Manual&vacuum&aspira.on:&aservice&evalua.on.& …...Manual&vacuum&aspira.on:&aservice&evalua.on.&...
1
Manual vacuum aspira.on: a service evalua.on. Dr. J. Chester, 1 Miss M. Shehmar. 2 1. Good Hope Hospital, Su?on Coldfield. 2. Birmingham Women’s Hospital, Birmingham. In the United Kingdom over 45,000 of the 900,000 pregnancies end in miscarriage. 1, 2 For those where products of concep.on remain there are three op.ons for management: expectant, medical or surgical. Studies have shown that expectant and medical management are successful in 7080% of cases. 3 In some cases these op.ons are unacceptable to women, for these pa.ents and where previous management op.ons are unsuccessful, surgical interven.on is required. Classically this has been using electric vacuum aspira.on (EVA). However an alterna.ve does exist in the form of manual vacuum aspira.on (MVA). This uses a manually ac.vated syringe to aspirate the contents of the uterus. The equipment is lightweight and inexpensive and the procedure can o^en be done under local anaesthe.c only . Studies have shown it to be comparable in efficacy and complica.on rates, such as perfora.on and bleeding, to EVA. 4, 5, 6, 7, 8 MVA’s use in the UK is increasing, however it s.ll remains a less common procedure than EVA. This prospec.ve cohort study looked at MVA procedures done between November 2010 and January 2013. All women where an incomplete or missed miscarriage had been confirmed under 12 weeks were offered the procedure as one of their op.ons. The procedure was offered under local anaesthe.c and the pa.ent fully consented. Exclusions included suspected sep.c miscarriage, uterine anomalies, molar pregnancies or mul.ple pregnancies. Women op.ng for the procedure had 800 micrograms of per vaginal misoprostol two hours before the procedure, unless done as an emergency. The procedure itself was carried out in a variety of suitable sedngs. At the start of the procedure 6.6mls of 3% mepivacaine was infiltrated to the cervix at the 12, 3, 5, 6, 7 and 9 o’clock posi.ons. The cervix was then dilated to a minimum of 7mm. Extra analgesia was available to all women throughout the procedure; either entenox or morphine. Data was collected via a database with informa.on entered immediately post procedure and then update at the point of pa.ent discharge. Pa.ents were also given a voluntary anonymous ques.onnaire to assess their experience of the procedure Demographic data Indica.on for procedure Missed miscarriage 112 (85%) Incomplete miscarriage 19 (15%) Gesta.onal age (by ultrasound) < 9 weeks 91 (70%) 912 weeks 33 (25%) >12 weeks 7 (5%) Dilata.on and intraopera.ve complica.ons 72% of pa.ents required further instrumental dilata.on before the procedure. Intraopera.ve complica.ons were rare affec.ng only 5%. There was one suspected uterine perfora.on requiring no further treatment, two vaso vagal episodes and two episodes of minor cervical trauma. Efficacy and postopera.ve complica.ons 98% of pa.ents had a successful procedure. One pa.ent required an ultrasound scan to confirm a complete uterine evacua.on. One pa.ent needed a repeat procedure for retained products of concep.on. There were no life threatening or fatal complica.ons. All pa.ents reported minimal or mild vaginal bleeding a^er the procedure but no pa.ent required transfusion. All pa.ents were discharged the same day . Pa.ent experience 28 women completed the ques.onnaire. 82% reported the procedure was shorter or of a dura.on they expected. 61% felt they would be willing to undergo the procedure again if necessary and 68% felt they would recommend the procedure to a friend. Most women rated the pain as mild to moderate during the procedure. A^er one hour most felt there pain was mild, with pain con.nuing to se?le un.l the point of discharge. Many women also commented on the posi.ve impact of the nurses present during the procedure. 10 107 14 None Diclofenac and/or paracetamol Further analgesia A total of 131 women underwent the procedure during the period studied. The mean gesta.onal age was 8.3 weeks (SD +/ 1.8 weeks). Theatre was used for the ini.al MVAs (4.6%) un.l the procedure became established. 82% were done in a dedicated sedng in the Early Pregnancy Assessment Unit whilst some emergency procedures were carried out in A&E (0.8%) and on the gynaecology ward (13.0%). Intraopera.ve pain relief 70% of pa.ents required local anaesthe.c only . 21% declined local anaesthe.c. Higher levels of pain relief were needed only by those undergoing the MVA as an emergency requiring morphine (9%) and entonox (5%). 0 2 4 6 8 10 12 During 1 hour Discharge Pa0ents’ Experience of Pain None Mild Moderate Severe No answer The MVA procedure was introduced to the Birmingham Women’s Hospital to provide an alterna.ve surgical method for dealing with miscarriages, increasing choice for women. Previous studies have shown it to be a safe effec.ve method for dealing with retained products of concep.on. 5, 8, 9 Our study supports this evidence showing it effec.ve in 98% of cases with no major complica.ons. Mi?al et al demonstrated the benefits of use of misoprostol to reduce the need for cervical dilata.on and improve the efficacy of the procedure. 