Management of Stroke in the Intensive Care...
20
9/18/16 1 Kyle B Walsh MD Assistant Professor - UC Dept of Emergency Medicine Fellow Physician - Neurocritical Care, Stroke, Research Management of Ischemic Stroke in the Intensive Care Unit Why ICU care matters for ischemic stroke patients Patient Cases To illustrate: Complications following ischemic stroke Subsequent treatments Outline Phases of Stroke Diagnosis and Treatment 1. Making the Diagnosis • Variable complexity of presentation 2. Deciding about Immediate Treatment • tPA, endovascular therapy 3. Subsequent Care • Prevention of further damage and deterioration • Treating potential complications • ICU Care Introduction
Transcript of Management of Stroke in the Intensive Care...

9/18/16
1
KyleBWalshMDAssistantProfessor-UCDeptofEmergencyMedicine
FellowPhysician-NeurocriticalCare,Stroke,Research
ManagementofIschemicStrokeintheIntensiveCareUnit
WhyICUcaremattersforischemicstrokepatientsPatientCases
Toillustrate:
ComplicationsfollowingischemicstrokeSubsequenttreatments
Outline
PhasesofStrokeDiagnosisandTreatment
1. MakingtheDiagnosis• Variablecomplexityofpresentation
2. DecidingaboutImmediateTreatment• tPA,endovasculartherapy
3. SubsequentCare• Preventionoffurtherdamageanddeterioration
• Treatingpotentialcomplications
• ICUCare
Introduction
9/18/16
2
-Howmanypatientsreceiveacutetreatment?
• 370,351acuteischemicstrokeprimarydischargediagnosis• 4%receivedtPA
• 0.5%receivedendovasculartherapy
• Continuedeffortstoincreaseacutetreatmentrates• Subsequentcareisimportant
