Management of Pain in Cancer Patients and Chemotherapy

of 21
-
Upload
sj-eclipse -
Category
Documents
-
view
227 -
download
0
Transcript of Management of Pain in Cancer Patients and Chemotherapy
-
8/7/2019 Management of Pain in Cancer Patients and Chemotherapy
1/20
1 | P a g e
Management of Pain in Cancer Patients
Causes of Cancer Pains
Bone Destruction
Obstructionofanorgan
Compressionofa peripheral nerve
Infiltration anddistensionoftissue
Inflammation andnecrosis
Psychological factors such as fear and anxiety
Treatment Modalities
Analgesic Therapies for Cancer Pains
Therapy ExamplesPrimary Therapy Chemotherapy
Radiotherapy Hormone therapy Immunotherapy Surgery Antibiotics
Systemic
Analgesic
Pharmacotherapy
Non-opioid analgesics Opioids Adjuvant analgesics
AnestheticTechniques
Intraspinal opioids/local anesthetic Chemical rhizotomy (interruption of a nerve root by the use of glycerol) Somatic neurolysis (destruction or dissolution of nerve tissue) Sympathetic blockade (blocking of the effect of a hormone or neurotransmitter
at a cell-surface receptor by a pharmacologic antagonist)
Neurosurgical
Techniques
Rhizotomy (Surgical resection/interruption of nerve root) Cordotomy (cutting of spinal cord fibers) Cingulotomy (producing lesions in the tissue of the cingulate gyrus of the
frontal lobe)
Pituitary ablation(removal of or a part of pituitary gland)Physiatric
Techniques
Orthoses (orthopedic appliances or apparatus used to support, align, prevent,or correct deformities or to improve function of movable parts of the body.)
Physical therapyPsychological
Techniques
Relaxation training Distraction techniques
Neurostimulatory
Techniques
Transcutaneous electrical nerve stimulation (electronic stimulation to blocktransmission of pain information to the brain.)
Acupuncture (inserting thin needles into the body at specific points to relievepain)
-
8/7/2019 Management of Pain in Cancer Patients and Chemotherapy
2/20
-
8/7/2019 Management of Pain in Cancer Patients and Chemotherapy
3/20
3 | P a g e
General Nursing Management for Cancer Pain
1. Asses the severity ofpain;pain is what the client describes or says that it is2. Collaborate withother members ofthe health care team todevelop a painmanagement
program.
3. Administer oral preparation ifpossible and ifthey provide adequate reliefofpain; thetransdermal route may also be prescribed.
4. Mild tomoderate painmay be treatedwith salicylates, acetaminophen andNSAIDS.5. Severe pain is treatedwithopioids such as codeine sulfate, morphine sulfate, methadone,
hydromorphone hydrochloride. Neuropathic pain is treatedwith a variety ofanticonvulsant and
anti-depressants, as well as opioids.
6. Subcutaneous injections and continuous IV administrationofopioids provide rapid control .7. Monitor vital signs andfor side effects ofmedications.8. Monitor for effectiveness ofmedications9. Provide non-pharmacological techniques to relieve pain, such as relaxation, guided imagery,
biofeedback, massage andheat and cold application10.Donot under medicate a cancer patient who is inpain.
-
8/7/2019 Management of Pain in Cancer Patients and Chemotherapy
4/20
4 | P a g e
Chemotherapy
Chemotherapy, in its most general sense, refers to treatmentofdisease by chemicals that kill cells, specifically those ofmicro-organisms or cancer. Inpopular usage, it will usually refer to
antineoplastic drugs used to treat cancer or the combinationofthesedrugs into a standardized treatment regimen.
In its non-oncological use, the termmay also refer toantibiotics (antibacterial chemotherapy). In that sense, the firstmodern chemotherapeutic agent was Paul Ehrlich's arsphenamine,an arsenic compounddiscovered in 1909 and used to treat syphilis.This was later followed by sulfonamides discovered by Domagk and
penicillindiscovered by Alexander Fleming.
