Managing Nutrition, Hydration & Electrolytes In the Older...
33
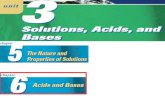
Managing Nutrition, Hydration & Electrolytes In the Older Adult Janet Reid Janet Reid Janet Reid Janet Reid- - -Hector, Ed.D, RD Hector, Ed.D, RD Hector, Ed.D, RD Hector, Ed.D, RD January 26 January 26 January 26 January 26 th th th th , 2012 , 2012 , 2012 , 2012 Nutrition and Hydration the Elderly Nutrition and Hydration the Elderly Nutrition and Hydration the Elderly Nutrition and Hydration the Elderly Organ System Change Potential Outcome Body composition ↑ Fat ↓ LBM ↓ Body water (20%) ↓ BMR ↑ Fat-soluble drug storage, w/ prolonged ½ - life ↑ Concentration of H2O -soluble drugs Gastrointestinal ↓ Gastric acid secretion ↓ Gastric motility ↓ Lactase activity ↓ Absorption of folate, protein-bound vitamin B12 ↓ Bioavailability of minerals, vitamins, protein Avoidance of milk products, with ↓ intake of Vit D & calcium Hepatic ↓ Size & blood flow ↓ Activity drug-metabolizing enzymes ↓ Albumin synthesis rate Poor or delayed metabolism of certain drugs Immune ↓ T-cell function Anergy ↓ Resistance to infection Neurologic Brain atrophy ↓ Cognitive function Renal ↓ Glomerular filtration rate ↓ Renal activation of 1,25,(OH)2 D3 Reduced renal excretion of metabolites; drugs ↓ Vit D, Calcium Sensory-perceptual ↓ Taste buds, papilla on tongue ↓ Olfactory nerve endings Altered taste threshold, ↓ ability to detect sweet/salt, ↑ use of salt/sugar Altered smell threshold, ↓ palatability causing poor food intake Skeletal ↓ Bone density ↓ Fractures SOURCE: Nutrition Screening Initiative. 2626 Pennsylvania Ave. NW, Suite 301, Washington, DC 20037. (2003)
Transcript of Managing Nutrition, Hydration & Electrolytes In the Older...

Managing Nutrition, Hydration & Electrolytes In the Older Adult
Janet ReidJanet ReidJanet ReidJanet Reid----Hector, Ed.D, RDHector, Ed.D, RDHector, Ed.D, RDHector, Ed.D, RDJanuary 26January 26January 26January 26thththth, 2012, 2012, 2012, 2012
Nutrition and Hydration the ElderlyNutrition and Hydration the ElderlyNutrition and Hydration the ElderlyNutrition and Hydration the Elderly
Organ System Change Potential Outcome
Body composition ↑ Fat
↓ LBM
↓ Body water (20%)
↓ BMR
↑ Fat-soluble drug storage, w/ prolonged ½ - life
↑ Concentration of H2O -soluble drugs
Gastrointestinal ↓ Gastric acid secretion
↓ Gastric motility
↓ Lactase activity
↓ Absorption of folate, protein-bound vitamin B12
↓ Bioavailability of minerals, vitamins, protein
Avoidance of milk products, with ↓ intake of
Vit D & calcium
Hepatic ↓ Size & blood flow
↓ Activity drug-metabolizing enzymes
↓ Albumin synthesis rate
Poor or delayed metabolism of certain drugs
Immune ↓ T-cell function Anergy
↓ Resistance to infection
Neurologic Brain atrophy ↓ Cognitive function
Renal ↓ Glomerular filtration rate
↓ Renal activation of 1,25,(OH)2 D3
Reduced renal excretion of metabolites; drugs
↓ Vit D, Calcium
Sensory-perceptual ↓ Taste buds, papilla on tongue
↓ Olfactory nerve endings
Altered taste threshold, ↓ ability to detect
sweet/salt, ↑ use of salt/sugar
Altered smell threshold, ↓ palatability
causing poor food intake
Skeletal ↓ Bone density ↓ Fractures
SOURCE: Nutrition Screening Initiative. 2626 Pennsylvania Ave. NW, Suite 301, Washington, DC 20037. (2003)

Overview of Composition & Volume of
Body Fluid Components
� TBW = 60% Body Wt.
� ⅔ is ICF space, ⅓ ECF space� ECF: Interstitial, Plasma, Na+, CL-, HCOӡ-
• Na+ Correlates with ECF osmolality
• ICF: K+, Mg, PO₄-, Proteins –Osmolality correlates with conc. of K+ & Mg+
• ICF & ECF have similar osmolality ~ 285 mOsm/kg
• 360 ml fluid lost / c°°°° / fever / day
• Respiratory fluid loss ↓ with humidified air given by mask or ET tube
• Janet Reid-Hector, Ed.D, RD, CNSD
Fluid & Electrolytes Changes In the Older Adult
• Creat. clearance ↓ with age by 1 ml/min/yr after 40 years of age.
• S. Creatinine remains constant due to ↓muscle mass.
• ↓ of water intake occur in the elderly 2° ↓ sensation of thirst;
associated with a tendency to lose water with urine.
• Capacity to respond to sodium( NA) load is impaired in aged
kidneys, →ECV expansion & HTN.
• The elderly have a ↓ capacity for retaining NA making old
subjects sensitive to salt depletion & ECV contraction. • Hypernatremia (NA > 150 mmol/l) is not infrequent in the elderly
& is usually due to water deficiency and rarely to iatrogenic excess of sodium.
•
• Janet Reid-Hector, Ed.D, RD, CNSD
Fluid & Electrolytes Changes In the Older Adult
• An abrupt occurrence of severe hypernatremia ↠
neurological symptoms due to dehydration & brain
shrinking, which may lead to cerebral hemorrhage & death.
• Hyponatremia (NA < 130 mmol/l) is frequent among the
elderly ; mainly due to iatrogenic water overload.
• Hypovolemic hyponatremia occurs when salt depletion ↠
ECV contraction > 10%, & is due to water retention in an
attempt to normalize ECV.
• Hypervolemic hyponatremia is due to ADH hyper secretion
because of a ↓ in 'effective' circulating blood volume.
• 'Pseudo hyponatremia' may occur because of
hyperlipidemia or hyperproteinemia. • Janet Reid-Hector, Ed.D, RD, CNSD
Fluid & Electrolytes Changes In the Older Adult
• An abrupt occurrence of severe hyponatremia that → neurological
symptoms (water intoxication), 2° the edematous swelling of the
brain within the skull.
• Rapidly occurring hyponatremia may be lethal, slowly occurring
hyponatremia is usually asymptomatic.
• Rapid correction of hyponatremia may cause cerebral dehydration
& 'osmotic demyelination syndrome' ('central pontine
myelinosis').
• ↓ (e.g. by diuretics) or⇡⇡⇡⇡ (e.g. by ACE-inhibitors, NSAID, ℬ-
blockers) of serum potassium may occur in the elderly.
• Diuretics should be used with caution in elderly subjects to avoid
salt depletion, hypotension & renal function impairment• Janet Reid-Hector, Ed.D, RD, CNSD

Gender differences in Fluid Metabolism• Semin Nephrol. 1996 Jul;16(4):277-88. Abnormalities of water metabolism in the elderly. Ayus JC, Arieff AI.
• Hypernatremia (high sodium in the blood that occurs with excessive fluid loss) is a frequent problem at the extremes of age, but particularly so in elderly individuals.
• When comparing healthy elderly men to younger controls, there are differences in the response to water deprivation. In older men, there are deficits in both the intensity & threshold of the thirst response.
• The ability to concentrate the urine also declines with age. There is both a decline in GFR & an ֈ incidence of renal disease with advancing age, to impaired ability to conserve water.
• A ⇓ in % TBW of equal volumes of fluid loss in young & old individuals ⇝⇝⇝⇝ more severe dehydration in the elderly.
MDS triggers that indicate hydration may be at risk?
↠ •UTI in the past 30 days
↠ • Dehydration diagnosis
↠ •Weight +/- 3 lbs. in the last 7 days
↠ • Fluid output exceeds intake
↠ •Fever
↠ • Internal bleeding
↠ •Tube feeding in place
↠ • Certain medications
↠ •Over the last 3 days beverages offered are not consumed• Janet Reid-Hector, Ed.D, RD, CNSD
Electrolyte Balance
• Hyponatremia
• The most common electrolyte imbalance.
• Associated with kidney disease : nephrotic
syndrome & ARF
• Very young & old people affected more often
than young adults.
• Janet Reid-Hector, Ed.D, RD, CNSD
Electrolyte Balance
• Causes of HyponatremiaH20
retention &
renal failure
Pseudo
hyponatremia
Psychogenic
polydipsia
Hypovolemic
hyponatremia
Hypervolemic
hyponatremia
Euvolemic
hyponatremia
⇥ in a low
NA level in
the blood
too much water
is drawn into
the blood;
commonly seen
in
hypoglycemia
compulsively
drink > 4
gallons of
water/ day.
low blood
volume due
to fluid loss
► in
dehydrated
people who
rehydrate too
quickly,
thiazide
diuretics,&
S/P severe
vomiting or
diarrhea
high blood
volume due
to fluid
retention ►
in cirrhosis,
heart disease,
nephrotic
syndrome,
edema
⇓in TBW in hypothyroidism,
adrenal gland
disorder, &
disorders
that⇑ release
of ADH, such
as TB,
pneumonia, &
brain trauma.
• Janet Reid-Hector, Ed.D, RD, CNSD

