Management of Pediatric Hemangiomas - UCSF CME · Management of Pediatric Hemangiomas Anna K....
23
1 Management of Pediatric Management of Pediatric Hemangiomas Hemangiomas Anna K. Meyer, M.D., F.A.A.P. Anna K. Meyer, M.D., F.A.A.P. Assistant Professor Assistant Professor Division of Pediatric Otolaryngology Division of Pediatric Otolaryngology Otolaryngology Otolaryngology- Head & Neck Surgery Head & Neck Surgery University of California, San Francisco University of California, San Francisco February 13, 2010 February 13, 2010 Case Case 21 day old infant 21 day old infant presented to the ER presented to the ER – biphasic biphasic stridor stridor and and retractions retractions At birth At birth – telangiectasias telangiectasias of of upper chest, ears and upper chest, ears and mandibular mandibular areas areas
Transcript of Management of Pediatric Hemangiomas - UCSF CME · Management of Pediatric Hemangiomas Anna K....

1
Management of Pediatric Management of Pediatric HemangiomasHemangiomas
Anna K. Meyer, M.D., F.A.A.P.Anna K. Meyer, M.D., F.A.A.P.Assistant ProfessorAssistant Professor
Division of Pediatric OtolaryngologyDivision of Pediatric OtolaryngologyOtolaryngologyOtolaryngology--Head & Neck SurgeryHead & Neck SurgeryUniversity of California, San FranciscoUniversity of California, San Francisco
February 13, 2010February 13, 2010
CaseCase
21 day old infant 21 day old infant presented to the ERpresented to the ER–– biphasic biphasic stridorstridor and and
retractionsretractions
At birthAt birth–– telangiectasiastelangiectasias of of
upper chest, ears and upper chest, ears and mandibularmandibular areasareas

2
CaseCase
CutaneousCutaneous lesions lesions proliferated over first proliferated over first three weeks of lifethree weeks of life‘‘beardbeard’’ distributiondistributionlower liplower liptongue, tongue, gingivagingivaanterior chestanterior chest

3
CaseCase
Flexible Flexible fiberopticfiberoptic laryngoscopylaryngoscopy–– ErythemaErythema and edema of and edema of supraglottissupraglottis–– SubglottisSubglottis was difficult to visualizewas difficult to visualizePatient admittedPatient admittedDirect Direct laryngoscopylaryngoscopy and and bronchoscopybronchoscopyperformed on HD #2performed on HD #2

4
How would you manage?How would you manage?
a)a) TracheotomyTracheotomyb)b) Oral steroidsOral steroidsc)c) LaserLaserd)d) SubmucosalSubmucosal resectionresectione)e) PropanololPropanolol
You are considering using You are considering using propranololpropranolol::Which of the following is true?Which of the following is true?
a)a) There are no serious risks to using There are no serious risks to using propranololpropranolol and it and it should be firstshould be first--line treatment.line treatment.
b)b) A risk of A risk of propranololpropranolol is complete is complete heartblockheartblock and it and it should be used with caution.should be used with caution.
c)c) A risk of A risk of propranololpropranolol is hypoglycemia and infants is hypoglycemia and infants should be fed every 3 hours to prevent this problem.should be fed every 3 hours to prevent this problem.
d)d) Severe airway Severe airway hemangiomashemangiomas should almost always should almost always be managed with tracheotomy and be managed with tracheotomy and propranololpropranololshould not be considered.should not be considered.
5
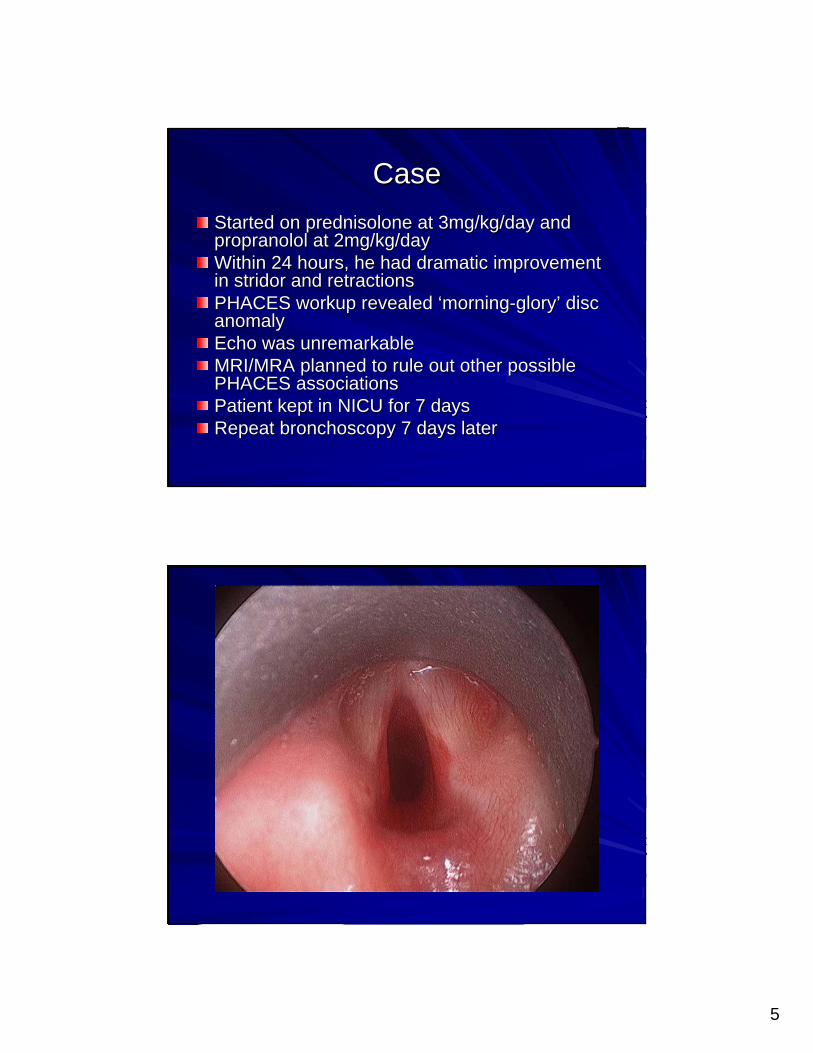
CaseCaseStarted on Started on prednisoloneprednisolone at 3mg/kg/day and at 3mg/kg/day and propranololpropranolol at 2mg/kg/dayat 2mg/kg/dayWithin 24 hours, he had dramatic improvement Within 24 hours, he had dramatic improvement in in stridorstridor and retractionsand retractionsPHACES workup revealed PHACES workup revealed ‘‘morningmorning--gloryglory’’ disc disc anomalyanomalyEcho was unremarkableEcho was unremarkableMRI/MRA planned to rule out other possible MRI/MRA planned to rule out other possible PHACES associationsPHACES associationsPatient kept in NICU for 7 daysPatient kept in NICU for 7 daysRepeat Repeat bronchoscopybronchoscopy 7 days later7 days later

