Manejo de Antagonist As de Vitamina k

of 41
-
Upload
camilo-coy -
Category
Documents
-
view
217 -
download
0
Transcript of Manejo de Antagonist As de Vitamina k
-
8/6/2019 Manejo de Antagonist As de Vitamina k
1/41
DOI 10.1378/chest.08-06702008;133;160S-198SChest
and Gualtiero PalaretiJack Ansell, Jack Hirsh, Elaine Hylek, Alan Jacobson, Mark CrowtherPractice Guidelines (8th Edition)
Clinicalof Chest Physicians Evidence-Based: American College*Vitamin K Antagonists
Pharmacology and Management of the
http://chestjournal.chestpubs.org/content/133/6_suppl/160S.full.htmlservices can be found online on the World Wide Web at:The online version of this article, along with updated information and
ISSN:0012-3692)http://chestjournal.chestpubs.org/site/misc/reprints.xhtml(
written permission of the copyright holder.this article or PDF may be reproduced or distributed without the priorDundee Road, Northbrook, IL 60062. All rights reserved. No part ofCopyright2008by the American College of Chest Physicians, 3300Physicians. It has been published monthly since 1935.
is the official journal of the American College of ChestChest
2008 American College of Chest Physicians by guest on June 2, 2011chestjournal.chestpubs.orgDownloaded from
http://chestjournal.chestpubs.org/content/133/6_suppl/160S.full.htmlhttp://chestjournal.chestpubs.org/content/133/6_suppl/160S.full.htmlhttp://chestjournal.chestpubs.org/site/misc/reprints.xhtmlhttp://chestjournal.chestpubs.org/site/misc/reprints.xhtmlhttp://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/site/misc/reprints.xhtmlhttp://chestjournal.chestpubs.org/content/133/6_suppl/160S.full.html -
8/6/2019 Manejo de Antagonist As de Vitamina k
2/41
Pharmacology and Management of the Vitamin K Antagonists*
American College of Chest PhysiciansEvidence-Based Clinical Practice Guidelines(8th Edition)
Jack Ansell, MD; Jack Hirsh, MD; Elaine Hylek, MD, MPH; Alan Jacobson, MD;Mark Crowther, MD; and Gualtiero Palareti, MD
This article concerning the pharmacokinetics and pharmacodynamics of vitamin K antagonists(VKAs) is part of the American College of Chest Physicians Evidence-Based Clinical PracticeGuidelines (8th Edition). It describes the antithrombotic effect of the VKAs, the monitoring of anticoagulation intensity, and the clinical applications of VKA therapy and provides specificmanagement recommendations. Grade 1 recommendations are strong and indicate that thebenefits do or do not outweigh the risks, burdens, and costs. Grade 2 recommendations suggestthat the individual patients values may lead to different choices. (For a full understanding of thegrading, see the Grades of Recommendation chapter by Guyatt et al, CHEST 2008; 133:123S131S.) Among the key recommendations in this article are the following: for dosing of VKAs, werecommend the initiation of oral anticoagulation therapy, with doses between 5 mg and 10 mg forthe first 1 or 2 days for most individuals, with subsequent dosing based on the internationalnormalized ratio (INR) response (Grade 1B); we suggest against pharmacogenetic-based dosing
until randomized data indicate that it is beneficial (Grade 2C); and in elderly and other patientsubgroups who are debilitated or malnourished, we recommend a starting dose of < 5 mg (Grade1C). The article also includes several specific recommendations for the management of patients with nontherapeutic INRs, with INRs above the therapeutic range, and with bleeding whetherthe INR is therapeutic or elevated. For the use of vitamin K to reverse a mildly elevated INR, werecommend oral rather than subcutaneous administration (Grade 1A). For patients with life-threatening bleeding or intracranial hemorrhage, we recommend the use of prothrombincomplex concentrates or recombinant factor VIIa to immediately reverse the INR (Grade 1C).For most patients who have a lupus inhibitor, we recommend a therapeutic target INR of 2.5(range, 2.0 to 3.0) [Grade 1A]. We recommend that physicians who manage oral anticoagulationtherapy do so in a systematic and coordinated fashion, incorporating patient education,systematic INR testing, tracking, follow-up, and good patient communication of results and doseadjustments [Grade 1B]. In patients who are suitably selected and trained, patient self-testing orpatient self-management of dosing are effective alternative treatment models that result inimproved quality of anticoagulation management, with greater time in the therapeutic range andfewer adverse events. Patient self-monitoring or self-management, however, is a choice made bypatients and physicians that depends on many factors. We suggest that such therapeuticmanagement be implemented where suitable (Grade 2B). (CHEST 2008; 133:160S198S)
Key words: anticoagulation; pharmacogenetics; pharmacology; quality of care; vitamin K antagonists; warfarin
Abbreviations: AMS anticoagulation management service; CHF congestive heart failure; CI confidence interval;DVT deep vein thrombosis; HR hazard ratio; INR international normalized ratio; ISI international sensitivity index;NSAID nonsteroidal antiinflammatory drug; OR odds ratio; PCC prothrombin complex concentrate; POC point of care; PSM patient self-management; PST patient self-testing; PT prothrombin time; SNP single nucleotide poly-morphism; TTR time in the therapeutic range; UC usual care; VKA vitamin K antagonist; VKOR vitamin K oxidereductase; WHO World Health Organization
SupplementANTITHROMBOTIC AND THROMBOLYTIC THERAPY 8TH ED: ACCP GUIDELINE
160S Antithrombotic and Thrombolytic Therapy 8th Ed: ACCP Guidelines
2008 American College of Chest Physicians by guest on June 2, 2011chestjournal.chestpubs.orgDownloaded from
http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/ -
8/6/2019 Manejo de Antagonist As de Vitamina k
3/41
Summary of Recommendations
2.1 Initiation and Maintenance Dosing
2.1.1. In patients beginning vitamin K antago-nist (VKA) therapy, we recommend the initia-tion of oral anticoagulation with doses between5 mg and 10 mg for the first 1 or 2 days for mostindividuals, with subsequent dosing based onthe international normalized ratio (INR) re-sponse (Grade 1B). At the present time, forpatients beginning VKA therapy without evi-dence from randomized trials, we suggestagainst the use of pharmacogenetic-based ini-tial dosing to individualize warfarin dosing(Grade 2C).
2.2 Initiation of Anticoagulation in Elderly or Other Populations
2.2.1. In elderly patients or patients who aredebilitated, are malnourished, have congestiveheart failure (CHF), have liver disease, have hadrecent major surgery, or are taking medicationsknown to increase sensitivity to warfarin ( eg, ami-odarone), we recommend the use of a startingdose of < 5 mg (Grade 1C) with subsequent dosingbased on the INR response .
2.3 Frequency of Monitoring
2.3.1. In patients beginning VKA therapy, wesuggest that INR monitoring be started afterthe initial two or three doses of oral anticoagu-lation therapy (Grade 2C).2.3.2. For patients who are receiving a stabledose of oral anticoagulants, we suggest mon-itoring at an interval of no longer than every4 weeks (Grade 2C).
2.4 Management of Nontherapeutic INRs
2.4.1. For patients with INRs above the therapeu-tic range but < 5.0 and with no significant bleed-
ing, we recommend lowering the dose or omittinga dose, monitoring more frequently, and resum-ing therapy at an appropriately adjusted dose when the INR is at a therapeutic level. If onlyminimally above therapeutic range or associated with a transient causative factor, no dose reduc-tion may be required (all Grade 1C).2.4.2. For patients with INRs of > 5.0 but < 9.0and no significant bleeding, we recommend omit-ting the next one or two doses, monitoring morefrequently, and resuming therapy at an appropri-ately adjusted dose when the INR is at a thera-peutic level (Grade 1C). Alternatively, we suggestomitting a dose and administering vitamin K (1 to2.5 mg) orally, particularly if the patient is atincreased risk of bleeding (Grade 2A). If morerapid reversal is required because the patientrequires urgent surgery, we suggest vitamin K(< 5 mg) orally, with the expectation that a reduc-tion of the INR will occur in 24 h. If the INR is stillhigh, we suggest additional vitamin K (1 to 2 mg)orally (Grade 2C).2.4.3. For patients with INRs > 9.0 and no signif-icant bleeding, we recommend holding warfarintherapy and administering a higher dose of vita-min K (2.5 to 5 mg) orally, with the expectationthat the INR will be reduced substantially in 24 to48 h (Grade 1B). Clinicians should monitor theINR more frequently, administer additional vita-min K if necessary, and resume therapy at anappropriately adjusted dose when the INRreaches the therapeutic range.2.4.4. In patients with serious bleeding and ele-vated INR, regardless of the magnitude of theelevation, we recommend holding warfarin ther-apy and giving vitamin K (10 mg) by slow IVinfusion supplemented with fresh frozen plasma,prothrombin complex concentrate (PCC), or re-combinant factor VIIa, depending on the urgencyof the situation. We recommend repeating vita-min K administration every 12 h for persistentINR elevation (all Grade 1C).2.4.5. In patients with life-threatening bleeding(eg, intracranial hemorrhage) and elevated INR,regardless of the magnitude of the elevation, werecommend holding warfarin therapy and admin-istering fresh frozen plasma, PCC, or recombi-nant factor VIIa supplemented with vitamin K, 10mg by slow IV infusion, repeated, if necessary,depending on the INR (Grade 1C).2.4.6. In patients with mild to moderately ele-vated INRs without major bleeding, we recom-mend that when vitamin K is to be given, it beadministered orally rather than subcutaneously(Grade 1A).
