™
Post Baseline: Subject Assessment for Treated vs. Untreated Scar at Week 81
Softness*0.0
1.0
2.0
3.0
Redness* Texture* Overall*
treateduntreated
0 = no change, 1 = mild improvement, 2 = moderate improvement, 3 = significant improvement
Mean
Scar
Rati
ng

61
TABLE OF CONTENTS
EDITORIAL
Scabies Then and Now .................................................................................................................................. 67 Michael Joseph Lavery, MB BCh BAO; Lawrence Charles Parish, MD, MD (Hon); Ronni Wolf, MD
ORIGINAL CONTRIBUTIONS
Erlotinib-Induced Scalp Perifolliculitis ............................................................................................................ 70 Efstathios Rallis, MD, PhD; Vesna Petronic-Rosic, MD, MSc; Chrysovalantis Korfitis, MD
New Findings in Delusions of Parasitosis ........................................................................................................ 72 Michael J. Fellner, MD
REVIEW
Wound Care in Short-Term Rehabilitation Facilities and Long-Term Care: Special Needs for a Special Population ..................................................................................................................................... 75
E. Foy White-Chu, MD; Madhuri Reddy, MD, MSc
Self-Test Review Questions (p. 81)
CORE CURRICULUMVirendra N. Sehgal, MD, Section Editor
Cutaneous Tuberculosis: A Diagnostic Dilemma— Laboratory Inputs ................................................................ 82 Virendra N. Sehgal, MD; Prashant Verma, MD; Sambit N. Bhattacharya, MD; Sonal Sharma, MD; Navjeevan Singh, MD; Nishant Verma, MD
DEPARTMENTS
PERILS OF DERMATOPATHOLOGY
W. Clark Lambert, MD, PhD, Section Editor
Sometimes It Takes Darkness to See the Light: Pitfalls in the Interpretation of Cell Proliferation Markers (Ki-67 and PCNA) ............................................................................................................................ 90 Carmen Castilla, BS; Patrick McDonough, BA; Gizem Tumer, MD; Peter C. Lambert, BA, MS; W. Clark Lambert, MD, PhD
INFECTIOUS DISEASE CAPSULES
Jack M. Bernstein, MD, Section Editor
The Lion Is NOT Sleeping Tonight ................................................................................................................... 94 David R. Carr, MD; Jack M. Bernstein, MD; Julian Trevino, MD
PHOTO CAPSULES
Ncoza C. Dlova, MBChB, FCDerm, Section Editor
Actinomycetoma ........................................................................................................................................... 98 Ncoza C. Dlova, MBChB, FCDerm; Anisa Mosam, MBChB, FCDerm
CASE STUDIESVesna Petronic-Rosic, MD, MSc, Section Editor
Malignant Melanoma Arising Within Nevus Spilus ......................................................................................... 100 Susan L. Karam, BS; Scott M. Jackson, MD
Pseudocyst of the Auricle: An Uncommon Entity of the Ear ........................................................................... 104 Alexis Sheaffer, BS; Joya Sahu, MD; Jason B. Lee, MD
Necrotic Ulcer: A Manifestation of Leukemia Cutis ....................................................................................... 108 Ayse Esra Koku Aksu, MD; Zeynep Nurhan Saracoglu, MD; Ilham Sabuncu, MD; Evrim Ciftci, MD; Zafer Gulbas, MD; Serap Isiksoy, MD
Inflammatory Linear Verrucous Epidermal Nevus With Genital Involvement ................................................... 112 Didem Didar Balci, MD; Jülide Zehra Yenin, MD; Ebru Çelik, MD; Gökhan Sarikaya, MD; Esin Atik, MD

62
TABLE OF CONTENTS
EDITORIAL DIRECTOR
COPYEDITOR
MEDIA WEB DIRECTOR
PUBLISHER ASSOCIATE PUBLISHER
PRESIDENT
CHIEF EXECUTIVE OFFICER
ABOUT OUR JOURNAL
SKINmed: Dermatology for the Clinician®
©
Corporate
Publishing
Editorial
GENERAL COUNSEL
Oral Frictional Hyperkeratosis (Morsicatio Buccarum): An Entity to Be Considered in the Differential Diagnosis of White Oral Mucosal Lesions .......................................................................... 114
Kristin Cam, MD; Anthony Santoro, MD; Jason B. Lee, MD
Vesicular Palmoplantar Pityriasis Rosea....................................................................................................... 116 Varinder Singh, MD; Meghna Sharma, MD; Tarun Narang, MD; Manas Madan, MD
BOOK REVIEWNoah S. Scheinfeld, MD, JD, Section Editor
Hall’s Manual of Skin as a Marker of Underlying Disease .............................................................................. 120 Edited by John C. Hall and Brian J. Hall. 300 pages. Shelton, CT; People’s Medical Publishing House–USA; 2011. $89.95. ISBN 1607951029


THE Aesthetic Show of the Year
World-Class FacultyPre-Show Educational SessionsAdvanced Hands-On Training
Patient Tx Workshops
To register visit www.aestheticshow.com or call + 1 (949) 830-5409
Register with Promo Code TAS3AD:
Aesthetic TV
THE Aesthetic Awards TM

March/April 2012 EDITORIAL BOARD
65
Mohamed Amer, MD
Cairo, Egypt
Robert L. Baran, MD
Cannes, France
Anthony V. Benedetto, DO
Philadelphia, PA
Brian Berman, MD, PhD
Miami, FL
Jack M. Bernstein, MD
Dayton, OH
Sarah Brenner, MD
Tel Aviv, Israel
Joaquin Calap Calatayud, MD
Cadiz, Spain
Henry H.L. Chan, MB, MD, PhD, FRCP
Hong Kong, China
Noah Craft, MD, PhD, DTMH
Torrance, CA
Ncoza C. Dlova, MBChB, FCDerm
Durban, South Africa
Richard L. Dobson, MD
Mt Pleasant, SC
William H. Eaglstein, MD
Palo Alto, CA
Boni E. Elewski, MD
Birmingham, AL
Charles N. Ellis, MD
Ann Arbor, MI
Howard A. Epstein, PhD
Philadelphia, PA
Ibrahim Hassan Galadari, MD, PhD, FRCP
Dubai, United Arab Emirates
Anthony A. Gaspari, MD
Baltimore, MD
Michael Geiges, MD
Zurich, Switzerland
Michael H. Gold, MD
Nashville, TN
Lowell A. Goldsmith, MD, MPH
Chapel Hill, NC
Aditya K. Gupta, MD, PhD, FRCP(C)
London, Ontario, Canada
Seung-Kyung Hann, MD, PhD
Seoul, Korea
Roderick J. Hay, BCh, DM, FRCP, FRCPath
London, UK
Tanya R. Humphreys, MD
Philadelphia, PA
Camila K. Janniger, MD
Englewood, NJ
Abdul-Ghani Kibbi, MD
Beirut, Lebanon
Andrew P. Lazar, MD
Highland Park, IL
Jasna Lipozencic, MD, PhD
Zagreb, Croatia
Eve J. Lowenstein, MD, PhD
New York, NY
George M. Martin, MD
Kihei, HI
Marc S. Micozzi, MD, PhD
Bethesda, MD
George F. Murphy, MD
Boston, MA
Oumeish Youssef Oumeish, MD, FRCP
Amman, Jordan
Joseph L. Pace, MD, FRCP
Naxxar, Malta
Art Papier, MD
Rochester, NY
Johannes Ring, MD, DPhil
Munich, Germany
Roy S. Rogers III, MD
Rochester, MN
Donald Rudikoff, MD
New York, NY
Robert I. Rudolph, MD
Wyomissing, PA
Vincenzo Ruocco, MD
Naples, Italy
Noah S. Scheinfeld, MD, JD
New York, NY
Virendra N. Sehgal, MD
Delhi, India
Charles Steffen, MD
Oceanside, CA
Alexander J. Stratigos, MD
Athens, Greece
James S. Studdiford III, MD
Philadelphia, PA
Robert J. Thomsen, MD
Los Alamos, NM
Julian Trevino, MD
Dayton, OH
Snejina Vassileva, MD, PhD
Sofia, Bulgaria
Daniel Wallach, MD
Paris, France
Michael A. Waugh, MB, FRCP
Leeds, UK
Wm. Philip Werschler, MD
Spokane, WA
Joseph A. Witkowski, MD
Philadelphia, PA
Ronni Wolf, MD
Rechovot, Israel
EDITOR IN CHIEF
EDITORIAL BOARD
DEPUTY EDITORS
William Abramovits, MD
Dallas, TX
W. Clark Lambert, MD, PhD
Newark, NJ
Larry E. Millikan, MD
Meridian, MS
Jennifer L. Parish, MD
Philadelphia, PA
Lawrence Charles Parish, MD, MD (Hon)Philadelphia, PA
Vesna Petronic-Rosic, MD, MSc
Chicago, IL
Marcia Ramos-e-Silva, MD, PhD
Rio de Janeiro, Brazil


March/April 2012
67SKINmed. 2012;10:67–69
There’s a squeak of pure delight from a matey little mite,
As it tortuously tunnels in the skin,
Singing furrow, folly furrow, come and join me in my burrow,
And we’ll view the epidermis from within1
-
2
The cheese-mites asked how the cheese got there,
And warmly debated the matter;
The Orthodox said that it came from the air,
And the Heretics said from the platter.
They argued it long and they argued it strong,
And I hear they are arguing now;
But of all the choice spirits who lived in the cheese,
Not one of them thought of a cow.3
-
4
INCIDENCE
5 -6
7
9
CONTRIBUTING FACTORS
-
ENTOMOLOGY
Sarcoptes scabiei var. Hominis
10
11; 5 Sarcoptes
scabiei 10
11
CLINICAL FEATURES
9 12
From the Department of Dermatology, Altnagelvin Area Hospital, Derry, North Ireland;1 the Department of Dermatology and Cutaneous Biology, Jefferson Center for International Dermatology, Jefferson Medical College of Thomas Jefferson University, Philadelphia, PA;2 and the Dermatology Unit, Kaplan Medical Center, Rechovet, Israel3
Address for Correspondence: Michael Joseph Lavery, MB BCh BAO, Altnagelvin Area Hospital, Department of Dermatology, Glenshane Road, Derry BT47 6SB, North Ireland E-mail: [email protected]
EDITORIAL
Scabies Then and Now Michael Joseph Lavery, MB BCh BAO;1 Lawrence Charles Parish, MD, MD (Hon);2 Ronni Wolf, MD3

March/April 2012
SKINmed. 2012;10:67–69
1 5
14 There 10
15
TREATMENT
-
16
Figure 1. The scabies mite, showing 8 legs.
Figure 2. The characteristic red papules on the finger webs.
Figure 3. Red papules on the penile corona indicating sca-bies, until proven otherwise.
Figure 4. Crusted scabies in an older man who had neglected himself.

