
MANUAL Brothers Jaypee - Postgraduate Books | Jaypee ...
33
ICU MANUAL Jaypee Brothers
Transcript of MANUAL Brothers Jaypee - Postgraduate Books | Jaypee ...

ICU MANUAL
Jayp
ee B
rothe
rs

Jayp
ee B
rothe
rs
Editor-in-Chief
Prem Kumar MD DA DNB
Assistant Professor Department of Anesthesiology
Critical Care and Pain Medicine Saveetha Medical College and Hospital
Chennai, Tamil Nadu, India
New Delhi | London | PanamaThe Health Sciences Publishers
ICU MANUAL
TA Naufal Rizwan MD CCEBDM (Diabetology)
Assistant Professor Department of Internal Medicine
Saveetha Medical College and Hospital Chennai, Tamil Nadu, India
G Ninoo George MD DM
Consultant Department of Nephrology
Billroth Hospitals Chennai, Tamil Nadu, India
Sushma Vijay Pingale MD DA
Assistant Professor Department of Anesthesiology
Critical Care and Pain Medicine Saveetha Medical College
and Hospital Chennai, Tamil Nadu, India
Marun Raj MS MCh
Assistant Professor Department of Vascular Surgery
Saveetha Medical College and Hospital Chennai, Tamil Nadu, India
Editors
Jayp
ee B
rothe
rs

Jaypee Brothers Medical Publishers (P) Ltd.
HeadquartersJaypee Brothers Medical Publishers (P) Ltd.4838/24, Ansari Road, DaryaganjNew Delhi 110 002, IndiaPhone: +91-11-43574357Fax: +91-11-43574314E-mail: [email protected]
Overseas OfficesJ.P. Medical Ltd.83, Victoria Street, LondonSW1H 0HW (UK)Phone: +44-20 3170 8910Fax: +44 (0)20 3008 6180E-mail: [email protected]
Jaypee-Highlights Medical Publishers Inc.City of Knowledge, Bld. 237, ClaytonPanama City, PanamaPhone: +1 507-301-0496Fax: +1 507-301-0499E-mail: [email protected]
Jaypee Brothers Medical Publishers (P) Ltd.17/1-B, Babar Road, Block-BShaymali, MohammadpurDhaka-1207, BangladeshMobile: +08801912003485E-mail: [email protected]
Jaypee Brothers Medical Publishers (P) Ltd.Bhotahity, Kathmandu, NepalPhone: +977-9741283608E-mail: [email protected]
Website: www.jaypeebrothers.comWebsite: www.jaypeedigital.com
© 2017, Jaypee Brothers Medical Publishers
The views and opinions expressed in this book are solely those of the original contributor(s)/author(s) and do not necessarily represent those of editor(s) of the book.
All rights reserved. No part of this publication may be reproduced, stored or transmitted in any form or by any means, electronic, mechanical, photo copying, recording or otherwise, without the prior permission in writing of the publishers.
All brand names and product names used in this book are trade names, service marks, trademarks or registered trademarks of their respective owners. The publisher is not associated with any product or vendor mentioned in this book.
Medical knowledge and practice change constantly. This book is designed to provide accurate, authoritative information about the subject matter in question. However, readers are advised to check the most current information available on procedures included and check information from the manufacturer of each product to be administered, to verify the recommended dose, formula, method and duration of administration, adverse effects and contra indications. It is the responsibility of the practitioner to take all appropriate safety precautions. Neither the publisher nor the author(s)/editor(s) assume any liability for any injury and/or damage to persons or property arising from or related to use of material in this book.
This book is sold on the understanding that the publisher is not engaged in providing professional medical services. If such advice or services are required, the services of a competent medical professional should be sought.
Every effort has been made where necessary to contact holders of copyright to obtain permission to reproduce copyright material. If any have been inadvertently overlooked, the publisher will be pleased to make the necessary arrangements at the first opportunity.
Inquiries for bulk sales may be solicited at: [email protected]
ICU ManualFirst Edition: 2017
ISBN: 978-93-5270-030-1
Printed at
Jayp
ee B
rothe
rs

Dedicated to
My Lord Jesus Christ, whom I love more for His grace and mercy towards me and He is the reason for all the exaltation in my life. My dear wife Vero, and my loving son Sammy, who are my greatest joy. My dear parents, sister and in-laws, especially Dr Joseph, who encouraged me to write this book. All my teachers, especially to my mentor Professor Naheed Azhar, who inspired me to become anesthesiologist and intensivist.
Jayp
ee B
rothe
rs
Jayp
ee B
rothe
rs