10 In our study its use was enough to begin dilata.on but further dilata.on was required in the majority of women. For most women in our cohort cervical block was sa.sfactory for providing adequate analgesia and allowing comple.on of the procedure. This supports previous findings by Lopez et al. 11 Our study demonstrated the importance of having stronger analgesics available for those pa.ents who cannot tolerate the procedure with local anaesthe.c alone, especially in emergency situa.ons. Post opera.vely the majority of pa.ents’ pain was controlled with simple and cheap analgesic methods. This helps keep costs low and facilitates rapid discharge. Women’s experiences of the procedure were posi.ve. The majority were sa.sfied with the procedure and would opt for it again. This indicates the procedure is acceptable and provides a viable choice for women. Although most experienced mild or moderate pain, this se?led quickly a^er the procedure. Ul.mately this feedback is vital to guide our prac.ce and support its con.nued use. The World Health Organisa.on supports the use of MVA for management of miscarriage. Despite this and mul.ple studies demonstra.ng its benefits it remains underused in the UK. 8, 9, 12 Recently its use has grown with specialist nurses also being trained to carry out the procedure. The evidence and our study show it to be a safe and effec.ve procedure for use in an daycase sedng. Given current economic pressures and the need for increased pa.ent choice it requires further considera.on as a safe, efficient and versa.le method for dealing with early miscarriages. Our experiences of MVA under local anaesthe.c for early pregnancy correlate well with previous studies. MVA provides a valid alterna.ve surgical method for uterine evacua.on. Its benefits; low cost, high efficacy, short post procedure stay and ability to be carried out in a variety of outpa.ent sedngs, make it an a?rac.ve op.on for healthcare providers in the current changing climate. Given the posi.ve feedback from pa.ents, it does represent a viable choice for women, with large benefits. As a result of our posi.ve findings, MVA is a procedure that will con.nue to be offered to all women at the Birmingham Women’s Hospital. Introduc.on Method Results Discussion Conclusion References 1. Office of Na.onal Sta.s.cs. Concep.on in England and Wales 2009. Office of Na.onal Sta.s.cs [Online]. 2011. Access date Feb 2013. Available at h?p://www.ons.gov.uk/ons/rel/vsob1/concep.onsta.s.csenglandandwales/2009/index.html 2. Hospital Episode Sta.s.cs. Total deliveries, miscarriages and ectopic pregnancies per 100 deliveries, 199798 to 200910. Hospital Episode Sta.s.cs [Online]. 2010. Access date Feb 2013. www.hesonline.nhs.k/Ease/servlet/ContentServer?siteID=1937&categoryID=1064 3. Shelley JM, Healy D, Grover S. A randomised trial of surgical, medical and expectant management of first trimester spontaneous miscarriage. Aust N Z J Obstet Gynaecol, 2005; 45(2):1227. 4. Edwards S, Tureck R, Fredrick M et al. Pa.ent acceptability of manual versus electric vacuum aspira.on for early pregnancy loss. J Womens Health (Larchmt). Dec 2007; 16(10):142936. 5. Wen J, Cai QY, Deng F, Li YP. Manual versus electric vacuum aspira.on for first trimester abor.on: a systema.c review . BJOG. 2008; 115(1):513. 6. Bird ST, Harvey SM, Beckman LJ et al. Similari.es in women’s percep.ons and acceptability of manual vacuum aspira.on and electric vacuum aspira.on for first trimester abor.on. Contracep.on. 2003; 67(3): 20712. 7. Wesxall JM, Sophocles A, Burggraf H et al. Manual vacuum aspira.on for first trimester abor.on. Arch Fam Med, 1998; 7(6):55962. 8. Gazvani R, Honey E, MacLennan FM et al. Manual vacuum aspira.on in the management of trimester pregnancy loss. EJOG. 2004; 112(2):197200 9. Milingos DS, Mathur M, Smith NT et al. Manual vacuum aspira.on: a safe alterna.ve for the surgical management of early pregnancy loss. BJOG. 2009; 116(9): 126871 10. Mi?al S, Sehgral R, Aggarwal S et al. Cervical priming with misoprostol before manual vacuum aspira.on versus electric vacuum aspira.on for first trimester surgical abor.on. Int J Gynaecol Obstet. 2011; 112 (1): 349/ 11. Lopez JC, VigilDe Gracia P, VegaMalek JC et al. A randomised comparison of different methods of analgesia in abor.on using manual vacuum aspira.on. Int J Gynaecol Obstet. 12. Dean G, Cardenas L, Darney P et al. Acceptability of manual versus electric aspira.on for first trimester abor.on: a randomised trial. Contracep.on. 2003; 67(3): 2016 8 4 18 Further analgesia NB Some women had mul/ple types Strong opiates Codeine Entenox Post opera.ve analgesia
Transcript of Manual&vacuum&aspira.on:&aservice&evalua.on.& …...Manual&vacuum&aspira.on:&aservice&evalua.on.&...