March/April 2012
69SKINmed. 2012;10:67–69
17
CONCLUSIONS
5
7
Poor Giovanni Bonomo,
Would be filled with such woe,
To have this tiny little mite,
Still causing affliction by its bite.
REFERENCES
1 Graham-Brown RAC, Burns T. Lecture notes. Dermatology. 9th ed. Malden, MA: Blackwell Publishing; 2007:41–45.
2 Cheese mites and other wonders. BBC News Online. http://news.bbc.co.uk/1/hi/magazine/7423847.stm. Accessed July 30, 2011.
3 Arthur Conan Doyle. A Parable 1916. http://rpo.library.utoronto.ca/poem/3284.html. Accessed July 30, 2011.
4 Ramos-e-Silva M. Giovan Cosimo Bonomo (1663-1696): discoverer of the etiology of scabies. Int J Dermatol. 1998;37;625–630.
5 Vandergriff T, Harting M, Rosen T. Venereal diseases. In: Hall JC, Hall BJ. Skin Infections: Diagnosis and Treatment. Cambridge, England; Cambridge University Press; 2009; Part VI, Ch 24; 317–318.
6 Scabies Homepage. (American incidence) http://www.stanford.edu/group/parasites/ParaSites2005/Scabies/SCABIES.html. Accessed July 30, 2011.
7 Lassa S, Campbell MJ, Bennett CE. Epidemiology of scabies prevalence in the UK from general practice records. Br J Dermatol. 2011;164;1329–1334.
8 Downs AMR, Harvey I, Kennedy CTC. The epidemiology of head lice and scabies in the UK. Epidemiol Infect. 1999;3;471–477.
9 Johnston G, Sladden M. Scabies: diagnosis and treatment. Clinical review. BMJ. 2005;331:619
10 Parasites and Health. Scabies. www.cdc.gov/scabies/risk.html. Accessed July 30, 2011.
11 Harrison S, Knott H, Bergfeld WF. Infections of the Scalp. In: Hall JC, Hall BJ. Skin Infections: Diagnosis and Treatment. Cambridge, England; Cambridge University Press: 2009; Part V, Ch 20; 260.
12 Currie BJ, McCarthy JS. Permethrin and ivermectin for scabies. New Engl J Med. 2010;362;717–725.
13 Cestari TF, Martignago BF. Scabies, pediculosis, bedbugs and stinkbugs: uncommon presentations. Clin Dermatol. 2005;23;545–554.
14 Wolf R, Davidovici B. Treatment of scabies and pediculosis: facts and controversies. Clin Dermatol. 2010;28;511–518.
15 Currie BJ, Harumal P, McKinnon M, et al. First documentation of in vivo and in vitro ivermectin resistance in sarcoptes scabiei. Clin Infect Dis. 2004;39;e8–e12.
16 Wolf R, Davidovici B, Parish LC. Can the scabies mite be tamed? SKINmed. 2006;5:214–216.
17 Cox NH. Permethrin treatment in scabies infestation: importance of the correct formulation. Clinical Review. BMJ. 2000;320:37.
Candidiasis, Infection with Candida albicans. Moulage No 238–239, made by Lotte Volger in the Dermatology Clinic in Zurich in 1923. Museum of Wax Moulages Zurich, www.moulagen.ch
Courtesy of Michael Geiges, MD
WAX MOULAGE

March/April 2012
70SKINmed. 2012;10:70–71
E-
1
2
CASE 1
-
-
Staphylococcus aureus
-
-
CASE 2
-
-
DISCUSSION
-
-
-
3
ORIGINAL CONTRIBUTION
Erlotinib-Induced Scalp PerifolliculitisEfstathios Rallis, MD, PhD;1 Vesna Petronic-Rosic, MD, MSc;2 Chrysovalantis Korfitis, MD1
ABSTRACT
From the Department of Dermatology, Veterans Administration Hospital (NIMTS), Athens, Greece;1 and the Section of Dermatology, University of Chicago Pritzker School of Medicine, Chicago, IL2
-
SKINmed

March/April 2012
71SKINmed. 2012;10:70–71
-
2
-
-
-2
-
-2
-
REFERENCES
1 Cyto-
kine Growth Factor Rev
2 Pathogenesis, clinical significance and management in pancreatic can-
J Pancreas (Online)
3
J Clin Oncol
4 Hautarzt
5 J Drugs Dermatol
Figure 2.
Figure 3.
Figure 4.
Figure 1.

March/April 2012
72SKINmed. 2012;10:72–74
From the Metropolitan Hospital, New York Medical College, New York, NY
Address for Correspondence: Michael J. Fellner, MD, Metropolitan Hospital, New York Medical College, 50 East 89th Street, New York,
T -
-
-
1
CASE 1
-
-
-
-
-
ORIGINAL CONTRIBUTION
New Findings in Delusions of ParasitosisMichael J. Fellner, MD
SKINmed.
ABSTRACT

Delusions of Parasitosis
ORIGINAL CONTRIBUTIONMarch/April 2012
73SKINmed. 2012;10:72–74
CASE 2
A 90-year-old woman was referred from a major medical der-
matology center with a diagnosis of delusions of parasitosis. On
the first visit she described worms and strings coming out of
her body including the skin, eyes, and mouth. She reported the
onset as September 2009 following a bout of diarrhea during
the summer that lasted for 2 months. She was treated with
albendazole by a noted parasitologist for trichuris infection. The
diarrhea abated with the treatment.
By September 2009, she had described worms and strings com-
ing out of her body, causing her great discomfort. She first went
to her primary care physician at the medical school center. He
examined the material she brought and told her there were no
parasites or strings but only mucous. This angered her and she
refused to return to the physician. She brought a drawing of the
worms and strings on her first dermatology visit (Figure 1).
Examination revealed a thin elderly woman in no acute dis-
tress whose stream of thought was verbose and rambling. The
skin showed a reddened and ulcerated area on the right thigh
(Figure 2). The remainder of the physical examination was
within normal limits. Results from laboratory tests were within
normal limits. The patient was given mupirocin ointment for
the ulcer and ammonium lactate 12% lotion for the skin on
the body and was reassured there was some possibility that the
disturbance might abate.
On follow-up 2 weeks later, she claimed the parasites had started
in June 2009, contradicting her previous statement that they had
started in September 2009. She now claimed slight improve-
ment with the treatment. There were, however, new lesions on
the right thigh (Figure 3). Once again she was unclear about
whether these resulted from the parasites. She indicated that the
strings and worms were coming out of her ears, eyes, nose, and
skin on the face.
She was encouraged to take doxepin 25 mg at night and con-
tinue with ammonium lactate 12% lotion and mupirocin oint-
ment. She was also encouraged to ventilate about her multiple
social problems, including her family, her will, and her eating
problems. She said she weighed 87 pounds because she was
unable to eat any carbohydrates since she believed the parasites
lived on sugars. She said she was in the process of getting assis-
tance in daily-living activities at home.
Figure 3. The patient’s thigh lesions on second visit.
Figure 1. The patient’s drawing of string and parasite coming out of her skin.
Figure 2. The patient’s thigh lesion on first visit.

Delusions of Parasitosis
ORIGINAL CONTRIBUTIONMarch/April 2012
74SKINmed. 2012;10:72–74
On third follow-up, she said she felt considerably better
(2 weeks after second visit) using emollients. She did not men-
tion parasites, but said the problem was improving. She was
encouraged to seek psychologic or psychiatric counseling but was
not accepting of this suggestion. She said she was going to make
an appointment for a visit at a nearby medical center geriatric
unit to help her with nutrition and memory problems. She was
encouraged to take doxepin at bedtime and to use emollients.
DISCUSSION
These cases are the first to exhibit findings of Morgellons dis-
ease and delusions of parasitosis at the same time. Morgellons is
a pattern of dermatologic symptoms very similar, if not identi-
cal, to those of delusions of parasitosis, and many patients with
Morgellons are diagnosed with another psychosomatic illness.2 In
delusional parasitosis, patients hold a delusional belief that they
are infested with parasites. They may experience formication, the
sensation that insects are crawling under the skin. It is a common
symptom in cocaine abusers as well. Individuals who experience
this condition may develop elaborate rituals of inspection and
cleansing to locate and remove parasites and fibers, resulting in
a form of self-mutilation; they injure themselves in attempts to
be rid of the “parasites” by picking at the skin, causing second-
ary lesions. Continuous picking of the lesions prevents healing.
Patients with delusional parasitosis often present at the doctor’s
office with what physician’s term the matchbox sign, a medical sign
characterized by the patient making collections of fibers and other
foreign objects supposedly retrieved from the skin, and, because of
“unshakeable delusional ideation,” strongly reject diagnoses that
do not involve parasites. The Morgellons Research Foundation, a
nonprofit organization, considers Morgellons to be a newly emerg-
ing infectious disease, but the medical community disagrees, not-
ing that the described symptoms of Morgellons are associated with
the psychotic disorder known as delusional parasitosis.2
Due to the second patient’s age, it was deemed inappropriate
to give pimozide or treatment with an SSRI medication since
sudden death in the elderly has been reported.3 The treatment
plan was to gain the patient’s confidence before attempting to
refer her for psychologic or psychiatric care, since there did not
appear to be any insight on her part at the first 2 visits.
Therapy is often unsuccessful because many patients, such as
those reported here, refuse consultation with a psychiatrist either
because they believe the problem is organic or because they fear
mental illness and the stigma of psychiatry. In extremely severe
cases, suicide has been reported, illustrating the urgency of cor-
rective medication and prompt psychiatric referral.4 Standard
treatment with pimozide risks substantial side effects.3 This has
led to trial with additional psychotropic agents. Recent success
has been reported with the use of risperdal5 and olanzapine.6
Nowhere have these diseases been more graphically illustrated
than in the Oscar-nominated 2010 film “Black Swan” wherein
the heroine played by Natalie Portman suffers from the delusion
that parasites and strings are coming out of her skin. This is a
must-see film for dermatologists and psychiatrists alike.
REFERENCES
1 Fellner MJ, Majeed MH. Tales of bugs, delusions of parasitosis, and what to do. Clin Dermatol. 2009;27:135–138.
2 Savely VR, Leitao MM, Stricker RB. The mystery of Morgellon’s disease: infection or delusion? Am J Clin Dermatol. 2006;7:1–5.
3 van Vloten WA. Pimozide use in dermatology. Dermatol Online J. 2003;9:3.
4 Monk BE, Rao YJ. Delusions of parasitosis with fatal outcome. Clin Exp Dermatol. 1994;19:341–342.
5 Friedmann AC, Ekeowa-Anderson A, Taylor R, Bewley A. Delusional para-sitosis presenting as folie a trois: successful treatment with risperidone. Br J Dermatol. 2006;155:841–842.
6 Atilganoglu U, Ugurad I, Arikan M, Ergun SS. Monosymptomatic hypo-chondriacal psychosis presenting with recurrent oral mucosal ulcers and multiple skin lesions responding to olanzapine treatment. Int J Dermatol. 2006;45:1189–1192.
VINTAGE LABEL
Courtesy of BuyEnlarge, Philadelphia, PA