Other uses ofcytostatic chemotherapy agents (including the
ones mentioned below) are the treatment ofautoimmune diseasessuch as multiple sclerosis and rheumatoid arthritis and the suppressionoftransplant rejections
Objectives:
y Todestroy all malignant tumor cells without excessive destructionofnormal cellsy To control tumor growth ifcure is no longer possibley Used as adjuvant therapy
Contraindications:
y Infection. The anti-tumor drugs are immunosuppresivesy Recent surgery. The drugs may retardhealing processy Impaired renal / hepatic function. The drugs are nephrotoxic & hepatotoxicy RecentRadiation Therapy. Also immunisuppresivey Pregnancy. The drugs may cause congenital defectsy Bone Marrow Depression. The drugs may aggravate the condition. The WBC level must be
withinnormal limits.
AntiNeoplastic Medications
y Kills or inhibit the reproductionofneoplastic cellsy Normal cells are also affectedy Cell cycle phase specific medications
o Affects cells only during a certainphase ofthe reproductivecycle
y Cell cycle phase non-specific medicationso Affects cells in any phase ofthe reproductive cycle
y Can use combinationmedications or withother treatment modalities
-
8/7/2019 Management of Pain in Cancer Patients and Chemotherapy
5/20
5 | P a g e
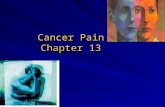
Routes of Administration
1. Oral -capsule, tablet, or liquid2. I.V. push (bolus) or infusionover a specified time
period
3. Intramuscular4. Intrathecal/ intraventricular given by injection via
an Ommaya reservoir or by lumbar puncture
(Figures 1 and2)
5. Intra-arterial (Figure 3)6. Intracavitary such as peritoneal cavity (Fig. 5)7. Intravesical into uterus or bladder (Fig. 4)8. Topical Figure 1 Intraventricular Administration via
Ommaya Reservoir
Figure 3 Intrathecal and Intraventricula route
Figure 2 Intraarterial route
Figure 4 Intravesical into Bladder
-
8/7/2019 Management of Pain in Cancer Patients and Chemotherapy
6/20
6 | P a g e
Dosage is basedon surface area(mg/m2) in both adults and children.
Most chemotherapeutic agents havedose-limiting toxicities that require nursing
interventions Chemotherapy predictably
affects normal, rapidly growing cells (eg, bone
marrow; GI tract lining, hair follicles). It is
imperative that these toxicities be recognized
early on by the nurse.
Figure 5 Intracavitary (Peritoneal Cavity)
-
8/7/2019 Management of Pain in Cancer Patients and Chemotherapy
7/20
7 | P a g e
Nursing Process: Side Effects of Chemotherapy
Adverse effects ofchemotherapy are gradedon a scale of0 to 4, with 0 being normal and 4
indicating life-threatening. Scoring ofadverse effects will determine ifa delay in therapy is necessary,
dose modification is necessary, or cessationoftherapy must occur.
A. Alopecia1. Most chemotherapeutic agents cause some degree ofalopecia. This is dependent on the
drug dose, half-life ofdrug, anddurationoftherapy.
2. Usually begins 2weeks after administrationofchemotherapy. Regrowth takes about 3 to 5months.
3. The use ofscalphypothermia and tourniquets is highly controversial.B. Anorexia
1. Chemotherapy changes the reproductionoftaste buds.2. Absent or altered taste can lead to a decreasedfood intake.3. Concurrent renal or hepatic disease can increase anorexia.
C. Fatigue1. The cause offatigue is generally unknown but can be related to anemia, weight loss,
altered sleeppatterns, and coping.
D.Nausea and Vomiting1. Caused by the stimulationofthe vagus nerve by serotonin released by cells in the upper GI
tract.
