Managing Acute Non-Cancer Pain in the Hospital · Managing Acute Non-Cancer Pain in the Hospital...
101
Managing Acute Non-Cancer Pain in the Hospital October 21, 2017 1 Ramana K. Naidu, MD Director of Pain Management at Marin General Hospital Mt Tam Orthopedics & Spine Center [email protected]
-
Upload
vuongquynh -
Category
Documents
-
view
215 -
download
0
Transcript of Managing Acute Non-Cancer Pain in the Hospital · Managing Acute Non-Cancer Pain in the Hospital...
ManagingAcuteNon-CancerPainintheHospital
October21,20171
RamanaK.Naidu,MDDirectorofPainManagementatMarinGeneralHospitalMtTamOrthopedics&[email protected]
RamanaK.Naidu,MDhasdisclosedrelationshipswithanentityproducing,marketing,reselling,ordistributinghealthcaregoodsorservicesconsumedby,orusedon,patients.
Speaker’sBureauHalyardHealthAbbott
DisclosuresofFinancialRelationships
2

BLISSFULINSENSATION?CONGENITALINSENSITIVTYTOPAIN
DENTALABSCESSESCORNEALABRASIONSBONEFRACTURES
INFECTIONS
HeckertJ.TheHazardsofGrowingUpPainlessly.NYTimesMagazine.Nov15,2012.
BLISSFULINSENSATION?CONGENITALINSENSITIVTYTOPAIN
DENTALABSCESSESCORNEALABRASIONSBONEFRACTURES
INFECTIONS
HeckertJ.TheHazardsofGrowingUpPainlessly.NYTimesMagazine.Nov15,2012.
Thephilosophicaldichotomyofacutepain…
SufferingDepressionHelplessness
WarningSignalAvoidanceReminder
Healing
4
Thephilosophicaldichotomyofacutepain…
SufferingDepressionHelplessness
WarningSignalAvoidanceReminder
Healing
4
Definitions
Pain:anunpleasantsensoryandemotionalexperienceassociatedwithactualorpotentialtissuedamage,ordescribedintermsofsuchdamage.
AcutePain:•Painthatislimitedtotheexpectedperiodofhealing.•Temporaldefinitionsvary.<1month.<3months.<6months.SubacutePain:•Atransitionalperiodbetweenacuteandchronicpainwhereoneisconcernedtheacutepainisbecomingpersistent.
•Temporaldefinitionsvary.1-6months.ChronicPain:•Painthatpersistsbeyondtheexpectedperiodofhealing.•Temporaldefinitiionsvary.>3months.>6months.
Merskey,H.(1964),AnInvestigationofPaininPsychologicalIllness,DMThesis,Oxford
5
Trauma•BoneFractures•Burns•Weapons
Surgery
AcuteMedicalIllness•DentalCaries• InfectiousSequelae•Lumbago•Headache•AbdominalPain
TypesofAcuteNon-CancerPain
Rice,A.S.C.,Smith,B.H.&Blyth,F.M.Painandtheglobalburdenofdisease.Pain157,791–6(2016).
6
Trauma•BoneFractures•Burns•Weapons
Surgery
AcuteMedicalIllness•DentalCaries• InfectiousSequelae•Lumbago•Headache•AbdominalPain
TypesofAcuteNon-CancerPain
Rice,A.S.C.,Smith,B.H.&Blyth,F.M.Painandtheglobalburdenofdisease.Pain157,791–6(2016).
Globalburdenofdisease:Pain4.3%ofthetheworld’spopulationisfreeofdisease,injury,orsequelae.
GlobalprevalenceofDentalCaries:2.4billionindividuals
GlobalprevalenceofTension-TypeHeadaches:1.6billionindividuals
Greatestcauseofyearslivedwithdisabilityis:Lowbackpain
6
Doweneedtotreatormanageoracutenon-cancerpain?
Rich,B.Physicians’legaldutytorelievesuffering.West.J.Med.175,151–2(2001).
7
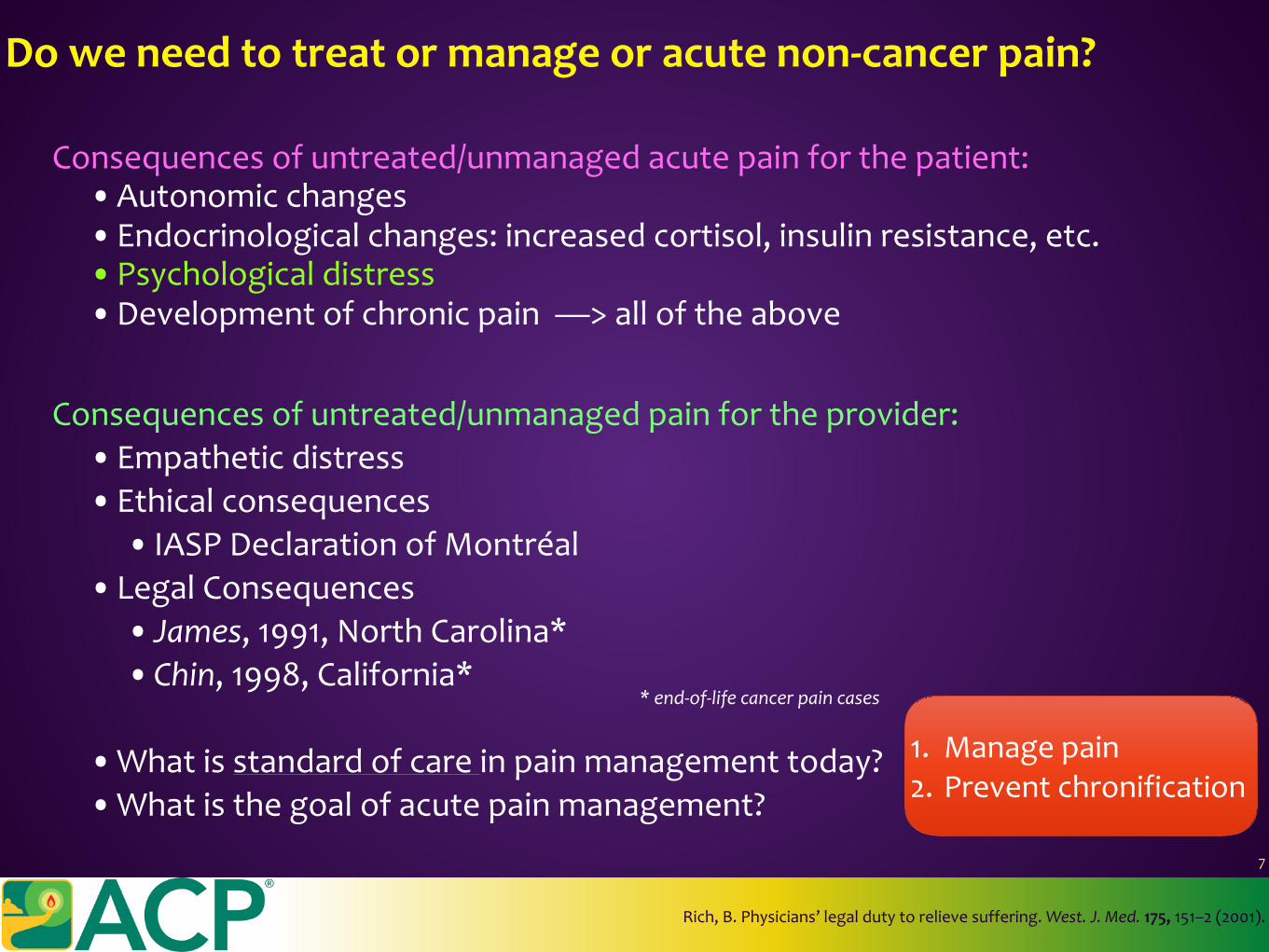
Doweneedtotreatormanageoracutenon-cancerpain?
Rich,B.Physicians’legaldutytorelievesuffering.West.J.Med.175,151–2(2001).
Consequencesofuntreated/unmanagedacutepainforthepatient:•Autonomicchanges•Endocrinologicalchanges:increasedcortisol,insulinresistance,etc.•Psychologicaldistress•Developmentofchronicpain—>alloftheabove
7
Doweneedtotreatormanageoracutenon-cancerpain?
Rich,B.Physicians’legaldutytorelievesuffering.West.J.Med.175,151–2(2001).
*end-of-lifecancerpaincases
Consequencesofuntreated/unmanagedpainfortheprovider:•Empatheticdistress•Ethicalconsequences
• IASPDeclarationofMontréal•LegalConsequences
• James,1991,NorthCarolina*•Chin,1998,California*
•Whatisstandardofcareinpainmanagementtoday?•Whatisthegoalofacutepainmanagement?
Consequencesofuntreated/unmanagedacutepainforthepatient:•Autonomicchanges•Endocrinologicalchanges:increasedcortisol,insulinresistance,etc.•Psychologicaldistress•Developmentofchronicpain—>alloftheabove
7
Doweneedtotreatormanageoracutenon-cancerpain?
Rich,B.Physicians’legaldutytorelievesuffering.West.J.Med.175,151–2(2001).
*end-of-lifecancerpaincases
Consequencesofuntreated/unmanagedpainfortheprovider:•Empatheticdistress•Ethicalconsequences
• IASPDeclarationofMontréal•LegalConsequences
• James,1991,NorthCarolina*•Chin,1998,California*
•Whatisstandardofcareinpainmanagementtoday?•Whatisthegoalofacutepainmanagement?
Consequencesofuntreated/unmanagedacutepainforthepatient:•Autonomicchanges•Endocrinologicalchanges:increasedcortisol,insulinresistance,etc.•Psychologicaldistress•Developmentofchronicpain—>alloftheabove
7
Doweneedtotreatormanageoracutenon-cancerpain?
Rich,B.Physicians’legaldutytorelievesuffering.West.J.Med.175,151–2(2001).
*end-of-lifecancerpaincases
Consequencesofuntreated/unmanagedpainfortheprovider:•Empatheticdistress•Ethicalconsequences