6
CaseCase
Weaned off of Weaned off of prednisoloneprednisolone at 3 months.at 3 months.Currently 10 months old with no Currently 10 months old with no stridorstridor..

7
ObjectivesObjectives
Epidemiology of infant Epidemiology of infant hemangiomahemangiomaPresentation and evaluationPresentation and evaluationManagementManagement–– MedicalMedical–– SurgicalSurgical
EpidemiologyEpidemiology
Most common pediatric head and neck tumorMost common pediatric head and neck tumorIncidence Incidence (Bruckner & Frieden, 2003)(Bruckner & Frieden, 2003)
–– Neonatal: 1.1Neonatal: 1.1--2.6% 2.6% –– 12 months: 1012 months: 10--12% of white children12% of white children
SubglotticSubglottic hemangiomahemangioma rarerare–– 1.5% of congenital airway lesions 1.5% of congenital airway lesions (Holinger & Brown, 1967)(Holinger & Brown, 1967)
–– Beard distributionBeard distribution–– PHACES syndromePHACES syndrome

8
SubglotticSubglottic HemangiomaHemangiomaPresentationPresentation
Asymptomatic at birthAsymptomatic at birthProliferative phaseProliferative phase–– Begins 1 to 2 monthsBegins 1 to 2 months
InspiratoryInspiratory biphasic biphasic stridorstridorRespiratory distressRespiratory distressFeeding problemsFeeding problemsMisdiagnosis as croupMisdiagnosis as croupProliferation for one yearProliferation for one yearInvolution over 5+ yearsInvolution over 5+ years