StrokeTreatment
Adeoyeetal.Stroke.2014Oct;45(10):3019-24.
ICUCareMatters
• Managementbyaneurocriticalcareteam• Decreasedhospitallengthofstay
• DecreasedICUlengthofstay
• Increasedproportionofhomedischarges
NeurocriticalCare
Bershadetal.NeurocritCare.2008;9(3):287-92.
62yearoldmalewokeupwithMildrightarmweakness
Minorfacialdroop
Partialarmsensoryloss
Lastknownnormal7hourspriorNIHSS3
PastMedicalHistory:Diabetes,Hypertension,Hyperlipidemia
SocialHistory:Smoking
Case#1
9/18/16
3
• NotacandidatefortPAorendovasculartherapy• CTheadshowsnohemorrhage• Bloodpressureis210/110Whatshouldbedoneforthepatient’sbloodpressure?
Case#1
• TreatmentthresholdBP>220/120• Lowerthresholdforcomplications(e.g.CHF)
• BPmustbe<185/110toqualifyfortPA• MaintainBP<180/105for24hoursaftertPA
Manypatientswillbehypertensiveafterstroke• SBP>139in77%and>184in15%uponarrivaltoED
Whyallowsuchahighbloodpressure?
Hypertension
Jauchetal.Stroke.2013Mar;44(3):870-947denHertogetal.LancetNeurol.20098:434–440
-Toperfusethepenumbra,theareaofbrainthatisatrisk-Impairedautoregulation,thus,dependentonsystemicBP www.radiologyassistant.nl
9/18/16
4
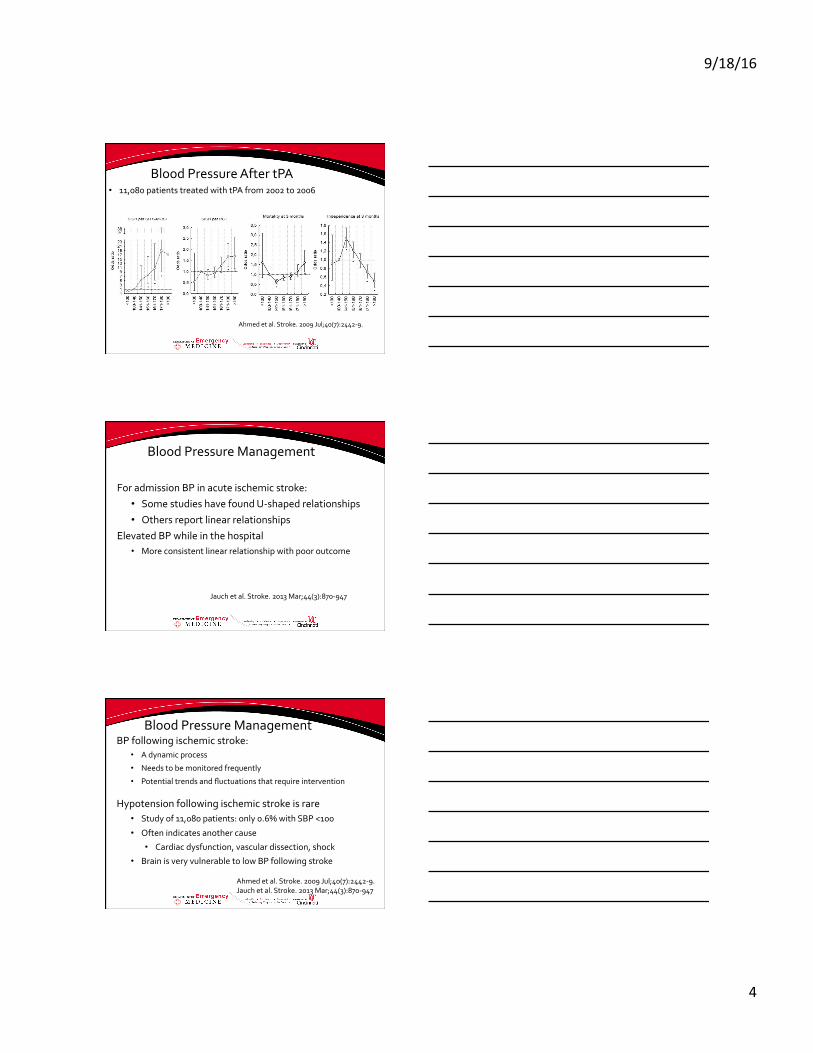
• 11,080patientstreatedwithtPAfrom2002to2006
BloodPressureAftertPA
Ahmedetal.Stroke.2009Jul;40(7):2442-9.
ForadmissionBPinacuteischemicstroke:
• SomestudieshavefoundU-shapedrelationships• Othersreportlinearrelationships
ElevatedBPwhileinthehospital• Moreconsistentlinearrelationshipwithpooroutcome
BloodPressureManagement
Jauchetal.Stroke.2013Mar;44(3):870-947
