Management of Thumb Hypoplasia - Northwestern...
25
The Pediatric Upper Extremity EPIDEMIOLOGY Conway and Bowe ~’°’ 75 have reported the incidence of congenital deformity involving the hand-forearm unit as 1 in 626 live births. Naujoks "a2 reported similar findings of 34 in 17,800 live births, and Hegdekattff z has re- ported it to be 1 in 200 live births. Major defects of development involving the thumb were reported by Entin z3 as i6% of his series of upper-limb congenital anomalies. Congenital failure of thumb formation is a rather commonly observed birth defect and may in certain cases be part of a more complicated picture: Thumb abnormalities, for example, are often seen in association with pre-axial longitu- dinal failure of formation of the radius (Fig. 1: radial agenesis) and have been reported with variable penetrance and expressivity in Lamb’s 4~ series of 117 consecutive cases. Syn- drome complexes that involve cardiovascular, genitourinary, and musculoskeletal manifesta- tions may also have associated thumb abnor- malities, including Holt-Oramsyndro~ne, Fan- toni syndrome, diastrophic dwarfism, and Cornelia deLange syndrome. Each of the three tubular bones of the thumb osteoarticular column may be affected differ- ently, depending on causative genetic or envi- r0nmental factors. Certain characteristic defor- mities reflect specific syndromes, e.g., the short, flat, broad distal phalanx of Apert’s aerocephalosyndaetyly (Fig. 2A and B) and Car- penter’s syndrome, or the slender terminal pha- 0749-0712/90 $0.00 + .20 Management of Thumb Hypoplasia William B. Kleinman, MD* langeal hypoplasia characteristic of both Holt- Oram and Faneoni syndromes. Longitudinal growth deficiency of the thumb proximal phalanx is usually not an isolated phe- nomenon and can occur in combination ~vith some type of general phalangeal growth distur- bance involving the medial fingers, e.g., braeh- ydaetyly (most commonly attributable to growth arrest of the middle phalanx) and synbraehydae- tyly (Fig. 3A-D), or more complex museulo- skeletal syndromes, such as brachydaetyly in association with absence of the sternoeostal por- tion of the peetoralis major muscle (Fig. 4: Poland’s syndrome). Congenital absence, shortness, instability, or deformity of the thumb can result potentially in profound compromise to grasp and pinch. The rationale for surgical reconstruction should .,be based on consideration not only of the func- tional, but of the emotionalimpact of the child’s congenital deformity. The demanding technical considerations involved in surgically creating an anatomic potential for grasp or pinch are only part of a decision-makingprocess; a process that might, unfortunately, include complete lack of patient cooperation. Unpredictability of growth potential in those tissues to, be used for recon- struction, and a general predisposition for re- calcitrant anatomic abnormalities encountered at the time of surgery also confuse the decision- making process. Add to this the absende of normal cerebroeortieal thumb representation, and the surgeon can readily appreeiat_e prob-_ lems inherent in functional reeonstruetion, of *Clinical Associate Professor of Orthopaedic Surgery, Indiana University School of Medicine; Director, Congenital Hand.. Service, Riley Children’s Hospital, Indiana University Medical Center; Clinical Assistant Professor of Plastic Surgery, University of Kentucky School of Medicine, Lexington, Kentucky; Attending Staff Surgeon, The Indiana Center for Surgery and Rehabilitation of the Hand and Upper Extremity, .Indianapolis, Indiana Hand Clinics--Vol. 6, No. 4, November 1990 - 617
Transcript of Management of Thumb Hypoplasia - Northwestern...

The Pediatric Upper Extremity
EPIDEMIOLOGY
Conway and Bowe~’°’ 75 have reported theincidence of congenital deformity involving thehand-forearm unit as 1 in 626 live births.Naujoks"a2 reported similar findings of 34 in17,800 live births, and Hegdekattffz has re-ported it to be 1 in 200 live births. Majordefects of development involving the thumbwere reported by Entinz3 as i6% of his seriesof upper-limb congenital anomalies.
Congenital failure of thumb formation is arather commonly observed birth defect and mayin certain cases be part of a more complicatedpicture: Thumb abnormalities, for example, areoften seen in association with pre-axial longitu-dinal failure of formation of the radius (Fig. 1:radial agenesis) and have been reported withvariable penetrance and expressivity inLamb’s4~ series of 117 consecutive cases. Syn-drome complexes that involve cardiovascular,genitourinary, and musculoskeletal manifesta-tions may also have associated thumb abnor-malities, including Holt-Oram syndro~ne, Fan-toni syndrome, diastrophic dwarfism, andCornelia deLange syndrome.
Each of the three tubular bones of the thumbosteoarticular column may be affected differ-ently, depending on causative genetic or envi-r0nmental factors. Certain characteristic defor-mities reflect specific syndromes, e.g., theshort, flat, broad distal phalanx of Apert’saerocephalosyndaetyly (Fig. 2A and B) and Car-penter’s syndrome, or the slender terminal pha-
0749-0712/90 $0.00 + .20
Management of Thumb Hypoplasia
William B. Kleinman, MD*
langeal hypoplasia characteristic of both Holt-Oram and Faneoni syndromes.
Longitudinal growth deficiency of the thumbproximal phalanx is usually not an isolated phe-nomenon and can occur in combination ~vithsome type of general phalangeal growth distur-bance involving the medial fingers, e.g., braeh-ydaetyly (most commonly attributable to growtharrest of the middle phalanx) and synbraehydae-tyly (Fig. 3A-D), or more complex museulo-skeletal syndromes, such as brachydaetyly inassociation with absence of the sternoeostal por-tion of the peetoralis major muscle (Fig. 4:Poland’s syndrome).
Congenital absence, shortness, instability, ordeformity of the thumb can result potentiallyin profound compromise to grasp and pinch.The rationale for surgical reconstruction should
.,be based on consideration not only of the func-tional, but of the emotional impact of the child’scongenital deformity. The demanding technicalconsiderations involved in surgically creating ananatomic potential for grasp or pinch are onlypart of a decision-making process; a process thatmight, unfortunately, include complete lack ofpatient cooperation. Unpredictability of growthpotential in those tissues to, be used for recon-struction, and a general predisposition for re-calcitrant anatomic abnormalities encounteredat the time of surgery also confuse the decision-making process. Add to this the absende ofnormal cerebroeortieal thumb representation,and the surgeon can readily appreeiat_e prob-_lems inherent in functional reeonstruetion, of
*Clinical Associate Professor of Orthopaedic Surgery, Indiana University School of Medicine; Director, Congenital Hand..Service, Riley Children’s Hospital, Indiana University Medical Center; Clinical Assistant Professor of Plastic Surgery,University of Kentucky School of Medicine, Lexington, Kentucky; Attending Staff Surgeon, The Indiana Center forSurgery and Rehabilitation of the Hand and Upper Extremity, .Indianapolis, Indiana
Hand Clinics--Vol. 6, No. 4, November 1990 - 617

618 $Villiam B. Kleinman
Figure 1. Congenital anomaly of the thumb is a frequentoccurrence in radial club hand, observed to some degreein each of Lamb’s first i17 cases of radial agenesis.45
partial or complete congenital thumb defi-ciency.
DEVELOPMENT OF A CONTEMPORARYSURGICAL APPROACH TO CONGENITAL
THUMB RECONSTRUCTION
Through the last century of thumb recon-structive surgery, an appreciation has existedfor the importance of an opposable nnit to theprehensile human hand.5° Since 1874, whenHuguier~8 reported deepening a remaining cleftbetween a partial traumatic thumb and indexfinger amputation in an adult, exhaustive sur-gical efforts have been directed towards salvageand reconstruction of an opposable thumb unit.The issue of thumb reconstruction has been
controversial throughout the last century. Es-tablished doctrines are challenged frequently,and thoughtful new principles and techniquesregularly introduced into the literature. Few ofthese innovations have endured to become con-temporary hallmarks of reconstruction of thecongenitally deficient thumb.
Differences between congenital failure ofthumb formation and traumatic thumb loss can-not be overstated, and must be appreciated bythe reconstructive hand surgeon during his orher assessment of the functionally compromisedpatient. The child with congenital thumb defi-ciency has a markedly reduced, or absent cer-ebrocortical representation for thumb function,which is normally a rather large portion of thesensory cortex (Fig. 5A and B). To compensatefor inadequacies of prehensile thumb function,the child afflicted by complete or partial thumb
Figure 2. A and B, Certain syn-dromes demonstrate characteristicthumb deformities (e.g., the short,fiat, broad distal phalanx of Apert’sacrocephalosyndactyly).