Signs & Symptoms
HyponatremiaTreatmentGoal of treatment
Methods include:
Symptoms of hyponatremia
are related to the severity &
rate at which the conditions
develop.
The first symptoms: fatigue,
weakness, nausea, &
headache.
More severe cases: confusion,
seizure, coma, and death.
Restore electrolyte balance for
proper hydration & use of
total body fluid.
NA deficiency must be
corrected slowly because
drastic change in NA level ⇛
brain cell shrinkage and
central pontine myelinolysis
(damage to the pons region of
the brain).
Fluid & water restriction
IV saline solution of 3% NA
Salt tablets
Signs , Symptoms & Treatment of Hyponatremia
• Janet Reid-Hector, Ed.D, RD, CNSD
Hypernatremia
• Hypernatremia commonly affects older hospitalized people, 50% of whom have underlying diseases that, when combined with excessive NA & fluid loss, are fatal.
• Hypernatremia : occurs with excessive fluid loss; not replaced, sodium is not adequately excreted from the body.
• Causes:
• * Diabetes insipidus (caused by deficiency of or insensitivity to ADH)* Diarrhea; * Diuretic medication* Excessive salt intake* Excessive vomiting* Heavy respiration (e.g., exercise, exertion)* Severe burn* Sweating It is associated with the same symptoms as hyponatremia, and also causes the following:* Delerium* Irritability* Muscle twitching
• Janet Reid-Hector, Ed.D, RD, CNSD
Treating Hypernatremia
• Slowly replenish H2O loss, usually over 48
hours, through drinking or IV solution.
• In cases of DM, the imbalance is treated with
adequate water intake and NSAIDS or with
synthesized hormones (e.g., desmopressin)
that aid in fluid retention & decrease
urination.
• Janet Reid-Hector, Ed.D, RD, CNSD
Hypokalemia• An abnormally low level of K+ ; The adrenal gland makes
aldosterone; that signals the kidneys to excrete or conserve potassium, based on the body's needs.
• In hypokalemia, the adrenal gland retains the hormone & the kidneys conserve potassium when more is needed.
• Causes• The most common cause of K+ depletion is diuretics that ⇈ urination. Other causes include:
• * Diarrhea* Dietary deficiency* Excessive sweating* Magnesium deficiency (causes over excretion of fluid)
• Janet Reid-Hector, Ed.D, RD, CNSD

Signs, Symptoms & Treatment of Hypokalemia
• Symptoms of deficiency: cardiac arrhythmia, muscle pain, general discomfort or irritability, weakness, & paralysis.
• Diagnosis
• May require urinalysis & blood tests to determine the amount of K+ being excreted by the kidneys.
• Treatment
• K+ supplements, diet, IV solution.
• ***Patients on diuretics are given K+ supplements.
• Potassium is given slowly to avoid hyperkalemia.
• Janet Reid-Hector, Ed.D, RD, CNSD
Hyperkalemia
• An abnormally high level of potassium.
• K+ is released into the blood when cells are damaged.
• Causes include:
• * Burn* Chemotherapy* Hemolysis (RBC destruction caused by infection or burn)* Rhabdomyolysis (destruction of skeletal muscle; associated with acute tubule necrosis, or ATN)* Strenuous exercise (rarely)
• Urinary excretion of potassium can be impaired by the following:
• * Acute & Chronic Renal failure * * Impaired aldosterone release or production* Medications that ⇓ K+ excretion:o Amiloride (diuretic)o Bactrimo Cyclosporine (immunosuppressive)
• Janet Reid-Hector, Ed.D, RD, CNSD
Signs, Symptoms & treatment of Hyperkalemia
• Hyperkalemia affects the heart & ↠↠↠↠ EKG changes, ventricular fibrillation, & cardiac arrest.
• Other symptoms include:
• Tingling in the extremities, weakness, & numbness.
• Treatment
• IV Diuretics &calcium to promote K+ excretion.
• Insulin is given with glucose to help cell absorption of K+
• Albuterol may be added to ⇡⇡⇡⇡ absorption.
• Drugs that bind to K+ such as Kayexalate, force K+ into the intestine to be excreted.
Hydration ManagementPromotion of adequate fluid balance that prevents
complications resulting from abnormal fluid levels.
Maintaining adequate fluid balance is an essential component of
health across the life span; older adults are more vulnerable to
shifts in H20 balance, over-hydration & dehydration, 2° age-
related changes & ⇡⇡⇡⇡ medical conditions. Dehydration is the
most frequently occurring problem.
Seniors are at ⇡⇡⇡⇡ risk dehydration; they are not as sensitive as
younger adults to the sensation of thirst.
Age-related changes in the body’s ability to balance H2O & NA
sodium ⇡⇡⇡⇡ increase the danger.
Older persons with diarrhea / vomiting consume at least 1.7 L
fluid/q 24 hr. = about (7) 8 Oz. glasses of water. ****Liquid meal replacements are also recommended.

� Essential to all functions
� Affects cellular metabolism & integrity
� Catalyst in biological Rxs.
� Regulation of body temperature
� Transport of nutrients & electrolytes
� Dilution & transport of medication
� Maintain normal body waste removal
• Janet Reid-Hector, Ed.D, RD, CNSD
Disturbances of Volume & Concentration of Body Fluids.
• The general clinical terms for volume abnormalities are dehydration & overhydration. Both conditions are associated with a Δ in ECF volume.
� ADH secretion regulated by osmotic, volume, hormonal & neural stimuli
� Osmolarity & Osmolality are a measure of the # H2O attracting particles� Osmolarity: # osmoles of particles (solute) / kg of solvent (mosmol/kg/ H2O))))� Osmolarity: # osmoles of particles / vol. Of solvent (mosmol/L)
� Thirst = 1-2 % deficit in BW� Soduim (Na): Primary ECF cation
� Integrity of ECF determined by Na & its accompanying onions.
• Janet Reid-Hector, Ed.D, RD, CNSD
»FLUID BALANCE
� Obligatory: minimum required for survival
� Facultative: 500 – 1000ml – margin of safety for
� Conservatory/Excretory mechanisms of the body which use H2O.
� A wt Δ of 1 kg. unattributable to anything else = fluid loss / gain of 1L
Obligatory Input Obligatory Output
Fluids 750ml Urine 750
Metabolism 350ml Sweat 500
Facultative 1000ml
Lungs 400
Total 2800ml Feces 150
Facultative 1000
Total 2800

� **********General recommendations:
30 ml/kg / BW / day or 1 ml/kcal ingested.• Fluid intake must replace measurable losses (urine, feces,
drain tubes & insensible losses from respiration & skin.
• Recommended minimum total fluid intake is 1500-
• 2000ml, (equivalent to 6-8 250ml cups) /day from all sources including soups and beverages.
• Formula: to calculate fluid requirements for older people
• 100 ml fluid/ kg BW for the first 10 kg
• 50 ml fluid/ kg for the next 10 kg
• 15 ml fluid/ kg for each kg after 20 kg.
Dehydration – common anomaly
Dehydration is a frequent etiology of morbidity and mortality in elderly people.
It causes hospitalization of many patients & its outcome may be fatal.
Often linked to infection, & if overlooked, mortality may be over 50%.
� 1. ↓ thirst response
� 2. Kidney’s ⇩ concentrating capacity
� 3. Diuretic medications
� 4. Dementia• Janet Reid-Hector, Ed.D, RD, CNSD
Risk Factors Associated with Dehydration
Risk Factors Etiology in the
Elderly
Clinical Signs of
Dehydration?
Consequences of
dehydration
Acute or chronic
illness
Lack of sense for thirst Dizziness upon
sitting/standing Confusion—
Δ in mental status
⇓ functional ability
Medication use—
especially
laxatives, diuretics,
enemas
Aged kidney—⇓ ability
to concentrate urine
⇓ urine output
• Poor skin turgor;
dry mucous membranes
Constipation • Fever
Predisposition to falls
& Infection
Restriction of fluid ⇓muscle mass,
therefore, ⇓ total body
water
⇓ auxiliary sweating
Dry oral mucosa
Recent Δ in consciousness
Fecal impaction
•Fear of
incontinence
⇑ need for feeding
assistance
Dry oral mucosa Fluid and electrolyte
imbalance
•Dysphagia Darker urine • Death
• Janet Reid-Hector, Ed.D, RD, CNSD
Diagnosing Dehydration
• The most accurate test is serum osmolarity –
• A value above 295 mOsmol is diagnostic of ⇓ body water in all but
very exceptional circumstances.
• Other tests include: an ⇡⇡⇡⇡ BUN: Creatinine, ⇡⇡⇡⇡ S. Na
• ***These tests are more liable to be abnormal for reasons other
than dehydration.
• All 3 values are stable in non-ill residents of nursing homes, so a Δ
from baseline is reliable to suggest dehydration has occurred.
• Urine specific gravity: H2O balance & urine concentration
• Janet Reid-Hector, Ed.D, RD, CNSD

� Mucosal xerosis
� Swollen tongue
� Sunken eyeballs
� ↑ body temperature
� ↓ urine output
� Constipation
� Nausea
� Vomiting
� ↓ blood pressure
� Mental confusion
� Acute renal failure
� Altered drug effects
� Electrolyte disturbance
• Janet Reid-Hector, Ed.D, RD, CNSD
Biochemical Signs of Dehydration*
Signs Value
Raised serum osmolarity
Raised serum sodium
Raised BUN/creatinine ratio
Urine specific gravity
*****Conditions under which the test may be performed:
Complicated UTI (pyelonephritis)
High blood sodium level (hypernatremia)
Low blood sodium level (hyponatremia)
Excessive urination
Above 295 mOsmol
Above 145 mmol/L
Above 50 (urea in mmol/L
1.002 to 1.030.
• Janet Reid-Hector, Ed.D, RD, CNSD
Dehydration
• 3 types of dehydration:– Isotonic; Hypotonic ; Hypertonic
• Proportional balance of Na & H2O losses
• Dehydration can be measured as % of BW loss.
• Effects– Increases resting rate
– Susceptibility to development of UTI
– Pneumonia
– Pressure ulcers
– Confusion, disorientation, dementia
•• Janet Reid-Hector, Ed.D, RD, CNSD
� Hypertonic Dehydration
� Body H20 losses > NA Losses
� Reduced Oral Intake
� Excessive loss from sweating or prolonged fever
� NA concentration ↑ in the ECF
� ↑ Bun/ Creatinine in absence of renal failure
• Janet Reid-Hector, Ed.D, RD, CNSD