2. Incidence depends upon the particular chemotherapeutic agent anddosage.3. Patterns ofnausea and vomiting:
a. Anticipatory conditioned response from repeated association between therapy andvomiting.
b. Acute occurs 0 to24 hours after chemotherapy administration.c. Delayed canoccur 1 to 4 days after chemotherapy administration.
E. Mucositis1. Caused by the destructionofthe oral mucosa, causing an inflammatory response.2. Initially presents as a burning sensationwithno changes in the mucosa andprogresses to
significant breakdown, erythema, andpainofthe oral mucosa.
3. Consistent oral hygiene is important to avoid infection.
-
8/7/2019 Management of Pain in Cancer Patients and Chemotherapy
8/20
8 | P a g e
F. Anemia1. Caused by suppressionofthe stem cell or interference with cell proliferationpathways.2. May require red blood cell transfusionor injectionoferythropoietinor darbepoetin.
G.Neutropenia
1. Defined as an absolute neutrophil count (ANC) of1,500/mm3or less.2. Risk ofinfection is greatest with anANC less than 500/mm3.3. Caused by suppressionofthe stem cell.4. Usually occurs 7 to 14 days after administrationofchemotherapy.5. Can be prolonged.6. Patients should be taught to avoid infection throughproper handwashing, avoiding those
with illness, proper hygiene.
7. Patients need to be monitored and treatedpromptly for fever or other signs ofinfection.H. Thrombocytopenia
1. Caused by suppressionofmegakaryocytes.2. Incidence depends on the agent being used.3. Risk ofbleeding is present whenplatelet count falls below 50,000/mm3.4. Risk is highwhen count falls below20,000/mm3.5. Risk is critical when count falls below 10,000/mm3.6. Patient should be taught to avoid injury, eg, no razors, avoid vaginal douches and rectal
suppositories, and avoiddental floss during the periodofthrombocytopenia.
7. May require platelet transfusions ifcount drops below20,000/mm3.I. Hypersensitivity Reactions
1. Nearly all ofthe available chemotherapeutic agents canproduce hypersensitivity reactions(HSRs) in at least anoccasional patient, and some cause reactions in 5% or more ofpatients
receiving the drug. There are several agents (L-asparaginase, paclitaxel, docetaxel,
teniposide, anddoxil) for whichHSRs are frequent enough to be a major formoftreatment-
limiting toxicity.
2. The mechanism is unknownfor most ofthe chemotherapeutic agents in use.3. Signs and symptoms include hives, pruritus, back pain, shortness ofbreath, hypotension,and anaphylaxis.4. All unexpecteddrug reactions should be reported to the manufacturer.
-
8/7/2019 Management of Pain in Cancer Patients and Chemotherapy
9/20
9 | P a g e
Nursing AssessmentA. Integumentary System
1. Inspect for pain, swelling with inflammationor phlebitis, necrosis, or ulceration.2. Inspect for skin rash, characteristics,whether pruritus, general or local.3. Assess areas oferythema and associated tenderness or pruritus. Instruct patient to avoid
irritation to skin, sun exposure, or irritating soaps.
4. Assess changes in skinpigmentation.5. Note reports ofphotosensitivity, tearing ofthe eyes.6. Assess conditionofgums, teeth, buccal mucosa, and tongue.
a. Determine whether any taste changes have occurred.b. Check for evidence ofstomatitis, erythematous areas, ulceration, infection, or painon
swallowing.
c. Determine whether the patient has any complaints ofpainor burning ofthe oralmucosa or on swallowing.
B. GI System1. Assess for frequency, timing ofonset, duration, and severity ofnausea and vomiting
episodes before and after chemotherapy.
a. Usually occurs from 1 to24 hours after chemotherapy but may be delayed.Anticipatory vomiting may occur after first course oftherapy. Can be initiated by
various cues, including thoughts, smell, or even sight ofthe medical personnel.