CONTRIBUTORS
A Meenakshi Sundaram MS DNB Assistant Professor Department of Otorhinolaryngology Saveetha Medical College and Hospital Chennai, Tamil Nadu, India
Deepalakshmi MBBS Postgraduate Department of Biochemistry KAPV Medical College Trichy, Tamil Nadu, India
Dianitta Devapriya Veronica MBBS
Postgraduate Department of Otorhinolaryngology Kilpauk Medical College and Hospital Chennai, Tamil Nadu, India
G Ninoo George MD DM Consultant Department of Nephrology Billroth Hospitals Chennai, Tamil Nadu, India
Jenu Santhosh MD Assistant Professor Department of Internal Medicine Thoothukudi Medical College and Hospital Thoothukudi, Tamil Nadu, India
K Gunalan MS Assistant Professor Department of Orthopedics Saveetha Medical College and Hospital Chennai, Tamil Nadu, India
Marun Raj MS MCh Assistant Professor Department of Vascular Surgery Saveetha Medical College and Hospital Chennai, Tamil Nadu, India
Prem Kumar MD DA DNB
Assistant Professor Department of Anesthesiology Critical Care and Pain Medicine Saveetha Medical College and Hospital Chennai, Tamil Nadu, India
Sumathy MD Assistant Professor Institute of Anesthesiology and Critical Care Madras Medical College and Hospital Chennai, Tamil Nadu, India
Surendran GD MD Assistant Professor Department of Cardiology Kilpauk Medical College and Hospital Chennai, Tamil Nadu, India
Sushma Vijay Pingale MD DA Assistant Professor Department of Anesthesiology Critical Care and Pain Medicine Saveetha Medical College and Hospital Chennai, Tamil Nadu, India
S Yuvaraj MBBS DA Consultant Intensivist Raghavendra Multispeciality Hospital Madurai, Tamil Nadu, India
TA Naufal Rizwan MD CCEBDM (Diabetology)
Assistant Professor Department of Internal Medicine Saveetha Medical College and Hospital Chennai, Tamil Nadu, India
Vinoj MBBS DA PGDHS (Diabetology)
Postgraduate Department of Internal Medicine Tirunelveli Medical College and Hospital Tirunelveli, Tamil Nadu, India
V Thanga Thirupathi Rajan MS MCh Associate Professor Department of Neurosurgery Saveetha Medical College and Hospital Chennai, Tamil Nadu, India
Jayp
ee B
rothe
rs

Jayp
ee B
rothe
rs

PREFACE
Critical care medicine is relatively new but increasingly important medical specialty, which has become fully established in the current decade. ICU Manual focuses on the basic principles of intensive care which every practicing intensivist and postgraduate should be aware of. The concept of conditions commonly prevalent in intensive care has been dealt with in detail making it useful for the reader to gain a thorough knowledge of the intensive care. The scientific content is streamlined so that it would be of immense use for practicing intensivists in developing countries.
Flow charts, tables, algorithms and pictures have also been added to facilitate easy understanding of the subject. Many authors from various specialties have contributed for this book. It covers extensively on all the essentials—from the basics and system-specific topics to the recent advances—thereby making it comprehensive for intensive care. The recent articles and the current guidelines of sepsis and deep vein thrombosis (DVT) have also been included. The special feature of this book is the inclusion of the chapter ‘Role of Ultrasound in Critical Care’, since the use of ultrasound in critical care has tremendously increased in the past five years and has totally changed the practice of intensive care in certain areas.
We hope that this book will be a good resource to all the readers and help in intensive care practice and would be of immense use in treating the critically ill patients.
Prem Kumar
Jayp
ee B
rothe
rs

Jayp
ee B
rothe
rs

ACKNOWLEDGMENTS
I offer my gratitude to all the contributors and editors of this book, without whom, this book would have not been possible. I thank our respected Chancellor of Saveetha University, Dr NM Veeraiyan; and, our Director, Dr Saveetha Rajesh, for their constant motivation in writing this book. To my professors, colleagues, postgraduates, illustrators and all the supporting staff, who helped me in bringing this book to its present shape. Finally, I thank Mr Jayanandan, Mrs Samina Khan, Ms Saima Rashid, and all the supporting staff of M/s Jaypee Brothers Medical Publishers (P) Ltd., New Delhi, India, for their support in bringing up this ICU Manual, which would be of immense help to the readers.
Jayp
ee B
rothe
rs

Jayp
ee B
rothe
rs

CONTENTS
SECTION 1: ICU
1. Setting Up an ICU 3Prem KumarInitial Planning 3; Infrastructure 3; Indian Society of Critical Care Medicine (ISCCM) Provide Guidelines for Each Level ICU Planning in India 4; Other Issues 6
SECTION 2: Physiology of Critically Ill Patient 2. Critically Ill Patient and Oxygenation 9
Prem Kumar Oxygen Cascade 9; Tissue Oxygenation 12
SECTION 3: Vascular Access and Hemodynamic Monitoring 3. Peripheral Arterial Catheterization 17
Prem KumarIndications 17; Equipment 17; Monitoring Sites 17; Technique 18
4. Peripheral Venous Catheterization 24Prem KumarInsertion Techniques 24; Precautions 24; Equipment 24; Principle 24; Midline Catheters 26
5. Central Venous Catheterization 27Prem KumarApplied Anatomy 28; Techniques 30; Ultrasound-Guided Techniques 38
6. Pulmonary Artery Catheterization 43Prem KumarHistory 43; Perioperative Indications 44; Physiological Variables with PA Catheterization 46
7. Hemodynamic Monitoring 51Prem KumarThoracic Bioimpedance Plethysmography 51; Esophageal and Transcutaneous Doppler Monitoring 51; Mucosal Tonometry 53; Systolic Pressure Variation 58; Limitations of Dynamic Parameters 59
Jayp
ee B
rothe
rs