• IASPDeclarationofMontréal•LegalConsequences
• James,1991,NorthCarolina*•Chin,1998,California*
•Whatisstandardofcareinpainmanagementtoday?•Whatisthegoalofacutepainmanagement?
Consequencesofuntreated/unmanagedacutepainforthepatient:•Autonomicchanges•Endocrinologicalchanges:increasedcortisol,insulinresistance,etc.•Psychologicaldistress•Developmentofchronicpain—>alloftheabove
7
Doweneedtotreatormanageoracutenon-cancerpain?
Rich,B.Physicians’legaldutytorelievesuffering.West.J.Med.175,151–2(2001).
*end-of-lifecancerpaincases
Consequencesofuntreated/unmanagedpainfortheprovider:•Empatheticdistress•Ethicalconsequences
• IASPDeclarationofMontréal•LegalConsequences
• James,1991,NorthCarolina*•Chin,1998,California*
•Whatisstandardofcareinpainmanagementtoday?•Whatisthegoalofacutepainmanagement?
Consequencesofuntreated/unmanagedacutepainforthepatient:•Autonomicchanges•Endocrinologicalchanges:increasedcortisol,insulinresistance,etc.•Psychologicaldistress•Developmentofchronicpain—>alloftheabove
1. Managepain2. Preventchronification
7
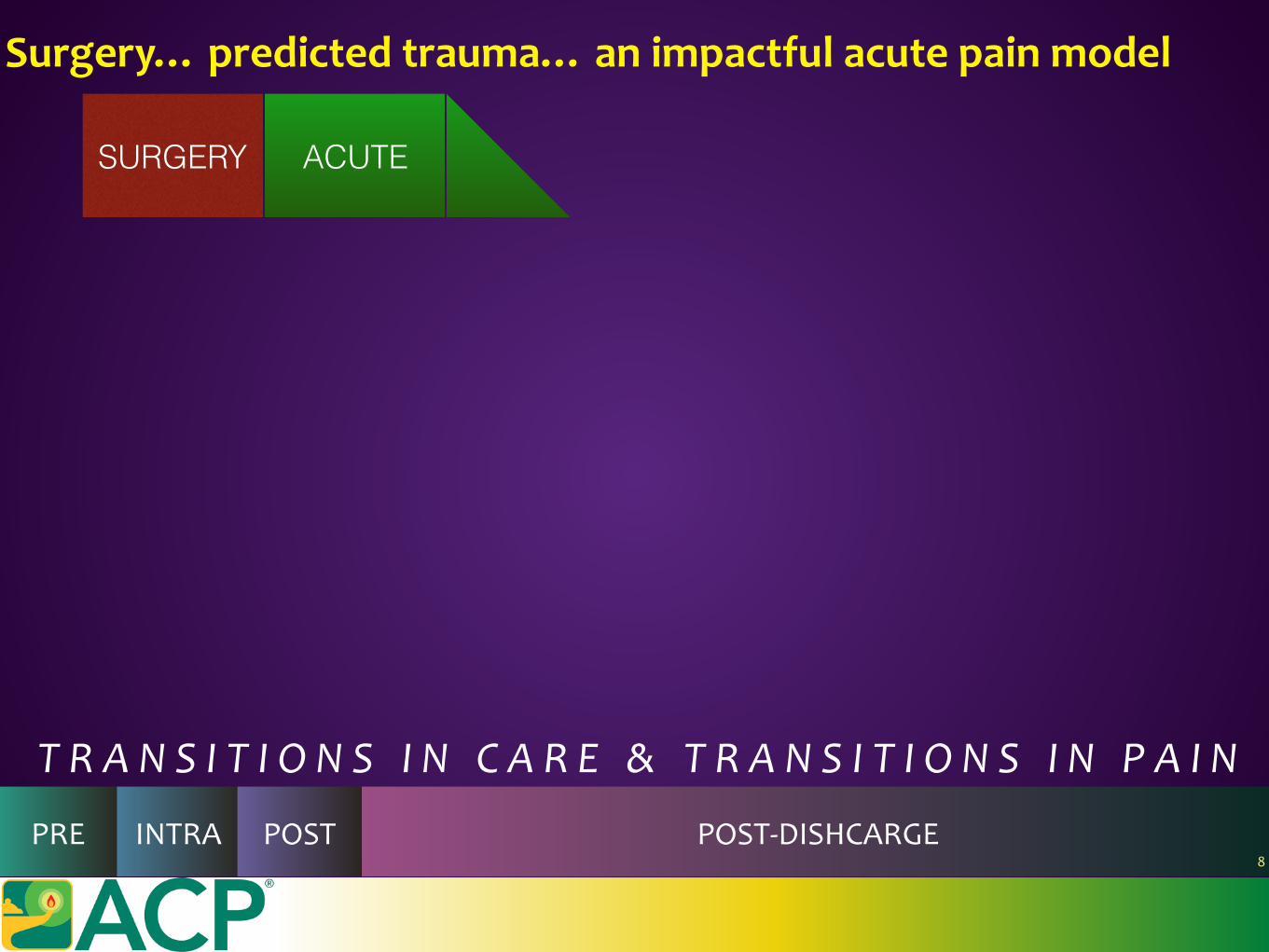
Surgery…predictedtrauma…animpactfulacutepainmodel
SURGERY ACUTE
TRANSITIONSINCARE&TRANSITIONSINPAIN
PRE INTRA POST POST-DISHCARGE8
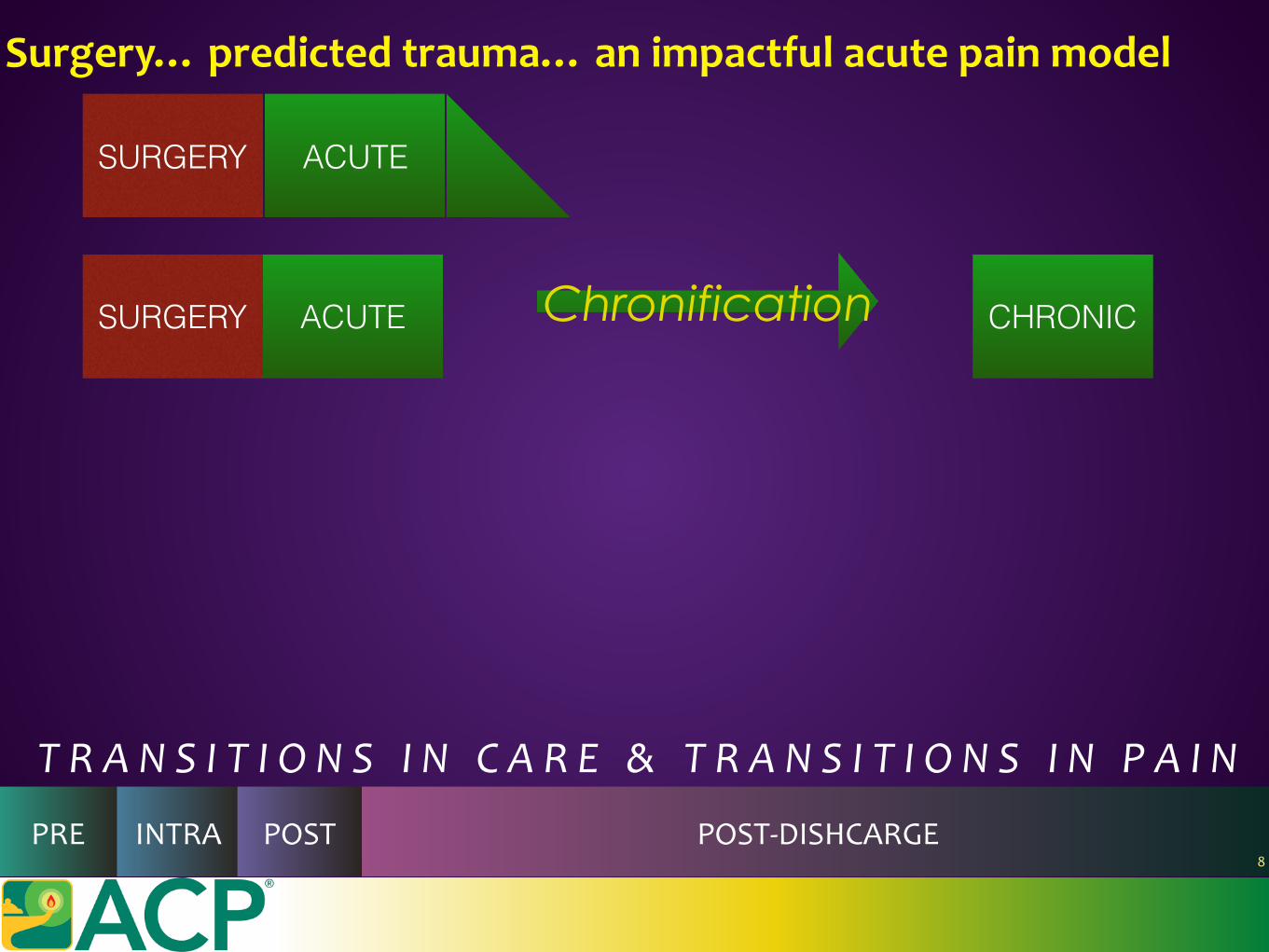
Surgery…predictedtrauma…animpactfulacutepainmodel
ACUTE CHRONICChronificationSURGERY
SURGERY ACUTE
TRANSITIONSINCARE&TRANSITIONSINPAIN
PRE INTRA POST POST-DISHCARGE8
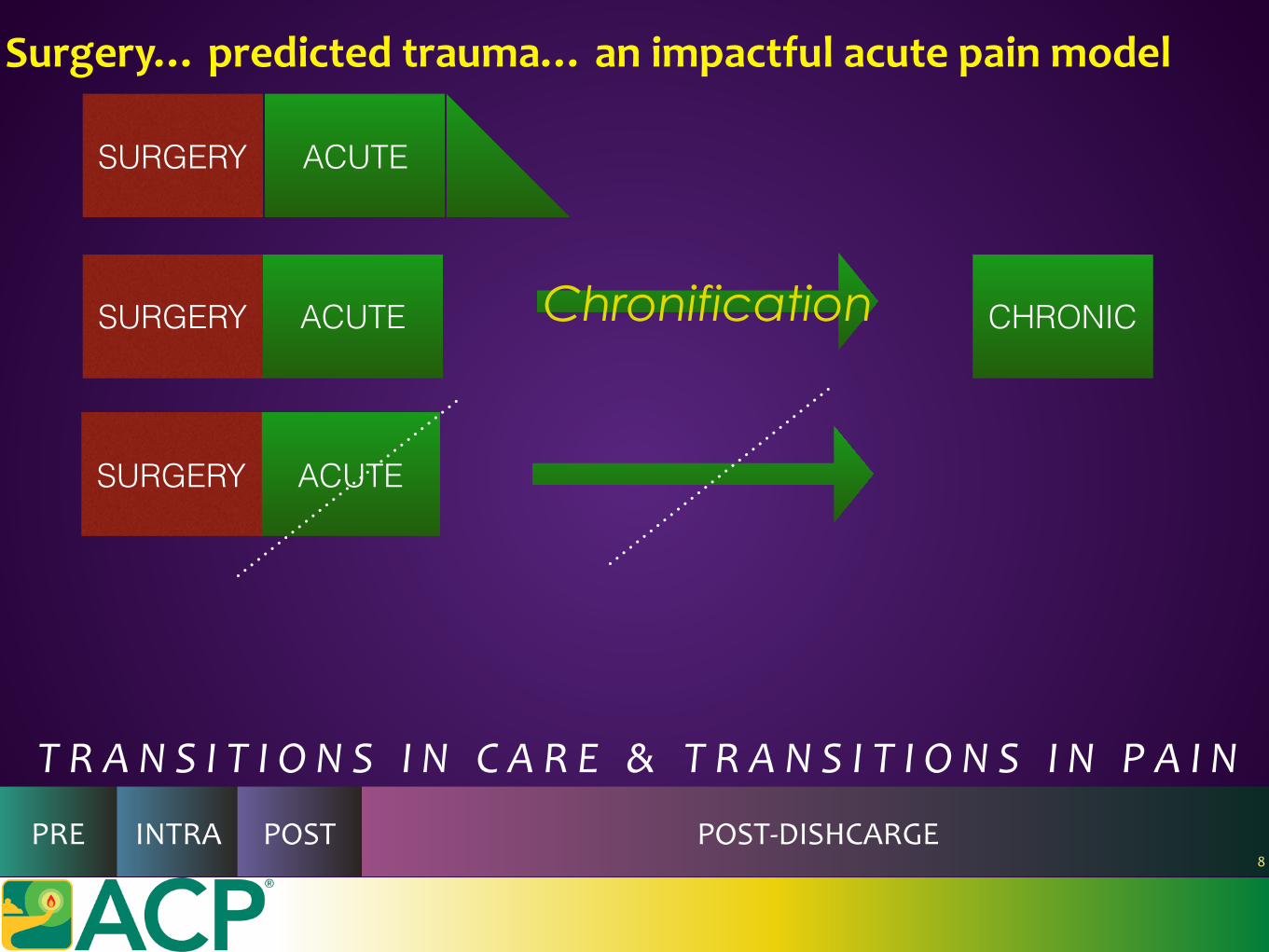
Surgery…predictedtrauma…animpactfulacutepainmodel
ACUTE CHRONICChronificationSURGERY
ACUTESURGERY
SURGERY ACUTE
TRANSITIONSINCARE&TRANSITIONSINPAIN
PRE INTRA POST POST-DISHCARGE8
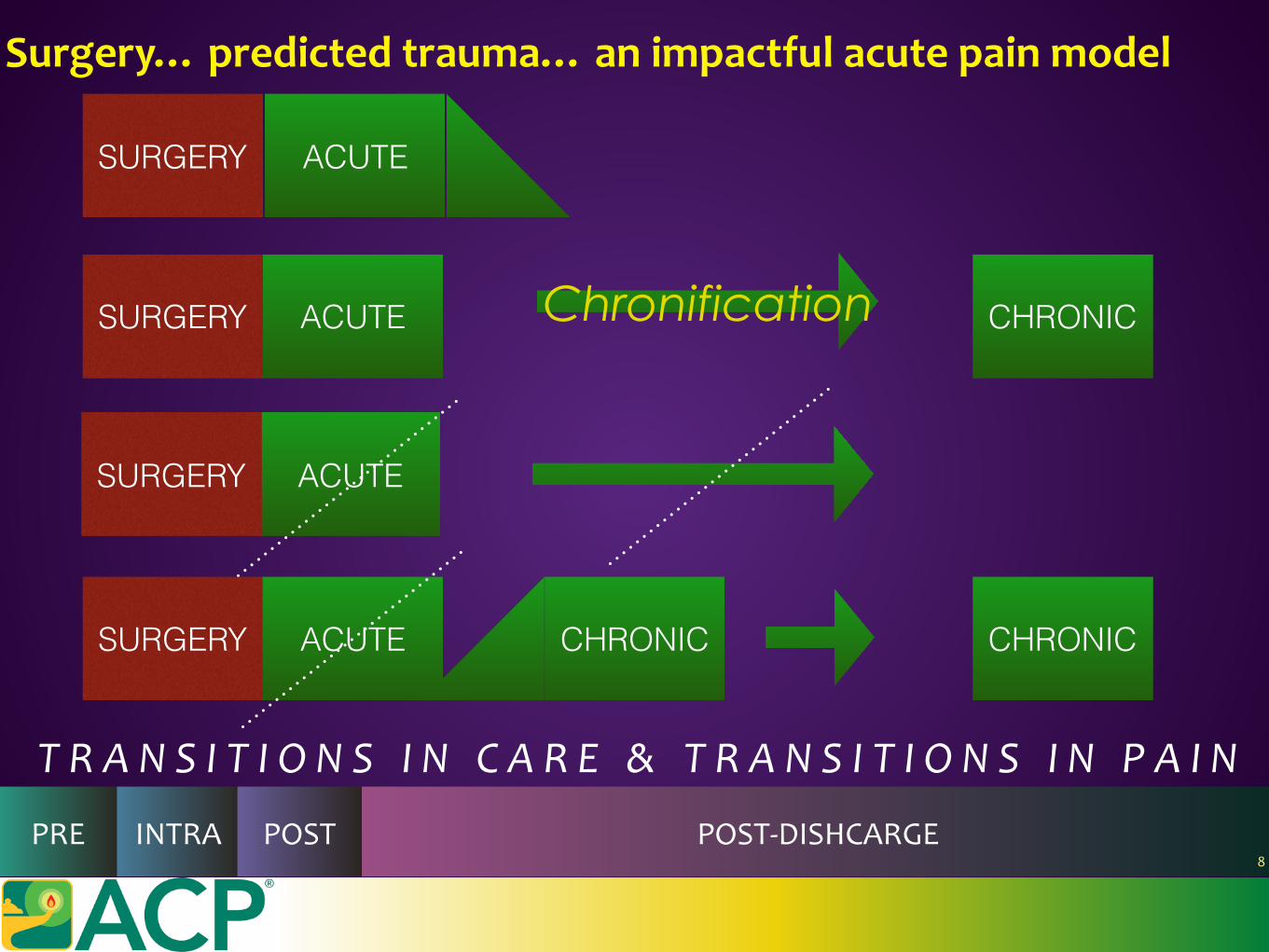
Surgery…predictedtrauma…animpactfulacutepainmodel
ACUTE CHRONICChronificationSURGERY
ACUTESURGERY
SURGERY ACUTE
CHRONICSURGERY CHRONICACUTE
TRANSITIONSINCARE&TRANSITIONSINPAIN
PRE INTRA POST POST-DISHCARGE8
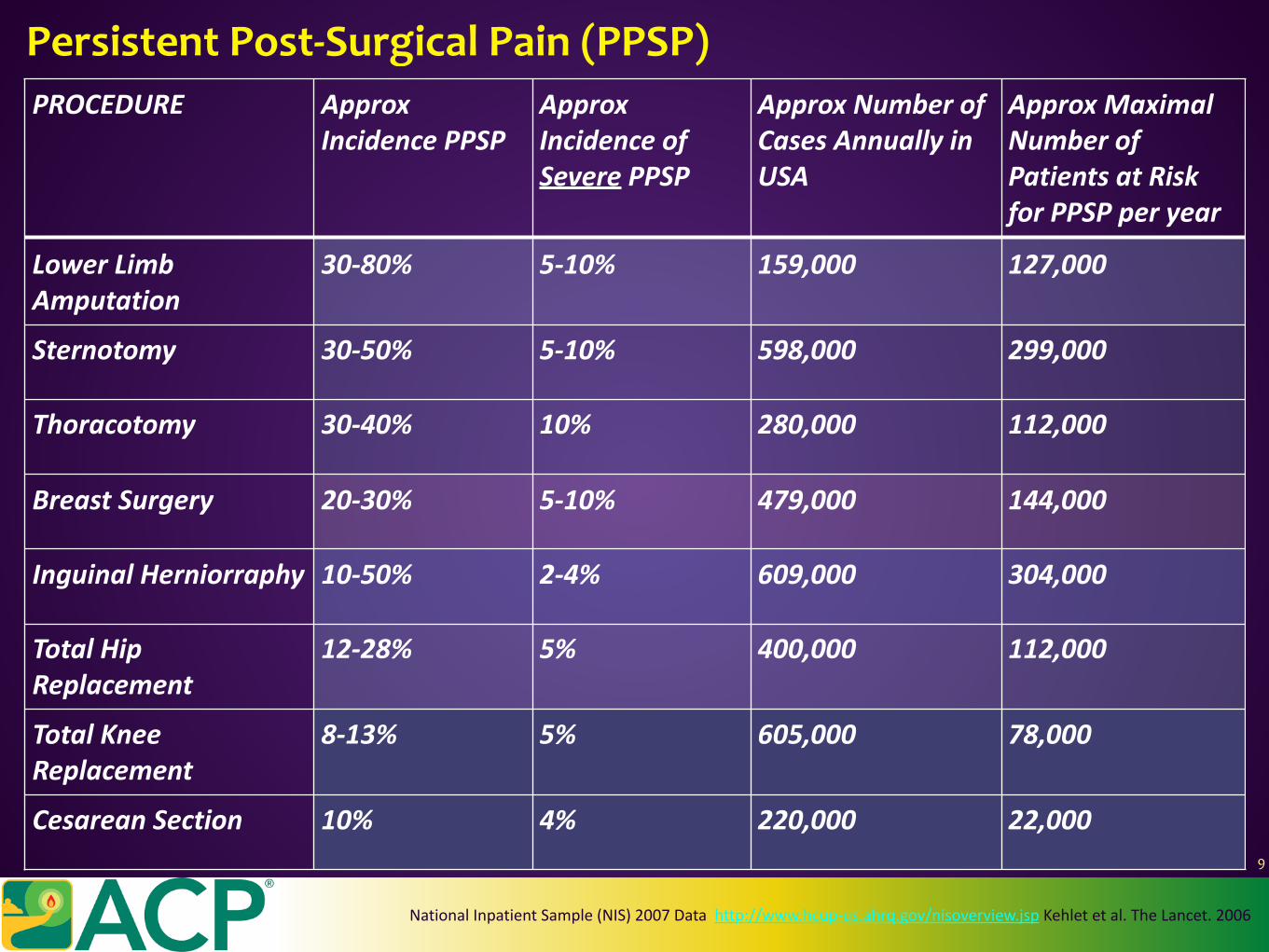
PROCEDURE ApproxIncidencePPSP
ApproxIncidenceofSeverePPSP
ApproxNumberofCasesAnnuallyinUSA
ApproxMaximalNumberofPatientsatRiskforPPSPperyear
LowerLimbAmputation
30-80% 5-10% 159,000 127,000
Sternotomy 30-50% 5-10% 598,000 299,000
Thoracotomy 30-40% 10% 280,000 112,000
BreastSurgery 20-30% 5-10% 479,000 144,000
InguinalHerniorraphy 10-50% 2-4% 609,000 304,000
TotalHipReplacement
12-28% 5% 400,000 112,000
TotalKneeReplacement
8-13% 5% 605,000 78,000
CesareanSection 10% 4% 220,000 22,000
PersistentPost-SurgicalPain(PPSP)
NationalInpatientSample(NIS)2007Datahttp://www.hcup-us.ahrq.gov/nisoverview.jspKehletetal.TheLancet.2006
9
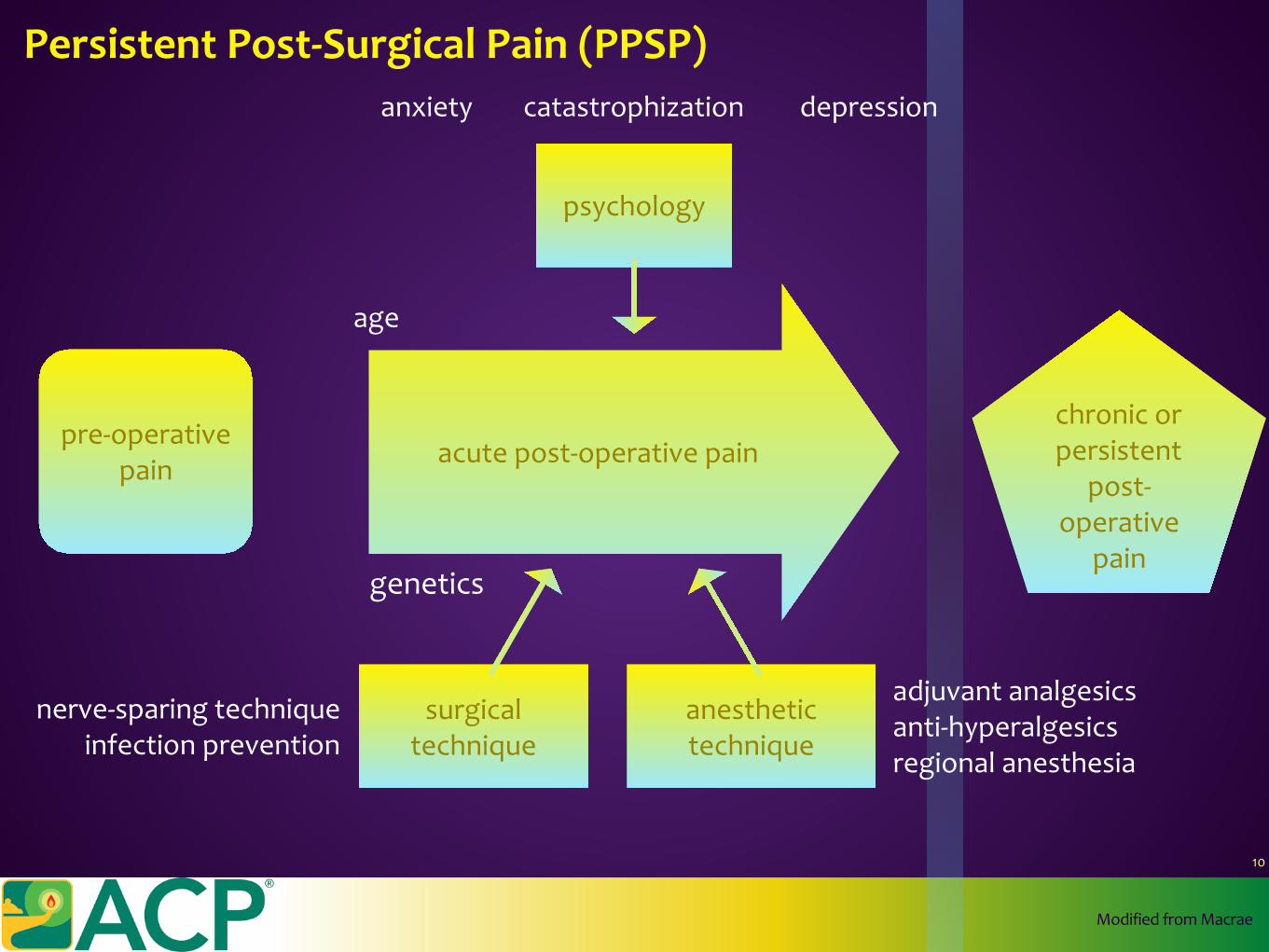
acutepost-operativepainpre-operative
pain
chronicorpersistent
post-operative
pain
surgicaltechnique
anesthetictechnique
psychology
genetics
age
adjuvantanalgesicsanti-hyperalgesicsregionalanesthesia
nerve-sparingtechniqueinfectionprevention
anxiety depressioncatastrophization
ModifiedfromMacrae
PersistentPost-SurgicalPain(PPSP)
10
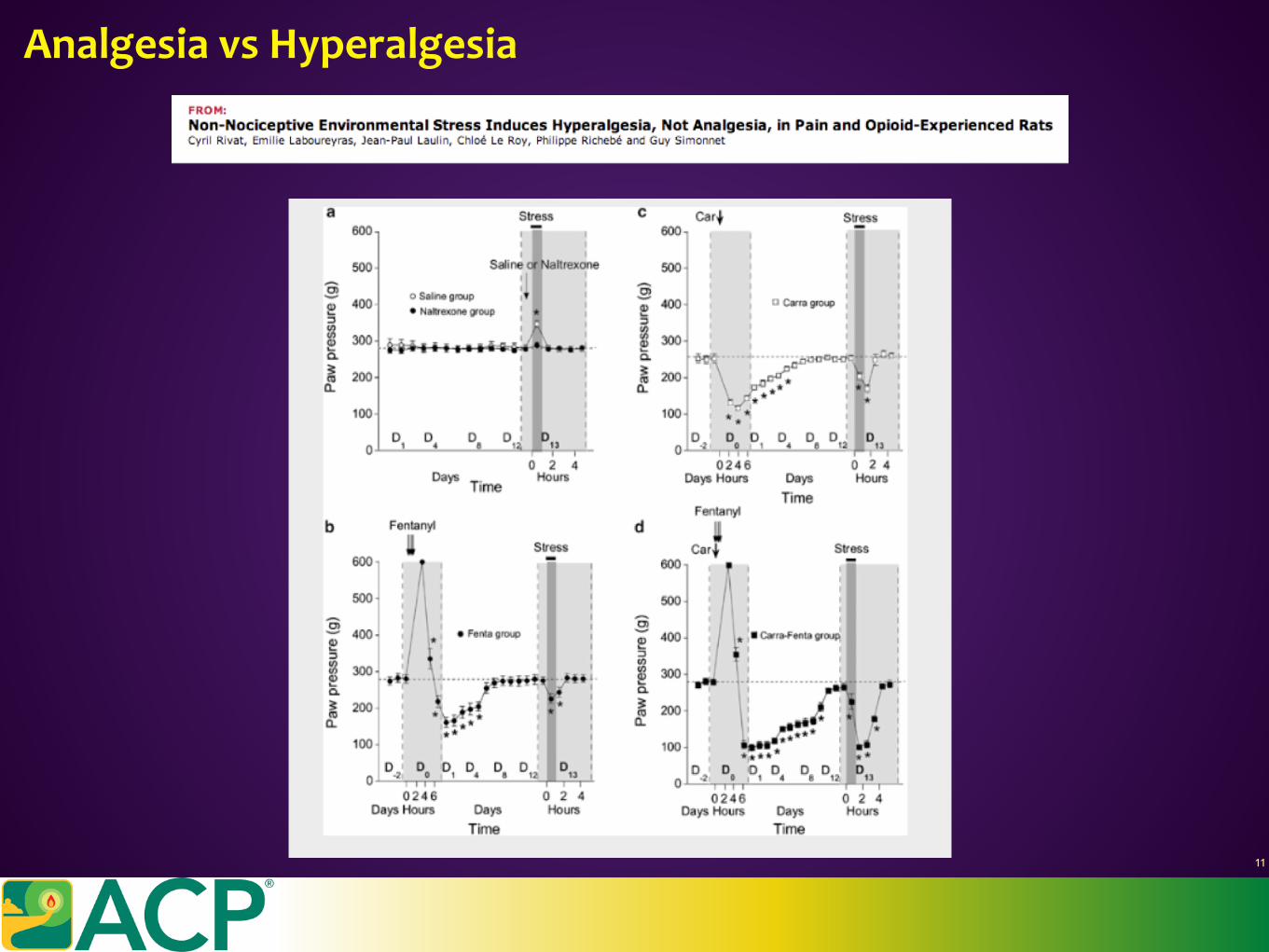
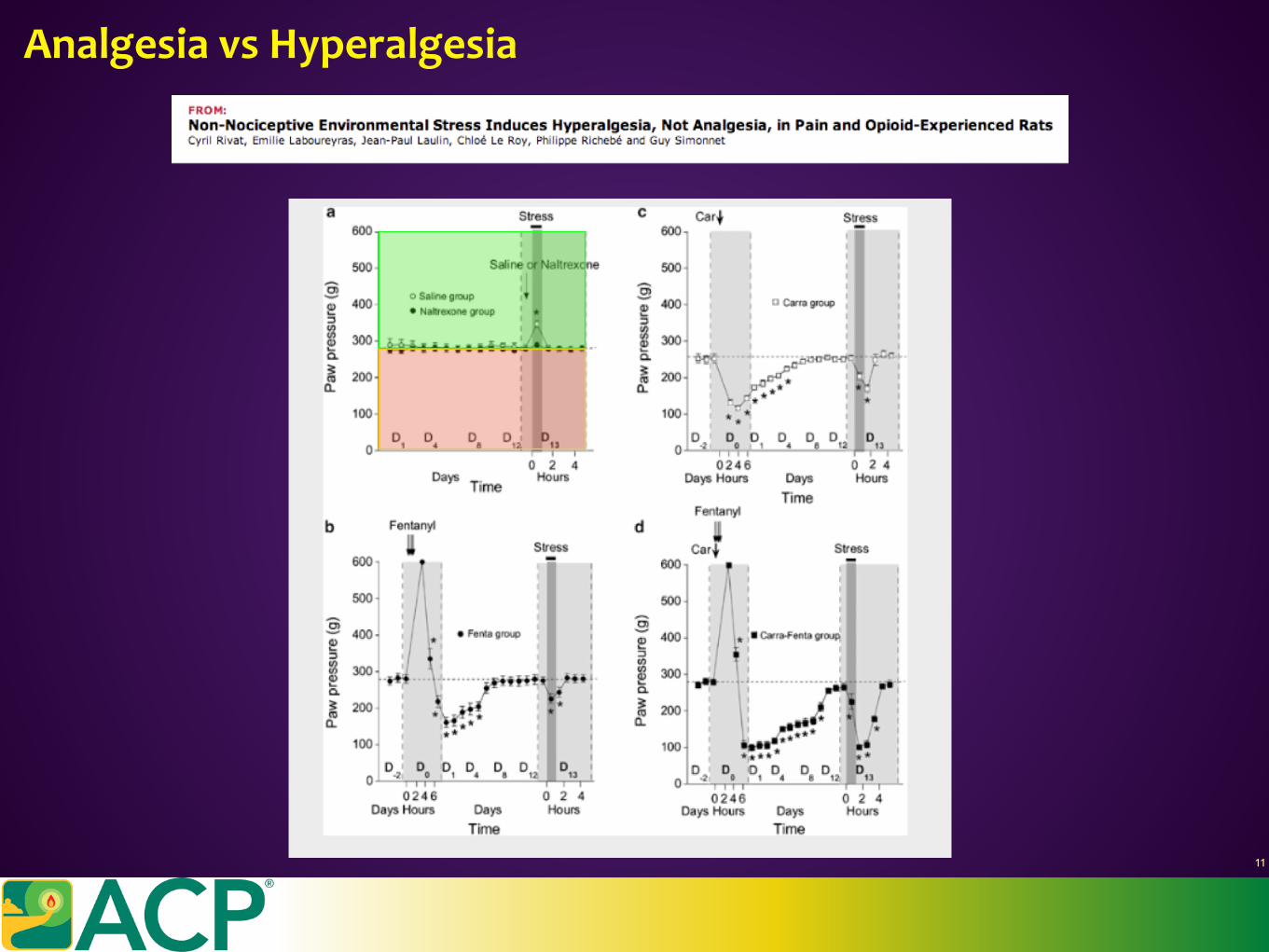
AnalgesiavsHyperalgesia
11
AnalgesiavsHyperalgesia
11
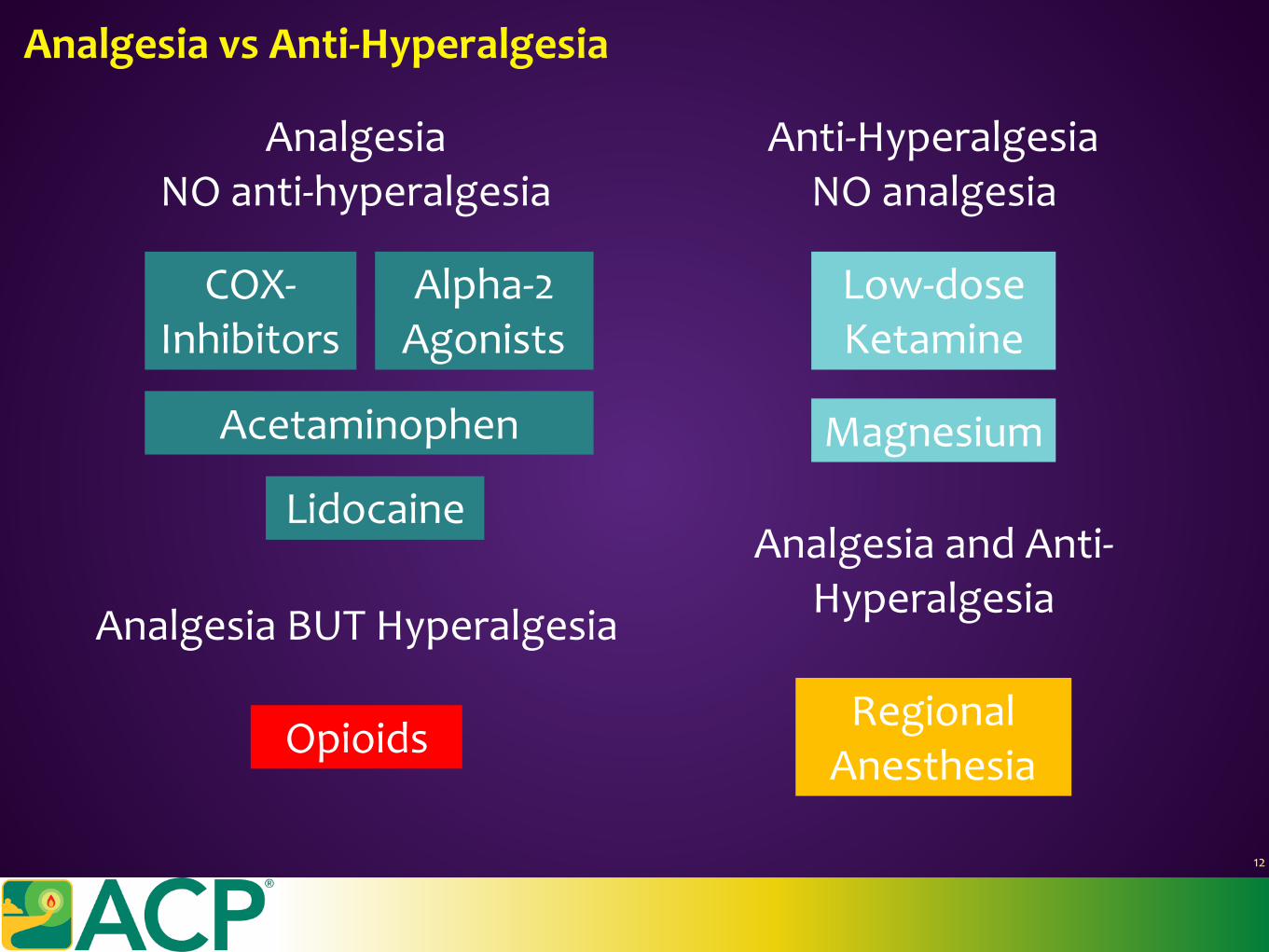
COX-Inhibitors
Acetaminophen
Alpha-2Agonists
Lidocaine
Low-doseKetamine
Magnesium
AnalgesiaNOanti-hyperalgesia
AnalgesiaBUTHyperalgesia
Opioids
Anti-HyperalgesiaNOanalgesia
RegionalAnesthesia
AnalgesiaandAnti-Hyperalgesia
AnalgesiavsAnti-Hyperalgesia
12
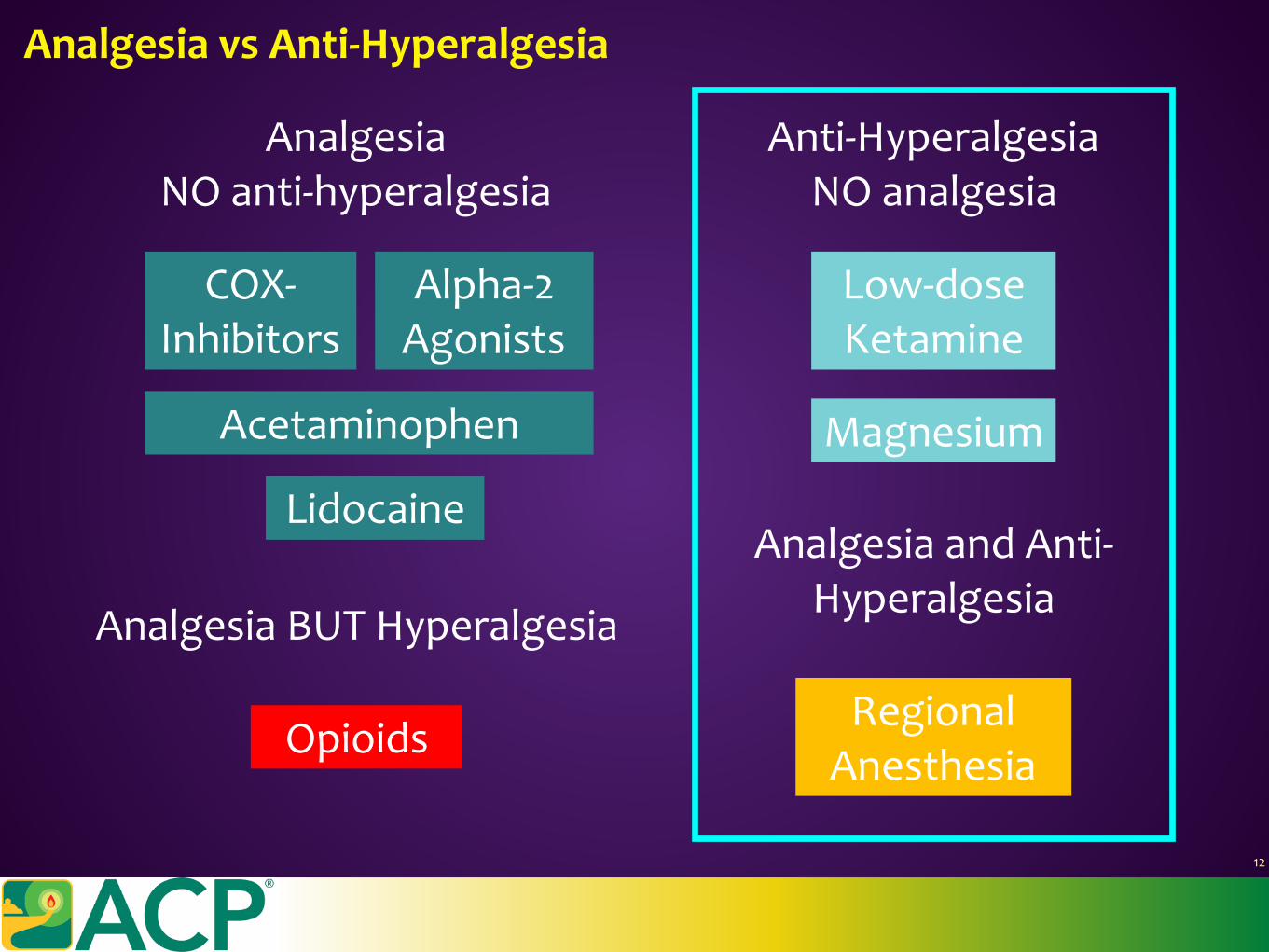
COX-Inhibitors
Acetaminophen
Alpha-2Agonists
Lidocaine
Low-doseKetamine
Magnesium
AnalgesiaNOanti-hyperalgesia
AnalgesiaBUTHyperalgesia
Opioids
Anti-HyperalgesiaNOanalgesia
RegionalAnesthesia
AnalgesiaandAnti-Hyperalgesia
AnalgesiavsAnti-Hyperalgesia
12
Themanagementofpainmustinvolvebothanalgesiaandanti-hyperalgesia
Analgesiawilladdressacutephysiologicalandpsychologicaladverseeffects.
Anti-hyperalgesiawilladdressthechronificationofpainandtheresultantlongdurationofphysiologicalandpsychologicaladverseeffects.
Pearl:AnalgesiavsAnti-Hyperalgesia
13
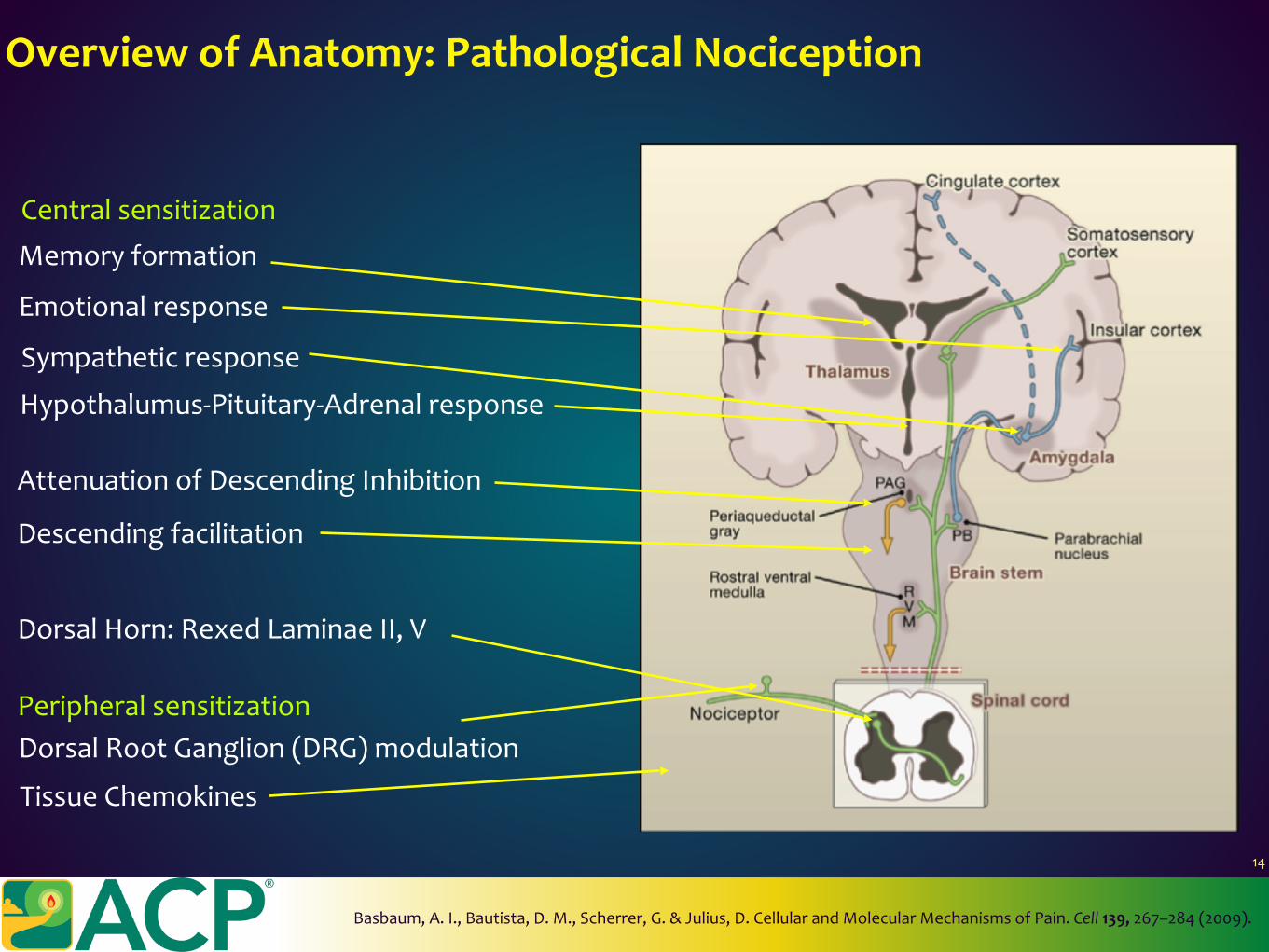
OverviewofAnatomy:PathologicalNociception
PeripheralsensitizationDorsalRootGanglion(DRG)modulation
DorsalHorn:RexedLaminaeII,V
Descendingfacilitation
AttenuationofDescendingInhibition
Sympatheticresponse
Emotionalresponse
Memoryformation
TissueChemokines
Centralsensitization
Hypothalumus-Pituitary-Adrenalresponse
14
Basbaum,A.I.,Bautista,D.M.,Scherrer,G.&Julius,D.CellularandMolecularMechanismsofPain.Cell139,267–284(2009).
BiologicalPharmacologics:Opioids
15
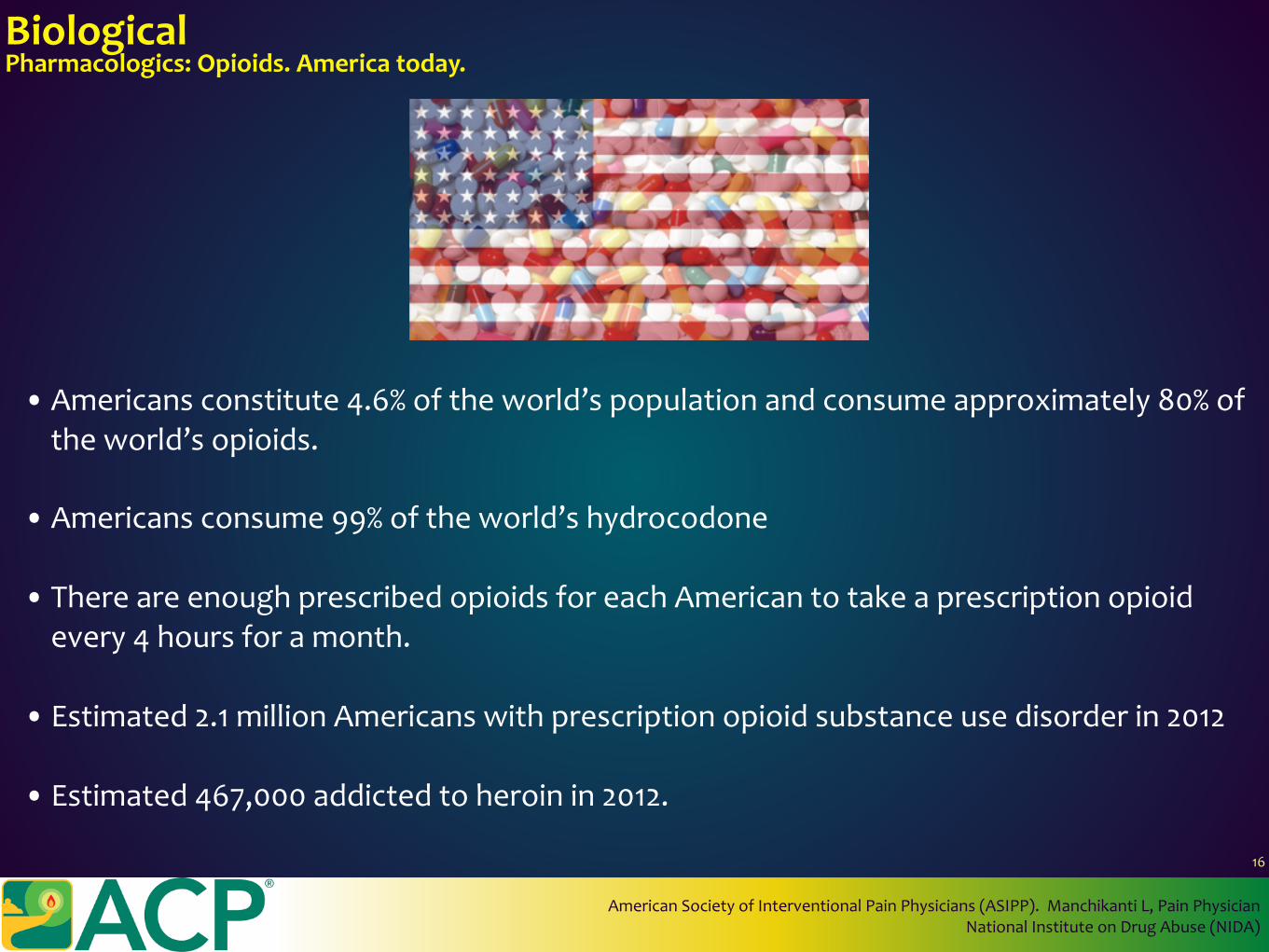
BiologicalPharmacologics:Opioids.Americatoday.
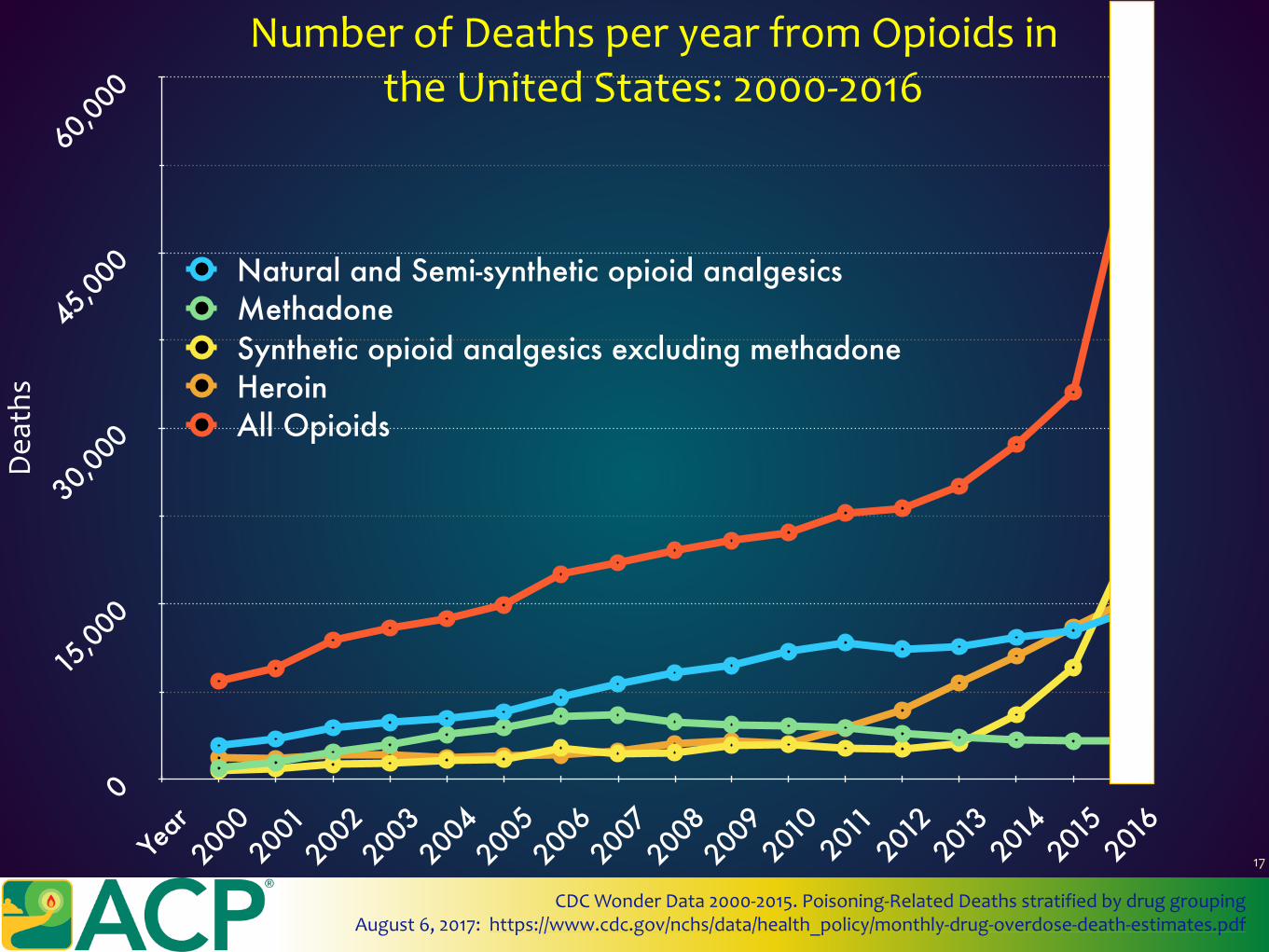
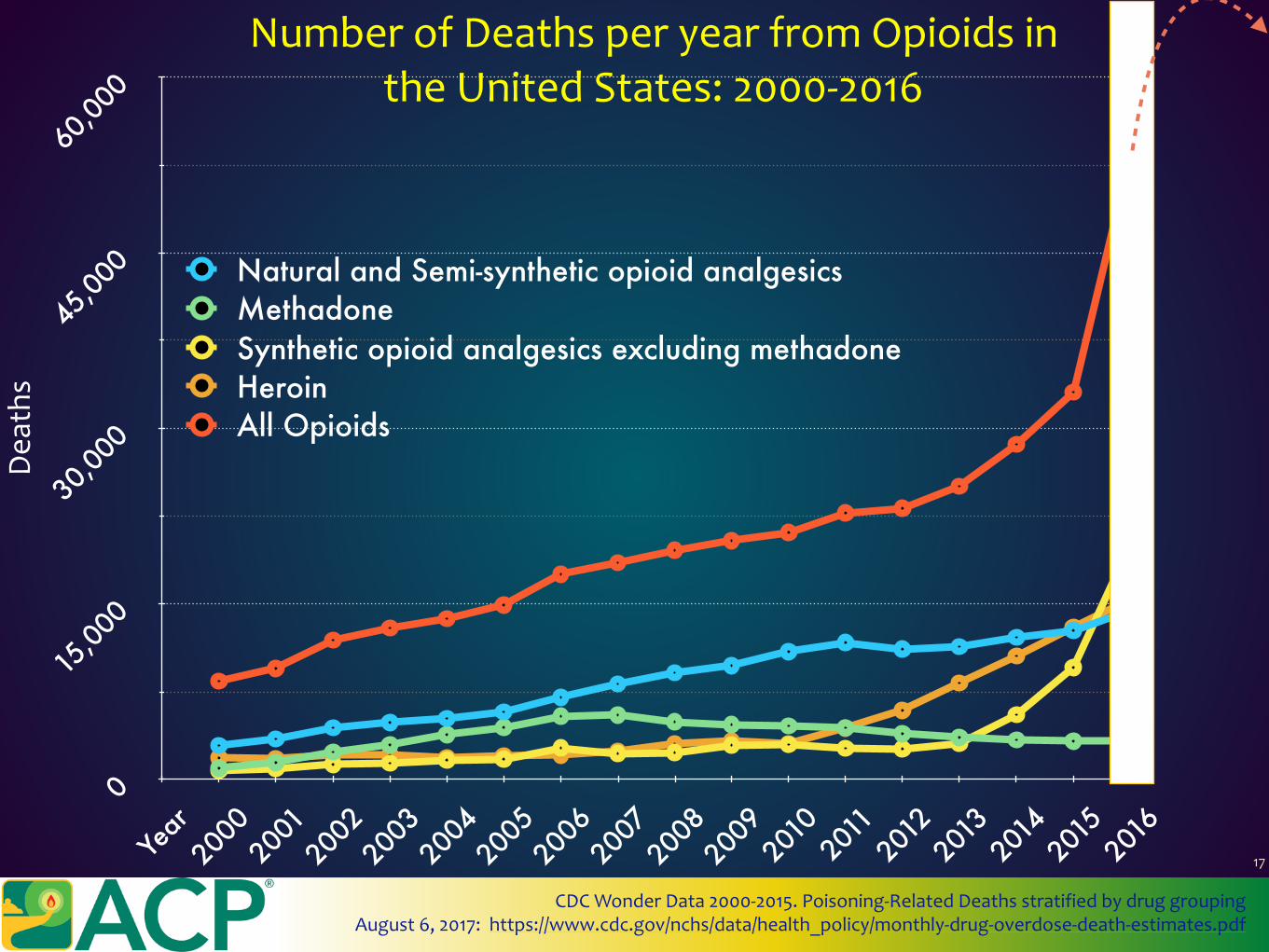
•Americansconstitute4.6%oftheworld’spopulationandconsumeapproximately80%oftheworld’sopioids.