March/April 2012
75SKINmed. 2012;10:75–81
March/April 2012
From the Wound Healing Center, Hebrew Senior Life Department of Medicine, Boston, MA
Address for Correspondence: E. Foy White-Chu, MD, Director of Wound Healing Center, Hebrew Senior Life Department of Medicine, 1200
1 2
3
4
CASE 1: SKIN TEAR THAT IS SLOW TO HEAL
REVIEW
Wound Care in Short-Term Rehabilitation Facilities and Long-Term Care: Special
Needs for a Special PopulationE. Foy White-Chu, MD; Madhuri Reddy, MD, MSc
SKINmed.
ABSTRACT

March/April 2012
76SKINmed. 2012;10:75–81
SKIN TEARS
5–7
6
VENOUS ULCERS
8
10
11 12
10
Figure 1. Venous ulcer status post-debridement. Photo courtesy of E. Foy White-Chu, MD.
Figure 2. Proper wrapping technique on the right leg. Note the inclusion of the heel from toes to knee. Photo courtesy of E. Foy White-Chu, MD.
Table I. Prevention of Skin Tears
DO DON ’ T

March/April 2012
77SKINmed. 2012;10:75–81
13 14
15
stocking
16
17
16
18
17
CASE 2: STAGE IV PRESSURE ULCER AND FEVER
Table II. Venous Ulcer Challenges and Treatments
PROBLEM APPROACH

March/April 2012
78SKINmed. 2012;10:75–81
PRESSURE ULCERS
20
21 22
23
24
22
24 25
Figure 3. -
courtesy of E. Foy White-Chu, MD.
Figure 4. Healing stage IV pressure ulcer. Photo courtesy of E. Foy White-Chu, MD.

March/April 2012
SKINmed. 2012;10:75–81
26 27
28
30
24 25 31 32
Staphylococcus aureus33–35
CASE 3: TOE ULCERS AND REFRACTORY PAIN
PALLIATIVE WOUND CARE
Figure 5: Worsening arterial ulcers. Photo courtesy of E. Foy White-Chu, MD.

March/April 2012
80SKINmed. 2012;10:75–81
36
37 38
CONCLUSIONS
Disclosure: The authors declare no financial interests. There was no
funding source provided for this contribution.
REFERENCES
1 hospital stay. Infect Control Hosp Epidemiol. 2005;26:293–297.
2 Belowitz DR, Brandeis GH, Anderson J, Du W, Brand H. Effect of pres-J Gerontol A Biol
Sci Med Sci. 1997;52:M106–M110.
3
4
5 Cough-Csarny J, Kopac CA. Skin tears in institutionalized elder-ly: an epidemiological study. Ostomy Wound Manage. 1998;44(3A suppl):14S–24S.
6 Ostomy Wound Manage. 2007;53:32–34, 36,
38–40.
7 J Wound Ostomy Continence Nurs. 2007;34:256–259.
8 --
tion using MDS. Adv Skin Wound Care. 2000;13:218–224.
9 -
study. Arch Surg. 2001;136:1364–1369.
10 Br J Surg.
1999;86:338–341.
11 quality of life. Ostomy Wound Manage. 1998;44:38–49.
12 their impact on daily life. J Clin Nurs. 2004;13:341–354.
13
ulceration. Wound Repair Regen. 2003;11:166–171.
14 BMJ. 1997;315:576–580.
15 Chronic
Wound Care: A Clinical Source Book for Healthcare Professionals. 4th ed. Wayne, PA: Health Management Publications, Inc; 2007:481–488.
16 Romanelli M, Dini V, Willliamson D, et al. Measurement: lower
Chronic Wound Care: A Clinical Source Book for Healthcare Professionals, Fourth Edition. Wayne, PA: Health Manage-ment Publications, Inc; 2007:463–480.
17 Palfreyman SSJ, Nelson EA, Lochiel R, Michaels JA. Dressings for healing Cochrane Database Syst Rev. 2006;(3):CD001103.
18 Second European Consensus Document on chronic critical leg ischemia. Circulation. 1991;84(4 suppl):IV1–IV26.
19
20 Langemo DK, Brown G. Skin fails too: acute, chronic, and end-stage skin failure. Adv Skin Wound Care. 2006;19:206–211.
21 -
sory Panel monograph. Adv Skin Wound Care. 2001;14:208–215.
22 Allman RM, Goode PS, Patrick MM, et al. Pressure ulcer risk fac-JAMA.
1995;273:865–870.
23 -J Am Geriatr
Soc. 2000;48:73–81.
24 debridement, bacterial balance and moisture balance. Ostomy Wound Manage. 2000;46:14–22, 24–28, 30–35.
25 Schultz GS, Sibbald RG, Falanga V, et al. Wound bed preparation: a sys-temic approach to wound management. Wound Rep Reg. 2003;11:1–28.
26 West J Med. 1991;154:219–223.

March/April 2012
81SKINmed. 2012;10:75–81
27 Allen C, Glasziou P, Del Mar C. Bed rest: a potentially harmful treatment Lancet. 1999;354:1229–1233.
28 Treatment of Pressure Ulcers: Quick Reference Guide.
29 JAMA. 2008;300:2647–2662.
30 Cullum N, McInnes E, Bell-Syer SEM, Legood R. Support surfaces
31 Sibbald RG, Woo K, Ayello EA. Increased bacterial burden and infection: the Adv Skin Wound Care. 2006;19:447–461.
32 Drosou A, Falabella A, Kirsner RS. Antiseptics on wounds: an area of Wounds. 2003;15:149–166.
33 Am J Surg. 1986;151:400–406.
34 -
J Clin Pathol. 1976;29:752–755.
35 -
Postgrad Med J.
1993;69 suppl 3:S78–S83.
36 -
Chronic Wound
Care: A Clinical Source Book for Healthcare Professionals, Fourth Edi-
tion. Wayne, PA: Health Management Publications, Inc; 2007:443–449.
37 neuropathy with isosorbide dinitrate spray: a double-blind placebo-
Diabetes Care. 2002; 25:1699.
38 ulcers with nitroglycerin ointment. J Dermatol Surg Oncol. 1983;9:548.
SELF-TEST REVIEW QUESTIONSW. Clark Lambert, MD, PhD, Section EditorInstructions: For each of the following numbered questions, choose the appropriate lettered response(s). Unless directed to choose only one lettered response, all, some, or none of the responses may be correct.
1) skin tears in elderly patients are: (Choose the single best
response.)
a. facilities.
b.
c.
d. and waiting rooms.
e. bedroom.
2) (Choose the single best response.)
a. b. fourteen days.
c. d. e. three months.
3) Which of the following statements regarding treatment of
(Answer as many as apply.)
a. Compression is the most important aspect for
b. c. Arterial disease is not a contraindication for treatment
with compression.
d. -
cation for treatment with compression.
e. f.
compression treatment.
4) blood flow in: (Choose the single best response.)
a. elderly patients.
b. patients with diabetes mellitus.
c. d. e. all of these are correct.
5) Nitroglycerin patches should be applied: (Answer as many
as apply.)
a. early in management of all symptomatic ulcers in
b. early in management of all symptomatic ulcers in
patients who smoke more than one pack of cigarettes
per day.
c. for pain management only.
d. e.
potential to heal.
ANSWERS TO SELF-TEST REVIEW QUESTIONS:
1) e 2) c; 3) a, d, e; 4) e; 5) c, e

March/April 2012
82SKINmed. 2012;10:82–89
CORE CURRICULUMVirendra N. Sehgal, MD, Section Editor
Cutaneous Tuberculosis: A Diagnostic Dilemma— Laboratory Inputs
Virendra N. Sehgal, MD; Prashant Verma, MD; Sambit N. Bhattacharya, MD; Sonal Sharma, MD; Navjeevan Singh, MD; Nishant Verma, MD
-
-
DIAGNOSTIC MODALITIES
SKIN TESTS
TUBERCULIN TEST
-
-
proviso
-
-1
-2
-
6
7
6
MYCOBACTERIAL ANTIGEN, MPB64 TRANSDERMAL PATCH TEST
-8
9
INTERFERON-γ RELEASE ASSAYS
QUANTIFERON-TB GOLD TEST
Mycobacterium tuberculosis
Bacterial cultures are the gold standard for diagnosing cutaneous tuberculosis, but there are limitations, despite the advances embracing the innovative technologies, including interferon γ release assays, enzyme-linked immunoabsorbant assay, and molecular diagnostics, in addition to conventional skin tests and microscopic pathology. The results and their interpretation of cultures are reviewed for use in day-to-day practice.
From the Dermato-Venereology (Skin/VD) Center, Sehgal Nursing Home, Panchwati, Delhi; Department of Dermatology and STD, Department of Pathology, University College of Medical Sciences and Associated Guru Teg Bahadur Hospital, Delhi; Department of Microbiology, Maulana Azad Medical College and Associated Chacha Nehru Bal Chikitsalaya, Delhi, India
E-mail: [email protected]