Manual vacuum aspira.on: a service evalua.on. Dr. J. Chester,1 Miss M. Shehmar.2
1. Good Hope Hospital, Su?on Coldfield. 2. Birmingham Women’s Hospital, Birmingham.
In the United Kingdom over 45,000 of the 900,000 pregnancies end in miscarriage.1, 2 For those where products of concep.on remain there are three op.ons for management: expectant, medical or surgical. Studies have shown that expectant and medical management are successful in 70-‐80% of cases.3 In some cases these op.ons are unacceptable to women, for these pa.ents and where previous management op.ons are unsuccessful, surgical interven.on is required. Classically this has been using electric vacuum aspira.on (EVA). However an alterna.ve does exist in the form of manual vacuum aspira.on (MVA). This uses a manually ac.vated syringe to aspirate the contents of the uterus. The equipment is lightweight and inexpensive and the procedure can o^en be done under local anaesthe.c only. Studies have shown it to be comparable in efficacy and complica.on rates, such as perfora.on and bleeding, to EVA.4, 5, 6, 7, 8 MVA’s use in the UK is increasing, however it s.ll remains a less common procedure than EVA.
This prospec.ve cohort study looked at MVA procedures done between November 2010 and January 2013. All women where an incomplete or missed miscarriage had been confirmed under 12 weeks were offered the procedure as one of their op.ons. The procedure was offered under local anaesthe.c and the pa.ent fully consented. Exclusions included suspected sep.c miscarriage, uterine anomalies, molar pregnancies or mul.ple pregnancies. Women op.ng for the procedure had 800 micrograms of per vaginal misoprostol two hours before the procedure, unless done as an emergency. The procedure itself was carried out in a variety of suitable sedngs. At the start of the procedure 6.6mls of 3% mepivacaine was infiltrated to the cervix at the 12, 3, 5, 6, 7 and 9 o’clock posi.ons. The cervix was then dilated to a minimum of 7mm. Extra analgesia was available to all women throughout the procedure; either entenox or morphine. Data was collected via a database with informa.on entered immediately post procedure and then update at the point of pa.ent discharge. Pa.ents were also given a voluntary anonymous ques.onnaire to assess their experience of the procedure
Demographic data Indica.on for procedure
Missed miscarriage 112 (85%) Incomplete miscarriage 19 (15%)
Gesta.onal age (by ultrasound) < 9 weeks 91 (70%)
9-‐12 weeks 33 (25%) >12 weeks 7 (5%)
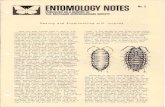
Results A total of 131 women underwent the procedure during the period studied. The mean gesta.onal age was 8.3 weeks (SD +/-‐ 1.8 weeks). Seven pa.ents had MVAs at a gesta.onal age of over 12 weeks for incomplete miscarriage. Theatre was used for the ini.al MVAs (4.6%) un.l the procedure became established. Following this pilot the procedure was then carried out in various outpa.ent sedngs. 82% were done in a dedicated sedng in the Early Pregnancy Assessment Unit whilst some emergency procedures were carried out in A&E (0.8%) and on the gynaecology ward (13.0%). Intra-‐opera.ve pain relief 21 (16%) of pa.ents required no local anaesthe.c during the procedure. 70% of pa.ents required local anaesthe.c only, with the remaining pa.ents needing morphine (9%) and entonox (5%). The higher levels of pain relief were needed mostly by those undergoing the MVA as an emergency. Dilata.on and intra-‐opera.ve complica.ons 72% of pa.ents required further instrumental dilata.on before the procedure. Intra-‐opera.ve complica.ons were rare (5%). There was one suspected uterine perfora.on requiring no further treatment, two vaso-‐vagal episodes and two episodes of minor cervical trauma. Efficacy and post-‐opera.ve complica.ons 98% of pa.ents had a successful procedure. One pa.ent required an ultrasound scan to confirm a complete uterine evacua.on. One pa.ent needed a repeat procedure for retained products of concep.on. There were no life threatening or fatal complica.ons. All pa.ents reported minimal or mild vaginal bleeding a^er the procedure, however in no pa.ent was this severe enough to require blood products. Post opera.ve analgesia 8% of pa.ents required no post-‐opera.ve analgesia. The majority of women (82%) were managed with the use of simple analgesia; either paracetamol, diclofenac or both. A small amount of women required codeine, strong opiates or entonox (3%, 6% and 14% respec.vely), either alone or in combina.on. Pa.ent experience 28 women completed and returned the ques.onnaire. 82% reported the procedure was shorter or of a dura.on they expected. 61% felt they would be willing to undergo the procedure again if necessary and 68% felt they would recommend the procedure to a friend. Only 11% of pa.ents felt they experienced severe pain during the procedure but this had eased in all pa.ents by the .me of discharge.
