Management of Penetrating Neck Trauma
124
Management of Penetrating Neck Trauma Ottawa Civic
-
Upload
judah-mclaughlin -
Category
Documents
-
view
36 -
download
3
description
Management of Penetrating Neck Trauma. Ottawa Civic. MVA, aphasia, R hemiplegia. Types of Weapons. Low velocity – knives, ice picks, glass High velocity – handguns, shotguns, shrapnel. K=1/2mv^2. Guns.
Transcript of Management of Penetrating Neck Trauma

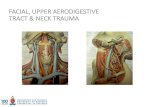
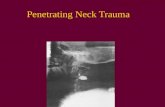
Management of Penetrating Neck Trauma
Ottawa Civic

MVA, aphasia, R hemiplegia

Types of Weapons Low velocity – knives, ice picks, glass High velocity – handguns, shotguns, shrapnel

Guns

Ballistics

Anatomy

Anatomy

Incidence and Mortality


Signs of Injury:

Signs of Injury:

Initial Management

Management of the Stable Patient:
The Standard:

The Standard: Based on wartime experiences Fogelman et al (1956) :
immediate neck exploration-> better outcomes in vascular injuries.
negative neck explorations in > 50% Arteriogram?
screening tool before exploration zone 1 and 3 injuries
hard to detect on physical Safe answer on board exam…

Arteriogram Flint et al (1973):
negative P.E. in 32% of pts. with major zone 1 vascular injury. Arteriogram can be accompanied by treatment (e.g.
embolization).

A Newer Algorithm
Mansour et al 1991 retrospective study

Newer Algorithm (Mansour) 63% of the study population was in the observation
group. Overall mortality 1.5%
similar to those in more rigorous treatment protocols. Similar results obtained in other large studies with
similar protocols (e.g. Biffi et al 1997). NOTE: Arteriogram in asymptomatic patients with zone 1
injury.

Points of Controversy: Most trauma surgeons accept observation of select
patients similar to the Mansour algorithm. Study by Eddy et al
questions the necessity for arteriogram / esophagoscopy in asymptomatic zone 1 injury (use of P.E. and CXR resulted in no false negatives).
Other noninvasive modalities than arteriogram exist for screening patients for vascular injury.

CT scan
Can id weapon trajectory and structures only in stable patients. Gracias et al (2001)
CT scan in stable patients: able to save patients from arteriogram indicated by other protocols 50% of
the time avoid esophagoscopy in 90% of tested patients who might otherwise have
undergone it.

Duplex Ultrasonography Requires the presence of reliable technician and
radiologist. A double blinded study by Ginsburg et al (1996) showed
100% true negative, 100% sensitivity in detecting arterial injury, using arteriography as the gold standard.



Is this really wise??

Incision for Neck Exploration:

Incisions for Neck Exploration:

Management of Vascular Injuries:
Common carotid: repair preferred over ligation in almost all cases. Saphenous vein graft may be used. Shunting is rarely necessary. Thrombectomy may be necessary.
Internal carotid: Shunting is usually necessary
Vertebral: Angiographic embolization proximal ligation can be used if the contralateral vertebral artery is intact.
Internal Jugular: Repair vs. ligation.

Esophageal Injury: Diagnosis:
esophagoscopy and esophagram in symptomatic patients. Injection of air or methylene blue in the mouth may aid in
localizing injuries. Controlled fistula with T-tube
exteriorization of low non-repairable wounds Small pharyngeal lesions above arytenoids can be
treated with NPO and observation 5-7 days All patients should be NPO for 5-7 days.