*From Boston University School of Medicine (Dr. Ansell), Boston,MA; Hamilton Civic Hospitals (Dr. Hirsh), Henderson ResearchCentre, Hamilton, ON, Canada; Boston University School of Med-icine (Dr. Hylek), Boston, MA; Loma Linda VA Medical Center(Dr. Jacobson), Loma Linda, CA; McMaster University, St. JosephsHospital (Dr. Crowther), Hamilton, ON, Canada; and University Hospital S. Orsola-Malpighi (Dr. Palareti), Bologna, Italy.Manuscript received December 20, 2007.Reproduction of this article is prohibited without written permissionfrom the American College of Chest Physicians (www.chestjournal.org/misc/reprints.shtml).Correspondence to: Jack Ansell, MD, Department of Medicine, Lenox Hill Hospital, 100 E 77th St, New York, NY 10075; e-mail: [email protected]: 10.1378/chest.08-0670
www.chestjournal.org CHEST / 133 / 6 / JUNE, 2008 SUPPLEMENT 161S
2008 American College of Chest Physicians by guest on June 2, 2011chestjournal.chestpubs.orgDownloaded from
http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/ -
8/6/2019 Manejo de Antagonist As de Vitamina k
4/41
2.5 Management of Variable INRs
2.5.1. For patients receiving long-term warfarintherapy with a variable INR response not attrib-utable to any of the usual known causes forinstability, we suggest a trial of daily low-dose oralvitamin K (100 to 200 g), with close monitoringof the INR and warfarin dose adjustment tocounter an initial lowering of the INR in responseto vitamin K (Grade 2B).
2.7 Management of INRs in the AntiphospholipidSyndrome
2.7.1. In patients who have a lupus inhibitor, who have no additional risk factors, and whohave no lack of response to therapy, we recom-mend a therapeutic target INR of 2.5 (INRrange, 2.0 to 3.0) [Grade 1A]. In patients whohave recurrent thromboembolic events with atherapeutic INR or other additional risk factorsfor thromboembolic events, we suggest a targetINR of 3.0 (INR range, 2.5 to 3.5) [Grade 2C].
4.1 Optimal Management of VKA Therapy
4.1.1. For health-care providers who manageoral anticoagulation therapy, we recommendthat they do so in a systematic and coordinatedfashion, incorporating patient education, sys-tematic INR testing, tracking, follow-up, andgood patient communication of results and dos-ing decisions as occurs in an anticoagulationmanagement service (AMS) [Grade 1B].
4.3 Patient Self-Testing and PatientSelf-Management
4.3.1. Patient self-management (PSM) is a choicemade by patients and health-care providers thatdepends on many factors. In patients who aresuitably selected and trained, patient self-testingor PSM is an effective alternative treatment
model. We suggest that such therapeutic manage-ment be implemented where suitable (Grade 2B).
T he coumarins or vitamin K antagonists (VKAs)have been the mainstay of oral anticoagulanttherapy for more than 60 years. Their effectivenesshas been established by well-designed clinical trialsfor the primary and secondary prevention of venousthromboembolism, for the prevention of systemicembolism in patients with prosthetic heart valves oratrial fibrillation, as an adjunct in the prophylaxis of systemic embolism after myocardial infarction, and
for reducing the risk of recurrent myocardial infarc-tion. VKAs are challenging to use in clinical practicefor the following reasons: (1) they have a narrowtherapeutic window; (2) they exhibit considerable variability in dose response among patients due togenetic and other factors; (3) they are subject tointeractions with drugs and diet; (4) their laboratory control is difficult to standardize; and (5) mainte-nance of a therapeutic level of anticoagulation re-quires a good understanding of the pharmacokineticsand pharmacodynamics of warfarin and good patientcommunication. Because warfarin is the most com-monly used VKA worldwide, we will use it inter-changeably with VKA throughout this article.
1.0 Pharmacology and Monitoring of VKAs
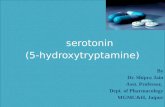
The VKAs produce their anticoagulant effect by interfering with the cyclic interconversion of vitaminK and its 2,3 epoxide (vitamin K epoxide), thereby modulating the -carboxylation of glutamate resi-dues (Gla) on the N-terminal regions of vitaminK-dependent proteins17 (Fig 1). The vitamin K-dependent coagulation factors II, VII, IX, and Xrequire -carboxylation for their procoagulant activ-ity, and treatment with VKAs results in the hepaticproduction of partially carboxylated and decarboxy-lated proteins with reduced coagulant activity.8,9Carboxylation is required for a calcium-dependentconformational change in coagulation proteins1012that promotes binding to cofactors on phospholipidsurfaces. In addition, the VKAs inhibit carboxylationof the regulatory anticoagulant proteins C, S, and Zand thereby have the potential to be procoagulant.13Under most circumstances, however, the anticoagu-lant effect of the VKAs is dominant. Carboxylationrequires the reduced form of vitamin K (VKH2), a
-glutamyl carboxylase, molecular oxygen, and car-bon dioxide.1 Vitamin K epoxide can be reused by reduction to VKH2 . The oxidation-reduction reac-tion involves a reductase pair. The first, vitamin Kepoxide reductase, is sensitive to VKA, whereas vitamin K reductase is less sensitive.13 Therefore,the anticoagulant effect of the VKAs can be over-come by low doses of vitamin K (phytonadione) [Fig1]. Patients treated with large doses of vitamin K canbecome resistant to warfarin for up to 1 week ormore because the vitamin K accumulating in theliver is available to the VKA-insensitive reductase.
The VKAs also interfere with the carboxylation of Gla proteins that are synthesized in bone.1417 Al-though these effects contribute to fetal bone abnormal-ities when mothers are treated with a VKA duringpregnancy,18,19 it is unclear how they might affectchildren. Two uncontrolled cohort studies described
162S Antithrombotic and Thrombolytic Therapy 8th Ed: ACCP Guidelines
2008 American College of Chest Physicians by guest on June 2, 2011chestjournal.chestpubs.orgDownloaded from
http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/ -
8/6/2019 Manejo de Antagonist As de Vitamina k
5/41
reduced bone density in children on warfarin for 1 year, but the role of the underlying disorders in reduc-ing bone density remains unclear.20
1.1 Pharmacokinetics and Pharmacodynamicsof Warfarin
Warfarin is the most common VKA in clinical use.It is a racemic mixture of two optically active iso-mers, the R and S enantiomers. Warfarin is highly water soluble, rapidly absorbed from the GI tract,has high bioavailability,21,22 and reaches maximalblood concentrations about 90 min after oral admin-istration.21,23 Racemic warfarin has a half-life of 36 to42 h24 (R-warfarin, 45 h; S-warfarin, 29 h); circulatesbound to plasma proteins (mainly albumin); andaccumulates in the liver, where the two enantiomersare metabolically transformed by different pathways(Fig 1).24 The S enantiomer of warfarin (2.7 to 3.8times more potent than the R enantiomer) is metab-olized primarily by the CYP2C9 enzyme of thecytochrome P450 system.25 The less potent R enan-
tiomer is metabolized primarily by two cytochromeenzymes, 1A2 and 3A4. The relationship betweenthe dose of warfarin and the response is modified by genetic and environmental factors that can influencethe absorption of warfarin, its pharmacokinetics, andits pharmacodynamics.
Like warfarin, acenocoumarol and phenprocou-mon also exist as optical isomers but with differentstereochemical characteristics. R-acenocoumarol hasan elimination half-life of 9 h; is primarily metabo-lized by CYP2C9 and CYP2C19; and is more potentthan S-acenocoumarol due to faster clearance of S-acenocoumarol, which has an elimination half-lifeof 0.5 h and is primarily metabolized by CYP2C9.26Phenprocoumon is a much longer-acting agent, withboth the R- and the S-isomers having eliminationhalf-lives of 5.5 days. Both are metabolized by CYP2C9, and S-phenprocoumon is 1.5 to 2.5 timesmore potent than R-phenprocoumon.27
Superwarfarin rodenticides are commonly used inthe United States, and most contain brodifacoum, a
Figure 1. Vitamin K1 is reduced to vitamin KH2 . The major warfarin-sensitive enzyme in this reactionis the vitamin K oxide reductase mainly inhibited by the S enantiomer of warfarin. S-warfarin ismetabolized by the p450 cytochrome enzyme, CYP2C9.
www.chestjournal.org CHEST / 133 / 6 / JUNE, 2008 SUPPLEMENT 163S
2008 American College of Chest Physicians by guest on June 2, 2011chestjournal.chestpubs.orgDownloaded from
http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/ -
8/6/2019 Manejo de Antagonist As de Vitamina k
6/41
4-hydroxycoumarin with high lipid solubility and anelimination half-life of 24 days.28 In cases of acciden-tal or intentional brodifacoum poisoning, the princi-pal treatment is vitamin K, with repeated doses givenanywhere from daily to every few days to counteractthe long half-life of brodifacoum.28,29 For patients who are actively bleeding, immediate reversal can beachieved with factor concentrates, such as prothrom-bin complex concentrates (PCCs) or recombinantfactor VIIa along with repeated daily administrationof vitamin K.30
1.1.1 Genetic Factors
There are a number of mutations in the genecoding for the cytochrome P450 2C9 hepatic micro-somal enzyme, which is responsible for the oxidativemetabolism of the more potent warfarin S enantio-mer,24,3135 and these mutations will alter the phar-macokinetics of warfarin. The most common and
best documented alleles, designated 2C9*
2 or2C9* 3 to differentiate it from the wild type, 2C9* 1,are associated with an impaired ability to metabolizeS-warfarin, resulting in an increased S-warfarinelimination half-life. Mutations in this gene areindependently responsible for the reduced war-farin requirements seen in individuals with one ormore combinations of these polymorphisms(Table 1).32,36,37 Several investigations32,37,38 haveshown that these mutations, as well as others,34,39,40also are associated with an increase in adverseclinical outcomes that also occur with the use of
acenocoumarol but not with phenprocoumon.41,42
The target for warfarins inhibitory effect on the vitamin K cycle is the vitamin K oxide reductase
(VKOR) enzyme first described in 1974.43 The genecoding for the VKOR protein was recently identifiedand found to be located on the short arm of chro-mosome 16.44,45 The gene encodes for several iso-forms of the protein that collectively are termed the VKOR complex 1 (VKORC1). Subsequently, muta-tions in this gene have been identified, leading toenzymes with varying sensitivities to inhibition by warfarin,45,4650 thereby affecting the pharmacody-namics of warfarin. These mutations are likely to bethe cause of hereditary warfarin resistance in someindividuals.50 The mutations occur with differingfrequencies in various ethnic populations and ac-count, in part, for the difference in warfarin dosesrequired to maintain a therapeutic international nor-malized ratio (INR)35,46 48,51 (Table 1).
