Management of the First Stage of Labour Lecture
48
MANAGEMENT OF THE FIRST STAGE OF LABOUR FNP LECTURE THEME 4 Lecturer : Ms Aliti Qarikau
-
Upload
josateki-qioniwasa -
Category
Documents
-
view
218 -
download
0
Transcript of Management of the First Stage of Labour Lecture

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 1/48
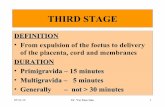
MANAGEMENT OF THEFIRST STAGE OF LABOUR
FNP LECTURE
THEME 4Lecturer : Ms Aliti Qarikau

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 2/48
Objectives
� At the end of this theme students would beable to :
� Discuss normal labour
� Define terminologies� Describe the management of first stage of
labour� describe events/ care of the first stage of
labour� Discuss promotion and maintenance of
aseptic technique

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 3/48
Introduction� Care during labour should be aimed towards achieving the
best possible physical, emotional and psychologicaloutcome for the woman and baby.
� The onset of labour is a complex physiological process andtherefore it cannot be easily defined by a single event.Although labour is a continuous process, it is convenient to
divide it into stages.
� Definitions of the stages of labour need to be clear in orderto ensure that women and the staff providing their carehave an accurate and shared understanding of the conceptsinvolved, enabling them to communicate effectively.

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 4/48
1- Latent Phase of Labor:
�
Uterine contractionmay be very mild,irregular
� not forceful enough tocause much pressure
on the cervix.� the cervix slowlybecomes shorter andsofter. This is knownas 'Effacement'.
� Dilation of the cervixoccurs from 0 cm to 4cm.
� frequency at thisstage is from 1-3 per 10minutes and eachcontraction lasts forless than a minute.
� The uterus maybecome firm and moreprominent with everycontraction.

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 5/48
� In some women, the labor pains start at the
back. This is more likely if the head of the fetusis more posteriorly placed and presses on themother's spine or ligaments.

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 6/48

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 7/48

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 8/48
2.Active Phase of Labor:
� uterus contractsmore frequently andthe pain ismaximum.
� Uterine contractionoccurs after every 3-5
minutes and lasts formore than a minute.
� The uterus becomeshard and moreprominent as thepain increases andsofter as the uterusrelaxes

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 9/48
� The pains sometimes start at the back and
radiates down to the thighs. Later on, at theend of this stage, the pains come even morefrequently and appear to run into each other inquick succession.
� The cervix dilates from 4 cm to 8 cm. Womenwhose waters have not ruptured at the onset oflabour, can experience a gush of water flowing
out of the vagina at this stage.

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 10/48
3.Transitional Phase of Labor:
� marks the transitionfrom the first stage oflabour to the secondstage of labour.
� The cervix dilates from8 cm to 10 cm
� At full dilatation at theend of the first stage oflabour, the cervix isabout 10 cm in diameter
� ( the maximum diameterof the fetal head is also10 cm when it is in anormal position, the
baby can be born easilythrough the cervix)

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 11/48
Characteristics of T/phase
� Restlessness
� Hyperventilation
� Bewilderment andsometimes anger
� Difficulty followingdirections
� Focus on self
� Irritability
� Statements like ´don·ttouch meµ
� Nausea, occasionallyvomiting
� Very warm feeling
�
Perspiration on upperlips
� Increasing rectalpressure

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 12/48
ADMISSION OF CLIENT IN LABOUR
� May be different foreach person
� Each client must be
cared for individuallybased on herparticular situation
� Assessing thecondition of mother
and fetus may beundertaken in a
sequential order ormay need to beperformed
simultaneously.� It is important todetermine whichstage of labour thewoman may be in
at the time ofadmission

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 13/48
When a woman is admitted in early labour,time can be taken to establish the nurse client
relationship by:� Making the woman
and her partner orfamily feel welcome
� Determining theirexpectations aboutthe birth (did theyattend childbirthclasses/)
� Identifying culturalvalues andpreferences related to
the birth process

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 14/48
Initial assessment
� A copy of the prenatal record is added to theclient·s admission record
� Clients who have not received prenatal care
will need more extensive assessment.