BPfollowingischemicstroke:• Adynamicprocess
• Needstobemonitoredfrequently
• Potentialtrendsandfluctuationsthatrequireintervention
Hypotensionfollowingischemicstrokeisrare• Studyof11,080patients:only0.6%withSBP<100
• Oftenindicatesanothercause
• Cardiacdysfunction,vasculardissection,shock
• BrainisveryvulnerabletolowBPfollowingstroke
BloodPressureManagement
Ahmedetal.Stroke.2009Jul;40(7):2442-9.Jauchetal.Stroke.2013Mar;44(3):870-947
9/18/16
5
62yearoldmalewokeupwithMildrightarmweakness
Minorfacialdroop
Partialarmsensoryloss
Lastknownnormal7hoursagoNIHSS3
Bloodpressure180/90
Case#1Revisited
Case#1Revisited
2hourslater
Worseningweaknessofrightface,arm,leg,aphasiaNIHSSincreased:3to11
Bloodpressuredecreased:180/90to130/70
Shouldthepatient’sbloodpressurebeincreased?
TherapytoincreasebloodpressureinischemicstrokeApotentialtherapyintheICUEvidencefromsmallstudies
Suggestsafetyandeffectivenessinselectpatients
Whichpatients?
PressorTherapy
9/18/16
6
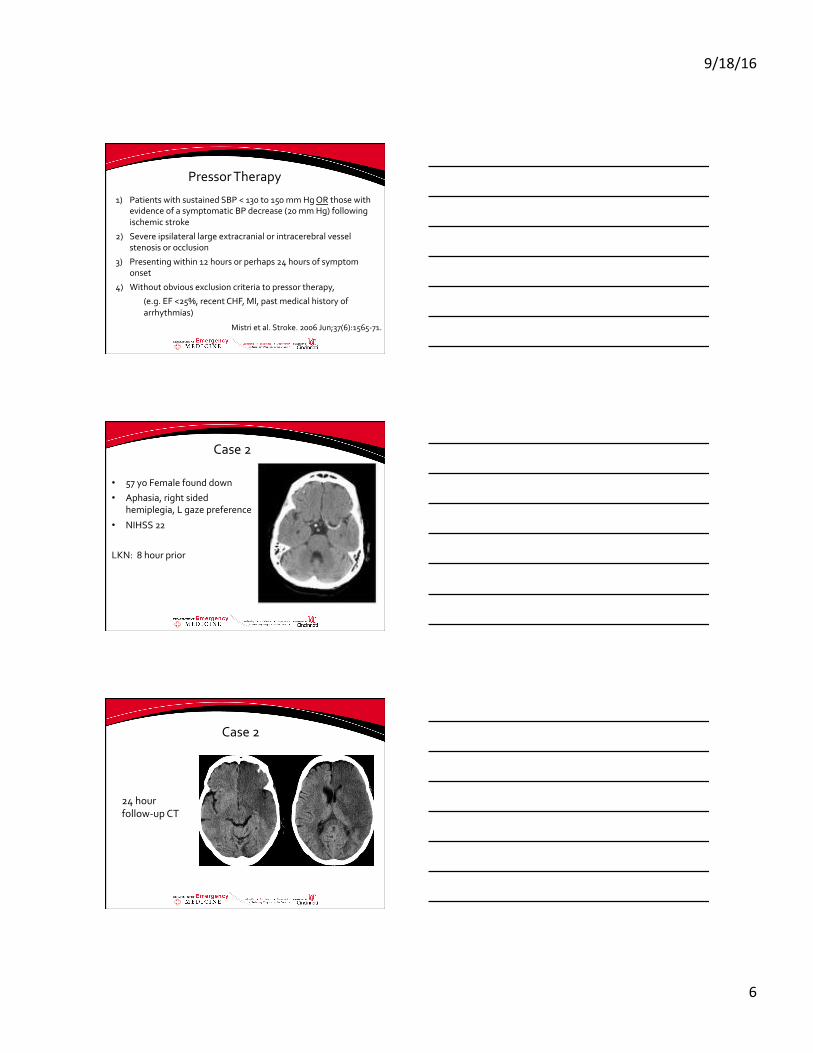
1) PatientswithsustainedSBP<130to150mmHgORthosewithevidenceofasymptomaticBPdecrease(20mmHg)followingischemicstroke
2) Severeipsilaterallargeextracranialorintracerebralvesselstenosisorocclusion
3) Presentingwithin12hoursorperhaps24hoursofsymptomonset
4) Withoutobviousexclusioncriteriatopressortherapy,
(e.g.EF<25%,recentCHF,MI,pastmedicalhistoryofarrhythmias)
PressorTherapy
Mistrietal.Stroke.2006Jun;37(6):1565-71.
• 57yoFemalefounddown• Aphasia,rightsided
hemiplegia,Lgazepreference
• NIHSS22
LKN:8hourprior
Case2
Case2
24hourfollow-upCT