Laryngeal/Tracheal Injury
Thorough Direct Laryngoscopy for suspicious wounds Tracheotomy for suspected laryngeal injury

Thoracic Trauma

Thoracic Trauma 2nd leading cause of trauma deaths
after head injury 10-20% of all trauma deaths
Many deaths are preventable

Thoracic Trauma Mechanisms of Injury
Blunt Injury Deceleration Compression
Penetrating Injury Combination

Thoracic Trauma
Anatomical Injuries Thoracic Cage (Skeletal) Cardiovascular Pleural and Pulmonary Mediastinal Diaphragmatic Esophageal Penetrating Cardiac

Thoracic Trauma
Hypoxia hypovolemia pulmonary V/P mismatch in intrathoracic pressure relationships
Hypercarbia in intrathoracic pressure relationships level of consciousness
Impairments to cardiac output blood loss increased intrapleural pressures blood in pericardial sac myocardial valve damage
Acidosis – final result hypoperfusion of tissues

Thoracic Trauma Initial exam directed toward life
threatening: Injuries
Open pneumothorax Flail chest Tension pneumothorax Massive hemothorax Cardiac tamponade

Thoracic Trauma
Assessment Findings Mental Status
decreased Pulse
absent, tachy or brady BP
narrow PP, hyper- or hypotension, pulsus paradoxus Ventilatory rate & effort
tachy- or bradypnea, labored, retractions Skin
diaphoresis, pallor, cyanosis, open injury, ecchymosis

Thoracic Trauma
Assessment Findings Neck
tracheal position, SQ emph, JVD, open injury Chest
contusions, tenderness, asymmetry, abN a/e, bowel sounds, abnormal percussion, open injury, impaled object, crepitus, hemoptysis
Heart Sounds muffled, distant, regurgitant murmur
Upper abdomen contusion, open injury

Thoracic Trauma
Assessment Findings ECG (ST segment abnormalities, dysrhythmias)
History Dyspnea Pain Past hx of cardiorespiratory disease Restraint devices used Item/Weapon involved in injury

Thoracic Trauma
Specific Injuries

Rib Fracture
MC chest wall injury from direct trauma More common in adults than children Especially common in elderly
Most commonly 5th - 9th ribs Poor protection

Rib Fracture
Fractures of 1st and 2nd second require high force Frequently have injury to aorta or bronchi Occur in 90% of patients with tracheo-bronchial
rupture May injure subclavian artery/vein
30% will die

Rib Fracture Fractures of 10 to 12th ribs can cause damage
to underlying abdominal solid organs: Liver Spleen Kidneys

Rib Fracture Management
PPV Analgesics for isolated trauma Non-circumferential splinting Monitor elderly and COPD patients closely
Broken ribs can cause decompensation Patients will fail to breathe deeply and cough, resulting in poor
clearance of secretions

Sternal Fracture
Uncommon, 5-8% in blunt chest trauma Large traumatic force Direct blow to front of chest by
Deceleration steering wheel dashboard
Other object

Sternal Fracture
25 - 45% mortality due to associated trauma: Disruption of thoracic aorta Tracheal or bronchial tear Diaphragm rupture Flail chest Myocardial trauma
High incidence of myocardial contusion, cardiac tamponade or
pulmonary contusion

Sternal Fracture Management
Establish airway High concentration oxygen Assist ventilations as needed IV NS/LR
Restrict fluids Rule out associated injuries

Flail Chest
Usually secondary to blunt trauma Most commonly in MVA Also results from
falls from heights industrial accidents assault birth trauma
More common in older patients

Flail Chest
Mortality rates 20-40% due to associated injuries
Mortality increased with advanced age seven or more rib fractures three or more associated injuries shock head injuries

Flail Chest Consequences of flail chest
Respiratory failure due to pulmonary contusion inadequate diaphragm movement Paradoxical movement of the chest
must be large to compromise ventilation Increased work of breathing
decreased chest expansion pain

Flail Chest
Suspect spinal injuries Establish airway Assist ventilation
Treat hypoxia from underlying contusion Promote full lung expansion
Consider need for intubation and PEEP Mechanically stabilize chest wall
questionable value

Flail Chest Management
IV of LR/NS Avoid rapid replacement in hemodynamically stable patient Contused lung cannot handle fluid load
Monitor EKG Chest trauma can cause dysrhythmias

Simple Pneumothorax
Incidence 10-30% in blunt chest trauma almost 100% with penetrating chest trauma Morbidity & Mortality dependent on
extent of atelectasis associated injuries