• Americansconsume99%oftheworld’shydrocodone
• ThereareenoughprescribedopioidsforeachAmericantotakeaprescriptionopioidevery4hoursforamonth.
• Estimated2.1millionAmericanswithprescriptionopioidsubstanceusedisorderin2012
• Estimated467,000addictedtoheroinin2012.
AmericanSocietyofInterventionalPainPhysicians(ASIPP).ManchikantiL,PainPhysicianNationalInstituteonDrugAbuse(NIDA)
16
0
15,00
0
30,00
0
45,00
0
60,00
0
Year
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
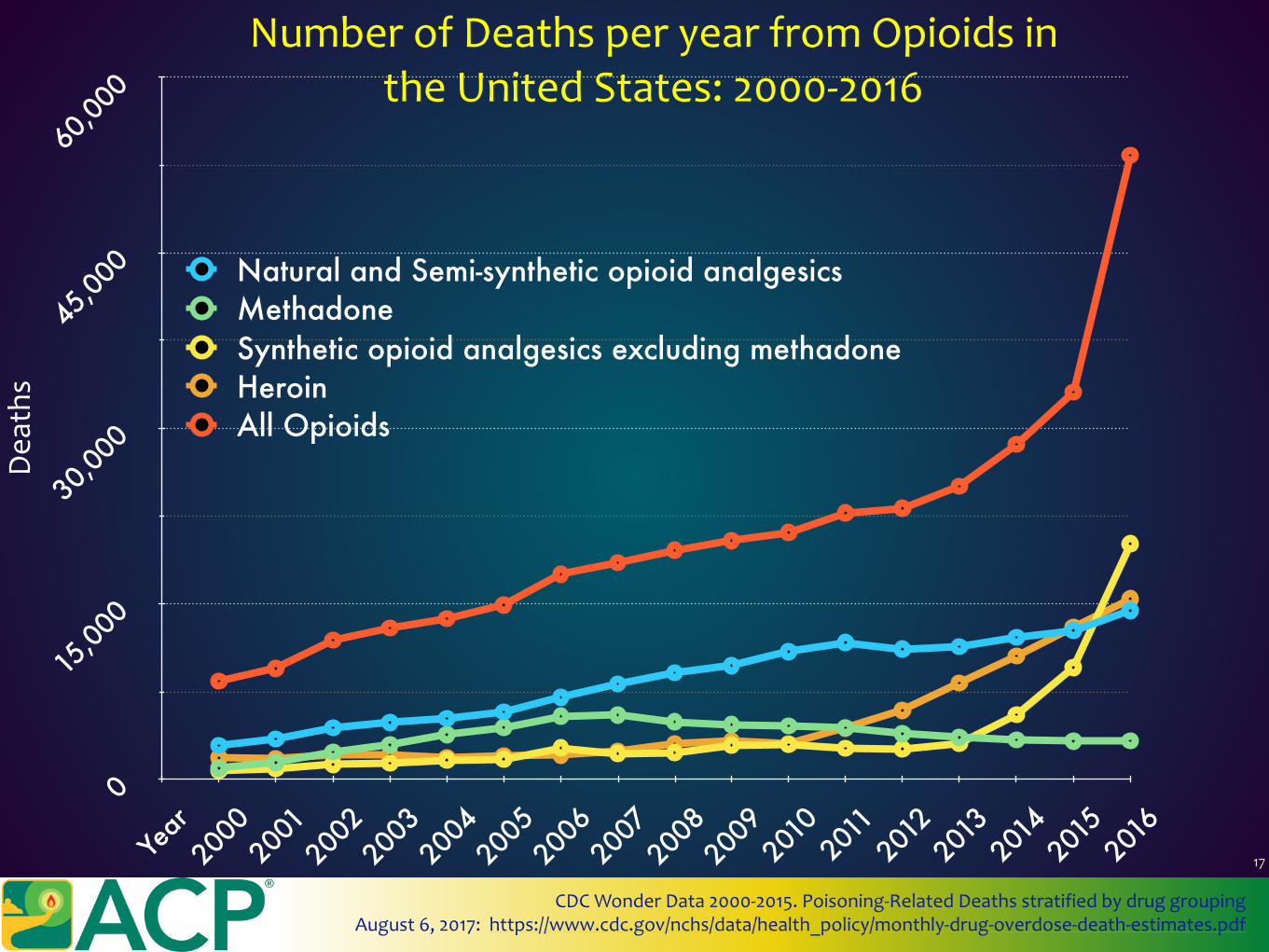
Natural and Semi-synthetic opioid analgesicsMethadoneSynthetic opioid analgesics excluding methadoneHeroinAll Opioids
NumberofDeathsperyearfromOpioidsintheUnitedStates:2000-2016
Dea
ths
CDCWonderData2000-2015.Poisoning-RelatedDeathsstratifiedbydruggroupingAugust6,2017:https://www.cdc.gov/nchs/data/health_policy/monthly-drug-overdose-death-estimates.pdf
17
0
15,00
0
30,00
0
45,00
0
60,00
0
Year
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
Natural and Semi-synthetic opioid analgesicsMethadoneSynthetic opioid analgesics excluding methadoneHeroinAll Opioids
NumberofDeathsperyearfromOpioidsintheUnitedStates:2000-2016
Dea
ths
CDCWonderData2000-2015.Poisoning-RelatedDeathsstratifiedbydruggroupingAugust6,2017:https://www.cdc.gov/nchs/data/health_policy/monthly-drug-overdose-death-estimates.pdf
17
0
15,00
0
30,00
0
45,00
0
60,00
0
Year
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
Natural and Semi-synthetic opioid analgesicsMethadoneSynthetic opioid analgesics excluding methadoneHeroinAll Opioids
NumberofDeathsperyearfromOpioidsintheUnitedStates:2000-2016
Dea
ths
CDCWonderData2000-2015.Poisoning-RelatedDeathsstratifiedbydruggroupingAugust6,2017:https://www.cdc.gov/nchs/data/health_policy/monthly-drug-overdose-death-estimates.pdf
17
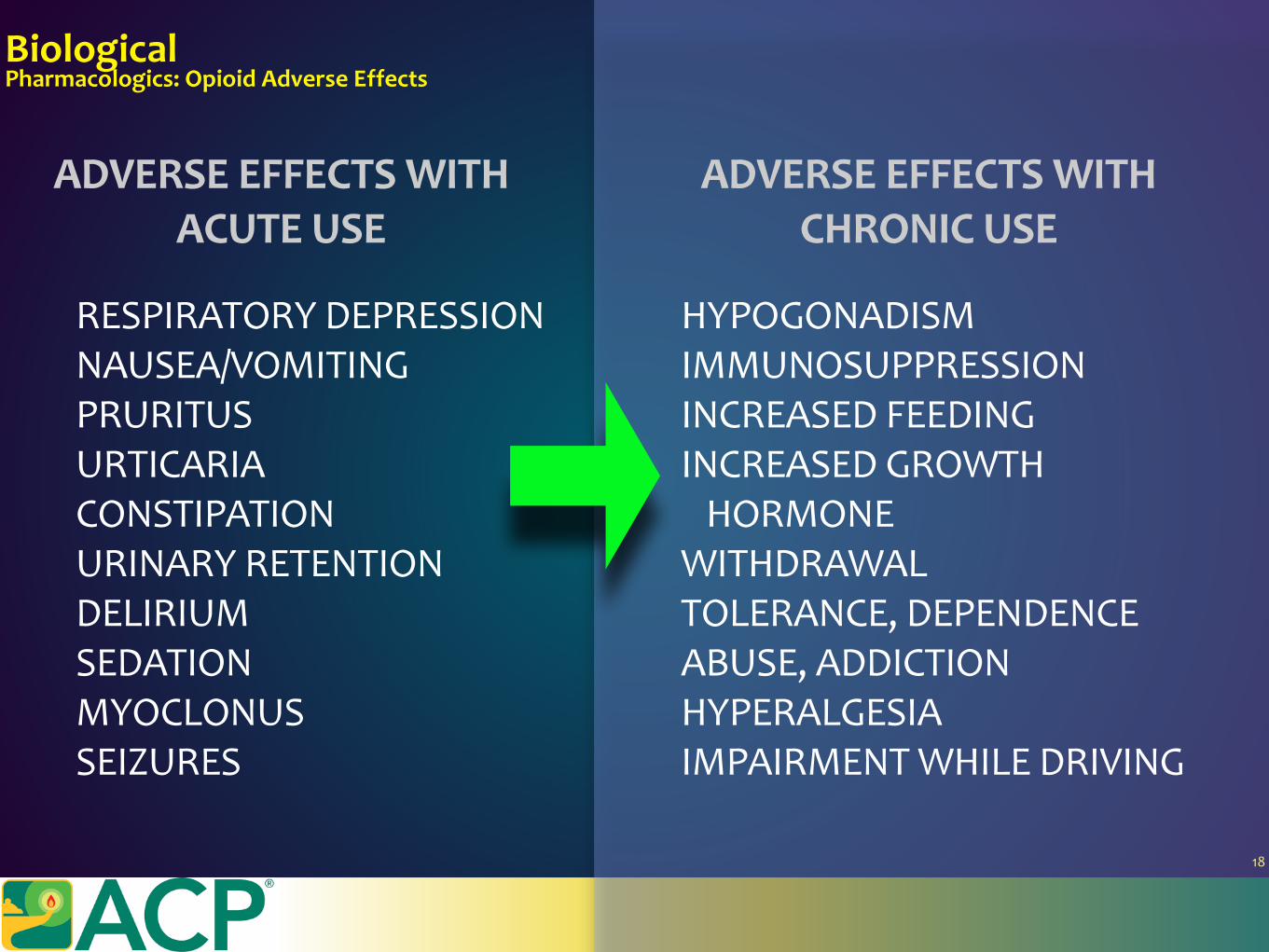
BiologicalPharmacologics:OpioidAdverseEffects
HYPOGONADISMIMMUNOSUPPRESSIONINCREASEDFEEDINGINCREASEDGROWTHHORMONEWITHDRAWALTOLERANCE,DEPENDENCEABUSE,ADDICTIONHYPERALGESIAIMPAIRMENTWHILEDRIVING
RESPIRATORYDEPRESSIONNAUSEA/VOMITINGPRURITUSURTICARIACONSTIPATIONURINARYRETENTIONDELIRIUMSEDATIONMYOCLONUSSEIZURES
ADVERSEEFFECTSWITHCHRONICUSE
ADVERSEEFFECTSWITHACUTEUSE
18
BiologicalPharmacologics:OpioidAdverseEffects
HYPOGONADISMIMMUNOSUPPRESSIONINCREASEDFEEDINGINCREASEDGROWTHHORMONEWITHDRAWALTOLERANCE,DEPENDENCEABUSE,ADDICTIONHYPERALGESIAIMPAIRMENTWHILEDRIVING
RESPIRATORYDEPRESSIONNAUSEA/VOMITINGPRURITUSURTICARIACONSTIPATIONURINARYRETENTIONDELIRIUMSEDATIONMYOCLONUSSEIZURES
ADVERSEEFFECTSWITHCHRONICUSE
ADVERSEEFFECTSWITHACUTEUSE
18
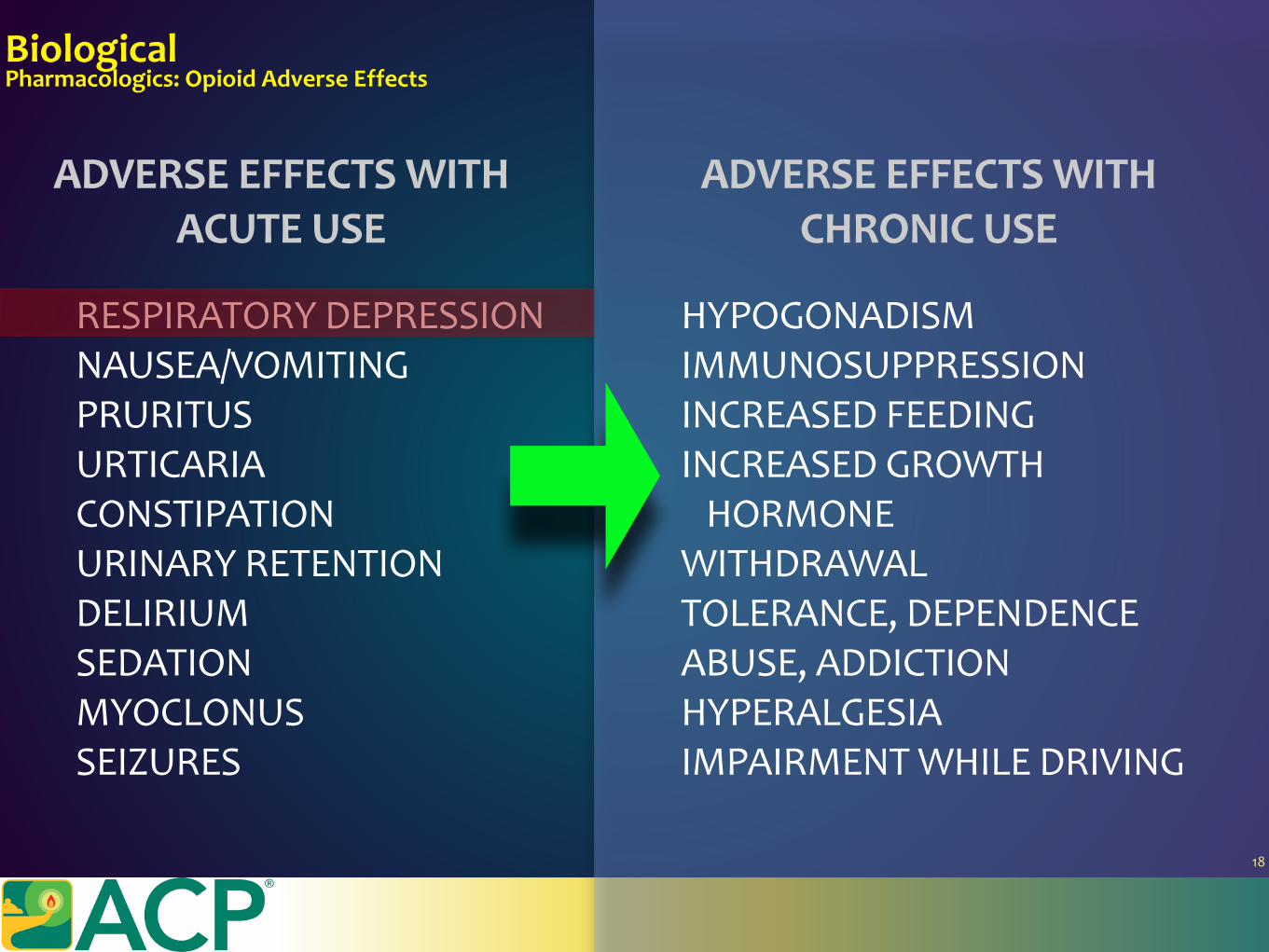
BiologicalPharmacologics:OpioidAdverseEffects
HYPOGONADISMIMMUNOSUPPRESSIONINCREASEDFEEDINGINCREASEDGROWTHHORMONEWITHDRAWALTOLERANCE,DEPENDENCEABUSE,ADDICTIONHYPERALGESIAIMPAIRMENTWHILEDRIVING
RESPIRATORYDEPRESSIONNAUSEA/VOMITINGPRURITUSURTICARIACONSTIPATIONURINARYRETENTIONDELIRIUMSEDATIONMYOCLONUSSEIZURES
ADVERSEEFFECTSWITHCHRONICUSE
ADVERSEEFFECTSWITHACUTEUSE
Tracknaloxonerespiratorydepressioneventdataatyour
institutionasaqualitymeasure
18
BiologicalPharmacologics:OpioidAdverseEffects
HYPOGONADISMIMMUNOSUPPRESSIONINCREASEDFEEDINGINCREASEDGROWTHHORMONEWITHDRAWALTOLERANCE,DEPENDENCEABUSE,ADDICTIONHYPERALGESIAIMPAIRMENTWHILEDRIVING
RESPIRATORYDEPRESSIONNAUSEA/VOMITINGPRURITUSURTICARIACONSTIPATIONURINARYRETENTIONDELIRIUMSEDATIONMYOCLONUSSEIZURES
ADVERSEEFFECTSWITHCHRONICUSE
ADVERSEEFFECTSWITHACUTEUSE
Tracknaloxonerespiratorydepressioneventdataatyour
institutionasaqualitymeasure
18
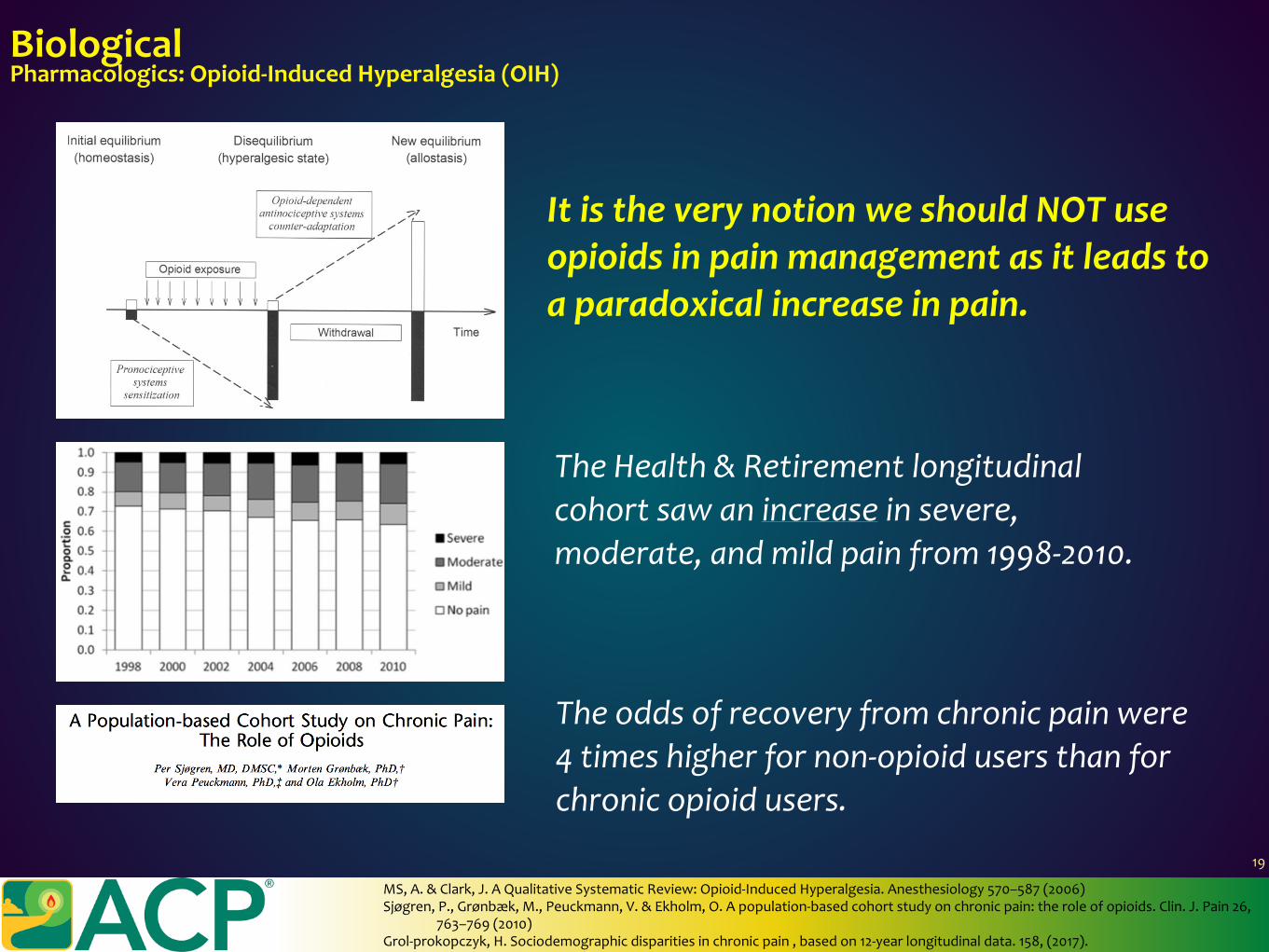
BiologicalPharmacologics:Opioid-InducedHyperalgesia(OIH)
ItistheverynotionweshouldNOTuseopioidsinpainmanagementasitleadstoaparadoxicalincreaseinpain.
TheHealth&Retirementlongitudinalcohortsawanincreaseinsevere,moderate,andmildpainfrom1998-2010.
Theoddsofrecoveryfromchronicpainwere4timeshigherfornon-opioidusersthanforchronicopioidusers.
MS,A.&Clark,J.AQualitativeSystematicReview:Opioid-InducedHyperalgesia.Anesthesiology570–587(2006)Sjøgren,P.,Grønbæk,M.,Peuckmann,V.&Ekholm,O.Apopulation-basedcohortstudyonchronicpain:theroleofopioids.Clin.J.Pain26,
763–769(2010)Grol-prokopczyk,H.Sociodemographicdisparitiesinchronicpain,basedon12-yearlongitudinaldata.158,(2017).
19
20
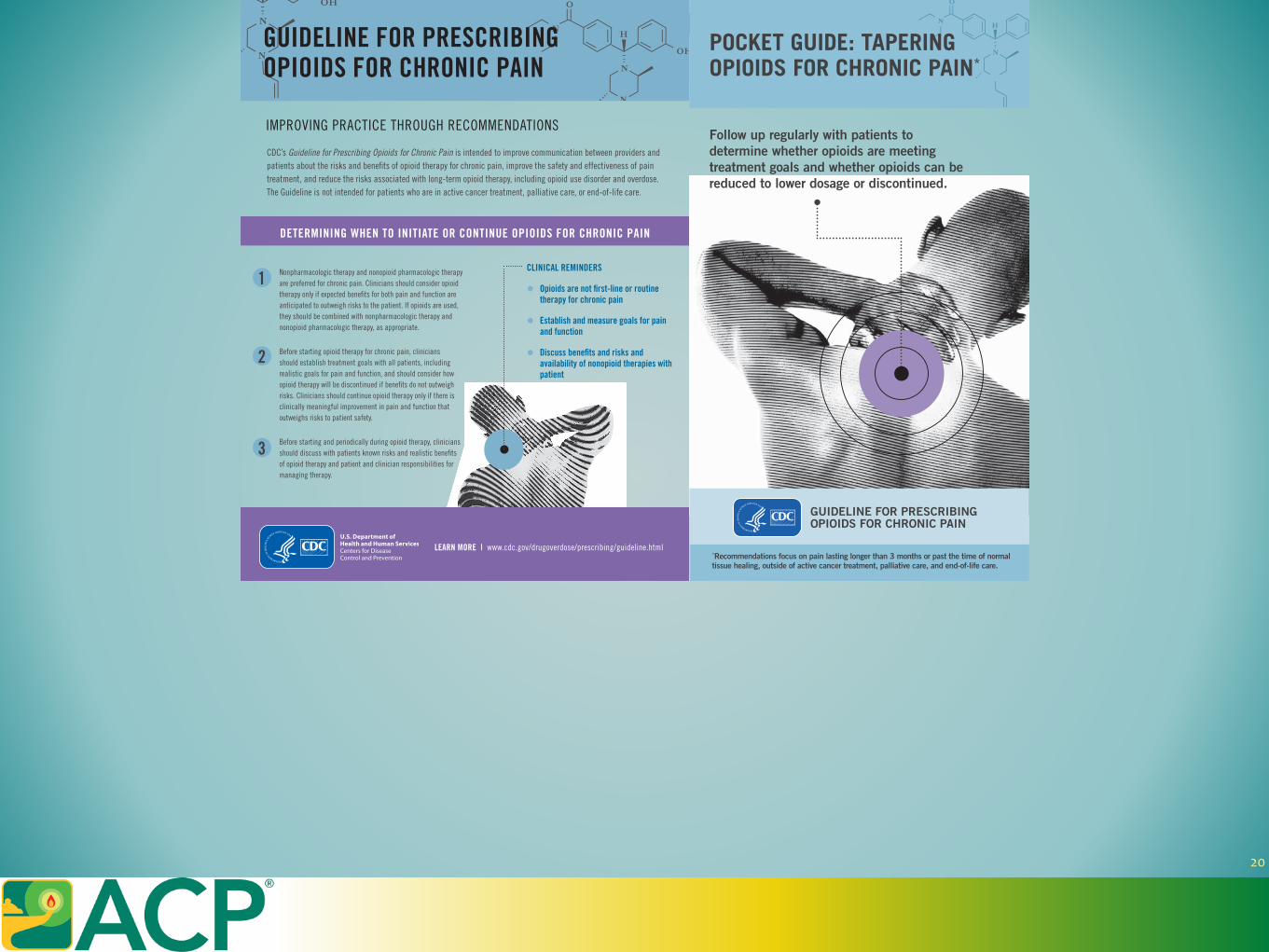
POCKET GUIDE: TAPERING OPIOIDS FOR CHRONIC PAIN*
Follow up regularly with patients to determine whether opioids are meeting treatment goals and whether opioids can be reduced to lower dosage or discontinued.
GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN
*Recommendations focus on pain lasting longer than 3 months or past the time of normal tissue healing, outside of active cancer treatment, palliative care, and end-of-life care.
1
2
3
LEARN MORE | www.cdc.gov/drugoverdose/prescribing/guideline.html
GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN
IMPROVING PRACTICE THROUGH RECOMMENDATIONS
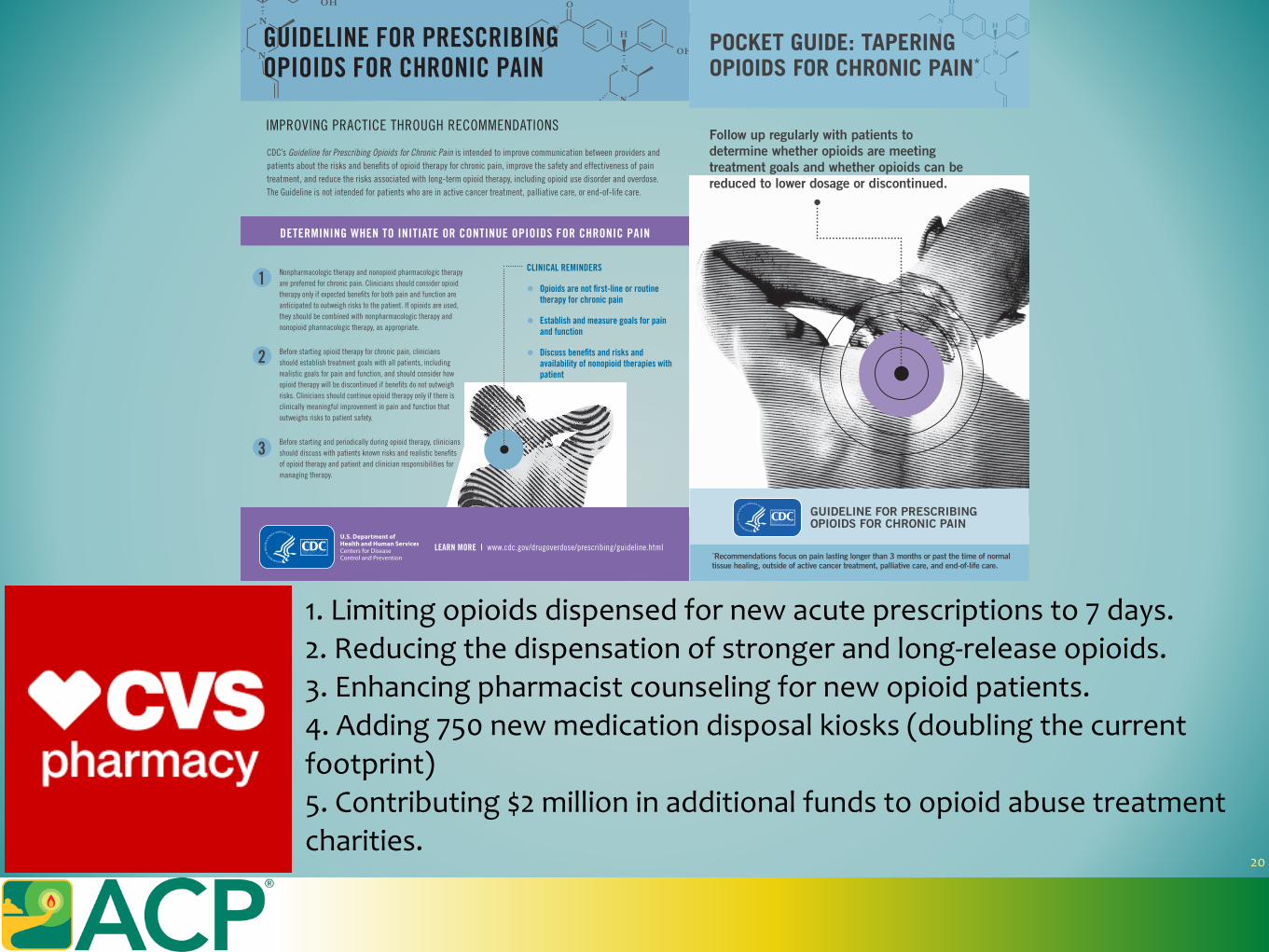
CDC’s Guideline for Prescribing Opioids for Chronic Pain is intended to improve communication between providers and patients about the risks and benefits of opioid therapy for chronic pain, improve the safety and effectiveness of pain treatment, and reduce the risks associated with long-term opioid therapy, including opioid use disorder and overdose. The Guideline is not intended for patients who are in active cancer treatment, palliative care, or end-of-life care.
DETERMINING WHEN TO INITIATE OR CONTINUE OPIOIDS FOR CHRONIC PAIN
Nonpharmacologic therapy and nonopioid pharmacologic therapy are preferred for chronic pain. Clinicians should consider opioid therapy only if expected benefits for both pain and function are anticipated to outweigh risks to the patient. If opioids are used, they should be combined with nonpharmacologic therapy and nonopioid pharmacologic therapy, as appropriate.
Before starting opioid therapy for chronic pain, clinicians should establish treatment goals with all patients, including realistic goals for pain and function, and should consider how opioid therapy will be discontinued if benefits do not outweigh risks. Clinicians should continue opioid therapy only if there is clinically meaningful improvement in pain and function that outweighs risks to patient safety.
Before starting and periodically during opioid therapy, clinicians should discuss with patients known risks and realistic benefits of opioid therapy and patient and clinician responsibilities for managing therapy.
CLINICAL REMINDERS
• Opioids are not first-line or routine therapy for chronic pain
• Establish and measure goals for pain and function
• Discuss benefits and risks and availability of nonopioid therapies with patient
20
POCKET GUIDE: TAPERING OPIOIDS FOR CHRONIC PAIN*
Follow up regularly with patients to determine whether opioids are meeting treatment goals and whether opioids can be reduced to lower dosage or discontinued.
GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN
*Recommendations focus on pain lasting longer than 3 months or past the time of normal tissue healing, outside of active cancer treatment, palliative care, and end-of-life care.
1
2
3
LEARN MORE | www.cdc.gov/drugoverdose/prescribing/guideline.html
GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN
IMPROVING PRACTICE THROUGH RECOMMENDATIONS
CDC’s Guideline for Prescribing Opioids for Chronic Pain is intended to improve communication between providers and patients about the risks and benefits of opioid therapy for chronic pain, improve the safety and effectiveness of pain treatment, and reduce the risks associated with long-term opioid therapy, including opioid use disorder and overdose. The Guideline is not intended for patients who are in active cancer treatment, palliative care, or end-of-life care.
DETERMINING WHEN TO INITIATE OR CONTINUE OPIOIDS FOR CHRONIC PAIN
Nonpharmacologic therapy and nonopioid pharmacologic therapy are preferred for chronic pain. Clinicians should consider opioid therapy only if expected benefits for both pain and function are anticipated to outweigh risks to the patient. If opioids are used, they should be combined with nonpharmacologic therapy and nonopioid pharmacologic therapy, as appropriate.
Before starting opioid therapy for chronic pain, clinicians should establish treatment goals with all patients, including realistic goals for pain and function, and should consider how opioid therapy will be discontinued if benefits do not outweigh risks. Clinicians should continue opioid therapy only if there is clinically meaningful improvement in pain and function that outweighs risks to patient safety.
Before starting and periodically during opioid therapy, clinicians should discuss with patients known risks and realistic benefits of opioid therapy and patient and clinician responsibilities for managing therapy.
CLINICAL REMINDERS
• Opioids are not first-line or routine therapy for chronic pain
• Establish and measure goals for pain and function
• Discuss benefits and risks and availability of nonopioid therapies with patient
1.Limitingopioidsdispensedfornewacuteprescriptionsto7days.2.Reducingthedispensationofstrongerandlong-releaseopioids.3.Enhancingpharmacistcounselingfornewopioidpatients.4.Adding750newmedicationdisposalkiosks(doublingthecurrentfootprint)5.Contributing$2millioninadditionalfundstoopioidabusetreatmentcharities.