PresentationPresentation
SubglotticSubglottichemangiomahemangioma–– 50% have 50% have cutaneouscutaneous
beard distributionbeard distribution
CutaneousCutaneous–– 99--63% have SGH 63% have SGH
Frieden, et al., 2005
9
PresentationPresentation
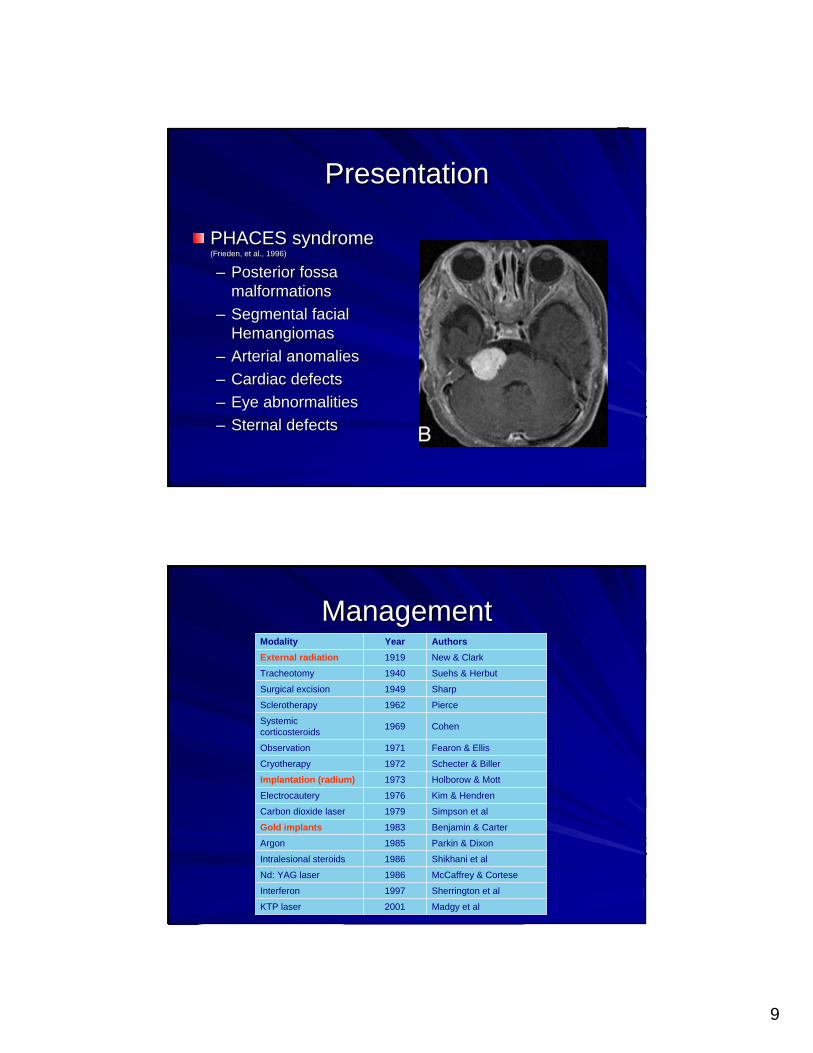
PHACES syndrome PHACES syndrome (Frieden, et al., 1996)(Frieden, et al., 1996)
–– Posterior Posterior fossafossamalformationsmalformations
–– Segmental facial Segmental facial HemangiomasHemangiomas
–– Arterial anomaliesArterial anomalies–– Cardiac defectsCardiac defects–– Eye abnormalitiesEye abnormalities–– SternalSternal defectsdefects
ManagementManagement
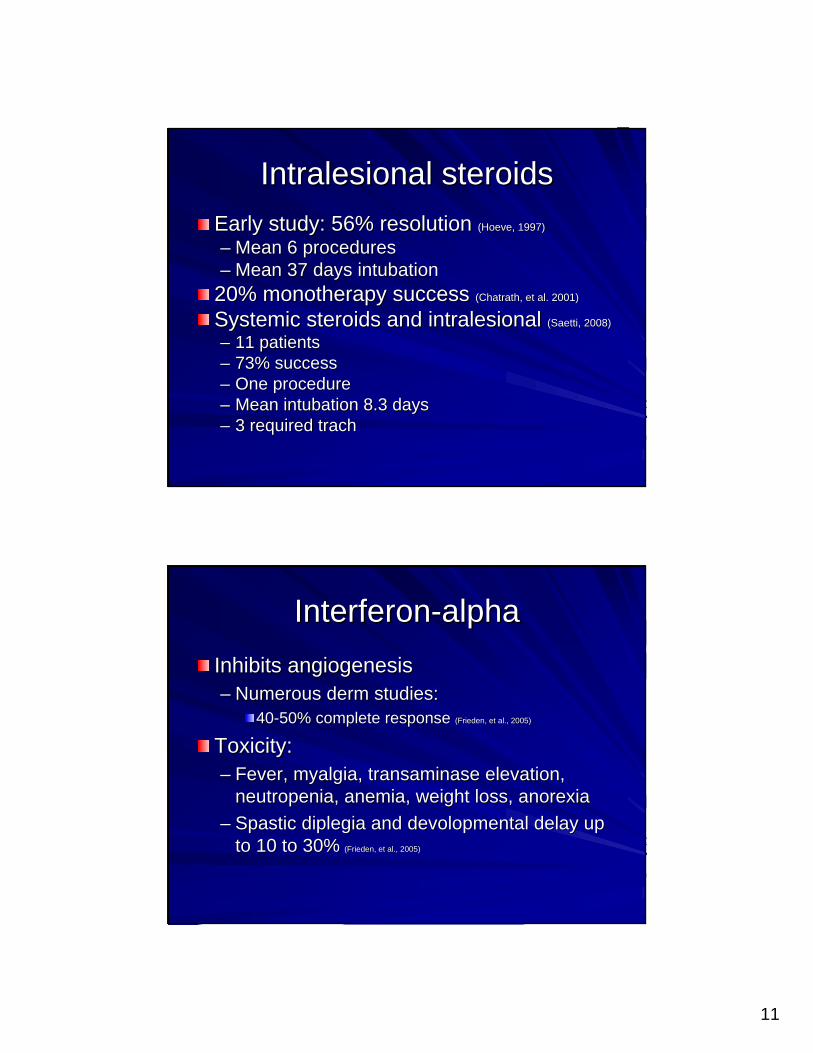
Madgy et al2001KTP laser
Sherrington et al1997Interferon
McCaffrey & Cortese1986Nd: YAG laser
Shikhani et al1986Intralesional steroids
Parkin & Dixon1985Argon
Benjamin & Carter1983Gold implantsSimpson et al1979Carbon dioxide laser
Kim & Hendren1976Electrocautery
Holborow & Mott1973Implantation (radium)Schecter & Biller1972Cryotherapy
Fearon & Ellis1971Observation
Cohen1969Systemic corticosteroids
Pierce1962Sclerotherapy
Sharp1949Surgical excision
Suehs & Herbut1940Tracheotomy
New & Clark1919External radiationAuthorsYearModality