Simple Pneumothorax
a # rib lacerates lung Usually well-tolerated in the young & healthy Severe compromise can occur in the elderly or
patients with pulmonary disease Degree of distress depends on amount and speed of
collapse

Simple Pneumothorax
HDI and respiratory distress High index of suspicion Chest tube when in doubt before CXR

Open Pneumothorax
If the trauma patient does not ventilate well with an open airway, look for a hole May be subtle Abrasion with deep punctures Opening in the chest wall Sucking sound on inhalation HDI/resp distress SQ Emphysema

Open Pneumothorax
Profound hypoventilation may occur communication between pleural space and
atmosphere Prevents development of negative intrapleural
pressure Results in ipsilateral lung collapse
inability to ventilate affected lung

Open Pneumothorax V/Q Mismatch
shunting hypoventilation hypoxia large functional dead space
Pressure may build within pleural space Return from Vena cava may be impaired

Open Pneumothorax
Cover chest opening with occlusive dressing Assist with positive pressure ventilations prn Monitor for progression to tension
pneumothorax

Tension Pneumothorax
Incidence Penetrating Trauma Blunt Trauma
Morbidity/Mortality Severe hypoventilation Immediate life-threat if not managed early

Tension Pneumothorax
Pathophysiology One-way valve forms in lung or chest wall
Air enters pleural space, but cannot leave Pressure collapses lung on affected side Mediastinal shift to contralateral side
Reduction in cardiac output Increased intrathoracic pressure deformed vena cava reducing preload

Tension Pneumothorax
Severe dyspnea extreme resp distress Restlessness, anxiety, agitation Decreased/absent breath sounds Worsening or Severe Shock Cardiovascular collapse
Tachycardia Weak pulse Hypotension Narrow pulse pressure

Tension Pneumothorax Jugular Vein Distension
absent if also hypovolemic
Hyperresonance to percussion Subcutaneous emphysema Late
Tracheal shift away from injured side Cyanosis

Tension Pneumothorax
Recognize & Manage early Establish airway Needle thoracostomy then chest tube

Tension Pneumothorax
Decompress with 14g (lg bore), 2-inch needle Midclavicular line: 2nd intercostal space Midaxillary line: 4-5th intercostal space Go over superior margin of rib to avoid blood vessels Be careful not to kink or bend needle or catheter If available, attach a one-way valve

Hemothorax
Most common result of major trauma to the chest wall Present in 70 - 80% of penetrating and major non-
penetrating trauma cases Associated with pneumothorax Rib fractures are frequent cause

Hemothorax
Each can hold up to 3000 cc of blood Life-threatening often requiring chest tube and/or
surgery If assoc. with great vessel or cardiac injury
50% die immediately 25% live five to ten minutes 25% may live 30 minutes or longer
Blood loss results in Hypovolemia Decreased ventilation of affected lung

Hemothorax
Accumulation of blood in pleural space penetrating or blunt lung injury chest wall vessels intercostal vessels myocardium
Massive hemothorax indicates great vessel or cardiac injury Intercostal artery can bleed 50 cc/min

Hemothorax
Chest tube, go to OR if 1000 cc out on insertion 200 cc/h for 4 hours

Pulmonary Contusion Pathophysiology
Blunt trauma to the chest Rapid deceleration forces cause lung to strike chest wall high energy shock wave from explosion high velocity missile wound low velocity as with ice pick
Most common injury from blunt thoracic trauma 30-75% of blunt trauma mortality 14-20%

Pulmonary Contusion
Pathophysiology Rib Fx in many but not all cases Alveolar rupture with hemorrhage and edema
increased capillary membrane permeability Large vascular shunts develop
Gas exchange disturbances Hypoxemia Hypercarbia

Pulmonary Contusion Assessment Findings
Evidence of blunt chest trauma Cough and/or Hemoptysis Apprehension Cyanosis CXR changes late

Pulmonary Contusion Management
Supportive therapy Early use of positive pressure ventilation
reduces ventilator therapy duration Avoid aggressive crystalloid infusion Severe cases may require ventilator therapy

Myocardial Contusion
Most common blunt injury to heart Usually due to steering wheel Significant cause of morbidity and mortality
in the blunt trauma patient