Another genetic mutation that affects the phar-macodynamics of warfarin is in the factor IXpropeptide. It causes selective reduction in factor
IX during treatment with coumarin drugs withoutexcessive prolongation of the prothrombin time(PT).33 Factor IX activity decreases to about 1 to3% of normal, whereas levels of other vitaminK-dependent coagulation factors decrease to 30 to40% of normal. Two distinct missense mutationsinvolving the propeptide coding region have beendescribed. They are estimated to occur in 1.5%of the population and are expressed as selectively increased sensitivity to the VKA-mediated reduc-tion of factor IX activity.52 This selective markedreduction in factor IX activity has been report-
ed33,52
to increase the risk of bleeding duringanticoagulant therapy, and management of suchrare patients can be difficult.53
Table 1 Observed Frequency of CYP2C9 and VKORC * Variants Among Various Ethnic Groups (Section 1.1.1)
CYP2C9 geneticalleles pointmutation
CYP2C9* 1Arg144 /IIc359 , %
CYP2C9* 2Cys144 /IIc359 , %
CYP2C9* 3Arg144 /Leu351 , %
CYP2C9* 4Arg144 /Thr359 , %
CYP2C9* 5Arg144 /Glu360 , %
Ethnic group White 7986 819.1 610 ND NDIndigenous Canadian 91 3 6 ND NDAfrican American 98.5 13.6 0.51.5 ND 2.3Asian 9598.3 0 1.75 01.6% 0
VKORC geneticHaplotype H1 CCGATCTCTG H7 TCGGTCCGCASequence H2 CCGAGCTCTG H8 TAGGTCCGCA
H9 TACGTTCGCGEthnic group, %
European 37 58African 14 49Asian 89 10
* CYP2C9 and VKORC data from Wittkowsky 32 and Rieder et al.47 ND not determined.CYP2C9* 2, * 3, * 4, and * 5 represent genetic polymorphisms of the wild-type enzyme, CYP2C9* 1.H1 and H2 represent warfarin-sensitive haplotype. H7, H8, and H9 represent warfarin-resistant haplotype.
164S Antithrombotic and Thrombolytic Therapy 8th Ed: ACCP Guidelines
2008 American College of Chest Physicians by guest on June 2, 2011chestjournal.chestpubs.orgDownloaded from
http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/ -
8/6/2019 Manejo de Antagonist As de Vitamina k
7/41
1.1.2 Environmental Factors and Drug Interactions
Environmental factors such as drugs, diet, and various disease states can alter the pharmacokineticsof warfarin.54 Consequently, the INR should bemeasured more frequently than the usual 4-weekinterval when virtually any drug, dietary supplement,or herbal medicine is added or withdrawn from theregimen of a patient treated with warfarin. Drugssuch as cholestyramine can reduce the anticoagulanteffect of warfarin by reducing its absorption. Otherdrugs potentiate the anticoagulant effect of warfarinby inhibiting its clearance, whereas some drugs may inhibit the anticoagulant effect by enhancing itsclearance.55 These latter effects may be throughstereoselective or nonselective pathways.56,57 (Ste-reoselective interactions may affect the oxidativemetabolism of either the S enantiomer or R enan-tiomer of warfarin.) Table 2 provides a comprehen-sive list of drugs that potentiate, inhibit, or have noeffect on the anticoagulant effect of warfarin.54 Amajor problem with the literature on this topic isthat many reports are single case studies and not well documented. Thus, the drugs categorized inTable 2 are listed by their probability of causationbased on the quality of documentation as assessedby Holbrook et al54 in their systematic review.
The inhibition of S-warfarin metabolism is moreimportant clinically because this enantiomer is fivetimes more potent than the R enantiomer as a VKA.56,57 Phenylbutazone,58 sulfinpyrazone,59 met-ronidazole,60 and trimethoprim-sulfamethoxazole61
inhibit the clearance of S-warfarin, and each poten-tiates the effect of warfarin on the PT. In contrast,drugs such as cimetidine and omeprazole, whichinhibit the clearance of the R-isomer, potentiate thePT only modestly in patients who have been treated with warfarin.57,60,62 Amiodarone is a potent inhibitorof the metabolic clearance of both the S enantiomerand the R enantiomer and potentiates warfarinanticoagulation.63 The anticoagulant effect is inhib-ited by drugs like barbiturates, rifampin, azathio-prine, and carbamazepine, which increase hepaticclearance. Long-term alcohol consumption has asimilar potential to increase the clearance of warfa-rin, but ingestion of even relatively large amounts of wine had little influence on the PT in normal volunteers who were given warfarin.64 The effect of enzyme induction on warfarin therapy has beendiscussed in more detail in a critical review.65
Drugs also may influence the pharmacodynamics of warfarin by inhibiting the synthesis of or increasing theclearance of vitamin K-dependent coagulation factorsor by interfering with other pathways of hemostasis.The anticoagulant effect of warfarin is augmented by second-generation and third-generation cephalospo-
rins, which inhibit the cyclic interconversion of vitaminK66,67 ; by thyroxine, which increases the metabolism of coagulation factors68 ; and by clofibrate through anunknown mechanism.69 Doses of salicylates of 1.5g/d70 may augment the anticoagulant effect of warfarin.The commonly held view that acetaminophen does notsignificantly augment warfarins effect has been chal-lenged. Thus, a potentiating effect of acetaminophenhas been reported when large doses are used overprolonged periods.71,72 Although the potentiating effectmay be minimal and inconsistent in some cases, largedoses of acetaminophen have been shown to prolongthe INR in a recent randomized, blinded trial.73 Acet-aminophens mechanism of warfarin potentiation ispossibly by inhibition of VKOR by a toxic metabolite of the drug,74 although the accumulation of this metabo-lite may vary among individuals, thus accounting for a variable potentiating effect.75 Heparin potentiates theanticoagulant effect of warfarin but in therapeuticdoses produces only a slight prolongation of the PT.The mechanisms by which erythromycin76 and someanabolic steroids77 potentiate the anticoagulant effectof warfarin are unknown. Sulfonamides and severalbroad-spectrum antibiotic compounds may augmentthe anticoagulant effect of warfarin in patients consum-ing diets that are deficient in vitamin K by eliminatingbacterial flora and aggravating vitamin K deficiency.78
Aspirin,79 nonsteroidal antiinflammatory drugs(NSAIDs),80,81 penicillins in high doses,82,83 and moxa-lactam67 increase the risk of warfarin-associated bleed-ing by inhibiting platelet function. Of these drugs,aspirin is the most important because of its widespreaduse and prolonged effect.84,85 Aspirin and NSAIDs alsocan produce gastric erosions that increase the risk of upper GI bleeding. This effect can occur even withcyclooxygenase-2 inhibitors, which were originally be-lieved to be less likely to predispose to gastric bleedingthan NSAIDs.81 In one case-controlled analysis of 98,821 subjects on warfarin identified in linked data-bases, celecoxib and rofecoxib were associated with a1.7-fold or 2.4-fold risk of GI hemorrhage, respective-ly.81 The risk of clinically important bleeding is height-ened when high doses of aspirin are taken duringhigh-intensity warfarin therapy (INR range, 3.0 to4.5).79,86 However, low doses of aspirin ( ie, 75 to 100mg daily) combined with moderate-intensity and low-intensity warfarin anticoagulation therapy also are asso-ciated with increased rates of bleeding.87,88
Nutritional supplements and herbal products areparticularly problematic in that warfarin-treated pa-tients often fail to inform physicians that they areusing such products, and physicians rarely ask. Inone survey of 1,200 subjects from four large antico-agulation clinics, one third used dietary supplements,and one third indicated that their provider failed todiscuss potential interactions with them.89 There is
www.chestjournal.org CHEST / 133 / 6 / JUNE, 2008 SUPPLEMENT 165S
2008 American College of Chest Physicians by guest on June 2, 2011chestjournal.chestpubs.orgDownloaded from
http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/ -
8/6/2019 Manejo de Antagonist As de Vitamina k
8/41
T a b l e 2 D r u g , F o o d , a n d D i e t a r y S u p p
l e m e n t I n t e r a c t i o n s W i t h W a r
f a r i n
b y L e v e
l o f S u p p o r t
i n g E v i
d e n c e a n
d D i r e c t i o n o f I n t e r a c t i o n
( S e c t i o n 1 . 1 . 2 ) *
L e v e l o f
C a u s a t i o n
A n t i i n f e c t i v e s
C a r d i o v a s c u l a r
A n a l g e s i c s ,
A n t i i n f l a m m a t o r i e s ,
a n d I m m u n o l o g i c s
C N S D r u g s
G I
D r u g s a n d F o o d
H e r b a l S u p p l e m e n t s
O t h e r D r u g s
P o t e n t i a t i o n
H i g h l y
p r o b a b l e
C i p r o f l o x a c i n
C o t r i m o x a z o l e
E r y t h r o m y c i n
F l u c o n a z o l e
I s o n i a z i d
M e t r o n i d a z o l e
M i c o n a z o l e O r a l G e l
M i c o n a z o l e V a g S u p p
V o r i c o n a z o l e
A m i o d a r o n e
C l o f i b r a t e
D i l t i a z e m
F e n o f i b r a t e
P r o p a f e n o n e
P r o p r a n o l o l
S u l f i n p y r a z o n e
( b i p h a s i c w i t h l a t e r
i n h i b i t i o n )
P h e n y l b u t a z o n e
P i r o x i c a m
A l c o h o l ( i f c o n c o m i t a n t
l i v e r d i s e a s e )
C i t a l o p r a m
E n t a c a p o n e
S e r t r a l i n e
C i m e t i d i n e
F i s h o i l
M a n g o
O m e p r a z o l e
B o l d o - f u n u g r e e k
Q u i l i n g g a o
A n a b o l i c s t e r o i d s
Z i l e u t o n
P r o b a b l e
A m o x i c i l l i n / c l a v u l a n a t e
A z i t h r o m y c i n
C l a r i t h r o m y c i n
I t r a c o n a z o l e
L e v o f l o x a c i n
R i t o n a v i r
T e t r a c y c l i n e
A s p i r i n
F l u v a s t a t i n
Q u i n i d i n e
R o p i n i r o l e
S i m v a s t a t i n
A c e t a m i n o p h e n
A s p i r i n
C e l e c o x i b
D e x t r o p r o p o x p h e n e
I n t e r f e r o n
T r a m a d o l
D i s u l f i r a m
C h l o r a l h y d r a t e
F l u v o x a m i n e
P h e n y t o i n ( b i p h a s i c