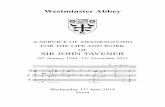
Dilata.on and intra-‐opera.ve complica.ons 72% of pa.ents required further instrumental dilata.on before the procedure. Intra-‐opera.ve complica.ons were rare affec.ng only 5%. There was one suspected uterine perfora.on requiring no further treatment, two vaso-‐vagal episodes and two episodes of minor cervical trauma. Efficacy and post-‐opera.ve complica.ons 98% of pa.ents had a successful procedure. One pa.ent required an ultrasound scan to confirm a complete uterine evacua.on. One pa.ent needed a repeat procedure for retained products of concep.on. There were no life threatening or fatal complica.ons. All pa.ents reported minimal or mild vaginal bleeding a^er the procedure but no pa.ent required transfusion. All pa.ents were discharged the same day. Pa.ent experience 28 women completed the ques.onnaire. 82% reported the procedure was shorter or of a dura.on they expected. 61% felt they would be willing to undergo the procedure again if necessary and 68% felt they would recommend the procedure to a friend. Most women rated the pain as mild to moderate during the procedure. A^er one hour most felt there pain was mild, with pain con.nuing to se?le un.l the point of discharge. Many women also commented on the posi.ve impact of the nurses present during the procedure.
10
107
14
None
Diclofenac and/or paracetamol
Further analgesia
A total of 131 women underwent the procedure during the period studied. The mean gesta.onal age was 8.3 weeks (SD +/-‐ 1.8 weeks). Theatre was used for the ini.al MVAs (4.6%) un.l the procedure became established. 82% were done in a dedicated sedng in the Early Pregnancy Assessment Unit whilst some emergency procedures were carried out in A&E (0.8%) and on the gynaecology ward (13.0%). Intra-‐opera.ve pain relief 70% of pa.ents required local anaesthe.c only. 21% declined local anaesthe.c. Higher levels of pain relief were needed only by those undergoing the MVA as an emergency requiring morphine (9%) and entonox (5%).
0
2
4
6
8
10
12
During 1 hour Discharge
Pa0ents’ Experience of Pain
None
Mild
Moderate
Severe
No answer
The MVA procedure was introduced to the Birmingham Women’s Hospital to provide an alterna.ve surgical method for dealing with miscarriages, increasing choice for women. Previous studies have shown it to be a safe effec.ve method for dealing with retained products of concep.on.5, 8, 9 Our study supports this evidence showing it effec.ve in 98% of cases with no major complica.ons. Mi?al et al demonstrated the benefits of use of misoprostol to reduce the need for cervical dilata.on and improve the efficacy of the procedure.10 In our study its use was enough to begin dilata.on but further dilata.on was required in the majority of women. For most women in our cohort cervical block was sa.sfactory for providing adequate analgesia and allowing comple.on of the procedure. This supports previous findings by Lopez et al.11 Our study demonstrated the importance of having stronger analgesics available for those pa.ents who cannot tolerate the procedure with local anaesthe.c alone, especially in emergency situa.ons. Post opera.vely the majority of pa.ents’ pain was controlled with simple and cheap analgesic methods. This helps keep costs low and facilitates rapid discharge. Women’s experiences of the procedure were posi.ve. The majority were sa.sfied with the procedure and would opt for it again. This indicates the procedure is acceptable and provides a viable choice for women. Although most experienced mild or moderate pain, this se?led quickly a^er the procedure. Ul.mately this feedback is vital to guide our prac.ce and support its con.nued use. The World Health Organisa.on supports the use of MVA for management of miscarriage. Despite this and mul.ple studies demonstra.ng its benefits it remains underused in the UK.8, 9, 12 Recently its use has grown with specialist nurses also being trained to carry out the procedure. The evidence and our study show it to be a safe and effec.ve procedure for use in an day-‐case sedng. Given current economic pressures and the need for increased pa.ent choice it requires further considera.on as a safe, efficient and versa.le method for dealing with early miscarriages.