March/April 2012
SKINmed. 2012;10:82–89
γ γ-
-
10
-11 -
γ
γγ
-
M tuber-
culosis 12
T-SPOT.TB TEST
M tuberculosis γ -
γ
-
γ -
-
γ -
-
-
12
MICROSCOPIC PATHOLOGY
FINE-NEEDLE ASPIRATION CYTOLOGY
-
16
-
-
-
17
HISTOPATHOLOGIC UNDERTONES
-18 19
SCROFULODERMA
-
-20 21

March/April 2012
SKINmed. 2012;10:82–89
TB CUTIS ORIFICIALIS
-
20
TUBERCULOUS GUMMA
-
Figure 1. (A) Cohesive epithelioid cell granuloma in an aspirate from a cervical lymph node (May-Grunwald-Giemsa stain, magnification ×400). (B) Single acid-fast bacillus in a fine-needle aspirate smear from a lymph node (Ziehl-Neelsen stain, magnification ×400).
A
B
Figure 2. Tuberculosis verrucosa cutis: Section show-ing marked hyperkeratosis and acanthosis. Epithelioid cell granulomas mixed with neutrophilic abscesses is prominent in the upper dermis (hematoxylin-eosin stain, original magnification ×40). Inset: hematoxylin-eosin stain, original magnification ×400.
DISSEMINATED MILIARY TB
TB VERRUCOSA CUTIS
22
LUPUS VULGARIS
LICHEN SCROFULOSORUM
-

March/April 2012
SKINmed. 2012;10:82–89
ERYTHEMA INDURATUM OF BAZIN
-
-
PAPULONECROTIC TUBERCULIDS
-
IMMUNOHISTOCHEMISTRY
M tuberculosis
M tuber-
culosis
-
-
-
26
Figure 4. Lichen scrofulosorum: Section showing perifollicular epithelioid cell granulomas with relative sparing of arrector pili muscle (hematoxylin-eosin stain, original magnification ×100).
Figure 5. Erythema induratum: Section showing septal pannicultis, vascular damage, neutrophil and macrophage infiltrate in the vessel wall, and thrombosis (hematoxylin-eosin stain, original magnification ×40). Inset: hematoxylin-eosin stain, original magnification ×400.
Figure 3. Lupus vulgaris: Section showing epithelioid cell granulomas with conspicuous prominent giant cells extending to mid-dermis along with hyperplastic epithelium depicting hyperkeratosis and acanthosis (hematoxylin-eosin stain, original magnification ×40). Inset: hematoxylin-eosin stain, original magnification ×100.

March/April 2012
86SKINmed. 2012;10:82–89
ISOLATION AND IDENTIFICATION OF M TUBERCULOSIS, IN VITRO CULTURE AND GUINEA PIG INOCULATION
IN VITRO RECOVERY OF M uberculosis
-
27–29
29
BACTEC SYSTEM
-
-
BACTEC MGIT 960 SYSTEM
-
MB-REDOX
-
MB CHEK (BIPHASIC MEDIUM)M tuberculosis
M tuberculosis
GUINEA PIG INOCULATION
-
IMMUNOCHROMATOGRAPHY
M tuberculosis
-
-
-
M
tuberculosis
HIGH-PERFORMANCE LIQUID CHROMATOGRAPHY
M tuberculosis
ENZYME-LINKED IMMUNOSORBENT ASSAY
-
-
-

March/April 2012
87SKINmed. 2012;10:82–89
MOLECULAR DIAGNOSIS
M tuberculosis -
-
M tuberculosis
M tuberculosis
-
-
M tuberculosis -
M tuberculo-
sis
M
tuberculosis
M tuberculosis
M tuberculosis
-
M tuberculosis
REAL-TIME PCR TECHNIQUE
-
M tuberculosis
DNA PROBES
–20
M tuberculo-
sis Mycobacterium avium
-
RIBOSOMAL RRNA-BASED PROBES
-
M tuberculosis,
Mycobacterium leprae M avium.
-
GENE AMPLIFICATION METHODS FOR IDENTIFICATION

March/April 2012
88SKINmed. 2012;10:82–89
-
-
kat
M tuberculosis -
ANTITUBERCULAR THERAPY AS A DIAGNOSTIC ADJUNCT
-
-
-
CONCLUSIONS
REFERENCES
1 World Health Organization: The WHO standard tuberculin test 1963.WHO/TB/Tech guide/3, Chahda VK. Tuberculin test. Ind J Paed. 2001;68:53–58.
2 Frankel A, Penrose C, Emer J. Cutaneous tuberculosis: a practical case report and review for the dermatologist. J Clin Aesthet Dermatol. 2009;2:19–27.
3 Brown FS, Anderson RH, Burnett JW. Cutaneous tuberculosis. J Am Acad Dermatol. 1982;6:101–106.
4 MacGregor RR. Cutaneous tuberculosis. Clin Dermatol. 1995;13:245–255.
5 Frankel A, Penrose C, Emer J. Cutaneous tuberculosis: a practical case report and review for the dermatologist. J Clin Aesthet Dermatol. 2009;2:19–27.
6 Pereira J. Tuberculids. Rev Port Pneumol. 2004;10:97–105.
7 Marcoval J, Servitje O, Moreno A, et al. Lupus vulgaris. Clinical, histo-pathologic, and bacteriologic study of 10 cases. J Am Acad Dermatol. 1992;26:404–407.
8 Nakamura RM, Einck L, Velmonte MA, et al. Detection of active tubercu-losis by an MPB-64 transdermal patch: a field study. Scand J Infect Dis. 2001;33:405–407.
9 Nakamura RM, Velmonte MA, Kawajiri K, et al. MPB64 mycobacterial an-tigen: a new skin-test reagent through patch method for rapid diagnosis of active tuberculosis. Int J Tuberc Lung Dis. 1998;2:541–546.
10 National Tuberculosis Controllers Association; Centers for Disease Con-trol and Prevention (CDC) Guidelines for the investigation of contacts of persons with infectious tuberculosis. Recommendations from the National Tuberculosis Controllers Association and CDC. MMWR Recomm Rep. 2005;54(RR-15).
11 Bocchino M, Chairadonna P, Matarese A, et al. Limited usefulness of QuantiFERON-TB Gold In-Tube for monitoring anti- tuberculosis therapy. Respir Med. 2010;104:1551–1556.
12 Centers for Disease Control and Prevention. Updated Guidelines for Using Interferon Gamma Release Assays to Detect Mycobacterium Tu-berculosis Infection, United States. MMWR. 2010;59(No.RR-5).
13 Ribeiro S, Dooley K, Hackman J, et al. T-SPOT.TB responses during treat-ment of pulmonary tuberculosis. BMC Infect Dis. 2009;9:23.
14 Huo FF, Zhang LF, Liu XQ. Sensitivity of interferon-gamma release assay T-SPOT.TB in diagnosing extrapulmonary tuberculosis. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2009;31:449–452.
15 Domínguez J, De Souza-Galvão M, Ruiz-Manzano J, et al. T-cell responses to the Mycobacterium tuberculosis-specific antigens in active tuberculo-sis patients at the beginning, during, and after antituberculosis treat-ment. Diagn Microbiol Infect Dis. 2009;63:43–51.
16 Kathuria P, Agarwal K, Koranne RV. The role of fine-needle aspiration cytology and Ziehl Neelsen staining in the diagnosis of cutaneous tuber-culosis. Diagn Cytopathol. 2006;34:826–829.
17 Bezabih M, Mariam DW, Selassie SG. Fine needle aspiration cytology of suspected tuberculous lymphadenitis. Cytopathology. 2002;13:284–290.
18 Elder DE, Elenitsas R, Ioffreda MD, et al. Atlas and Synopsis of Lever’s Histopathology of the Skin. 2nd ed. Philadelphia, PA: Lipincott Willams & Wolters Kluwer; 2007:230.
19 Bravo FG, Gotuzzo E. Cutaneous tuberculosis. Clin Dermatol. 2007;25:173–180.
20 Baek SE, Kang WH, Lee KH. Tuberculosis cutis orificialis. Korean J Der-matol. 1985;23:667–671.
21 Singal A, Bhattacharya SN. Lichen scrofulosorum: a prospective study of 39 patients. Int J Dermatol. 2005;44:489–493.
22 Sehgal VN, Sardana K, Bajaj P, Bhattacharya SN. Tuberculosis verrucosa cutis: antitubercular therapy, a well-conceived diagnostic criterion. Int J Dermatol. 2005;44:230–232.
23 Sehgal VN. Lichen scrofulosorum: current status. Int J Dermatol. 2005;44:521–523.
24 Padmavathyi L, Rao LL, Ramanadhan, et al. Mycobacterial antigen in tissues in diagnosis of cutaneous tuberculosis. Indian J Tuberc. 2005;52:31–35.
25 Mustafa T, Wiker HG, Mfinanga SG, et al. Immunohistochemistry using a Mycobacterium tuberculosis complex specific antibody for improved diagnosis of tuberculous lymphadenitis. Mod Pathol. 2006;19:1606–1614.
26 Kutzner H, Argenyi ZB, Requena L, et al. A new application of BCG anti-body for rapid screening of various tissue microorganisms. J Am Acad Dermatol. 1998;38:56–60.
27 Fariña MC, Gegundez MI, Piqué E, et al. Cutaneous tuberculosis: a clinical, histopathologic, and bacteriologic study. J Am Acad Dermatol. 1995;33:433–440.
28 Brown FS, Anderson RH, Burnett JW. Cutaneous tuberculosis. J Am Acad Dermatol. 1982;6:101–106.
29 API TB Consensus Guidelines 2006: Management of pulmonary tuber-culosis, extra-pulmonary tuberculosis and tuberculosis in special situa-tions. J Assoc Physicians India. 2006;54:219–234.
30 Diagnostic Standards and Classification of Tuberculosis in Adults and Children. This official statement of the American Thoracic Society and the Centers for Disease Control and Prevention was adopted by the ATS Board of Directors, July 1999. This statement was endorsed by the Council of the Infectious Disease Society of America, September 1999. Am J Respir Crit Care Med. 2000;161:1376–1395.