2. Observe for alterations inhydration, electrolyte balance.3. Assess for diarrhea or constipation.
a. Ascertain any changes in bowel patterns.b. Discuss the consistency ofstools.c. Consider the frequency anddurationofdiarrhea (the number ofstools eachday for
the number ofdays).
d. Evaluate dietary changes or use ofmedications such as opioids or 5-HT3 blockers thathave had an impact ondiarrhea or constipation.
4. Assess for anorexia.a. Discuss taste changes and changes infoodpreferences.b. Ask about daily food intake andnormal eating patterns.
5. Assess forjaundice, right upper quadrant abdominal pain, changes in the stool or urine, andelevated liver function tests that indicate hepatotoxicity.
6. Monitor liver function tests and total bilirubin.
-
8/7/2019 Management of Pain in Cancer Patients and Chemotherapy
10/20
10 | P a g e
C. Hematopoietic System1. Assess for neutropenia ANC less than 500/mm3.
a. Assess for any signs ofinfection (pulmonary, integumentary, central nervous system,GI, and urinary).
b. Auscultate lungs for adventitious breath sounds.c. Assess for productive coughor shortness ofbreath.d. Assess for urinary frequency, urgency, pain, or odor.e. Monitor for elevationoftemperature above 101 F, chills.
2. Assess for thrombocytopenia platelet count less than 50,000/mm3 (mild risk ofbleeding);less than20,000/mm3 (high risk ofbleeding).
a. Assess skin andoral mucous membranes for petechiae, bruises on extremities.b. Assess for signs ofbleeding (including nose, urinary, rectal, or hemoptysis).c. Assess for blood in stools, urine, or emesis.d.
Assess for signs and symptoms ofintracranial bleeding ifplatelet count is less than20,000/mm3; monitor for changes in level ofresponsiveness, vital signs, andpupillary
reaction.
3. Assess for anemia.a. Assess skin color, turgor, and capillary refill.b. Ascertainwhether patient has experienceddyspnea on exertion, fatigue, weakness,
palpitations, or vertigo. Advise rest periods as needed.
D.Respiratory and Cardiovascular Systems1. Assess lung sounds.2. Assess for pulmonary fibrosis, evidenced by a dry, nonproductive coughwith increasing
dyspnea. Patients at risk include those over age 60, smokers, those receiving or having had
pulmonary radiation, those receiving cumulative dose ofbleomycin (Blenoxane), or those
with any preexisting lung disease.
3. Assess for signs and symptoms ofheart failure or irregular apical or radial pulses.4. Verify baseline cardiac studies (eg, electrocardiogram, multiple-gated acquisition
scan/ejectionfraction) before administering doxorubicin (Adriamycin) or high-dose
cyclophosphamide (Cytoxan).
E. Neuromuscular System1. Determine whether patient is having difficulty withfine motor activities, such as zipping
pants, tying shoes, or buttoning a shirt.
2. Determine the presence ofparesthesia (tingling, numbness) offingers or toes.3. Evaluate deep tendon reflexes.4. Evaluate patient for weakness, ataxia, or slapping gait.
-
8/7/2019 Management of Pain in Cancer Patients and Chemotherapy
11/20
11 | P a g e
5. Determine impact on activities ofdaily living anddiscuss changes.6. Discuss symptoms ofurinary retentionor constipation.7. Assess for ringing in ears or decreasedhearing acuity.
F.
Genitourinary System1. Monitor urine output.2. Assess for urinary frequency, urgency, or hesitancy.3. Evaluate changes inodor, color, or clarity ofurine sample.4. Assess for hematuria, oliguria, or anuria.5. Monitor BUN and creatinine.