� Body Na+ loss exceeds H2O loss
� Na+ depletion or hyponatremia
� Diuretics, diarrhea / vomiting
� Renal wasting syndrome
� Lab Tests: � abnormally low serum Nat Levels
� Reduced ECF
� Tx: H2O/ Electrolytes solutions to rehydrate
• Janet Reid-Hector, Ed.D, RD, CNSD
• Body loses equal amounts of Nat & H2O
• Extreme diarrhea/vomiting
• Food borne Illnesses/severe bleeding
• S. NA, Osmolality & specific gravity are WNL
• Patients do not sense thirst/need for fluid
• Both fluid & NA are required to rehydrate
• Janet Reid-Hector, Ed.D, RD, CNSD
Lab Test Hypertonic Isotonic Hypotonic
Osmolality, serum >Normal WNL <Normal
Sodium, serum >Normal WNL <Normal
Hemoglobin >Normal >Normal >Normal
Hematocrit >Normal >Normal >Normal
Albumin, serum >Normal >Normal >Normal
BUN >Normal >Normal >Normal
Urine specific Gravity
>Normal >Normal <Normal
Laboratory Screening For Dehydration
• Janet Reid-Hector, Ed.D, RD, CNSD
OverHydration• ↑ in ECF volume
• Fluid shifts from ECF→ IFC → edema
• ↑ capillary hydrostatic pressure (CHF)
• ↓ colloid osmotic pressure (hypoalbuminemia)
• ↑ capillary permeability (inflammation)
• Lymphatic obstruction (following surgery)
• Liver / Kidney failure
• Physical inactivity
• CHF, Low BP
• Tx. Edema – Loop Diuretics
• Janet Reid-Hector, Ed.D, RD, CNSD

Laboratory Screening For Overhydration by TypeLab Test Hypotonic Isotonic Hypertonic
Osmolality, serum <normal WNL >normal
Sodium, serum <normal WNL >normal
Albumin <normal WNL or slightly low
<normal
H/H <normal WNL or slightly low
<normal
Blood Urea Nitrogen
<normal WNL or slightly low
<normal
Dehydration
Fluid Balance/ Homeostasis
� ICF Deficit ECF Loss Excess
� Tx: Hyponatremia� H2O restriction (w) 150gm CHO orally or 25%
dextrose slowly.
� True Na+ Deficit
� 100-150mg NaCL as 3% or 5% NaCL slowly IV
followed by strict fluid restriction.
� Hyponatremia
� Isotonic dilute saline solution IV.
■ ICF loss & dehydration due to H20 loss.
■ with higher osmotically active fluids.
Eg. Non- Ketotic hyperosmolar
syndrome.
■ Tx: Hypotonic Fluid
If BP is ↓ due to ECF deficit,
Tx with isotonic fluid.
ICF Excess■ H2O intoxication
Inappropriate ADH secretion.
■ Hyponatremia – (< 135 ) dilutional
or artifactual.
■ Hyperglycemia
■ Hyperlipemia
■ G.J. hemorrhage
Addisonian crisis
■ Renal DS. (w) Na+
wasting
■ NG Suction
■ Vomiting, diarrhea
■ Diuretic Tx.
■ Edema
■ Heart Failure
■ Ascites
■ Excessive infusion of
hypotonic fluid.
• Janet Reid-Hector, Ed.D, RD, CNSD
Calculating Water Deficit (Liters0.6 x BW (1- 140)
[Na]
S.Na+↑3mEq/L for each liter of H2O deficit
Bun ↑3mg/100ml
Reverse for Over hydration
Calculating Fluid Deficit
70 kg male, S. Na+ = 170 mEq/L
H2O Deficit: = 0.6 (70) (1-140 / Na)
= 42 – 34.6 = 7.4 L Deficit
• Calculating Excess H20 to be Excreted to
Correct HyponatremiaSerum Osmolality
Glucose (mg/dl) Bun (mg/dl)
mosm/kg/ H2O = 2 x Na + 18 + 2.8
Normal = 285 – 290 mOsmol/kg/h₂₂₂₂0
Chloride Deficit
mEq Cl = 0.2 x BW (kg) x (103 – S.CL-)
Bicarbonate Deficit (HCOӡӡӡӡ))))mEq HCO3 = (24 - PHCOӡӡӡӡ) ) ) ) x 0.4 x BW (kg)
PHCOPHCOPHCOPHCOӡӡӡӡ = Arterial Blood Gas
E.g. 70kg male, 60% BW, Serum Na+ Conc.
= 120 mEq/L
70 x 0.6 = 42 L TBW
120 mEq/L (PT) x 42L =36L
140 mEq/L (normal)
42 – 36 = 6L excess fluid

• Hyperglycemia → ↑ ECF Osmolality
• H2O moves from ICF → ECF → Nutriuresis
• Theory = ↓ for q 100mg/dl ↑ in Gluc → 2.8 meq/L↓ in Serum Na+ conc.
• Actual = 1.6 meg / ↓ in S. Nat Conc.
E.g. Patient with Serum Glu = 800mg/dl
Serum Na+ expected to ↓ 129 meq/L
(140 - 1.6 x 7)
Any Variation Suggests:
• Superimposed dehydration or salt loss.
• Mannitol infusions.
• Janet Reid-Hector, Ed.D, RD, CNSD
Fluid Balance / Homeostasis
• No edema Present
• No Jugular Vein
distension
• Adequate urine output
• Normal S. electrolytes &
arterial pH.
• Janet Reid-Hector, Ed.D, RD, CNSD
Nutritional Interventions for Dehydration
• Rehydrate slowly
– Guidelines
• Provide 1/4 to 1/3 overall fluid deficit
• Use water of 5% glucose solution
• Thickened liquids count as fluid
• Offering fluids hourly and with medication – achieve higher levels of hydration
• Janet Reid-Hector, Ed.D, RD, CNSD
Strategies to maintain / increase fluid intake
� Ensure all staff are adequately trained in the importance of hydration.
� Regularly offer fluids – e.g. every 1 ½ hours by day
� Offer fluids at specific routine events
� before / after showering or washing
� after toileting
� before / after physiotherapy or other activity program
� medication rounds
� Regular hydration cart rounds
� Offer residents their preferred drinks
� Prompt residents to drink at meal times
� Ensure fluid is within residents’ reachEducate families / visitors to offer fluids when visiting
� Encourage “wet” foods such as jelly, custard, yogurt, ice cream, soup, pureed fruit
� Have a social hour where fluids are offered
� Keep a fluid intake chart especially for at risk residents
� Use a symbol such as a drop of water on trays of residents who need to drink more, to prompt staff.
� Measure urine specific gravity monthly
� Measure osmolarity, NA /BUN /creatinineratio
.
� Identify at risk residents and pay more attention to them – e.g. confused, refusing fluids, febrile, on diuretics
• Janet Reid-Hector, Ed.D, RD, CNSD

Alternative to IV Hydration in the elderly
• Hyaluronidase, an enzyme obtained from bull testes, has been used to enhance fluid absorption from subcutaneous tissue.
• Temporarily lyses normal interstitial barrier, which consists mainly of hyaluronic acid, a polysaccharide found in the intercellular ground substance of connective tissue.
• Hyaluronidase⇩ the viscosity of the connective tissue, thus ⇑diffusion of the fluid administered subcutaneously for about 24 to 48 hours
• One method : add 150 U/ L to a fluid infusion bag & inject 75 U of into each clysis site through the tubing near the needle.
• Some physicians have used 10X this dose for hypodermoclysis by priming the needle and infusion set with Hyaluronidase(1,500 U) & 1 - 2 mL of lidocaine.
• This dosage can cause discomfort / local reaction.
• Janet Reid-Hector, Ed.D, RD, CNSD
Alternative to IV Hydration in
the elderly
• Hypodermoclysis has been an alternative option to the traditional IV route for ≫ 50 years.
• This method involves the insertion of a 21 or 23 gauge butterfly cannula under aseptic conditions into subcutaneous tissue
• As subcutaneous tissue tends to diminish peripherally and increase in central areas as part of the ageing process, the abdomen, scapula or thighs are all prime sites for administration of subcutaneous fluids.
• Once the cannula is inserted, it is attached to a giving set and connected to a bag of parenteral fluids, commonly infused at a rate of 2L over a 24 h period.
.
• As the use of electrolyte-free and hypotonic solutions has been associated with cardiovascular collapse and shock, it is now standard practice to use either 5% dextrose or 0.9% saline solutions.
• Up to 34 mmol of potassium can be given safely with each litre of fluid
• Up to 2 litres of dextrose-saline solution can be safely administered every 24 hours using this route; but physician supervision and close patient monitoring is essential
• Janet Reid-Hector, Ed.D, RD, CNSD
Maintaining Hydration in Gastroenteritis
► Dehydration can occur very rapidly – within hours with vomiting and diarrhea ֈ fluid los.
► Electrolytes are also being lost
►Prevention of dehydration should be combined with electrolyte replacement.
� The use of glucose & salt in rehydrating solutions ensures the most rapid absorption of H2O & electrolytes from the bowel.
� Fluids too high in sugars will not be absorbed as rapidly & replacement fluids with no sugar or electrolytes can actually ֈ gut loss of fluid.
� It is essential that rehydration fluids are used early – from the beginning of an episode of gastroenteritis – & frequently.
� Examples of rehydrating fluids, include:: Hydralyte & Gastrolyte ⇩ the high risk of dehydration.
� It is recommended that Hydralyte, be administered as 200ml q 30 mins .
� When oral intake remains insufficient, Hypodermoclysis can avoid transfer to hospital for dehydration.
• Janet Reid-Hector, Ed.D, RD, CNSD
NYHA Classification - The Stages of Heart Failure
• In order to determine the best course of therapy, physicians often assess the stage of heart failure
according to the New York Heart Association (NYHA) functional classification system. This system
relates symptoms to everyday activities and the patient's quality of life.
Class Class I (Mild) Class II (Mild) Class III
(Moderate)
Class IV (Severe)
Patient
Symptoms
No limitation of
physical activity.
Ordinary physical
activity does not
cause undue
fatigue,
palpitation, or
dyspnea
(shortness of
breath).
Slight limitation
of physical
activity.
Comfortable at
rest, but ordinary
physical activity
results in fatigue,
palpitation, or
dyspnea.
Marked
limitation of
physical activity.
Comfortable at
rest, but less
than ordinary
activity causes
fatigue,
palpitation, or
dyspnea.
Unable to carry
out any physical
activity without
discomfort.
Symptoms of
cardiac
insufficiency at
rest. If any
physical activity
is undertaken,
discomfort is
increased.
• Janet Reid-Hector, Ed.D, RD, CNSD