w i t h l a t e r i n h i b i t i o n )
G r a p e f r u i t
D a n s h e n
D o n q u a i
L y c i u m B a r b a r u m l
P C - S
P E S
F l u o r o u r a c i l
G e m c i t a b i n e
L e v a m i s o l e / f l u o r o u r a c i l
P a c l i t a x e l
T a m o x i f e n
T o l t e r o d i n e
P o s s i b l e
A m o x i c i l l i n
A m o x i c i l l i n / t r a n e x a m i c
r i n s e
C h l o r a m p h e n i c o l
G a t i f l o x a c i n
M i c o n a z o l e
T o p i c a l G e l
N a l i d i x i c A c i d
N o r f l o x a c i n O f l o x a c i n
S a q u i n a v i r
T e r b i n a f i n e
A m i o d a r o n e - i n
d u c e d
t o x i c o s i s
D i s o p y r a m i d e
G e m f i b r o z i l
M e t o l a z o n e
C e l e c o x i b
I n d o m e t h a c i n
L e f l u n o m i d e
P r o p o x p h e n e
R o f e c o x i b
S u l i n d a c
T o l m e t i n
T o p i c a l s a l i c y l a t e s
F e l b a m a t e
O r l i s t a t
D a n s h e n / m e t h y l
s a l i c y l a t e s
A c a r b o s e
C y c l o p h o s p h a m i d e /
m e t h o t r e x a t e /
f l u o r o u r a c i l
C u r b i c i n D a n a z o l
i f o s p h a m i d e
T r a s t u z u m a b
H i g h l y
i m p r o b a b l e
C e f a m a n d o l
C e f a z o l i n
S u l f i s o x a z o l e
B e z a f i b r a t e
H e p a r i n
L e v a m i s o l e
M e t h y l p r e d n i s o l o n e
N a b u m e t o n e
F l u o x e t i n e / d i a z e p a m
Q u e t i a p i n e
E t o p o s i d e / c a r b o p l a t i n
L e v o n o r g e s t r e l
I n h i b i t i o n
H i g h l y
p r o b a b l e
G r i s e o f u l v i n
N a f c i l l i n R i b a v i r i n
R i f a m p i n
C h l e s t y r a m i n e
M e s a l a m i n e
B a r b i t u r a t e s
C a r b a m a z e p i n e
H i g h
v i t a m i n k c o n t e n t
f o o d s / e n t e r a l f e e d s
A v o c a d o ( l a r g e
a m
o u n t s )
M e r c a p t o p u r i n e
P r o b a b l e
D i c l o x a c i l l i n
R i t o n a v i r
B o s e n t a n
A z a t h i o p r i n e
C h l o r a d i a z e p o s i d e
S o y m i l k
S u c r a l f a t e
G i n s e n g
C h e l a t i o n t h e r a p y
I n f l u e n z a v a c c i n e
M u l t i v i t a m i n s u p p l e m e n t
R a l o x i f e n e H C L
P o s s i b l e
T e r b i n a f i n e
T e l m i s a r t a n
S u l f a s a l a z i n e
S u s h i c o n t a i n i n g
s e a w e e d
C y c l o s p o r i n e
E t r e t i n a t e
U b i d i c a r e m o n e
H i g h l y
i m p r o b a b l e
C l o x a c i l l i n
N a t c i l l i n / d i c l o x a c i l l i n
T e i c o p l a n i n
F u r o s e m i d e
P r o p o f o l
G r e e n t e a
* D a t a f r o m H o l b r o o k e t a l
5 4
w i t h p e r m i s s i o n .
166S Antithrombotic and Thrombolytic Therapy 8th Ed: ACCP Guidelines
2008 American College of Chest Physicians by guest on June 2, 2011chestjournal.chestpubs.orgDownloaded from
http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/ -
8/6/2019 Manejo de Antagonist As de Vitamina k
9/41
also little or no standardization of the content of suchproducts, especially herbal remedies, and reports of interactions often are anecdotal or single-case stud-ies without good substantiation.9093 Of the higher-quality studies, ginkgo and ginger were shown not tohave an effect on warfarin in healthy subjects in arandomized, open-label, crossover study,94 and co-enzyme Q10 (and ginkgo) were shown not to have aneffect in a randomized, double-blind, crossoverstudy.95 Ginseng was shown to reduce the effect of warfarin in a randomized, placebo-controlled trial.96Not surprisingly, products with a high content of vitamin K, such as green tea, were shown to reducethe anticoagulant effect of warfarin.54
Subjects receiving long-term warfarin therapy aresensitive to fluctuating levels of dietary vitaminK,97,98 which is derived predominantly from phyllo-quinones in plant material.98 Sadowski et al99 havelisted the phylloquinone content of a wide range of foodstuffs, which also can be found on the Internet(http://ods.od.nih.gov/factsheets/cc/coumadin1.pdf).Phylloquinones act through the warfarin-insensitivepathway.100 Important fluctuations in vitamin K in-take can occur in both healthy and sick subjects.101An increased intake of dietary vitamin K that issufficient to reduce the anticoagulant response to warfarin97 occurs in patients consuming green vege-tables or vitamin K-containing supplements, whilefollowing weight-reduction diets, and in patients whohave been treated with vitamin K supplements.Reduced dietary vitamin K intake potentiates theeffect of warfarin in sick patients who have beentreated with antibiotics and IV fluids without vitaminK supplementation and in patients who have states of fat malabsorption.
Hepatic dysfunction potentiates the response to warfarin through the impaired synthesis of coagula-tion factors. Hypermetabolic states produced by fever or hyperthyroidism increase warfarin respon-siveness, probably by increasing the catabolism of vitamin K-dependent coagulation factors.68,102
1.2 The Antithrombotic Effect of VKAs
The antithrombotic effect of VKAs has conven-tionally been attributed to their anticoagulant effect, which in turn is mediated by the reduction of four vitamin K-dependent coagulation factors. Evidencesuggests, however, that the anticoagulant and anti-thrombotic effects can be dissociated and that thereduction of prothrombin and possibly factor X aremore important than the reduction of factors VII andIX for the antithrombotic effect. This evidence isindirect and has been derived from the followingobservations. First, the experiments of Wessler andGitel103 more than 40 years ago using a stasis model
of thrombosis in rabbits showed that the antithrom-botic effect of warfarin requires 6 days of treatment, whereas an anticoagulant effect develops in 2 days.The antithrombotic effect of warfarin requires thereduction of prothrombin (factor II), which has arelatively long half-life of about 60 to 72 h compared with 6 to 24 h for other vitamin K-dependent factorsthat are responsible for the more rapid anticoagulanteffect. Second, in a rabbit model of tissue factor-induced intravascular coagulation,104 the protectiveeffect of warfarin was mainly a result of loweringprothrombin levels. Third, Patel and associates105demonstrated that clots formed from umbilical cordplasma containing about half the prothrombin con-centration of plasma from adult control subjectsgenerated significantly less fibrinopeptide A thanclots formed from maternal plasma. The view that warfarin exerts its antithrombotic effect by reducingprothrombin levels is consistent with observationsthat clot-bound thrombin is an important mediatorof clot growth106 and that reduction in prothrom-bin levels decreases the amount of thrombin gen-erated and bound to fibrin, thereby reducingthrombogenicity.105
The suggestion that the antithrombotic effect of warfarin is reflected in lower levels of prothrombinforms the basis for overlapping the administration of heparin with warfarin until the PT or INR is prolongedinto the therapeutic range during the treatment of patients with thrombosis. Because the half-life of pro-thrombin is about 60 to 72 h, at least 4 days of overlapis necessary. Furthermore, the levels of native pro-thrombin antigen during warfarin therapy more closely reflect antithrombotic activity than the PT.107
1.3 Monitoring Anticoagulation Intensity
The PT test108 is the most common test used tomonitor VKA therapy. The PT responds to a reductionof three of the four vitamin K-dependent procoagulantclotting factors ( ie, II, VII, X) that are reduced by warfarin at a rate proportional to their respectivehalf-lives. Thus, during the first few days of warfarintherapy, the PT reflects mainly a reduction of factor VII, the half-life of which is approximately 6 h. Subse-quently, the reduction of factors X and II contributes toprolongation of the PT. The PT assay is performed by adding calcium and thromboplastin to citrated plasma.Thromboplastins vary in responsiveness to a reductionof the vitamin K-dependent coagulation factors. Anunresponsive thromboplastin produces less prolonga-tion of the PT for a given reduction in vitamin K-dependent clotting factors than a responsive one. Theresponsiveness of a thromboplastin can be measured by assessing its international sensitivity index (ISI) [seebelow]. Highly sensitive thromboplastins (ISI, approx-
www.chestjournal.org CHEST / 133 / 6 / JUNE, 2008 SUPPLEMENT 167S
2008 American College of Chest Physicians by guest on June 2, 2011chestjournal.chestpubs.orgDownloaded from
http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/ -
8/6/2019 Manejo de Antagonist As de Vitamina k
10/41
imately 1.0) that comprise human tissue factor pro-duced by recombinant technology and defined phos-pholipid preparations are now available. Poller109 andKirkwood,110 have reviewed the history of standardiza-tion of the PT, and more detailed discussions can befound in prior editions of this article.111
PT monitoring of warfarin treatment is not stan-dardized when expressed in seconds, as a simpleratio of the patients plasma value to that of plasmafrom a healthy control subject, or as a percentage of diluted normal plasma. A calibration model,110 which was adopted in 1982, is now used to standardizereporting by converting the PT ratio measured withthe local thromboplastin into an INR, calculated asfollows:
INR (patient PT/mean normal PT)ISI
orlog INR ISI (log observed PT ratio)
where ISI denotes the ISI of the thromboplastinused at the local laboratory to perform the PTmeasurement. The ISI reflects the responsiveness of a given thromboplastin to the reduction of the vitamin K-dependent coagulation factors compared with the primary World Health Organization (WHO)international reference preparations so that the moreresponsive the reagent, the lower the ISI value.109,110As the INR standard of reporting was widely adopted, a number of problems surfaced, which arelisted in Table 3 and reviewed briefly below.