xiv ICU Manual
SECTION 4: Shock 8. An Overview of Shock 65
Prem KumarDefinition 65; Classification 65; Clinical Features 66
9. Hypovolemic Shock 71Prem KumarEtiology 71; Pathophysiology 71; Key Elements of Managing Hemorrhagic Shock 74
10. Obstructive Shock 77Prem KumarCauses 77; Pathophysiology 77; Clinical Features 77; Air Embolism 78
11. Cardiogenic Shock 81TA Naufal RizwanDefinition 81; Characteristics 81; Pathogenesis 82; Clinical Features 82; High-risk Patients for Cardiogenic Shock 82; Left Heart Catheterization and Angiography 83; Invasive Procedures in Cardiogenic Shock 84; Vasopressors 85
12. Multiple Organ Dysfunction Syndrome 87Prem KumarDefinition 87; Etiology 87; Pathophysiology 87; Clinical Syndromes 89; Scoring Systems 89
SECTION 5: Infection and Immune Disorders in ICU 13. Approach to Nosocomial Infections 97
Prem KumarRisk Factors 97; Mechanisms of Drug Resistance 98; Nosocomial Pneumonia 98
14. Urinary Tract Infections 108Prem KumarDefinitions 108; Risks 108; Common Organisms Causing Urinary Tract Infection 109; Prevention of CAUTI—Recommendations by HICPAC (Healthcare Infection Control Practices Advisory Committee) 2009 Guidelines 113
15. Sepsis and Septic Shock 115Prem KumarDefinitions 115; Pathogenesis 115; Sepsis 117; Severe Sepsis 117; Antimicrobial Therapy 121; Hemodynamic Support 122
16. Principles of Antibiotic Use in ICU 127Prem KumarPrinciples of Antibiotic Prescription 127; Common Causes of Infection in ICU 128; Pharmacokinetic Principles 128; Steps Taken to Prevent Antibiotic Resistance 131
Jayp
ee B
rothe
rs

Contents xv
17. Tropical Infections 134Jenu SanthoshSevere Malaria 134; Dengue 137
18. Anaphylaxis 140Prem KumarDefinitions 140; Etiology and Predisposing Factors 140; Clinical Manifestations 141; Role of Epinephrine in Anaphylaxis 144
SECTION 6: Poisoning and Envenomation 19. General Principles of Poisoning 149
Jenu SanthoshManifestations 149; Neurological Examination 149; Cardiovascular 150; Metabolic 150; Management 150
20. Poisoning 153Jenu Santhosh, TA Naufal RizwanOrganophosphorus and Carbamate Poisoning 153; Organochlorine and Pyrethroid Poisoning 155
21. Drug Overdose 159Jenu Santhosh, TA Naufal RizwanSedatives and Hypnotics 159; Antidepressants 159; Acetaminophen Poisoning 160; Opioids 160; Beta-blockers 161
22. Envenomation 162Jenu SanthoshScorpions (Scorpionidae) 162; Caterpillars and Moths (Lepidoptera) 162; Reptile Bites 163
SECTION 7: Burns 23. Classification and Evaluation of Burns 173
Prem KumarClassification 173; Physiological Disturbances 173; Burns Assessment 174; Secondary Survey 179
24. Management of Burns 180Prem KumarEarly Resuscitative Phase 180; Wound Management Phase 182; Rehabilitative Phase 183; Management of Carbon Monoxide Poisoning 183; Complications 184
SECTION 8: Respiratory Diseases in ICU 25. Approach to Acute Respiratory Failure 187
Prem KumarPathophysiology 188; Clinical Presentation 188; Treatment 189
26. Acute Lung Injury and Acute Respiratory Distress Syndrome 193Prem KumarDefinition 193; Pathophysiology 194; Management 195; Weaning Protocol for ARDS 196; Fluid Management 197; Nutritional Support 197
Jayp
ee B
rothe
rs

xvi ICU Manual
27. Acute Exacerbation of Chronic Obstructive Pulmonary Disease 199Prem KumarRisk Factors 199; Pathophysiology 199; Diagnosis 200; Clinical Assessment 202
28. Acute Severe Asthma 206Prem KumarClinical Features 206; Diagnosis 206; Management 209
29. Deep Venous Thrombosis and Pulmonary Embolism 214Prem Kumar, Marun RajPathophysiology 214; Clinical Features and Diagnosis 214; Prevention 218; Treatment 222
30. Obstructive Sleep Apnea and Obesity Hypoventilation Syndrome 225Prem KumarHistory 225; Obstructive Sleep Apnea 226; Obesity Hypoventilation Syndrome 227
SECTION 9: Approach to Mechanical Ventilation 31. Basics of Mechanical Ventilation 233
Prem Kumar, S YuvarajNegative Pressure Ventilation 233; Positive Pressure Ventilation 233; Ventilator Design 233; Nomenclatures and their Significance 234; Breath Type 234
32. Initiation of Ventilation 239Prem KumarInitial Ventilator Settings 240
33. Modes of Ventilation 245Prem KumarBasic Modes of Ventilation 245; Pressure Support Ventilation 249
34. Weaning from Mechanical Ventilation 258Prem KumarDefinition of Weaning 258; Weaning Criteria 258
35. Patient Ventilator Asynchrony 264Prem KumarVariables Contributing to Asynchrony 265
36. Noninvasive Ventilation 269Prem Kumar, S YuvarajEquipment (Interface) 269; Protocol for Managing Patients Planned for NIPPV 269; Asthma 272; Pneumonia 272
SECTION 10: Cardiovascular Diseases in ICU 37. Cardiac Arrhythmias 277
Surendran GDSupraventricular Arrhythmias 277; Ventricular Arrhythmias 286
Jayp
ee B
rothe
rs