Fluid Management in Heart FailureHeart failure Consequences
Heart failure develops gradually over several
years, or move quickly S/P an MI or a disease of
the Cardiac muscle.
Rate of death is ~ 10% after 1 year. ½ die w/n 5
yr. S/P diagnosis. Advances in research are
providing more options and improving.
The pumping action of the becomes less
powerful.. blood does not move efficiently
through the circulatory system & back up, ↑
pressure in blood vessels & forcing fluid into
body tissues.
When the (ℒ )side of the starts to fail, fluid
collects in the lungs ⇝Pulmonary edema. This
extra fluid congests the lungs ,makes it more
difficult for airways to expand as you inhale.
Breathing becomes more difficult, , SOB occurs
particularly with activity or lying down.
ℛ) side of the heart starts to fail, fluid collects in
the feet and lower legs. As the upper legs swell
and abdomen collects fluid (ascites). Weight gain
is an excellent measure of how much fluid is
being retained.
Edema is a sign of (ℛ) heart failure, especially
with pitting edema. Non pitting edema is Ȉcaused by heart failure.
• Janet Reid-Hector, Ed.D, RD, CNSD
Fluid & Electrolyte Concepts in Heart Failure-
Raging HormonesHormones Effect Consequences
Angiotensin II
markedly ⇈
Cause renal & peripheral vasoconstriction.
GFR may initially maintained , but eventually
both RBF & GFR are inadequate
Limits the amount of Na reaching
the proximal tubules; ⇛ more Na
reabsorbed.
Angiotensin stimulates the secretion of Aldosterone from the
adrenal cortex which acts on the distal tubules
Enhances both Na & Cl-
reabsorption, & K+ and H- excretion.
ADH ⇈Enhances vasoconstriction; allows H2O & urea to be
reabsorbed into the medullary interstitium which ⇛
urine to concentrate.
Potentiates abnormal sodium and
water retention.
Edema results from dilutional
hyponatremia & H2O retention
Oliguria is a late sign of CHF resulting
from ⇩ RBF & CO output.
Nocturia may also occur.
• Janet Reid-Hector, Ed.D, RD, CNSD
Congestive Heart Failure Treatment
• The treatment of heart failure depends on the exact cause, but it can usually be treated effectively.
• The overall goals of treatment:
1. Correct underlying caus,
2. Relieve symptoms
3. Prevent worsening of the condition.
4. Symptoms are relieved by removing excess fluid from the body
5. Improving blood flow,
6. Improving heart muscle function,
7. Increasing delivery of O2 to the body tissues.
• Janet Reid-Hector, Ed.D, RD, CNSD
Recommendations for Heart failure TX.Labs , Vitals, MNT Rationale
Daily weight checks: mandatory
in persons with heart failure
B-type natriuretic peptide(BNP)
The amount of fluid retention is usually reflected by the
amount of ⇑ SOB & weight gain.
Hormone produced at ⇈ by the failing heart muscle. Levels ⇑severity of heart failure worsens.
Fluid Intake 1.4 - 1.9 L (48-64 oz.)/ day, depending on clinical symptoms
(i.e. edema, fatigue, SOB. Fluid ℟ improve clinical symptoms
& quality of life.
Sodium Intake <<<< 2000 mg (2 g) /day. Na+℟ will improve clinical
symptoms (i.e. edema, fatigue) & quality of life.

Risks/Harms of Implementing ♥ Failure
Recommendations
• Potential risk of a fluid & Na+ ℟ diet is ⇑ BUN/ Creat.
• Patients may be Hypovolemic & alterations in diuretics, fluid & Na+ intake should be considered.
• ***Consider a lower range of fluid ℟ in NYHA stage IV patients
• 2-g Na+ diet is unpalatable for some patients, a 3-g Na+ may be a more realistic target for patients with mild – mod. ♥ failure.
• For some patients, fluid ℟ are difficult to follow because of excessive thirst related to ⇓ CO.
• Avoid other dietary ℟s unless clearly indicated (e.g., a LF, low-Chol diet for hypercholesterolemia in patients with ischemic cardiomyopathy.
• Although some ♥ failure patients are obese, other patients with advanced ♥ failure experience a syndrome of chronic wasting, which can be exacerbated by unnecessary dietary ℟s.
• Frequent, small meals may combat the effect of anorexia caused by congestion of the GIT.
• Janet Reid-Hector, Ed.D, RD, CNSD
Effect of Pharmacological Management Of ♥♥♥♥ Failure
on Fluid & Electrolyte management
• There are 4 categories of drugs
which are used to improve cardiac
performances in CHF :
• inotropics,
• diuretics,
• vasodilators,
• and ACE inhibitor
Diuretics.
• The aim of diuretic
therapy is to reduce
pulmonary venous
pressure and to
• promote the excretion of
edema fluid.
• Janet Reid-Hector, Ed.D, RD, CNSD
Effect of Pharmacological Management Of ♥♥♥♥ Failure on Fluid
& Electrolyte Management
• Loop diuretics. Bumetanide(Bumex), Furosemide (Lasix), ethacrynic acid (Edecrin).
• Potent diuretics often used when pulmonary congestion must be
• ⇓ rapidly.
• Promote excretion of Na+ & H2O by blocking their reabsorption in the Loop of Henle.
• Over-vigorous Tx ⇛ to volume depletion which ⇛ to a ⇩ in CO.
•• Other adverse effects include:
hypokalemia, hyponatremia, & hyperglycemia
• Thiazide diuretics. Chlorothiazide (Diuril), Hydrochlorothiazide (Hydro Diuril).
• Widely used because they can be administered easily & are relatively inexpensive.
• Promote excretion of Na+, CL- & H2O by blocking their reabsorption in the renal tubules.
• Adverse side effects include: hypokalemia & hyperglycemia
• Janet Reid-Hector, Ed.D, RD, CNSD
Effect of Pharmacological Management Of ♥♥♥♥ Failure
on Fluid & Electrolyte Management
• Potassium-sparing diuretics. Spironolactone (Aldactone)
• Produces diuretic effect by inhibiting the action of Aldosterone in the distal tubule which ⇛ to Na+ & K+ potassium excretion .
• An adverse effect is hyperkalemia.
• Be aware that diuretics can produce dehydration& electrolyte depletion which can cause circulatory collapse.
• For this reason, monitor I/O, weight & serum Na+
• ACE inhibitors
• Allow kidneys to retain K+ while excreting Na+ & fluid.
• Therefore, patients receiving K+-sparing diuretics must be carefully monitored for hyperkalemia
• Janet Reid-Hector, Ed.D, RD, CNSD

Lymphedema
• Lymphedema is the buildup of lymph (a fluid that helps fight Infection & disease) in the fatty tissues just under the skin.
• A common complication of cancer/ cancer treatment & can result in long-term physical, psychological &social issues for patients.
• Janet Reid-Hector, Ed.D, RD, CNSD
Lymphedema
• Most common type of acute
Lymphedema develops very
slowly ; noticeable 18- 24
months after surgery or not
until many years after cancer
treatment.
• Patient may experience
discomfort of the skin; aching
in the neck, shoulders, spine
or hips ; or posture changes
caused by ⇑weight of arm/
leg.
• Recurrence or spread of a
tumor to the lymph nodes.
• Infection of and/or injury to
the lymphatic vessels.
• Periods of not being able to
move the limbs.
• Radiation Tx. or surgery.
• Blockage of a vein by a
blood clot
• Janet Reid-Hector, Ed.D, RD, CNSD
Diagnosis & Management of Lymphedema
Diagnosis Drug Therapy Dietary Management
To evaluate a patient for Lymphedema, a medical Hx & PE should be completed to include any past surgeries, and the time between surgery and the onset of symptoms of edema.
**Surgery may be required to remove excess fluid & Lipids
**A rare but fatal complication of Lymphedema is Lymphangiosarcoma, a tumor of the lymphatic vessels.
After a patient develops lymphangiosarcoma, the average survival time is a little > than 1 year.
Antibiotics may be used to treat/ prevent infections. Other types of drugs such as diuretics or anticoagulants are generally not helpful, and may make the problem worse.
***Coumarin: It was found to cause liver damage, has been banned since the 1950s; is available in several countries, but Φ approved for use in the US or Canada
Blood protein levels and weight should be monitored regularly, & patients should be encouraged to eat protein-rich foods.
Edema can make tissues less able to take in nutrients. Patients should be monitored for areas of skin breakdown, especially over areas with very little tissue between the skin & bone.
• Janet Reid-Hector, Ed.D, RD, CNSD
Hydration Case Study #1
• Joan is a 45kg lady with mild dementia and
urinary incontinence. She suffers with frequent
urinary tract infections and is slightly
underweight having lost 5kg in the last 12
months. She feeds herself however requires
prompting and encouragement. A fluid intake
chart shown Joan only consumed around 1L of
fluid/ day. How can we improve Joan’s
nutritional status focusing on her fluid intake?