Management of Thumb Hypoplasia 619
immb is a frequent:,d to some degreetl agenesis.4~
;t century. Es-;ed frequently,?,nd techniques~rature. Few ofto become con-~ruction of the
aital failure ofthumb loss can-appreciated by
n during his or[y compromisedital thumb deft-. or absent cer-:humb function,e portion of theTo compensate
:humb function,)r partial thumb
and B, Certain syn-strafe characteristicies (e.g., the short,d phalanx of Apert’s~actyly).
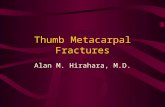
Figure 3. A and B, Synbrachydactvly in a 2-year-old hand is manifested by absence of the middle ~lmlange andundergrowth of the distal phalanges, i~cluding the thumb. C and D, In contrast to panels A and B, this 9-year-old childhas failure of middle phalangeal formation in the index and middle fingers, delta middle phalanges of the ring and littlefingers, and an essentially normal thumb. Middle phalangeal hypoplasia or absence is characteristic of brachydactyly.
aplasia may develop insidiously a progressivepronatory curve of the index ray, enlargementof the interdigital cleft between index and mid-dle fingers, and gradual increased breadth ofthe index pulp (Fig. 6). A primitive but func-tional level of prehensile grasp and pinch maybe afforded between index and middle fingers,even in the absence of thumb cortical represen-tation.
Figure 4. Poland’s syndrome is characterized by a clas-¯, sically congenital absence of the sternocostal portion of the
pectoralis major muscle, with ipsilateral brachydactyly. Thisl~atient represents the "Poland’s qariant": acheiria (tran-
: scarpal failure of hand formation) in combination withabsence of the sternocostal portion of the pectoralis major.
HISTORY
Contemporary. principles of thumb recon-struction for the congenitally compromisedhand are based on surgical experience followingtraumatic thumb loss. In the latter part of the19th and early 20th centuries, two distinctsurgical philosophies evolved: (1) local thumbphalangealization postpar~ial amputation, essen-tially a deepening of the first web space as firstdescribed by Huguier~S; and (2) distant pedideflap attachment with delayed secondary detach-ment, described in 1897 by Nicoladoni. ~ Ni-coladoni approached the tedious task of rebuild-ing the thumb following traumatic amputationby staged, attached great toe-to-thumb transfer(Fig. 7), a reconstructive effort of substantialtechnical magnitude for its time, requiring anenormous degree of patient motivation and co-operation. In 1966, Tubiana and coauthorst" ~
reported that on long-term follow-up of Nico-ladonfs three patients in whom this technique;vas used, each refused subsequent bone graft-ing procedures and remained with unstable,

620
SENSORY CORTEX
William B. Kleinman
~ ..,,~/ ARMHIP } TRUNK ~
NECKTHIGH
HAND
KNEE
LEG
FOOT
TOES ~
GENITALIA
FINGERS
THUMB
EYES
NOSE
FACE
LIPS
TEETH
JAWS
TONGUE
;~ ~ LARYNX
I~TESTINE
Figure 5. A and B, The importance of the thumb to normal human hand fnnctiou is obvious on the sensory, homunculns.Children with congenitally absent thumbs have no cerebrocortical thumb representation.
floppy thumbs after detachment. Clarkson18 asrecently as 1955, however, reported the largestknown series using Nicoladoni’s principles oftwo-stage distant pedicle toe tran sfer in 15 digitstransferred in six patients, one of whom under-went a 5-toe transfer for the treatment of corn-
plete congenital transverse failure of formationat the midpalmar level. Results were reportedas completely successful, requiring only a laterweb-space deepening between the great andsecond toes.
The idea of using distant pedicle flaps in
Figure 6. Congenital thumb absence is associated withprogressive widening of the index-middle finger web space,mild pronation of the index finger, and broadening of theindex pulp; these adaptive changes facilitate elementarygrasp and pinch between index and middle fingers.

FINGERS
LIMB
~ EYES~ NOSE
FACE
~ TEETH
~ JAWS
~ TONGUE
~ ~. LARYNX
~ INTESTINE
sensoD" homunculus.
lure of formation.ts were reportedtiring only a later~n the great and
ped{cle flaps in
ace is associated with",Idle finger web space,md broadening of thetitcilitate elementary
..niddle fingers.
Management of Thumb HypopIasia 621
and information after World War II found Gos-set’s techniques being used worldwide in cen-ters for hand reconstruction. His initial tech-niques have been modified over the past fourdecades from those that involved simple lateraldisplacement of the index ray without bonyshortening, to metacarpal recession and rota-tion, intrinsic muscle transfers, and skin flapsespecially designed for a wide first web space,free of sear eontracture.
Before these principles gained wide accep-tance, Barskya-5 and others42, 7~ sought to im-prove prehensile grasp in the congenitally de-ficient hand by surgical enhancement of thenatural progressive pronatory deformity of the
Figure 7. Early efforts to rebuild a thumb lost by traumaincluded Nicoladonfs tedious staged attachment of theinjured hand to the contratateral great toe. Originallyperformed in three patients, not one returned after detach-ment procedure for secondary stabilizing bone grafting.
rebuilding amputated thurnbs was also pro-posed by Luksch5~ in 1903, first describing theuse of the contralateral index finger as a staged:edicle transfer. His work was based on anarlier extensive reconstructive experience by
Guermonprez,a~-aa which unfortunately wentunnoticed and unappreciated for more than ahalf-century. Joyce,4~ in 1918, reported recon-struction of the amputated thumb with the ringfinger of the opposite hand in a manner similarto Guermonprez’s work, relying on the princ!.-pies of a distant pedicle flap with delayed de-tachment.
The "osteoplastic" reconstruction, e’ ~-~7. 74 wasused extensively prior to World War II, usingeither one or two stages to attach the injuredthumb stump to a random tubed pedicle ofvascularized skin and subcutaneous, tissue fromthe abdomen or groin, with iliac crest cortico-
bone grafting for skeletal reconstruc-.tion.
The historic principles that evolved duringearly decades of this century continued in
when BunnelPa reported the first use offan index finger remnant (distal metacarpal and
phalanx) to reconstruct the lost basilarjoint of a thumb. But not until 1949 did Gos-
in Paris, report the first transfer of anfinger on its neurovascular pedicle alone
remote position on the hand. In introducingtechnique, Gosset not only revolutionized
traumatic thumb reconstruction,pioneered seminal principles of congenital
for the absent thumb.An international exchange of medical ideas
index finger in these children. Barsky advocatedsimple surgical deepening of the index-middlefinger web space, with rotational osteotomy ofthe index metacarpal; the pulps of the "reposi-tioned" index finger could be opposed for pinchand primitive grasp (Fig. 8A-C). Although atthe time these principles were quite sound andwere widely practiced, following World War IIthe technique was quickly replaced by neuro-vascular pediele transfer with index recessionand repositioning, adapted from techniquesbeing practiced by Bunnell, Littler, and othersfor traumatic thumb loss.
For historic accuracy, Gersuny~7 in Vienna in1887, was the first to describe the principle ofthe neurovaseular island pediele flap. However,his reports identified no named artery. Notuntil 1893, when Dunhamz~ of New York de-scribed a permanently vaseularized island ped-iele flap with identifiable blood vessels, wereprinciples established. The technique waswidely applied throughout the first half-of thiscentury in the field of plastic surgery and era-niofaeial reconstruction,~7 and became the basisfor Gosset’s later historic work in France.
A plethora of respectable contributions to thefield of digital neurov~iseular pediele transferfollowed Gosset’s original description,a° Successwith index ray transfer led to the use of themiddle,~. ~. a~. ~. ~_. ~7 ring,S. ~4. ~. ~, ~7. 7~ and lit-tle ~a" ~ fingers for reconstruction of thumb po-sition, length, and sensibility. As recently as1955, even the traditional osteoplastic stagedpedicle-and-graft reconstruction received aboost by Moberg’s~° introduction of the "islandpedicle" transfer of vascularized, sensible, cor-nified skin from an uninjured portion of thehand, used to restore stereognosis to the tactileportion of the osteoplastic thumb. Thus, this.type of staged reconstruction used combinedprinciples of preliminary tubed abdominal ped-icle, iliac crest corticocancellous bone graft, and

622 William B. KIeinman
Incision
Figure 8. A-C, Barsky’s technique for surgical Improvement of grasp and pinch in the hand afflicted by congenitalabsence of the thumb involved index-middle finger web space deepening and abduction/rotation osteotomy to "reposition"the index finger. Principles were sound but, historically, the results were disappointing.
neurovascular island pedicle transfer fi’om an-other digit (usually the ulnar border of themiddle finger), with subsequent: cosmetic de-bulking. This technique was widely practiced.17
The thalidomide tragedy in Europe resultedin a devastating number of drug-induced con-genital deformities of the upper and lowerextremities between 1959 and 1962. Over a 10-year period, Buck-Gramckon performed an un-precedented series of 100 index finger pollici-zations for congenital failure of thumb forma-tion, mostly drug-induced. Through carefulstudy and revision of both principles and teCh-nique, Buck-Gramcko presented the results of
his work at the 1971 meeting of the AmericanSociety for Surgery of the Hand in a landmarkpaper on congenital thumb reconstruction. Heemphasized in his report that digital transposi-tion should be performed during infancy, asRiordan had advocated.ll, ~s, 69, 7~ Using contri-butions of Gosset,~° Hilgenfeldt,a6 Littler,4~-~0
Harrison,a4, a~ and Riordan,~s, ~. 7~ Buck-Gram-cko designed a surgical approach for the thumb-less child, using the index finger, that resultedin stability,, mobility, and optimum position andstrength for prehensile grasp and pinch. Histheoretical and practical contributions, includ-ing intrinsic muscle transfers, carpometacarpal
Figure 9. A and B, Completefailure of formation of the thumbhas neither soft tissue nor bonythumb remnants. The entire os-teoarticular column, including tra-pezium and scaphoid, are absent(Buck-Gramcko grade V thumb hy-poplasia).