Myocardial Contusion Pathophysiology
Behaves like acute MI Hemorrhage with edema
Cellular injury vascular damage may occur
Hemopericardium may occur from lacerated epicardium May produce arrhythmias
hypotension unresponsive to fluid or drug therapy

Myocardial Contusion
Cardiac arrhythmias following blunt chest trauma
Angina-like pain unresponsive to nitroglycerin Precordial discomfort independent of
respiratory movement Pericardial friction rub (late)

Myocardial Contusion
ECG Changes Persistent tachycardia ST elevation, T wave inversion RBBB Atrial flutter, Atrial fibrillation PVCs PACs

Myocardial Contusion
IV LR/NS Cautious fluid administration due to injured myocardium
ECG Standard drug therapy for arrhythmias 12 Lead ECG if time permits
Admit to monitored evironment

Pericardial Tamponade Incidence
Usually associated with penetrating trauma Rare in blunt trauma Occurs in < 2% of chest trauma GSW wounds have higher mortality than stab wounds Lower mortality rate if isolated tamponade

Tamponade is hard to diagnose Hypotension is common in chest trauma Heart sounds are difficult to hear Bulging neck veins may be absent if hypovolemia is
present High index of suspicion is required

Pericardial Tamponade Pathophysiology
Space normally filled with 30-50 ml of straw-colored fluid lubrication lymphatic discharge immunologic protection for the heart
Rapid accumulation of blood in the inelastic pericardium

Pericardial Tamponade Pathophysiology
Heart is compressed decreasing blood entering heart Decreased diastolic expansion and filling Hindered venous return (preload)
Myocardial perfusion decreased due to pressure effects on walls of heart decreased diastolic pressures
Removal of as little as 20 ml of blood may drastically improve cardiac output

Pericardial Tamponade
Beck’s Triad Resistant hypotension Increased central venous pressure
distended neck/arm veins in presence of decreased arterial BP
Small quiet heartdecreased heart sounds

Pericardial Tamponade Signs and Symptoms
Narrowing pulse pressure Pulsus paradoxicus
Radial pulse becomes weak or disappears when patient inhales
Increased intrathoracic pressure on inhalation causes blood to be trapped in lungs temporarily

Pericardial Tamponade Management
ECHO if stable to diagnose In ER –
consider pericardiocentesis Pericardial window followed by sternotomy in OR



Traumatic Aortic Dissection/Rupture
Caused By: Motor Vehicle Collisions Falls from heights Crushing chest trauma Animal Kicks Blunt chest trauma
15% of all blunt trauma deaths

Traumatic Aortic Dissection/Rupture
1 of 6 persons dying in MVC’s has aortic rupture 85% die instantaneously 10-15% survive to hospital
1/3 die within six hours 1/3 die within 24 hours 1/3 survive 3 days or longer
Must have high index of suspicion

Traumatic Aortic Dissection/Rupture
Separation of the aortic intima and media Tear 2° high speed deceleration at points of relative
fixation Blood enters media through a small intima tear
Thinned layer may rupture Descending aorta at the isthmus distal to left
subclavian artery most common site of rupture ligamentum arteriosom

Traumatic Aortic Dissection/Rupture Assessment Findings
Retrosternal or interscapular pain Pain in lower back or one leg Respiratory distress Asymmetrical arm BPs Upper extremity hypertension with
Decreased femoral pulses, OR Absent femoral pulses
Dysphagia

CXR

Work up CTA
Angio is rarely used Address other injuries first Ideally, repaire when stable
Stent vs open

Diaphragmatic Penetration Suspect intra-abdominal trauma with any injury below
4th ICS Suspect intrathoracic trauma with any abdominal injury
above umbilicus

Diaphragmatic Rupture
Usually due to blunt trauma but may occur with penetrating trauma
Usually life-threatening Likely to be associated with other severe
injuries

Diaphragmatic Rupture
Pathophysiology Compression to abdomen resulting in increased
intra-abdominal pressure abdominal contents rupture through diaphragm into chest bowel obstruction and strangulation restriction of lung expansion mediastinal shift
90% occur on left side due to protection of right side by liver