Hydration Case Study #2Ted is a healthy weight gentleman at 80kg. He has
developed a swallowing problem after a recent stroke and is now having semi- thickened fluids & soft foods. He dislikes the semi thickened drinks and has recently been drinking very little. His urine is very dark and with a strong odor. He is feeling quite lethargic and has a dry mouth making it difficult to swallow his food. Ted is not enjoying the thickened drinks.
What would you recommend to help Ted Consume adequate fluids and nutrients?
Knowledge Check• 1. Dehydration is best described as:
• a. Input exceeds Output
• b. Output exceeds Input
• c. Input equals Output
• d. None of the above
• 2. What are some risk factors associated with dehydration? Circle the correct answer(s)
• a. Frequent diuretic, laxative, or enema use
• b. Lack of sense for thirst
• c. Increased need for feeding assistance
• d. Dysphagia
• e. All of the above
• 3. What are some of the physical changes that make the elderly more susceptible
• to dehydration? Circle the correct answer(s)
• a. Increased bladder capacity
• b. Acute illness
• c. Increased body water
• d. Inability
• 4. The nursing staff are the only ones responsible for ensuring patients /residents
• receive adequate fluids.
• True or False
• 5. What are possible effects of dehydration? Circle the correct answer(s)
• a. Decreased functional ability
• b. Fluid and electrolyte imbalance
• c. Fecal impaction
• d. All of the above
• 6. Besides mealtime, when might fluids be offered? Circle the correct answer(s)
• a. Medication Pass
• b. Activities
• c. At family visits
• d. Snack time
• e. All of the above
Nutrition Support in Older AdultsJanet Reid- Hector Ed. D, RD
1/26/11
PN is increasingly used in the elderly. Aging is accompanied by metabolic changes that can alter substrate utilization :
In the fasting state, REE was significantly higher in the elderly patients than in the middle-aged patients
In the elderly, TPN is associated with significantly higher lipid oxidation & lower glucose oxidation than in younger patients. TPN formulas and flow rates should therefore be adapted in the elderly.
• Janet Reid-Hector, Ed.D, RD, CNSD

� Insulin resistance⇝⇝⇝⇝ to a ⇓ glucose utilization &� Hyperglycemia with impairment of cardiac & renal Fxn are
the most relevant features.
� They may warrant the use of formula with ⇑lipid content –up to 50% of total energy intake.
� Deficiencies in vitamins, trace elements & minerals should be suspected in older subjects.
� In both the UK and the USA up to 40% of individuals aged ⋝65 or have an inadequate intake of one or more vitamins or minerals (ascorbate, folate, B12, B2, B1, magnesium, iron & Zn) with associated low blood concentrations.
• Janet Reid-Hector, Ed.D, RD, CNSD
� The effect of nutritional support on restoration of depleted body cell mass is ⇓ in older patients than in younger subjects.
� In addition, mild to severe hypophosphatemia is frequently found on admission, and commmonly develops, in older malnourished patients.
� Peripheral PN Both central and peripheral nutrition can be used in geriatric patients. Osmolarity of PPN nutrition should not be higher than 850 mOsmol/l. limited to 10-14 days
� Subcutaneous fluid administration is possible for fluid administrationn order to correct mild to moderate dehydration but not to meet other nutrient requirements.
• Janet Reid-Hector, Ed.D, RD, CNSD
� Functional status PN can support improvement of functional status, but the margin of improvement is lower than in younger patients.
� Active physical rehabilitation however, is essential for muscle gain.
� PN can ⇓mortality & morbidity in both older & middle-aged adults.
� Cardiac & renal functions are more likely to be impaired in older persons. Therefore fluid & Na+ intake should be limited, especially during periods of mobilization of ECF H2O that has accumulated due to inflammatory processes or during an earlier stage of refeeding
• Janet Reid-Hector, Ed.D, RD, CNSD
� Complications tend to be more frequent due to associated co-morbidities.
� Confusion during somatic illness is more common in geriatric patients & the syndrome of geriatric delirium may occur. During periods of confusion the tolerability of the IV catheter is ⇓.
� Due to the risk of cardiac failure, Na+ intake is often limited. With more vulnerable H2O homeostasis, & a tendency to⇑ EC & ⇩ in IC H2) both hypo- & hypervolemia are prone to occur.
� This is further complicated by ⇈ use of diuretics in this n population. These factors may also contribute to the thrombosis which is more common in the elderly on PN
• Janet Reid-Hector, Ed.D, RD, CNSD

� Older age was associated with a higher risk of central catheter vascular erosion.
� Hypophosphatemia plays a major role in the development of the refeeding syndrome. As PO4- is mainly IC, great losses occur in parallel with loss of muscle mass & progressive osteoporosis.
� PN (especially glucose) infusion can provoke a rapid drop in plasma PO4- level ⇒ to acute psychotic changes & Delirium.
� Glucose infusion, through the sudden increase in insulin can cause acute H2O and/or Na+ retention.
• Janet Reid-Hector, Ed.D, RD, CNSD
� Very low plasma levels of K+ or magnesium have also been reported, as a result of IC ion shift.
� In severely malnourished older subjects a stepwise increase of substrate intake (especially glucose) is necessary with strict monitoring of plasma electrolyte levels & timely corrections.
� Thiamine deficiency can also be evoked in the refeeding syndrome causing Wernicke’s Korsakov’s syndrome, with related features such as diplopia, confabulation, confusion & coma.
• Janet Reid-Hector, Ed.D, RD, CNSD
� TPN Electrolytes maintain normal cellular metabolism during TPN . Providing electrolytes in appropriate amounts prevents deficiency symptoms which otherwise would occur in their absence.
� In general, dosage usually starts at the low end of the dosing range, 2° the greater frequency of ⇓ hepatic, renal, & cardiac function, and of concomitant disease or other drug therapy.
� Na+ PO4- ions are substantially secreted by the kidney, & risk of toxic Rx may be greater in patients with impaired renal function.
� Care should be taken in dose selection, with monitoring of renal function.
� Sodium excess can cause edema & exacerbation of CHF.
� Excess potassium can cause deviations from the normal ECG . Potassium deficits can impair neuromuscular function, causing muscle weakness or frank paralysis, intestinal dilatation & ileus.
� Calcium deficits can produce neuromuscular hyper excitability ranging from paresthesias, cramps , laryngospasm, tetany & grand mal seizures.⇓ Ca+ levels can accompany administration of PN PO4- or large amounts of albumin.
� MG deficiency can precipitate neuromuscular dysfunction, hyperirritability, psychotic behavior, tachycardia & HTN. Magnesium excess can cause muscle weakness, ECG changes, sedation mental confusion.

Sodium Chloride Potassium
(K+)
Magnesium
(Mg)
Acetate
(CH3COO−)
Calcium
/The principal
EC cation; it
helps
maintain
motor nerves
, proper fluid
balance &
normal renal
metabolism
The principal
extracellular
anion which,
along with
Hco3,
maintains
proper anion
balance
The principal
IC cation;
transport
dextrose
across cell
membrane;
contributes to
normal renal
function.
Poorly
conserved by
kidney .
Mg is an
important
cofactor for
enzymatic
Rxs; maintain
normal CNS
activity & AA
utilization.
Eexcreted
solely by the
kidney at a
rate
+=plasma
conc. & GFR
Acetate
(CH3COO−)
provides
bicarbonate
(HCO3−) by
metabolic
conversion in
the liver even
in the severe
liver disease.
Muscle
contraction,
blood
coagulation ;
maintain
normal
neuromuscular
function.
• Janet Reid-Hector, Ed.D, RD, CNSD
� Energy
� Use of an easy calculation formula to measure
energy expenditure (REE) is strongly
recommended in the elderly. For people over 60
years old, the World Health Organization
(WHO) recommends the following:
� Males : REE= 8.8(W kg) + 1.128 (Ht m) - 1071
� Females : REE= 9.2 (W kg) + 637 (Ht m) - 302
� Adult RDA should be maintained.
� At least 0.8 g protein/ kg BW must be provided.
� The amount of protein that the elderly really receives
in relation to their BCM is higher compared with the
younger adult because cell mass is lost as people get
older, being replaced by fat mass.
� In metabolic stress: protein content ⇑ 1.5 g kg.
� More than 2 g/ kg does not improve N2 balance & serum urea could ⇑.
• Janet Reid-Hector, Ed.D, RD, CNSD
Weight Status & Anabolism During PN
♦ ECW is lost at a more rapid rate than ICW is ↑ during adequate nutrient delivery via TPN
♦ Initial weight loss during early phase of TPN induced anabolism
♦ Up to 3.6 kg wt. Loss/ first 4-5 days of PN in severely malnourished patients.
♦ After 1 - 4 days TBW and ICW both ↑ Normal Hydration restored
♦ Weight ↑ 0.2 - 0.5 kg/dy - gains in body fat mass & LBM
Janet Reid-Hector, Ed.D, RD, CNSD

Factors To Consider For Initiating Fluid Administration
for TPN Patients
1. Correct Imbalances
2. Provide Base & Maintenance Requirements
3. Replace Ongoing Losses
Janet Reid-Hector, Ed.D, RD, CNSD
Fluid Management Guidelines
1. Correct fluid, electrolyte deficits and acid balances
before initiating TPN.
2. Total fluid intake should be ↑ to achieve normal
urine output. i.e. not < 900mL/dy.
3. First sign of fluid overload : distention of IJ vein
4. Maximum acceptable central venous pressure
(cvp) → is 14.
* If Protein is < 5•0 gm/dl, hypooncontic edema
develops with cvp as low as 8 - 10 cm H2O
Janet Reid-Hector, Ed.D, RD, CNSD
Electrolyte Mgt. In TPN
Goal:
Provide elements for the conservation or repletion of cell compartments while also preserving the EC Environment.
The physical, chemical, functional anatomy of all body compartments must be considered in planning & delivering nutrition by vein.
Janet Reid-Hector, Ed.D, RD, CNS
Three Phases of Electrolyte/Mineral Requirement
Occurs during the first 3-5 days of IV Nutrition Support
Frequent changes in solution composition are necessaryFirst 24-48 hours Phase –2 Total Body Deficits May Begin – Sometime
of Electrolytes/ Mins. during 1st 24 hours & Must be replaced Lasts 2 – 3 days
Phase – 3Conversion To An Anabolic State
Requirement For K+, Mg+, Po4 – IC ElectrolytesFollowed by Stable Period of Maintenance Electrolyte & Mineral
Requirement
Janet Reid-Hector, Ed.D, RD, CNSD