March/April 2012
89SKINmed. 2012;10:82–89
31 Aggarwal P, Singal A, Bhattacharya SN, et al. Comparison of the radio-metric BACTEC 460 TB culture system and Löwenstein-Jensen medium for the isolation of mycobacteria in cutaneous tuberculosis and their drug susceptibility pattern. Int J Dermatol. 2008;47:681–687.
32 Tortoli E, Cichero P, Piersimoni C, et al. Use of BACTEC MGIT 960 for recovery of mycobacteria from clinical specimens: multicenter study. J Clin Microbiol. 1999;37:3578–3582.
33 Piersimoni C, Scarparo C, Cichero P, et al. Multicenter evaluation of the MB-Redox medium compared with radiometric BACTEC system, myco-bacteria growth indicator tube (MGIT), and Löwenstein-Jensen medium for detection and recovery of acid-fast bacilli. Diagn Microbiol Infect Dis. 1999;34:293–299.
34 Luquin M, Gamboa F, Barcelo MG, et al. Comparison of a biphasic non radiometric system with Lowenstein Jensen and BACTEC 460 system for recovery of mycobacteria from clinical samples. Tuber Lung Dis. 1996;77:449–453.
35 Piersimoni C, Morbiducci V, De Sio G, et al. Comparative evaluation of the MB-check system for recovery of mycobacteria from clinical speci-mens. Eur J Clin Microbiol Infect Dis. 1992;11:1174–1177.
36 Abe C, Hosojima S, Fukasawa Y, et al. Comparison of MB chek, BACTEC and egg-based media for recovery of mycobacteria. J Clin Microbiol. 1992;30:878–881.
37 Pallen MJ. The inoculation of tissue specimens into guinea-pigs in sus-pected cases of mycobacterial infection does it aid diagnosis and treat-ment? Tubercle. 1987;68:51–57.
38 Peluffo G, de Kantor IN. Bacteriologic diagnosis of extrapulmonary tuberculosis in a general hospital. Rev Argent Microbiol. 1982;14:91–96.
39 Schneider JW, Jordaan HF, Geiger DH, et al. Erythema induratum of Bazin. A clinicopathological study of 20 cases and detection of Mycobacterium tuberculosis DNA in skin lesions by polymerase chain reaction. Am J Dermatopathol. 1995;17:350–356.
40 Hasegawa N, Miura T, Ishii K, et al. New simple and rapid test for cul-ture confirmation of Mycobacterium tuberculosis complex: a multicenter study. J Clin Microbiol. 2002;40:908–912.
41 Jost KC, Chiu SH, Kenney TM, et al. American Society for Microbiology. General Meeting. Identification and quantitation of Mycobacterium tuber-culosis directly from clinical specimens by fluorescence detection high-performance liquid chromatography. Abstr Gen Meet Am Soc Microbiol. 1997;97:568.
42 Charpin D, Herbault H, Gevaudan MJ, et al. Value of ELISA using A 60 antigen in the diagnosis of active pulmonary tuberculosis. Am Rev Respir Dis. 1990;142:380–384.
43 Arya L, Koranne RV, Deb M. Cutaneous tuberculosis in children a clinico-microbiological study. Indian J Dermatol Venereol Leprol. 1999;65:137–139.
44 Rao L, Padmavathy L. Utility of MycoDot test in the diagnosis of cutane-ous tuberculosis. Indian J Dermatol Venereol Leprol. 2003;69:428–429.
45 Balasingham SV, Davidsen T, Szpinda I, et al. Molecular diagnostics in tuberculosis: basis and implications for therapy. Mol Diagn Ther. 2009;13:137–151.
46 Honoré-Bouakline S, Vincensini JP, Giacuzzo V, et al. Rapid diagnosis of
extrapulmonary tuberculosis by PCR: impact of sample preparation and
DNA extraction. J Clin Microbiol. 2003;41:2323–2329.
47 Cheng VC, Yew WW, Yuen KY. Molecular diagnostics in tuberculosis. Eur
J Clin Microbiol Infect Dis. 2005;24:711–720.
48 Abdalla CM, de Oliveira ZN, Sotto MN, et al. Polymerase chain reac-
tion compared to other laboratory findings and to clinical evaluation in
the diagnosis of cutaneous tuberculosis and atypical mycobacteria skin
infection. Int J Dermatol. 2009;48:27–35.
49 Padmavathy L, Rao L, Veliath A. Utility of polymerase chain reaction as
a diagnostic tool in cutaneous tuberculosis. Indian J Dermatol Venereol
Leprol. 2003;69:214–216.
50 Salian NV, Rish JA, Eisenach KD, et al. Polymerase chain reaction to
detect Mycobacterium tuberculosis in histologic specimens. Am J Respir
Crit Care Med. 1998;158:1150–1155.
51 Ortu S, Molicotti P, Sechi LA, et al. Rapid detection and identification of
Mycobacterium tuberculosis by Real Time PCR and Bactec 960 MIGT.
New Microbiol. 2006;29:75–80.
52 Katoch VM. Newer diagnostic techniques for tuberculosis. Indian J Med
Res. 2004;120:418-428.
53 Katoch VM, Kanaujia GV, Shivannavar CT, et al. Progress in developing
ribosomal RNA and rRNA gene(s) based probes for diagnosis and epi-
demiology of infections diseases specially leprosy. In: Sushil Kumar, Sen
AK, Dutta GP, Sharma RN, eds. Tropical Diseases—Molecular Biology and
Control Strategies. 1st ed. New Delhi, India: Council for Scientific and
Industrial Research; 1994:581–587.
54 Roth A, Reischl U, Streubel A, Naumann L, et al. Novel diagnostic algo-
rithm for identification of mycobacteria using genus specific amplifica-
tion of 16S-23S rRNA gene spacer and restriction endonucleases. J Clin
Microbiol. 2000;38:1094–1104.
55 Sehgal VN, Sardana K, Bajaj P, et al. Tuberculosis verrucosa cutis: anti-
tubercular therapy, a well-conceived diagnostic criterion. Int J Dermatol.
2005;44:230–232.
56 Sehgal VN, Sardana K, Sehgal R, et al. The use of anti-tubercular therapy
(ATT) as a diagnostic tool in pediatric cutaneous tuberculosis. Int J Der-
matol. 2005;44:961–963.
57 Ramam M, Mittal R, Ramesh V. How soon does cutaneous tuberculosis
respond to treatment? Implications for a therapeutic test of diagnosis. Int
J Dermatol. 2005;44:121–124.
58 Sehgal VN, Sardana K, Sharma S. Inadequacy of clinical and/or laboratory
criteria for the diagnosis of lupus vulgaris, re-infection cutaneous tuberculo-
sis: fallout/implication of 6 weeks of anti-tubular therapy (ATT) as a precise
diagnostic supplement to complete the scheduled regimen. J Dermatolog
Treat. 2008;19:164–167.
FORMULARY OF DR GEORGE C. ANDREWS
LIQUID ROUGE
Carmine gr.v
Aq. Ammon mx.v
Alcohol 3 i ss
Ol. Rose gtt.1
Aq. Rosae 3 i
Mix and filter
Submitted by Douglas D. Altchek, MD, New York, NY.

March/April 2012
90SKINmed. 2012;10:90–92
From the Class of 2012, New Jersey Medical School, Newark, NJ;1 the Departments of Pathology and Dermatology, UMDNJ-New Jersey Medical School, Newark, NJ;2 and the Class of 2015, St. George’s University School of Medicine, Grenada, West Indies3
Address for Correspondence: W. Clark Lambert, MD, PhD, Room C520 MSB, UMDNJ-NJMS, 185 South Orange Avenue, Newark, NJ 07103
K -1 -
2
-
3
-
-4 5
6
7 8
-9 10
-
CHARACTERISTICS
-
-
-
11
12
12 13
PERILS OF DERMATOPATHOLOGYW. Clark Lambert, MD, PhD, Section Editor
Sometimes It Takes Darkness to See the Light: Pitfalls in the Interpretation of Cell Proliferation
Markers (Ki-67 and PCNA) Carmen Castilla, BS;1 Patrick McDonough, BA;1 Gizem Tumer, MD;2 Peter C. Lambert, BA, MS;3
W. Clark Lambert, MD, PhD2
“[Clarity], like a photograph, develops in the dark.

March/April 2012
91SKINmed. 2012;10:90–92
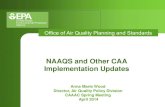
Figure 1. (A) Multiple nests of melanocytes are shown in malignant melanoma. (B) Ki-67 immunostain showing increased reactivity. Black arrowhead indicates a melanin pigment. Red arrowheads indicate increased Ki-67 labeling in or above the basal layer, indica-tive of cell proliferation or of ultraviolet exposure within the previous 24 hours. Full black arrows indicate a hypocellular dermis, indicative of long term ultraviolet exposure.
Figure 2. showing increased Ki-67 proliferation index above the basal layer (arrowheads) due to ultraviolet exposure.
Figure 3. DNA replication fork illustrating DNA synthesis along the leading and lagging strand. Proliferating cell nuclear antigen (PCNA) is shown in pink acting as a clamp to secure polymerase delta (shown in green) and polymerase epsilon (shown in teal) to the DNA strand, allowing for greater efficiency of nucleotide addition.