by congenitalo "reposition"
~ Americana landmark’uetion. He1 transposi-infancy, as;ing contri-Littler,47-~°
;uek-Gram-the thumb-tat resulted~osition andpinch. His,ns, inelud-~meta~arpal
B, Completeof the thumb;ue nor bonyhe entire os-including tra-5, are absent.~ V~thumb hy-
Management of Thumb Hypoplasia 623
reconstruction, and the geometry of skirt flaps poplasia in-to five reasonably distinct categoriesto avoid first web space contracture, have be- (Fig. 11A-E). Using this classification, severecome hallmarks of contemporary congenital thumb involvement with absence of the entirethumb reconstruction, osteoarticular column and all soft tissue would
CONGENITAL FAILURE OF THUMBFORMATION: THE APLASTIC THUMB
AND THE "POUCE FLOTTANT"
Phenotypic expressivity of congenital defor-mity of the thumb has wide variations, includingfailure of formation of the entire osteoarticularcolumn (including trapezium and scaphoid)(Fig. 9A and B) and the so-called floating thumb"~.ouce flottant") (Fig. 10A and B).
A useful classification of the spectrum ofcongenital thumb involvement was suggestedby Mtiller 6~ in 1937 as a "teratologic sequence,"and later by Blauth7 in 1967. Buck-Gramcko(D. Buck-Gramcko, MD, personal communi-cation, 1989) has refined and detailed theseearlier contributions, and classified thumb by-
Figure 10. A and B, The pouce flottant (grade IV thumbis nonfunctional and devoid of metacarpal or
base for the thumb; its origin is distal and dors~d alongthe radial midaxial border of the hand. Although oftenassociated with a narrowed base, the neurovascular statusof the floating thumb is normal.
be Grade V hypoplasia, or aplasia (the finalmost severe stage of thumb reduction in Mtill-er’s "teratologic sequence").
Grade IV hypoplasia describes the "pouceflottant’" or "floating thumb" as a rudimentaryappendage connected to the hand by a smallskin tag, and usually containing two rudimen-tary phalanges and a single well-developed neu-rovascular bundle. The remainder of the thumbosteoarticular column is absent; the origin ofthis severely deficient appendage is along theradial midaxial line of the hand, and quite distal(Fig. 12A and B). The appendages are variablein size.
Assuming fundamental understanding and co-operation of both patient and family, completeabsence of the thumb (grade V hypoplasia)should be treated early in life by pollicizationof the index finger using the principles of Gos-set, Littler, Riordan, and Buck-Gramcko. Pro-gressive moderate pronation of the index ray,widening of the index-middle interdigitalspace, and broadening of the index pulp, allpredispose the untreated patient to functionalscissoring between index and middle fingers(Fig. 13).
Index ray development in patients afflictedby either complete thumb absence or pouceflottant (grade V or IV thumb hypoplasia) de-mands pollicization. Attempts to mobilizepoorly developed and contracted joints to re-establish a proper orientation to the base of agrade IV floating thumb are unjustified, evenwithout considering the problems inherent in--multiple tendon transfers.
The constriction at the base of the pouceflottant permits digital survival during the post-natal period. The thumb unit ,is severely hypo-plastic, usually devoid of metacarpal, trape-zium, and scaphoid, and has neither intrinsicnor extrinsic tendons; the proximal and distalphalanges may be only cartilage remnants (seeFig. 11D). A thumb nail is usually present anddeveloped to an extent similar to the generaldevelopment of the entire distal thumb unit. Itis important to emphasize that within the nar-rowed base of the grade IV hypoplastic thumbis a distinct neurovascular pedicle (Fig. 14Aand B).
The pouce flottant should be amputated,either as an independent procedure or in con-junction with pollicization. In the newbornnursery, the base of the thumb can be anesthe-tized locally and a sterile silk tie applied tightly

624 William B. Kleinman
$~ight Decrease
~
Ad6ucted Posture
~!~n~i i~!itl~~ ~ ~ .....
A ’ " B ’ C
Figure li. A, Grade I thumb hypoplasia has an essentially complete complement of bones in the osteoarticular column;thenar and first web-space musculature is normal, joint range of motion is normal, and only the gross size of the thumb isdiminished. B, Grade II thumb hypoplasia is manifest by an even smaller thumb stature than grade I hypoplasia and eitherreduction of volume or complete absence of |~e thenar muscles. Because of imbalance between thumb abductors andadductors, first web-spaee c~ntraeture is common. The bones of the osteoarticular column are,narrow, and instability ofthe ulnar collateral ligament of the metaearpophalangeal joint is common. Basilar thumb instability may also be found,although the radial carpus (seaphoid, trapezium, and trapezoid) is nsually present. C, Grade III thumb hypoplasia isassociated with severe first web-space contraeture secondary to a usual complete absence of thenar muscles. The thumb isshort, and global instability of the metacarpophalangeal joint is common. Osseous and articular relationships at the thumbbase are variable in their formation. D, Grade IV thumb hypoplasia is the classic pouce flot~ant (floating thumb). A well-formed neurovascular pedicle can be found coursing through the pediele; the origin of the pedicle is quite distal along theradial mid-axial line. All thenar and adductor thumb musculature is absent, except for the second metaearpal origin of thefirst dorsal interosseous (abductor indicis). The trapezium and seaphoid are usually absent; the trapezoid is often normal.E, Grade V thumb hypoplasia is complete congenital absence of the thumb (aplasia); even the abductor indicis are absentor deficient in more than ~0% of cases. The index finger usually undergoes pulp widening, digital pronation, and index-.middle finger web-space widening, with progressive curvature of the index ray. These eases are ideal candidates for indexfinger pollieization.

Management of Thumb Hypoplasia 625
far column;e thumb isand either.uctors and.stability ofbe found,
poplasia ise thumb isthe thumbb). A well-I along the5gin of the~n normal.are absentand index-s for index
Figure 12. A and B, Distal and dorsal origin of the pouceflottant makes functional reconstitution difficult. To performprehensile tasks, the origin of the thumb unit must besurgically moved more proximal and volar, and bone graftsused to create a stable base.
Figure 14. A, In spite of severeunderdevelopment, gross instabil-ity, and a narrow constricting ped-icle at its base, the pouce flottanthas a normal complement of digitalnerves and a single large digitalartery with its venae comitantes(arrow). B, Arteriogram of a pa-tient with grade IV hypoplasiaclearly demonstrates a single largeunconstricted digital artery passingthrough its narrow base.
ffigure 13. Patients with severe thumb hypoplasia preferthe scissoring action of index-middle abductiordadductionfor pinch and minor grasp. Left untreated, even the "rich"hypoplastic thumb will frequently be bypassed because ofits subnormal stability and mobility and its less than normal --cerebrocortical representation.

626 William B. Kleinman
Figure 15. A major principle of pollicization is construc-tion of a scar-free, contracture-free first web space. If wellplanned, the pouce flottant can be filleted and effectivelyused in this process.~
at the bas4 to induce ischemic necrosL’;. A smallamount of long-acting anesthetic prevents thepain associated with crushing a well-developeddigital nerve with the tie.
Match~4 reported filleting open the floatingunit at the time ofpollieization, and incorporat-ing the skin of the deficient thumb into thenew first web space (Fig. 15), Whether the partis ablated as an independent procedure or re-moved at the time of pollieization, efforts shouldnot be made to reconstruct a grade IV hypo-plastic thumb with a functional unit as a surgicalgoal. The results of such efforts are poor bothfunctionally and cosmetically. The child--oftenafter a plethora of surgical procedures--willbypass the reconstructed unit, preferring amore natural index-middle finger scissoringaction. Dexterity of the medial four fingersoutweighs any effort to create a functionalthumb unit from the pouceflottant.
There are, however, exceptions to any rule.Particularly in cultures in which a five-fingeredhand has extreme importance, seteet eases mayjustify efforts to reconstruct a Grade IV hypo-plastic thumb. In these rare ihstanees~ the siteof origin of the thumb base must be shifted toa more palmar and proximal locus, ensuring
stability by either autogenous eortieoeaneellousiliae crest graft or longitudinal fibular strut,inserted between the base of the index meta-ear-pal and the hypoplastie thumb rudimentaryproximal phalanx (Fig. 16 A and B). Concomi-tant reconstruction of a wide first web space isobviously necessary. Tajima76 has advocated alarge dorsal skin flap designed over the indexmetacarpal and proximal phalanx, which can berotated with the. fioating thumb to.create anacceptable first ~veb; skin graft is applied to theflap donor site. Osseous stability in these gradeIV hypoplastic thumbs can also be achievedusing a free nonvascularized transfer of themetatarsophalangeal joint of the fourth toe,potentially providing a degree of thumb mobil-ity (Fig. 17 A-E). Because of the importance ofthe five-fingered hand in Japanese culture,techniques oriented towards salvage and recon-struction of the congenital floating thumb haveemanated principally from that country. Recon-struction is obviouslv a major surgical effort,which involves stabilizing the digit by bonegraft or whole joint transfer, complex skin flapsand grafts, and three subsequent individualtendon transfers as potential balanced motors.Thumb extension can be achieved by transferof the extensor indieis proprius; abduction and/or opposition by the Huber transfer ~7 of theabductor digiti quinti (modified by Littler4V-5°);and flexion/adduetion by direct transfer of thering finger flexor digitorum superfieialis (Fig.18A and B).
The surgeon must realize that results of thesereconstructions are disappointing at best. Poorjoint development should be an absolute _c_on-traindieation for tendon transfer: by definition,tendon excursion is severely limited by poorjoint mechanics, and the natural pattern offunctional index-middle finger scissoring con-tinues. The potential for index pollieization mayalso be lost by irreparable surgical damage toskin incurred during primary efforts to makethe grade IV hypoplastie thumb functionallyuseful. None of White’ss° priorities for thumbreconstruction can be met: despite excellentsensibility, opposition cannot be effeetiZcely gen-erated from a rigidly fixed thumb base. Polliei-zation of the index finger becomes a very at-tractive alternative.
POLLICIZATION FOR CONGENITALTHUMB DEFICIENCY
Far more challenging than the theoreticallysimilar reconstruction for traumatic thumb loss,