Factors Affecting Electrolyte Requirement
• New Cell Synthesis
• Individual Variation Due to Differences In:
Total body deficits/ Excesses
Serum Concentrations
Maintenance requirements
• Ongoing Losses
♦ Third space fluid, surgery, trauma
♦ Hemorrhage into soft tissues, abdominal cavity
♦ Burns, wounds
• Renal Function
Janet Reid-Hector, Ed.D, RD, CNSD
HYPOKALEMIA in PN
• Glucosuria in spite of adequate insulin release.
• IC ratio of K+ : N of 35 :1 required for optimal protein synthesis.
• For optimal metabolic conditions, serum K+ must be maintained in high – NL. range.
• The more K+ retained by the body, the greater the increase in LBM.
Janet Reid-Hector, Ed.D, RD, CNSD
Treatment
Body K+ Deficits
• IV replacement, infusing ½ of calculated deficit
over 8-12 hours or up to 40 mEq/ hr via central line.
Excess
• Resin Binders, Dialysis
Emergent Cardiac Arrythmias
IV CA² , NaHCo , or ampule of
D50 with Insulin
Janet Reid-Hector, Ed.D, RD, CNSD
Insulin, K+ Connection in TPN Solutions
1. Not recommended to give insulin unless K+ supplementation is
adequate and s. conc. of K+ is normal
2. Recommend limit insulin to no > 70 - 80 u/dy
♦ Excessive insulin :
• Favors Diversion of Glucose → Fat Synthesis
• Down Regulates Insulin Receptors → Insulin
Resistance
Janet Reid-Hector, Ed.D, RD, CNSD

Insulin & Diabetes Mellitus
Type 1 DM: start with 100
gms dextrose/dy
Type 2 DM start with ≥ 200
gms dextrose/dy
****Cover enteral CHO with
NPH
Cover PN dextrose with IV
regular Insulin in TPN &
Sliding scale.
Insulin Sliding Scale****>400mg/dl IV drip
Capillary Glucose mg/dL
IDDM NIDDM(STRESS)
201-250 3 5
251-300 6 10
301-350 9 15
351-400 12 20
• Janet Reid-Hector, Ed.D, RD, CNSD
How much Insulin in TPN?
Practical Guidelines
Estimating insulin Insulin Dose =
Initial PN Kcals X Pre Hospital Insulin
BEE
***Check BS q 6 hrs; On Avg, Patients require 2X home dose of insulin
0.1 unit of insulin/gm dextrose
• Minimum dose = 10 U / bag/ ↑ Dose in 10 U increments
Avoid putting too much in TPN
Supplement with sliding scale
Add ½ of previous day’s SS to TPN
• Janet Reid-Hector, Ed.D, RD, CNSD
Final Dextrose concentration
• Conc. of Dextrose X Vol. of Dextrose
Total Volume
Example
D70 X 500= D14%
2450
• Janet Reid-Hector, Ed.D, RD, CNSD
Acetate
• Average TPN Patient Requires 50 mEq/L
• Quickly converted to HCO3 by Liver
• Most commercial AA Solutions contain acetate &
CL-
• Virtually impossible to create an acetate free TPN
solution
• CL- - acetate Imbalance Hyperchloremic
Acidosis/Alkalosis
Janet Reid-Hector, Ed.D, RD, CNSD

Sample CL-/ Acetate composition of Selected Amino
Acid Solutions (mEq/L)
Amino Acid Product CL Acetate
Travasol 8.5% 34 73
Travasol 10% 40 60
Trophamine 10% < 3 97
Novamine 15% - 151
Novamine 11.4% - 114
Janet Reid-Hector, Ed.D, RD, CNSD
Hyperchloremic Metabolic Acidosis
• For each 6 mEq/kg/day drop in C02, buffering capacity is cut in 1/2
• Tx : Substitute Acetate for the CL- salts of Na+, K+
• Correct underlying cause
• HCO3 may not be added to TPN soln. Incompatible/ Precepitation
Janet Reid-Hector, Ed.D, RD, CNSD
Calcium & PTH
• If serum CA² ↓↓↓↓ <10mg/100ml PTH ↑↑↑↑ .
• If ↑↑↑↑ >10mg/100ml PTH is suppressed.
• PTH ↓↓↓↓ Tubular reabsorption of PO4- & HCO3 by the kidney.
• Reabsorption of CL- →→→→ Hyperchloremic RTA.
• Excessive infusion of CA² or Vitamin D →→→→ Pancreatitis, Metabolic Bone DS.
• Should be given as Gluconate, Glucoheptonate or Glucoheptatesalt.
• Chloride salt is less soluble – should not be used. Janet Reid-Hector, Ed.D, RD, CNSD
Phosphate (Po4)
• Energy transfer & O2 transport & release
• Influence Leukocyte phagocytosis &
microbial resistance.
• Rapid Hypophosphatemia with Po4 deficient TPN soln.
Janet Reid-Hector, Ed.D, RD, CNSD

Po4- Requirement in TPN soln.
NL serum Conc.
• Begin TPN day #1 with 7-9 mm Po4/1000Kcal
Low serum conc.
• Begin TPN Day #1 with additional 3-5mm Po4/1000Kcal as K+ or Na salt.
• ↑↑↑↑ as necessary to maintain normal serum concentration.
• Po4 Ions may be given either as KPo4 (3mm Po4 & 4.4 mEq/K+/ml) or
As NaPo4 (3mm Po4 & 4 mEq/ml)
Janet Reid-Hector, Ed.D, RD, CNSD
Total Parenteral Nutrition Compatibility
• Calcium-Phosphate compatibility
– Factors which affect stability
• Additive concentration
• Choice of calcium salt
• Order of mixing
• Amino acid product (brand)
• Amino acid concentration
• Dextrose Concentration
• Temperature
• Storage time
• Addition of l-cysteine (neonatal)
• Janet Reid-Hector, Ed.D, RD, CNSD
Total Parenteral Nutrition Compatibility
• How to minimize calcium phosphate precipitation
• Additive concentration……..……....use lower the conc.
• Choice of Ca salt.…..…...use Ca Gluconate, not CaCl2
• Order of mixing…....add phosphate first, calcium last
• Amino acid product …Aminosyn® best, FreAmine® worst
• Amino acid concentration……….…use higher AA conc.
• Dextrose concentration………use higher Dextrose conc.
• Temperature………………………………………….…Refrigerate
• Storage time……………………....Minimized storage time
• l-cysteine (neonatal) ……..greatly increases solubility
• Janet Reid-Hector, Ed.D, RD, CNSD
Total Parenteral Nutrition Compatibility
• Normal range for serum calcium is – 8.5 to 10.5 mg/dL.
• Additional calcium is often added to TPN unnecessarily.
• 40% of calcium is protein bound.
• Only the free calcium is physiologically active.
• In hypoalbunemia the free calcium may be normal although the total serum calcium (measured value) may be low.
• How do you estimate free calcium?
• Janet Reid-Hector, Ed.D, RD, CNSD

Total Parenteral Nutrition Compatibility
–Correction of Calcium in Hypoalbunemia:
• Corrected Ca• =Observed Ca + 0.8 (Normal albumin– Observed albumin)
• =Observed Ca + 0.8 (4.0 – Observed albumin)
– Example
• Serum albumin = 2.8 ; Serum calcium = 7.9 mg/dL
• What is the corrected calcium?
• Should this patient receive additional calcium in the TPN?
• Corrected Ca = 7.9 + 0.8 (4.0 – 2.8)
• = 8.9 mg/dL
• Additional calcium not warranted.
Magnesium
• 2000 mEq in body, 60% in bone & unavailable for metabolism.
• 40% ICF
• NL Req. Pn. = 0.35 – 0.45 mEq/kg/day.
• GI losses : 30 – 40 mEq/day.
• Low serum levels, should be corrected gradually over days.
• High doses/short time = toxicity.
• In TPN, give as Mg So4. Janet Reid-Hector, Ed.D, RD, CNSD
Iron
♦ 3-5 gm in adult body
♦ Sl. > 50% in Hgb, 30-35% storage forms, tissue,
enzymes
♦ 1/2 life 60 - 120 minutes.
♦ Required for Hgb & myoglobin production,
essential metabolic enzymes. Janet Reid-Hector, Ed.D, RD, CNSD
The Paradox of Fe²+ Deficiency and Infection in PN
On one handFe²+ Deficiency: may ↑↑↑↑ susceptibility to some infections
: depress cellular immunity
: ↓↓↓↓ Leukocyte bactericidal activity
On the other handFe²+ Deficiency: →→→→ less Fe²+ available for Fe²+ dependent
microbes
result: ↑↑↑↑ host resistance to some bacterial infections
Janet Reid-Hector, Ed.D, RD, CNSD

Iron & TPN
♦ Maintenance Fe not typically provided in short term TPN
♦♦♦♦ Long term TPN requires supplement with Iron Dextran
0.1mg Iron Dextran/ day for maintenance
♦♦♦♦ Anemia
1.) Iron Dextran mixed in 500-1000mL D5W via separate line
2.) IM injections
3.) Calculating amount of Iron Dextran required
mg Fe required = 0.3 (wt lb.)
x (100 - Hgb x 100)
14.8
4.) Iron Dextran will break or destabilize 3 - 1 TPN mixtures, use is not recommended
Janet Reid-Hector, Ed.D, RD, CNSD
Janet Reid-Hector, Ed.D, RD, CNSD
• Janet Reid-Hector, Ed.D, RD, CNSD
Lipids are cleared by 2 mechanisms
Plasma Lipid Concentration ↓↓↓↓as the duration of infusion lengthens
1. First order Kinetics
As the Infusion Rate↑↑↑↑Plasma concentration ↑↑↑↑Clearance Rate ↑↑↑↑
Lipid Clearance is in direct relation
to plasma level
2. Above the max. clearance capacity
Lipid is metabolized via
Zero order Kinetics
Clearance rate is constant
Plasma concentration rises
Janet Reid-Hector, Ed.D, RD, CNSD
Key Points of Lipid Infusion to prevent
Complications
Lipid infused over 12 - 24 hours with 24 hrs continuously will result in rate of infusion remaining at or below max clearance capacity
Continuous Lipid Administration
Lipids are oxidized more efficiently than repeated discontinuous doses.
• Janet Reid-Hector, Ed.D, RD, CNSD