Diaphragmatic Rupture
Assessment Findings Decreased breath sounds
Usually unilateral Dullness to percussion
Dyspnea or Respiratory Distress Scaphoid Abdomen Usually impossible to hear bowel sounds
Management suspect NG tube CT Laparoscopy
Sensitive and specific

Esophageal Injury
Penetrating Injury most frequent cause Rare in blunt trauma Can perforate spontaneously
violent emesis carcinoma

Esophageal Injury
Assessment Findings Pain, local tenderness Hoarseness, Dysphagia, Respiratory distress Mediastinal esophageal perforation
mediastinal emphysema / mediastinal crunch SQ Emphysema
Shock Abx resuscitation Early diagnosis Gastrographin -> dilute Ba Repair vs exclude

Tracheobronchial RuptureUncommon injury
less than 3% of chest traumaOccurs with penetrating or blunt chest trauma
High mortality rate (>30%)Respiratory DistressObvious SQ emphysemaHemoptysis Especially of bright red blood
Signs of tension pneumothorax unresponsive to needle decompression

Tracheobronchial Rupture
Majority (80%) occur at or near carina rapid movement of air into pleural space Tension pneumothorax refractory to needle
decompression Consider early intubation
intubating right or left mainstem may be life saving If arrest and suspect air embolysm, may have to do ERT…

Damage control

Damage control principle…




ED Thoractomy Thoracotomy performed in ER for resuscitation of patients arriving in extremis Plan to take to OR afterwards AIM:
Expeditious control of hemorrhage Maximization of coronary and cerebral perfusion Release of pericardial tamponade Tx of massive air-embolysm

Procedure – Left Anterolateral Thoracotomy

Clamshell Thoracotomy


Release Pericardial Tamponade

Control Intrathoracic Hemorrhage

Eliminate massive air embolism or bronchopleural fistula
Post intubation & positive pressure ventilation Get air transfer across traumatic alveolovenous
channels Pulmonary hilar cross clamping Air aspirated from L ventricular apex and aortic
root Cardiac massage


Perform Open Cardiac Massage
Bimanual internal massage with hands in a hinged clapping motion
Ventricular compression proceeding from apex to base of heart

Occlude Descending Thoracic Aorta

Futile?
Overall survival ~4-5% Little to Lose
risk to Health care workers Risk blood contact 26% trauma pts HIV+ or Hepatitis+
Health care costs
J Trauma. 1998 Jul;45(1):87-94

Selective Application of ED Thoracotomy
Mechanism of Injury Presence of Vital Signs Location of Injury Other Signs of Life

Survival based on mechanism
J Trauma. 1998 Jul;45(1):87-94

Presence of vital signs
J Trauma. 1998 Jul;45(1):87-94

Survival based on organ injured
JACS 2000 Mar;190(3):288-98.

Other Signs of Life (SOL)
JACS 2000 Mar;190(3):288-98.

What about PEA?
JACS 199:211-215, 2004
26/62 (42%) ED Thoracotomy survivors had PEA requiring CPR

Conclusions ER thoracotomy considered in pts w/:
Presence of vital signs in field or hospital Better results in penetrating cardiac injury Results w/ Blunt trauma poor, but survivors exist PEA after penetrating trauma from stabs
Up to 70% good outcomes
Contraindicated in pts with: No vital signs, prolonged asystole and unwitnessed arrest/loss of SOL
JACS 199:211-215, 2004

Finally… PEA after blunt trauma? Typically poor outcome, but occasionally will have a
survivor If CPR > 5 min, contraindicated

References and thanks Thank God for internet and Google several websites specifically:
http://www.adhb.govt.nz/trauma/presentations/Forums/major%20chest%20injuries/sld001.htm
http://www.templejc.edu/dept/ems/Pages/PowerPoint.html http://www.mssurg.net www.nordictraumarad.com/Syllabus06/mo%2015/NORDTERpenetrating.pdf www.iformix.com/spu/chest_trauma.ppt Greenfield textbook of surgery