The INR is based on ISI values derived from theplasma of patients who had received stable antico-agulant doses for at least 6 weeks.112 As a result, theINR is less reliable early in the course of warfarintherapy, particularly when results are obtained fromdifferent laboratories. Even under these conditions,however, the INR is more reliable than the uncon- verted PT ratio113 and is thus recommended duringboth the initiation and maintenance of warfarintreatment. The validity of the INR in other condi-tions of impaired coagulation has not been fully evaluated. Although the INR may be no worse ameasure of impaired coagulation in liver disease thanthe PT in raw seconds or the unconverted PTratio,114,115 there is evidence that the PT reported inpercent activity based on a dilution curve of normalplasma is a more accurate reflection of liver-inducedcoagulation impairment.116,117
The INR accuracy can be influenced by reagentsof different sensitivities118 and by the automated clotdetectors now used in most laboratories.119126 Ingeneral, the College of American Pathologists hasrecommended127 that laboratories use thromboplas-tin reagents that are at least moderately responsive( ie, ISI, 1.7) and reagent/instrument combinationsfor which the ISI has been established and validated.
ISI values provided by the manufacturers of thromboplastin reagents are not invariably correct when applied locally,128130 and this adversely affectsthe reliability of measurements. Local calibrationscan be performed using plasma samples with certi-fied PT values to determine the instrument-specificISI. The mean normal plasma PT is not interchange-able with a laboratory control PT.131 Therefore, theuse of other than a properly defined mean normalPT can yield erroneous INR calculations, particularly when less responsive reagents are used. The meannormal PT should be determined with each newbatch of thromboplastin with the same instrumentused to assay the PT.131
The concentration of citrate that is used to anti-coagulate plasma may affect the INR.132,133 In gen-eral, higher citrate concentrations (3.8%) lead tohigher INR values,132 and underfilling the bloodcollection tube spuriously prolongs the PT because
Table 3 Potential Problems With the INR (Causes of Erroneous INR) [Section 1.3] *
Problems Description
Incorrect PTR fromerroneous PT determinationdue to pretest variables(sampling and bloodcollection problems)
Trisodium citrate concentration,storage time, storagetemperature, evacuated tubeeffects, inadequate sample, variations in manual technique
Incorrect normal value From nonuse of MNPT, errorin MNPT due to:(1) unrepresentative selection;(2) technical faults (see above);(3) nonuse of geometric mean
Incorrect ISI of localthromboplastin reagent/testsystem from lack of reliability of the ISI resultprovided by themanufacturer
Incorrect choice of IRP; poordistribution of coumarin testsamples across treatment range;inadequate numbers of testsamples in ISI calibration;incorrect transformation of PTR of test plasmas to INR
Drift of ISI since originalcalibration
Instrument (coagulometer)effects on INR at local siteLupus anticoagulant effects on
some thromboplastinreagents
Lack of reliability of the INRsystem when used at theonset of warfarin therapy and for screening for acoagulopathy in patients with liver disease
Relative lack of reliability of INR 4.5, as these valuesare excluded from ISIcalibrations
* IRP international reference preparation; MNPT mean normalPT; PTR prothrombin time ratio.
168S Antithrombotic and Thrombolytic Therapy 8th Ed: ACCP Guidelines
2008 American College of Chest Physicians by guest on June 2, 2011chestjournal.chestpubs.orgDownloaded from
http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/ -
8/6/2019 Manejo de Antagonist As de Vitamina k
11/41
-
8/6/2019 Manejo de Antagonist As de Vitamina k
12/41
showed that the efficacy of oral anticoagulant agents isreduced when the INR falls to 2.0.
In contrast to studies in the primary and secondary prevention of venous thrombosis and in the preven-tion of systemic embolism in patients with atrialfibrillation, warfarin at an INR of 2.0 to 3.0 has notbeen compared to a higher target INR in patients with acute myocardial infarction except when theoral anticoagulant was combined with aspirin. Tworandomized trials183,184 reported that a higher-inten-sity warfarin regimen (INR, 3.0 to 4.0) is moreeffective than aspirin alone in preventing recurrentinfarction, stroke, or death and is as effective and atleast as safe as the combination of aspirin and amoderate-intensity anticoagulant regimen (INR, 2.0to 2.5) following an episode of acute coronary syn-drome. In contrast, the combination of aspirin andmoderate-intensity anticoagulation (INR, 2.0 to 3.0)is more effective than aspirin alone following anepisode of acute coronary syndrome, albeit, at asignificantly greater risk of major bleeding.85 Thecombination of a lower-intensity anticoagulant regi-men (INR, 1.5 to 2.5) and aspirin has been shown tobe no more effective than aspirin alone.185,186 Thesesecondary prevention studies contrast with thosereported in the primary prevention of myocardialinfarction in which low-intensity warfarin therapy (INR, 1.3 to 1.8) either used alone or in combination with aspirin was effective in high-risk men.88
In conclusion, a single therapeutic range for VKAsmay not be optimal for all indications. However, amoderate-intensity INR(2.0 to 3.0) is effective formostindications. The possible exception is the primary pre- vention of myocardial infarction in high-risk patients in which a lower INR is preferable. In addition, a lowerINR range (1.5 to 2.0) is effective in patients with venous thrombosis who have received 6 months of full-dose treatment (INR, 2.0 to 3.0), although thelower intensity is less effective than thehigher intensity.Fixed-dose warfarin therapy has a reduced efficacy ornone at all. The optimal intensity for patients withprosthetic heart valves remains uncertain, althoughthere is evidence that such patients do not require the very-high-intensity regimens that have been used in thepast. Although defining an appropriate range is animportant step in improving patient outcomes, it is only the first of two steps. The second is ensuring that thetargeted range is achieved promptly and maintained. Ingeneral, success in achieving this second goal has beensuboptimal. It is better when the INR is controlled by experienced personnel in anticoagulant clinics and by using computer-assisted dosage adjustment.187 Clini-cians can find specific recommendations regarding theoptimal intensity of therapy for each of these indica-tions in the articles in this supplement that deal witheach indication.
2.0 Dose Management of VKA Therapy
Using the correct intensity of a coumarin antico-agulant and maintaining the patient in the therapeu-tic range are two important determinants of itstherapeutic effectiveness and safety. High-quality dose management is needed to achieve and maintainthe INR in the therapeutic range. The ability of the
health-care provider to make appropriate dosage andfollow-up decisions can have a major impact ontherapeutic effectiveness. The comprehensive man-agement of the VKAs requires a knowledgeablehealth-care provider, an organized system of follow-up, reliable PT monitoring, and good patient com-munication and education.187189
The following discussion addresses a number of management issues pertaining to the use of VKAs. Asystematic review of the literature was performedbased on predefined criteria for the population atrisk, the intervention or exposure evaluated, the
outcomes assessed, and the methodology of the trialsevaluated (Table 4).
