Management of the Axilla in Patients Receiving Neoadjuvant Chemotherapy (neoCTX) for Breast Cancer...
24
Management of the Axilla in Management of the Axilla in Patients Receiving Patients Receiving Neoadjuvant Chemotherapy Neoadjuvant Chemotherapy (neoCTX) for Breast Cancer (neoCTX) for Breast Cancer Lisa A. Newman, M.D., M.P.H., F.A.C.S. Professor of Surgery Director, Breast Care Center University of Michigan Ann Arbor, MI
-
Upload
ella-palmer -
Category
Documents
-
view
220 -
download
1
Transcript of Management of the Axilla in Patients Receiving Neoadjuvant Chemotherapy (neoCTX) for Breast Cancer...
Management of the Axilla in Patients Management of the Axilla in Patients Receiving Receiving
Neoadjuvant Chemotherapy (neoCTX) Neoadjuvant Chemotherapy (neoCTX) for Breast Cancerfor Breast Cancer
Lisa A. Newman, M.D., M.P.H., F.A.C.S.Professor of Surgery
Director, Breast Care CenterUniversity of Michigan
Ann Arbor, MI

CTX Effect on Primary Tumor
Expanding BCS Eligibility: Neoadjuvant Systemic Therapy

Preop vs Postop CTX: Randomized Trials
Study Stg F/UBCS LR after BCS
OverallSurvival
Pre Post Pre Post Pre Post
InstitutCurie
2-3 66 m 82% 77% 24% 18% 86% 78%
RoyalMars
1-3 48 m 89% 78% 3% 4% 80% 80%
NSABP B18
1-3 108 m 68% 60% 10.7% 7.6% 69% 70%

Surgical Staging of the Axilla
Axillary Lymph Node Dissection
•Morbidity: Lymphedema, Numbness, Shoulder dysfunction
Lymphatic Mapping & SLN Bx
•Alternative surgical staging strategy; minimizes risks of axillary surgery without compromising staging/treatment•Goal: Replicate pathway of cancer cells from primary tumor to initial draining axillary lymph node(s)

Is SLN Bx Compatible with Neoadjuvant CTX Protocols?Should it be performed pre-; post-; or pre- and post-CTX?
•What happens to intramammary lymphatics as the primary breast tumor enlarges?
•Does chemotherapy have a uniform effect on all axillary nodal metastases?
•Does chemotherapy alter lymphatic drainage patterns?

SLN ACCURACY IN T2/T3 TUMORS
Findings Study Year
Tumor Size
N ID Rate FN Rate
Bedrosian 2000 2 cm 104 99% 3% (2/61)
Chung 2001 5 cm 41 100% 3% (1/31)
• What happens to intramammary lymphatics as the primary breast tumor enlarges?
Are SLN non-identification and false negative rates higher in cases of bulky breast tumors?
CTX EFFECT ON AXILLARY METASTASES
• Inferential Evidence:Decreased rates of node-positive disease in pts
treated with neoadjuvant CTX• NSABP B-18
• Direct Evidence: Studies of pts with node-pos disease (documented
by sono-guided FNA Bx) treated with neoadjuvant CTX:
23-33% converted to node-negative status on post-CTX axillary lymph node dissection
• Newman et al, Ann Surg Onc 2002• Rouzier et al, JCO 2002• Kuerer et al, Ann Surg 1999

SLN BX AFTER NEOADJUVANT CTX
Study N ID FN Mets Limited to SLN
Breslin 2000 51 85% 12% 40%
Nason 2000 15 87% 33% NR
Haid 2001 33 88% 0% 50%
Tafra 2001 29 93% 0% NR
Julian 2002 34 91% 0% 42%
Miller 2002 35 86% 0% 44%
Brady 2002 14 93% 0% 60%
Piato 2003 42 98% 17% 0%
Balch 2003 32 97% 5% 56%
Schwartz 2003 21 100% 9% 64%
Reitsamer 2003 30 87% 7% 53%
Mamounas 2005 428 85% 11% 50%
Tanaka 2006 70 90% 5% 42%

SLN BX PRIOR TO NEOADJUVANT CTX
Study NPre-CTX Post-CTXSLNID SLN +
ALNDperformed
ALND neg (%)
Zirngibl2002
15 93% 43% Only SLN+ 100%
Sabel2003
24 100% 42% Only SLN+ 30%
Olilla2003
22 100% 45% All pts
12 SLN-neg pts: 100%
10 SLN-pos pts: 60%