Contents xvii
38. Acute Heart Failure 296Surendran GDDefinition 296; Classification 296; Pathophysiology 296; Clinical Features 296; Biomarkers 297; Specific Therapies for Acute Heart Failure 299; Vasodilators 299; Other Drugs Used in the Treatment of Acute Heart Failure 302
39. Approach to Acute Myocardial Infarction 306Surendran GDDefinition 306; Universal Definition of Myocardial Infarction 306; Universal Myocardial Infarction Classification of Type 306; Clinical Features 307; ECG Manifestations of Ischemia in the Setting of LBBB 310; Antiplatelet Therapy 312; Pain Control 313; Limitations of Infarct Size 315; Percutaneous Coronary Intervention 316
40. Hypertensive Crisis 322Surendran GDDefinition 322; Hypertensive Emergency (Previously Malignant Hypertension) 322; Hypertensive Urgency 323; Investigations 324
41. Cardiac Tamponade 328Surendran GDDefinition 328; Pathophysiology 328; Precipitating Factors 328; Clinical Features 328; Becks Triad (Useful Clue for Diagnosis of Tamponade) 329; Differential Diagnosis 329; Investigations 329; Management 330
SECTION 11: Renal and Electrolyte Disturbances in ICU 42. Acute Kidney Injury 335
Jenu Santhosh, Prem KumarCharacteristics 335; Categories 335; Diagnosis 337; Markers for Renal Dysfunction in AKI 338
43. Renal Replacement Therapy 342G Ninoo GeorgeAccess 343; Hemodialysis Versus Peritoneal Dialysis 344; Intermittent Hemodialysis Versus Slow Low Efficiency Dialysis 344; Slow Low Efficiency Dialysis Versus Continuous Renal Replacement Therapy 344; Adverse Effects of Renal Replacement Therapy 344
44. Hyponatremia 346TA Naufal RizwanCauses 346; Pseudohyponatremia 347; True Hyponatremia (< 275 mOsm/Kg) 347; Asymptomatic Hyponatremia 348; Symptomatic Hyponatremia 348; Osmotic Demyelination Syndrome 349; Hypernatremia 349; Management of Diabetes Insipidus 351
45. Potassium 353Prem Kumar, Sushma Vijay PingalePotassium Balance in Health and Disease 353; Hypokalemia 353; Hyperkalemia 355
Jayp
ee B
rothe
rs
xviii ICU Manual
46. Calcium 359TA Naufal RizwanCalcium Metabolism 359; Hypocalcemia 359; Chvostek’s Sign 360; Trousseau Sign 360; Hypercalcemia 361; Diagnostic Workup 362
47. Phosphorus 366TA Naufal RizwanMetabolism 366; Hypophosphatemia 366; Hyperphosphatemia 369
48. Magnesium 372TA Naufal RizwanHypomagnesemia 372; Hypermagnesemia 374
SECTION 12: Gastrointestinal Diseases in ICU 49. Upper Gastrointestinal Bleeding 379
TA Naufal RizwanPeptic Ulcer 379; Variceal Bleed 379; Mallory-Weiss Tear 380; Boerhaave’s Syndrome 380; Vascular Anomalies 380; Management 380; Pharmacologic Therapy 382; Endoscopy 382; Specific Conditions 382
50. Lower Gastrointestinal Bleeding 385TA Naufal RizwanEtiology 385; Investigations 386; Treatment 386; Specific Measures 387
51. Acute Pancreatitis 389TA Naufal RizwanGeneral Considerations 389; Etiology 389; Pathogenesis 389; Clinical Features 390; Investigations 390; Radiology 391; Differential Diagnosis 392; Management 392
52. Acute Liver Failure 394TA Naufal RizwanClassification 394; Causes of Acute Liver Failure 394; Pathophysiology 395; Clinical Features 395; Associations of Acute Hepatic Failure 395; Prognosis 398; Treatment 398; Liver Transplantation 400
53. Abdominal Infections in ICU 402TA Naufal RizwanClassification 402; Pathophysiology 403; Clinical Features 403; Investigations 404; Management 404; Duration of Treatment 406
SECTION 13: Hematological Disorders in ICU 54. Hemolytic Anemia and Sickle Cell Crisis 411
VinojHemolytic Anemia 411; Sickle Cell Crisis 413
55. Disseminated Intravascular Coagulation and Heparin-induced Thrombocytopenia 416VinojDisseminated Intravascular Coagulation 416; Heparin-induced Thrombocytopenia 418
Jayp
ee B
rothe
rs