March/April 2012
92SKINmed. 2012;10:90–92
14
-
15 -
16
CONCLUSIONS
-
-
-
-
REFERENCES
1 Scholzen T, Gerdes J. The Ki-67 protein: from the known and the unknown. J Cell Physiol. 2000;182:311–322.
2 Duchrow M, Schluter C, Wholenberg C, Flad HD, Gerdes J. Molecular characterization of the gene locus of the human cell proliferation- associated nuclear protein defined by monoclononal antibody Ki-67. Cell Prolif. 1996;29:1–12.
3 Schmidt M, Broll R, Bruch H, Duchrow M. Proliferation marker pKi-67 affects the cell cycle in a self regulated manner. J Cell Biochem. 2002;87:334–341.
4 Soyer HP. Ki 67 immunostaining in melanocytic skin tumors. Correlation with histological parameters. J Cutan Pathol. 1991;18:264–272.
5 of p27kip1, p45skp2 and Ki67 expression profiles in Merkel cell
carcinoma, extracutaneous small cell carcinoma, and cutaneous squamous cell carcinoma. Histopathology. 2005;46:614–621.
6 Chen GS, Wu TM, Yang SA, Yu HS. Quantitative assessments of physiological and biological parameters in psoriatic lesions and its correlations to the clinical severity of psoriasis. Kaohsiung J Med Sci. 2001;17:408–418.
7 Yazici AC, Tursen U, Apa DD, et al. The changes in expression of icam-3, ki-67, pcna, and cd31 in psoriatic lesions before and after methotrexate treatment. Arch Dermatol Res. 2005;297:249–255.
8 -noic acid metabolism blocking agent rambazole for plaque pso-riasis: an immunohistochemical study. Br J Dermatol. 2005;156:263–270.
9 keratinocyte proliferation and epidermal hyperplasia through the activation of the epidermal growth factor receptor. Carcinogenesis. 2006;27:225–231.
10 expression of Ki-67, topoisomerase IIalpha, PCNA, p53 and p21WAF1/Cip1 reflecting proliferation and repair activity in UV-irradiated melano-cytic nevi. Hum Pathol. 1998;29:1480–1487.
11 Overmeer RM, Gourdin AM, Giglia-Mari A, et al. Replication factor C recruits DNA polymerase delta to sites of nucleotide excision repair but is not required for PCNA recruitment. Mol Cell Biol. 2010;30:4828–4839.
12 on the expression of proliferating cell nuclear antigen in murine skin. Photochem Photobiol. 2004;80:587–595.
13 proteins (proliferating cell nuclear antigen and Ki-67 antigen) in Bowen’s disease. Br J Dermatol. 1994;131:231–236.
14 Hall PA, McKee PH, Menage HD, Dover R, Lane DP. High levels of p53 pro-tein in UV-irradiated normal human skin. Oncogene. 1993;8:203–207.
15 Freudenthal BD. Studies of proliferating cell nuclear antigen and its role in translesion synthesis [PhD dissertation]. Iowa City: University of Iowa; 2010.
16 McDonough P, Castilla C, Tumer G, Lambert WC. Interpretation of Ki-67 stain confounded by patient exposure to ultraviolet radiation prior to skin biopsy. J Euro Acad Venereol Dermatol. [In press.]
VINTAGE LABEL

Soothing and alcohol-free — part of a complete approach to acne treatment
TM C A L M I N G
WIPES(30 WIPES)
Complementary T3 Calming Wipes
A dual approach to acne care
ONE PRESCRIPTION.TWO POWERFUL EFFECTS.
The power to eradicate P acnesSignificant reduction in P acnes—even up to 3 weeks after discontinuation2
A decrease in P acnes can lead to a drop in pro-inflammatory cytokines and reduced inflammation1
Minimal resistance in an in vitro study
—The majority of tetracycline-resistant P acneswere cross-resistant to doxycycline—but sensitive to minocycline*3
The power to calm inflammatory acneInflammation is an important aspect in the pathophysiology of acne1
Both laboratory and clinical studies document the anti-inflammatory effects of minocycline1
+
The most common adverse events associated with MINOCIN are nausea, vomiting, and diarrhea. CNS adverse effects may includedizziness, vertigo, and headache.
References: 1. SapadinAN,Fleischmajer R.Tetracyclines:nonantibiotic properties and their clinical implications.JAmAcad Dermatol. 2006;54(2):258-265. 2. Leyden JJ,McGinley KJ,KligmanAM.Tetracycline and minocyclinetreatment.Arch Dermatol. 1982;118(1):19-22. 3. Hubbell CG,Hobbs ER,RistT,White JW Jr.Efficacy of minocycline compared with tetracycline in treatment of acne vulgaris.Arch Dermatol.1982;118(12):989-992.
*In vitro activity does not necessarily correlate to in vivo activity.
©2010 Triax Pharmaceuticals, LLC All rights reserved. Printed in USA. MN-0810-280
Important InformationThe most common adverse events associated with MINOCIN are nausea, vomiting, and diarrhea. Central nervous system adverse events includinglight-headedness, dizziness, or vertigo have been reported with minocycline therapy, but are generally transient in nature. Other adverse eventsinclude tinnitus, headache, sedation, and skin pigmentation, particularly on the face and mucous membranes. MINOCIN is contraindicated in personswho have shown hypersensitivity to any of the tetracyclines or to any of the components of the product formulation. WARNING: MINOCIN Pellet-Filled Capsules, like other tetracycline-class antibiotics, can cause fetal harm when administered to a pregnant woman. The use of drugs of thetetracycline class during tooth development (last half of pregnancy, infancy, and childhood to the age of 8 years) may cause permanent discoloration of teeth (yellow-gray-brown). Concurrent use of tetracyclines may render oral contraceptives less effective.
For more information, go to www.minocin-kit.com
The only pelletized form of Minocycline available...

March/April 2012
94SKINmed. 2012;10:94–97
A
-
-
-
Mycobacterium leprae
-
1 2
4 5
DIAGNOSIS
CLINICAL PRESENTATION
-
-
-
-
M leprae
-
-
INFECTIOUS DISEASE CAPSULESJack M. Bernstein, MD, Section Editor
The Lion Is NOT Sleeping Tonight David R. Carr, MD;1,4 Jack M. Bernstein, MD;2,3 Julian Trevino, MD1,4
From Medical1 and Research2 Services, VA Medical Center, Dayton, OH; and the Department of Medicine3 and the Department of Dermatology,4 Boonshoft School of Medicine, Wright State University, Dayton, OH

March/April 2012
95SKINmed. 2012;10:94–97
-
-
7
-
M leprae
-
Figure 3.
Figure 2. Multiple, 2–8 mm dermal papules over the dorsal surface of the feet.Figure 1. Multiple, 2–8 mm dermal papules over the ears.
-

March/April 2012
SKINmed. 2012;10:94–97
-
9
DIAGNOSTIC TOOLS
-
M leprae -10
4
M leprae
11
M leprae -
12
M leprae.
M leprae -
TREATMENT
-14
-
-
1 15
Table I. Ridley-Jopling Leprosy Classification
CATEGORIES CLINICAL FINDINGS NERVE INVOLVEMENT BACILLI PRESENCE
−
+/−
+/−
-
culoid+
-+
+/−

March/April 2012
97SKINmed. 2012;10:94–97
M leprae
-
CONCLUSIONS
-
REFERENCES
1 Clin Dermatol. 2007;25:165–172.
2 Global leprosy situation. Wkly Epidemiol Rec. 2005;80:289–295. 25:165–172.
3 Global leprosy situation. Wkly Epidemiol Rec. 2005;80:289–295.
4 nia J, Jorizzo JL, Rapini RP. Dermatology1145–1152.
5 Canizares O, Harman R, Adriaans B. Leprosy. In: Clinical Tropi-cal Dermatology165–200.
6 Int J Lepr. 1966;34:255–273.
7 impairment in leprosy: design, methodology, and intake status of a
Lepr Rev. 1999;70:140–159.
8 Quismorio FP, Rea T, Chandors, et al. Lucio’s phenomenon: an immune complex deposition syndrome in lepromatous leprosy. Clin Immunol Immunopathol. 1978;9:184–193.
9 Kaur C, Thami GP, Mohan H. Lucio phenomenon and Lucio leprosy. Clin Exp Dermatol. 2005;30:525–527.
10 Job CKreference to early diagnosis and leprous neuropathy. Indian J Lepr. 2007;79:75–83.
11 Silva EA, Iyer A, Ura S, et al. Utility of measuring serum levels of
Trop Med Int Health. 2007;12:1450–1458.
12 Kamal R, Dayal R, Katoch VM, Katoch K. Analysis of gene probes and
in childhood leprosy. Lepr Rev. 2006;77:141–146.
13 Scollard DM, Adams LB, Gillis TP, et al. The continuing challenges of leprosy. Clin Microbiol Rev. 2006;19:338–381.
14
15 World Health Organization. Chemotherapy of leprosy for control programmes. Tech Rep Ser Geneva. 1982:675.
Table II. Multidrug Therapy: World Health Organization Guidelines14
TYPE OF LEPROSY TREATMENT REGIMEN
TREATMENT DURATION

March/April 2012
98SKINmed. 2012;10:98
From the Department of Dermatology, Nelson R. Mandela School of Medicine, Durban, South Africa
PHOTO CAPSULESNcoza C. Dlova, MBChB, FCDerm, Section Editor
ActinomycetomaNcoza C. Dlova, MBChB, FCDerm; Anisa Mosam, MBChB, FCDerm
A Norcadia brasiliensis
Figure 1. Actinomycetoma of the right foot. Figure 2. Actinomycetoma of the groin.
VINTAGE LABEL

University of AthensMedical School,Athens, Greece
DERMATOLOGYOF COSMETICWORLD CONGRESS
BY THE INTERNATIONAL ACADEMYOF COSMETIC DERMATOLOGY
ATHENS, GREECEJUNE 27-30, 2013
C o n g r e s s O r g a n i s i n g B u r e a uERASMUS CONFERENCES TOURS & TRAVEL S.A.E-mail: [email protected]: www.erasmus.gr

March/April 2012
100SKINmed. 2012;10:100–102
From the Department of Dermatology, Louisiana State University Health Science Center, New Orleans, LA
Address for Correspondence: Scott M. Jackson, MD, LSUHSC, New Orleans, Department of Dermatology, 1542 Tulane Avenue, 6th Floor,
CASE STUDYVesna Petronic-Rosic, MD, MSc, Section Editor
Malignant Melanoma Arising Within Nevus SpilusSusan L. Karam, BS; Scott M. Jackson, MD
-
-
-
N 1
2–
7
8
-8–22
2
7
11
12
-6
-
12
-
-
10
12

March/April 2012
101SKINmed. 2012;10:100–102
26
2
-
-
1
Figure 1. Oval tan patch studded with hyperpigmented macules and melanoma at the margin of lesion.
Figure 3. and eosin, original magnification ×40).
Figure 2. and eosin, original magnification ×10).