ncelloustr strut,~x meta-mentaryoneomi-space isaeated am indexh can bereate an,~d to these grade~ehieved: ofxtherth toe,b mobil-rtanee ofculture,
~d recon-mb have. Reeon-~1 effort,by bone;kin flaps~dividualmotors.transfer
tion and/~7 of the
:tler4V-~o);~r of the~li~ (Fig.
; of these~st. Poorlute con-efinition,by poor~ttern of:ing con-Ltion may~mage toto make
rationally~r thumbexcellentvely gen-,’. Pollici-very at-
~ITAL
oi:eticallyamb loss,
Management of Thumb Hypoplasia
(~.~~ Deepening of I st Web Space byDorsal Flap or Graft
Initial Distal-DorsalLocation of Pouce Flottant
of Pouce Flottant
Iliac Crest Dowel Graft
A "Figure 16. A, In those rare instances where reconstruc-
tion of a floating thumb is indicated, stability can be¯ attained by a corticoeaneellous pelvic strut graft placedbetween the distal osteoarticular remnant and the base ofthe second metacarpal. B, Improper reconstruction of thebase of the floating thumb affords absolutely no increasedpotential for prehensile grasp or pinch.
627
Siin Graf,,~ !
E
Incision
Figure 17. A-E, The Tajimar~ technique forreconstruction of a pouce flottant achieves basilarjoint stability by nonvascularized metatarsophalan-geal joint transfer from the fourth toe (A) andestablishes a wide first web space by large dorsalrotation flap design (B and C). After achievingt~mporary bony fixation with Kirschner wires (D),full-thickness skin graft is applied to the flap donorsite (E).

628 William B. Kleinman
Transferred EIP
Extensor DigitorumCommunus Tendon
to Index
(abduction/opposition)
Absence of ~ i~,<(4/ ~,
A EPL i ~\~B ~~,x~
Figure 18. A and B, Motors for the reconstructed grade IV floating thumb mav consist of extensor indicis proprius (EIP)transfer for extension, flexor digitorum superficialis (FDS) IV for flexion/adducti~n, and the abductor digiti quinti (AbDQ)for abduction/opposition. The EIP (with or without graft prolongation) can also be used to reconstitute active interphalangealjoint extension in cases of congenital deficiency of the thumb’s long extensor tendon, provided that full passive range ofmotion is present and lateral joint stability exists (see text).
pollicization for congenital thumb deficiencymay require use of a digit that itself may b~anatomically deficient, particularly in the caseof radial club hand. Pollicization was first suc-cessfully adapted to congenital hand reconstruc-tion in 1960 by Zaneolli84; but the thalidomidetragedy of 1959-1962 led Buck-Gramckon tohis unparalleled experience and confirmed theusefulness of index finger pollicization as theprocedure of choice for treatment of grade IVand V congenital thumb formation failure.
Pre-op Position:
FDS IV
4th Dorsal
Figure 19. A and B, Stability of the basilar joint of the pollicized index finger is best achieved by hyperextending theindex metacarpophalangeal joint before insetting it into the capsule of the disarticulated index carpometacarpal joint; inthis manner, functional hyperextension of the pollicized digit is prevented.
The functional goals of pollicization arereached only with painstaking attention paid totechnical details. The incisions must be de-signed to allow shortening, rotation, and repo-sitioning of the digit to be pollicized. Skin flapsmust form a well-contoured first web space,free of restraining scar. Stabilization of the baseof the new thumb can be achieved by a varietyof techniques; but the propensity for severebasilar joint hyperextension must be addressedif the index metacarpophalangeal (MCP) joint

Juction)
~osition)<
,prius (EIP)nti (AbDQ)rphalangealve range of
.tion aren paid tct be de-md repo-~kin flaps,b space,the basea variety)r severe:ddressedCP) joint
:ending the~al joint; in
Management of Thumb Hypoplasia
is used as the new thumb carpometacarpal(CMC) joint. Buck-Gramcko recognized thisproblem, rectifying it by hyperextending thecondyloid surfaces of the index MCP joint atthe time of surgical stabilization, thereby redi-recting the new carpometacarpal arc of motion!:co the flexion rather than hyperextensionrange (Fig. 19A). Osteotomy is performedthrough the distal index metacarpal physis andthe entire proximal index metacarpal is re-moved. The transposed index ray should besecured in 120° pronation, 40° palmar abduc-tion, and 15° extension. I prefer disarticulationof the index carpometacarpal joint, leaving asleeve of capsule to which the hyperextendedMCP joint can be securely anchored (see Fig.19A and B).
MOTORING THE POLLICIZED DIGIT
Although the time-tested principles of digitaltransposition on neurovaseular pedieles, firstrecommended in this country by Littler, 4r in1953, are still used as the basis for pollieization,new techniques for motoring the transposeddigit are regularly being introduced in the lit-erature. The currently popular intrinsic trans-" ’s of first dorsal and first volar interossei for~.umb abduction and adduetion stem from theaccumulated experiences of Riordan and Buek-Grameko.
629
Buck-Gramcko has reported it unnecessaryto shorten the extrinsic index (new thumb)flexor system or to remove the lumbrical fromthe index profundus tendon, despite resectionof the entire proximal index metacarpal. Hehas, however, advised shortening the extrinsicextensor tendons (extensor indicis proprius andindex extensor digitorum communis) by lengthequal to the segment of metacarpal removed.Manske and McCarroll~3 disagree with this rec-ommendation and report that in their experi-ence the extensor indicis proprius muscle-ten-don unit also spontaneously absorbs the slackof skeletal shortening. These authors believethat flexors and extensors should be left sur-:gically unshortened.
The currently popular Buck-Gramcko polli-cization technique suggests distal detachmentof the insertions of the abductor indicis (firstdorsal interosseous) and first volar interosseousfrom the index proximal phalanx (Fig. 20).These motors can then be advanced d2stally intothe radial and ulnar lateral bands of the dorsalapparatus and function in an abduction-adduc-tion plane (1st DI for abduction; 1st VI foradduction). The design of skin flaps serves sim-ply to accommodate the increased muscle vol-ume at the level of the new thumb metacarpal,and to minimize scar contraeture in the newfirst web space.
In personal experience with 45 pollicizationsfor congenital thumb deficiency, I have found
Figure 20. Principles of meta-shortening and tendon
for index pollicizationdeveloped by Buck-
following the thalido-tragedy in Europe. The tech-relies upon extensor indicis
(EIP) shortening by equal to the portion of index
resected; the extensorcommunis (EDC) II
rerouted to abduct the new thumbbase, with abduction
restored by the 1stinterosseous (DI) and 1stvolar interosseous (VI), respec-
tively.
II~DEX
DIP
PI
Redrawn fromBuck-Gramcko, JBJS, 1971
CM
MP
THUMB
IP
EIP .-,,. EPL
EDC (index, long) ~ AbPL
lstVolarlnt. ~ AddP
1st Dorsal Int. ~ AbPB

630 William B. Kleinman
PalmarI
EPL (EIP)
IEDC ]3~
Figure 21. The Buck-Gramcko technique for index pol-licization requires the presence of a healthv first DI anddistal dissection into the radial and ulnar l~teral bands ofthe digit. In the absence of a first DI, an alternative forthumb abduction is to advance the EDC II more distal onthe proximal phalanx of the index finger. Adduction can bealternatively achieved by proximal advancement of themuscle belly of the first VI (palmar I) on the shaft of thethird metacarpal, sparing dissection into the digit itself (seetext).
complete or partial absence of the abductorindieis (first dorsal interosseous) in more than50% of eases. In these patients, active palmarabduction of the new thumb can still beachieved by transfer of the extensor digitorumcommunis more ’distally on the volar border ofthe proximal phalangeal diaphysis (Fig. 21).This technique substitutes extensor digitorumeommunis (EDC) for the absent abductor indi-cis for thumb abduction. If necessary, supple-mentary use of either the ring flexor digitorumsuperficialis or the abductor digiti quinti as anopponensplasty can be made, either at the timeof pollicization or secondarily.aT, ~a
An alternative technique of pollicization,which I use on occasion, simplifies skin flapsand minimizes dissection into the index proxi-mal phalanx and its dorsal apparatus. The mus-cle belly of the first volar interosseous is rotatedand distally advanced along the periosteum ofthe adjacent third (middle) metacarpal, leavingits "~nsertion unchanged. This technique stillrelies upon the 1st VI for functional thumbadduetion, but without detachment and distaladvancement of the tendon to the ulnar lateralband as Buek-Grameko described (Fig. 2"2A-C;see Fig. 2i).
The surgeon must be aware of the potential
Figure 22. Incisions used for thepollicization technique described inFigure 21.