Contents xix
56. Immune Thrombocytopenic Purpura 420VinojPathogenesis 420; Classification of Immune Thrombocytopenic Purpura 420; Clinical Features 421; Laboratory Finding 421; Treatment 422; Emergency Treatment of Acute Bleeding 423
SECTION 14: Endocrine Disorders in ICU 57. Diabetic Ketoacidosis 427
Vinoj, G Ninoo GeorgePrecipitating Factors 428; Basic Pathophysiology of Diabetic Ketoacidosis 428; Clinical Features 428; Management Goals 429; Assessment and Monitoring 430; Fluid Replacement 430; Insulin Therapy 430; Electrolyte Correction 430
58. Hyperosmolar Hyperglycemic State 432Vinoj, G Ninoo GeorgePathophysiology 432; Clinical Features 433
59. Diabetes Insipidus 435Vinoj, G Ninoo GeorgeVasopressin: Neural Hormone 435; Etiology 436; Complications 439
60. Syndrome of Inappropriate Secretion of Antidiuretic Hormone 441Vinoj, G Ninoo GeorgePathophysiology 441
61. Thyroid Emergencies 449Vinoj, G Ninoo GeorgeThyroid Storm 449; Myxedema Coma 451; Pathogenesis 452
62. Adrenal Emergencies 455Vinoj, G Ninoo GeorgeAdrenal Crisis 455; Primary (↑ ACTH) 455
SECTION 15: Obstetric Emergencies 63. Obstetric Hemorrhage 463
Prem KumarCauses of Obstetric Hemorrhage 463; Classification 463; Antepartum Hemorrhage 464; Postpartum Hemorrhage 465
64. Hypertensive Disorders of Pregnancy 469Prem KumarClassification of Hypertensive Disorders in Pregnancy 469; Definitions 469; Pre-eclampsia 469; HELLP Syndrome 473; Eclampsia 474
65. Acute Fatty Liver of Pregnancy 476Prem KumarPathophysiology 476; Clinical Presentation 476; Lab Investigations 476; Differential Diagnosis 476; Complications 477; Management 477
Jayp
ee B
rothe
rs

xx ICU Manual
66. Amniotic Fluid Embolism 479Prem KumarPathophysiology 479; Clinical Features 479; Lab Investigations 480; Management 480
SECTION 16: Neurological Disorders in ICU 67. Cerebrovascular Diseases 483
TA Naufal RizwanTransient Ischemic Attack 483; Stroke 484; Ischemic Stroke (80%) 484; Clinical Features 485; Hemorrhagic Stroke 486; Clinical Features of Hemorrhagic Stroke 486; Management of Cerebral Edema 487
68. Status Epilepticus 490TA Naufal RizwanDefinition 490; Etiology 490; Types 490; Convulsive 490; Simple Partial Status Epilepticus 491; Complications 491; Investigations 491; Treatment 491
69. Meningitis and Encephalitis 494TA Naufal RizwanDefinition 494; Classification 494; Acute Bacterial Meningitis 494; Pathogenesis 495; Clinical Features 495; Investigations 496; Imaging 496; Differential Diagnosis 497; Treatment 497; Antibiotics Based on Organisms 497; Viral Meningitis 499; Investigations 500; Tubercular Meningitis 501; Fungal Meningitis 502; Viral Encephalitis 503; Treatment 504
70. Alcohol Withdrawal Syndrome 506TA Naufal RizwanSymptoms 506; Delirium Tremens 507; Management of Delirium Tremens 508
71. Delirium in Intensive Care Unit 510TA Naufal RizwanDefinition 510; Clinical Features 510; Terminal Delirium 510
SECTION 17: Neuromuscular Disorders 72. Guillain-Barré Syndrome 517
TA Naufal RizwanGeneral Considerations 517; Etiology 517; Pathogenesis 517; Clinical Features 518
73. Myasthenia Gravis 521TA Naufal RizwanEtiology 521; Pathogenesis 521; Clinical Features 522; Investigations 523; Treatment 524; Evaluating the Effectiveness of Treatment 526; Myasthenic Crisis 526
74. Periodic Paralysis 528TA Naufal RizwanHypokalemic Periodic Paralysis 528; Hyperkalemic Periodic Paralysis 529; Anderson’s Syndrome 530
Jayp
ee B
rothe
rs

Contents xxi
75. Critical Illness Polyneuropathy 531TA Naufal RizwanPredisposing Factors 531; Pathology 531; Pathogenesis 531; Clinical Features 531; Treatment 533
SECTION 18: Approach to a Trauma Patient 76. Advanced Trauma Life Support 537
Prem KumarAirway 537; Breathing 539; Circulation 539; Massive Transfusion 541; Complications 542
77. Open Fractures 545K GunalanClassification 545; Antibiotic Cover 546; Surgical Debridement and Irrigation 546; Wound Closure 547; Skeletal Fixation 547
78. Pelvic Fractures 551K GunalanAdvanced Trauma Life Support 552; Hemodynamic Status 552; Fracture Stability 552; Pneumatic Antishock Garment 553; Pelvic Binders 553; Anterior External Fixator 553; Acute Fracture Fixation 554; Angiography 554; Pelvic Packing 555; Open Pelvic Fractures 555
79. Fat Embolism Syndrome 557Sushma Vijay PingaleEtiology 557; Pathogenesis 557; Clinical Features 557; Diagnosis 558; Management 559
80. Abdominal Trauma 560Marun RajMechanism of Injury 560; Diagnostic Principles in General 560; Lab Investigations 562; Diagnostic Peritoneal Lavage 562; Angiography 563; Preoperative Management 563; Damage Control Surgery 564; Abdominal Compartment Syndrome 564
81. Vascular Trauma of Extremities 567Marun RajHistorical Perspective 567; Epidemiology 567; Clinical Presentation 568; Noninvasive Imaging 568; Management of Extremity Trauma 570; Compartment Syndrome 574
82. Traumatic Head Injury 576Sushma Vijay Pingale, V Thanga Thirupathi RajanPrimary Injury 576; Secondary Injury 579
83. Thoracic Trauma 588Sushma Vijay Pingale, Marun RajInjury to Chest Wall 588; Injury to Pleura 589; Injury to Lung 591; Injury to Heart 591; Injury to Aorta 592; Injury to Esophagus 594
Jayp
ee B
rothe
rs