10
ManagementManagementTracheotomyTracheotomy–– Historical standard of Historical standard of
carecare-- RahbarRahbar, et al., 2004:, et al., 2004:
-- 28% 28% trachedtrached-- 9% observed9% observed
-- no complicationsno complications-- complications 12complications 12--20% for 20% for
other treatmentsother treatments–– Significant morbidity for Significant morbidity for
a selfa self--limiting diseaselimiting diseaseComplications: 18Complications: 18--51%51%Mortality: 1Mortality: 1--2% 2% ((OzmenOzmen, et al., 2009; , et al., 2009; MahadevanMahadevan, et , et al., 2007)al., 2007)
Systemic SteroidsSystemic SteroidsFirst effect incidentally noted in treating First effect incidentally noted in treating thrombocytopenia thrombocytopenia Mainstay of more severe nonMainstay of more severe non--airway airway hemangiomashemangiomas–– Segmental, orbital, large or aggressiveSegmental, orbital, large or aggressive
Most often stop further growthMost often stop further growth–– Dermatology literature: response 30 to 60% Dermatology literature: response 30 to 60% –– ~20~20--25% symptomatic control of airway lesions25% symptomatic control of airway lesions–– Likelihood of readmission higher than other treatments Likelihood of readmission higher than other treatments
Complications:Complications:–– Behavior change, Behavior change, cushingoidcushingoid, growth delay, lipoid , growth delay, lipoid
pneumonia, peptic ulcer disease pneumonia, peptic ulcer disease ZaremZarem & Edgerton, 1967; Frieden, et al., 2005; & Edgerton, 1967; Frieden, et al., 2005; EnjolrasEnjolras, et al., 1990; Bennett, et al., 2001; , et al., 1990; Bennett, et al., 2001; RahbarRahbar, et al., , et al., 2004, 2004, SaettiSaetti, et al., 2008; , et al., 2008; ChathranChathran, et al., 2002; Perkins, et al., 2009, et al., 2002; Perkins, et al., 2009
11
IntralesionalIntralesional steroidssteroidsEarly study: 56% resolution Early study: 56% resolution ((HoeveHoeve, 1997), 1997)
–– Mean 6 proceduresMean 6 procedures–– Mean 37 days intubationMean 37 days intubation20% 20% monotherapymonotherapy success success ((ChatrathChatrath, et al. 2001), et al. 2001)
Systemic steroids and Systemic steroids and intralesionalintralesional ((SaettiSaetti, 2008) , 2008)
–– 11 patients11 patients–– 73% success73% success–– One procedureOne procedure–– Mean intubation 8.3 daysMean intubation 8.3 days–– 3 required 3 required trachtrach
InterferonInterferon--alphaalphaInhibits angiogenesisInhibits angiogenesis–– Numerous Numerous dermderm studies: studies:
4040--50% complete response 50% complete response (Frieden, et al., 2005)(Frieden, et al., 2005)
Toxicity: Toxicity: –– Fever, Fever, myalgiamyalgia, , transaminasetransaminase elevation, elevation,
neutropenianeutropenia, anemia, weight loss, anorexia, anemia, weight loss, anorexia–– Spastic Spastic diplegiadiplegia and and devolopmentaldevolopmental delay up delay up
to 10 to 30%to 10 to 30% (Frieden, et al., 2005)(Frieden, et al., 2005)