Our experiences of MVA under local anaesthe.c for early pregnancy correlate well with previous studies. MVA provides a valid alterna.ve surgical method for uterine evacua.on. Its benefits; low cost, high efficacy, short post procedure stay and ability to be carried out in a variety of outpa.ent sedngs, make it an a?rac.ve op.on for healthcare providers in the current changing climate. Given the posi.ve feedback from pa.ents, it does represent a viable choice for women, with large benefits. As a result of our posi.ve findings, MVA is a procedure that will con.nue to be offered to all women at the Birmingham Women’s Hospital.
Introduc.on
Method
Results
Discussion
Conclusion
References
1. Office of Na.onal Sta.s.cs. Concep.on in England and Wales 2009. Office of Na.onal Sta.s.cs [Online]. 2011. Access date Feb 2013. Available at h?p://www.ons.gov.uk/ons/rel/vsob1/concep.on-‐sta.s.cs-‐-‐england-‐and-‐wales/2009/index.html
2. Hospital Episode Sta.s.cs. Total deliveries, miscarriages and ectopic pregnancies per 100 deliveries, 1997-‐98 to 2009-‐10. Hospital Episode Sta.s.cs [Online]. 2010. Access date Feb 2013. www.hesonline.nhs.k/Ease/servlet/ContentServer?siteID=1937&categoryID=1064
3. Shelley JM, Healy D, Grover S. A randomised trial of surgical, medical and expectant management of first trimester spontaneous miscarriage. Aust N Z J Obstet Gynaecol, 2005; 45(2):122-‐7.
4. Edwards S, Tureck R, Fredrick M et al. Pa.ent acceptability of manual versus electric vacuum aspira.on for early pregnancy loss. J Womens Health (Larchmt). Dec 2007; 16(10):1429-‐36.
5. Wen J, Cai QY, Deng F, Li YP. Manual versus electric vacuum aspira.on for first trimester abor.on: a systema.c review. BJOG. 2008; 115(1):5-‐13. 6. Bird ST, Harvey SM, Beckman LJ et al. Similari.es in women’s percep.ons and acceptability of manual vacuum aspira.on and electric vacuum aspira.on
for first trimester abor.on. Contracep.on. 2003; 67(3): 207-‐12. 7. Wesxall JM, Sophocles A, Burggraf H et al. Manual vacuum aspira.on for first trimester abor.on. Arch Fam Med, 1998; 7(6):559-‐62. 8. Gazvani R, Honey E, MacLennan FM et al. Manual vacuum aspira.on in the management of trimester pregnancy loss. EJOG. 2004; 112(2):197-‐200 9. Milingos DS, Mathur M, Smith NT et al. Manual vacuum aspira.on: a safe alterna.ve for the surgical management of early pregnancy loss. BJOG. 2009;
116(9): 1268-‐71 10. Mi?al S, Sehgral R, Aggarwal S et al. Cervical priming with misoprostol before manual vacuum aspira.on versus electric vacuum aspira.on for first
trimester surgical abor.on. Int J Gynaecol Obstet. 2011; 112 (1): 34-‐9/ 11. Lopez JC, Vigil-‐De Gracia P, Vega-‐Malek JC et al. A randomised comparison of different methods of analgesia in abor.on using manual vacuum
aspira.on. Int J Gynaecol Obstet. 12. Dean G, Cardenas L, Darney P et al. Acceptability of manual versus electric aspira.on for first trimester abor.on: a randomised trial. Contracep.on.
2003; 67(3): 201-‐6
8
4 18
Further analgesia NB Some women had mul/ple types
Strong opiates
Codeine
Entenox
Post opera.ve analgesia