March/April 2012
102SKINmed. 2012;10:100–102
-
-
CONCLUSIONS
10
-
-
REFERENCES
1 Dermatol-
ogy
2 Cohen JH, Minkin W, Frank SB. Nevus spilus. Arch Dermatol. 1970;
3 spilus. Int J Dermatol
4 nous melanomas: case report and literature review. J Cutan Med Surg.
5 Sigg C, Pelloni F, Schnyder UW. Frequency of congenital nevi, nevi spili
Dermatologica
6 other pigmented lesions of schoolchildren: the Vancouver Mole Study. J Am Acad Dermatol
7 like nevi, nevi spili, and café au lait spots. Arch Dermatol
8 noma developing in a speckled lentiginous nevus. Int J Dermatol.
9 case report and review of the literature. J Cutan Med Surg. 2010;14:
10 within the spectrum of congenital melanocytic nevi. Arch Dermatol.
11 teriform lentiginous nevus. Int J Dermatol
12 dysplastic nevus spilus. Arch Dermatol
13
J Cutan Pathol
14 spilus. Cutis
15 nous nevus. Arch Dermatol
16 Haenssle HA, Kaune KM, Buhl T, et al. Melanoma arising in segmental J Am Acad
Dermatol
17 spilus. Int J Dermatol
18 spilus. Int J Dermatol
19 acquired dermal melanocytosis on congenital nevus spilus. J Dermatol.
20 cursor of cutaneous melanoma: report of a case and literature review. Clin Exp Dermatol
21 Arch Dermatol
22 lentiginous nevus. J Am Acad Dermatol
23 Kaur TD, Kanwar AJ. Giant nevus spilus and centrofacial lentiginosis. Pediatr Dermatol
24 Br J Dermatol
25 Arch Dermatol
26 Cohen LM. Nevus spilus: congenital or acquired? Arch Dermatol.


March/April 2012
104SKINmed. 2012;10:104–106
From the Department of Dermatology and Cutaneous Biology, Jefferson Medical College of Thomas Jefferson University, Philadelphia, PA
Address for Correspondence: Alexis Sheaffer, BS, 1000 Walnut Street, Orlowitz Apartment 609, Philadelphia, PA 19107
CASE STUDY
Pseudocyst of the Auricle: An Uncommon Entity of the Ear
P 1–5
5
HISTOLOGY
8–10 -
9 -10
10
11
-
8
-10
THEORIES
-
4
12
-
-11
1
-
-10

March/April 2012
105SKINmed. 2012;10:104–106
-
12 -14
15
16
-16
β1
18 -
1
TREATMENTS
-
-
10
19
-
-
-10
Figure 1. Pseudocyst at the junction of the scaphoid fossa and superior
Figure 2. surface of an intracartilagenous cystic cavity at the base of the specimen (hematoxy
Figure 3.
flanked by degenerative cartilage at

March/April 2012
106SKINmed. 2012;10:104–106
-10
-
-
-10
-
6
1
-
1
10
-
-
-19
1
CONCLUSIONS
-
-
REFERENCES
1 Am J Otolaryngol
2 Lever’s Histopathology of the Skin
3 Arch Otolaryngol Head Neck Surg
4 Arch Otolaryngol
5 Arch Otolaryngol
6 Cutis
7 J Am Acad Dermatol
8 Laryngoscope
9 Weedon’s Skin Pathology
10 J Am Acad Dermatol
11 Laryngoscope
12 J Dermatol Surg Oncol
13 J Laryngol Otol
14 J Clin Pathol
15 Ann Plast Surg
16 in and intralesional steroid injection therapy for pseudocyst of the au
Inter J Dermatol
17
Am J Reprod Immunol
18
Ann Rheum Dis
19 J Otolaryngol


March/April 2012
108SKINmed. 2012;10:108–110
From the Department of Dermatology, Eskisehir Osmangazi University Faculty of Medicine, Eskisehir, Turkey
Address for Correspondence: Ayse Esra Koku Aksu, MD, Eskisehir Osmangazi University Faculty of Medicine, Department of Dermatology,
CASE STUDY
Necrotic Ulcer: A Manifestation of Leukemia CutisAyse Esra Koku Aksu, MD; Zeynep Nurhan Saracoglu, MD; Ilham Sabuncu, MD; Evrim Ciftci, MD;
Zafer Gulbas, MD; Serap Isiksoy, MD
-
-
2 -
-
-
-
7– -
10–12
12
-

March/April 2012
SKINmed. 2012;10:108–110
-
-
-
-17
-
18
8
CONCLUSIONS
12
-
-
REFERENCES
1 Br J Haema-
tol
2
WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues
3 Hypertension: Pathophysiology, Diagnosis and Man-
agement.
4 Cutis
5 J Cutan Pathol
6
Fitzpatrick’s Dermatology Treatment in General Medicine
7 tion, treatment and prognosis in a series of eight patients with leukaemia
Clin Exp Dermatol
8 trates in patients with myelogenous leukemia: a clinicopathologic study
J Am Acad Derma-tol
9 Arch Dermatol
10 Cancer
11
Cutis
Figure 2.
Figure 1.

March/April 2012
110SKINmed. 2012;10:108–110
12 mographic, hematological, and cytogenetic findings and prognosis in
Ann Hematol
13 following allogeneic bone marrow transplantation for acute myeloge
Bone Marrow Transplant
14 J Cutan Pathol
15 Br J Derma-
tol
16 Haematologica
17 Pathology of the Skin With Clinical
Correlations
18 Lever’s Histopathology of the Skin
Diagnosis and treatments have advanced over the past century. This feature depicts conditions from a collection of steroptic cards published in 1910 by by Dr. S. I. Rainforth.
HISTORICAL DIAGNOSIS & TREATMENT
SYPHILIS PRIMARIA:
A few days after the appearance of the chancre it is not uncommon to palpate a few hard painless cords which vary in thick
They are lymphatic vessels which have become specifically indurated, plugged with agglutinated leucocytes or compressed by
inflammatory edema however, in that it is very firm and elastic, like caoutchouc, and does not pit on pressure, its border is rather abrupt in its substance the hard lymphatic cords can often be felt, the skin over the affected area is nearly always dusky
Although a comparatively rare accompaniment of the primary sore this peculiar form of edema, when it is well marked, is a

Arnika Forte®
SPEED THE HEALING
Arnika Forte®
The New Gold Standardfor treating bruising,swelling, pain
1st and only combination of Arnica Montana 30x and Bromelain
One convenient capsuletwice a day
All natural, safe,physician - formulated
Speed the healing timefrom bruising, swelling andpain after surgery or dermalfiller injections
To Order Call 484-568-0306
�
�
�

March/April 2012
112SKINmed. 2012;10:112–113
CASE STUDY
Inflammatory Linear Verrucous Epidermal Nevus With Genital Involvement
Didem Didar Balci, MD;1 Jülide Zehra Yenin, MD;1 Ebru Çelik, MD;1 Gökhan Sarikaya, MD;1 Esin Atik, MD2
From the Departments of Dermatology,1 and Pathology,2 Mustafa Kemal University, Hatay, Turkey
Address for Correspondence: Didem Didar Balci, MD, Associate Professor, Mustafa Kemal University, Faculty of Medicine, Department of
E -
1–3 Ver-
-
1 -
-
3
-
-4
2
5 -2
-1– 5
1–3
-
2
5–
-
5
-
-

March/April 2012
113SKINmed. 2012;10:112–113
-
-1–3
-
CONCLUSIONS
-
10
11
-
-
REFERENCES
1
Fitzpatrick’s Dermatology in General Medicine
2 Pediatrik Dermatoloji
3 Dermatology
4 Arch Dermatol
5 Australas J Dermatol
6 Australas J Dermatol
7 Pediatr Dermatol
8
Aesthetic Plast Surg
9 Acta Derm Venereol
10 Arch Derma-
tol
11
Ann Plast Surg
Figure. Linear erythematous, lichenified, verrucous papules
CASE STUDY
Chronic Lymphocytic Leukemia Revealed by a Granulomatous Zosteriform EruptionSondes Trojjet, MD; Houda Hammami, MD; Inès Zaraa, MD; Alia Bouzguarrou, MD; Meriem Joens, MD; Slim Haouet, MD;
Amel Ben Osman, MD; Mourad Mokni, MD

March/April 2012
114SKINmed. 2012;10:114–115
O1
2
3
CASE STUDY
Oral Frictional Hyperkeratosis (Morsicatio Buccarum): An Entity to Be Considered in the Differential
Diagnosis of White Oral Mucosal LesionsKristin Cam, MD;1 Anthony Santoro, MD;2 Jason B. Lee, MD1
From the Department of Dermatology and Cutaneous Biology, Jefferson Medical College of Thomas Jefferson University, Philadelphia, PA;1 and Doylestown Dermatology, Doylestown, PA2
Address for Correspondence: Jason B. Lee, MD, Department of Dermatology and Cutaneous Biology, Jefferson Medical College of Thomas
Figure 1. Whitish plaque with an irregular surface on the left mucosa near the line of dental occlusion.

March/April 2012
115SKINmed. 2012;10:114–115
4
4
CONCLUSIONS
Figure 2. A biopsy of the lesion showing psoriasiform hyperplasia, surface epithelium with ballooning degeneration,* and parakeratosis colonized by numerous bacteria** (hematoxylin and eosin stain, magnification ×100).
Figure 3. Swabbed specimen from the buccal mucosa show
(hematoxylin and eosin stain, original magnification ×100).
keratosis (hematoxylin and eosin stain, magnification ×400).
REFERENCES
1 Obermayer M. Cheekbiting (morsicatio buccarum). Arch Dermatol. 1964;90:185–190.
2 tal patients. Ann Saudi Med. 2009;29:365–368.
3 Krahl D, Altenburg A, Zouboulis CC. Reactive hyperplasias, precancerous and malignant lesions of the oral mucosa. J Dtsch Dermatol Ges. 2008;6:217–232.
4 Woo S and Lin D. Moriscatio mucosae oris—a chronic oral frictional keratosis, not a leukoplakia. J Oral Maxillofac Surg. 2009;67:140–146.