12
VincristineVincristine
Induces apoptosisInduces apoptosisLess toxicity than IFNLess toxicity than IFN--alphaalphaEfficacy close to 100% with weekly infusionEfficacy close to 100% with weekly infusionReplaced IFNReplaced IFN--alphaalphaComplications: peripheral neuropathy, GI upset, Complications: peripheral neuropathy, GI upset, jaw pain, constipation, fever, headache, jaw pain, constipation, fever, headache, hematologic toxicity, SIADH, PICC line hematologic toxicity, SIADH, PICC line complications complications (Frieden, et al., 2005; (Frieden, et al., 2005; EnjolrasEnjolras, et al., 2004), et al., 2004)
CO2 Laser ResectionCO2 Laser ResectionHighly popular modalityHighly popular modality–– Success 88.9 % Mean: 2 Success 88.9 % Mean: 2
procedures (range 1procedures (range 1--5)5)Complications:Complications:–– Web formationWeb formation–– PneumothoraxPneumothorax–– InterarytenoidInterarytenoid scarringscarring–– SubglotticSubglottic stenosisstenosis: 5.5: 5.5-- 25%25%
Not ideal for bilateral or Not ideal for bilateral or circumferentialcircumferentialMay require temporary May require temporary trachtrach
Saetti, et al., 2008Cotton & Tewfik, 1985; Cotton & Tewfik, 1985; BitarBitar, et al., 2005, et al., 2005
13
KTP Laser ResectionKTP Laser Resection
Laser resection: KTPLaser resection: KTP–– Preferential absorption by hemoglobinPreferential absorption by hemoglobin–– Potentially less destructivePotentially less destructive–– Deep penetrationDeep penetration–– Low complication rate in limited studies Low complication rate in limited studies ((PranskyPransky, et , et
al., 2004; al., 2004; KackerKacker, et al., 2001), et al., 2001)
Other lasers: Other lasers: Nd:YAGNd:YAG, pulse dye, pulse dye
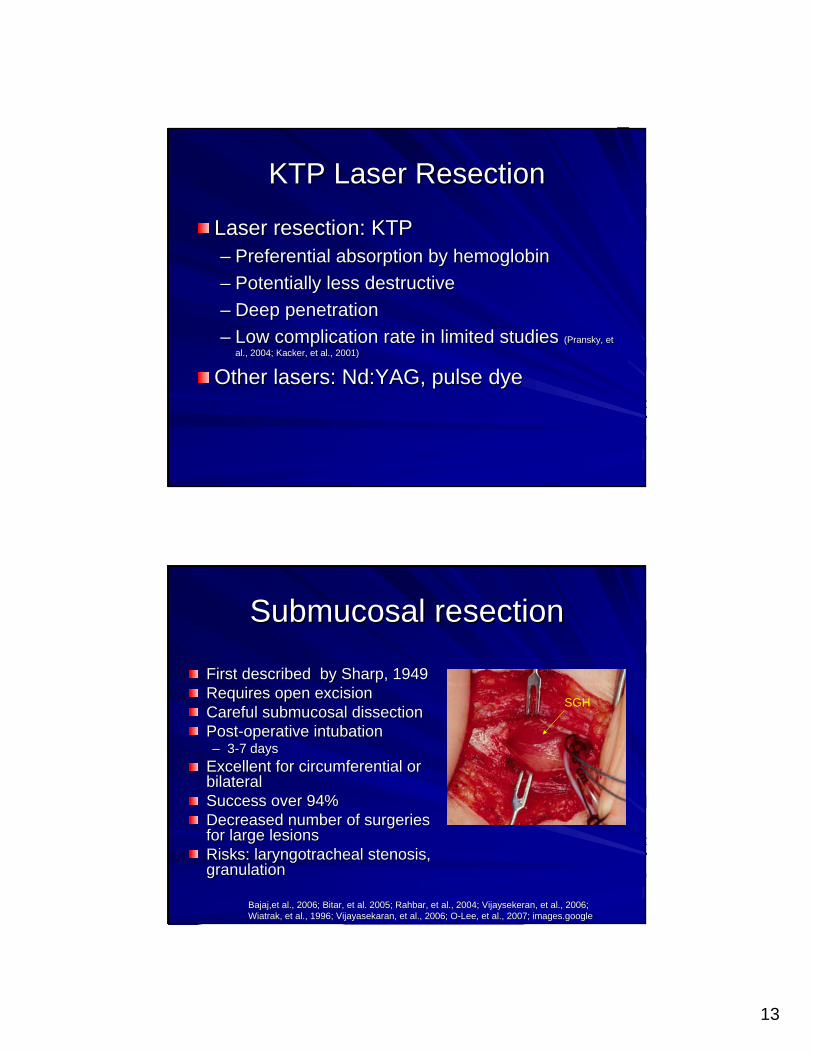
SubmucosalSubmucosal resectionresection