ADVANTAGES OF PRE-neoCTX VS. POST-neoCTX SLN BX
Following neoCTX Before neoCTX
Pro
• More data on results of SLN Bx performed after neoadjuvant CTX delivered
• Surgical sequence consistent with conventional neoadjuvant regimen
• Significance of nodal status better understood when axillary staging performed at diagnosis
• Preferred by many medical and radiation oncologists
• More surgical experience with SLN Bx in the pre-CTX setting
Con
• False negative rates not yet optimized- range, 0-40%
• Significant learning curve
• ? Unnecessary ALND’s- metastatic disease limited to
the excised SLN in 30-50% - CTX sterilizes 25-30% node-
pos pts• Requires additional surgery

UNIVERSITY OF MICHIGAN NEOCTX PROGRAM
Comprehensive pre- and post-
Neoadjuvant CTX axillary evaluation
• Baseline axillary ultrasound– With sono-guided FNA-Bx of any suspicious nodes
• Baseline SLN Bx in sono-neg pts
• After completion of neoCTX:– Pre-CTX node-neg pts → → No further axillary surgery– Pre-CTX node-pos pts → → SLN Bx + cALND

Rationale for SLN Bx after Negative Axillary Ultrasound: Risk of False Negative Imaging
• University of Michigan
• Growney et al, SSO 2009–121 node-positive cases
–Nodal mets documented by sono FNA in 88 (73%) and by SLN biopsy in 33 (27%)
–Follow-up SLN necessary for accurate staging in ultrasound-negative cases

UM Approach to NeoCTX and Axillary Staging
–Pts presenting with node-neg disease–Pts presenting with node-pos disease,
downstaged to pN-0–Pts presenting with node-pos disease that is
chemoresistant
Pre- and post-CTX staging allows stratification of pts into 3 distinct categories

Is it necessary to document the pathologic axillary status prior to delivery of
neoadjuvant chemotherapy?

Operable Breast CancerOperable Breast Cancer
StratificationStratification
• • AgeAge• • Clinical Tumor SizeClinical Tumor Size• • Clinical Nodal StatusClinical Nodal Status
SurgerySurgery
AC x 4AC x 4 SurgerySurgery
NSABP B-18: NSABP B-18: Patterns of Locoregional FailurePatterns of Locoregional Failure
AC x 4AC x 4
Tamoxifen X 5 years for pts Tamoxifen X 5 years for pts >> 50 after completion of chemo 50 after completion of chemo
Fisher B. et al: JCO 1997, JCO 1998; Fisher B. et al: JCO 1997, JCO 1998; Wolmark N. et al: JNCI 2001Wolmark N. et al: JNCI 2001
Neoadjuvant vs. Adjuvant ACNeoadjuvant vs. Adjuvant AC
–Stages I-IIIStages I-III
–Lumpectomy patients received Lumpectomy patients received breast XRTbreast XRT
–Mastectomy patients received Mastectomy patients received no chest wall or regional XRTno chest wall or regional XRT
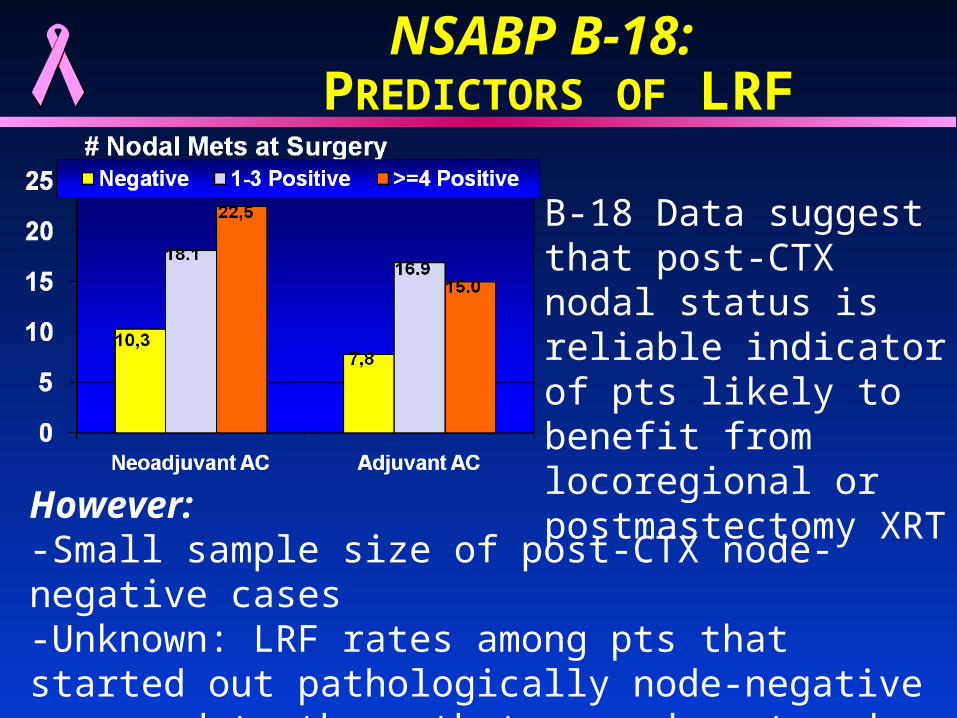
NSABP B-18: PREDICTORS OF LRF
B-18 Data suggest that post-CTX nodal status is reliable indicator of pts likely to benefit from locoregional or postmastectomy XRT
However:-Small sample size of post-CTX node-negative cases-Unknown: LRF rates among pts that started out pathologically node-negative compared to those that were downstaged to node-negativity