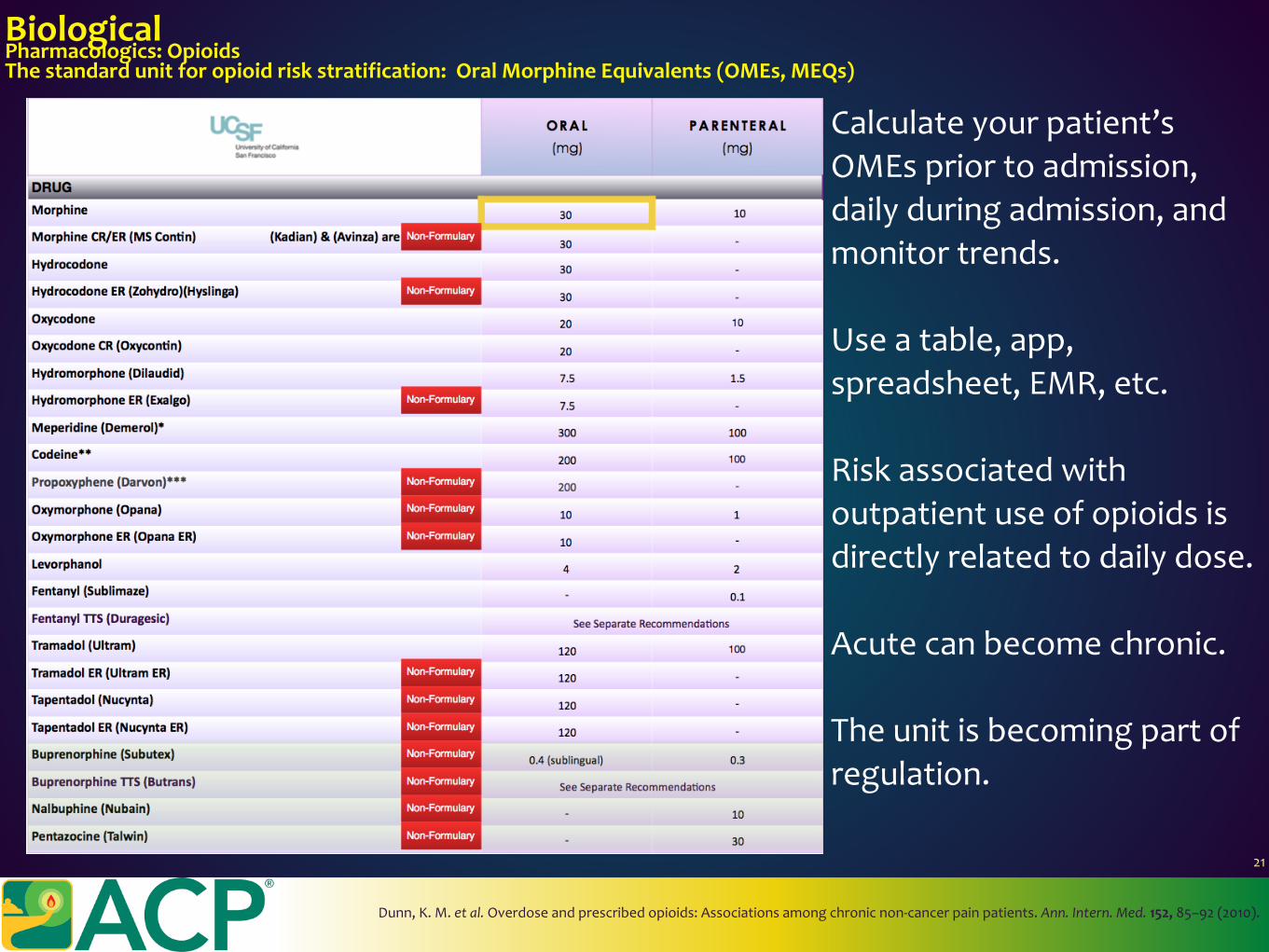
BiologicalPharmacologics:OpioidsThestandardunitforopioidriskstratification:OralMorphineEquivalents(OMEs,MEQs)
Calculateyourpatient’sOMEspriortoadmission,dailyduringadmission,andmonitortrends.
Useatable,app,spreadsheet,EMR,etc.
Riskassociatedwithoutpatientuseofopioidsisdirectlyrelatedtodailydose.
Acutecanbecomechronic.
Theunitisbecomingpartofregulation.
Dunn,K.M.etal.Overdoseandprescribedopioids :Associationsamongchronicnon-cancerpainpatients.Ann.Intern.Med.152,85–92(2010).
21
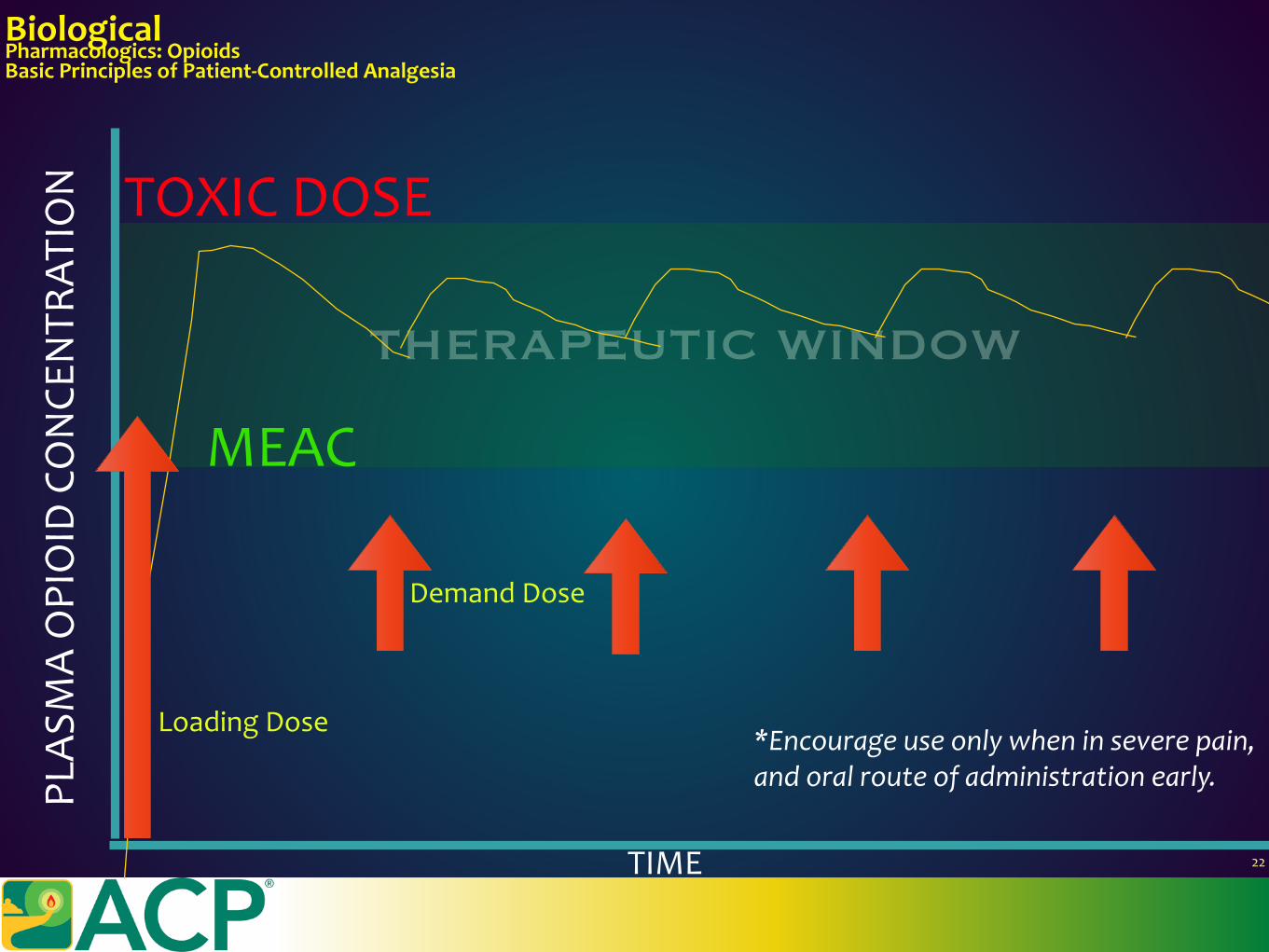
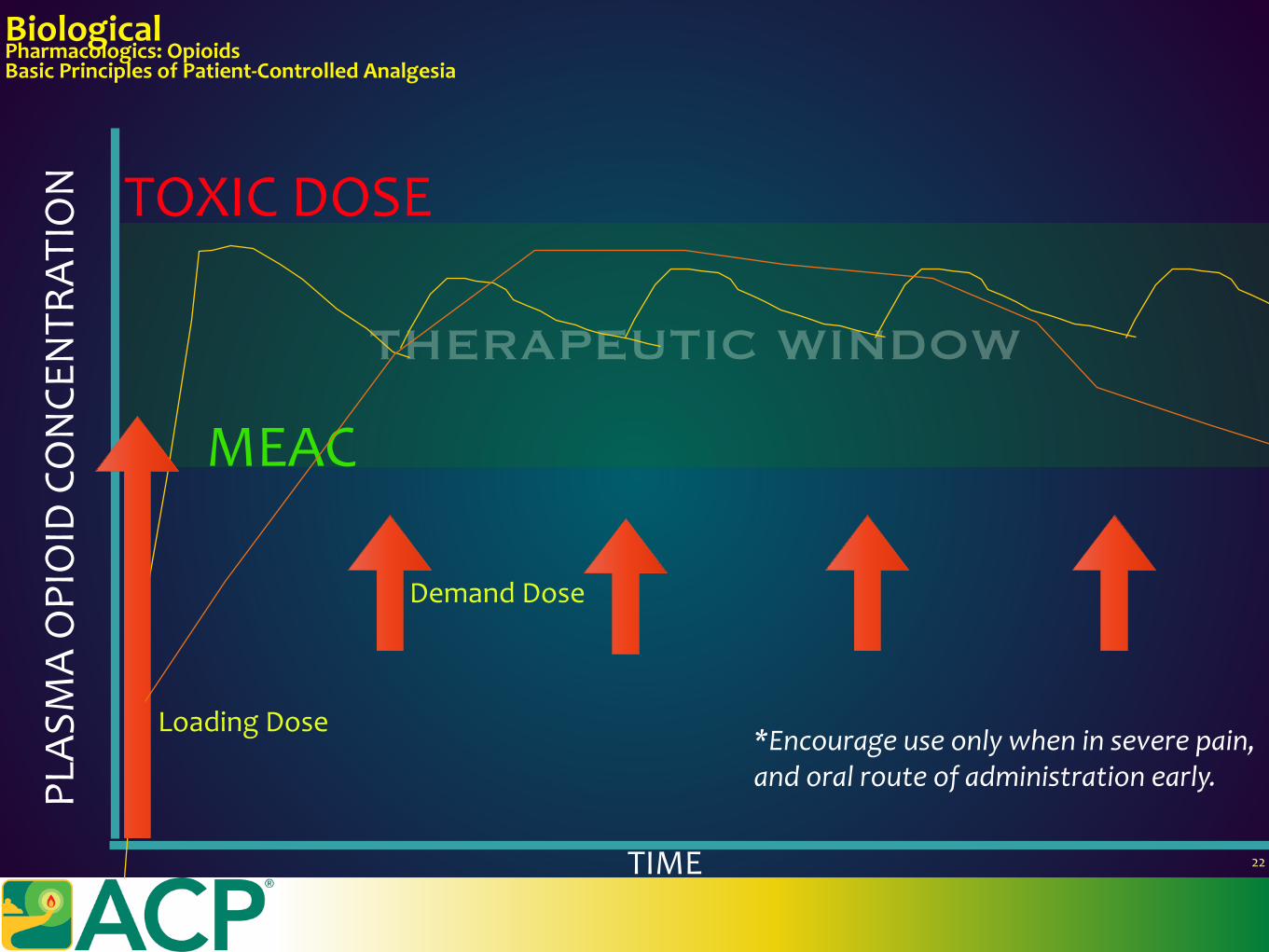
BiologicalPharmacologics:OpioidsBasicPrinciplesofPatient-ControlledAnalgesia
TIME 22
THERAPEUTIC WINDOW
PLAS
MAOPIOID
CONCE
NTR
ATIO
N
MEAC
TOXICDOSE
LoadingDose
DemandDose
*Encourageuseonlywheninseverepain,andoralrouteofadministrationearly.
BiologicalPharmacologics:OpioidsBasicPrinciplesofPatient-ControlledAnalgesia
TIME 22
THERAPEUTIC WINDOW
PLAS
MAOPIOID
CONCE
NTR
ATIO
N
MEAC
TOXICDOSE
LoadingDose
DemandDose
*Encourageuseonlywheninseverepain,andoralrouteofadministrationearly.
BiologicalPharmacologics:OpioidsTransitionsinCare
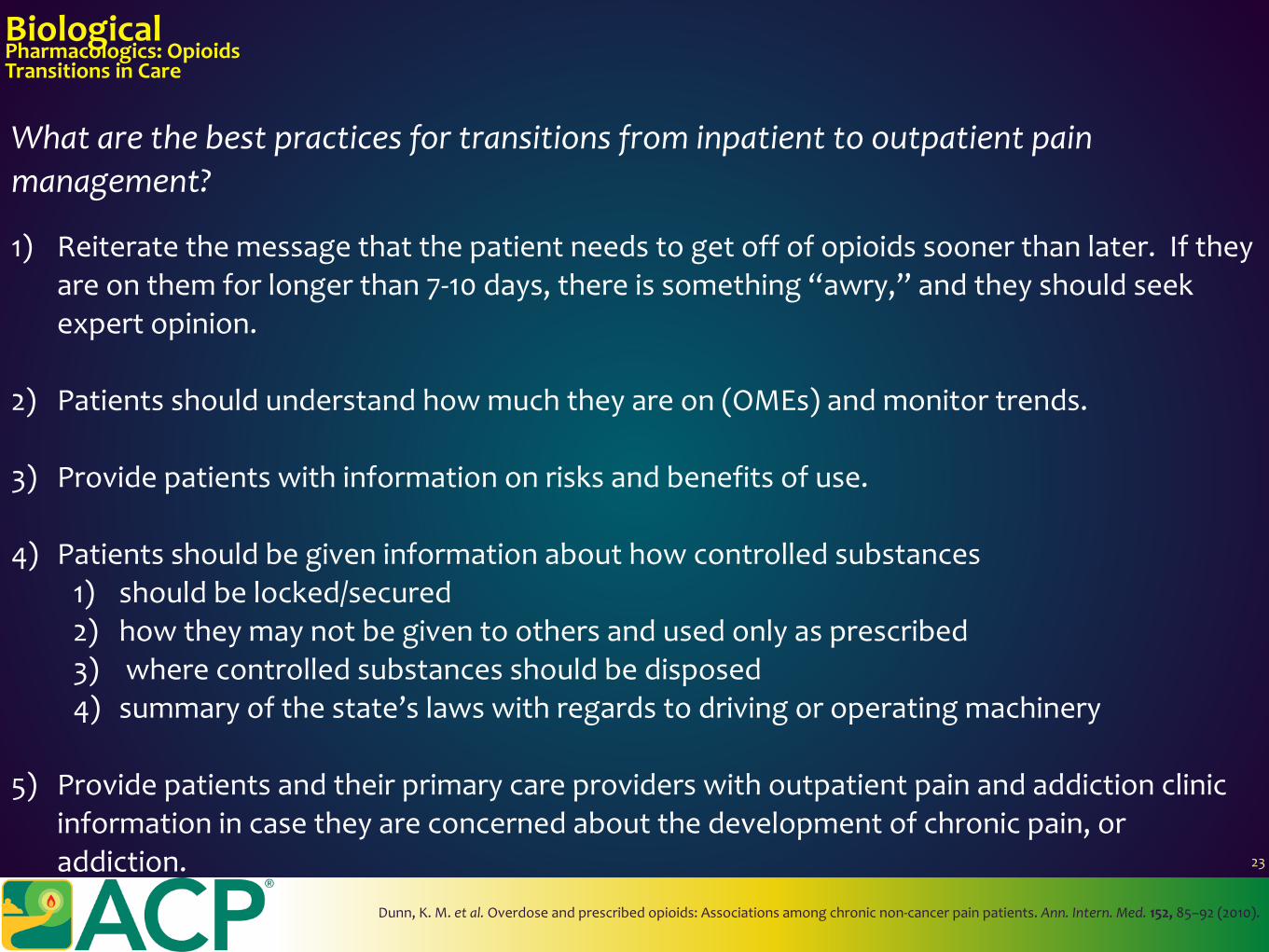
Whatarethebestpracticesfortransitionsfrominpatienttooutpatientpainmanagement?
Dunn,K.M.etal.Overdoseandprescribedopioids :Associationsamongchronicnon-cancerpainpatients.Ann.Intern.Med.152,85–92(2010).
1) Reiteratethemessagethatthepatientneedstogetoffofopioidssoonerthanlater.Iftheyareonthemforlongerthan7-10days,thereissomething“awry,”andtheyshouldseekexpertopinion.
2) Patientsshouldunderstandhowmuchtheyareon(OMEs)andmonitortrends.
3) Providepatientswithinformationonrisksandbenefitsofuse.
4) Patientsshouldbegiveninformationabouthowcontrolledsubstances1) shouldbelocked/secured2) howtheymaynotbegiventoothersandusedonlyasprescribed3) wherecontrolledsubstancesshouldbedisposed4) summaryofthestate’slawswithregardstodrivingoroperatingmachinery
5) Providepatientsandtheirprimarycareproviderswithoutpatientpainandaddictionclinicinformationincasetheyareconcernedaboutthedevelopmentofchronicpain,oraddiction. 23
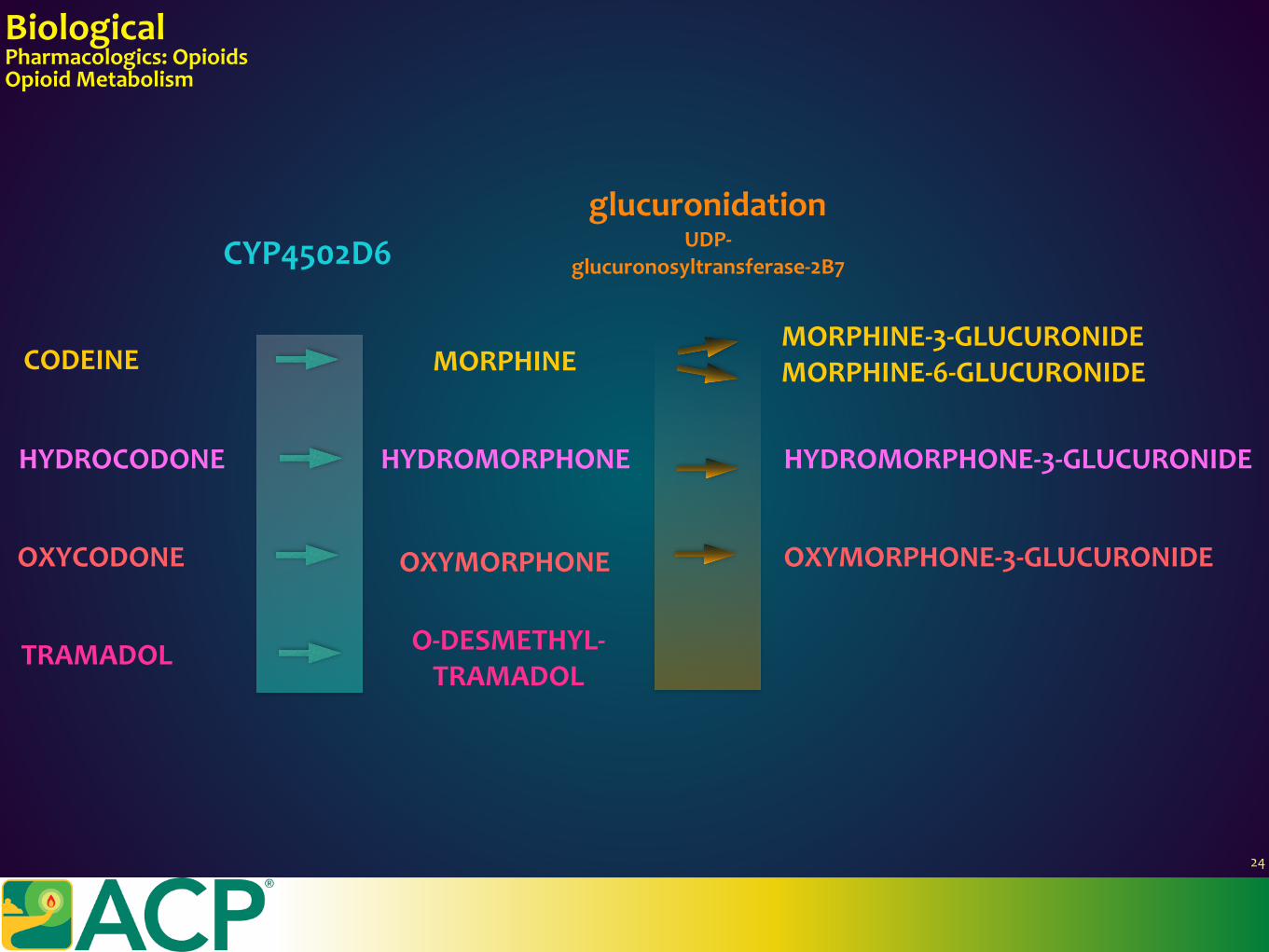
BiologicalPharmacologics:OpioidsOpioidMetabolism
HYDROCODONE
OXYCODONE
MORPHINE-3-GLUCURONIDE
MORPHINE-6-GLUCURONIDE
CYP4502D6glucuronidation
UDP-glucuronosyltransferase-2B7
MORPHINE
HYDROMORPHONE HYDROMORPHONE-3-GLUCURONIDE
OXYMORPHONE OXYMORPHONE-3-GLUCURONIDE
TRAMADOL O-DESMETHYL-TRAMADOL
CODEINE
24
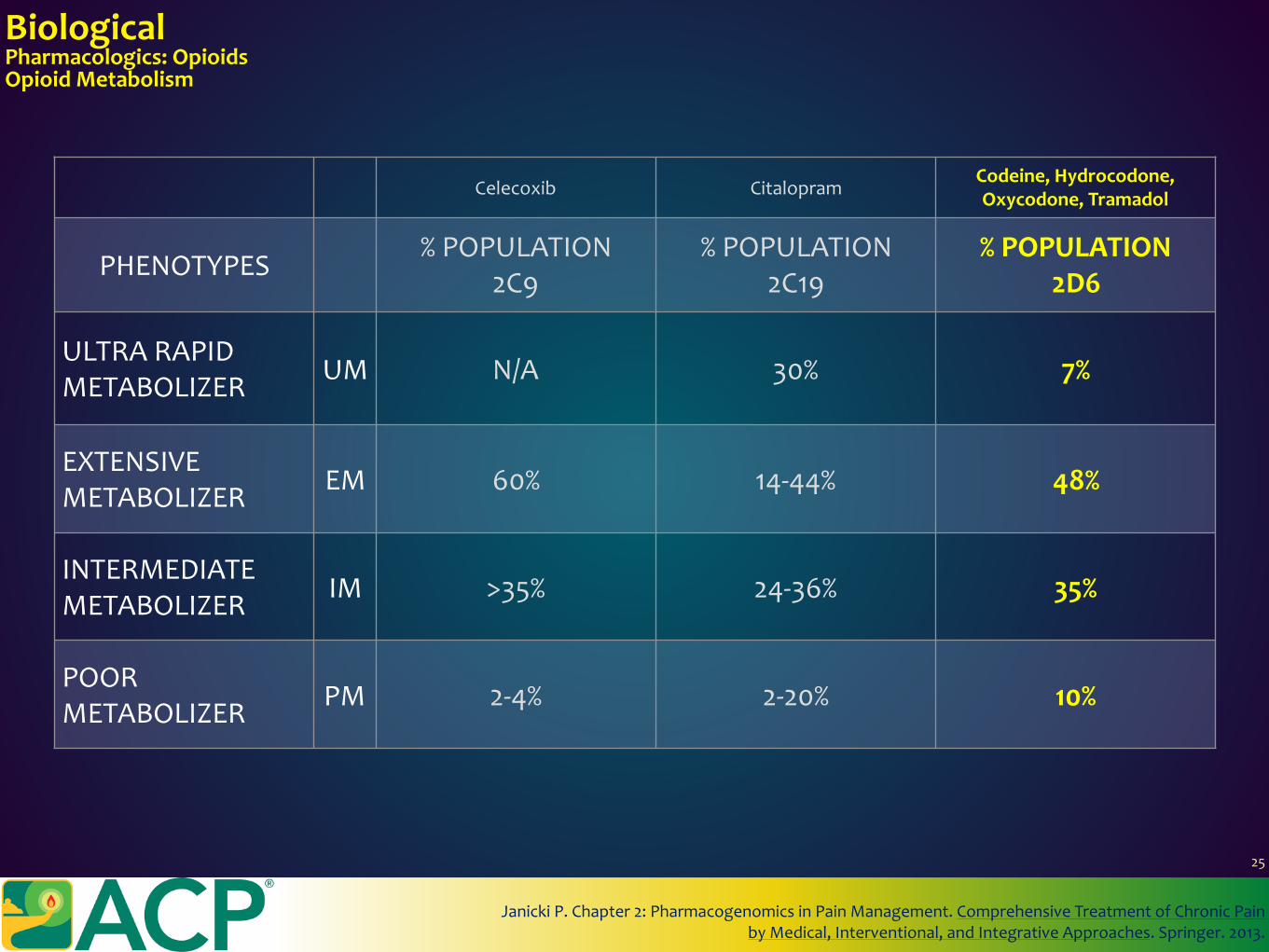
Celecoxib CitalopramCodeine,Hydrocodone,Oxycodone,Tramadol
PHENOTYPES%POPULATION
2C9%POPULATION
2C19%POPULATION
2D6
ULTRARAPIDMETABOLIZER UM N/A 30% 7%
EXTENSIVEMETABOLIZER EM 60% 14-44% 48%
INTERMEDIATEMETABOLIZER IM >35% 24-36% 35%
POORMETABOLIZER PM 2-4% 2-20% 10%
BiologicalPharmacologics:OpioidsOpioidMetabolism
JanickiP.Chapter2:PharmacogenomicsinPainManagement.ComprehensiveTreatmentofChronicPainbyMedical,Interventional,andIntegrativeApproaches.Springer.2013.
25
BiologicalPharmacologics:OpioidsEfficacyinAcutePain
Richards,D.TheOxfordPainGroupLeaguetableofanalgesicefficacy.Evid.Based.Dent.5,22–23(2004).
Opioidsare… “powerful”“painkillers” “strong”
26
BiologicalPharmacologics:OpioidsEfficacyinAcutePain
Richards,D.TheOxfordPainGroupLeaguetableofanalgesicefficacy.Evid.Based.Dent.5,22–23(2004).
26
BiologicalPharmacologics:OpioidsEfficacyinAcutePain
Richards,D.TheOxfordPainGroupLeaguetableofanalgesicefficacy.Evid.Based.Dent.5,22–23(2004).
Opioidscanbeeffectiveforstaticpain,butarethatnoteffectivefordynamicpain. Mostacutepainisdynamicpain-painassociatedwithmovement.
Considertheimportanceofdynamicpainmanagementfor:•DVT/PEprophylaxis•Atelectasis/pneumoniaprophylaxis•Urinarycatheterizationremoval
26
BiologicalPharmacologics:OpioidsEfficacyinAcutePain
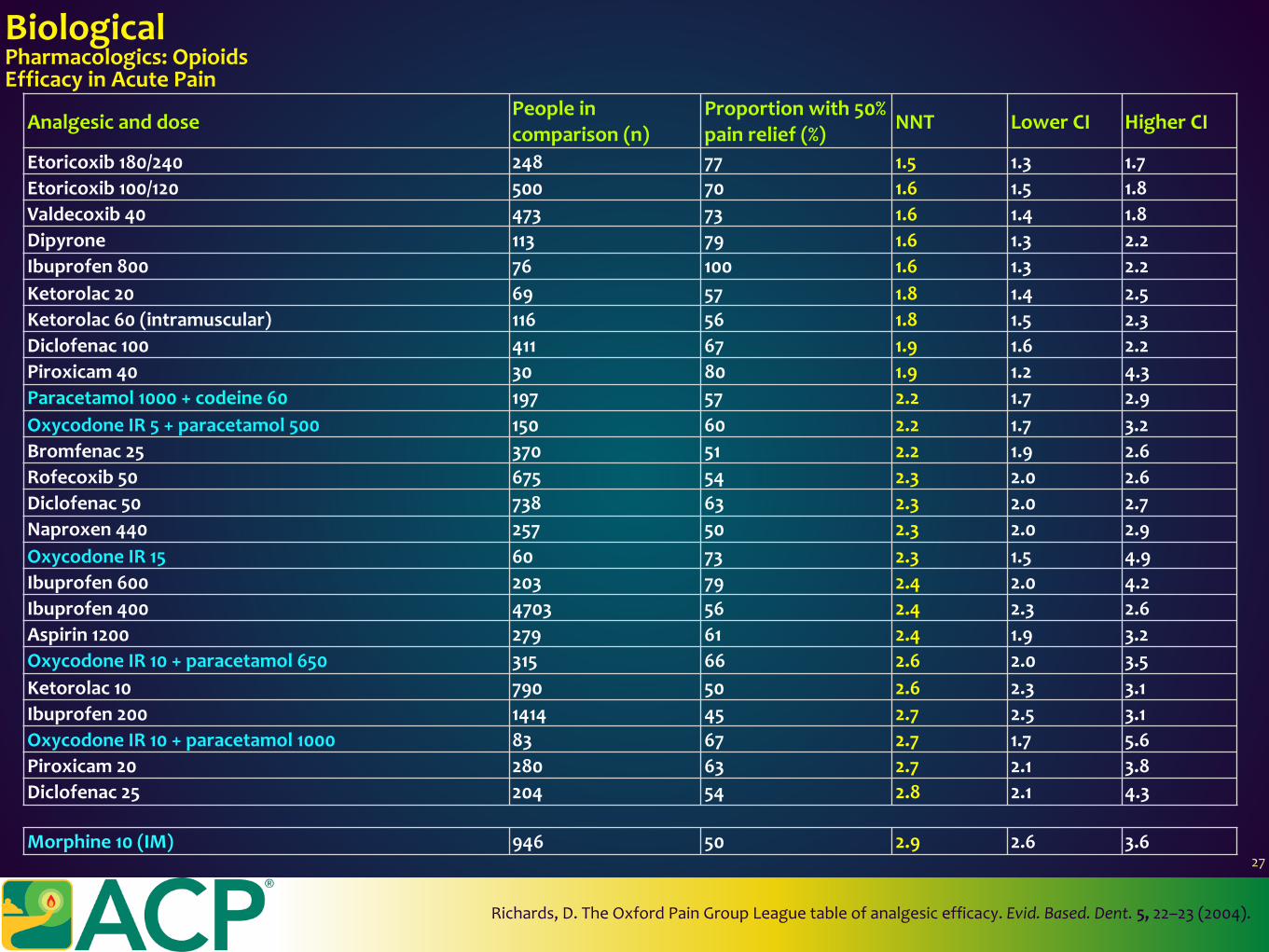
AnalgesicanddosePeopleincomparison(n)
Proportionwith50%painrelief(%) NNT LowerCI HigherCI
Etoricoxib180/240 248 77 1.5 1.3 1.7Etoricoxib100/120 500 70 1.6 1.5 1.8Valdecoxib40 473 73 1.6 1.4 1.8Dipyrone 113 79 1.6 1.3 2.2Ibuprofen800 76 100 1.6 1.3 2.2Ketorolac20 69 57 1.8 1.4 2.5Ketorolac60(intramuscular) 116 56 1.8 1.5 2.3Diclofenac100 411 67 1.9 1.6 2.2Piroxicam40 30 80 1.9 1.2 4.3Paracetamol1000+codeine60 197 57 2.2 1.7 2.9OxycodoneIR5+paracetamol500 150 60 2.2 1.7 3.2Bromfenac25 370 51 2.2 1.9 2.6Rofecoxib50 675 54 2.3 2.0 2.6Diclofenac50 738 63 2.3 2.0 2.7Naproxen440 257 50 2.3 2.0 2.9OxycodoneIR15 60 73 2.3 1.5 4.9Ibuprofen600 203 79 2.4 2.0 4.2Ibuprofen400 4703 56 2.4 2.3 2.6Aspirin1200 279 61 2.4 1.9 3.2OxycodoneIR10+paracetamol650 315 66 2.6 2.0 3.5Ketorolac10 790 50 2.6 2.3 3.1Ibuprofen200 1414 45 2.7 2.5 3.1OxycodoneIR10+paracetamol1000 83 67 2.7 1.7 5.6Piroxicam20 280 63 2.7 2.1 3.8Diclofenac25 204 54 2.8 2.1 4.3
Richards,D.TheOxfordPainGroupLeaguetableofanalgesicefficacy.Evid.Based.Dent.5,22–23(2004).