First described by Sharp, 1949First described by Sharp, 1949Requires open excisionRequires open excisionCareful Careful submucosalsubmucosal dissectiondissectionPostPost--operative intubationoperative intubation–– 33--7 days7 days
Excellent for circumferential or Excellent for circumferential or bilateralbilateralSuccess over 94% Success over 94% Decreased number of surgeries Decreased number of surgeries for large lesions for large lesions Risks: Risks: laryngotracheallaryngotracheal stenosisstenosis, , granulationgranulation
Bajaj,etBajaj,et al., 2006; al., 2006; BitarBitar, et al. 2005; , et al. 2005; RahbarRahbar, et al., 2004; , et al., 2004; VijaysekeranVijaysekeran, et al., 2006; , et al., 2006; WiatrakWiatrak, et al., 1996; , et al., 1996; VijayasekaranVijayasekaran, et al., 2006; O, et al., 2006; O--Lee, et al., 2007; Lee, et al., 2007; images.googleimages.google
SGH
14
PropranololPropranolol
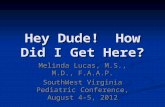
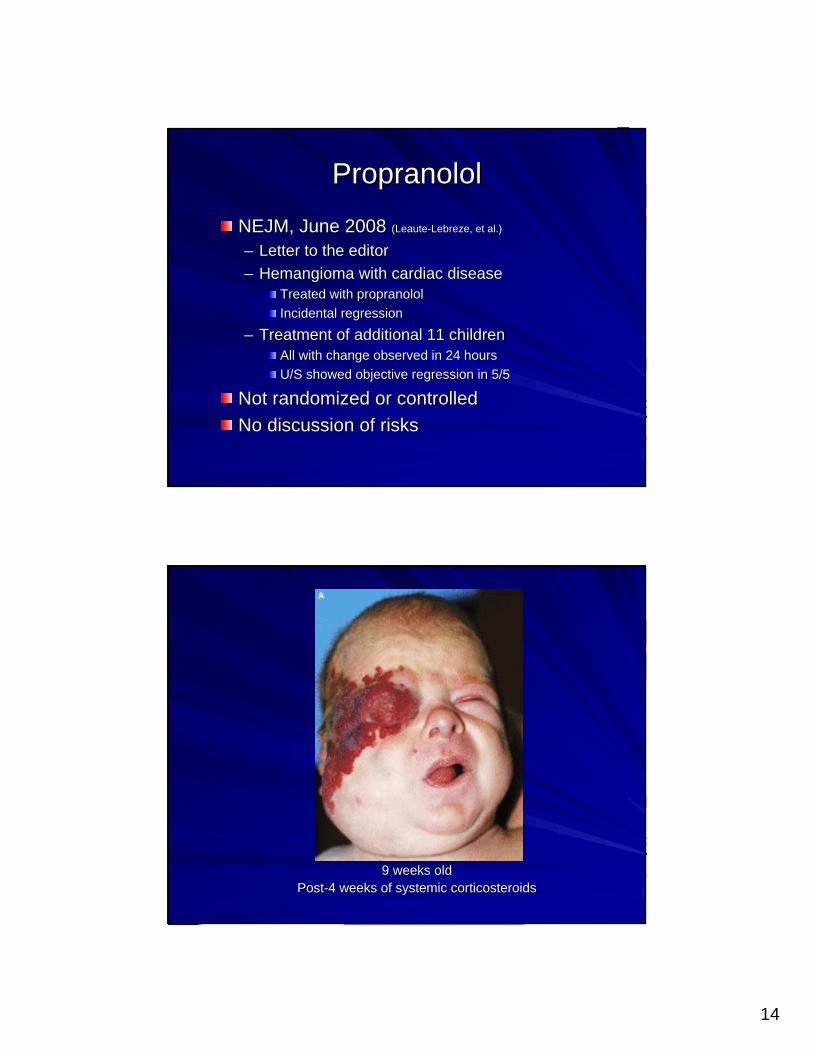
NEJM, June 2008 NEJM, June 2008 ((LeauteLeaute--LebrezeLebreze, et al.), et al.)
–– Letter to the editorLetter to the editor–– HemangiomaHemangioma with cardiac disease with cardiac disease
Treated with Treated with propranololpropranololIncidental regressionIncidental regression
–– Treatment of additional 11 childrenTreatment of additional 11 childrenAll with change observed in 24 hoursAll with change observed in 24 hoursU/S showed objective regression in 5/5U/S showed objective regression in 5/5
Not randomized or controlledNot randomized or controlledNo discussion of risksNo discussion of risks
9 weeks old9 weeks oldPostPost--4 weeks of systemic corticosteroids4 weeks of systemic corticosteroids
15
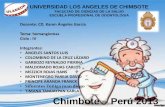
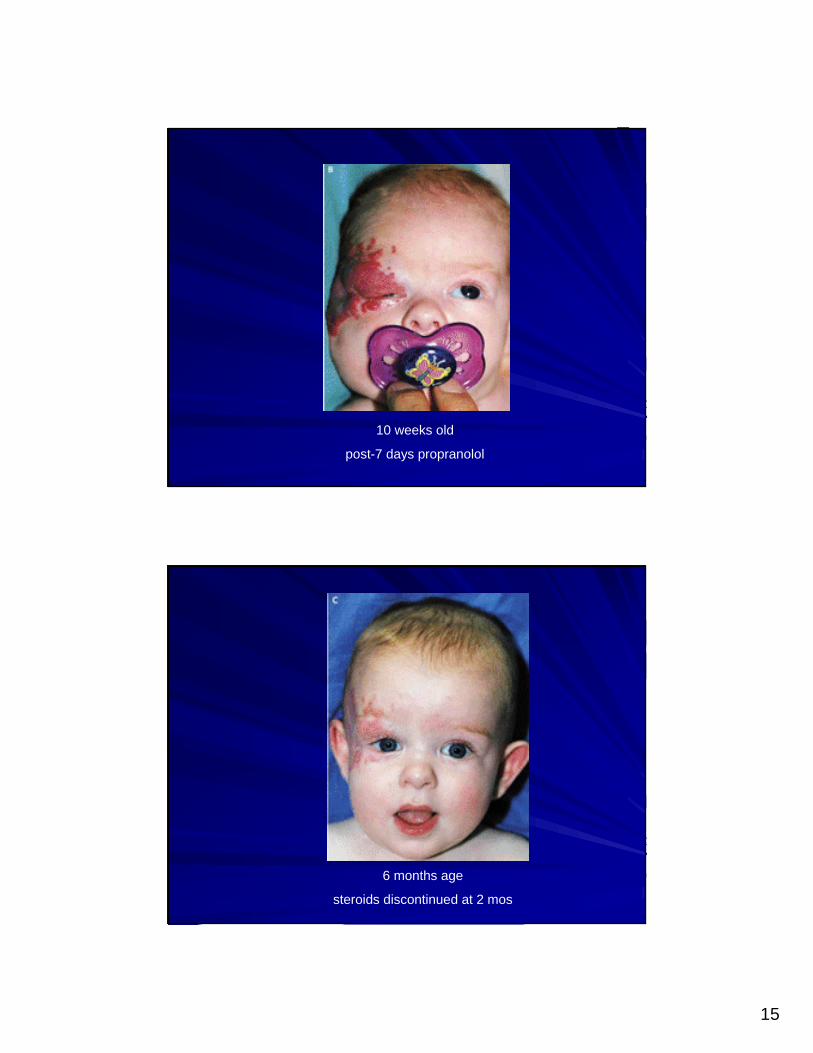
10 weeks old
post-7 days propranolol
6 months age
steroids discontinued at 2 mos

