Managing critical care facilities Dr Sarah Ramsay Consultant Anaesthetist Western Infirmary, Glasgow...
21
Managing critical care facilities Dr Sarah Ramsay Consultant Anaesthetist Western Infirmary, Glasgow Pandemic Flu – Planning Scotland’s Health Response, 5th June 2007, RCPE
-
Upload
ellen-chase -
Category
Documents
-
view
225 -
download
0
Transcript of Managing critical care facilities Dr Sarah Ramsay Consultant Anaesthetist Western Infirmary, Glasgow...
Managing critical care
facilities
Dr Sarah Ramsay
Consultant Anaesthetist
Western Infirmary, Glasgow
Pandemic Flu – Planning Scotland’s Health Response, 5th June 2007, RCPE
Contingency planning
• Global
• National (DoH, SEHD etc)
• NHS Scotland Boards
• Local ICU groups
• Individual Hospitals

Spectrum of illness
Seasonal influenza
• Extremes of ages
• Exacerbation of other co-morbid conditions
• Secondary bacterial infections
> primary viral pneumonia
• Rare: myocarditis, GBS, encephalitis, etc.

Spectrum of illness
NB…
• 10-25% of CAP patients require ICU
• ~ 50% require other organ support
• ICU stay longer than non respiratory conditions
• Mortality ~ 30%
– Increased if delay prior to ICU admission

Spectrum of illness
Pandemic influenza– As seasonal flu?– Excess cases & deaths
Or…– Younger adults affected?– Primary viral pneumonia?– Cytokine storm multiple
organ failure?
Patient subgroups
• Elderly
• Paediatrics
• Obstetrics
• Immuno-compromised
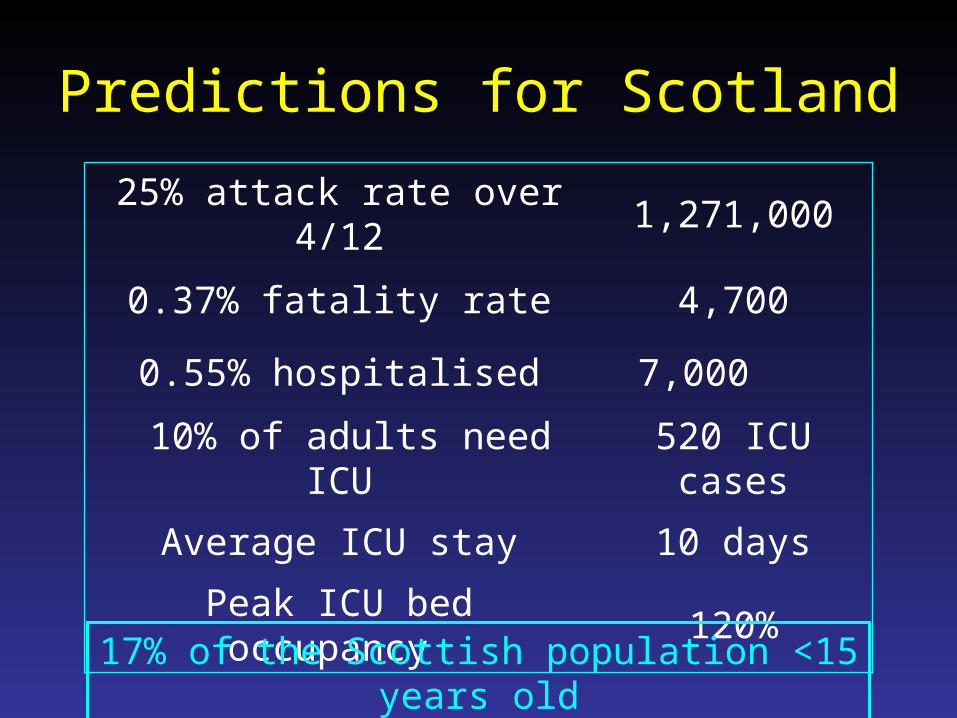
Predictions for Scotland
25% attack rate over 4/12 1,271,000
0.37% fatality rate 4,700
0.55% hospitalised 7,000
10% of adults need ICU 520 ICU cases
Average ICU stay 10 days
Peak ICU bed occupancy 120%
17% of the Scottish population <15 years old

ICU beds required, varying mortality (25% attack rate)
0200
400600800
10001200
14001600
1 9
17
25
33
41
49
57
65
73
81
89
97
10
5
113
Days of pandemic
0.37%1.00%
1.50%
Mortality rate

Increasing capacity
Realistic & sustainable
• Identify current HDU/ICU capacity• Identify additional capacity• Reduce elective work• Remember…
– Non-flu ICU patients– Transport of critically ill patients– Paediatric cases?

Increasing capacity
• Bed spaces• Ventilators• Piped gases• Drugs & supplies• Other equipment• PPE• Most important = staff

Increasing staffing
• Remember impact of staff sickness
• Profile current staff
• Identify reserve staff
• Engage in advance
• Train & maintain
• Ensure staff confidence

Risks of unfamiliar staff in ICU
• Clinical errors
• Infection control failures
• Fatigue
• Stress

Additional staff
• Appropriate key skills in intensive care
• Supervision
• Protocols & guidelines
• Infection control– Self protection– Prevention of HAIs
• Rosters
• Support and communication

Containment and infection control
• Education –staff, patients & visitors
• Exclude / restrict ill workers & visitors
• Cohort affected patients; cohort staff
• Appropriate infection control precautions
– Environmental infection control
– Standard infection control principles
– Droplet precautions
– Higher level protection for aerosol generating procedures
DH Draft guidance for IC in the ICU during pandemic flu

Aerosol generating procedures
• Minimise occurrence– Closed circuits, minimise breaks, filters
• Maximise safety– Use full garb including FFP3 masks
– Minimum number of staff present
– Preferably in a negative pressure side room
– Consider extended use of PPE in busy units
Common in ICU: Intubation, physio, bronchoscopy, suctioning, nebulisers, tracheostomy care, NIV

Managing demand
Referral, admission and discharge criteria• Work with other specialities (A&E, respiratory,
infectious diseases)

DoH clinical guidelines for HDU/ICU transfer
• Primary viral pneumonia• Severe CAP (CURB-65
score of 4-5)• General indications:
– persistent hypoxia on maximal O2
– progressive hypercapnia– severe acidosis (pH < 7.25)– septic shock– exacerbation of underlying
co-morbid disease

Managing demand
Triage decisions
• Who & who not to admit
• What to start and not start?
• When to stop?
• National ethics framework in development
• Transparency
Strange times…
• Indemnity
– For unit staff
– For reserve staff
• Derogations
– EWTD
– Targets waiting lists, standards of care
• Duty of care of individuals & institutions
– Conscientious objectors?

Picking up the pieces
• Exhaustion
• Deaths
• Backlog
• Further wave(s)
Flu in the ICU
• Important role for ICU• Exact disease unclear• Escalation realistic and
sustainable • Staff confidence vital• Integrated and co-operative
preparedness planning