Nursing DiagnosesA. Risk for Infection related toneutropeniaB. Risk for Injury related to bleeding from thrombocytopeniaC. Fatigue related to anemiaD. ImbalancedNutrition: Less ThanBody Requirements related to adverse effects oftherapyE. Ineffective protection and risk for hypersensitivity reaction related to chemotherapyF. Impaired Oral Mucous Membranes related to stomatitisG. DisturbedBody Image related to alopecia andweight loss
Nursing InterventionsA. Preventing Infection
1. Monitor vital signs every 4 hours; report occurrence offever greater than 101 F (38.3 C) andchills.
2. Provide patient education.a. Instruct patient to report signs and symptoms ofinfection:
i. Fever greater than 101 F and/or chillsii. Mouth lesions, swelling, or redness
iii. Redness, pain, or tenderness at rectumiv.
Change in bowel habits
v. Areas ofredness, swelling, induration, or painon skin surfacevi. Painor burning when urinating or odor from urine
vii. Coughor shortness ofbreathb. Reinforce goodpersonal hygiene habits (routine bathing [preferably a shower], clean
hair, nails, andmouth care).
c. Avoid contact withpeople whohave a transmissible illness.
-
8/7/2019 Management of Pain in Cancer Patients and Chemotherapy
12/20
12 | P a g e
d. Encourage deep breathing and coughing todecrease pulmonary stasis.3. Avoidperforming invasive procedures rectal temperatures, enemas, or insertionofindwelling
urinary catheters.
4. Monitor white blood cell count (WBC) anddifferential.5. Be aware that hematologic nadirs (lowest level) generally occur within 7 to 14 days after drug
administration. Lengthofmyelosuppressiondepends on specific drug. Institutionoffurther
therapy usually depends on an adequateWBC andANC.
6. Calculate ANC todetermine the number ofneutrophils capable offighting an infection by:7. Interpretation: 105 ofthe 700 WBCs are neutrophils and capable offighting an infection
(indicates severe neutropenia).
8. Administer prophylactic antibiotics as prescribed (ifWBC is less than 500).9. Administer growthfactors as prescribed. Neupogen 5 mcg/kg S.C. starting 24 hours after
chemotherapy for 10 days for neutropenia prophylaxis or Neulasta 6mg S.C. for one dose 24
hours after chemotherapy. Should also be administeredwith subsequent courses of
chemotherapy tohastenneutrophil maturity.
B. Preventing Bleeding1. Avoid invasive procedures whenplatelet count is less than 50,000/mm3, including I.M.
injections, suppositories, enemas, and insertionofindwelling urinary catheters.
2. Apply pressure on injection sites for 5 minutes.3. Monitor platelet count; administer platelets as prescribed.4. Monitor and test all urine, stools, and emesis for blood.5. Provide patient education.6. Instruct patient to avoid straight-edge razors, nail clippers, vaginal or rectal suppositories.7. Avoid intercourse whenplatelet count is less than 50,000/mm3.8. Encourage patient to blownose gently.9. Avoiddental work or other invasive procedures while thrombocytopenic.10.Avoid the use ofNSAIDs, aspirin, and aspirin-containing products.
C. Minimizing Fatigue1. Monitor blood counts (hemoglobin andhematocrit).2. Administer bloodproducts as prescribed.3. Administer growthfactors as prescribed. Erythropoetin 150 U/kg S.C. 3 per week.4. Provide patient education and counseling
a. Information about fatigueb. Reassurance that treatment-relatedfatigue does not mean your cancer is worsec. Why fatigue and shortness ofbreathmay occurd. Suggestions for ways to cope withfatigue
-
8/7/2019 Management of Pain in Cancer Patients and Chemotherapy
13/20
13 | P a g e
i. Energy conservationii. Caution the patient about physical overexertion; encourage rest frequently and
warnpatient to expect a tiredfeeling
iii. Planfrequent rest periods betweendaily activities; take naps that donotinterrupt nighttime sleep
iv. Set priorities anddelegate tasks tootherse. Stress managementf. Explain that blood transfusions, ifgiven, are a part oftherapy andnot necessarily an
indicationofa setback
g. Observe skin colorh. Monitor nutritional status
D. Promoting Nutrition1. Administer antiemetics before chemotherapy andon a routine schedule (not as needed).2. Be aware that certain antiemetic combinations are more effective than single agents.