2.1 Initiation and Maintenance Dosing
Following the administration of warfarin, an initialeffect on the INR usually occurs within the first 2 or3 days, depending on the dose administered, and anantithrombotic effect occurs within the next severaldays.190,191 Heparin or low-molecular-weight heparinshould be administered concurrently when a rapidanticoagulant effect is required, and its administra-tion should be overlapped with warfarin until theINR has been in the therapeutic range for at least 2days to allow for further reduction of factors X andII. A loading dose ( ie, 10 mg) of warfarin is notrecommended. A number of randomized studieshave supported the use of a lower initiation dose.Harrison et al190 and Crowther et al192 found that inhospitalized, predominantly elderly patients, com-mencing with an average maintenance dose of 5 mg warfarin usually results in an INR of 2.0 in 4 or 5days with less excessive anticoagulation compared tothat with an initial 10-mg dose. Kovacs et al,193however, found that in outpatients who had beentreated for venous thromboembolism, an initial10-mg dose for the first 2 days of therapy comparedto a 5-mg dose resulted in a more rapid achievementof a therapeutic INR (1.4 days earlier) without adifference in rates of excessive anticoagulation. Thisstudy,193 however, included fewer patients over 75 years of age than did the study of hospitalizedpatients.192 Thus, there is room for flexibility in select-ing a starting dose of warfarin. Some clinicians prefer touse a large starting dose (eg, 7.5 to 10 mg), whereas astarting dose of 5 mg might be appropriate in elderly patients; in patients with impaired nutrition, liver dis-
170S Antithrombotic and Thrombolytic Therapy 8th Ed: ACCP Guidelines
2008 American College of Chest Physicians by guest on June 2, 2011chestjournal.chestpubs.orgDownloaded from
http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/ -
8/6/2019 Manejo de Antagonist As de Vitamina k
13/41
ease, or congestive heart failure (CHF); and in patients who are at high risk of bleeding. An initial dose of 2 to3 mg is appropriate for patients who have undergoneheart valve replacement.194,195
In the past few years, studies have shown thatpharmacogenetics plays an important role in the phar-macokinetic and pharmacodynamic behavior of warfa-rin. Single nucleotide polymorphisms (SNPs) in thegene coding for CYP2C9, the principal enzyme respon-sible formetabolizing theS enantiomer of warfarin,willsignificantly alter the rate of metabolism ( ie, half-life) of warfarin, affecting both the rapidity of initial effect andthe dose required to maintain a therapeutic INR.Similarly, various mutations in the gene coding for the VKORC1 enzyme will lead to a protein that is eithersensitive or resistant to warfarin inhibition and, thus,affect the initial dose required to achieve a therapeutic
INR as well as the dose required to maintain a thera-peutic INR. In a retrospective, observational analysis,Joffe et al196 found that CYP2C9 polymorphisms inde-pendently predicted low warfarin requirements afteradjusting for body mass index, age, acetaminophen use,and race (odds ratio [OR], 24.8; 95% confidenceinterval [CI], 3.83 to 160.78). Gage et al197 developed adosing algorithm based on CYP2C9 polymorphismsalong with clinical and demographic factors in 369patients on stable warfarin therapy. Older age, lowbody surface area, and the presence of CYP2C9* 2 orCYP2C9* 3 alleles were strongly associated with lower warfarin dose requirements (p 0.001). The mainte-nance dose decreased by 8% per decade of age, by 13%per SD in body surface area, by 19% per CYP2C9* 2allele, and by 30% per CYP2C9* 3 allele. These factors,along with gender, accounted for 39% of the variance
Table 4 Question Definition and Eligibility Criteria for Managing Oral Anticoagulant Therapy for Which Recommendations Are Being Proposed (Section 2.0) *
Section PopulationIntervention or
Exposure Outcomes Methodology Exclusion Criteria
2.1.1 Patients taking VKA Initial dosing of VKA Time to achieve therapeuticrange; rates of supratherapeutic orsubtherapeutic INR
RCT 25 patients
2.1.2 Elderly patientstaking VKA
Initial dosing of VKA Time to achieve therapeuticrange; rates of supratherapeutic orsubtherapeutic INR
RCT; prospective cohort;observational
25 patients
2.1.3 Patients taking VKA Frequency of INRmonitoring (higher vslower frequency)
TTR; rates of hemorrhage orthromboembolism
RCT; prospective cohort;observational
None
2.1.4 Patients taking VKA withnontherapeuticINR withoutbleeding
Dose management; useof vitamin K tocorrect INR
Time to return totherapeutic INR;hemorrhage orthromboembolism
RCT; prospective cohorts;observational
Reports before1995
2.1.4 Patients taking VKA with any INR and
active bleeding orneed for emergentreversal of INR
Dose management; useof vitamin K, FFP,
PCCs, rVIIa toreverse INR orbleeding
Time to return totherapeutic INR;
hemorrhage orthromboembolism
RCT; prospective cohorts;observational
None
2.1.5 Patients taking VKA with unstable or variable INR overtime
Dose management; useof vitamin K tostabilize INR
Stability of INR withintherapeutic range
RCT; prospective cohorts None
2.1.7 Patients withantiphospholipidsyndrome andtaking VKA
INR therapeutic range Hemorrhage orthromboembolism
RCT; prospective cohort;observational; registries
None
2.3.1 Patients taking VKA UC vs AMS care TTR; hemorrhage orthromboembolism
RCT; prospective cohort;observational
100 patients; useof PT ratherthan INR
2.3.3 Patients taking VKA Use of POC monitor athome to measureINR and/or to adjust VKA dose comparedto UC or AMS
TTR; hemorrhage orthromboembolism
RCT; prospective cohort;observational
50 patients
* FFP fresh frozen plasma; rVIIa recombinant factor VIIa; RCT randomized controlled trial.
www.chestjournal.org CHEST / 133 / 6 / JUNE, 2008 SUPPLEMENT 171S
2008 American College of Chest Physicians by guest on June 2, 2011chestjournal.chestpubs.orgDownloaded from
http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/ -
8/6/2019 Manejo de Antagonist As de Vitamina k
14/41
in the maintenance dose of warfarin. Sconce et al49similarly found that age, height, and CYP2C9 genotypesignificantly contributed to S-warfarin clearance in 297patients on stable anticoagulation. The mean daily warfarin dose was highest in those who were homozy-gous for the CYP2C9 wild type compared to theCYP2C9* 2 and CYP2C9* 3 alleles. The impact of thesemutations in CYP2C9 also affects acenocoumarol, al-though to a lesser degree because the anticoagulationpotencies of the R and S enantiomers are comparable.198
Genetic mutations in the gene coding for the VKORC1 often involve several mutations, leading to various haplotypes that cause greater resistance to warfarin therapy. Harrington et al50 found a warfarin-resistant individual who had high serum warfarin con-centrations and a 196G A transition, predicting a Val66Met substitution in VKORC1. In a study of 147patients, DAndrea et al46 found that patients with a1173CC genotype required a higher mean mainte-nance dose than those with a CT orTT genotype, asdidQuteineh et al,199 who found that a 1173 C Tpolymorphism was significantly associated with the riskof anticoagulation overdose. By identifying a number of noncoding SNPs, Rieder et al47 were able to infer thatfive major haplotypes are associated with different doserequirements for maintaining a therapeutic INR. Themaintenance doseranged from a low of 2.7 mg warfarinper day for the sensitive haplotypes up to 6.2 mg perday for the resistant haplotypes. Asian Americans hadthe higher proportion of sensitive haplotypes, whereasAfrican Americans more frequently exhibited the resis-tant haplotypes (Table 1). Sconce et al49 found that acombination of CYP2C9 and VKORC1 genotypes plusheight produced the best predictive model for estimat-ing warfarin dose, whereas Vecsler et al200 reportedthat CYP2C9 and VKORC1 genotypes together withage and body weight could explain as much as 63% of the dose variance, and Herman et al35 could explain60% of dose variability due to CYP2C9 and VKORC1polymorphisms, age, and body surface area.
These findings are significant not only becausethey may predict initial and maintenance warfarindosing requirements, but also because certain geno-types have been associated with adverse events.Thus, Higashi et al38 studied 185 patients, 58 with atleast one variant genotype of CYP2C9, and found inthose with variant genotypes an increased risk of having INRs above range (hazard ratio [HR], 1.40;95% CI, 1.03 to 1.90) and a significant risk of aserious or life-threatening bleeding event (HR, 2.39;95% CI 1.18 to 4.86). The latter hazard estimate wasbased on a few events in a very small number of patients with the variant genotypes. Joffe et al,196also studying CYP2C9 SNPs, found an upward trendin rates of an INR 6.0 or of bleeding in patients who were categorized as heterozygotes or compound
hetero/homozygotes compared to wild types, as did Veenstra et al.34 A similar increased risk of bleeding was seen in patients with these polymorphisms who were taking acenocoumarol but not phenprocoumon.41
The ability to determine mutations in the genescoding for these two proteins will likely influencefuture dosing patterns (eg, algorithms), but just howmuch value they will add to conscientious monitoringof the INR and dose management remains to bedetermined. 201 To date, only pilot trials of genetic-based dosing have been performed with mixed results.Hillman et al202 randomized 38 patients to standard vsgenetic-based dosing and showed a nonstatistical de-crease in adverse events (6 of 20 in the standard group vs 2 of 18 in the genetic-based dosing group). Allpatients were dosed based on an algorithm taking intoaccount mutations in CYP2C9. Voora et al203 dosed asingle cohort of 48 orthopedic patients according totheir CYP2C9 genotype in addition to age, weight,height, gender, race, and use of simvastatin or amioda-rone. Although patients with a CYP2C9 variantpromptly achieved a stable dose, they continued to beat higher risk of an INR 4.0 than patients with anormal genotype. The use of genetic testing beforeinitiating warfarin therapy is impractical in most centersbecause it is not available in a timely manner. Thefuture role of genetic testing in assisting dose predic-tion only can be determined by appropriately designedrandomized trials.