March/April 2012
116SKINmed. 2011;10:116–118
From the Department of Dermatology, Venereology & Leprology,1 and the Department of Pathology,2 Gian Sagar Medical College & Hospital, Ram Nagar, Banur, Patiala, India
Address for Correspondence: Varinder Singh, MD, Associate Professor, Department of Dermatology, Venereology & Leprology, Gian Sagar
CASE STUDY
Vesicular Palmoplantar Pityriasis RoseaVarinder Singh, MD;1 Meghna Sharma, MD;1 Tarun Narang, MD;1 Manas Madan, MD2
-
-
P 1
-
2
2
-
-
-
-
6
6 -
-
9

March/April 2012
SKINmed. 2012;10:116–118
10
11
chlamydia12
CONCLUSIONS
Figure 3. Focal spongiosis and slight exocytosis in the
Figure 4.
Figure 1.
Figure 2.
A
B

March/April 2012
118SKINmed. 2012;10:116–118
REFERENCES
1 Textbook of Dermatology
2 J Am Acad Dermatol.
3 Dermatologica.
4
Dermatology.
5 Arch Dermatol Syph.
6 J Eur Acad Dermatol Venereol.
7 Arch Dermatol.
8 Cochrane Database Syst Rev.
9 J Drugs Dermatol.
10 J Drugs Dermatol.
11 potential? J Antimicrob Chemother.
12 Eur J
Dermatol.
VINTAGE LABELS


March/April 2012
120SKINmed. 2012;10:120
nosocological mobius
-
-
-
-
review Hall’s Manual of Skin as a Marker of Underlying Disease
1 2 3 -
-
-
-
-
REFERENCES
1 Braverman IM. Skin Signs of Systemic Disease. 3rd ed. Philadelphia, PA: W.B. Saunders Co; 1998.
2 Callen, JP, Jorizzo, JL, Bolognia, JL, Piette, W, Zone JJ. Dermatological Signs of Internal Disease. 4th ed. Philadelphia, PA: W.B. Saunders Co; 2009.
3 Provost TT, Flynn JA. Cutaneous Medicine: Cutaneous Manifestations of Systemic Disease. Hamilton, Ontario: BC Decker Inc; 2001.
BOOK REVIEWNoah S. Scheinfeld, MD, JD, Section Editor
Hall’s Manual of Skin as a Marker of Underlying Disease
Edited by John C. Hall and Brian J. Hall. 300 pages. Shelton, CT; People’s Medical Publishing House–USA; 2011. $89.95. ISBN 1607951029
Reviewed by Noah S. Scheinfeld, MD, JD
From the Department of Dermatology, Columbia University, College of Physicians and Surgeons, New York, NY
Address for Correspondence: Noah S. Scheinfeld, MD, JD, Department of Dermatology, Columbia University, College of Physicians and Surgeons, 150 West

Locoid Lipocream® Cream, 0.1% Rx Only(hydrocortisone butyrate 0.1% cream)For Topical Use Only
BRIEF SUMMARY
INDICATIONS AND USAGELocoid Lipocream is a topical corticosteroid indicated for: relief of the inflammatoryand pruritic manifestations of corticosteroid-responsive dermatoses in adults andthe treatment of mild to moderate atopic dermatitis in patients 3 months to 18 yearsof age.
WARNINGS AND PRECAUTIONSReversible hypothalamic-pituitary-adrenal (HPA) axis suppression may occur, withthe potential for glucocorticosteroid insufficiency. Consider periodic evaluations forHPA axis suppression if Locoid Lipocream is applied to large surface areas or usedunder occlusion. If HPA axis suppression is noted, reduce the application frequency,discontinue use, or switch to a lower potency corticosteroid. Systemic effects of topical corticosteroids may also include manifestations ofCushing’s syndrome, hyperglycemia, and glucosuria. Pediatric patients may be more susceptible to systemic toxicity due to their largerskin surface-to-body-mass ratios. Initiate appropriate therapy if concomitant skin infections develop. Discontinue use if irritation develops.
ADVERSE REACTIONSThe most common adverse reactions (>1%) are HPA axis suppression andapplication site reactions.The following additional local adverse reactions have been reported infrequentlywith topical corticosteroids, and they may occur more frequently with the use ofocclusive dressings and higher potency corticosteroids. These reactions included:irritation, folliculitis, acneiform eruptions, hypopigmentation, perioral dermatitis,allergic contact dermatitis, secondary infection, skin atrophy, striae, miliaria andtelangiectasia.
USE IN SPECIFIC POPULATIONSPregnancyPregnancy Category C. Corticosteroids have been shown to be teratogenic inlaboratory animals when administered systemically at relatively low dosage levels.Some corticosteroids have been shown to be teratogenic after dermal applicationin laboratory animals.There are no adequate and well-controlled studies inpregnant women. Therefore, Locoid Lipocream should be used during pregnancyonly if the potential benefit justifies the potential risk to the fetus.Please refer to full prescribing information for detailed information regardingsystemic embryofetal development studies.Nursing MothersSystemically administered corticosteroids appear in human milk and couldsuppress growth, interfere with endogenous corticosteroid production, or causeother untoward effects. It is not known whether topical administration ofcorticosteroids could result in sufficient systemic absorption to produce detectablequantities in human milk. Because many drugs are excreted in human milk, cautionshould be exercised when Locoid Lipocream is administered to a nursing woman.Pediatric UseSafety and efficacy in pediatric patients below 3 months of age have not beenestablished. Because of higher skin surface-to-body-mass ratios, pediatric patients are at agreater risk than adults of HPA axis suppression when they are treated with topicalcorticosteroids. They are therefore also at a greater risk of glucocorticosteroidinsufficiency after withdrawal of treatment and of Cushing’s syndrome while ontreatment. Eighty-six (86) pediatric subjects (5 months to less than 18 years of age) withmoderate to severe atopic dermatitis affecting at least 25% of body surface area(BSA) treated with Locoid Lipocream three times daily for up to 4 weeks wereassessed for HPA axis suppression. The disease severity (moderate to severeatopic dermatitis) and the dosing regimen (three times daily) in this HPA axis studywere different from the subject population (mild to moderate atopic dermatitis) andthe dosing regimen (two times daily) for which Locoid Lipocream is indicated. Five of the 82 evaluable subjects (6.1%) demonstrated laboratory evidence ofsuppression, where the sole criterion for defining HPA axis suppression was aserum cortisol level of less than or equal to 18 micrograms per deciliter aftercosyntropin stimulation. Suppressed subjects ranged in age from 5 months to 16 years and, at the time of enrollment, had 25% to 95% BSA involvement. Thesesubjects did not develop any other signs or symptoms of HPA axis suppression. At the first follow up visit, approximately one month after the conclusion oftreatment, cosyntropin stimulation results of all subjects had returned to normal,with the exception of one subject. This last subject recovered adrenal function bythe second post treatment visit, 65 days post-treatment. Cushing’s syndrome, linear growth retardation, delayed weight gain, andintracranial hypertension have also been reported in pediatric patients receivingtopical corticosteroids. Manifestations of adrenal suppression in pediatric patientsinclude low plasma cortisol levels to an absence of response to ACTH stimulation.Manifestations of intracranial hypertension include bulging fontanelles, headaches,and bilateral papilledema.
Geriatric UseClinical studies of Locoid Lipocream did not include sufficient numbers of subjectsaged 65 and over to determine whether they respond differently from youngersubjects.Carcinogenesis, Mutagenesis, Impairment of FertilityNo studies were conducted to determine the photococarcinogenic or dermalcarcinogenic potential of Locoid Lipocream.Hydrocortisone butyrate revealed no evidence of mutagenic or clastogenicpotential based on the results of two in vitro genotoxicity tests (Ames test andL5178Y/TK+ mouse lymphoma assay) and one in vivo genotoxicity test (mousemicronucleus assay).No evidence of impairment of fertility or effect on mating performance wasobserved in a fertility and general reproductive performance study conducted inmale and female rats at subcutaneous doses up to and including 1.8 mg/kg/day(0.7X maximum topical human dose [MTHD]). Mild effects on maternal animals,such as reduced food consumption and a subsequent reduction in body weight gain,were seen at doses ≥0.6 mg/kg/day (0.2X MTHD).
PATIENT COUNSELING INFORMATIONPatients using Locoid Lipocream should receive the following information and instructions:Apply a thin layer to the affected skin two or three times daily for corticosteroid-responsive dermatoses in adults. Consult with your physician to determine iftreatment is needed beyond 2 weeks. Apply a thin film to the affected skin areastwo times daily for atopic dermatitis in patients 3 months of age and older. Safety of Locoid Lipocream in pediatric patients has not been established beyond 4weeks of use.Rub in gently.Avoid contact with the eyes. Do not bandage, otherwise cover, or wrap the affected skin area so as to beocclusive unless directed by your physician.Do not use Locoid Lipocream in the diaper area, as diapers or plastic pants mayconstitute occlusive dressings.Do not use Locoid Lipocream on the face, underarms, or groin areas unlessdirected by your physician.If no improvement is seen within 2 weeks, contact your physician.Do not use other corticosteroid-containing products while using Locoid Lipocreamwithout first consulting your physician.
Store at 25°C (77°F); excursions permitted to 15-30°C (59-86°F) [see USP ControlledRoom Temperature]. Protect from freezing. Keep out of the reach of children.
Marketed and Distributed By:Triax Pharmaceuticals, LLCCranford NJ 07016www.Locoid.com
Manufactured for: Triax Pharmaceuticals, LLCCranford NJ 07016By: Ferndale Laboratories, Inc.Ferndale MI 48220
131B301Rev 11/09
Locoid Lipocream is a registered trademark of Astellas Pharma Europe BV licensed to Triax Pharmaceuticals, LLC.

Now younger eczema patients have something
to smile about
Now approved for use in children down to 3 months of age
(hydrocortisone butyrate 0.1%) Cream
Locoid Lipocream is indicated for the relief of the inflammatory and pruritic manifestations of corticosteroid-responsive dermatoses, including the treatment of mild to moderate atopic dermatitis in patients 3 months of age and older.Safety and effectiveness in pediatric patients below 3 months of age have not been established.Reversible HPA axis suppression may occur, with the potential for corticosteroid insufficiency. Consider periodic evaluations for HPA axis suppression if applied to large surface areas or used under occlusion . Systemic effects of topical corticosteroids may also includemanifestations of Cushing’s syndrome, hyperglycemia, and glucosuria. Pediatric patients may be more susceptible to systemic toxicity due to their large skin surface-to-body-mass ratios. Initiate appropriate therapy if concomitant skin infection develops. Discontinue use if irritation develops. Please see full Prescribing Information on adjacent page. Visit us at www.locoid.com
©2010 Triax Pharmaceuticals, LLC. All rights reserved. Locoid is a registered trademark of Astellas Pharma Europe B.V. licensed to Triax Pharmaceuticals, LLC. LOC-0410-01
The power of an ointment with the elegance of a cream