xxii ICU Manual
SECTION 19: Ultrasonography 84. Role of Ultrasound in Critical Care 597
Prem KumarPhysics of Ultrasound 598; Ultrasound Image Characteristics 600; Needle Orientation 602; Pulmonary Embolism 603; Procedural Uses of Ultrasound 608
SECTION 20: Acid-Base Disorders 85. Basics of Acid-Base Balance 617
Sushma Vijay PingaleBasic Concepts and Terminologies 617
86. Metabolic and Respiratory Acid-Base Disorders 623Sushma Vijay PingaleMetabolic Acidosis 623
87. Interpretation of Acid-Base Disorder 631Sushma Vijay PingaleStepwise Approach for Interpretation of ABG 631; Arterial Blood Gas Exercises 632
SECTION 21: Nutritional Support 88. Nutrition and Metabolism in Critically Ill Patients 639
Sushma Vijay PingalePathophysiology of Nutrition in Illness 639; Nutritional Assessment 640
89. Enteral and Parenteral Nutrition 647Sushma Vijay PingaleTiming of Nutritional Support 647; Routes for Giving Nutritional Support 647; Refeeding Syndrome 653
SECTION 22: Sedation and Analgesia in ICU 90. Sedation and Analgesia for Critical Care Patients 657
Prem KumarIssues to be Addressed for Management of Pain and Sedation in ICU 657; Pain and Sedation Considerations 657; Assessment of Pain 658; Pain Scales 659
91. Patient-Controlled Analgesia 670Prem KumarPre-requisites 670; Mechanics about the Device 670; How to Write an Order for PCA? 670
SECTION 23: Airway Management in ICU 92. Rapid Sequence Induction 677
Prem KumarEssential Components of Rapid Sequence Induction 677; Indications of Rapid Sequence Induction 678; Cricoid Pressure 678
Jayp
ee B
rothe
rs

Contents xxiii
93. Endotracheal Intubation in Critical Care 680Prem Kumar, Dianitta Devapriya VeronicaBasic Anatomy 680; Fast-track Evaluation and Airway Assessment before Intubation 680; Adjuncts for Airway Management 682; Intubation Techniques 687; Management of Difficult Airway 688; Care of Endotracheal Tube in ICU 690
94. Tracheostomy 693A Meenakshi SundaramEmergency Tracheostomy 693; Elective Tracheostomy 694; Types of Tracheostomy 695; Cricothyroidotomy/Minitracheostomy 696
SECTION 24: Transfusion Practice in ICU 95. Blood Transfusion: Components and Indications 703
Prem Kumar Component Separation 703
96. Complications of Blood Transfusion 709Prem KumarAdverse Reactions to Transfusion 709; Massive Blood Transfusion 713
SECTION 25: Fluid Management 97. Perioperative Fluid Balance 717
Prem KumarBasic Physiology of Fluid Balance 717
98. Fluid Resuscitation 722Prem KumarFluid Management in Perioperative Patients 722
SECTION 26: Cardiopulmonary Resuscitation 99. Basic Life Support 731
Prem KumarPhysiology of Cardiopulmonary Resuscitation 732; Adult Basic Life Support Sequence 733; Sequence of Adult Basic Life Support Skills 734; Airway Management 735
100. Advanced Cardiac Life Support 739Prem KumarAdjuncts for Airway Management 740; Management of Adult Cardiac Arrest 741
101. Cardiac Arrest in Special Situations 750Prem KumarAnaphylaxis 750; Pregnancy 751; Trauma 752; Hypothermia 753; Asthma 754; Drowning 755; Percutaneous Coronary Intervention 756; Cardiac Tamponade 756; Cardiac Surgery 756
Jayp
ee B
rothe
rs