Morphine10(IM) 946 50 2.9 2.6 3.627
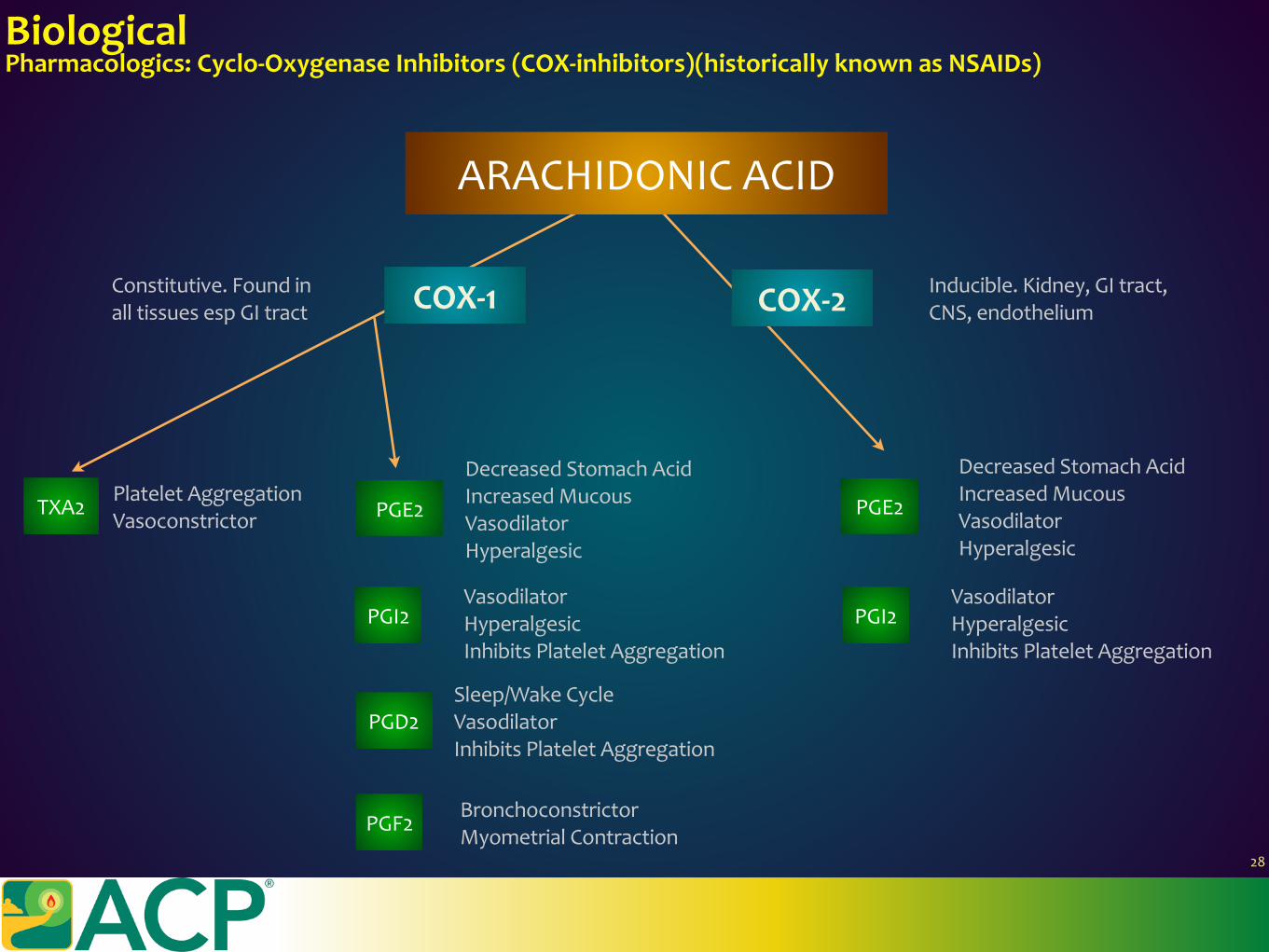
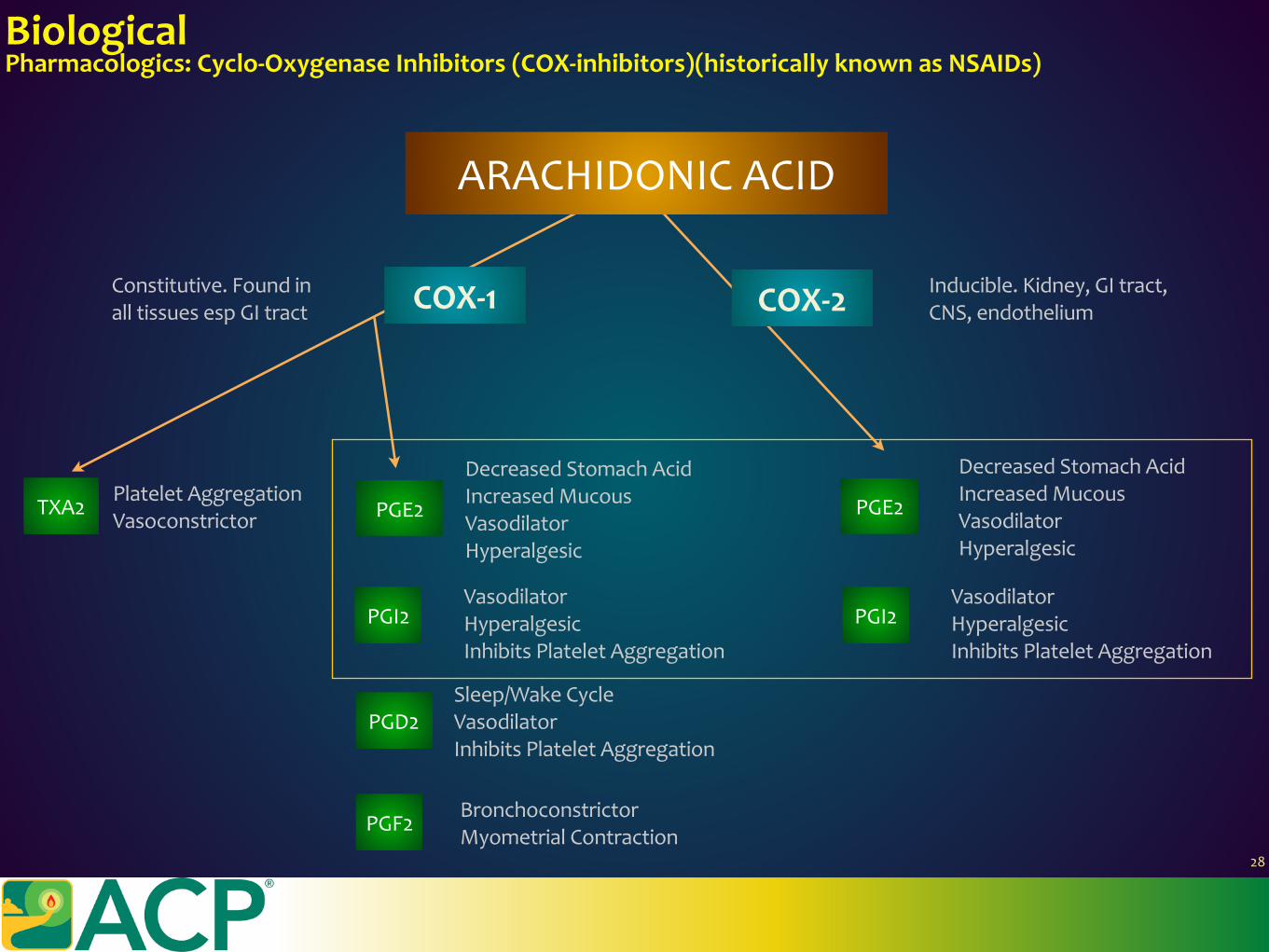
BiologicalPharmacologics:Cyclo-OxygenaseInhibitors(COX-inhibitors)(historicallyknownasNSAIDs)
ARACHIDONICACID
COX-1
PGI2
TXA2 PGE2
COX-2
PGD2
PGF2
PGE2
PGI2VasodilatorHyperalgesicInhibitsPlateletAggregation
Sleep/WakeCycleVasodilatorInhibitsPlateletAggregation
BronchoconstrictorMyometrialContraction
DecreasedStomachAcidIncreasedMucousVasodilatorHyperalgesic
VasodilatorHyperalgesicInhibitsPlateletAggregation
PlateletAggregationVasoconstrictor
Constitutive.FoundinalltissuesespGItract
Inducible.Kidney,GItract,CNS,endothelium
28
DecreasedStomachAcidIncreasedMucousVasodilatorHyperalgesic
BiologicalPharmacologics:Cyclo-OxygenaseInhibitors(COX-inhibitors)(historicallyknownasNSAIDs)
ARACHIDONICACID
COX-1
PGI2
TXA2 PGE2
COX-2
PGD2
PGF2
PGE2
PGI2VasodilatorHyperalgesicInhibitsPlateletAggregation
Sleep/WakeCycleVasodilatorInhibitsPlateletAggregation
BronchoconstrictorMyometrialContraction
DecreasedStomachAcidIncreasedMucousVasodilatorHyperalgesic
VasodilatorHyperalgesicInhibitsPlateletAggregation
PlateletAggregationVasoconstrictor
Constitutive.FoundinalltissuesespGItract
Inducible.Kidney,GItract,CNS,endothelium
28
DecreasedStomachAcidIncreasedMucousVasodilatorHyperalgesic
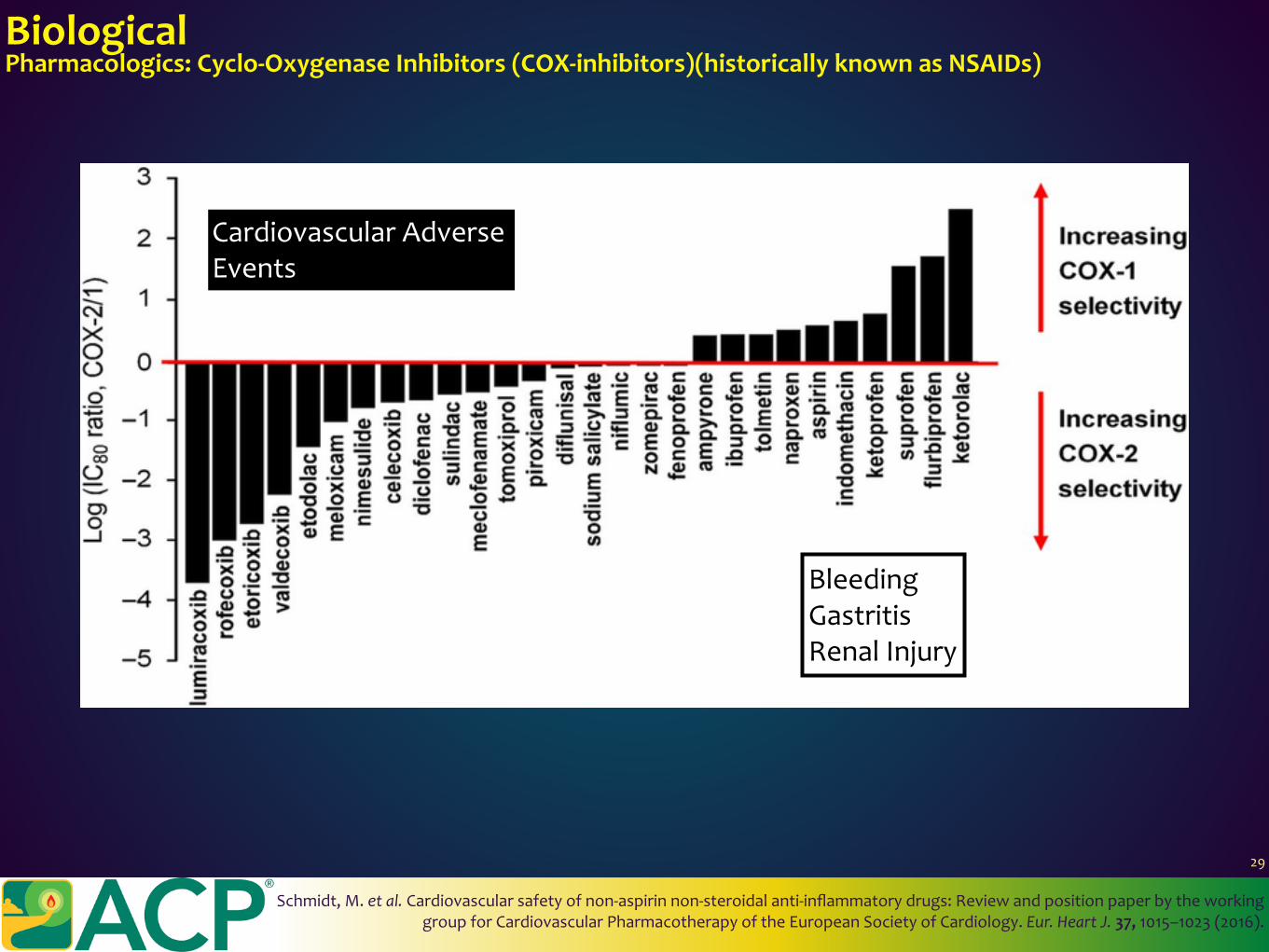
BiologicalPharmacologics:Cyclo-OxygenaseInhibitors(COX-inhibitors)(historicallyknownasNSAIDs)
Schmidt,M.etal.Cardiovascularsafetyofnon-aspirinnon-steroidalanti-inflammatorydrugs:ReviewandpositionpaperbytheworkinggroupforCardiovascularPharmacotherapyoftheEuropeanSocietyofCardiology.Eur.HeartJ.37,1015–1023(2016).
BleedingGastritisRenalInjury
CardiovascularAdverseEvents
29
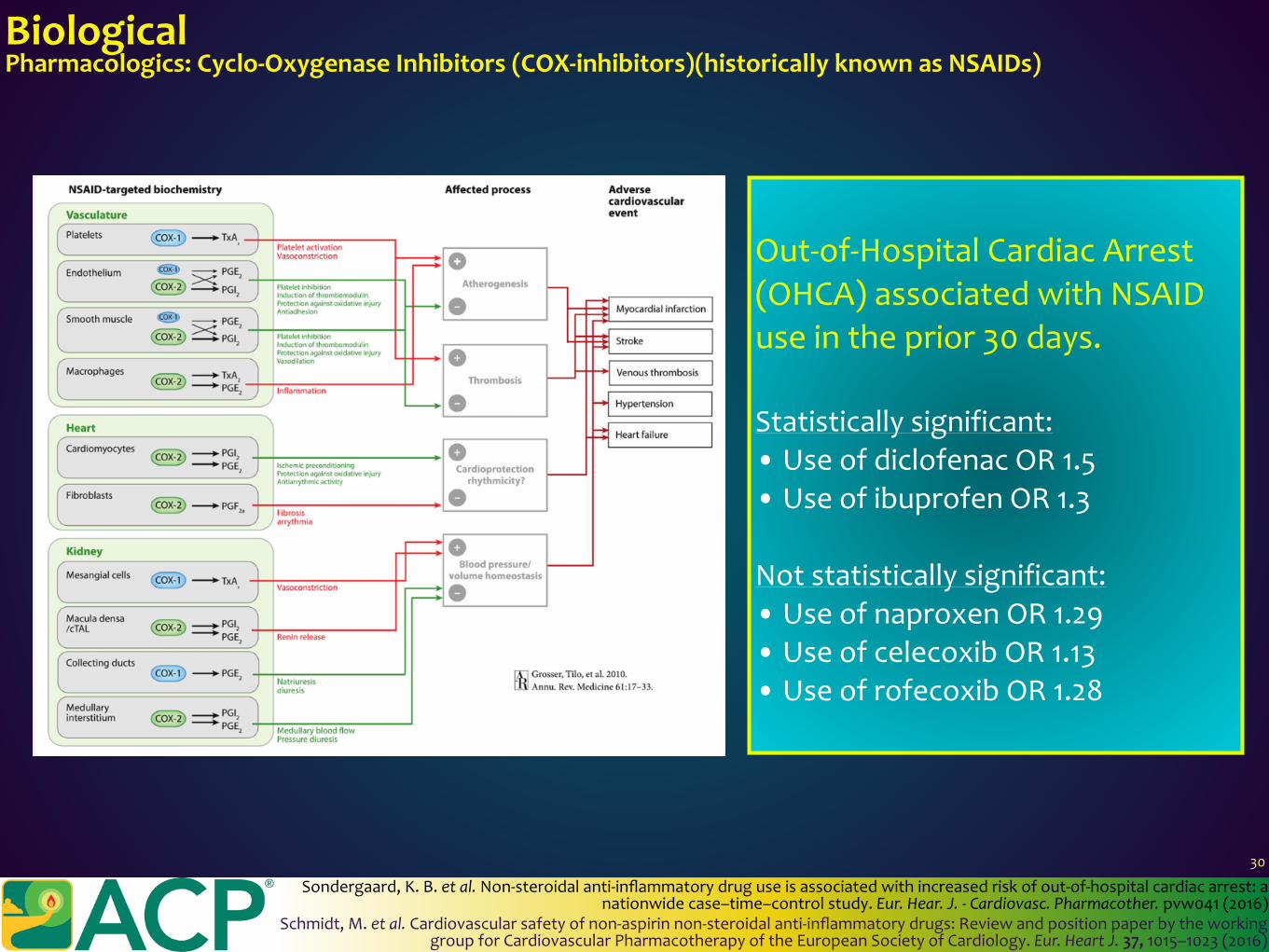
BiologicalPharmacologics:Cyclo-OxygenaseInhibitors(COX-inhibitors)(historicallyknownasNSAIDs)
Schmidt,M.etal.Cardiovascularsafetyofnon-aspirinnon-steroidalanti-inflammatorydrugs:ReviewandpositionpaperbytheworkinggroupforCardiovascularPharmacotherapyoftheEuropeanSocietyofCardiology.Eur.HeartJ.37,1015–1023(2016)
Out-of-HospitalCardiacArrest(OHCA)associatedwithNSAIDuseintheprior30days.
Statisticallysignificant:• UseofdiclofenacOR1.5• UseofibuprofenOR1.3
Notstatisticallysignificant:• UseofnaproxenOR1.29• UseofcelecoxibOR1.13• UseofrofecoxibOR1.28
Sondergaard,K.B.etal.Non-steroidalanti-inflammatorydruguseisassociatedwithincreasedriskofout-of-hospitalcardiacarrest:anationwidecase–time–controlstudy.Eur.Hear.J.-Cardiovasc.Pharmacother.pvw041(2016)
30
Steroids(glucocorticoids)reducepainbyreducingprostaglandinsynthesis.However,theirsideeffectprofileissignificantandshouldnotbeusedfornon-surgical,acutenon-cancerpainunlessotheroptionsarenoteffectiveorpossible.Theyshouldnotbeusedchronically.
Dexamethasoneisroutinelyusedintheperi-operativearenaforpost-operativenauseaandvomiting.ItisassociatedwithareductioninNRS/VASandopioidconsumption,8mg>4mg.
Sideeffects:•Increasedweightgain•Proximalmuscleweakness•Insomnia•Gastrointestinalsideeffects•Gastrointestinalbleeding•Psychatricsideeffects•Osteoporoseswithlong-termuse•Infections•Hyperglycemia•CushingSyndrome•Thromboembolism
BiologicalPharmacologics:Steroids
Vyvey,M.Steroidsaspainreliefadjuvants.Can.Fam.Physician56,1295–7,e415(2010)DeOliveiraGSJr.;AlmeidaMD;BenzonHT;McCarthyRJ.PerioperativeSingleDoseSystemic
Dexamethasonefor.Anesthesiology115,575–588(2011)
31
BiologicalPharmacologics:Acetaminophen/Paracetamol
•Lachiewicz,P.F.TheRoleofIntravenousAcetaminopheninMultimodalPainProtocolsforPerioperativeOrthopedicPatients.Orthopedics36,15–19(2013)•Toms,L.etal.Singledoseoralparacetamol(acetaminophen)forpostoperativepaininadults(Review)Singledoseoralparacetamol(acetaminophen)for
postoperativepaininadults.4–6(2012).•Tzortzopoulou,A.etal.Singledoseintravenouspropacetamolorintravenousparacetamolforpostoperativepain.CochranedatabaseSyst.Rev.CD007126
(2011).
32
BiologicalPharmacologics:Acetaminophen/ParacetamolAnilineanalgesic.Mechanismofactionremainsunknown.TheproposedCOX-3mechanismiscontroversial.
Safety:4grams/daylimitissafeinadults.Lean-bodyweightbased:60mg/kg/dayProspectivetrialsinvolvingcentralpainrelatedtostrokeshowssafetyupto6g/day
•Hepatitis:ifindolent,4g/dayok• Alcoholism:ifnotdrinking>2drinks/day,4g/dayok• CombinationHepatitisandAlcoholism:depends.2g/daylimitoravoid?
CautionincombinationwithCYP4503A4/2E1inhibitors:considereffectofcoumadin,anticonvulsants,andantipsychotics
•Lachiewicz,P.F.TheRoleofIntravenousAcetaminopheninMultimodalPainProtocolsforPerioperativeOrthopedicPatients.Orthopedics36,15–19(2013)•Toms,L.etal.Singledoseoralparacetamol(acetaminophen)forpostoperativepaininadults(Review)Singledoseoralparacetamol(acetaminophen)for
postoperativepaininadults.4–6(2012).•Tzortzopoulou,A.etal.Singledoseintravenouspropacetamolorintravenousparacetamolforpostoperativepain.CochranedatabaseSyst.Rev.CD007126
(2011).
32
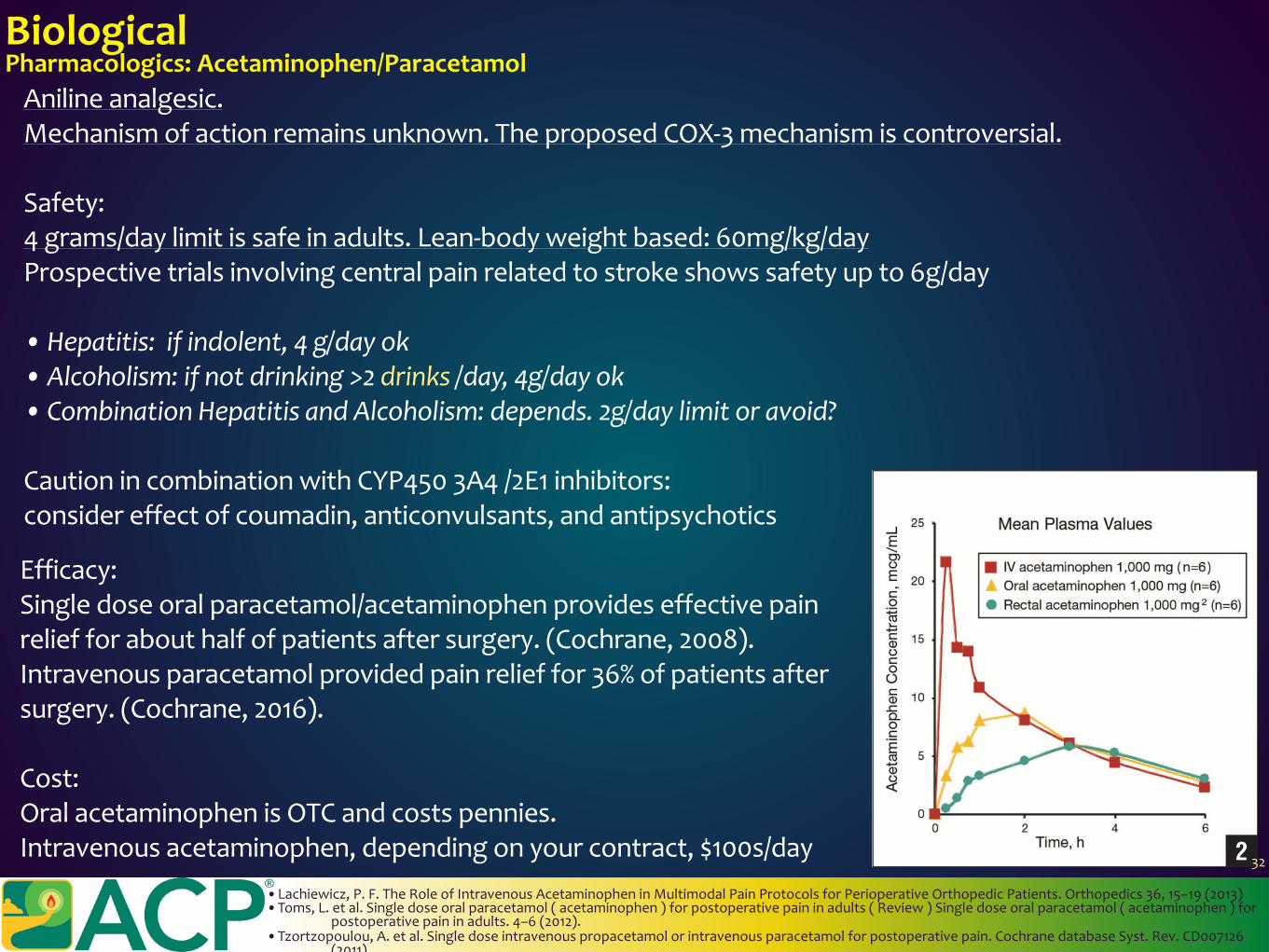
BiologicalPharmacologics:Acetaminophen/ParacetamolAnilineanalgesic.Mechanismofactionremainsunknown.TheproposedCOX-3mechanismiscontroversial.
Safety:4grams/daylimitissafeinadults.Lean-bodyweightbased:60mg/kg/dayProspectivetrialsinvolvingcentralpainrelatedtostrokeshowssafetyupto6g/day
•Hepatitis:ifindolent,4g/dayok• Alcoholism:ifnotdrinking>2drinks/day,4g/dayok• CombinationHepatitisandAlcoholism:depends.2g/daylimitoravoid?
CautionincombinationwithCYP4503A4/2E1inhibitors:considereffectofcoumadin,anticonvulsants,andantipsychotics
Efficacy:Singledoseoralparacetamol/acetaminophenprovideseffectivepainreliefforabouthalfofpatientsaftersurgery.(Cochrane,2008).Intravenousparacetamolprovidedpainrelieffor36%ofpatientsaftersurgery.(Cochrane,2016).
Cost:OralacetaminophenisOTCandcostspennies.Intravenousacetaminophen,dependingonyourcontract,$100s/day
•Lachiewicz,P.F.TheRoleofIntravenousAcetaminopheninMultimodalPainProtocolsforPerioperativeOrthopedicPatients.Orthopedics36,15–19(2013)•Toms,L.etal.Singledoseoralparacetamol(acetaminophen)forpostoperativepaininadults(Review)Singledoseoralparacetamol(acetaminophen)for
postoperativepaininadults.4–6(2012).•Tzortzopoulou,A.etal.Singledoseintravenouspropacetamolorintravenousparacetamolforpostoperativepain.CochranedatabaseSyst.Rev.CD007126
(2011).
32
ClonidineEffectiveinanimalmodelanalgesictrials.Whileitcanbeeffectiveinreducingpainandopioidconsumption,itislimitedbyitssideeffectofbradycardiaandhypotension.
BiologicalPharmacologics:Alpha-2Agonists
Dexmedetomidine:(alpha-2agonist)1620:1(alpha-1agonist)canbeusedforbothanalgesicandsedativeproperties.Itisparticularlyusefulinpatientswithheroinabusebecauseithelpswithwithdrawalsymptoms,providesanalgesia,andcalms/sedates.ThedrugcrossestheBBBandhasbeenstudiedviaseveralroutesofadministration:IM/IV/IN/RegionalthoughnotPO.
Itisexpensive,andcanonlybeusedintravenouslyinmonitoredsettingsduetothesameconcernsregardingbradycardiaandhypotension.
Stillearlyinourexperienceasfarastheliterature.Wehavesupportforitsuse,particularlyintheICUorinpediatrics.Itsbenefitremainsduringtheinfusion,anddoesnotseemtoprovidelonger-termbenefitduetoaneliminationhalf-liveof2hours.
33
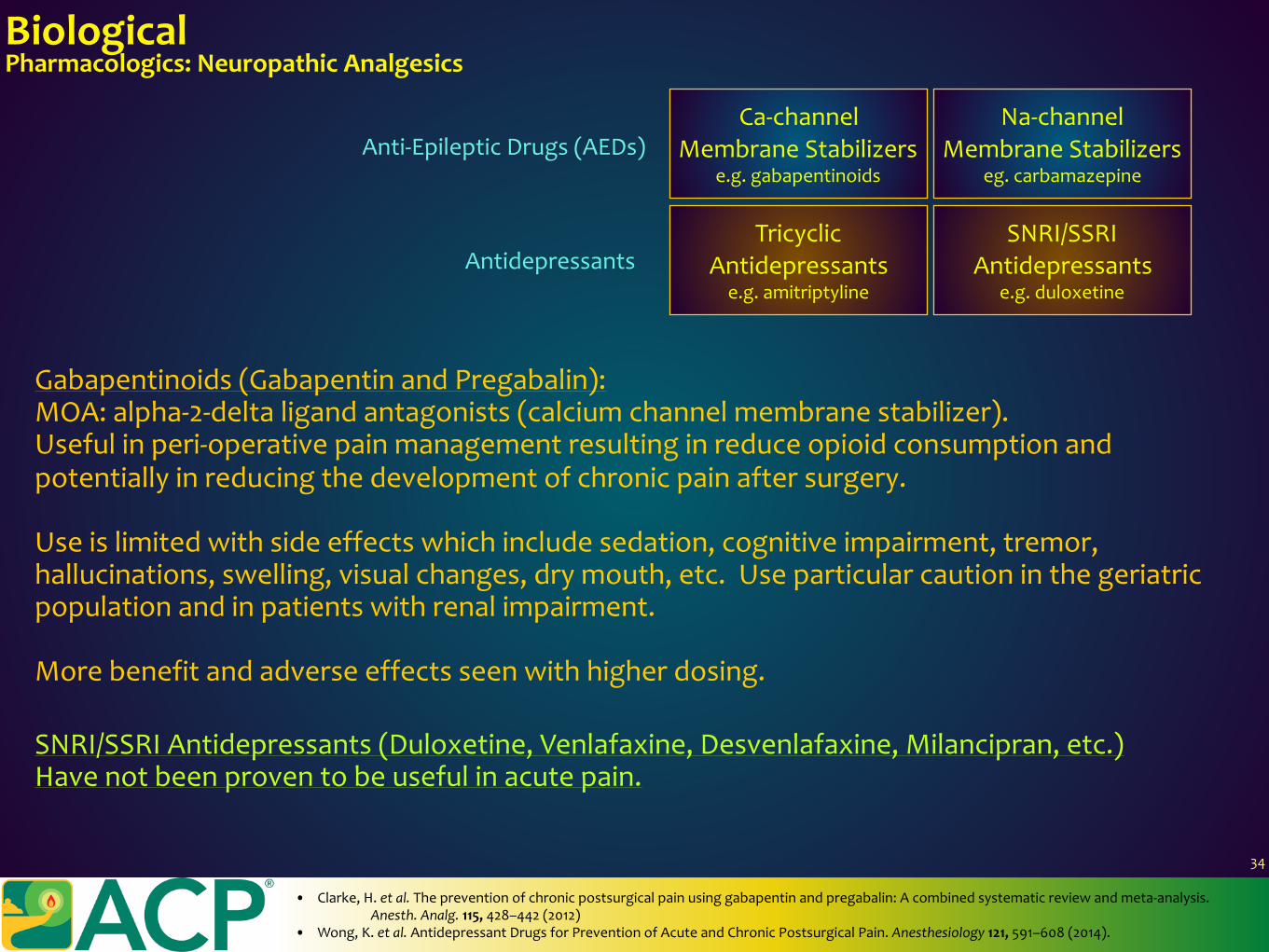
Gabapentinoids(GabapentinandPregabalin):MOA:alpha-2-deltaligandantagonists(calciumchannelmembranestabilizer).Usefulinperi-operativepainmanagementresultinginreduceopioidconsumptionandpotentiallyinreducingthedevelopmentofchronicpainaftersurgery.
Useislimitedwithsideeffectswhichincludesedation,cognitiveimpairment,tremor,hallucinations,swelling,visualchanges,drymouth,etc.Useparticularcautioninthegeriatricpopulationandinpatientswithrenalimpairment.
Morebenefitandadverseeffectsseenwithhigherdosing.
BiologicalPharmacologics:NeuropathicAnalgesics
• Clarke,H.etal.Thepreventionofchronicpostsurgicalpainusinggabapentinandpregabalin:Acombinedsystematicreviewandmeta-analysis.Anesth.Analg.115,428–442(2012)
• Wong,K.etal.AntidepressantDrugsforPreventionofAcuteandChronicPostsurgicalPain.Anesthesiology121,591–608(2014).
SNRI/SSRIAntidepressants(Duloxetine,Venlafaxine,Desvenlafaxine,Milancipran,etc.)Havenotbeenproventobeusefulinacutepain.
Ca-channelMembraneStabilizers
e.g.gabapentinoids
Na-channelMembraneStabilizers
eg.carbamazepine
TricyclicAntidepressants
e.g.amitriptyline
SNRI/SSRIAntidepressants
e.g.duloxetine
Anti-EpilepticDrugs(AEDs)
Antidepressants
34
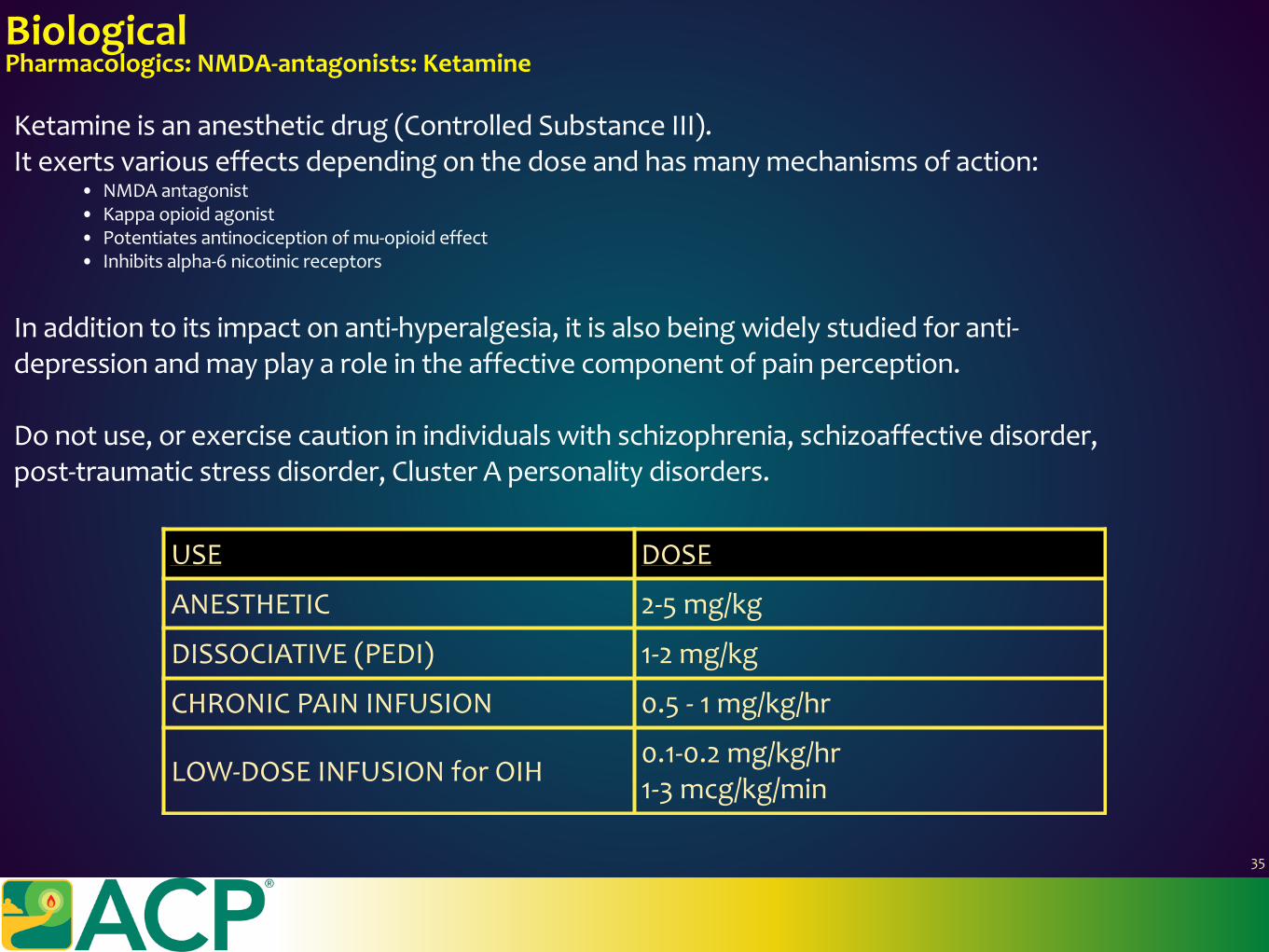
BiologicalPharmacologics:NMDA-antagonists:Ketamine
Ketamineisananestheticdrug(ControlledSubstanceIII).Itexertsvariouseffectsdependingonthedoseandhasmanymechanismsofaction:
• NMDAantagonist• Kappaopioidagonist• Potentiatesantinociceptionofmu-opioideffect• Inhibitsalpha-6nicotinicreceptors
Inadditiontoitsimpactonanti-hyperalgesia,itisalsobeingwidelystudiedforanti-depressionandmayplayaroleintheaffectivecomponentofpainperception.