a. A 5-HT3 inhibitor, such as ondansetron (Zofran), granisetron (Kytril), dolasetron(Anzemet), in combinationwithdexamethasone (Decadron)
b. Corticosteroids in combinationwithmetoclopramide (Reglan)3. For highly emetogenic chemotherapy regimens:
a. Premedicate with a 5-HT3 inhibitor anddexamethasone.b. Include an as-needed antiemetic such as metoclopramide, prochlorperazine
(Compazine), dexamethasone, or lorazepam (Ativan).
4. For moderately emetogenic regimens:a. Premedicate with either prochlorperazine or dexamethasone withmetoclopramide plus
diphenhydramine (Benadryl).
b. Include an as-needed antiemetic, such as prochlorperazine or lorazepam.c. Failures may receive a 5-HT3 inhibitor.
5. For low emetogenic regimens consider oral prochlorperazine.6. Extrapyramidal reactions occur frequently inpatients under age 30 andover age 65. Treat
dystonic reactions withdiphenhydramine; treat restlessness with lorazepam.
7. Ifdelayednausea and vomiting begin 8 hours after acute prophylactic antiemetic therapy andcontinue for 24 to 36hours, administer agents such as metoclopramide withdexamethasone
plus diphenhydramine, prochlorperazine, or lorazepam.8. Consider alternative measures for reliefofanticipatory nausea, such as relaxation therapy,
imagery, anddistraction.
9. Encourage small, frequent meals appealing topatient preferences.10. Encourage patient to eat a diet high in calories andproteins. Provide a high-protein supplement
as needed.
11. Discourage smoking and alcoholic beverages, whichmay irritate mucous membranes.
-
8/7/2019 Management of Pain in Cancer Patients and Chemotherapy
14/20
14 | P a g e
12. Encourage fluid intake toprevent constipation.13. Monitor intake andoutput, including emesis.14. Consult dietitian about patient's foodpreferences, intolerances, and individual dietary
interventions.
15. Recognize that the patient may have alterations in taste perception, such as a keener taste ofbitterness and loss ofability todetect sweet tastes.
E. Minimizing Stomatitis1. Report signs ofinfection erythematous areas, white patches, ulcers.2. Encourage goodoral hygiene.
a. Soft nylon bristled toothbrush, brush2 to 3 times daily, rinse frequentlyb. Floss once daily
3. Encourage the use oforal agents topromote cleansing, debridement, and comfort.Mouthwashes withmore than25% alcohol should be avoided.
4. Assess the needfor antifungal, antibacterial, or antiviral therapy (each infectionhas a differentappearance).
5. Administer local oral therapy such as combinations with viscous lidocaine (Xylocaine) forsymptomatic control andmaintenance ofcalorie intake.
F. Preventing and Managing Hypersensitivity Reactions1. Be alert for signs ofallergic reactions such as pruritus, urticaria, anddifficulty breathing, as
well as back pain. Situationmay worsen suddenly tohypotension and anaphylaxis.
2. Stop the medicationor infusion immediately, notify the health care provider, andmonitorthe patient closely. Treatment is supportive anddependent on type ofreaction and its
severity.
a. Donot administer the agent again ifthere was a severe reaction resulting in significanthypotension.
b. Premedicate the patient with antihistamine or corticosteroid as directed ifthere is ahistory ofmoderate reaction.
G. Strengthening Coping for AlteredBody Image1. Reassure patient that hair will usually grow back; however, it may grow back a different
texture or different color.
2. Suggest wearing a turban, wig, or headscarf, preferably purchased before hair lossoccurs. Many insurance companies will pay for a wig with a prescription.
3. Encourage patient to stay on therapeutic program.4. Be honest with the patient.
-
8/7/2019 Management of Pain in Cancer Patients and Chemotherapy
15/20
15 | P a g e
H. Patient Education andHealth Maintenance
1. Make sure that patient uses goodhygiene, knows symptoms ofinfection to report, andavoids crowds andpeople with infectionwhile neutropenic.