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 15/48
When a woman is admitted in active labour, ahistory is taken and an examination undertaken.
The examination includes:�temperature�pulse�Respiration�
blood pressure�Auscultation of heart and lungs�Fetal heart rate (FHR), continuous fetal monitoring-
CTG

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 16/48
� Contractions monitored for frequency,
duration and intensity
� state of hydration
� the urine should be tested for glucose, ketone
bodies and protein� Inspection for signs of edema of face, hands,
legs and sacrum

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 17/48
Examination of the abdomen:�
inspection, palpation and auscultation todetermine: the fetal lie, presentation and position,and the station of the presenting part, as well asto determine the presence of a fetal heartbeat�(The FH beat may be heard in various places on
the mother·s abdomen depending on the positionof the fetus)

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 18/48
VAGINAL EXAMINATION :should be performed only after cleansing of the
vulva and introitus and using an aseptic techniquewith sterile gloves and an antiseptic cream.

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 19/48
The following factors should be noted:
�
the consistency, effacement and dilatation of the cervix�whether the membranes are intact or rupturedand,
if ruptured, the colour of the amniotic fluid�presence of bloody show�nature and presentation of the presenting part�its relationship to the level of the ischial spines�
assessment of the bony pelvis and in particularof the pelvic outlet

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 20/48

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 21/48
CONTRACTIONS:� are assessed by
placing the fingers ofone hand on thefundus of the uterus,and using a light
pressure to keep thefingers still
� begin in the fundusand spreads down
the uterus
� Person assessing the
uterine contractionscan feel thetightening of theuterus before the
woman is aware of it

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 22/48
� At least 3 contractions ina row should be assessed
� The time eachcontraction begins andends (duration) and the
time lapse betweencontractions (frequency),should be noted.
� The intensity can beestimated by how easilythe uterus can be
indented during acontraction.

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 23/48
Mild contraction Uterus is easily indentedwith the fingertips; feels
like the tip of the nosemoderatecontraction
Uterus is more difficult toindent with the fingertips;feels similar to the chin
Strong contraction Uterus unable to beindented with fingertips;feels like the forehead

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 24/48

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 25/48

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 26/48
� Station is a term used to describe the descent ofthe baby into the pelvis. An imaginary line isdrawn between the ischial spines. This is the
"zero" line, and when the baby reaches this line itis considered to be in "zero station."
� When the baby is above this imaginary line it isin a minus station.
�
When the baby is below, it is in a "plus" station.� Stations are measured from -5 at the pelvic inlet
to +4 at the pelvic outlet

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 27/48

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 28/48

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 29/48
Nursing interventions
Focuses on continuous assessment of :� labour progress and fetal well-being
� providing maternal physical care
�
Assisting the client and her supportperson
� Providing and assisting withpharmacological comfort measures

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 30/48
1) Continuous assessment of labour and fetalwell-being
� The nurse personally assess labourprogress, times the contractions and
listens to the FHR at regular intervals� Records findings on the partogram
� One to one continuous support

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 31/48

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 32/48
Electronic fetal monitoring
� 2Types
- 1) intermittent auscultation(sonicaid/doppler)
2) continuous EFM (CTG)
� EFM provides a visual record of the FHR inrelation to the uterine contractions
� It allows early detection of fetal distressand abnormal uterine activity

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 33/48
Changing from intermittent auscultation to
continuous EFM
� Significant meconium stained liquor (alsoconsidered for light meconium stained
� Abnormal FHR detected by intermittent
auscultation-less than 110bpm greater than160bpm, any decelerations after contractions
� Maternal pyrexia defined > 38°C/once or
37.5°C on 2 occasions 2 hrs apart.� Fresh bleeding developing in labour

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 34/48
� External indirectmonitoring (CTGcardiotocograph
procedure:� A tocodynamometer
(for uterine activity) isplaced on the mother·sabdomen near the
fundus� A strap around the
mother holds it inplace
� A doppler transducer(ultrasonic device) isplaced on the mother·sabdomen and movedaround until the fetalheart is heard the best-this is also strapped inplace
� Sound waves are
bounced off the fetalheart and picked up anddisplayed by themonitor