16
9 mos age
propranolol discontinued
MechanismsMechanisms
HemangiomaHemangioma proliferationproliferation–– Two Two proangiogenicproangiogenic factorsfactors
Basic fibroblast growth factor (Basic fibroblast growth factor (bFGFbFGF))Vascular endothelial growth factor (VEGF)Vascular endothelial growth factor (VEGF)
Possible mechanisms Possible mechanisms –– VasoconstrictionVasoconstriction–– Decreased VEGF and Decreased VEGF and bFGFbFGF expressionexpression–– Triggered apoptosis of capillary endothelial cells Triggered apoptosis of capillary endothelial cells –– MesenchymalMesenchymal stem cell differentiation inhibitionstem cell differentiation inhibition
LeauteLeaute--LabrezeLabreze, et al., 2008; , et al., 2008; DD’’AngeloAngelo, et al. 1997; , et al. 1997; SommersSommers, et al., 2002, et al., 2002

17
PropranololPropranolol
TheletsaneTheletsane, et al., 2009, et al., 2009–– Single case: airway, good responseSingle case: airway, good response–– No risks discussedNo risks discussed
DenoyelleDenoyelle, et al., 2009, et al., 2009–– 2 patients with airway lesions2 patients with airway lesions–– Treated concomitant with Treated concomitant with vincristinevincristine and/or steroidsand/or steroids–– Spectacular regressionSpectacular regression–– Developed safety protocolDeveloped safety protocol–– Advocate as first line treatment for SGH Advocate as first line treatment for SGH
PropranololPropranololSans, et al., 2009: Sans, et al., 2009: –– Only published larger study: ObservationalOnly published larger study: Observational–– Complicated Complicated hemangiomahemangioma–– 32 children, mean age 4.2 32 children, mean age 4.2 mosmos; 13 with previous steroids; 13 with previous steroids–– Dose 2Dose 2--3 mg/kg/day divided in 2 or 3 doses3 mg/kg/day divided in 2 or 3 doses–– Monitored 6 hours: EKG, echo, BP, HRMonitored 6 hours: EKG, echo, BP, HR–– Results: Results:
immediate effect color and growth in allimmediate effect color and growth in allClinical and US regression at 2 Clinical and US regression at 2 mosmosSteroids stopped in few weeksSteroids stopped in few weeksMean duration treatment 6.1 Mean duration treatment 6.1 mosmosRelapses mild and responded to reRelapses mild and responded to re--initationinitation
–– Limited side effects: one discontinuation for wheezeLimited side effects: one discontinuation for wheeze

18
PropranololPropranolol
Since initial article in June 2008Since initial article in June 2008–– 24 articles in the literature24 articles in the literature–– 2 accepted publications from our group2 accepted publications from our group–– 46 patients total46 patients total–– 13 13 subglotticsubglottic casescases–– 100% response100% response–– FirstFirst--line therapy?line therapy?
RisksRisks
FollowFollow--up letter to NEJM up letter to NEJM (Siegfried, et al., 2008)(Siegfried, et al., 2008)
–– BradycardiaBradycardia–– HypotensionHypotension–– BronchospasmBronchospasm–– Blunted hypoglycemia signsBlunted hypoglycemia signs
Risk of longRisk of long--term neurologic term neurologic sequelaesequelae
–– Masked highMasked high--output heart failureoutput heart failure–– Easy to monitor inpatient, most patients are Easy to monitor inpatient, most patients are
outpatientoutpatient

19
LimitationsLimitationsNo No RCTsRCTs of efficacy and toxicityof efficacy and toxicityMany variables: Many variables: –– Location, size, reason for intervention, prior or concomitant Location, size, reason for intervention, prior or concomitant txtx, ,
age at initiationage at initiation–– No standardized criteria for measuring response or monitoring No standardized criteria for measuring response or monitoring
toxicity toxicity Evaluation/MonitoringEvaluation/Monitoring–– EKG, echo, admission, home nursing, CBC, BP, HR, EKG, echo, admission, home nursing, CBC, BP, HR, lyteslytes, ,
LFTsLFTs, glucose, , glucose, TFTsTFTs, urine glucose, abdominal US, urine glucose, abdominal USStarting dosage, max dosageStarting dosage, max dosageLength of treatmentLength of treatmentCombined vs. isolated treatmentCombined vs. isolated treatment
Proposed Protocol Proposed Protocol (Siegfried, et al., 2008)(Siegfried, et al., 2008)
Baseline echocardiographyBaseline echocardiography4848--hour hospitalization or home nursing hour hospitalization or home nursing visitsvisitsMonitor vital signs, blood glucoseMonitor vital signs, blood glucoseq8h deliveryq8h deliveryInitial dose 0.16mg/kg to max 2 mg/kg/dayInitial dose 0.16mg/kg to max 2 mg/kg/dayGradual taper over 2 weeksGradual taper over 2 weeks