ue ibr index pol-[thv first DI and’ lateral bands ci"~n alternative forII more distal on~.dduction can be~ncement of thethe shaft of the
~e digit itself (see
pollicization,ies skin flapsindex proxi-
us. Tile mus-ous is rotated~eriosteum of~rpal, leavingchnique still:ional thumbnt and distalulnar lateral
(Fig. 22A-C;
the potential
used for thedescribed in
Management of Thumb Hypoplasia
for anatomic variations in any type of congenitalhand reconstruction, particularly with respectto availability of useful motors for the pollicizeddigit. If present (and ff substantial), the firstdorsal interosseous should be used preferen-tiaii; for palmar abduction, as detailed by Buck-Gramcko; however, distal and volar advance-ment of the index EDC should al~vays be con-sidered an option when a poorly developed 1stDI exists. Tendon transfers described earlier inthis chapter for motoring the pouceflottant arereadily adaptable to a deficient pollicized indexfinger (e.g., abductor digiti quinti or ring flexorsuperficialis for opposition, or extensor digitiquinti proprius for thumb extension in theabsence of developed extrinsic index extensors).~fi: surgeon’s own ingenuity and skill in select-ing the most appropriate transfer ~vill yield thebest functional thumb unit.
HYPOPLASIA OF THE THUMB,EXCLUDING POUCE FLOTTANT AND
COMPLETE ABSENCE
631
Figure 23. Profound intrinsic and extrinsm muscle defi-ciency usually accompanies Buck-Grameko grade III thumbhypoplasia. Because of poor motor development, and po-sition-irregularity of the base, this thumb ~vill be perma-nently by-passed in t~avor of index-middle finger scissoring.
RECONSTRUCTION
While grade I hypoplasia is essentially a~: .:real functioning thumb, except for beingsiightly smaller than normal size, the grade IIhypoplastic thumb is considerably smaller andless stable. Thenar musculature is usually defi-cient and palmar abduction limited; the firstweb space is narrow, and thumb pronation is
(see Fig. 12B). The ligaments of the: metaearpophalangeal (MP)joint (particularly
ulnar collateral ligament) are poorly devel-which further compromises pinch.
Cases of grade II hypoplasia manifest a pie-. thora of abnormalities. Deficiency in extrinsic
flexor and/or extensor systems may also beparticularly an often-observed tendi-
nous connection between the flexor pollieisilongus and extensor pollieis longus tendons (G.Lister, MD; S. Stahl, MD, personal eommuni-
!.cation, 1989).~, ~4, ~. 7~ Any combination of ab-tendon vectors or insertions, absence or
:unusual presentation of pulleys, or completeof tendon systems may be found in the
grade II hypoplastic thumb category.Grade III thumb hypoplasia exhibits a more
,rofound reduction in thumb size, stability, and(see Fig. 12C). Instead of simple
collateral ligament attenuation observed inII hypoplasia, the MP joint of the grade
thumb is flail, with usually only a rudimen-tary CMC joint. Extrinsic tendon systems are
t, and there is essentially no participatoryfunction of the thumb unit in routine handfunction (Fig. 23).
The philosophy of surgical reconstruction ofthe grade III hypoplastic thumb (see Fig. 12C)is based on the potential for pinch-and-graspenhancement, using the patient’s own thumb.If the thumb lever arm is short only because ofcompromised longitudinal skeletal development(brachydactyly, as opposed to transverse t~ailureof formation), it can be lengthened, as long ascarpometacarpal stability and mobility are rea-sonable (grade II). Additional length can provided in a variety of ways; one is by extra-periosteal transfer of the fourth toe proximal
..phalanx into the collapsed soft-tissue digitaltube of the hypoplastic thumb (Fig. 24, A andB). A chevron incision is used, and the dorsalapparatus of the toe is split longitudinally; theproximal phalanx can then be disarticulated andremoved en bloc. Care must be taken to avoidinjury to the extrinsic toe flexors, which con-form intimately to the plantar contour of theproximal phalanx. Once removed, the longitu-dinal extensor tenotomy i~’ repaired and theskin closed. The resulting shortened toe isfunctionally stable, and not cosmetically disfig-uring.
Carroll and Green~ reported no activegrowth in their series of free phalangeal trans-fers removed by subperiosteal dissection. Gold-berg and Watson,e9 however, suggested up to90% preservation of normal growth from thetransplanted epiphyseal plate (age-dependent)using extraperiosteal dissection. Subperiostealharvesting and transfer can result in partialresorption of the transplanted phalanx; extra-periosteal transfers undergo no resorptivechange, and a variable rate of growth.
Once filled with transplanted bone, furtherthumb length can be attained by osteotomy and

632 William B. Kleinman
Figure 24. A and B, Thumb lengthening by nonvascularized toe phalangeal transfer can be performed by extraperiostealharvesting of the fourth or fifth toe proximal phalanx through a chevron incision; a temporary percutaneous Kirschner wirecan be used to maintain length until healed (3 to 4 ’weeks). C, Extraperiosteat toe proximal phalangeal transfer to lengthenand stabilize a grade III hypoplastic thumb (arrow).
distraction using an external fixation device(Matev,~5, 56 Kessler~4) designed to graduallycreate an intercalary defect, secondarily bonegrafted when an appropriate length has beenachieved (Fig. 25A-D). This technique, nsefulin both congenital and traumatic thumb recon-
struction, is usually combined with first webspace deepening by simple 60° Z-plasty, 4-flapZ-plastT (Broadbent and Woolia°), or a dorsalindex-finger rotation flap with full-thicknessskin graft to the donor site (Fig. 26). Donorbone graft for the intercalary skeletal defect
Figure 25. A-D, Extraperiosteal toe phalangeal transfer to the thumb, index, ring, and little finger metacarpal bases ina child with transverse failure of formation: Once bone transfer to the digital tube of the hypoplastic thumb has beenperformed, additional length can be secondarily achieved by osteotomy and progressive lengthening in an externaldistraction device (B and C); the intercalary defect is filled by corticocancellous iliac crest bone graft (D).

)y extraperiostealts Kirsehner wirensfer to lengthen
zith first web-plasty, 4-flapI, or a dorsalfull-thickness;. 26). Donorkeletal defect
~taearpal bases inthumb has been,~ /~n an external
Management of Thumb Hypoplasia 633
Figure 26. After thumb lengthening, first web-spacerelease is achieved by first DI recession and partial adductormyotomy. Skin coverage of the new first web can be byor:~ of a variety of methods, including dorsal :rotation flapi~’,:::~ the index finger ~vith adjunctive full-thickness skingraft.
Figure 27. An 8-year-old child after 2 of three plannedtendon transfers for grade III hypoplasia Results were sodisappointing that plans for the final stage were abandoned.
created by osteotomy and lengthening can befibula, toe proximal phalanx, or cort:icocancel-lous iliac crest, based on the patient’s age andquantity of bone required.
An alternative to external fixation and pro-gressive distraction is the intraoperative one-s~-:~ distraction technique using a spinal laminasd~eader; a 1.5 em lengthening can easily beattained without compromise to the neurovas-eular status of the digit. A toe proximal phalanx
then be transferred to the digit.The philosophy of surgical reconstruction in
of thumb hypoplasia always focuses on~’potential": will enhancement of length, inde-pendence, mobility, and/or stability improvethe patient’s real potential for grasp and pinch?If the prognosis is poor, the hypoplastie thumb
be ablated, and the index finger polli-This is a diffleult decision, not: only for
surgeon, but for parents who are alreadywith guilt. Recommendations should
made carefully, by educating parents, con-medical colleagues, and exposing theto other patients in whom successful
on has been performed. The poten-spontaneous active function of the re-
:l hypoplastie thumb is often over-by the inexperienced surgeon. Thepatient in Fig. 27 is 2-years post-
transfers for function: extensor indieis~rius for extension, and ring-finger flexor~rfieialis for opposition. In spite of her abil-
to demonstrate thumb performance in theenvironment at her doctor’s request, she
:l in using index-middle finger scissor-during activities not subject to medical
scrutiny. Plans for adduetorplasty to complete
the triad of transfers were abandoned. The childcontinues to use her index and middle fingersfor "prehensile" grasp and pinch.
Recommending ablation of a grade II hypo-plastic digit of substantial skeletal developmentand near-normal size (Fig. 28A and B) is
Figure 28. A and B, Mild hypoplasia of the thumbjustifies efforts to reconstruct it, particularly if only minortendhn transfers are necessary. It is difficult to recommendablation of a digit with near-normal skeletal development.