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 35/48
2- Providing maternal physical care
Includes:
� comfort measures
� hygiene measures� ambulation and position
� food and fluid intake
� elimination

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 36/48
a) Comfort measures
� Offering the clientfluids
� Providing oral care� Assisting the client
with frequent position
changes- (encourageside-lying or uprightpositions)
� Providingencouragement and
praise

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 37/48
� Suggesting the use ofcold wash cloth on
the forehead or napeof the neck
� Keeping clientinformed of theprogress
� Giving back rub
� Assist client in
walking to showers� Offering analgesics as
ordered

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 38/48
b) Hygiene measures
� Offer showers if not contraindicated for theclient
� Bed linens should be clean and dry
� Change mackintosh frequently if needed
� Perineal care/changing of sanitary padswhen soaked
�
Oral care

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 39/48
c) Ambulation and position
� May increase uterine
activity, providedistraction from thediscomforts of labour,enhance maternalcontrol of the situation
� Encourage client towalk only if: themembranes are stillintact
� Presenting part is
engaged after ROM� If she has not had
pain medication.
� Side- lying position
promotes utero-placental blood flow
� Upright position-
place pillow underone hip to keep
uterus fromcompressing theaorta and vena cava

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 40/48
d) Food and fluid intake
� Clear fluids are all that is offered
� Sometimes I.V fluids are started on clients
� Keep an accurate I&O record if I.V fluid sare infusing
� (danger of hypervolemia)

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 41/48
Elimination
�
Encourage client to void every2
hours� Allow to walk to bathroom if not
contraindicated
� Catheterize if client cannot void and
bladder is distended� Monitor input & output

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 42/48
Assisting client and support persons
� S/P can be : the baby·s father or may beanother man or woman
� Should be treated with respect regardless of
relationship to the mother or fetus� Breathing techniques 3 types:-
� Slow deep breathing
� Shallow breathing
� Pant- blow breathing

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 43/48
Providing pharmacologicalcomfort measures
� Non- pharmacological ² (as discussed earlier)
� Pharmacological- systemic medications,regional blocks, general anesthesia
�
Systemic medications should be administeredonly if:
� The client is willing to receive them and vitalsigns are stable

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 44/48
� The fetus is :
�
term� exhibits normal
movement, FHR is120-160bpm with no
late or variabledecelerations
� Amniotic fluid is notmeconium stained
� Contractions:
- Are well established- Cervix dilated at
least 4-5cm in anullipara, 3-4cm in a
multipara,presenting part isengaged
- No complications areidentified

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 45/48
� Effects on the fetus depends on:
� The dosage given, timing and route of
administration and the pharmacokinetics of thedrug (best avoided if there is less than 3 hoursbefore delivery).

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 46/48
Assessment Latentphase
Activephase
Transitionphase
2nd stage
BP,P, R q1h q1h q30min q5min
temperature q4h q4h q4h
(if ROM) q2h q2h q2h
FHR q1h q3omin q15min q5min
contractions q1h q30min q15min continuously
Suggested time frame for selected assessments
Promotion and maintenance of aseptic

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 47/48
Promotion and maintenance of aseptictechnique
� Wear disposal gloves
anytime hands mightcome in contact withamniotic fluid, bloodyshow, urine or feces
� Wear splash aprons and
eye-covering (goggles orface masks) when thesplashing of body fluidsis possible
� Wash hands before
putting on gloves and
immediately afterremoving them
� Before catheterization-cleanse vulva andperineum thoroughly toremove any amniotic
fluid and bloody show� Avoid unnecessary V.E
� Use of sterile trays/instruments

8/6/2019 Management of the First Stage of Labour Lecture
http://slidepdf.com/reader/full/management-of-the-first-stage-of-labour-lecture 48/48
Referencing
� White. L, (2005). F oundations of Maternal & pediatric nursing.(2nd ed.). Thomson, Delmarlearning
� Fraser, D. M, Cooper, A. (2003). Myles text book for Midwives (14th ed.).Churchill Livingston,Elsevier.
� Olds, London, Ladewig.(1992).Maternal-
Newborn Nursing A
family- centeredapproach.(4th ed.).Addison Wesley. RedwoodCity.