Donotuse,orexercisecautioninindividualswithschizophrenia,schizoaffectivedisorder,post-traumaticstressdisorder,ClusterApersonalitydisorders.
USE DOSE
ANESTHETIC 2-5mg/kg
DISSOCIATIVE(PEDI) 1-2mg/kg
CHRONICPAININFUSION 0.5-1mg/kg/hr
LOW-DOSEINFUSIONforOIH0.1-0.2mg/kg/hr1-3mcg/kg/min
35
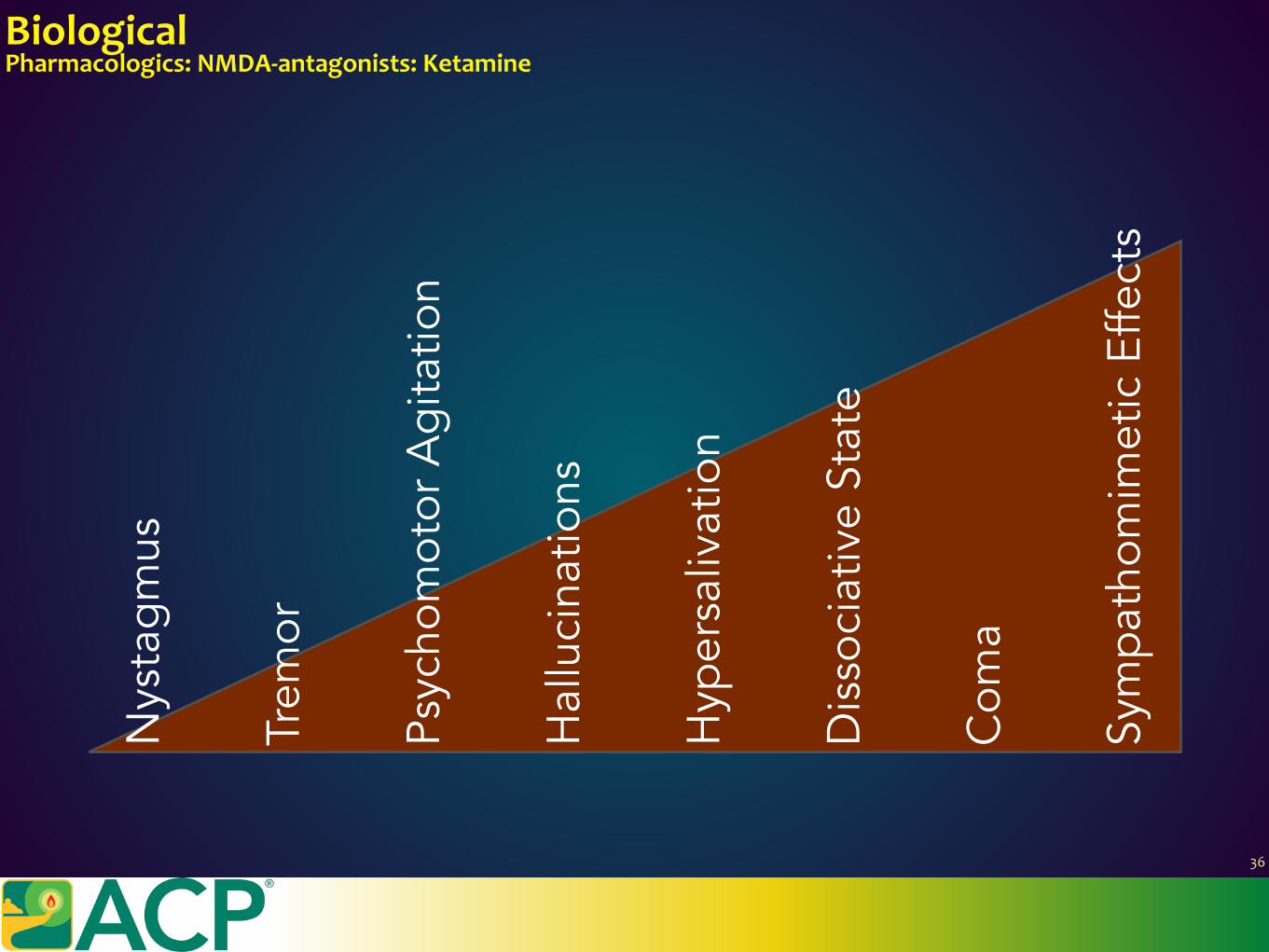
BiologicalPharmacologics:NMDA-antagonists:Ketamine
Nys
tagm
us
Trem
or
Psyc
hom
otor
Agi
tatio
n
Hal
luci
natio
ns
Hyp
ersa
livat
ion
Dis
soci
ativ
e St
ate
Com
a
Sym
path
omim
etic
Effe
cts
36
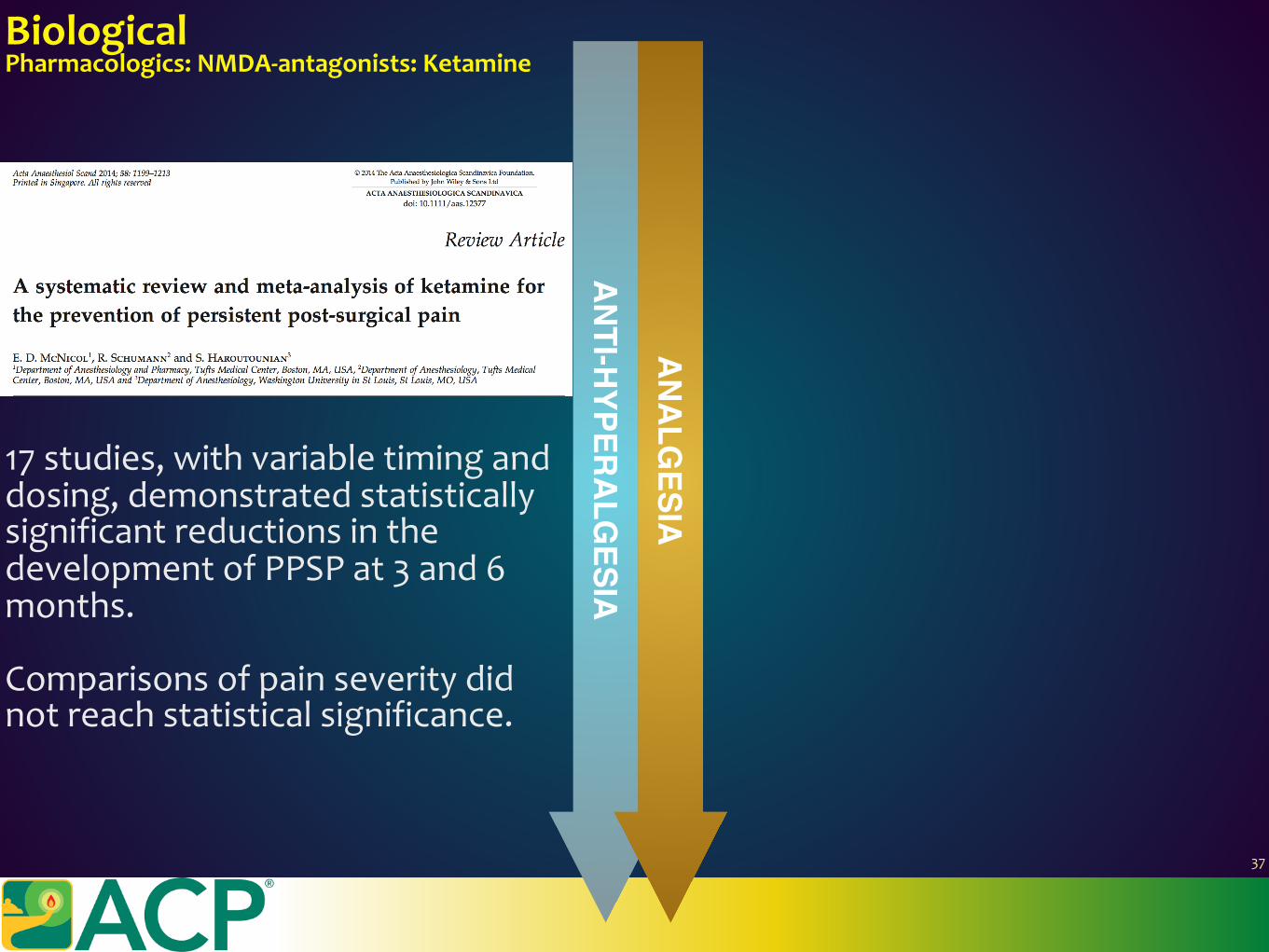
17studies,withvariabletiminganddosing,demonstratedstatisticallysignificantreductionsinthedevelopmentofPPSPat3and6months.
Comparisonsofpainseveritydidnotreachstatisticalsignificance.
ANTI-H
YPERALGESIA
ANALGESIA
BiologicalPharmacologics:NMDA-antagonists:Ketamine
37
17studies,withvariabletiminganddosing,demonstratedstatisticallysignificantreductionsinthedevelopmentofPPSPat3and6months.
Comparisonsofpainseveritydidnotreachstatisticalsignificance.
ANTI-H
YPERALGESIA
BiologicalPharmacologics:NMDA-antagonists:Ketamine
37
17studies,withvariabletiminganddosing,demonstratedstatisticallysignificantreductionsinthedevelopmentofPPSPat3and6months.
Comparisonsofpainseveritydidnotreachstatisticalsignificance.
ANTI-H
YPERALGESIA
BiologicalPharmacologics:NMDA-antagonists:Ketamine
37
17studies,withvariabletiminganddosing,demonstratedstatisticallysignificantreductionsinthedevelopmentofPPSPat3and6months.
Comparisonsofpainseveritydidnotreachstatisticalsignificance.
ANTI-H
YPERALGESIA
BiologicalPharmacologics:NMDA-antagonists:Ketamine
39clinicaltrials,5meta-analyses,wereincluded.Variabletiminganddosing,demonstratedstatisticallysignificantreductionsinopioidconsumptionby40%
37
BiologicalPharmacologics:Voltage-GatedSodiumChannelBlockade:LidocaineInfusion.
Lidocaineisananti-arrhythmicandlocalanestheticdrug.Itrelievespainatdosesfrom1-2mg/kg/hr
Ithasbeenwidelystudiedincolectomy,laparoscopicsurgery,andreducesopioidconsumption.Inchronicpain,ithasbeenstudiedforCRPS,headache,andotherneuropathicpainconditionssuchaserythromelalgia,whereitcanbethe“cure”forsodiumchannelopathy.
Itseffectlastsduringtheinfusionandshortlywearsoff.
Donotuse,orexercisecautioninindividualswheresodiumchannelcardiacblockadewouldbeproblematic,e.g.sinoatrialblockor2ndor3rddegreeblock.
Dunn,L.K.,Ph,D.,Durieux,M.E.&Ph,D.PerioperativeuseofLidocaine.Anesthesiology(2017)
38
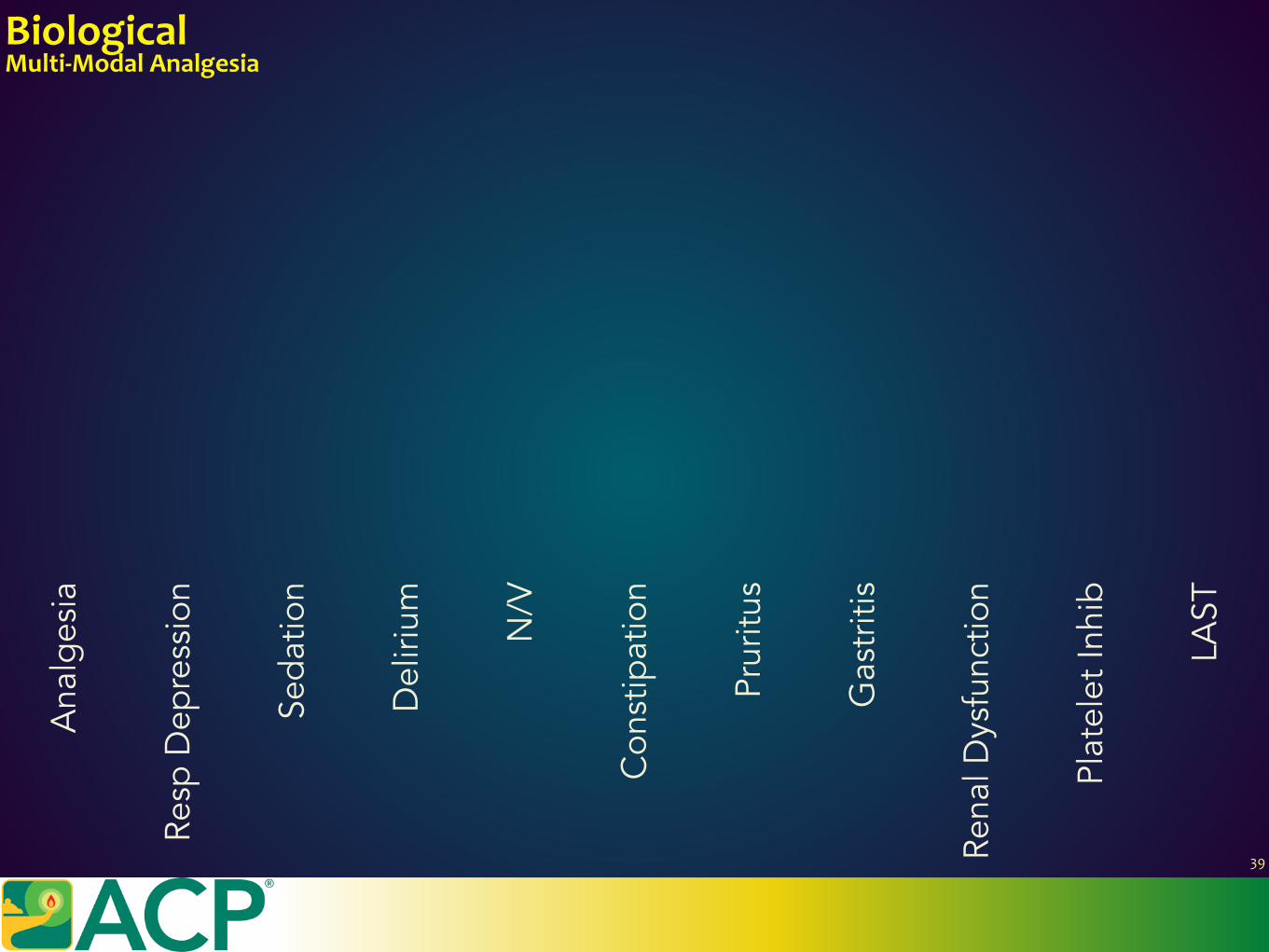
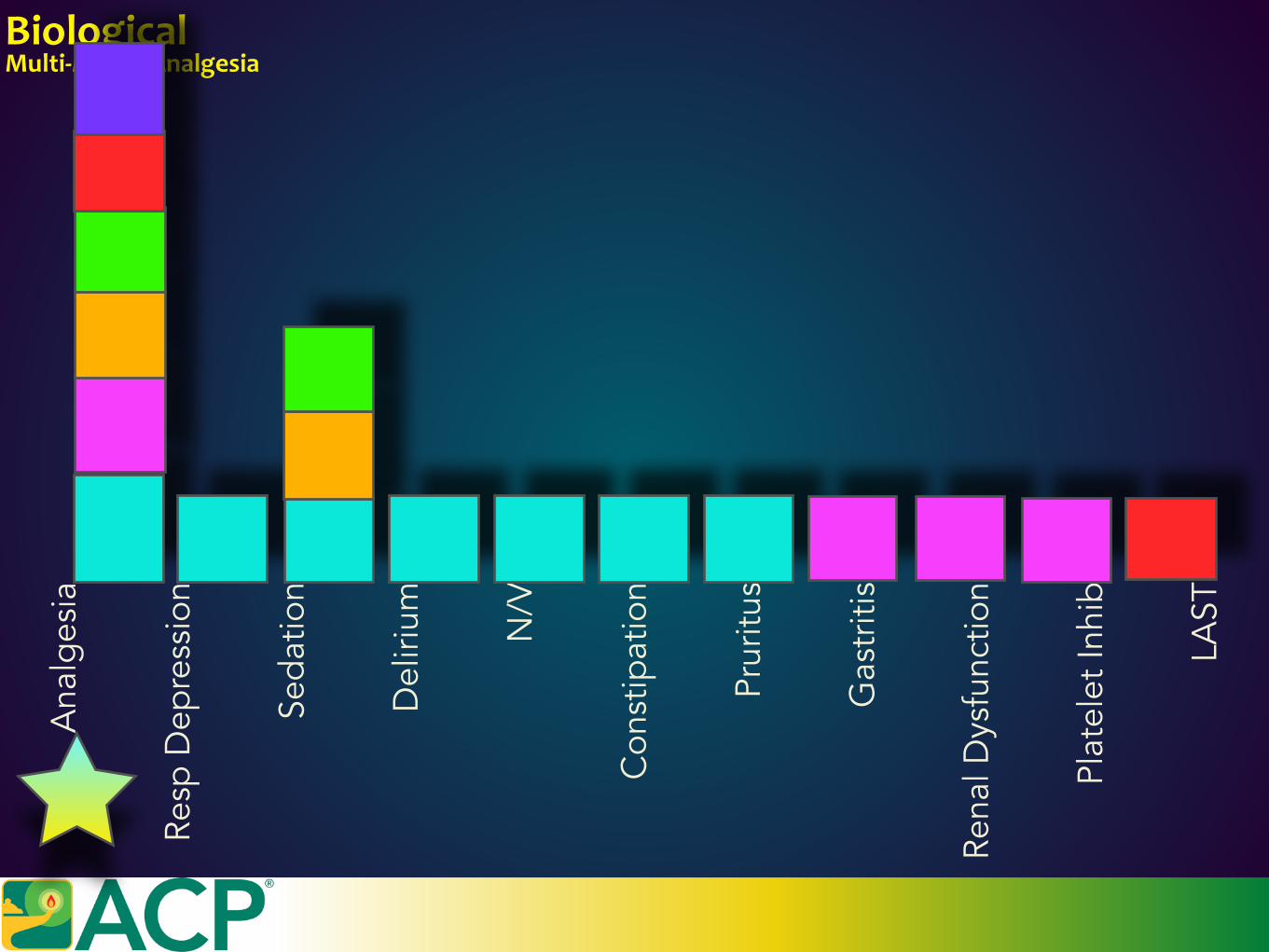
BiologicalMulti-ModalAnalgesia
Ana
lges
ia
Resp
Dep
ress
ion
Seda
tion
Del
irium
N/V
Con
stip
atio
n
Prur
itus
Gas
triti
s
Rena
l Dys
func
tion
Plat
elet
Inhi
b
LAST
39
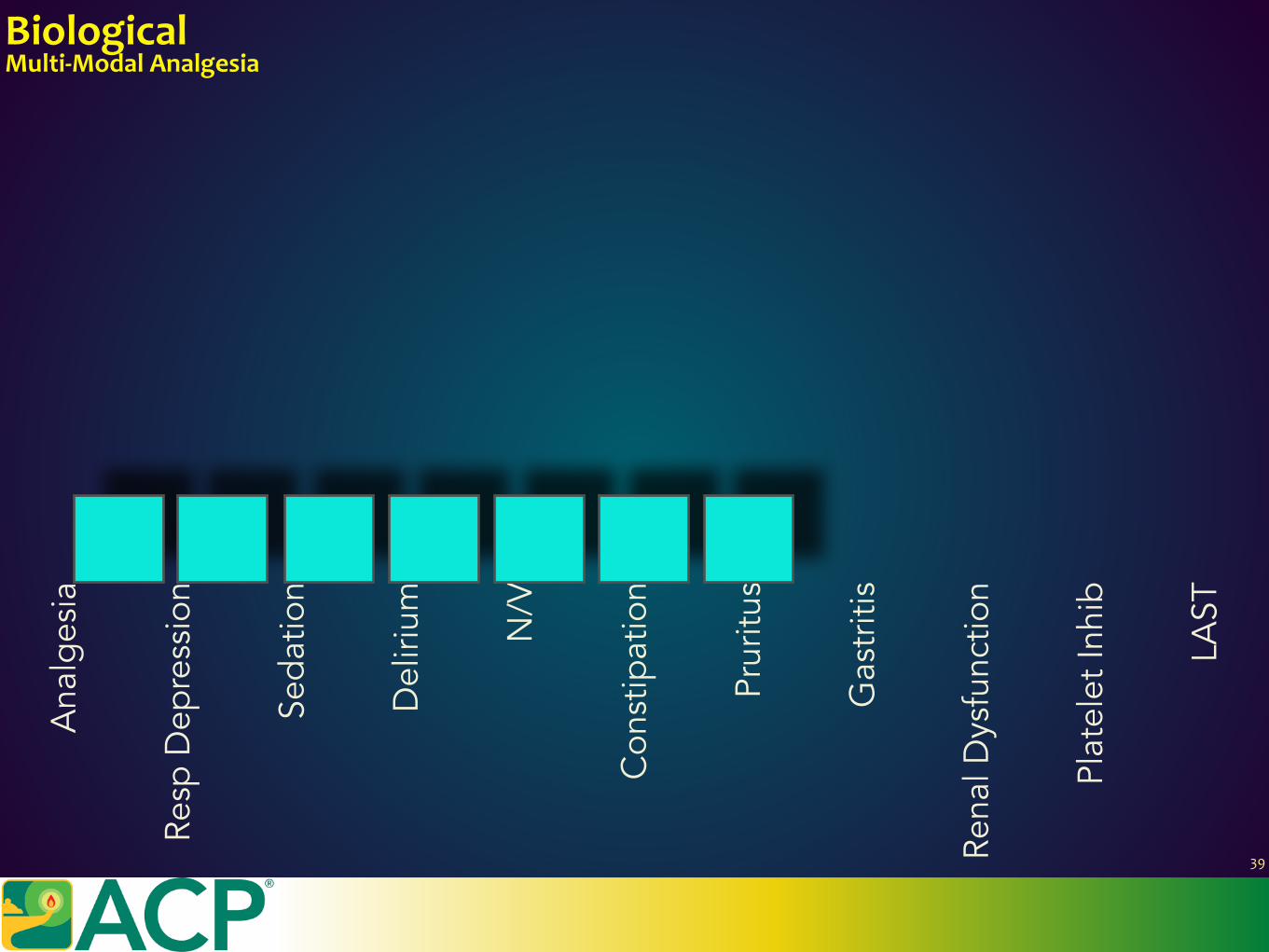
BiologicalMulti-ModalAnalgesia
Ana
lges
ia
Resp
Dep
ress
ion
Seda
tion
Del
irium
N/V
Con
stip
atio
n
Prur
itus
Gas
triti
s
Rena
l Dys
func
tion
Plat
elet
Inhi
b
LAST
39
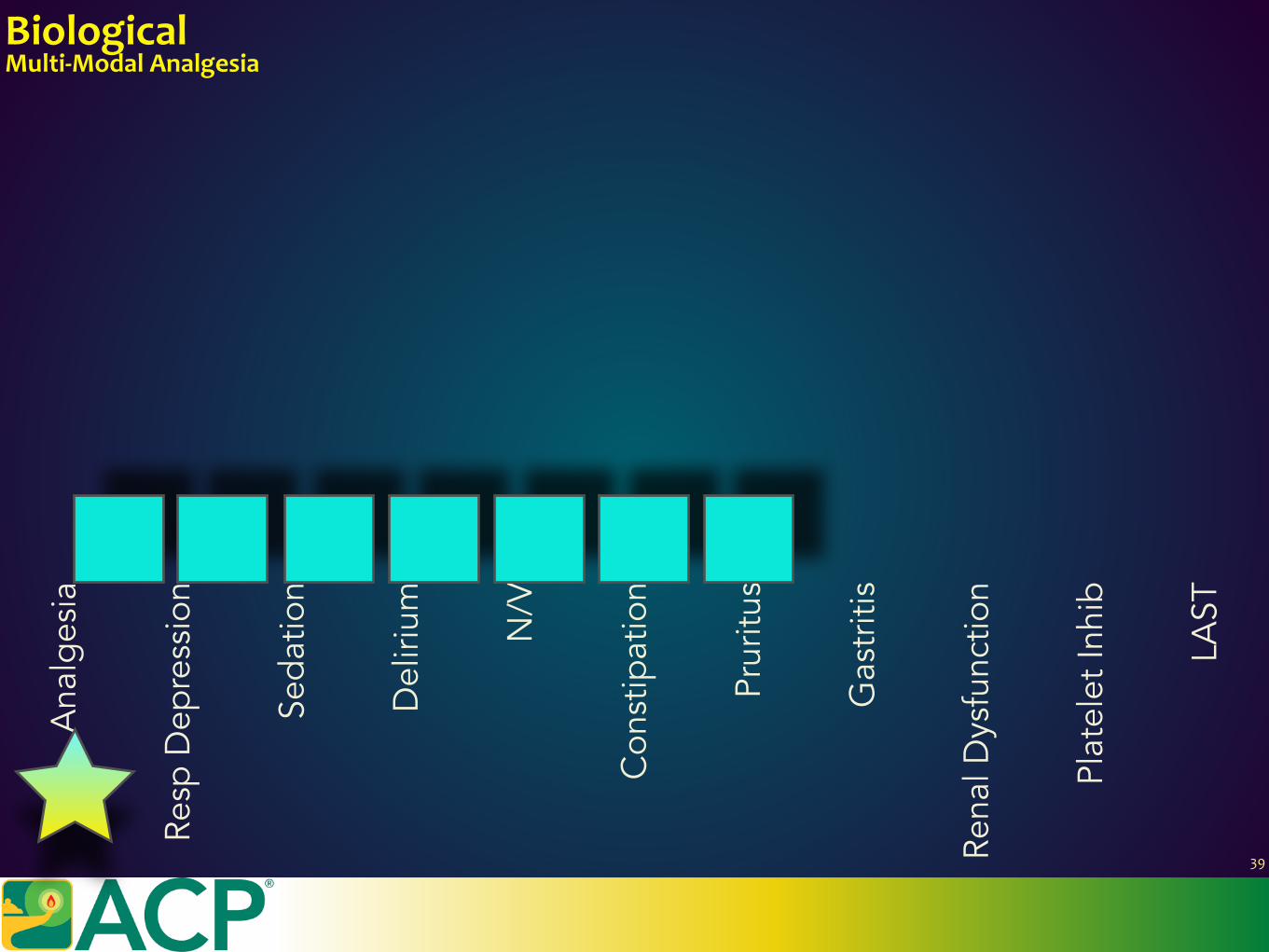
BiologicalMulti-ModalAnalgesia
Ana
lges
ia
Resp
Dep
ress
ion
Seda
tion
Del
irium
N/V
Con
stip
atio
n
Prur
itus
Gas
triti
s
Rena
l Dys
func
tion
Plat
elet
Inhi
b
LAST
39
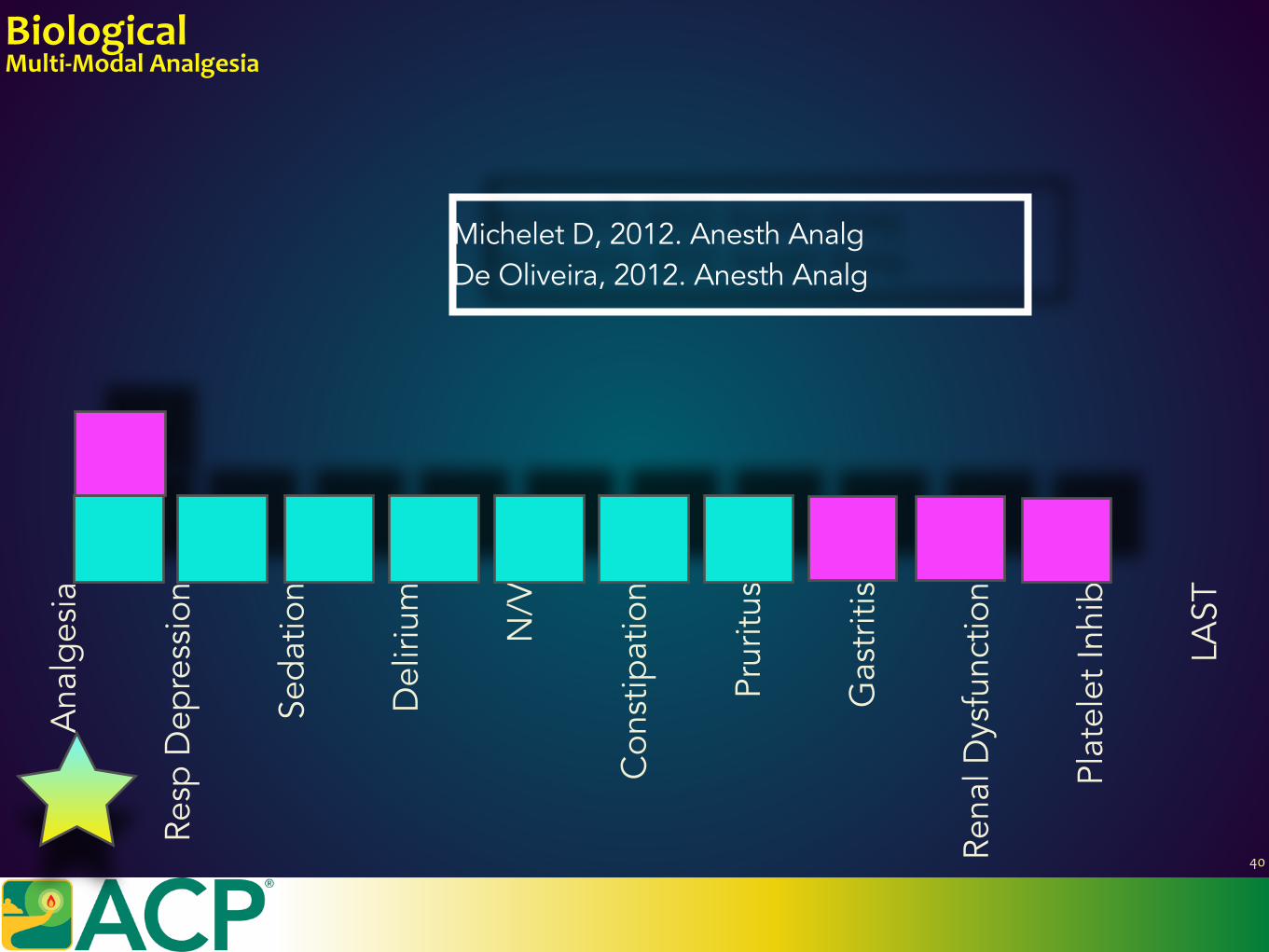
BiologicalMulti-ModalAnalgesia
Ana
lges
ia
Resp
Dep
ress
ion
Seda
tion
Del
irium
N/V
Con
stip
atio
n
Prur
itus
Gas
triti
s
Rena
l Dys
func
tion
Plat
elet
Inhi
b
LAST
Michelet D, 2012. Anesth Analg De Oliveira, 2012. Anesth Analg
40
BiologicalMulti-ModalAnalgesia
Ana
lges
ia
Resp
Dep
ress
ion
Seda
tion
Del
irium
N/V
Con
stip
atio
n
Prur
itus
Gas
triti
s
Rena
l Dys
func
tion
Plat
elet
Inhi
b
LAST
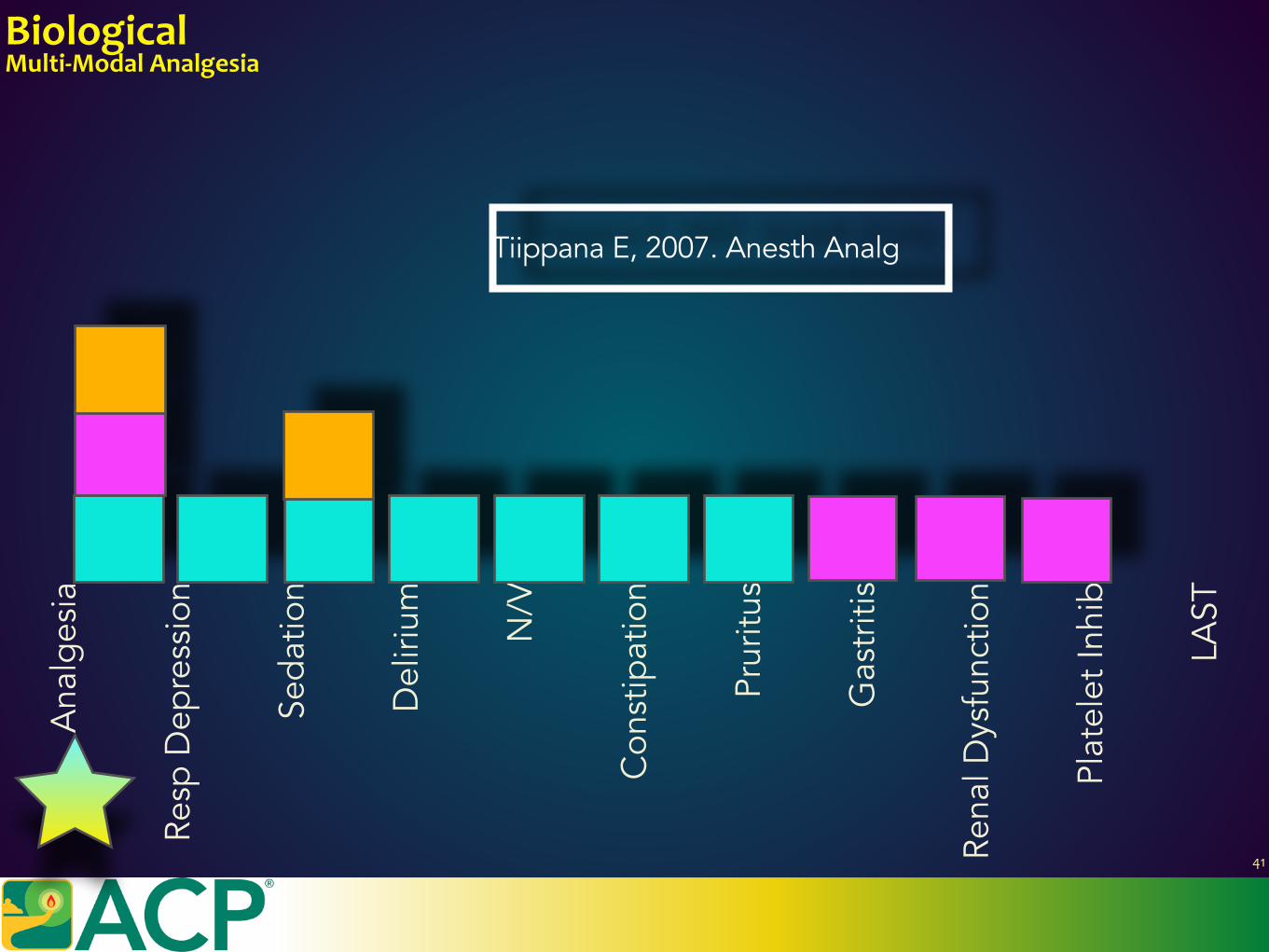
Tiippana E, 2007. Anesth Analg
41
BiologicalMulti-ModalAnalgesia
Ana
lges
ia
Resp
Dep
ress
ion
Seda
tion
Del
irium
N/V
Con
stip
atio
n
Prur
itus
Gas
triti
s
Rena
l Dys
func
tion
Plat
elet
Inhi
b
LAST
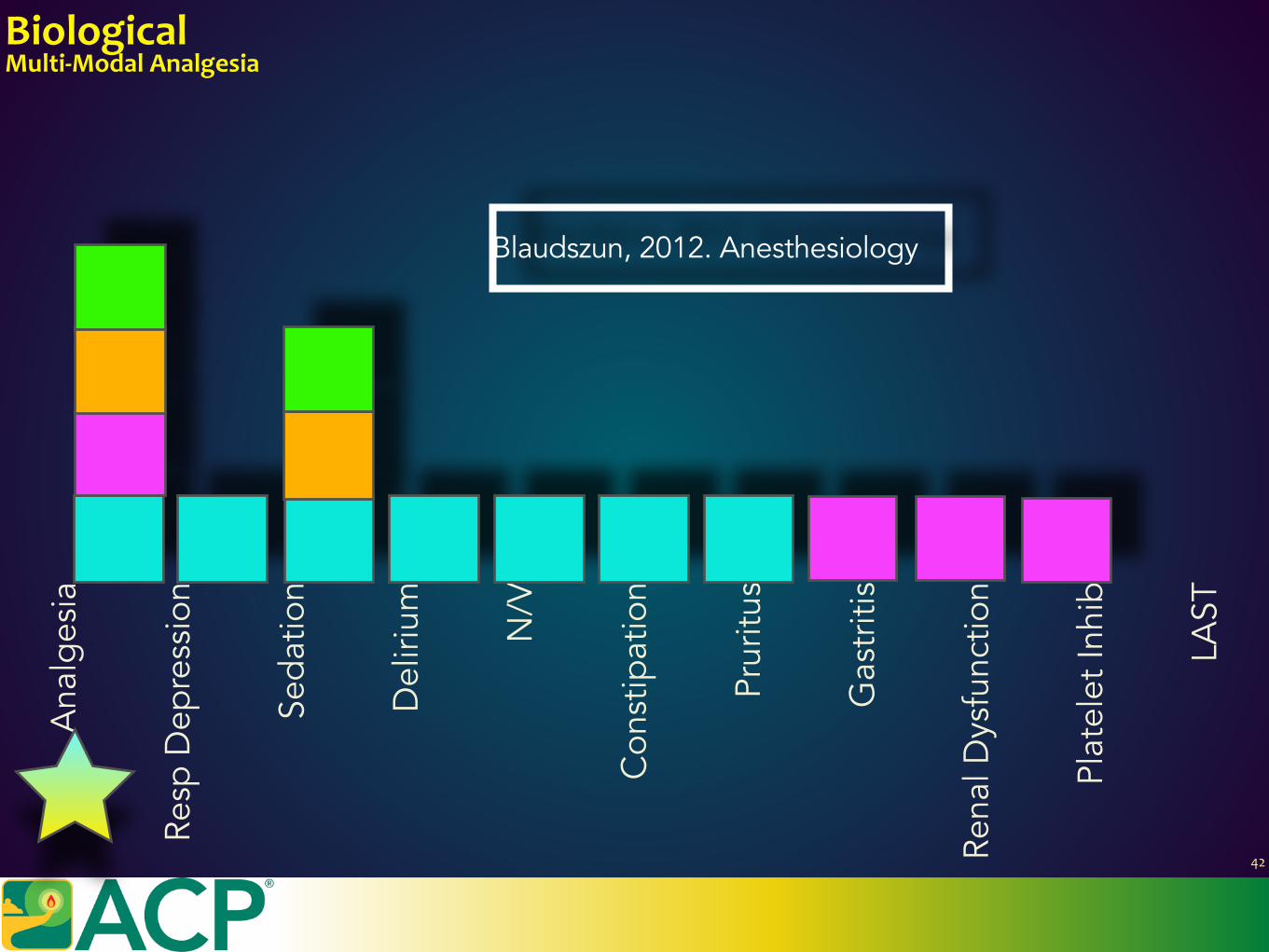
Blaudszun, 2012. Anesthesiology
42
BiologicalMulti-ModalAnalgesia
Ana
lges
ia
Resp
Dep
ress
ion
Seda
tion
Del
irium
N/V
Con
stip
atio
n
Prur
itus
Gas
triti
s
Rena
l Dys
func
tion
Plat
elet
Inhi
b
LAST
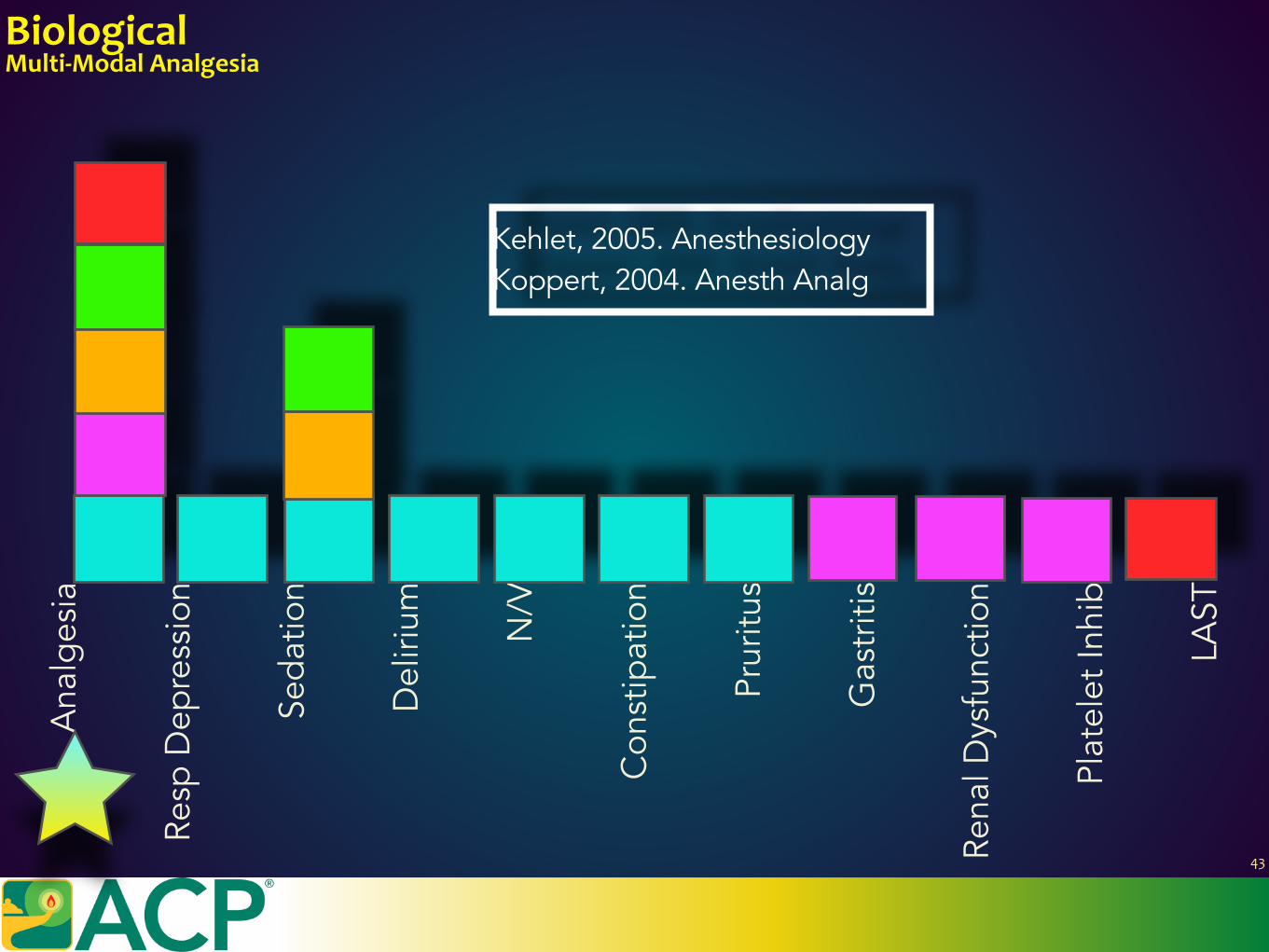