xxiv ICU Manual
SECTION 27: Brain Death 102. Care of a Brain Dead Patient 761
Sumathy, Prem Kumar, DeepalakshmiDefinition 761; Physiology of Brain Death 761; Steps for Determining Brain Death 763; Diagnostic Criteria for the Clinical Diagnosis of Brain Death 764; Management of Heartbeating Brain Death Organ Donor 766; Management of 2nd Phase 768; Management of Respiratory System 769; Management of Endocrine System 770; Quadruple Hormonal Replacement Therapy 770
SECTION 28: Medical Ethics 103. Ethics in Critical Care 775
Prem KumarEnd-of-life Care 775
SECTION 29: Appendices 1. Normal Biochemical Values 781
Reference Values for Laboratory Tests 781
2. Clinical Scores, Indices and Equations 789APACHE II Scoring System 789; MODS Scoring System 790; SOFA Scoring System 790; Gold Criteria for Grading Severity of COPD 791; Levels of Risk Associated with Increasing Body Mass Index 791; Waist Circumference and Risk 791; SF-MPQ (Short Form–Mcgill Pain Questionnaire) 792; Ramsay Sedation Scale (RSS) 793; Richmond Agitation Sedation Scale (RASS) 793
3. Drugs, Dosages and Side Effects 797Cardiovascular System 797; Respiratory System 801; Electrolyte Imbalance 803; Endocrine Disorders 804; Gastrointestinal Disorders 806; Hepatic Dysfunction 806; Hematopoietic Disorders 807; Central Nervous System 807; Infectious Diseases 809
4. ICU Rounds 815Essential Data and Assessment for Management of Critically Ill Patients 815
Index 817Jayp
ee B
rothe
rs

7SECTION
BURNS
Chapter 23 Classification and Evaluation of Burns Prem Kumar
Chapter 24 Management of Burns Prem Kumar
Jayp
ee B
rothe
rs
Jayp
ee B
rothe
rs

The incidence of burns in India is 6–7 million per year. About 10% of these are life-threatening and require hospitalization, and they require multiple surgeries and prolonged rehabilitation.
CLASSIFICATIONThere are 3 zones, 5 depths and 5 causative types of burns injury.
Three Zones1. Zone of coagulation2. Zone of stasis 3. Zone of hyperemia.
Five Depths (Fig. 23.1)1. First degree—superficial two epidermal 2. Second degree—it has two types: Superficial and deep partial thickness3. Third degree—full thickness4. Fourth degree—involvement of deep structures such as muscle and bone.
Five Causative Types1. Hot liquids 2. Fire—flame 3. Contact with hot objects4. Chemical 5. Electrical conduction.
PHYSIOLOGICAL DISTURBANCES (TABLE 23.1 AND FLOW CHART 23.1)Burns can affect all systems but it depends on the type of burns, depth of involvement and the timing of postinjury.
CLASSIFICATION AND EVALUATION OF BURNS
Prem Kumar23CHAPTER
Jayp
ee B
rothe
rs

174 Section 7 Burns
Table 23.1 Physiological disturbances due to burns on various systems
• Respiratory system:– Early phase—Inhalational injury causing airway obstruction, CO poisoning.– Delayed phase–After few days, patient may develop ARDS, pulmonary embolism,
pneumonia, respiratory failure. – Presence of inhalational injury is an indication for endotracheal intubation.
• Cardiovascular system: Hypovolemia causing reduced tissue perfusion and lactic acidosis. Myocardial depression and venous thromboembolism.
• Central nervous system: Seizures due to hyponatremia, peripheral nerve injury. • Gastrointestinal system: Curling’s ulcer, acute necrotizing enterocolitis, acalculous
cholecystitis, pancreatitis, hepatic dysfunction due to reduced hepatic blood flow. • Renal system: Acute renal failure occur due to reduced renal blood flow.• Endocrine system: Acute adrenal insufficiency can occur due to necrosis. • Hematology: Anemia, platelet dysfunction, thrombocytopenia, DIC.• Eye: Corneal ulcer, ectopia.
BURNS ASSESSMENTHistory: Ample history is asked and the cause and duration of burns is elicited.
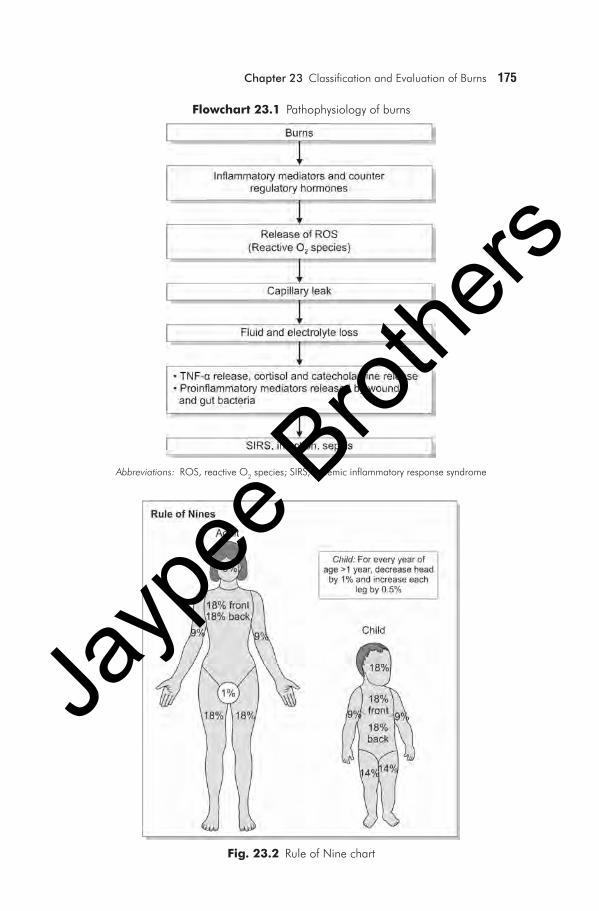
Clinical assessment of burns is based on:• Burnssurfaceareaestimation—ruleofNines,Lund and Browder chart, hand
method (Figs 23.2 and 23.3).• Depthofburns(Table23.2)• Presenceorabsenceofcircumferentialburns.
Fig. 23.1 Layers of skin and depth of burns
Jayp
ee B
rothe
rs
Chapter 23 Classification and Evaluation of Burns 175
Fig. 23.2 Rule of Nine chart
Abbreviations: ROS, reactive O2 species; SIRS, systemic inflammatory response syndrome
Flowchart 23.1 Pathophysiology of burns
Jayp
ee B
rothe
rs