2. Advise patient to avoid using a razor blade to shave, contact sports, manipulationofsharp articles, use ofhard bristle toothbrush, andpassage ofhard stool toprevent
bleeding while thrombocytopenic.
3. Advise women to report symptoms ofvaginal infectiondue toopportunistic fungal orviral infection.
4. Encourage patient participation inplanfor chemotherapy and to set realistic goals forwork and activities.
5. Assure patient that changes inmenses, libido, and sexual function are usually temporaryduring therapy.
Evaluation: Expected Outcomes1. Afebrile, no signs ofinfection2. No bruising or bleeding noted; stool and urine heme test negative3. Denies shortness ofbreathor severe fatigue4. Tolerates small, frequent meals following antiemetic5. Nooral lesions or painon swallowing6. No urticaria, shortness ofbreath, or change in vital signs7. Wears turban, expresses feelings about body image
-
8/7/2019 Management of Pain in Cancer Patients and Chemotherapy
16/20
Table 1 Classification of drugs Used in Chemotherapy
Classification Cell Cycle
Specificity
Mechanism of
Action
Side effects
ALKYLATING AGENTS Cell cycle non-specific
Alter DNAsynthesis bymisreading DNAcode, initiatingbreaks in theDNAmolecules,cross-linking DNA
strands.
Bone marrowsuppression,vomiting, nausea,cystitis,(cyclophossphamide,Ifosfamide),stomatitis, alopecia,gonadalsuppression, renal
toxicity (cisplatin)
Busulfan(Paraplatcisplatin(Cytoxan
or altretaMelphala(Mustarg
(Thioplex
NITROSOUREAS Cell cycle non-
Specific
Similar to
Alkylating agents;cross the blood-
brain barrier
Delayed and
cumulativemyelosuppression, ,especiallythrombocytopenia;
nausea and vomiting
Carmusti
Semustin
TOPOISOMERASE I
INHIBITORS
Cell cyclespecific (S-
Phase)
Induce breaks inthe DNA strandsby binding toenzymetopoisomerase I,
preventing cells
fromdividing
Bone marrowduppression,nausea, vomiting,diarrhea,
hepatotoxicity
Irinoteca
Topoteca
-
8/7/2019 Management of Pain in Cancer Patients and Chemotherapy
17/20
ANTIMETABOLITES Cell cyclespecific (S
Phase)
Interfere with thebiosynthesis of
metabolites or
nucleic acid
necessary for the
synthesis ofRNA
and DNA
nausea, vomiting ,
diarrhea, bone marrowsuppression, proctitis,stomatitis ,renal toxicity(methotrexate),
hepatotoxicity,
5-AzacytCytarabinFluourac
Methotre
ANTI-TUMOR ANTIBIOTICS Cell cycle non-
specific
Interfere DNAsynthesis bybinding DNA,prevent RNA
synthesis
Bone Marrowdepression, gonadalSuppression, vesication ,nausea, vomiting ,alopecia, anorexia,
cardiac toxicity
Bleomyc(DaunoX
Plicamyc
MITOTIC SPINDLE POISONS
Plant alkaloids
Taxenes
Cell cyclespecific (M
Phase)
Cell cycle
specific (MPhase)
Arrest metaphaseby inhibitingmitotic tubularformation(spindle); inhibitDNA andprotein
synthesis
Arrest metaphase
by inhibitingtubulin
depolymerization
Bone marrow suppression(mildwithVCR),Neuropathies (VCR),
stomatitis
Bradycardia,hypersensitivity, bonemarrow suppression,
alopecia, neuropathies
VincristinToposar)(Velban),
(Navelbin
Paclitaxe
-
8/7/2019 Management of Pain in Cancer Patients and Chemotherapy
18/20
HORMONAL AGENTS Cell cycle non-
specific
Binds tohormonereceptor site thatalters cellulargrowth; blockbinding of
estrogens toreceptor sites
(antiestrogens);inhibit RNAsynthesis;suppressaromatase ofp450 sytemwhichdecreaseslevel
Hypercalcemia,jaundice,Increased appetite,
masculinization,
femininization, sodiumandfluid retention,
nausea, vomiting, hotflashes, vaginal estrogen
dryness
Androgeand antieatiprogesluteinizin
analogue
Miscellaneous Agent Varies Unknownor toocomplex to
classify
Anorexia, nausea,vomiting, bone marrowsuppression,
hepatotoxicity,
hypotension,anaphylaxis, altered
glucose metabolism
Aspargin
(Matulan
-
8/7/2019 Management of Pain in Cancer Patients and Chemotherapy
19/20
19 | P a g e
Safety Measures in Handling Chemotherapy
A. Personal Safety to Minimize Exposure via Inhalation1. Chemotherapeutic agents should be prepared in a class II biologic safety cabinet (vertical
laminar flowhood).