9/18/16
7
MalignantMCAsyndromeSomewithlargestrokeswilldeteriorateininitial24-48hours
MassiveedemaandseveremidlineshiftMalignantstrokesconstituteupto10%ofstrokes
Mortalityisashighas80%Earlyidentificationisessential
MalignantIschemicStroke
Riskfactorsformalignantcerebraledema:1)EarlyCThypodensitygreaterthan50%oftheMCAterritoryORDiffusionlesionvolumegreaterthan82mLwithin6hoursofstrokeonset2)Involvementofadjacentvascularterritories(suchasACAorPCA)
MalignantIschemicStroke
Kasneretal.Stroke.2001Sep;32(9):2117-23.
DecompressivehemicraniectomyToallowspacefortheswellingtooccur
Reducefluidshifts,pressureintheintracranialcompartment
Isitbeneficial?Pooledanalysisof3RCTs,93patients,18-60yearsold
NIHSS>15,CTwithhypodensity>50%MCA
Maximumtimeof48hoursfromstrokeonset
MalignantEdemaTreatment
Vahedietal.LancetNeurol.2007Mar;6(3):215-22.

9/18/16
8
Outcomesat1yearfollowingstrokeMortality: 28%withsurgery,78%withoutmRS0-4: 75%withsurgery,24%without
mRS0-3: 43%withsurgery,21%without
DecompressiveHemicraniectomy
0 - No symptoms. 1 - No significant disability. Able to carry out all usual activities, despite some symptoms. 2 - Slight disability. Able to look after own affairs without assistance, but unable to carry out all previous activities. 3 - Moderate disability. Requires some help, but able to walk unassisted. 4 - Moderately severe disability. Unable to attend to own bodily needs without assistance, and unable to walk unassisted. 5 - Severe disability. Requires constant nursing care and attention, bedridden, incontinent. 6 - Dead.
Whataboutolderpatients?112patientswithmalignantMCA
>61years,(median71,range61-82)
Outcomeat6monthsfollowingstroke:
Mortality: 33%withsurgery,70%without
mRS0-4: 38%withsurgery,18%without
mRS0-2: Nopatients
mRS3: 7%withsurgery,3%without
mRS4: 32%withsurgery,15%without
mRS5: 28%withsurgery,13%without
Juttleretal.NEnglJMed.2014Mar20;370(12):1091-100.
• AtreatmentintheICUformalignantedemaMannitol
TypicallyadministeredasbolusesQ4to6hours
Longhistory,consideredbysometobe“goldstandard”
Hypertonicsaline
Bolusesorcontinuousinfusion
BothreduceICPthroughvariousmechanisms:Volumeredistribution,plasmaexpansion,rheologicmodifications,anti-inflammatoryeffects
HyperosmolarTherapy
Torre-Healyetal.NeurocritCare.2012Aug;17(1):117-30.

9/18/16
9
Mannitol:
Renalfailure,electrolytedisturbances,initialplasmavolumeexpansion,hypotension,ICPrebound
Hypertonicsaline(HS):Renalfailure(lesscommon),electrolytedisturbances,centralpontinemyelinolysis,infusionphlebitis
HSoftendescribedashaving“morefavorablesideeffectprofile.”
AdverseEffects
Markoetal,CritCare.2012Feb20;16(1):113.
Mannitolvs.HS:Whichismoreeffective?Limitedevidence:
• Inischemicstroke:
16of16episodesofincreasedICPrespondedtoHS
10of14respondedtomannitol
• MeanICPreduction11mmHgwithHS,5mmHgwithMannitol
• Meta-analysisof5trialsforelevatedICP(3includedstroke):ICPsuccessfullyreduced78%ofthetimewithmannitol,93%withHS
ShouldHSbethenewgoldstandard?
Schwarzetal.Stroke.1998Aug;29(8):1550-5.
Kameletal.CritCareMed.2011Mar;39(3):554-9.
• 51yearoldmale,suddenonsetofvertigo,vomiting
• Unabletostandorwalkindependently
• BP160/85
• Glucose170
• NIHSS1(ataxia)
• Onsetofsymptoms2hoursprior,treatedwithIVtPA
Case3

9/18/16
10
24hourrepeatCT
Case3
Case3
48hourrepeatCT
• PosteriorcirculationstrokeCanresultinseverecomplicationsdueto:
• Obstructivehydrocephalusfromcompressionofthe4thventricle
• Directcompressionofthebrainstem
Withsignsofbrainstemcompression,mortalityabout80%withoutsurgery
Surgeryreducesmortality
20%forthosetreatedsurgicallyincomatosestate
Case3
Juttleretal.Stroke.2009Sep;40(9):3060-6.

9/18/16
11
Edlowetal.LancetNeurol.2008Oct;7(10):951-64.
Monro-KellieDoctrine
ThebrainisenclosedintheskullThus,thevolumeisconstantAverageadultmale,approximately1500ml1250mlBrain150mlCerebrospinalFluid100mlBloodSomething(i.e.bloodorCSF)mustbepushedoutifpressurerises
Monro-KellieDoctrine

9/18/16
12
TreatmentsforPosteriorCirculationStroke:
EVD:ExternalVentricularDrain
DecompressiveSurgery
MakingthediagnosisiskeyClosemonitoringintheICUsettingEarlyMRI
Involveaneurosurgeonearly
Temporizingmeasuresifindicated
Hyperosmolartherapy
ICUcarefollowingEVDplacementand/ordecompressivecraniotomy
PosteriorCirculationStrokes
72yearoldfemale,leftface/arm/legweakness,rightgazepreference,leftsidedneglect
LKN24hoursprior
NIHSS16
BP160/90
Glucose350
Case4
9/18/16
13
ThoughttoincreasemetabolicdemandinthebrainResultsinlacticacid,variousfreeradical
Neuronalcelllysis,damagetobloodbrainbarrier
Negativeoutcomesnotedinhyperglycemicstrokepatients
• Increasedcerebraledema
• Morehemorrhagicconversion
• Moredisabilityanddeath
Hyperglycemia
Lindsbergetal.Stroke.2004Feb;35(2):363-4Capesetal.Stroke.2001Oct;32(10):2426-32
ControllingbloodglucoselevelsNICE-SUGARstudy:
• 6,104medical/surgicalICUpatients
• Randomizedtointensivecontrol(glucose81-108)vs.conventional(glucose<180)
• Highermortalityinintensivecontrol(27.5vs.24.9%)
• Moreseverehypoglycemia(<40)inintensivecontrol(6.8vs0.5%)
Hyperglycemia
Finferetal.NEnglJMed.2009Mar26;360(13):1283-97.
StrokeHyperglycemiaInsulinNetworkEffort(SHINE)TrialAcuteischemicstroke,RCTof1400patients
Enrolledwithin12hoursofsymptomonset
Randomizedto• Insulingtttomaintainglucose80-130forupto72hours
• Standardcare,i.e.slidingscaleinsulintokeepglucose<180
Outcome:Functionaloutcomeat3months(mRS)
Recentguidelines:Glucose140to180
Morepotentialstrokepatientsoninsulininfusions?
SHINETrial