UM Neoadjuvant CTX Experience
• N= 161 neoadjuvant chemotherapy cases• Median age at diagnosis 49 years
Mean tumor size at presentation 45.0 mm• Median follow-up 38.1 months • Relapse rate at median follow-up 21.7%
–35 patients–17 Local Recurrences–28 Distant Recurrences
Kilbride et al, Ann Surg Onc 2008

Outcome by Axillary Lymph Node Response
Lymph Node Response
nAny
RelapseLocoReg
RecurrenceDistant
Recurrence
Node-Negative at Presentation
37
(23%)13.5% 8.1% 8.1%
Downstaged to Node-Negative
36
(23%)19.4% 5.6% 13.9%
Persistently Positive
86
(54%)25.6% 14.0% 22.1%
P value 0.13 0.21 0.05

Use of regional radiation (PMRT or breast + nodal fields) in downstaged group
12.5%
3.6%
p=0.33

UM Approach to NeoCTX and Axillary Staging
• Pre- and post-CTX staging allows stratification of pts into 3 distinct categories– Pts presenting with node-neg disease– Pts presenting as node-pos, downstaged to pN-0– Pts presenting as node-pos disease, chemoresistant
• Sequential use of lymphatic mapping offers promise of minimizing number of cases subjected to ALND

UM: 54 Cases of Node-Pos Breast Cancer Undergoing SLN Bx & Completion ALND after
Neoadjuvant CTX
P o s it ive S LN3 3 /36 (92 % )
F a lse ne g a tive3 /3 6 (8 % )
L im ite d to S LN1 2 /36 (33 % )
R e m a ine d no d e p os it ive3 6 /53 (68 % )
N o res id ua l d ise a se1 7 /53 (32 % )
F in a l N o da l S ta tusn = 53
P o s it ive S LN3 3 /36 (92 % )
F a lse ne g a tive3 /3 6 (8 % )
L im ite d to S LN1 2 /36 (33 % )
R e m a ine d no d e p os it ive3 6 /53 (68 % )
N o res id ua l d ise a se1 7 /53 (32 % )
F in a l N o da l S ta tusn = 53 Newman E et al
Ann Surg Onc 2007
Non-identification of post-CTX SLN in 1/54 cases (2%)
The Future: Abandon completion ALND in cases with a neg post-CTX SLN

ACOSOG Z1071 Study Schema
Phase II Study Evaluating the Role of Sentinel Lymph Node Surgery and Axillary Lymph Node
Dissection Following Preoperative Chemotherapy in Women with Node Positive Breast Cancer
Accrual Target: 550 patients

Summary
• Neoadjuvant chemotherapy (neoCTX) improves eligibility for breast-conserving surgery
• Optimal strategy for integrating lymphatic mapping and neoadjuvant CTX remains undefined– Accuracy of sentinel lymph node biopsy not yet
optimally-defined when performed after neoCTX– SLN biopsy prior to neoCTX requires additional surgical
procedure and anesthetic exposure
• Combination of pre- and post- neoCTX axillary staging provides maximal information regarding CTX response and is important for planning XRT

University of Michigan Health CenterUniversity of Michigan Health Center
MUCHAS GRACIAS POR SU ATENCION!!!!