634 William B. Kleinman
Figure 29. The principles of opponensplasty rely on a change in motor vector from the pisiform to the radial borderthe thumb metacarpophalangea] joint. In this example, the FDS IV is ha~ested through an incision in the distal palmarcrease (A and B), rerouted deep to the FCU at the ~vrist (C), and passed subcutaneously from the pisiform to the thumt~(C and D) under appropriate tension.
exceedingly difficult task for the hand surgeon;but predictable functional failure in lengthen-ing, repositioning, and tendon transfers, willmake ablation and index pollicization an attrac-tive alternative occasionally. Reluctance toablate and pollicize by both the surgeon andthe parents is understandable; but the realisticpotential for incorporation of a reconstructedhypoplastic thumb into coordinated prehensileactivities of the hand must be given paramountconsideration in any treatment plan proposed.
CONGENITAL ABSENCE OF THETHENAR MUSCLES
A commonly observed manifestation of con-genital failure of formation of soft tissues of thehand is absence of the thenar muscles, oftenpart of grade II and invariably part of grade IIIhypoplasia (see Fig. 12B and C). These patientsare unable to lift the thumb from the plane ofthe palm for grasp, and present with a narrowfirst web space.
For simple thenar muscle group deficiencywith full passive thumb range of motion (ROM),opponensplasty using the ring or middle fingerflexor superficialis is recommended. These mo-
tors are usually available, certainly expendable,and have the appropriate cross-sectional areaand muscle amplitude for strong opposition.Using the distal flexor carpi ulnaris as a pulley,the "angle of attack" of the transfer on thethumb provides a palmar abduction/flexion pullfrom the vicinity of the pisiform (Fig. 29A-D).
Web Space
1st Ooi-salInterosseousMuscle
Figure 30. Sequential technique for release of the con-"tracted first web space: (1) recession of the first metacarpalorigin of the 1st DI muscle, and (2) myotomy of thetransverse head of the adductor pollicis.

radial border of:he distal palmarcm to the thumb
,’ expendable,;ectional areag opposition.is as a. pulley,:nsfer on the)n/flexion pulliFig. 29A-D).
¯.
~ Adductor Pollicis~ (transverse head)
:~ Adductor Pollicis
(oblique head)
,lease of the con-e ~first metacarpalmyotomy of the
Management of Thumb HypopIasia 635
Figure 31. A dorsal rectangle flap xvith subjacent full-thickness skin grafts (arrows) can be used to widen the firstweb space in cases of thumb hypoplasia with adduction
transfers can be considered. First web spacerelease may require recession of the first dorsalinterosseous from the first metacarpal, or my-otomy or recession of the transverse head ofthe adductor pollieis, as described by Matev~, s~(Fig. 30). Division of the oblique CMC and/ortransverse.intermetaearpal ligaments support-ing the base of the thumb is usually unneces-sary. If the initial thumb position is severelyaddueted, adjunctive full-thickness skin graftsmay be necessary to cover exposed raw areas,regardless of the flap design used to reconstructthe new first web space (Fig. 31). Skin re-arrangement, whether by Z-plasty flaps, rota-tion flaps,r6 or full-thickness skin grafts, provideboth breadth and increased depth.
The abductor digiti quinti (Huber transfer) extensor digiti quinti proprius are good alter-natives.at. ~s. ~a, s4. 6~ Regardless of the techniquechosen, the opponensplasty tendon vector mustbe palmar, from the pisiform to the radialborder of the thumb MCP joint (see Fig. 29C).Techniques of routing and insertion of trans-_: red tendons vary, and are beyond the scope~ this article.
Opponensplasty in the hypoplastie thumbwith thenar deficiency only, can restore un-compromised prehension. Left untreated, im-balance between strong adductors and absentthenars will result in a persistent adduetioneontraeture of the first web space, and severelycompromised grasp potential. If already estab-lished at the time of initial evaluation, surgicalrelease of the eontraeture is necessary to attain
passive ROM before appropriate tendon
ABSENCE OF THE EXTRINSICTENDONS OF THE THUMB
An unusual anomaly of the thnmb associatedwith hypoplasia involves failure of formation ofeither the long extensor (Fig. 3"2A and B) long flexor (Fig. 38A and B) tendon. Inheritanceis autosomal dominant, with a high penetranceand expressivity (Fig. 34).
Patients with absence of the extensor pollicislongus present with an interphalangeal (IP) flex-ion attitude (see Fig. 32A), similar to thatobserved in congenital trigger thumb. Con-versely, failure of formation of the flexor pollicistongus manifests itself as inability to activelyflex the IP joint, with absence of distal volardigital skin creases (see Figs. 38A and 84).
If the IP joint is laterally stable and passivelyflexible, the ring flexor digitorum superficial~
Figure 32. Failure of formationof the dorsal apparatus of the con-genitally deficient thumb results insevere extensor lag and absent ac-tive interphalangeal joint extension(A); the dorsal tefidon is vestigial,terminating in soft tissue (B).

636 William B. Kleinman
Figure 33. Absence of distal digital thumb flexion creases in the presence of full passive range of motion is the hallmarkof congenital failure of formation of the flexor pollicis long"as (A and B); the flexor pollicis longus is vestigial and can oftenbe excised from the system, allowing the ring flexor digitorum superficialis to be transferred directly through the obliquepulley to the terminal phalanx (C and D).
can be transferred to create active thumb flexion(see Fig. 33C). Although the terminal flexortendon is vestigial, a reasonably well-developedpulley system is usually present; the existingnonfunctional tendon system can be excised,and the ring superfieialis transferred throughthe oblique pulley to the distal phalanx of thethumb (see Fig. 33D).
Tendon reconstruction dorsally is more diffi-cult because of the wide variations in deficiencyof the extensor pollieis longus and dorsal appa-ratus. The extensor indieis proprius vcith orwithout free tendon graft (see Fig. 18A) canoften be used to restore active extension to thepassively extensible thumb IP joint. However,
Figure 34. The mother of the patient in Figure 33demonstrates similar findings: absence of active left thumbinterphalangeal joint flexion since birth and failure of for-mation of digital creases in the thumb.
if the joint remains stiffeven after conscientioustherapy, arthrodesis is indicated. Fusion is per-formed between the distal metaphysis of theproximal phalanx and the epiphysis (secondaryossification nucleus) of the distal phalanx, pre-serving the physis and gro~vth potential of themore distal bone (Fig. 35 is an example of thesame technique used at the thumb MP joint).
RECONSTRUCTION OF THECONGENITALLY DEFICIENT OR
ABSENT THUMB BY TOE-TO-THUMBVASCULARIZED TISSUE
TRANSPLANTATION
Additional length can be achieved in a con-genitally deficient thumb by various methods,including (1) the insertion of a free nonvascu-lafiz6d toe proximal phalanx into an existingcollapsed soft-tissue digital tube16, ~9 (see Fig.25A), (2) toe phalangeal transfer as intercalarygraft (see Fig. 24C), or (3) lengthening of exist-ing bone by osteotomy and progressive distrac-tion by means of an external fixation device,with secondary intercalary bone graft44, ~. ~ (seeFig. 25B-D).
Over the past two decades, another tech-nique has been added to the surgeon’s arma-mentarium: free-tissue transplantation usingmicrovascular surgical disciplines. Introducedby Cobbett,19 in London in 1969, for thumbreconstruction, the early technique was basedon pioneering microsurgical research byBunckela in primates 3 years before. Cobbett’s~9

~n is the hallmar!~gial and can oftenrough the oblique
conscientiousFusion is per-.physis of thesis (secondaryphalanx, pre-)tential of thexample of theb NIP joint).
~ THEENT ORO-THUMB;UEN
ved in a con-ous methods,"ee nonvascu-o an existin~. ~9 (see Fi
as~ning~ssive distrac::ation device,raft., ~5, ~ (see
mother tech-~’geon’s~tation using;. Introduced9, for thumb’,m was basedresearch bye. Cobbett’s~9
Figure 35. The longitudinal growth potential of phalangesarthrodesed at the metacarpophalangeal or interphalangeal
~.t can be preserved by fusing the distal metaphysis of~..~. proximal bone to the secondary, ossification nucleus ofti~e distal bone, without violating the physis. In this ex-ample, the arrow indicates the healed fusion between adistal metacarpal and the epiphysis of a thumb proximalphalanx. Note the persistent open physis of the proximalphalanx.
single case involved vascularized transplanta-tion of a great toe after traumatic loss of athumb The surgery and postoperative courseof this landmark case were quite storn~ty.
ollowing publication of Cobbett’s experi-techniques were refined, with many au-reporting successful series of microvascu-
toe-to-thumb transplants to restore function~g traumatic amputation. But not until
did O’Brien, and coauthors,~ report thecase of a free-vascularized great toe trans-
for congenital absence of the thumb.s~ in 1980, reported similar success
in two congenitally deficient patients. May andin 1981 reported a successful ex-
perience using techniques of microvasculartransfer to build a thumb in a hand
afflicted by multiple digital aplasia. ̄Only sporadic cases were reported in the
until Gilbert~s in 1982 reported a 4-experience with 21 microvascular second-
toe transplants in 17 patients ,;vith congenitalfailure of formation; four thumbs were included
Management of Thumb Hypoplasia 637
in this series. Gilbert pointed out that hisexperience using traditional techniques forthumb lengthening were disappointing: aes-thetic improvement was minimal and final func-tion was poor. He also emphasized that thetechnique offree-microvascular transplantation,while exciting in concept, should be reservedfor those patients afflicted by congenital am-niotic or constriction-band syndrome (Fig. 36A),or true transverse failure of formation (see Fig.37B), as opposed to longitudinal digital skeletaldeficiency with preservation of the nail ele-ments (Fig. 37). Patients with true transversefailure of formation usually show no pathologicinvolvement of the remainder of the hand. Athumb affected by generalized osteoarticularcolumn hypoplasia is more likely to have asso-ciated anomalous proximal vessel and nerveanatomy, making application of microvascularreconstructive techniques difficult and unpre-dictable. Arteriography may be helpful in as-sessing which congenital patients are suitablecandidates for microvascular free-tissue trans-fer. If proper patient selection is employed,marked functional and cosmetic improvementcan be attained (Fig. 38 A and B). The skilled
Figure 36: A and B, True transverse fail~re of formationcan be represented by either nonfunctional tissue distal tocongenital constriction bands (A) or by complete digitalabsence distal to a certain level (B). In either type, theanatomy of the hand proximal to the defect is normal andshould be a suitable recipient bed for free vascularized toe-to-hand transplantation.