20
UCSF ProtocolUCSF ProtocolDeveloped with dermatology, cardiology, OHNSDeveloped with dermatology, cardiology, OHNSSymptomatic airway disease or less than 3 months oldSymptomatic airway disease or less than 3 months old–– inpatient observationinpatient observation–– Initial dose: 1 mg/kg/day as initial dose and increase to 2 Initial dose: 1 mg/kg/day as initial dose and increase to 2
mg/kg/day a few days latermg/kg/day a few days later–– q8h dosing q8h dosing
Older than 3 months of age, no airway diseaseOlder than 3 months of age, no airway disease–– Heart rate monitored at home or by PCP every few days Heart rate monitored at home or by PCP every few days –– Slowly increasing doses: start 0.3 mg/kg/day increases every 3 Slowly increasing doses: start 0.3 mg/kg/day increases every 3
days at 0.3 mg/kg increments to a target dose of 2 mg/kg/day. days at 0.3 mg/kg increments to a target dose of 2 mg/kg/day. Patients less than 6 months of age must be fed every 3 Patients less than 6 months of age must be fed every 3 to 4 hours to avoid drugto 4 hours to avoid drug--induced hypoglycemiainduced hypoglycemia
UCSF experienceUCSF experience
Treated 18 patients to date. Treated 18 patients to date. One unexplained One unexplained bradycardiabradycardia and and hypoglycemia requiring brief hypoglycemia requiring brief hospitalization with rapid recovery.hospitalization with rapid recovery.Dose reduction for mild decrease in BP.Dose reduction for mild decrease in BP.Dose reduction for excessive sleepiness.Dose reduction for excessive sleepiness.A few parents have reported sleep A few parents have reported sleep disturbances.disturbances.

21
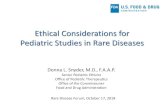
CaseCase
At admission 6 days post-propranolol
RecommendationsRecommendationsTreat in collaboration with Treat in collaboration with dermderm and cardsand cardsRefer to centers participating in randomized trialsRefer to centers participating in randomized trialsCurrent Current trials:clinicaltrial.govtrials:clinicaltrial.gov–– NCT00744185; NCT01056341, University Hospital, BordeauxNCT00744185; NCT01056341, University Hospital, Bordeaux
DBDB--RCT: RCT: PropranololPropranolol and and hemangiomashemangiomas–– NCT01010308 , Toronto Hospital for Sick ChildrenNCT01010308 , Toronto Hospital for Sick Children
NonNon--randomized, historical control: randomized, historical control: nadololnadolol and H&N and H&N hemangiomashemangiomas–– NCT00967226, Children National Medical CenterNCT00967226, Children National Medical Center
Randomized, Randomized, propranololpropranolol vsvs prednisoloneprednisolone
SubglotticSubglottic hemangiomahemangioma so rare: multiso rare: multi--institutional institutional RCTsRCTsneeded to fully evaluateneeded to fully evaluate

22
You are considering using You are considering using propranololpropranolol::Which of the following is true?Which of the following is true?
a)a) There are no serious risks to using There are no serious risks to using propranololpropranolol and it and it should be firstshould be first--line treatment.line treatment.
b)b) A risk of A risk of propranololpropranolol is complete is complete heartblockheartblock and it and it should be used with caution.should be used with caution.
c)c) A risk of A risk of propranololpropranolol is hypoglycemia and infants is hypoglycemia and infants should be fed every 3 hours to prevent this problem.should be fed every 3 hours to prevent this problem.
d)d) Severe airway Severe airway hemangiomashemangiomas should almost always should almost always be managed with tracheotomy and be managed with tracheotomy and propranololpropranololshould not be considered.should not be considered.
Thank you!Thank you!

23
articlesarticlesBuckmillerBuckmiller, et al., 2009, et al., 2009
–– One patientOne patient–– Tracheal lesions, persistent Tracheal lesions, persistent stridorstridor near 2 near 2 y/oy/o–– Late Late txtx with with propranololpropranolol–– Developed protocol with cardiologyDeveloped protocol with cardiology
MaturoMaturo & & HartnickHartnick, 2010, 2010–– 2 patients treated with 2 patients treated with propranololpropranolol onlyonly–– Initial dose of 0.5Initial dose of 0.5––11 mg/kg is started and if well tolerated increased to a dose of mg/kg is started and if well tolerated increased to a dose of
22––33 mg/kg divided bid to mg/kg divided bid to tidtid over 24over 24––4848 h h JephsonJephson, et al., 2009: one case airway, no SE, says 30 , et al., 2009: one case airway, no SE, says 30 cutaneouscutaneous treated treated but no data presentedbut no data presentedTruong, et al., 2009: Truong, et al., 2009: propranololpropranolol and steroids single case reportand steroids single case reportMarscianiMarsciani, et al., 2010: one case hepatic, et al., 2010: one case hepaticTabanTaban, et al., 2010: orbital , et al., 2010: orbital MousaMousa, et al. 2009: one case thorax, et al. 2009: one case thorax
–– Hypotension and Hypotension and hyperkalemiahyperkalemia
DenoyelleDenoyelle protocolprotocol
Baseline cardiac Baseline cardiac u/su/sBP, HRBP, HRMonitoring of blood glucose first 48hMonitoring of blood glucose first 48h0.16 mg/kg/8h to max 2mg/kg/day0.16 mg/kg/8h to max 2mg/kg/day