176 Section 7 Burns
Table 23.2 Depth of burns and its features
Depth of burns Skin color Sensory Blisters Wound healing
1st degree (Figs 23.4A and B)
Red and blanch to touch
Painful Absent • Within 1 week • No scarring
2nd degree—superficial partial (Figs 23.5A to C)
Pink, may blanch to touch
Painful Present • Within 2 weeks• May need skin grafting• Heals with scarring
2nd degree—deep partial (Figs 23.6A to C)
Red/white Painful Variable • Within 2–3 weeks• Needs skin grafting• Heals with scarring
3rd degree—full thickness (Figs 23.7A to C)
Black or cherry red
Painless Absent • Needs skin grafting• Heals with scarring
Figs 23.4A and B I Degree: Burns (For color version, see Plate 4)
A B
Fig. 23.3 Lund and Browder chart
Jayp
ee B
rothe
rs

Chapter 23 Classification and Evaluation of Burns 177
Figs 23.5A to C II Degree: Superficial burns (For color version, see Plate 4)
Figs 23.6A to C II Degree: Deep burns (For color version, see Plate 5)
A B
C
A B
C
In the hand method of burns assessment, 1% of total body surface area equals palm and fingers of the patient’s hand.
Patientwithburnsrequirescompleteinitialevaluationsimilartoevaluationof a trauma patient but with some differences. Once the initial evaluation is over, burn specific secondary survey should be done to recognize the insults on various systems.
Jayp
ee B
rothe
rs

178 Section 7 Burns
Initial EvaluationAirway compromise can occur due to pharyngeal edema/laryngeal edema which can cause airway obstruction. Hence, the decision to intubate the patient should be done at the earliest with clinical judgment. Securing the airway in burns patient is quite challenging due to airway edema. Endotracheal tube is secured with a tie over the back of neck.
Indications of Endotracheal Intubation• Airwayobstructionduetopharyngealorlaryngealedema• Depressedlevelofconsciousness• Hypoxemianotrespondingtotreatmentwithoxygen• Circumferentialfullthicknessnasolabialburns.
Modes of Securing the Airway • Nasal/oralintubation—blindorfiberopticbronchoscopyguided• Laryngealmaskairway• Needle/surgicalcricothyroidotomy• Surgicaltracheostomy
Intravenous access is initially done with peripheral vein for initial resuscitation followed by central venous access for fluid management.
Figs 23.7A to C III Degree, burns (Courtesy: Dr Surya C Rao MS, MCH, Plastic Surgeon) (For color version, see Plate 5)
A
B
C
Jayp
ee B
rothe
rs

Chapter 23 Classification and Evaluation of Burns 179
SECONDARY SURVEY• Historyofinjury• Head and face evaluation: Look for eye globe injury (clouded appearance
over cornea), signs of inhalational injury (singed hairs, carbonaceous debris), any pressure point over injured areas, whether endotracheal tube is secured with tie.
• Central nervous system evaluation: Look for neurologic injury, order for CT-brain and spine, if needed, pain and sedation management should be started as early as possible (narcotics, benzodiazepines), determine CO-Hb level to avoidCOtoxicity.
• Look for chest wall movement and examine neck: If there is deep circumferen-tial burns, patient may require escharotomy to increase ventilation and increase venous drainage.
• Evaluation of volume status: Most of the patients are hypovolemic. Start resuscitation according to calculated fluid volumes with various formulas.
• Evaluation of extremities: In case of fracture, external splinting is done.Dopplerisdonetodeterminebloodflowsothatescharotomyorfasciotomycan be done, if there is vascular compromise.
• Look for lab investigations: Do arterial blood gas analysis, CO-Hb level, serum urea, creatinine to rule out renal involvement, chest radiography is done to ruleoutribinjury,pneumothorax,placementofcentralvenouscatheter.
BIBLIOGRAPHY 1. CBrunicardiF.Schwartz’sPrinciplesofSurgery,8thedn.McGraw-HillPublications;
2004. 2. Civetta JM, Taylor RW, Kirby RR. Critical Care, 4th edn. Philadelphia: Lippincott-
Raven;2009. 3. Gupta JL,etal.NationalProgramme forPreventionofBurn Injuries. Indian JPlast
Surg.2010;43(Suppl):S6-10. 4. HettiaratchyS,PapiniR.Initialmanagementofamajorburn:Overview.BMJ.2004;
328(7455):1555-7. 5. Irwin, Richard S Rippe, James M Irwin, Rippe’s Intensive Care Medicine, 6th edn.
LippincottWilliamsandWilkinsPublications;2008. 6. Stabilization, transfer and transport, in Advanced Burn Life Support Course Instructor
Manual.Chicago,AmericanBurnAssociation.2005.pp.73-8.
Jayp
ee B
rothe
rs


