Kehlet, 2005. Anesthesiology Koppert, 2004. Anesth Analg
43
BiologicalMulti-ModalAnalgesia
Ana
lges
ia
Resp
Dep
ress
ion
Seda
tion
Del
irium
N/V
Con
stip
atio
n
Prur
itus
Gas
triti
s
Rena
l Dys
func
tion
Plat
elet
Inhi
b
LAST
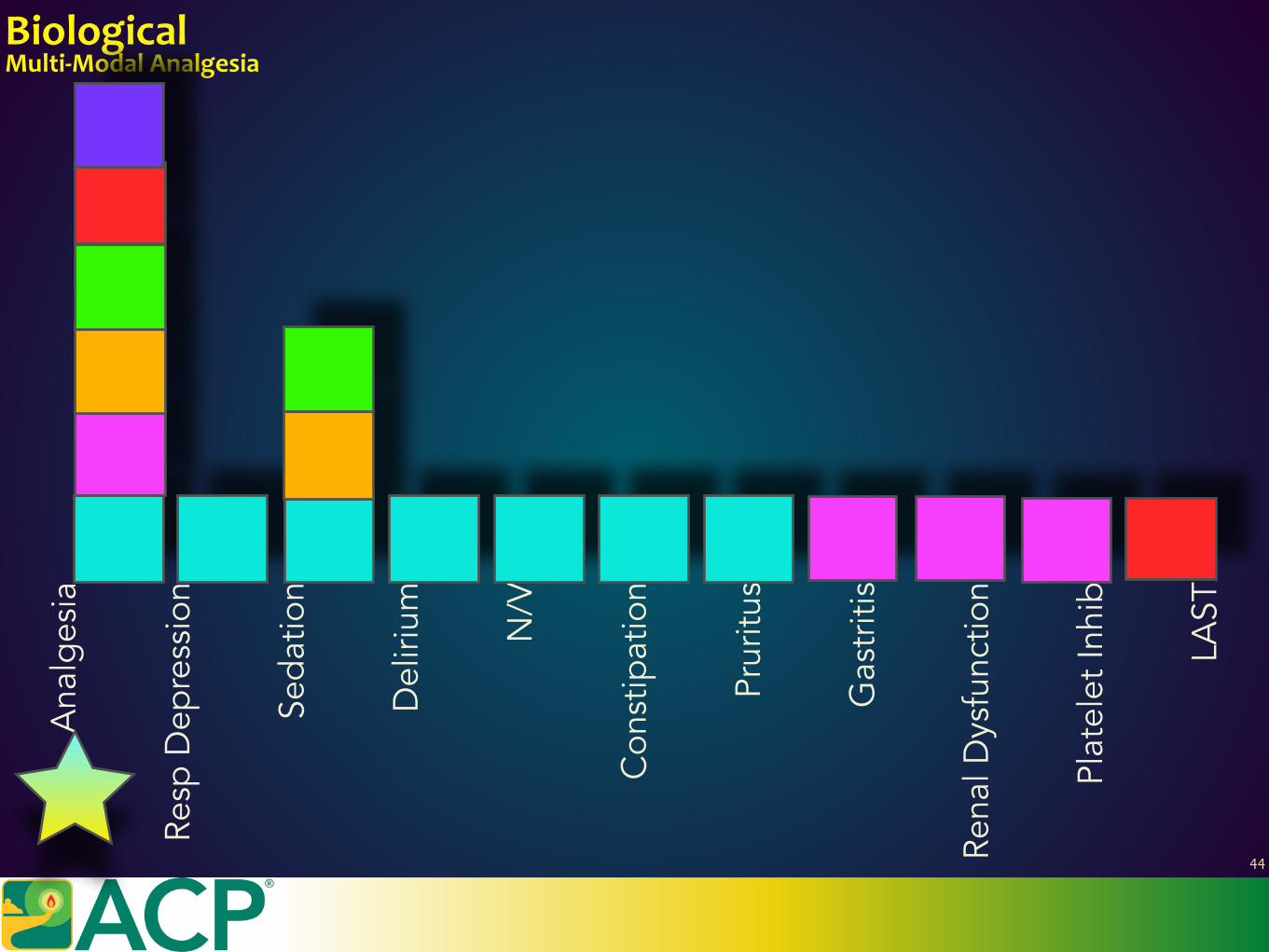
44
BiologicalMulti-ModalAnalgesia
Ana
lges
ia
Resp
Dep
ress
ion
Seda
tion
Del
irium
N/V
Con
stip
atio
n
Prur
itus
Gas
triti
s
Rena
l Dys
func
tion
Plat
elet
Inhi
b
LAST
BiologicalMulti-ModalAnalgesia
Ana
lges
ia
Resp
Dep
ress
ion
Seda
tion
Del
irium
N/V
Con
stip
atio
n
Prur
itus
Gas
triti
s
Rena
l Dys
func
tion
Plat
elet
Inhi
b
LAST
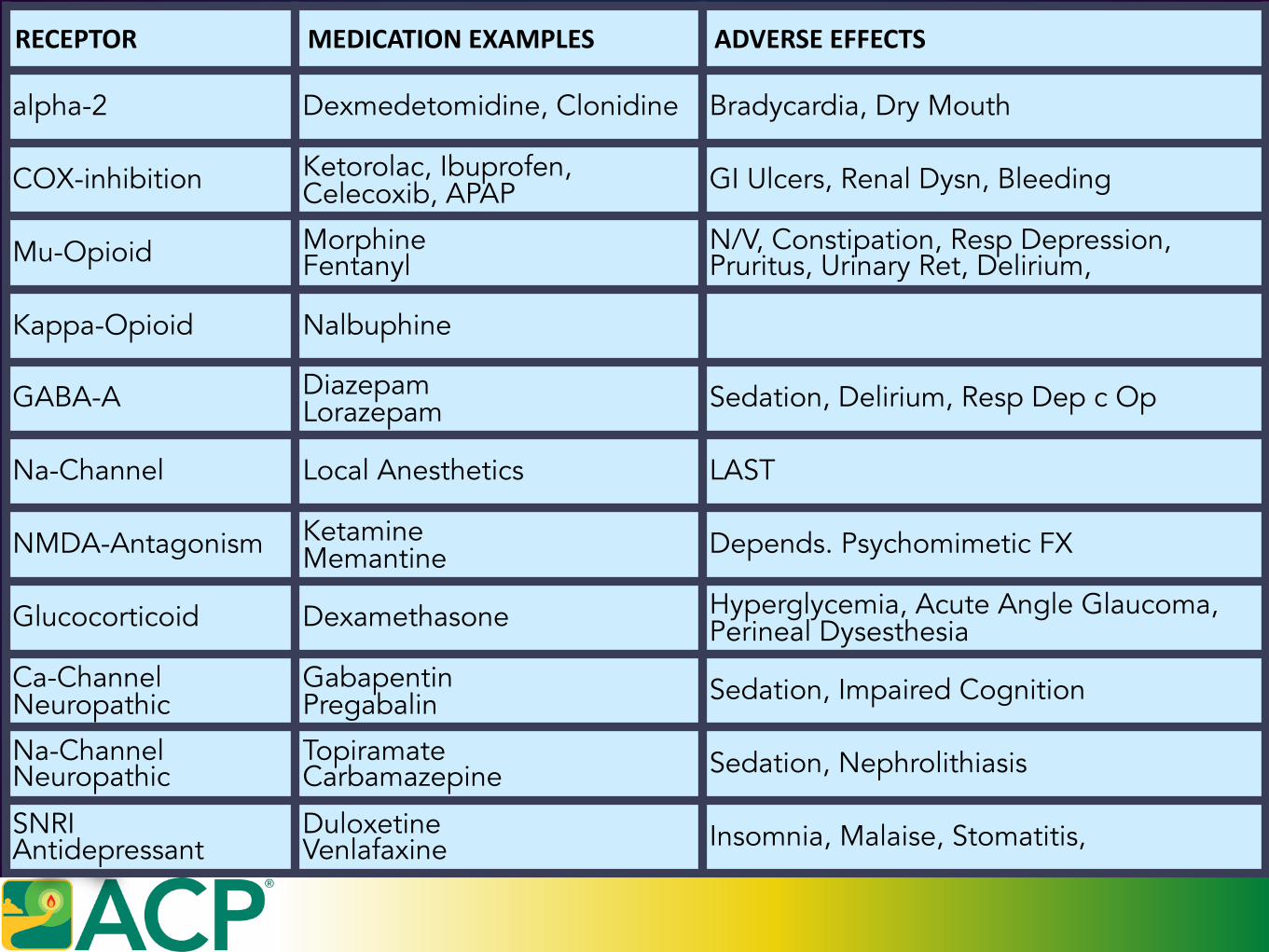
RECEPTOR MEDICATIONEXAMPLES ADVERSEEFFECTS
alpha-2 Dexmedetomidine, Clonidine Bradycardia, Dry Mouth
COX-inhibition Ketorolac, Ibuprofen, Celecoxib, APAP GI Ulcers, Renal Dysn, Bleeding
Mu-Opioid Morphine Fentanyl
N/V, Constipation, Resp Depression, Pruritus, Urinary Ret, Delirium,
Kappa-Opioid Nalbuphine
GABA-A Diazepam Lorazepam Sedation, Delirium, Resp Dep c Op
Na-Channel Local Anesthetics LAST
NMDA-Antagonism Ketamine Memantine Depends. Psychomimetic FX
Glucocorticoid Dexamethasone Hyperglycemia, Acute Angle Glaucoma, Perineal Dysesthesia
Ca-Channel Neuropathic
Gabapentin Pregabalin Sedation, Impaired Cognition
Na-Channel Neuropathic
Topiramate Carbamazepine Sedation, Nephrolithiasis
SNRI Antidepressant
Duloxetine Venlafaxine Insomnia, Malaise, Stomatitis,
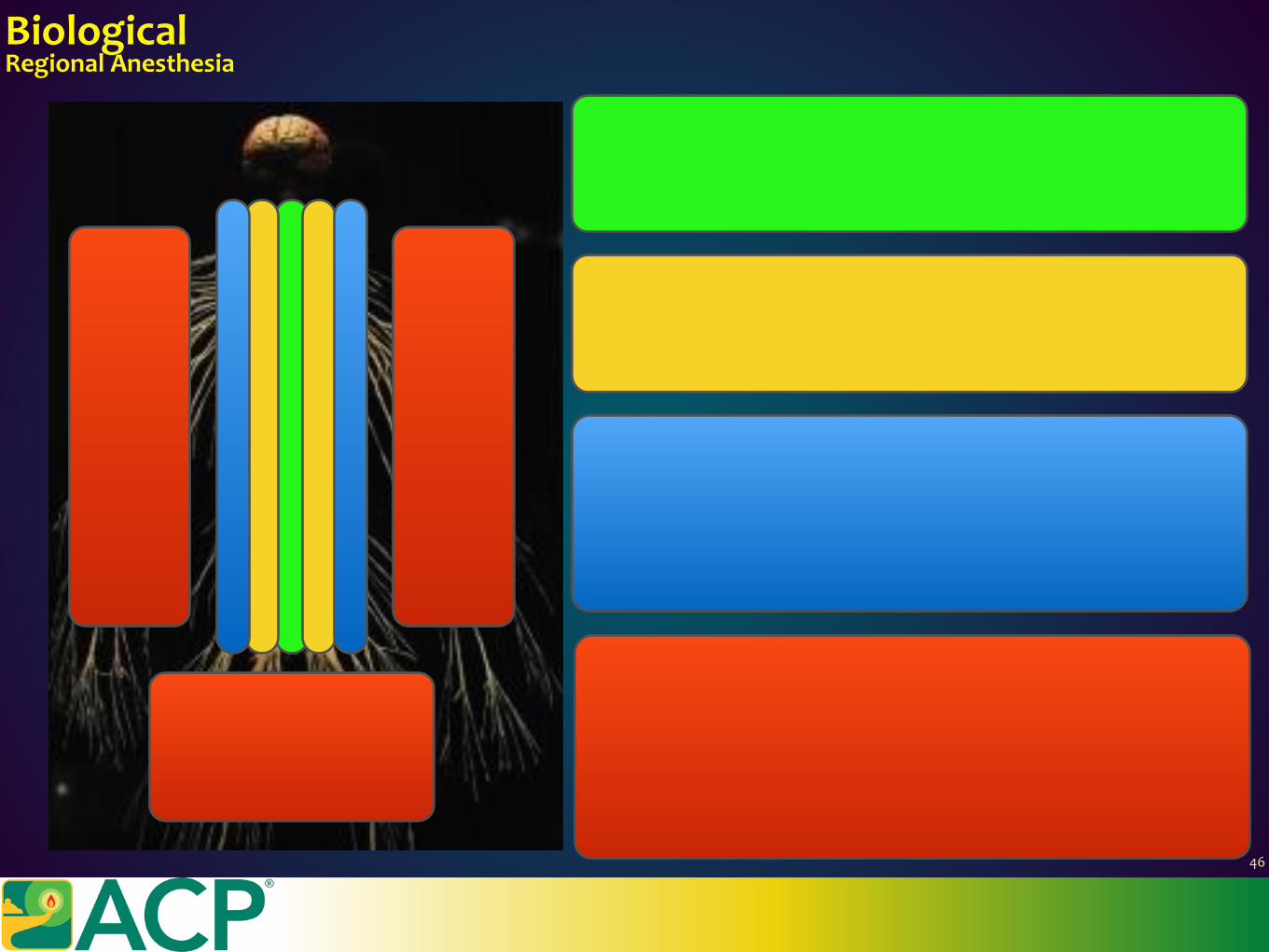
BiologicalRegionalAnesthesia
NEURAXIAL Intrathecal Epidural,Caudal
PARA-NEURAXIAL Paravertebral LumbarPlexus
PROXIMALPERIPHERALNERVE Interscalene,Supraclavicular,Infraclavicular Intercostal TransversusAbdominisPlane(TAP)
DISTALPERIPHERALNERVE Median,Radial,Ulnar Femoral,Saphenous Sciatic,Tibial,CommonPeroneal
46

Regionalanesthesiaisthemostimpactfulmodalityofacutepainmanagement.Itcaneliminateacutepain.
Regionalanesthesiacansignificantlyreduceopioidconsumption
Regionalanesthesiareducesthedevelopmentofchronicpainaftersurgery.
Epiduralanalgesiareducespersistentpost-surgicalpainafterthoracotomy Paravertebralanalgesiareduespersistentpost-surgicalpainaftermastectomy
Risksincludenerveinjury,hematoma,infectiouscomplications,localanestheticsystemictoxicity,cardiovascularcollapse,anaphylaxis
BiologicalRegionalAnesthesia
Andreae,M.H.&Andreae,D.A.Regionalanaesthesiatopreventchronicpainaftersurgery:ACochranesystematicreviewandmeta-analysis.Br.J.Anaesth.111,711–720(2013).
47
BiologicalComplementaryandIntegrativeMedicine
MUSICTOUCH
MASSAGEACUPUNCTUREACUPRESSURE
HYPNOSISBIOFEEDBACK
GUIDEDIMAGERYDISTRACTIONCREATIVEARTS
HERBALTHERAPYHOMEOPATHY
48
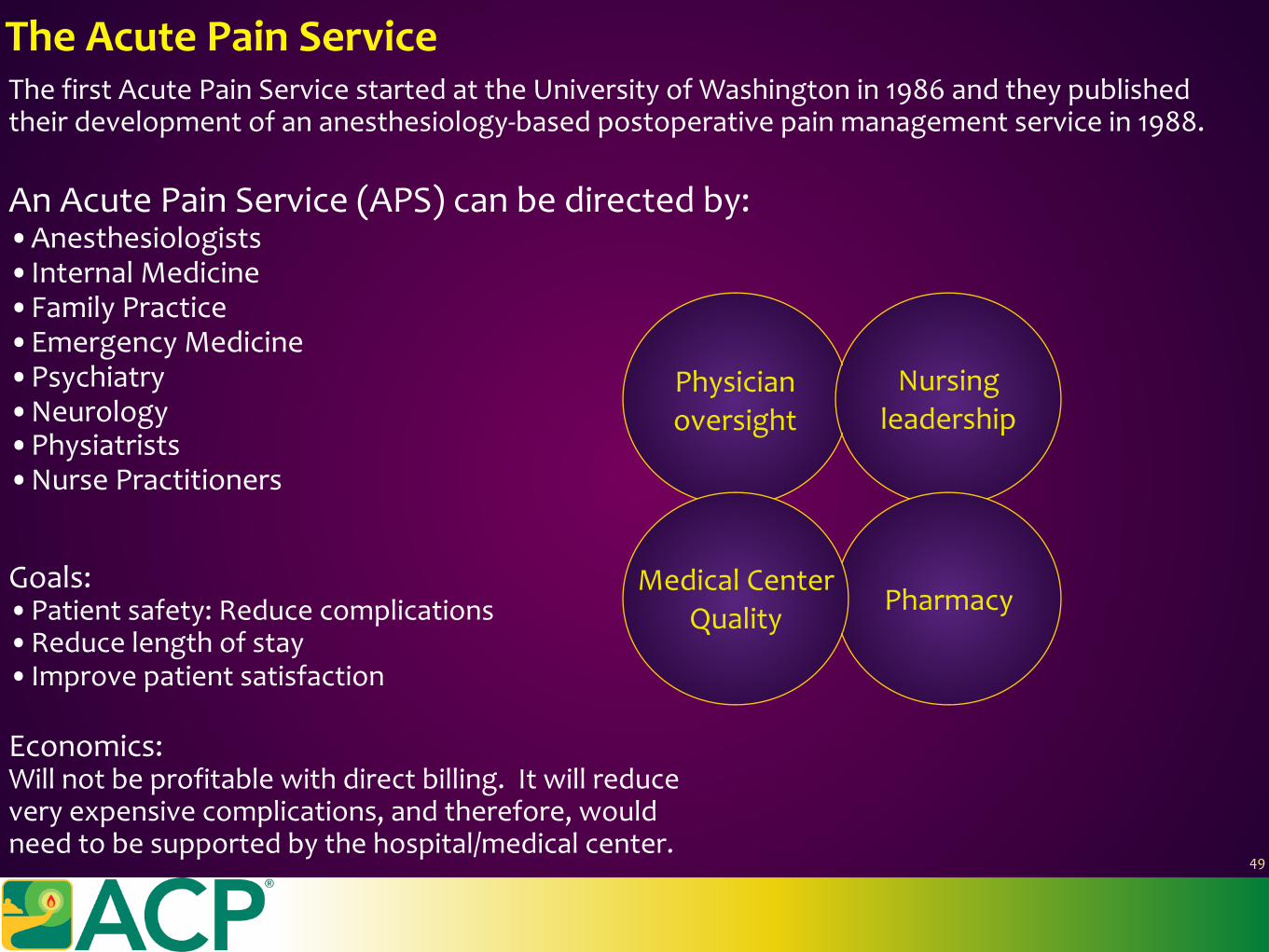
ThefirstAcutePainServicestartedattheUniversityofWashingtonin1986andtheypublishedtheirdevelopmentofananesthesiology-basedpostoperativepainmanagementservicein1988.
AnAcutePainService(APS)canbedirectedby:•Anesthesiologists•InternalMedicine•FamilyPractice•EmergencyMedicine•Psychiatry•Neurology•Physiatrists•NursePractitioners
TheAcutePainService
Physicianoversight
Nursingleadership
PharmacyMedicalCenter
QualityGoals:•Patientsafety:Reducecomplications•Reducelengthofstay•Improvepatientsatisfaction
Economics:Willnotbeprofitablewithdirectbilling.Itwillreduceveryexpensivecomplications,andtherefore,wouldneedtobesupportedbythehospital/medicalcenter.
49
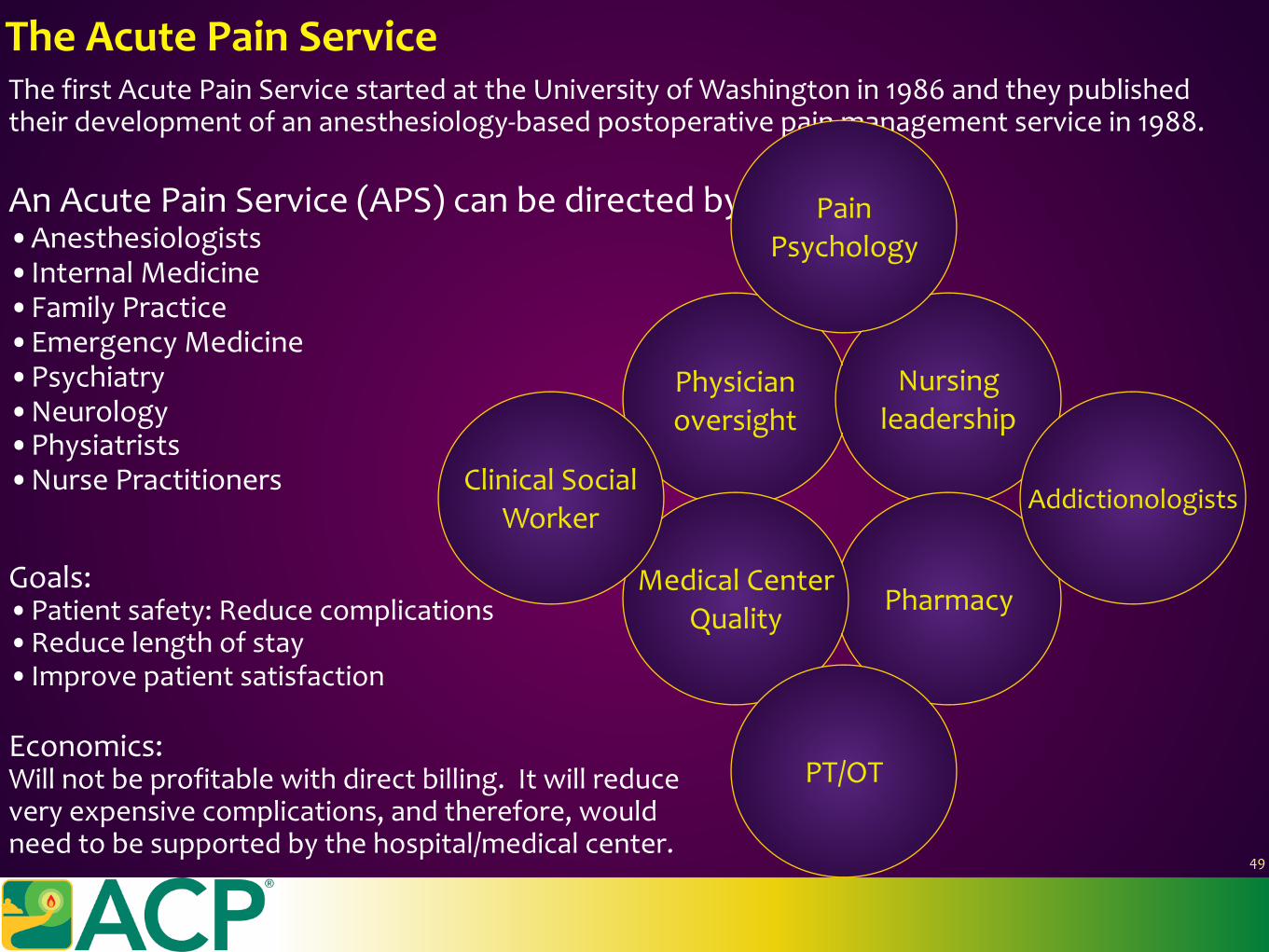
ThefirstAcutePainServicestartedattheUniversityofWashingtonin1986andtheypublishedtheirdevelopmentofananesthesiology-basedpostoperativepainmanagementservicein1988.
AnAcutePainService(APS)canbedirectedby:•Anesthesiologists•InternalMedicine•FamilyPractice•EmergencyMedicine•Psychiatry•Neurology•Physiatrists•NursePractitioners
TheAcutePainService
Physicianoversight
Nursingleadership
PharmacyMedicalCenter
Quality
PainPsychology
PT/OT
AddictionologistsClinicalSocial
Worker
Goals:•Patientsafety:Reducecomplications•Reducelengthofstay•Improvepatientsatisfaction
Economics:Willnotbeprofitablewithdirectbilling.Itwillreduceveryexpensivecomplications,andtherefore,wouldneedtobesupportedbythehospital/medicalcenter.