9/18/16
14
79yearoldmale,aphasiaandrightsidedweakness
LKN2hoursprior
NotPAforINR2.3
BP160/90
Glucose120
12hoursafter
admission:
Temperature101.5
Case5
Elevatedtemperatureafterneurologicinjury• Increasedbrainmetabolicdemand
• Elevatedlevelsofexcitatoryaminoacids
• Increasedischemicdepolarizations
• Blood-brainbarrierbreakdown
• Impairedfunctionofenzymes
Meta-analysiswith14,431patientswithstrokeandotherbraininjury
Increasedtemperatureassociatedwithworseoutcomes
7measuresincludingclinical,functional,economicoutcome
TemperatureManagement
Greeretal.Stroke.2008Nov;39(11):3029-35.
Typesoftemperaturemanagement:AcetaminophenPharmacologicsedation
Surfacecooling
Endovascularcoolingcatheters
Normothermiavs.HypothermiaHowistemperaturemeasured?Coretemperatures?
Theassumptionthatfeverisharmful
TemperatureManagement

9/18/16
15
SmallstudieshaveevaluatedfeasibilityofTTMinstrokePotentialsideeffects:arrhythmias,hypotension,pneumonia
Systematicreview:Noclearbenefitorharm
Shiveringcanbeamajorissue
Increasesmetabolicdemand,potentiallyincreasesICP
HypothermiacanreduceICP
Potentiallydangerousreboundincreasewithmorerewarming
TemperatureManagement
Jauchetal.Stroke.2013Mar;44(3):870-947.Hertogetal.CochraneDatabaseSystRev.2009Jan21
Largenumberofunansweredquestions:Whentostarthypothermia?
Whattargettemperature?Forwhatduration?
Howfasttorewarm?
Whattypeoftemperaturemanagement?(Surface,invasive)
Whichstrokepatients?(e.g.onlylargestrokeswithedema?)
Withothertherapies?(e.g.tPA,angiography,hemicranectomy)
Byitselforwithotherneuroprotectants?
TemperatureManagement
Jauchetal.Stroke.2013Mar;44(3):870-947.
Case664yearoldfemale
SuddenonsetRarmandlegweakness/numbnessIVtPAtreatmentat1.5hours
Diagnosisofnewonsetatrialfibrillation
SymptomsimprovedfollowingtPAAdmittedtoICU
Familymemberasks:“ItakewarfarinforA-Fibtohelppreventstrokes.Shejusthadastroke.Whyisn’tshegettingbloodthinners?”

9/18/16
16
Anticoagulation
Jauchetal.Stroke.2013Mar;44(3):870-947
Earlyadministrationofanticoagulantsfollowingstroke?• Increasedriskofbleeding
Evidencefromclinicaltrials
IncludesbothUFHandLMWH
• Doesnotlessenriskofearlyneurologicalworsening• Doesnotlowerriskofearlyrecurrentstroke
Includingcardioembolicstrokes(A-Fib)
Anticoagulation
TheAHAGuidelinesstate:“Dataareinsufficienttoindicatewhetheranticoagulantsmightbeeffectiveamongsomepotentiallyhigh-riskgroups,suchasthosepeoplewithintracardiacorintra-arterialthrombi.”Startinganticoagulantswithin24hoursofIVtPAisnotrecommendedPatientathighriskforfurtherworseningduetoarterialthrombus?
AnticoagulationpotentiallystartedinICUOftenhighleveldecisionwithmuchdiscussion
Anticoagulation
Toanswerthefamilymember’squestion:
Thepatientwillbeplacedonanticoagulation,butnotnow
Currently,theriskofbleedingismorethanthepotentialbenefit
Treatmentshouldbestartedaftertheriskofhemorrhageintothestroketissuehasreduced