After 4 to 5 days of concomitant warfarin andheparin therapy, heparin is discontinued when the INRhas been in the therapeutic range on two measure-ments approximately 24 h apart. This delay in discon-tinuing heparin allows factors X and II to be reduced totheir plateau levels. If treatment initiation is not urgent(eg, in chronic stable atrial fibrillation), warfarin admin-istration, without concurrent heparin administration,can be commenced out of hospital with an anticipatedmaintenance dose of 4 to 5 mg/d. In patients with aknown protein C deficiency or another thrombophilicstate, it would be prudent to begin heparin therapy before or at the same time as starting warfarin therapy to protect against a possible early hypercoagulable statecaused by a warfarin-mediated reduction in the vitaminK-dependent coagulation inhibitors.204
Because dose requirements often change duringmaintenance therapy, physicians use various strategiesto ensure that dosing instructions are simple and clearfor the patient. Some providers prefer to use a fixedtablet strength of warfarin and to use alternate doseamounts (tablets or fraction of tablets) per day. Othersprefer a uniform daily amount that might require thepatient to have different tablet strengths. Both methodsachieve similar outcomes, although the former practicemay be more confusing for the patient.205,206
172S Antithrombotic and Thrombolytic Therapy 8th Ed: ACCP Guidelines
2008 American College of Chest Physicians by guest on June 2, 2011chestjournal.chestpubs.orgDownloaded from
http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/ -
8/6/2019 Manejo de Antagonist As de Vitamina k
15/41
Recommendation
2.1.1. In patients beginning VKA therapy, werecommend the initiation of oral anticoagulation, with doses between 5 and 10 mg for the first 1 or2 days for most individuals and subsequent dosingbased on the INR response (Grade 1B). At thepresent time, for patients beginning VKA therapy, without evidence from randomized trials, we sug-gest against the use of pharmacogenetic-basedinitial dosing to individualize warfarin dosing(Grade 2C).
2.2 Initiation of Anticoagulation in the Elderly
The dose required to maintain a therapeutic rangefor patients over 60 years of age decreases withincreasing age,195,207209 possibly because of a reduc-tion in the clearance of warfarin with age.210,211Gender also influences dose, with women requiring
less warfarin to maintain a therapeutic INR thanmen at an equivalent age.195 In a prospective cohortstudy of elderly patients who were given three initialdoses of 4 mg, Siguret et al212 were able to accurately predict the maintenance dose based on the INR onthe third day in 73% of patients, and within 1 mg of the maintenance dose in 95% of patients; no patienthad an INR 4.0. Therefore, in elderly patients, theinitial dose of warfarin should not be 5 mg,213 andin some cases ( ie, in patients with a high risk of bleeding; in those who are undernourished, havecongestive heart failure (CHF), or have liver disease;
or in those who have undergone heart valve replace-ment surgery), it should be less.195,213 Other factorsthat may influence the response to anticoagulation inelderly patients include the potential for a greaternumber of other medical conditions and/or concur-rent drug use.207 Consequently, it is advisable tomonitor older patients more frequently in order tomaximize their time in the therapeutic range(TTR).214
Recommendation
2.2.1. In elderly patients or in patients who aredebilitated, malnourished, have CHF, haveliver disease, have had recent major surgery, orare taking medications known to increase thesensitivity to warfarin ( eg, amiodarone), we rec-ommend the use of a starting dose of < 5 mg(Grade 1C) with subsequent dosing based on theINR response.
2.3 Frequency of Monitoring
In hospitalized patients, PT monitoring is usually performed daily, starting after the second or third dose
until the TTR has been achieved and maintained for atleast 2 consecutive days; then two or three times weekly for 1 to 2 weeks; then less often, depending on thestability of INR results. In outpatients starting warfarintherapy, initial monitoring may be reduced to every fewdays until a stable dose response has been achieved. When the INR response is stable, the frequency of testing can be reduced to intervals as long as every 4 weeks, although evidence215,216 suggests that testingmore frequently than every 4 weeks will lead to greaterTTR. If adjustments to the dose are required, then thecycle of more frequent monitoring should be repeateduntil a stable dose response can again be achieved.
The optimal frequency of long-term INR monitor-ing is influenced by patient compliance, transientfluctuations in the severity of comorbid conditions,the addition or discontinuation of other medications,changes in diet, the quality of dose-adjustment de-cisions, and whether the patient has demonstrated astable dose response. Some investigators217,218 haveattempted to develop predictive models with the goalof reducing the frequency of testing without sacrificingquality. Pengo et al218 randomized 124 patients withprosthetic mechanical heart valves who were on stabletherapy for at least 6 months to INR monitoring eitherat 6-week or at 4-week intervals. They found nodifference in time in, above, or below range betweenthe groups; however, the actual interval of monitoring was 24.9 days in the 6-week group and 22.5 days in the4-week group (p 0.0003). Other clinical trials215,216have suggested that during long-term treatment, theTTR and, presumably, fewer adverse events can bemaximized by more frequent testing. This finding isparticularly true in studies using patient self-testing(PST) in which access to testing is virtually unlimited.Horstkotte et al215 addressed this issue in 200 patients with mechanical cardiac valves and found that thepercentage of INRs within the target range increasedfrom 48% when monitoring was performed at anaverage interval of 24 days to 89% when monitoring was performed at an average of every 4 days by homePST using a point-of-care (POC) monitor. In a recentstudy of 4,000 patients with chronic atrial fibrillationand 250,000 INRs, Shalev et al219 found a greatertime in range as the testing interval decreased fromevery 5 weeks to every 3 weeks (41 to 48%,p 0.0005), and the investigators suggested that pa-tients should be monitored no longer than every 4 weeks. More frequent monitoring may be advisable forpatients who exhibit an unstable dose response.
Recommendations
2.3.1. In patients beginning VKA therapy, wesuggest that INR monitoring be started after
www.chestjournal.org CHEST / 133 / 6 / JUNE, 2008 SUPPLEMENT 173S
2008 American College of Chest Physicians by guest on June 2, 2011chestjournal.chestpubs.orgDownloaded from
http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/ -
8/6/2019 Manejo de Antagonist As de Vitamina k
16/41
the initial two or three doses of oral anticoagu-lation therapy (Grade 2C).2.3.2. For patients who are receiving a stabledose of oral anticoagulants, we suggest moni-toring at an interval of no longer than every 4 weeks (Grade 2C).
2.4 Management of Nontherapeutic INRs With or
Without BleedingFluctuations in INR may occur because of any one
or more of the following conditions: (1) inaccuracy inINR testing; (2) changes in vitamin K intake; (3) changesin vitamin K or warfarin absorption; (4) changes in warfarin metabolism; (5) changes in vitamin K-dependent coagulation factor synthesis or metabo-lism; (6) other effects of concomitant drug use; or (7)patient noncompliance. The management of patients whose INR is outside the therapeutic range is con-troversial because many of the various options havenot been compared.
When the INR is nontherapeutic, there are many options for dose adjustments. Patients whose INR is just outside the therapeutic range can be managedby either adjusting the dose up or down in incre-ments of 5 to 20% based on the cumulative weekly dose of warfarin or by more frequent monitoring, thelatter with the expectation that the INR will returnto therapeutic levels without a dosage change. Be-cause the absolute daily risk of bleeding is low even when the INR is excessively prolonged, many physi-cians manage patients with minimally elevated INRsby more frequent monitoring without a dosechange220 or for higher INR values between 4.0 and10.0, by stopping warfarin for 1 day or more, reduc-ing the weekly dose, and monitoring more frequent-ly.221,222 Hylek et al223 reported that when two dosesof warfarin were withheld in patients whose INR was
6.0, the INR returned more slowly if their main-tenance dose was lower, they were of older age, they had a higher initial INR, they had decompensatedCHF, or they had active cancer. Among 562 patients with an INR between 6.0 and 10.0, the subsequentINR measurement after withholding two doses of warfarin was 4.0 in 67% of patients and 2.0 in12% of patients. Garcia et al222 assessed the manage-ment of 979 patients who presented with an INRbetween 5.0 and 9.0. Vitamin K was used in only 8.7% of the episodes of elevated INR values, andmajor bleeding occurred in 1% of all patients in thefollowing 30 days. If the patient is at intrinsically highrisk of bleeding or if bleeding has already developed,patients also can be managed by omitting one ormore doses, by more frequent monitoring, and by actively intervening to lower the INR more rapidly.The interventions include administering vitamin Kand/or infusing fresh frozen plasma,224 prothrombin
concentrates,225 or recombinant factor VIIa.226230The choice of approach is based largely on thepotential risk of bleeding, the presence of activebleeding, and the level of the INR. Crowther et al231compared either stopping warfarin or administeringoral vitamin K in a randomized trial of patients withan INR of between 4.5 and 10. Those not treated with vitamin K experienced a higher rate of minorbleeding in the following 3 months compared tothose who were treated with vitamin K (4% vs 17%,respectively; p 0.05). Ageno et al232 randomized59 mechanical heart valve patients with an INRbetween 6.0 and 12.0 to either 1 mg of oral vitaminK or to no treatment. Although no major bleedingoccurred in either group in this small study, 1 mg of oral vitamin K more commonly returned a prolongedINR value to the therapeutic or near-therapeuticrange within 1 day than in the no-treatment group(mean INR in 24 h, 2.99 vs 5.23, respectively). Threepatients in the vitamin K group had an INR of 1.8compared to zero in the control group. Finally,Gunther et al233 managed 75 episodes of an INR
10, treating 51 episodes with low-dose vitamin K(2 mg) compared with 24 episodes with no treat-ment. There were no major bleeds in the treatedpatients vs three clinically important bleeds in thenontreated patients.