Adverse Reactions to IV Lipid
Administration
Rapid Infusions Acute Reactors Long Term
Cyanosis
HeadacheNausea Oily Taste in MouthPain at Injection Site PalpitationsTachypneaWheezing
Pruritic UrticariaChest/ Back painChills/ FeverVomiting
EosinophiliaFat Overload SyndromeHepatomegalyJaundice/ CholestasisLeukopeniaSplenomegalyThrombocytopeniaTransient ↑ LFT’S
Janet Reid-Hector, Ed.D, RD, CNSD
Total Parenteral Nutrition
Electrolytes
Elect. Range of Daily Requirement
Standard Concentration
Na 60-150 meq 35-50 meq/L
K 40-240 meq 30-40 meq/L
Ca 3-30 meq 5 meq/L
Mg 10-45 meq 5-10 meq/L
Phos. 30-50 mM 12-15 mM/L
• Janet Reid-Hector, Ed.D, RD, CNSD
Electrolyte Requirement for Critically Ill TPN Patients
Electrolyte Daily Increased DecreasedRequirement Requirements Requirements
Na+ 60 - 150 mEq ♦♦♦♦ Loop Diuretics ♦♦♦♦ HTN, Fluid overload
K+ 70 - 100 mEq ♦♦♦♦ Early nutritional repletion ♦♦♦♦ Renal Failure
♦♦♦♦ Post obstruction diuresis♦♦♦♦ Diuretic Therapy
♦♦♦♦ ↑↑↑↑ GI Losses
Mg+ 10 - 20 mEq ♦♦♦♦ Early nutritional repletion ♦♦♦♦ Renal Failure
♦♦♦♦ Diuretic Therapy
♦♦♦♦ ↑↑↑↑ GI Losses
CA 5 - 20 mEq ♦♦♦♦ Multiple blood Transfusions
Po4 10 - 60 mmoL/dy ♦♦♦♦ Early nutritional repletion ♦♦♦♦ Renal Failure
CL 80 - 120 mEq ♦♦♦♦ Prolonged gastric losses
Acetate 10 - 60 mEq ♦♦♦♦ Metabolic Acidosis ♦♦♦♦ Metabolic Alkalosis
♦♦♦♦ Excessive Diarrhea
♦♦♦♦ Drug Therapy - Polybinders
Electrolytes ⇓ Requirements ⇑Requirements⇓ Requirements ⇑Requirements⇓ Requirements ⇑Requirements⇓ Requirements ⇑Requirements
• Janet Reid-Hector, Ed.D, RD, CNSD
Total Parenteral Nutrition
Electrolytes
• Electrolyte salts commercially available
• Sodium chloride
• Sodium acetate
• Sodium phosphate
• Potassium chloride
• Potassium acetate
• Potassium phosphate
• Calcium gluconate
• Calcium chloride (not recommended)
• Magnesium sulfate
• Magnesium chloride
• Incompatible: Sodium bicarbonate
• Janet Reid-Hector, Ed.D, RD, CNSD

Effects of Specific Drugs on Electrolyte Balance
Electrolyte Drugs Effect
Na+ ♦ Thiazide, Loop Diuretics, Cisplatin, ♦ ↑↑↑↑ urinary Na+ Excretion
Trimethoprim - sulfamethoxzole
♦ Antipseudomonal penicillins ♦ ↑↑↑↑ Na+ load to PT
K+ ♦ Thiazide, Loop Diuretics, ♦ ↑↑↑↑ urinary K+ excretion
Amphotericin-B, steroids,
Antipseudomonal penicillins
♦ Insulin, B - Agonists ♦ ICF K+ shift
♦ spironolactone, Amiloride, Heparin ♦ ↑↑↑↑ urinary K+ excretion
Po4 ♦ Antacids, sucralfate
♦ Precepitation of dietary & ``````` secreted Po4 in the GIT
Mg ♦ Aminoglycosides, Amphotericin-B, ♦ ↑↑↑↑ urinary Mg excretion
Loop Diuretics, Cisplatin,
Cyclosporine
Janet Reid-Hector, Ed.D, RD, CNSD
Trace Element Recommendations for Critically Ill
PatientsTrace Adult Daily MTE-5 *Special Requirements
Element TPN Requirements
Zinc 2.5 - 4.0 mg 5 mg * Add 2 mg/dy - Acute catabolic stress
10 - 15 mg (diarrhea, fistula, wounds
Copper 1.0 - 1.5 mg 1 mg * Reduced need /w/ biliary obstruction
Manganese 0.15 - 0.8 mg 0.5 mg * Reduced need /w/ biliary obstruction
Chromium 10 - 15 µg 10 µg * 40 µg (diarrhea, GI losses)
* Reduced need /w/ Renal Failure
Selenium 40 - 80 µg 60 µg * ↑ losses in burns, GI DS Janet Reid-Hector, Ed.D, RD, CNSD
Total Parenteral Nutrition
Vitamins
• Recommendations per NAG
– Multivitamin Infusion 10 ml
– Contain all essential vitamins
– MVI-Adult (Mayne) or Infuvite (Baxter)
– Fat soluble: A, D, E, K
– Water soluble: Thiamine, Riboflavin, Niacin, Pantothenic Acid,
Pyridoxine, C, Folic Acid, B12, Biotin
– In 2004 Vitamin K added per FDA recommendations
• Janet Reid-Hector, Ed.D, RD, CNSD
Multivitamin Requirement for TPN Patients
Vitamin IV Dose Requirement Special Requirements
in TPN/dy
A IU 3300 IU (1mq) 5000+ IU/dy (serious infection)
D IU 200 IU (5µg)
E 200 IU (10 mg)
Biotin 60 mg
Pantothenic Acid 15 mg
Folic Acid 0.4 mg 5 mg/dy ICU Patients/Thrombocytopenia
1 mg/dy - Dialysis
Thiamin 3 mg 50 mg Alcoholics - Wernicke - Karsakoff
Riboflavin 3.6
Niacin 40 mg
Pyridoxine 4.0 - 6.0
Ascorbic Acid 100
Cyanocobalamin 5.0 µg
Vitamin K 10 mg 1 - 2 x 1 week
Janet Reid-Hector, Ed.D, RD, CNSD

Osmolarity of Common PN Components
Central line blood flow = 2500mL/min Peripheral Blood Flow = 25-50mL/minPPN Solns > 600-900 m0sm/L=↑ risk of phlebitis
TPN Components
mOsmol Factor
Amino Acids 100 Per % final Conc.
Glucose 50 Per % final Conc.
lipid 1.7 Per gm
Calcium 1.4 Per mEq
• Janet Reid-Hector, Ed.D, RD, CNSD
Osmolarity of Common PN
Components
Electrolytes
TPN Components mOsmol Factor
Magnesium 1 Per mEq.
Potassium 2 Per mEq.
Sodium 2 Per mEq.
• Janet Reid-Hector, Ed.D, RD, CNSD
Selected Protocol for Determining Electrolyte/ Mineral Additives to TPN
1. Determine Total Fluid Volume.
2. Determine Macronutrients (Dextrose, AA, Lipids).
3. Determine Required Amount of Na+, K+, CL-, PO4 -, Ca�+, Mg+, Trace Elements.
4. Subtract Amount of Electrolytes in the AA Solution.
5. Add PO4 - (Na+ or K+) or Acetate Salt to Maintain NL ABB.
6. Determine Amount of CL-; Subtract Na+ Ion content in AA soln., from total CL- content, Add difference
as Na Acetate.
* Na + & CL- Ions are balanced.
7. Add remainder of required Na+ as CL salt.
* Na+ Ion is now = CL - Ion concentration.
8. Add Mg as MgSO4.
9. Add Ca as Ca Gluconate.
10. Add trace elements, vitamins, heparin, insulin as required.
Janet Reid-Hector, Ed.D, RD, CNSD
Total Parenteral Nutrition Formulation
Standardization vs. Customization
• Standardization
– Meets requirements of most patients
– Assists physician in order writing
– Reduces errors (writing, transcription and order entry)
– Increases pharmacy efficiency
– Cost savings
• Customization
• Patient Specific
• Consistent with current
recommendations
– Can be accomplished with and
without automated compounded
– Should be strongly considered b in
patients requiring fluid or CHO
restriction

Golden Rule for Calculating & Balancing
Electrolytes for TPNSum Total of Anions ¯
Must Equal
Sum Total of Cations +
Janet Reid-Hector, Ed.D, RD, CNSD
CONVERSION
mm K Phos -- > mEq K+
mm Na Phos --> mEq Na+
Each 3 mm Kphos = 4.4 mEq K+ Each 3 mm Na Phos = 4 mEq Na+
mm Kphos, Na Phos mEq K+ mEq Na+
5 7.3 6.7
10 14.6 13.3
15 22 20
20 29.3 26.7
25 36.6 33.3
30 44 40
35 51.3 46.7
40 58.6 53.3
45 66 60
50 73.3 66.7
Janet Reid-Hector, Ed.D, RD, CNSD
CALCULATING ELECTROLYTES FOR TPN
EXAMPLE
Na+ 100
K+ 70
CL- 63___________________
(170-44=126)
Acet 63___________________
PO4 30 ___________ 44mEq+ K+ & 30 mm Po4
CA²+ 9.0
Mg+ 9.0
Janet Reid-Hector, Ed.D, RD, CNSD
Steps for Balancing Electrolytes in TPN
Step 1
Na 100
CL 63
Step 2
100
- 63
37mEq of Na left to balance
use Na Acetate to Balance
Step 3
63
- 37
26mEq of AC- left to use
↓use as KAC-
Step 4
26mEq of K AC
since K+ = 70
70
- 26
Step 5 44mEq of K ↓ left to use
(balance use as KPo4 =
30)
Step 6 30mm Kphos - 44 mEq of K
Step 7 Then Ca as gluconate
↓Then Mg as sulphate
Lyn Roth, RPH