9/18/16
17
Case778yearoldfemalewithRMCAstroke3daysagoMoredifficulttoarousesincehavingaseizure2hoursagoSeizuretreatedwithLorazepam
Thoughttobesleepysecondarytothis
Withreassessment,slighttwitchingoffacialnoted
Mentalstatusimproveswithfurtherseizuretreatment
PatientismonitoredinICUformoreseizureswithcEEG
Theinternasks,“DidweforgettostartAEDs?”
SeizuresAfterIschemicStrokeIncidencevaries,usuallyreportedin<10%ofischemicstrokesMorecommonwithhemorrhagictransformation
Recurrentseizures?Lateonset?Incidencevariessignificantly
Nodemonstratedbenefitofprophylacticanticonvulsants
Recommendationsbasedonestablishedguidelinesfortreatingseizuresinanyneurologicillness
Advancedmonitoringforseizures(cEEG)intheICUsetting
Jauchetal.Stroke.2013Mar;44(3):870-947Kilinceretal.ActaNeurochir.2005;147:587–594
Case848yearoldmale• OnsetofRsidedweaknessand
aphasia24hoursago• TransferredfromOSHforICUcare
• Concernforedema
• Neurosurgeryconsultedforhemicraniectomy
Medicalstudentasks:“IhaveseenotherICUpatientswithbrainswellinghavethesecomplicatedmonitorsplaced.Willthispatienthavethatdone?”

9/18/16
18
MultimodalMonitoringintheICUIntracranialpressure(ICP)
Braintemperature
Braintissueoxygenation
Jugularvenousoxygensaturation
EEG
Biochemicalmilieuofthebrain
e.g.Microdialysis,testingbrainmicroenvironmentmolecules
Currently,morecommonlyperformedfor:
Traumaticbraininjury
Subarachnoidhemorrhage
AdvancedMonitoring
Risticetal.JNeuroanaesthesiolCritCare2015;2:97-103www.labautopedia.org/
Doesthismonitoringprovidemoreinformationthantheneurologicexamination?
• Wheretoplacemonitors
• Focalinjuryvsdiffuse
• Invasivevsnon-invasivemonitors
• Similarparameterstootherdiseasestates?e.g.TBI
-PotentialdifferencesinICPandvenousoxygensaturation
Likelymoremonitoringinthefuture
Goalofoptimizingrecoveryandreducingsecondaryinjury
AdvancedMonitoring
9/18/16
19
Bloodpressureafterstrokeinvolvescomplicatedphysiology• CurrentGuidelinesforfirst24hours:
BP<220/120withouttPA,<180/105aftertPA
Selectpatientsmightbenefitfrompressors
LowBPisrare-thinkaboutothercauses
Malignantedemacanoccurafterstroke
• Potentialtreatmentsincludehemicraniectomy,hypertonicfluid
Hemicrani-lifesavingvs.functionsaving?
Hypertonicsalinevs.mannitol
Summary
Posteriorcirculationstrokecanbedifficulttodiagnosis• Canresultinobstructivehydrocephalus,herniation,death
• EVDandsurgicaltreatmentcanbelifesaving
Hyperglycemiaisthoughttobeharmfultobebrainfollowingstroke
• Isaggressivetreatmenthelpful?Hypoglycemia?
• Currentguidelines:Maintainglucose140-180
• LookforresultsofSHINEtrial
Summary
Temperaturemanagementfollowingstrokeisimportant• Feveristhoughttobebad
• Limitedevidenceforhypothermiavs.normothermia
• Hypothermiainstrokepatientshasuniquechallenges
Anticoagulationearlyafterstrokeisnotacommontreatment
• Selectpatientsmightbenefit
• Morecommonlypatientsarestartedonanticoagulationlater
Summary
9/18/16
20
Seizurescanoccurafterstroke• cEEGmonitoringcantakeplaceintheICU
• Treatactualseizuresbasedonestablishedgeneralguidelines
• Prophylacticanticonvulsantsarenotrecommended
Advancedmultimodalmonitoringhassubstantialpotential
• Manyunansweredquestionsaboutbestmethods
• Likelymoreuseinthefuture
Summary
THANKYOU!