The response to vitamin K administered subcutane-ously is less predictable than to oral vitamin K and issometimes delayed.234236 Some studies236240 haveconfirmed earlier reports that oral administration ispredictably effective and has the advantages of safety and convenience over parenteral routes. If a decision ismade to use vitamin K, it should be administered in adose that will quickly lower the INR into a safe, but notsubtherapeutic range without causing resistance once warfarin is reinstated241 or without exposing the patientto the risk of anaphylaxis.242 High doses of vitamin K,though effective, may lower the INR more than isnecessary and may lead to warfarin resistance for 1 week or more. Low doses of vitamin K and slowinfusion rates are recommended, but there is no defin-itive evidence that anaphylaxis can be avoided by usinglow doses or slow infusion rates.243 A dose range of 1.0to 2.5 mg is effective when the INR is between 5.0 and9.0, but larger doses ( ie, 2.5 to 5 mg) are required tocorrect INRs of 9.0. Vitamin K also can be admin-istered by slow IV infusion when there is a greaterurgency to reverse anticoagulation234,244 or an impair-ment in vitamin K absorption. IV injection may beassociated with anaphylactic reactions,242,243 althoughsuch reactions have occurred with non-IV routes of administration.243
For life-threatening bleeding, immediate correc-tion of the INR is mandatory. Although fresh frozenplasma can be given in this situation, immediate and
174S Antithrombotic and Thrombolytic Therapy 8th Ed: ACCP Guidelines
2008 American College of Chest Physicians by guest on June 2, 2011chestjournal.chestpubs.orgDownloaded from
http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/ -
8/6/2019 Manejo de Antagonist As de Vitamina k
17/41
full correction can only be achieved by the use of factor concentrates225 because the amount of freshfrozen plasma required to fully correct the INR isconsiderable245 and may take hours to infuse. Yasakaet al246 found that a dose of 500 IU of PCC wasoptimal for rapid reversal for an INR of 5.0 butthat higher doses might be needed for more elevatedINRs. Although not currently approved for thisindication, recombinant factor VIIa has been shownto be effective in reversing therapeutic INRs tonormal at varying doses (10 g/kg to maximumcumulative dose of 400 g/kg) in healthy volun-teers230 and to reversing supratherapeutic INRsand/or bleeding in patients on warfarin,226 again at varying doses (15 to 90 g/kg). In a prospectiveobservational study of 16 patients with major bleed-ing on warfarin, Dager et al247 found that a dose of approximately 16 g/kg was adequate for rapidreversal of the INR and to achieve a desirablehemostatic effect in 14 patients. Recombinant factor VIIa has a short half-life, and vitamin K should beadministered simultaneously to stimulate factor pro-duction. Recombinant factor VIIa also has beenassociated with an increased risk of thromboembolicevents,248 as have some PCCs.249 Thus, one musttake this potential adverse effect into consideration when using such agents. Finally, the use of PCCs orrecombinant factor VIIa may vary depending on theavailability of such products in ones institution.Table 5 outlines the recommendations for managingpatients who are receiving coumarin anticoagulants who need their INR lowered because of actual orpotential bleeding.
For patients with subtherapeutic INRs duringlong-term therapy, no specific studies have examinedthe optimal method of correction. Because the aver-age daily risk of thrombosis for most indications isquite small, except in exceptional circumstances,most patients do not need to be covered with arapidly acting anticoagulant, such as heparin orlow-molecular-weight heparin. Rather, the weekly cumulative dose of warfarin is usually increased by 10 to 20%, and more frequent monitoring is insti-tuted until the INR is stable. In some cases, patientsmay be given a one-time larger dose followed by more frequent monitoring with or without a changein the cumulative weekly dose.
Recommendations
2.4.1. For patients with INRs above the therapeu-tic range but < 5.0 and with no significant bleed-ing, we recommend lowering the dose or omittinga dose, monitoring more frequently, and resum-ing therapy at an appropriately adjusted dose when the INR is at a therapeutic level. If onlyminimally above therapeutic range or associated with a transient causative factor, no dose reduc-tion may be required (all Grade 1C).2.4.2. For patients with INRs > 5.0 but < 9.0and no significant bleeding, we recommendomitting the next one or two doses, monitoringmore frequently, and resuming therapy at anappropriately adjusted dose when the INR is ata therapeutic level (Grade 1C). Alternatively, wesuggest omitting a dose and administering vita-
Table 5 Recommendations for Managing Elevated INRs or Bleeding in Patients Receiving VKAs (Section 2.4) *
Condition Intervention
INR more than therapeuticrange but 5.0; nosignificant bleeding
Lower dose or omit dose; monitor more frequently and resume at lower dose when INR therapeutic; if only minimally above therapeutic range, no dose reduction may be required(Grade 1C).
INR 5.0, but 9.0; nosignificant bleeding
Omit next one or two doses, monitor more frequently, and resume at an appropriately adjusted dose when INR in therapeutic range. Alternatively, omit dose and give vitamin K (12.5 mg po),particularly if at increased risk of bleeding(Grade 1C) . If more rapid reversal is required becausethe patient requires urgent surgery, vitamin K ( 5 mg po) can be given with the expectation that areduction of the INR will occur in 24 h. If the INR is still high, additional vitamin K (12 mg po)can be given (Grade 2C).
INR 9.0; no significantbleeding
Hold warfarin therapy and give higher dose of vitamin K (2.55 mg po) with the expectation that the INR will be reduced substantially in 2448 h(Grade 1B) . Monitor more frequently and use additional vitaminK if necessary. Resume therapy at an appropriately adjusted dose when INR is therapeutic.
Serious bleeding at any elevation of INR
Hold warfarin therapy and give vitamin K (10 mg by slow IV infusion), supplemented with FFP, PCC, orrVIIa, depending on the urgency of the situation; vitamin K can be repeated q12h(Grade 1C).
Life-threatening bleeding Hold warfarin therapy and give FFP, PCC, or rVIIa supplemented with vitamin K (10 mg by slow IVinfusion). Repeat, if necessary, depending on INR(Grade 1C).
Administration of vitamin K In patients with mild to moderately elevated INRs without major bleeding, give vitamin K orally rather thansubcutaneously (Grade 1A).
* See Table 4 for other abbreviations.If continuing warfarin therapy is indicated after high doses of vitamin K1 , then heparin or low-molecular-weight heparin can be given until theeffects of vitamin K1 have been reversed, and the patient becomes responsive to warfarin therapy. It should be noted that INR values 4.5 areless reliable than values in or near the therapeutic range. Thus, these guidelines represent an approximate guide for high INRs.
www.chestjournal.org CHEST / 133 / 6 / JUNE, 2008 SUPPLEMENT 175S
2008 American College of Chest Physicians by guest on June 2, 2011chestjournal.chestpubs.orgDownloaded from
http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/http://chestjournal.chestpubs.org/ -
8/6/2019 Manejo de Antagonist As de Vitamina k
18/41
min K (1 to 2.5 mg) orally, particularly if thepatient is at increased risk of bleeding (Grade2A). If more rapid reversal is required be-cause the patient requires urgent surgery, wesuggest vitamin K ( < 5 mg) orally with theexpectation that a reduction of the INR willoccur in 24 h. If the INR is still high, wesuggest additional vitamin K (1 to 2 mg) orally(Grade 2C).2.4.3. For patients with INRs > 9.0 and no signif-icant bleeding, we recommend holding warfarintherapy and administering a higher dose of vita-min K (2.5 to 5 mg) orally, with the expectationthat the INR will be reduced substantially in 24 to48 h (Grade 1B). Clinicians should monitor theINR more frequently, administer additional vita-min K if necessary, and resume therapy at anappropriately adjusted dose when the INRreaches the therapeutic range.2.4.4. In patients with serious bleeding and ele-vated INR, regardless of the magnitude of theelevation, we recommend holding warfarin ther-apy and giving vitamin K (10 mg) by slow IVinfusion supplemented with fresh frozen plasma,PCC, or recombinant factor VIIa, depending onthe urgency of the situation. We recommendrepeating vitamin K administration every 12 h forpersistent INR elevation (all Grade 1C).2.4.5. In patients with life-threatening bleeding(eg, intracranial hemorrhage) and elevated INR,regardless of the magnitude of the elevation, werecommend holding warfarin therapy and admin-istering fresh frozen plasma, PCC, or recombi-nant factor VIIa supplemented with vitamin K (10mg) by slow IV infusion, repeated, if necessary,depending on the INR (Grade 1C).2.4.6. In patients with mild to moderately ele-vated INRs without major bleeding, we recom-mend that when vitamin K is to be given, it beadministered orally rather than subcutaneously(Grade 1A).
2.5 Management of Variable INRs
Although it has long been known that changes indietary vitamin K intake may influence the stability of the INR in patients on warfarin, only recently havetrials been conducted to assess the impact that vitamin K can have on therapeutic stability. In 1993,Sorano et al250 showed that by stabilizing the intakeof dietary vitamin K, more stable anticoagulation canbe achieved. By comparing the daily vitamin Kintake in 26 unstable patients with 26 stable controlpatients, Sconce et al251 showed that the unstablepatients had poorer intake of vitamin K. Kurnik etal252 showed that in vitamin K-depleted patients,
very small amounts of vitamin K-containing vitamins will influence the INR to a greater extent than inthose with an adequate vitamin K status. In a study of 12 healthy volunteers on oral anticoagulation,Schurgers et al,253 found that a daily dose of vitaminK of at least 150 g was needed to alter the INRresponse. Reese et al254 used a retrospective analysisto assess the effect of a daily dose of 100 g of vitamin K1 in nine unstable patients. These patientsexperienced an increase in percent INRs (range, 32to 57%) in response to the daily vitamin K. In aprospective, open-label, crossover study, Ford etal255 found that five of nine patients improved theirstability with low-dose administration of vitamin K.As expected, the INR initially decreased in patientsgiven vitamin K, and an increased dose of warfarin was needed to reestablish an INR in the therapeuticrange, which took 2 to 35 days to achieve. Thus,patients must be monitored carefully if this interven-tion is tried. Finally, Sconce et al256 conducted thefirst rando