638 :i !William B.
Figure 37. Presence of nail elements in a congenitallydeformed hypoplastic digit defines a longitudinal, ratherthan transverse, failure of formation. Proximal vessel andnerve anatomy is anomalous and unpredictable, makingthese children poor candidates for microvascutar free-tissuereconstruction.
microsurgeon must, however, be able to explaincontraindications in those patients who are poormicrosurgical risks. This group is more appro-priately treated by the other standard, well-tested approaches discussed earlier in this arti-cle.
AGE CONSIDERATIONS
Selection of the most appropriate age for eachof the techniques of thumb reconstruction in
Kleinman
the congenitally deficient hand remains one ofthe more controversial facets of hand surgery.Riordan~a. ~9. 71 and Flatt 2~ have suggested that
pollicization can be safely performed at 6 to 12months of age. Buck-Gramcko has reportedgood results at an even earlier age (D. Buck-Gramcko, MD, personal communication, 1985).However, because the cardiopulmonary systemis sufficiently developed by 1 year postpartumto make general anesthetic risks minimal, andbecause bimanual grasp develops normally by12 months of age, perhaps pollicization shouldbe reserved until after the age of i year.
Another consideration is that although size isitself not a major contraindication for earlierpollicization, normal involution of embryonicendosteal circulation during the first year of lifemakes tourniquet control ofintraoperative hem-orrhage more effective if the surgeon delayssurgery until 1 year of age.
Toe phalangeal transfers for augmentation oflength in hypoplastic digits have been per-formed by Carroll and Green16 in patients asyoung as 13 months (using the subperiostealtechnique). Goldberg and Watson29 suggest theextraperiosteal technique is ideally performedbetween 6 and 18 months of age, maximizingthe growth potential of the nonvascularizedtransferred epiphyseal plate. In their experi-ence, the growth potential of the transfer de-creases as the child matures.
Gilbert ~8 suggests that the ideal age for thumbreconstruction using microvascular techniquesof free-tissue transplantation should be 2 years.Demanding mierosurgical efforts depend notonly upon acceptable vascular anatomy in boththe donor and recipient parts, but als0--~ponadequate vessel size, elasticity, and ease of
Figure 38. A and B, Appropriately selectedpatients can undergo free vascularized toe-to-thumb transplantation for congenital failure ofthumb formation; in this case, the second toewas used as donor tissue. With suitable indi-cations, tenorrhaphy, neurorrhaphy, and bonyreconstruction can afford sensibility, stability,and mobility to the reconstructed unit. Physesof all bones of the transplant remain open, andgro~vth potential parallels that of the normalbones of the hand.

nains one of~nd surgery.ggested that.’d at 6 to 12as reported~ (D. Buck-~tion, 1985).nary systempostpartum
,inimal, andaormally by~tion shouldyear.
ough size isfor~ earlierembryonicyear of life
=rative hem-,~eon delays
aentation ofbeen per-patients asLbperiostealsuggest theperformed
maximizing’ascularizedteir experi-:ransfer de-
e for thumbtechniquesbe 9. years.iepend notmy in bothalso upon
~d ease of
.tely selectedMzed toe-to-ital failure ofe second toe~uitable indi-~y, and bonyly, stability,t/nit. Physesin open, and¯ the normal
Management of Thumb Hypoplasia 639
Figure 39. A and B, The rewards of reconstruction of congenital aplasia or hypoplasia of the thumb are functionalimprovement in prehensile grasp and pinch. In these examples, three hands in two affected patients show typical resultsthat can be achieved by pollicization. Any of the techniques described in this article---when used appropriately---canenhance the functional capability of the hand.
~’ation in the abundant subcutaneous tis-sue of the normal infant hand. By 2 year.,; ofage, an infant’s friable arteries and veins have
developed into vessels of substantial thickness,for microvasdular anastomosis. Gilbert
feels that although it is not clearly under-how the new thumb is cerebrocortically
for grasp and pinch, these routinei activities seem easier for the patient when sur-
is performed at a younger age.What is the appropriate age for reconstruc-
tion? The surgeon should take into accountd~ese four points.
Development of the cardiopulmonary systemInvolution of the embryonic endosteal circu-
i i Size of structures and vessel friability, parl:ic-!: ularly in microvascular cases
Normal development of bimanual-grasp as afunctional landmark
SUMMARY
This chapter emphasizes the dilemma of sal-vage and reconstruction of the congenitallyaplastic or hypoplastic thumb .without normalcerebrocortical representation for prehensilegrasp and pinch. The philosophy of reconstruc-tion of the congenitally anomalous thumb isclearly divergent from thumb reconstructionfollowing trauma. It is difficult to advise parentswho seek surgical correction of the severely
deficient thumb ray that amputation is theprocedure of choice, to be followed by transferof an otherwise normal digit to become a func-tional thumb unit. The psychological impact ofthese recommendations may be devastating toparents. Informed understanding of the likelyprogressive development of index-middle fin-ger scissoring, pronation of the index ray withspontaneous broadening of the pulp, and the

640 William B. Kleinman
deteriorating use of an existing hypoplasticthumb may make the decision for ablation easierfor parents. It is critical that these decisions bemade through careful education and under-
standing, considering always the overall grasp-and-pinch capability of the hand as a whole.
Reconstruction of the aplastic or hypoplasticthumb is an exciting and challenging area ofhand surgery. The rewards are improvement ingrasp and pinch either by functional integrationof the reconstructed part, or by complete re-placement of the deficient thumb by tissue fromadjacent or distant donor sites. Success is meas-ured not only in terms of cosmetic appearance,but as enhanced capacity of the child’s hand inall activities of daily living (Fig. 39A and B).
REFERENCES
1. Ahstrom JP Jr: Pollicization in congenital absence ofthe thumb. Cnrr Pract Orthop Surg 5:1, 1973
2. Albee FH: Synthetic transplantation of tissue to form anew finger with restored function of hand. Ann Surg69:379, 1919
3. Barsk,’y AJ: Restoration of the thumb by transplantation,plastic repair, and prosthesis. Surgery 23:227, 1948
4. Barsky AJ: Congenital Anomalies of the Hand and TheirSurgical Treatment. Springfield (IL), Charles Thomas, 1958, p 104
5. Barsky AJ: Reconstructive surgery in congenital, anom-alies of the hand. Surg Clin North Am 39:449, 1959
6. Blair WF, Buckwalter JA: Congenital malposition offlexor pollicis longus: An anatomy note. J Hand Surg8:93, 1983
7. Blauth W: Der hypoplastische daumen. Arch OrthopUntZallchir 62:225, 1967
8. Bocca M, Fongo A, Rinaldi F: Pollicizzazione del quatrodito. Bollettino Societa Pediatria Medica y Chirurgica29:499, 1959
9. Boron R, Fabre A: Technique de reconstruction dupouce. Presse Med 60:1597, 1952
10. Broadbent TR, Woolf RM: Thumb reconstruction withcontiguous skin-bone pedicle graft. Plast ReconstrSurg 25:494, 1960
!1. Buck-Gramcko D: Pollicization of the index finger:Method and results in aplasia and hypoplasia of thethumb. J Bone Joint Surg [Am] 53:1605, 1971
12. Buncke HJ, Buncke CM, Schulz WP: Immediate Ni-choladoni procedure in the Rhesus monkey, or hal-lux-to-hand transplantation, utilizing micro-vascularanastomoses. Br J Plast Surg 19:332, 1966
13. Bunnell S: Physiological reconstruction of a thumb aftertotal loss. Surg Gynecol Obstet 52:245, 1931
14. Butler B Jr: Ring finger pollicization with transplanta-tion of nail bed and matrix on a volar flap. J BoneJoint Surg [Am] 45:1069, 1964
15. Candiollo I, Rinaldi F: Indagini anatomiche sulla vas-colarizzazione arteriosa del IV dito della mano tran-slato sul primo metacarpo (IV dito "pollicizzato"). Acad Med Torino 123:82, 1960
16. Carroll RE, Green DP: Reconstruction of the hypo-plastic digit using toe phalanges. J Bone Joint Surg[Am] 57:272, 1975
17. Chase RA: An alternate to pollicization in subtotal
thumb reconstruction. Plast Reconstr Surg 44:421,1969
18. Clarkson P: Reconstruction of hand digits by toe trans-fers. J Bone Joint Surg [Am] 37:270, 1955
19. Cobbett JR: Free digital transfer. Report of a case oftransfer of a great toe to replace an amputated thumb.J Bone Joint Surg [Br] 51:677, 1969
20. Conway G, Bowe J: Congenital deformities of the hand.Plast Reconstr Surg 18:286, 1956
21. Dunham T: A method for obtaining a skin flap fromthe scalp and a permanent buried vascular pediclefor covering defects of the face. Ann Surg 17:677,1893
22. Edgerton MT, Snyder GB, Webb WL: Surgical treat-ment of congenital thumb deformities (includingpsychological impact of correction). J Bone Joint Surg[Am] 47:1453, 1965
23. Entin MA: Reconstruction of congenital abnormalitiesof the upper extremity. J Bone Joint Surg [Am]41:681, 1959
24. Fitch RD, Urbaniak JR, Ruderman RJ: Conjoined flexorand extensor pollicis longus tendons iu the hypoplas-tic thumb. J Hand Surg 9A:417, i984
25. Flatt AE: The Care of Congenital Anomalies. St. Louis,CV Mosby, 1977, p 79
26. Gebauer T, Ihl W: Reparacion del pulgar por trans-plante de un dedo de la misma mano. Revista deOrthopedia y Traumatologia. Edicion Latino Ameri-cana 1:28, 1955
27. Gersuuy R: Kleiner mittheilungen: Plasticher ersatzder Wangen-Schleimbaut. Zentralblatt ffir Chirurgiei4:706, 1887
28. Gilbert A: Toe transfers for congenital hand defects. JHand Surg 7:i1S, 1982
29. Goldberg NH, Watson HK: Composite toe (phalanxand epiphysis) transfers in the reconstruction of theaphalangic hand. J Hand Surg 7:454, 1982
30. Gosset J: La pollicisation de l’index (technique chirurg-icale). J Chit (Paris) 65:403, 1949
31. Guermonprez F: Sur le prognostic des mutilations dela main. Bulletin de la Societe de Chirurgie Paris10:363, 1884
32. Guermonprez F: Notes Sure Quelques Resections et
Restaurations du Pouce. Paris, P. Asselin, 1887, p 133. Guermonprez F and Derode: Notes Sur Les Indications
de la Restauration du Pouce. Toulouse, Imprimerid~Pinel, 1889
34. Harrison SH: Pollicization in cases of radial club hand.Br J Plast Surg 23:192, 1970
35. Harrison SH: Pollicization in children. Hand 3:204,1971
36. Hilgenfeldt O: Operative Daumefiersatz und Seittigungvon Griefsverungen bei Fingerverlusten. Stuttgart,Enke V, 1950, p 1
37. Huber E: Hilfsoperation bei medianuslahmung.
Deutsche Zeitscrift f~r Chirurgie 162:271, 192138. Huguier PC: Replacement du pouce par son metacar-
pien, par l’angradissement du premier espace inter-osseoux. Arch Gen Med (Paris) 1:78, 1874
39. Jepson PN: Transformation of the middle finger into a "~thumb. Minn Med 8:552, 1925 : :
40. Johnson CF: Abnormal thumbs and physical diagnosisl !Cfin Pediatr 9:131, 1970
41. Joyce JL: A new operation for the substitution of athumb. Br J Surg 5:499, 1918
42. Kelikian H: Congenital Deformities of the Hand andForearm. Philadelphia, WB Saunders, 1974, p 825
43. Kelleher JC, Sullivian JG: Thumb reconstruction byfifth digit transposition. Plast Reconstr Surg 21:470,1958