2. Vent vials withfilter needle to equalize the internal pressure or use negative-pressuretechniques.
3. Wrap gauze or alcohol pads around the neck ofampules whenopening todecrease dropletcontamination.
4. Wrap gauze or alcohol pads around injection sites when removing syringes or needles fromI.V. injectionports.
5. Donot dispose ofmaterials by clipping needles or removing needles from syringes.6. Use puncture- and leak-proofcontainers for non-capped, non-clippedneedles.
B. Personal Safety to Minimize Exposure via Skin Contact1. Wear nitrile examination gloves at all times whenpreparing or working with
chemotherapeutic agents.
2. Washhands before putting on and after removing gloves.3. Change gloves after each use, tear, puncture, or medication spill or after every 60 minutes
ofwear.
4. Wear a long-sleeve, nonabsorbent gownwith elastic at the wrists and back closure.5. Eye andface shields should be worn ifsplashes are likely tooccur.6. Use syringes and I.V. tubing with Luer locks (whichhave a locking device toholdneedle
firmly inplace).
7. Label all syringes and I.V. tubing containing chemotherapeutic agents as hazardousmaterial.
8. Place an absorbent paddirectly under the injection site to absorb any accidental spillage.9. Ifany contact with the skinoccurs, immediately wash the area thoroughly with soap and
water.
10.Ifcontact is made with the eye, immediately flush the eye withwater and seek medicalattention.
11.Spill kits should be available in all areas where chemotherapy is stored, prepared, andadministered.
C. Personal Safety to Minimize Exposure via Ingestion1. Donot eat, drink, chew gum, or smoke while preparing or handling chemotherapy.2. Keep all food anddrink away frompreparation area.3. Washhands before and after handling chemotherapy.
-
8/7/2019 Management of Pain in Cancer Patients and Chemotherapy
20/20
20 | P a g e
4. Avoidhand-to-mouthor hand-to-eye contact while handling chemotherapeutic agents orbody fluids ofthe person receiving chemotherapy.
D. Safe Disposal ofAntineoplastic Agents, Body Fluids, and Excreta1. Discard gloves and gown into a leak-proofcontainer, which should be marked as
contaminatedor hazardous waste.
2. Use puncture- and leak-proofcontainers for needles andother sharpor breakable objects.3. Linens contaminatedwith chemotherapy or excreta frompatients whohave received
chemotherapy within 48 hours should be contained in specially markedhazardous waste
bags.
4. Wear non-sterile nitrile gloves for disposing ofbody excreta andhandling soiled linenswithin 48 hours ofchemotherapy administration.
5. In the home, wear gloves whenhandling bed linens or clothing contaminatedwithchemotherapy or patient excreta within 48 hours ofchemotherapy administration. Place
linens in a separate, washable pillow case.Wash separately inhot water and regular
detergent.