49

TheFutureofAcutePainMedicineGeneralMedicalEducationinPainMedicine
Mezei,L.&Murinson,B.B.PaineducationinNorthAmericanmedicalschools.J.Pain12,1199–208(2011).
WhatarethemediannumberofhoursdevotedtopaineducationinAmericanmedicalschoolsover4years?
50
TheFutureofAcutePainMedicineGeneralMedicalEducationinPainMedicine
Mezei,L.&Murinson,B.B.PaineducationinNorthAmericanmedicalschools.J.Pain12,1199–208(2011).
WhatarethemediannumberofhoursdevotedtopaineducationinAmericanmedicalschoolsover4years?
UnitedStates:9hoursCanada:19.5hours
50
TheFutureofAcutePainMedicineGeneralMedicalEducationinPainMedicine
Mezei,L.&Murinson,B.B.PaineducationinNorthAmericanmedicalschools.J.Pain12,1199–208(2011).
WhatarethemediannumberofhoursdevotedtopaineducationinAmericanmedicalschoolsover4years?
ITISACONTRIBUTINGCOMPONENTTOOUROPIOIDEPIDEMICTHISMUSTCHANGE.
UnitedStates:9hoursCanada:19.5hours
50
TheFutureofAcutePainMedicineGeneralMedicalEducationinPainMedicine
Mezei,L.&Murinson,B.B.PaineducationinNorthAmericanmedicalschools.J.Pain12,1199–208(2011).
WhatarethemediannumberofhoursdevotedtopaineducationinAmericanmedicalschoolsover4years?
ITISACONTRIBUTINGCOMPONENTTOOUROPIOIDEPIDEMICTHISMUSTCHANGE.
UnitedStates:9hoursCanada:19.5hours
ACGMEFellowshipinAcutePainMedicineandRegionalAnesthesiaStartinginJuly2017.1yeardurationafteraresidencyinanesthesiology.
50
TheFutureofAcutePainMedicineCodingandBillingInfluence.ICD-11MJ42.13
ICD-11willhaveapersistentpost-surgicalandpersistentpost-traumapaincode.Thiswillhaveanimpactintherecognitionandmanagementofchronifiedpain.
WehavenooutcomeparametersfromCMS,theJointCommission,orinsurersthatlookspecificallyatchronicpainaftersurgeryortrauma.EuropedoesbecauseofsinglepayersystemsandthisiswheremostoftheliteratureregardingPPSPorchronificationcomesfrom.
51
TheFutureofAcutePainMedicineCodingandBillingInfluence.ICD-11MJ42.13
ICD-11willhaveapersistentpost-surgicalandpersistentpost-traumapaincode.Thiswillhaveanimpactintherecognitionandmanagementofchronifiedpain.
WehavenooutcomeparametersfromCMS,theJointCommission,orinsurersthatlookspecificallyatchronicpainaftersurgeryortrauma.EuropedoesbecauseofsinglepayersystemsandthisiswheremostoftheliteratureregardingPPSPorchronificationcomesfrom.
51
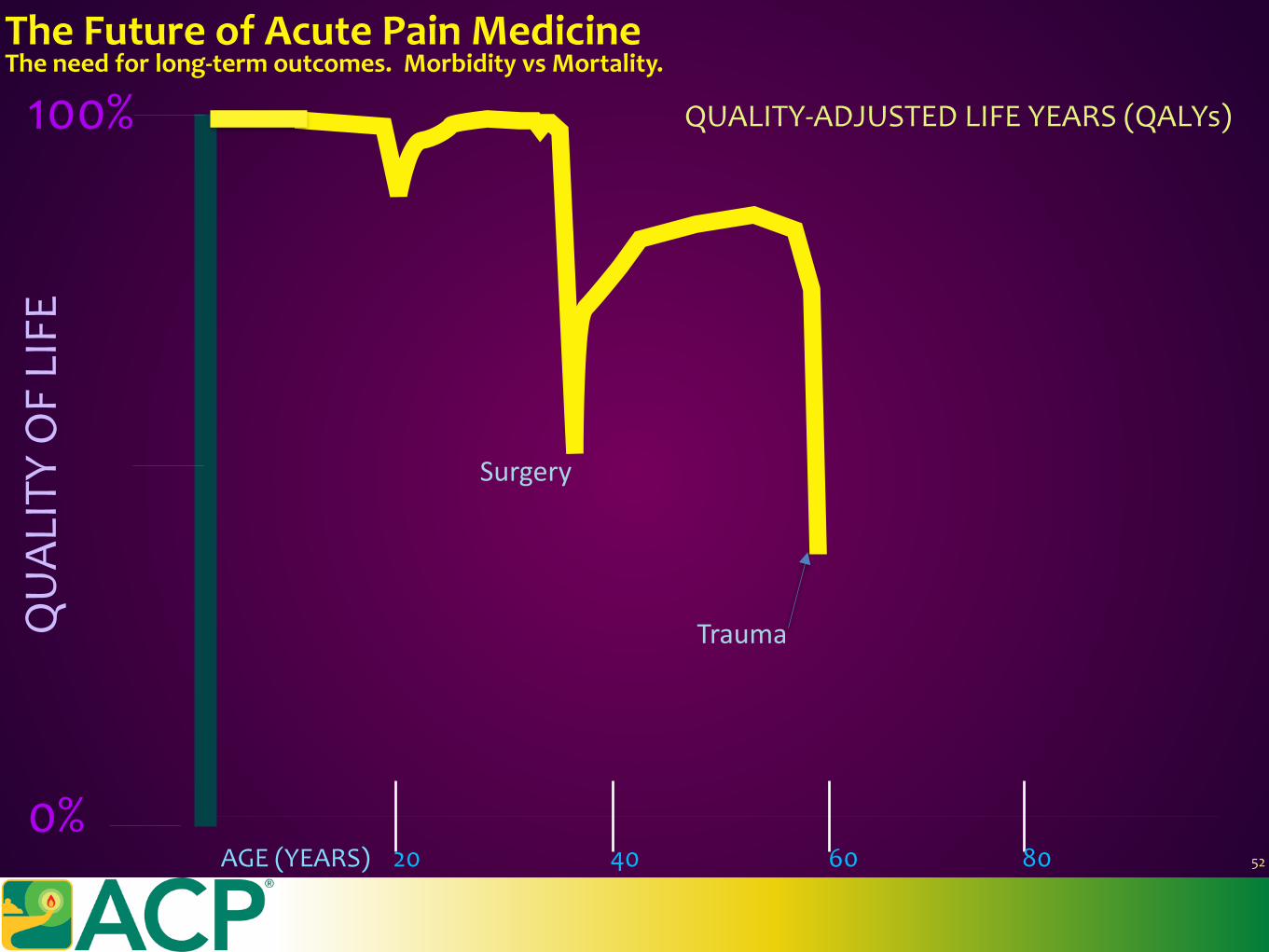
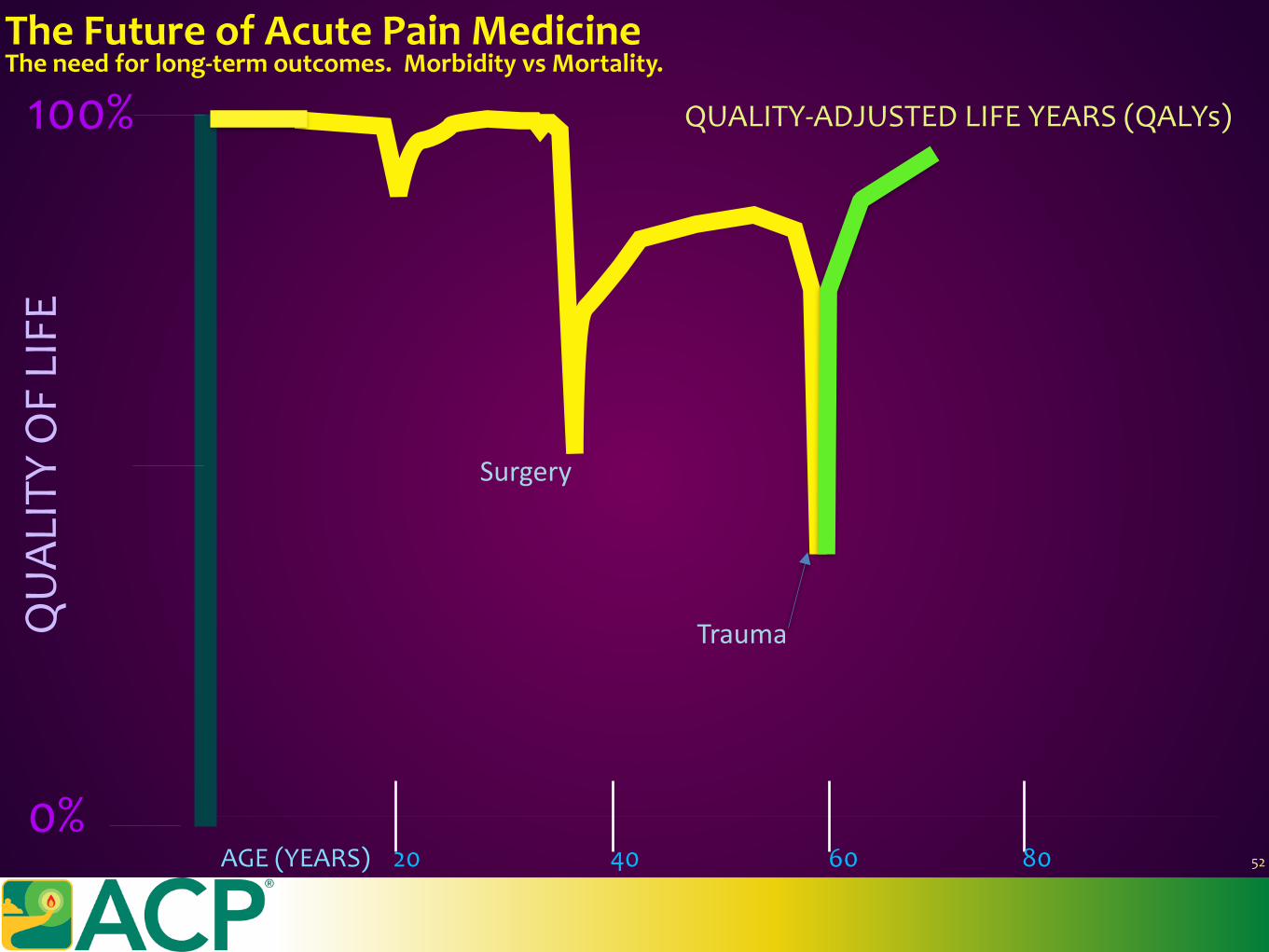
TheFutureofAcutePainMedicineTheneedforlong-termoutcomes.MorbidityvsMortality.
QUALITY-ADJUSTEDLIFEYEARS(QALYs)100%
4020 60 80AGE(YEARS)
QUAL
ITYOFLIFE
0%
Trauma
52
Surgery
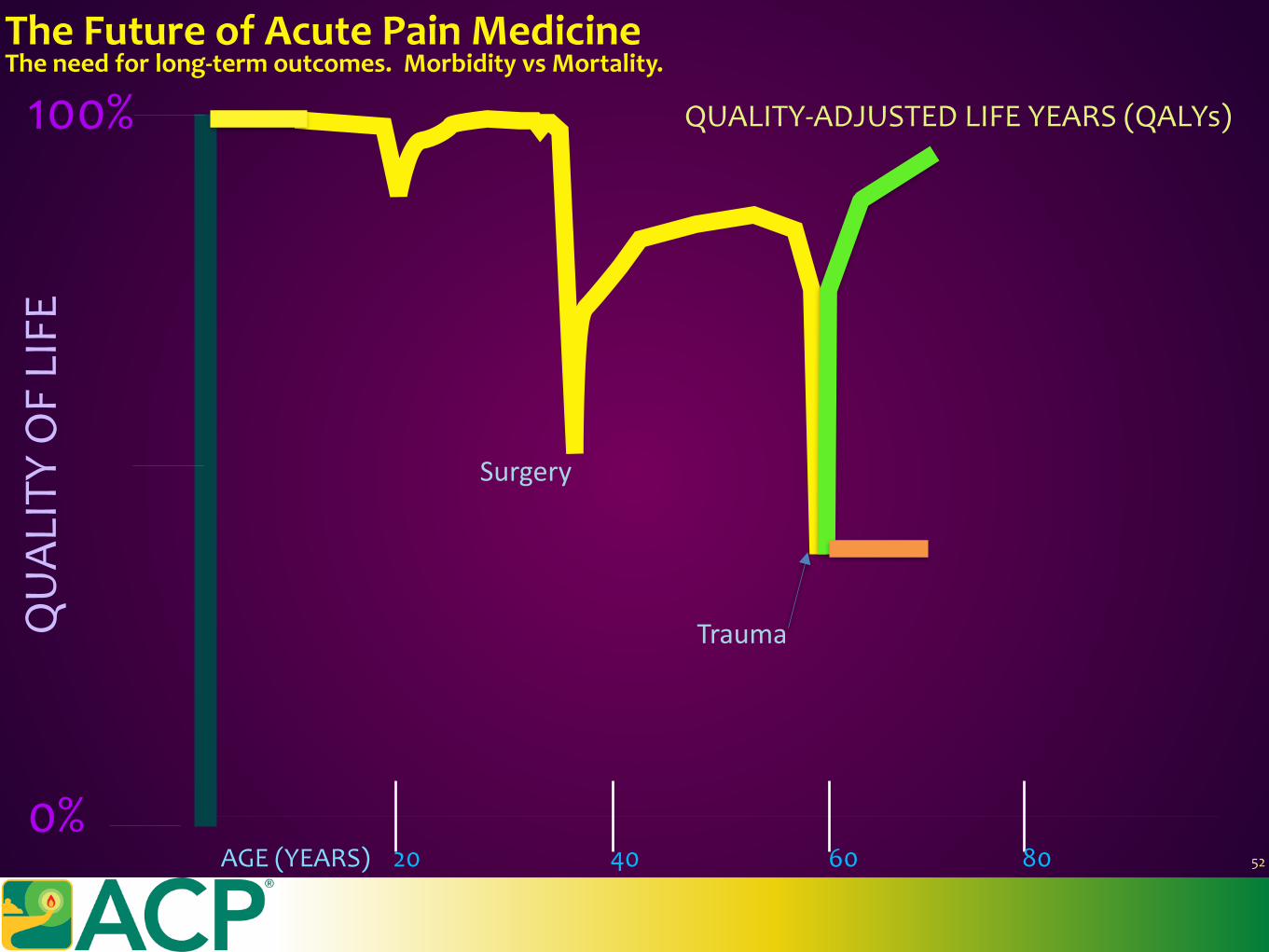
TheFutureofAcutePainMedicineTheneedforlong-termoutcomes.MorbidityvsMortality.
QUALITY-ADJUSTEDLIFEYEARS(QALYs)100%
4020 60 80AGE(YEARS)
QUAL
ITYOFLIFE
0%
Trauma
52
Surgery
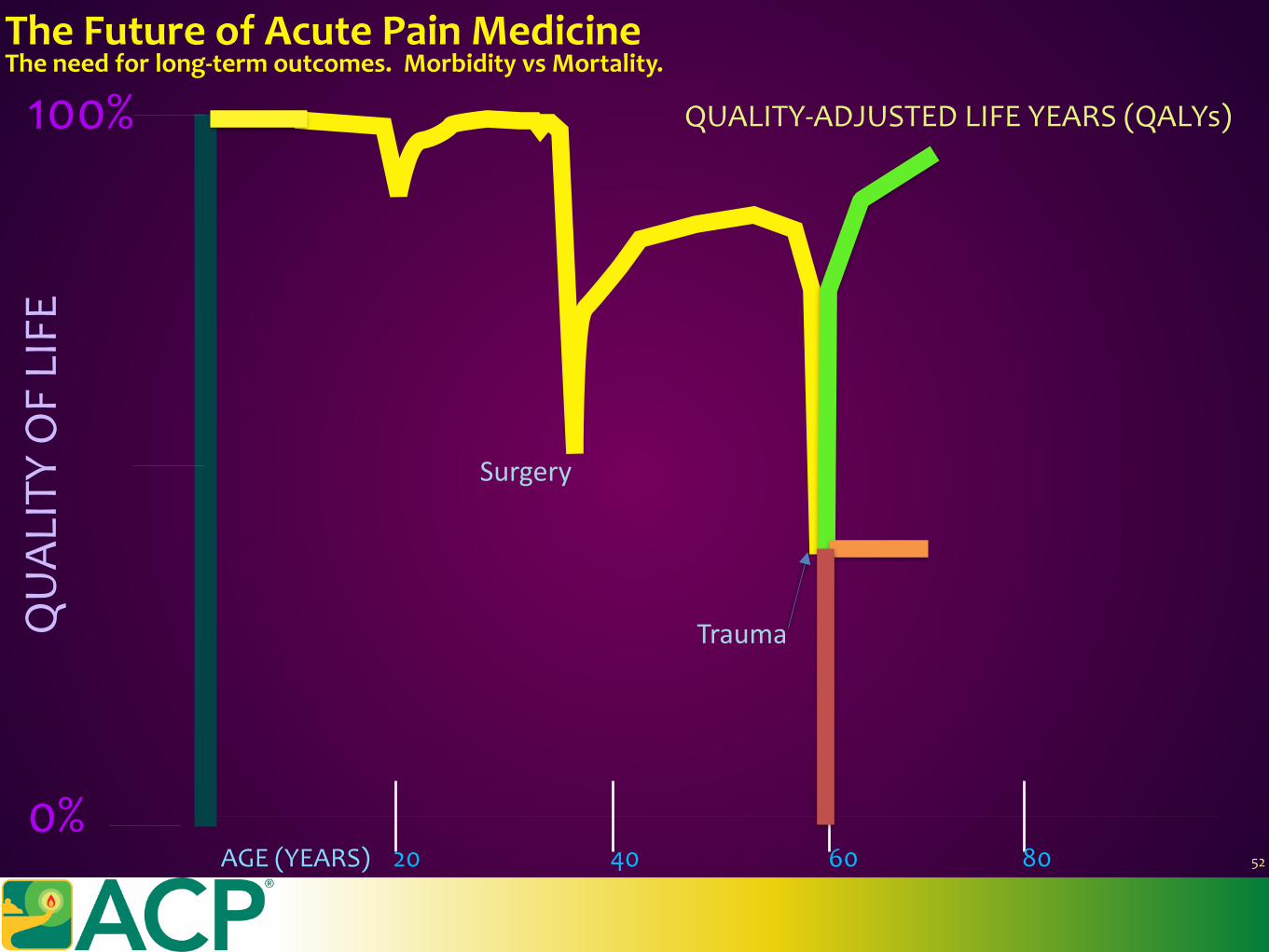
TheFutureofAcutePainMedicineTheneedforlong-termoutcomes.MorbidityvsMortality.
QUALITY-ADJUSTEDLIFEYEARS(QALYs)100%
4020 60 80AGE(YEARS)
QUAL
ITYOFLIFE
0%
Trauma
52
Surgery
TheFutureofAcutePainMedicineTheneedforlong-termoutcomes.MorbidityvsMortality.
QUALITY-ADJUSTEDLIFEYEARS(QALYs)100%
4020 60 80AGE(YEARS)
QUAL
ITYOFLIFE
0%
Trauma
52
Surgery

TheFutureofAcutePainMedicineTheneedforlong-termoutcomes.MorbidityvsMortality.
QUALITY-ADJUSTEDLIFEYEARS(QALYs)100%
4020 60 80AGE(YEARS)
QUAL
ITYOFLIFE
0%
Trauma
52
Surgery
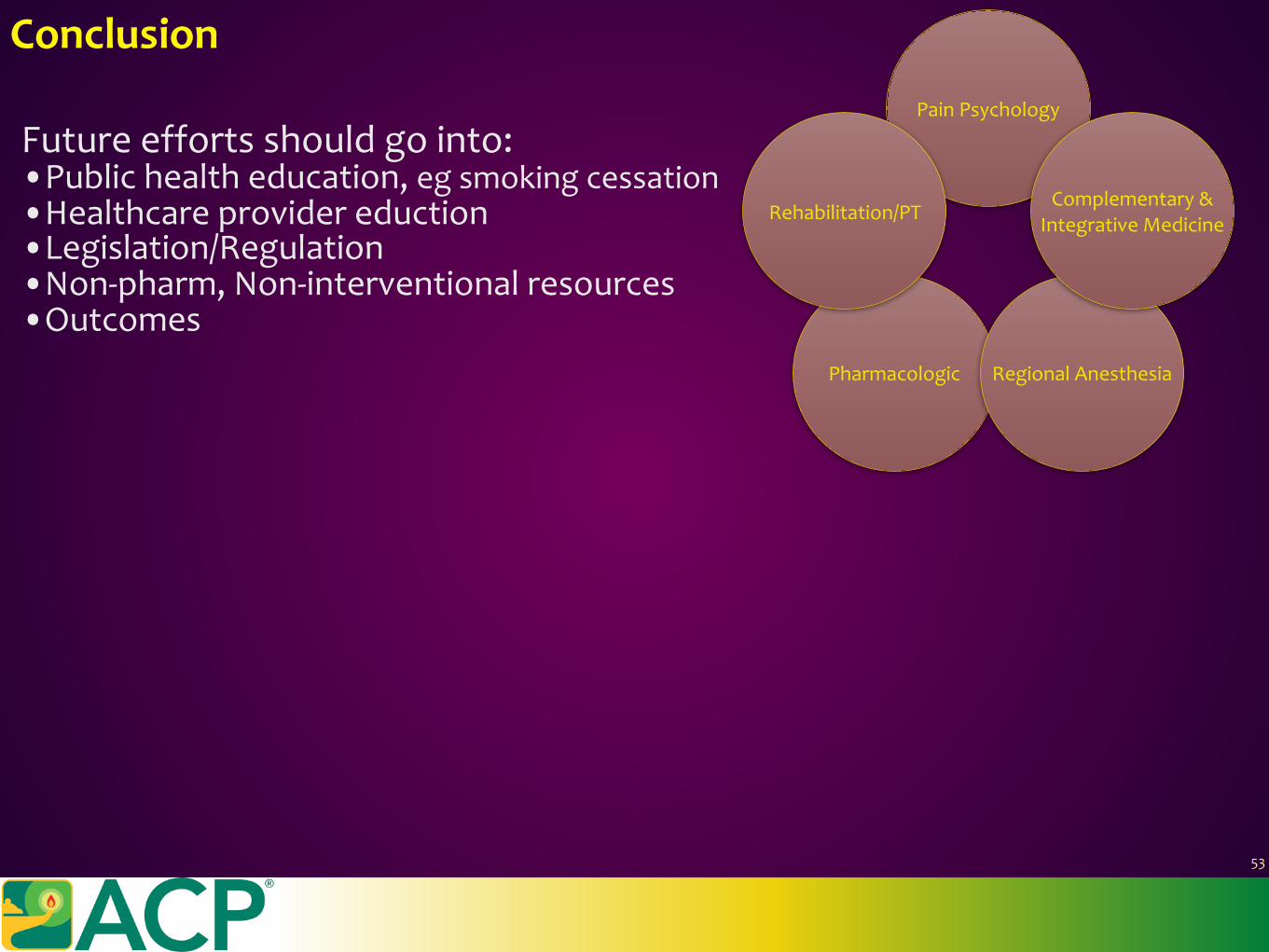
Conclusion
53
Pharmacologic RegionalAnesthesia
PainPsychology
Rehabilitation/PTComplementary&
IntegrativeMedicine
Futureeffortsshouldgointo:•Publichealtheducation,egsmokingcessation•Healthcareprovidereduction•Legislation/Regulation•Non-pharm,Non-interventionalresources•Outcomes
Conclusion
53
Pharmacologic RegionalAnesthesia
PainPsychology
Rehabilitation/PTComplementary&
IntegrativeMedicine
Understandthedifferencesbetweenanalgesiaandanti-hyperalgesia.
•Opioidshavearoleinacutepainmedicine,but…theyarenotthesolutiontopain.They,infact,canmakepainworseovertime.
•MultimodalAnalgesiaisimportanttoreduceconsequentialsideeffects•Non-PharmandNon-Interventionalmodalitiesshouldalwaysbeused.•Regionalanesthesiacanbeimpactful,thoughmustweighrisks.•GoalsaretoMANAGEPAINandPREVENTCHRONICPAIN
Futureeffortsshouldgointo:•Publichealtheducation,egsmokingcessation•Healthcareprovidereduction•Legislation/Regulation•Non-pharm,Non-interventionalresources•Outcomes
Conclusion
53
Pharmacologic RegionalAnesthesia
PainPsychology
Rehabilitation/PTComplementary&
IntegrativeMedicine
Understandthedifferencesbetweenanalgesiaandanti-hyperalgesia.
•Opioidshavearoleinacutepainmedicine,but…theyarenotthesolutiontopain.They,infact,canmakepainworseovertime.
•MultimodalAnalgesiaisimportanttoreduceconsequentialsideeffects•Non-PharmandNon-Interventionalmodalitiesshouldalwaysbeused.•Regionalanesthesiacanbeimpactful,thoughmustweighrisks.•GoalsaretoMANAGEPAINandPREVENTCHRONICPAIN
Futureeffortsshouldgointo:•Publichealtheducation,egsmokingcessation•Healthcareprovidereduction•Legislation/Regulation•Non-pharm,Non-interventionalresources•Outcomes
ThankYou
Questions?
54
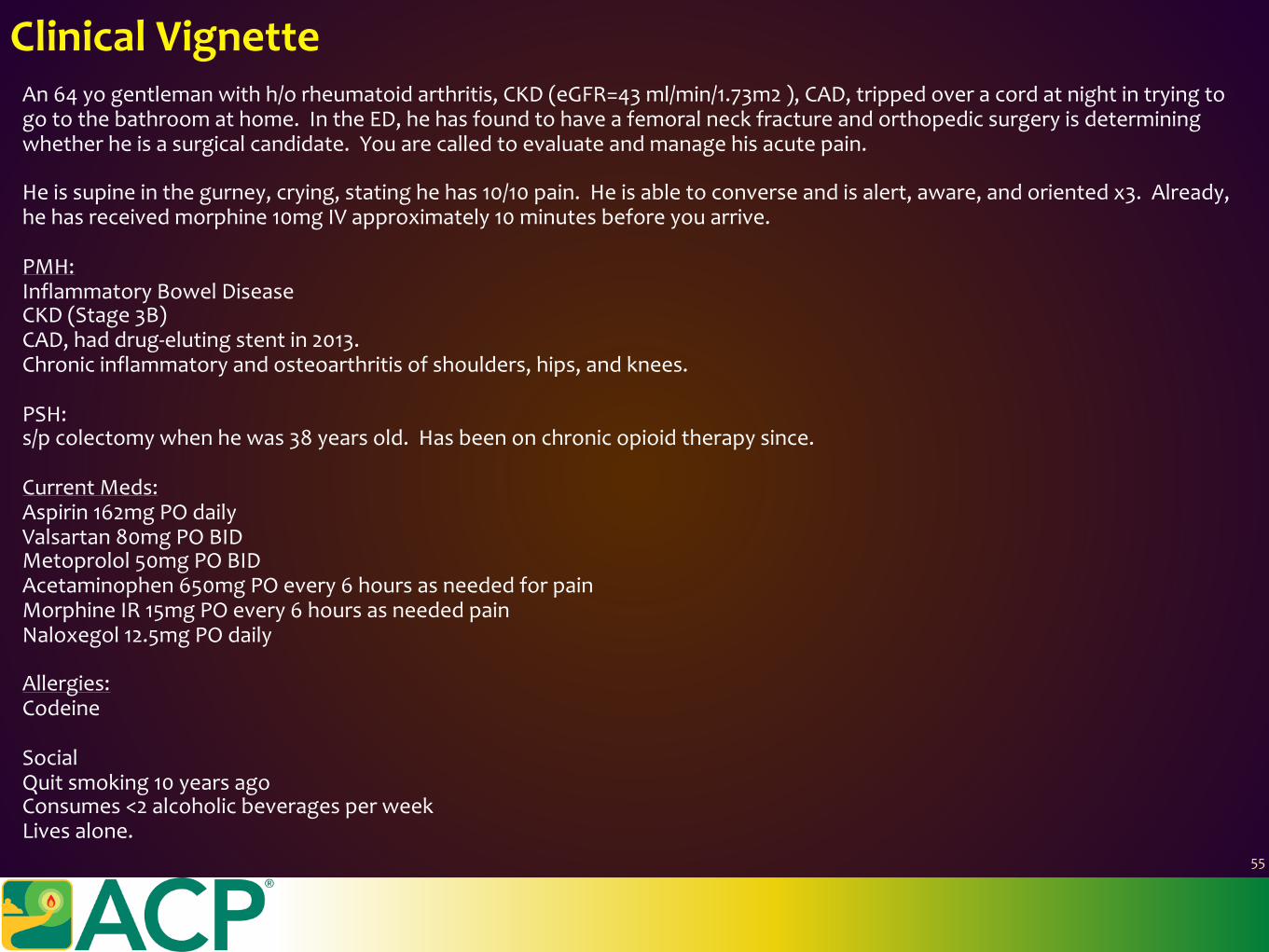
An64yogentlemanwithh/orheumatoidarthritis,CKD(eGFR=43ml/min/1.73m2),CAD,trippedoveracordatnightintryingtogotothebathroomathome.IntheED,hehasfoundtohaveafemoralneckfractureandorthopedicsurgeryisdeterminingwhetherheisasurgicalcandidate.Youarecalledtoevaluateandmanagehisacutepain.
Heissupineinthegurney,crying,statinghehas10/10pain.Heisabletoconverseandisalert,aware,andorientedx3.Already,hehasreceivedmorphine10mgIVapproximately10minutesbeforeyouarrive.
PMH:InflammatoryBowelDiseaseCKD(Stage3B)CAD,haddrug-elutingstentin2013.Chronicinflammatoryandosteoarthritisofshoulders,hips,andknees.
PSH:s/pcolectomywhenhewas38yearsold.Hasbeenonchronicopioidtherapysince.
CurrentMeds:Aspirin162mgPOdailyValsartan80mgPOBIDMetoprolol50mgPOBIDAcetaminophen650mgPOevery6hoursasneededforpainMorphineIR15mgPOevery6hoursasneededpainNaloxegol12.5mgPOdaily
Allergies:Codeine
SocialQuitsmoking10yearsagoConsumes<2alcoholicbeveragesperweekLivesalone.
ClinicalVignette
55
Whatisyournextstepformanaginghisacutepain?
ClinicalVignette
56
Whatisyournextstepformanaginghisacutepain?
ClinicalVignette
56
Possiblequestions:1)Askhimonaveragehowmuchmorphineoranyotheropioidheconsumes?Answer:“Itakethemorphine15mg4timesaday.ButIusedtobeOxyContin40mgPO3timesadaylikeamonthago.”WhatarehisOMEs?Isthathighrisk?WhatistheOMEofwhathereceived,morphine10mgIV?
2)Whereisyourpain?Answer:“Myhipandthighandshoulder…”
3)Canyoudescribethesethreepains?Whichoneistheworst?Answer:“Theshoulderfeelsachy,it’snotbadthough.Thehipisasharpstabbingpainandthethighisastrongache.It’s10/10,canyougetmesomething?”
4)Whydoyoutakemorphineonadailybasis?Answer:“ShoulderpainI’vehadforyears.”
5)Areyoutakinganybloodthinnersbesidestheaspirin?Answer:No
6)Doyouhaveanyonewholiveswithyouorsupportsyou?Answer:“Myex-wife.Theyalreadycalledherandsheiscomingin.”
6)Consider:Regionalanesthesia,low-doseketamineinfusion,acetaminophen,oralopioidtherapythatmustbeatleastwhathewastakingathome.WouldyougiveaCOX-inhibitor?Wouldyougiveagabapentinoid?Youcanconsiderlidocaine,dexmedetomidineaswell,buttheseshouldonlybeusedintheICU,andarenotwarrantedunlesspainwastoodifficulttomanagewiththecurrentregimen.Ice/heat,music,guidedimagery,therapydog,possiblyacupuncture/acupressure,psychologicalevaluationandsocialworkerevaluation.
ClinicalVignette
57
Hehasafasciailiacacatheterplacedandthenextmorninghehasafemoralintramedullarynailplacedbyorthopedicsurgery.Post-operatively,thefasciailiacacatheterisre-inserted.Hehasbeenmaintainedonlow-doseketamineandistakingmorphineIR15mgevery4hoursasneeded.
HeisdoingwellwithPT/function,satisfaction,POD0,1,andistoldhecangohomeonPOD2withhomehealth.
Theanesthesiologistremovestheregionalanesthesiacatheter,youstoptheketamineinfusion,andhestatesthepainhasreturnedto7/10.
Whatdoyoudo?
ClinicalVignette
57
Hehasafasciailiacacatheterplacedandthenextmorninghehasafemoralintramedullarynailplacedbyorthopedicsurgery.Post-operatively,thefasciailiacacatheterisre-inserted.Hehasbeenmaintainedonlow-doseketamineandistakingmorphineIR15mgevery4hoursasneeded.
HeisdoingwellwithPT/function,satisfaction,POD0,1,andistoldhecangohomeonPOD2withhomehealth.
Theanesthesiologistremovestheregionalanesthesiacatheter,youstoptheketamineinfusion,andhestatesthepainhasreturnedto7/10.
Whatdoyoudo?YouincreasethemorphineIRto15-30mgPOq4hPRN.
Whatdoyoutellhimondischarge?Opioidconsumptionreduction,Opioid-inducedhyperalgesia,DiscussopioidweaningwithyoursurgeonandPCPIsheaddicted?Screeningtools(COMM)canbeusedbyhisPCPWouldyougivehimCOX-inhibitorsnow?Whatabouttakingthemwithhisaspirin?Wouldyougivehimanythingelsebesidesacetaminophenandmorphine?Gabapentin?Whatwouldyoudoforhischronicshoulderpain?