Surg 44:421,
by toe trans-
: ofacase oftated thumb.
s of the hand.
kin flap fromcular pedicleSurg 17:677,
;urgical treat-es (includingme Joint Surg
abnormalities.t Surg [Am]
njoined flexorthe hypoplas-
ies. St. Louis,
;at por trans-a. Revista de~,atino Ameri-
sticher ersatzffir Chirurgie
and defects, j
toe (phalanxructiou of the.982aique, chirurg-
aautilations dehirurgie Paris
Resections etdin, 1887, p 1,es Indicationse, Imprimerie
~ial club hand.
Hand 3:204,
und Seittigungten. Stuttgart,,~
ianuslahmung.271, 1921r sonr espace inter-1874.e finger into a
bstitution of
the Hand and, 1~974,3ffstruction:r Surg 21:470,
Management of Thumb Hypoplasia 64144. Kessler I, Baruch A, Hecht O: Experience with dis-
traction lengthening of digital rays in congenitalanomalies. J Hand Surg 2:394, 1977
45. Lamb DW: Radial club hand: A continuing study ofsixty-eight patients with one hundred and seventeenclub hands. J Bone Joint Surg [Am] 59:1, 1977
46. LeTac R: Reconstitution du pouce detruit par pollicis-ation de l’annulaire ou du 5e doigt. Mere Acad Chir(Paris) 78:262, 1952
47. Littler JW: Neurovascular pedicle method of digitaltransposition for reconstruction of the thumb. PlastReconstr Surg 12:303, 1953
48. Littler JW: Panel II, Reconstruction of the thumb.Trans Int Soc Plast Surg (Third Congress, Washing-ton, D.C.), 1963
49. Littler JW: Digital transposition. Curr Pract OrthopSurg 3:157, 1966
:!L Littler JW: On making a thumb: One hundred years ofsurgical effort. J Hand Surg 1:35, 1976
5i. Luksch h Uber eine nene methode zum ersatz desverlorenen daumens. Verhandelingen der DeutscheGesellschaft Chirurgie 32:221, 1903
52. Machal: Beitrag zur daumenptastick. Beitr Klin Chir114:181, 1919
53. Manske PR, McCarroll HR: Abductor digit minimiopponens-plasty in congenital radial dysplasia. JHand Surg 3:552, 1978
54. Match RM: The use of a skin flap from a floating thumbin pollicization of the index. Plast Reconstr Surg61:790, 1978
.-’; Mater IB: Thumb reconstruction after amputation atthe metacarpophalangeal joint by bone-lengthening:A preliminary, report of three cases. J Bone JointSurg [Am] 52:957, 1970
56. /Vlatev IB: Thumb reconstruction in children throughmetacarpal lengthening. Plast Reconstr Surg 64:665,1979
57. May JW, Smith RJ, Piemer CA: Toe-to-hand free-tissue transfer for thumb construction with multipledigit aplasia. Plast Reconstr Surg 67:205, 1981.
58. Milford L: The Hand. In Edmonson AS and CrenshawAH (eds): Campbell’s Operative Orthopaedics, ed St. Lous, CV Mosby, 1987, p 419
59. Milford L: The Hand, ed 3. St. Louis, CV Mosby,1987, p 309
Moberg E: The place of nerve-grafting in orthopaedicsurgery. J Bone Joint Surg [Am] 37:305, 1955
L Mfiller W: Anatomische studien zur frage des daum-menersatzes.-Beitrage zur Klinik Chirurgie 120:595,
!,~i~ 1920~62 Mfiller W: Die angeborenen fehlbildungen der men-
schlichen. Hand 1937, Thieme, LeipzigNeviaser RJ: Congenital hypoplasia of the thumb with
absence of the extrinsic extensors, abductor pollicislongus, and thenar muscles. J Hand Surg 4:301, 1979
Nicoladoni C: Daumenplastic. Wein Klin Wochenschr10:663, 1897
Noesske K: Uber den plastischen ersatz von ganz oder
teilweise verlorene fingern, insbesondere des dau-mens, und uber handtelterplastik. Munch MedWochenschr 56:1403, 1909
66. O’Brien BM, Black MJ, Morrison WA, et al: Microvas-cular great toe transfer for congenital absence of thethumb. Hand 10:113, 1978
67. Oudard JS: Greffe de doigts par transplantation. Revd’Orthop (3rd series) 9:413, 1922
68. Pierce GW: Reconstruction of the thumb after totalloss. Surg Gynecol Obstet 45:825, 1927
69. Poznanski AK, Holt JF: The carpals in congenitalmalformation syndromes. Am J Roentgenol 122:443,1971
70. Poznanski AK, Garn SM, Holt JF: The thumb incongenital malformation syndromes. Radiology100:115, 1971
71. Riordan DC: Congenital absence of the radius. J BoneJoint Surg [Am] 37:1129, 1955
72. Salama R, Weissman SL: Congenital bilateral anoma-lous band betxveen flexor and extensor pollicis longustendons. Hand 7:25, 1975
73. Schmiedt W: Beitrag zur daumenplastik. DeutscheZeitschift ffir Chirurgie 145:420, 1918
74. Shepelmann: Plastieher ersatz bei totaldefekt des re-chten daumens. Z Orthop Clair 34:1914, 35:1916,39:1919
75. Smith RJ, Lipke RW: Treatment of congenital defor-mities of the hand and forearm, part 1. N Engl JMed 300:344, 1979
76. Tajima T: Classification of thumb hypoplasia. HandClin 1985, p 577
77. Tsuyuguchi Y, Masada K, Kawabata H, et al: Congen-ital collapsed thumb: A review of forty-three cases.J Hand Surg [Am] 10:613, 1985
78. Tubiana R, Stack HG, Hakistan RW: Restoration ofprehension after severe mutilation of the hand. JBone Joint Surg [Br] 48:455, 1966
79. Tupper JW: Pollex abductus due to congenital malpo-sition of the flexor pollicis longus. J Bone Joint Surg51A:285, 1969
80i" White WF: Fundamental priorities in pollicization. JBone Joint Surg [Br] 52:438, 1970
81. Wissinger HA, Singsen EG: Abductor digiti quintiopponensplasty. J Bone Joint Surg [Am] 59:895, 1977
82. Wood VE: Congenital thumb deformities. Clin Orthop--185:7, 1985
83. Yoshimura M: Toe-to-hand transfer. Plast ReconstrSurg 66:74, 1980
84. Zaucolli E: Transplantation of the index finger in con-genital absence of the thumbjJ Bone Joint Surg[Am] 42:658, 1960
Address reprint requests to
William B. Kleinman, MDThe Indiana Center for Surgery and Rehabilitation
of the Hand and Upper Extremity8501 Harcourt Road
Indianapolis, IN 46260