ORDERING BALANCED ELECTROLYTES
Na CL 63mEq
KCL - mEq
NA Acetate 37mEq
K Acetate 26mEq
Na Po4 - mmol
K Po4 30mmol
Ca Gluconate 9.0mEq
Mg So4 10.0mEq Janet Reid-Hector, Ed.D, RD, CNSD
Lyn Roth, RPH
Metabolic Monitoring Schedule for the Critically Ill TPN Client(1)
ParametersFluid Balance
Body Weight
Intake (po & IV)
Output
Monitor infusion rate
Infectious Complications
WBC
Vital signs
Catheter dressing change
Biochemical Measures
Serum electrolyte levels
BUN, Creat.
Ca, Mg, PO4
BS
ABB
Plasma protein
Triglyceride
LFT’s
PT, PTT
Hgb
Frequency
Daily
q 8 hr
q 8 hr
q 4 hr
Daily
As indicated
q 48 hr
Daily
Daily
Daily x 3 then 3 x/wk
Daily
As indicated
Weekly
Preinfusion and postinfusion, then weekly
Weekly
Weekly
Weekly Janet Reid-Hector, Ed.D, RD, CNSD
Complications of PN feeding in the elderly
• These fall into three groups:
• Mechanical (post-catheter pneumothorax)
• Infectious; (catheter sepsis)
• Metabolic (electrolyte disturbances,
• hyperglycemia, serum urea).
• PN-associated complications ⇑ in this population
• Janet Reid-Hector, Ed.D, RD, CNSD
Complications of PN feeding in the elderly
• Hyperglycemia, uremia & electrolyte disturbances
• are more frequent.
• Fluid overload associated with cardiac failure risk is always present.
• Respiratory failure & CO2 retention.
• Due to their depressed immunology response, catheter sepsis risk is prevalent.
• Although prolonged PN is rarely supplied to the
• elderly, when it is done, it should be borne in mind
• that both metabolic (mainly bone & liver diseases)
• Psychological complications will affect the elderly more deeply than the adult.
• Janet Reid-Hector, Ed.D, RD, CNSD

Refeeding Syndrome• The ℞ for people at high risk of developing refeeding
problems should consider:
• Starting nutrition support at a maximum of 10 kcal/kg/day, ⇑ levels slowly to meet or exceed full needs by 4–7 days.
• Using only 5 kcal/kg/day in extreme cases (for e.g.; BMI<14 kg/m2 or negligible intake for > 15 days) & monitoring cardiac rhythm continually for cardiac arrythmias
• Restoring circulatory volume, monitoring fluid balance & overall clinical status closely. Providing immediately before and during the first 10 days of feeding: oral thiamin 200–300 mg daily, vitamin B, (or daily IV vitamin B) & a balanced MVIT/TE supplement once daily
• Janet Reid-Hector, Ed.D, RD, CNSD
Refeeding Syndrome
• Providing K+: 2–4 mmol/kg/day)
• Phosphate: 0.3–0.6 mmol/kg/day)
• Mg : 0.4 mmol/kg/day; unless pre-
feeding plasma levels are high.
• Pre-feeding correction of low plasma
• levels is unnecessary.
PN Monitoring Protocol for the older adult
Parameter Frequency Rationale
Catheter entry site* Daily Signs of infection/inflammation
Skin over position of catheter
tip (PPN fed people)*
Daily Signs of thrombophlebitis
Temperature/BP Daily initially, then as
needed
Sign of infection/fluid balance
Drug therapy* Daily initially,⇩ to
monthly; when stable
To prevent / ⇩ DNI
Are goals being met?* Daily initially, ⇩ to
2x/week, then progress
to 3–6 mon., unless
clinical condition changes
To ensure that feeding is
appropriate to overall patient care
Sodium, potassium, urea,
creatinine
Baseline; Daily until
stable; then 1- 2 X a week
Assessment of renal function,
fluid status, & Na and K
Status; Glucose intolerance
PN Monitoring Protocol for the older adult
Parameter Frequency
Glucose Baseline; Daily until stable; Then 1 or 2 times a week
Magnesium, phosphate Baseline; 1 or 2 times a day (or more if needed) until stable
Then weekly
Temperature/BP Daily initially, then as needed
Drug therapy* Daily initially,⇩ to monthly; when stable
Are goals being met?* Daily initially, ⇩ to 2x/week, then progress to 3–6 mon., unless
clinical condition changes
Sodium, potassium, urea,
creatinine
Baseline; Daily until stable; then 1- 2 X a week
• Janet Reid-Hector, Ed.D, RD, CNSD

References• Landry DW, Bazari H. Approach to the patient with renal disease. In: Goldman L, Schafer AI, eds. Cecil Medicine. 24th ed. Philadelphia, Pa: Saunders
Elsevier; 2011:chap 116. Update Date: 8/21/2011; by: David C. Dugdale, III, MD, Professor of Medicine, Division of General Medicine, Department of Medicine, University of Washington School of Medicine. Also reviewed by David Zieve, MD, MHA, Medical Director, A.D.A.M., Inc.
• Nephrol Dial Transplant. 1996;11 Suppl 9:9-17. Some sodium, potassium and water changes in the elderly and their treatment. Andreucci VE, Russo D, Cianciaruso B, Andreucci M.Chair of Nephrology, Faculty of Medicine, University Federico II of Naples, Italy.
• Alvelos, M, Ferreira, A, Bettencourt P, et al. The effect of dietary sodium restriction on neurohumoral activity and renal dopaminergic response in patients with heart failure. Eur J Heart Failure. 2004; 6: 593-599.
Arcand JL, Brazel S, Joliffe C, et al, Education by a dietitian in patients with heart failure results in improved adherence with a sodium-restricted diet: A randomized trial. Am Heart J. 2005; 150: 716e1-716e5.
Damgaard M, Norsk P et al. Hemodynamic and neuroendocrine responses to changes in sodium intake in compensated heart failure, Am J Physiol Regul Integr Comp Physiol. 2006, 290: R1294-R1301.
Kuehneman T, Saulsbury D, Splett P, Chapman DB. Demonstrating the impact of nutrition intervention in a heart failure program. J Am Diet Assoc. 2002; 102: 1,790-1,794.
Ramirez EC, Martinez LC, et al. Effects of a Nutritional Intervention on Body Compositiion, Clinical Status, and Quality of Life in Patients with Heart Failure. Nutrition, 2004; 20: 890-895.
• Task Force for the Diagnosis and Treatment of Chronic Heart Failure, European Society of Cardiology. Guidelines for the diagnosis and treatment of chronic heart failure. Eur Heart J. 2001;22:1527-60.
• American College of Cardiology/American Heart Association. 2005 Guideline Update for the Diagnosis and Management for CHF in the Adult. Circulation. 2005;Sept 20:1-28.
• Heart Failure Society of America 2006 Comprehensive Heart Failure Practice Guideline. Journal of Cardiac Failure.
• 2006; 12.
References• Effect of age on substrate oxidation during total parenteral nutrition.Al-Jaouni R, Schneider SM, Rampal P, Hébuterne X. Nutrition.
2002 Jan;18(1):20-5.
• Public Health Nutrition: 4(6A), 1379±1384 Guidelines for nutrition support in the elderly
• Metheny, N. (2000). Fluid and electrolyte balance. In Nursing Considerations (4th Ed., pp. 3–12, 24–26). St. Louis, MO: Lippincott, Williams, & Wilkins. Evidence Level VI: Expert Opinion.
• Lindeman, R., Tobin, J., & Shock, N. (1985). Longitudinal studies on the rate of decline in renal function with age. Journal of the American Geriatrics Society, 33, 278–285. Evidence Level IV: Nonexperimental Study.
. Kenney, W. L., & Chui, P. (2001). Influence of age on thirst and fluid intake. Medicine & Science in Sports and Exercise, 33, 1524–1532. Evidence Level V: Literature Review.
• Mentes, J. (2006). A typology of oral hydration problems exhibited by nursing-home residents. Journal of Gerontological Nursing, 23(1), 13–21. Evidence Level IV: Nonexperimental Study
• Mentes, J. C., and The Iowa Veterans Affairs Nursing Research Consortium (2004). Evidence-based protocol: Hydration management. In M. G. Titler (Series Ed.), Series on evidence-based practice for older adults. Iowa City, IA: The University of Iowa College of Nursing Gerontological Nursing Interventions Research Center, Research Translation and Dissemination Core. Evidence Level I: Systematic Review.
• Ferry, M. (2005). Strategies for ensuring good hydration in the elderly. Nutrition Reviews, 63(6), S22–S29. Evidence Level V: Literature Review.
• Sullivan RJ. Fluid intake and hydration: critical indicators of nursing home quality. North Carolina Med J 2005; 66: 296-9.
•• Mentes JC. A typology of oral hydration problems exhibited by frail nursing home residents. Geront Nurs 2006; 32: 13-9.
References• Semin Nephrol. 1996 Jul;16(4):277-88. Abnormalities of water metabolism in
the elderly.
• Tullman, D. F., Mion, L. C., Fletcher, K., & Foreman, M. D. (2008). Oral hydration
management. In E. Capezuti, D. Zwicker, M. Mezey, & T. Fulmer (Eds.).
Evidence-based geriatric nursing protocols for best Practice (3rd ed.), (pp. 337-
351). New York: Springer Publishing Company, Inc.
• J Nutr Health Aging. 2009 Feb;13(2):150-7
• Musson ND, Kincaid J, Ryan P et al. Nature, nurture, nutrition; interdisciplinary
programs to address the prevention of malnutirition and dehydration.
Dysphagia 1990; 5: 96-101.
• . Amella EJ. Feeding and hydration issues for older adults with dementia. Nurs
Clin North Am 2004; 39: 607-23.
• A comparison of intravenous and subcutaneous hydration in elderly acute
stroke patients. Postgrad Med J 1994; 70: 195-7


















