Management of Mitral Stenosis Using 2D and 3D Echo...
15
iREVIEWS STATE-OF-THE-ART PAPERS Management of Mitral Stenosis Using 2D and 3D Echo-Doppler Imaging Nina C. Wunderlich, MD,*y Roy Beigel, MD,zx Robert J. Siegel, MDz Rostock and Darmstadt, Germany; Los Angeles, California; and Tel Hashomer and Tel Aviv, Israel From the *University Hospital Rostock, Rostock, Germany; yCardiovascular Center Darmstadt, Darmstadt, Germany; zThe Heart Institute, Cedars-Sinai Medical Center, Los Angeles, California; and xThe Heart Institute, Sheba Medical Center, Tel Hashomer, Sackler School of Medicine, Tel Aviv University, Tel Aviv, Israel. The authors have reported that they have no relationships relevant to the contents of this paper to disclose. Manuscript received May 10, 2013; revised manuscript received July 3, 2013, accepted July 18, 2013. JACC: CARDIOVASCULAR IMAGING CME CME Editor: Ragavendra R. Baliga, MD This article has been selected as this issue’s CME ac- tivity, available online at http://imaging.onlinejacc.org by selecting the CME tab on the top navigation bar. Accreditation and Designation Statement The American College of Cardiology Foundation (ACCF) is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. The ACCF designates this Journal-based CME activity for a maximum of 1 AMA PRA Category 1 Credit(s)™. Physicians should only claim credit commensurate with the extent of their participation in the activity. Method of Participation and Receipt of CME Certificate To obtain credit for this CME activity, you must: 1. Be an ACC member or JACC: Cardiovascular Imaging subscriber. 2. Carefully read the CME-designated article available online and in this issue of the journal. 3. Answer the post-test questions. At least 2 out of the 3 questions provided must be answered correctly to obtain CME credit. 4. Complete a brief evaluation. 5. Claim your CME credit and receive your certifi- cate electronically by following the instructions given at the conclusion of the activity. CME Objective for This Article: At the end of this activity the reader should be able to: 1) recognize and identify the severity of mitral stenosis (mild, moderate, severe) using various echocardiographic methods; 2) recognize those patients who would benefit and are amenable to treatment by percuta- neous mitral balloon valvuloplasty (PMBV); and 3) utilize echocardiography to guide and assess the result of PMBV. CME Editor Disclosure: JACC: Cardiovascular Imaging CME Editor Ragavendra R. Baliga, MD, has re- ported that he has no relationships to disclose. Author Disclosure: The authors have reported that they have no relationships relevant to the contents of this paper to disclose. Medium of Participation: Print (article only); online (article and quiz). CME Term of Approval: Issue Date: November 2013 Expiration Date: October 31, 2014 JACC: CARDIOVASCULAR IMAGING VOL. 6, NO. 11, 2013 ª 2013 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-878X/$36.00 PUBLISHED BY ELSEVIER INC. http://dx.doi.org/10.1016/j.jcmg.2013.07.008
Transcript of Management of Mitral Stenosis Using 2D and 3D Echo...

J A C C : C A R D I O V A S C U L A R I M A G I N G V O L . 6 , N O . 1 1 , 2 0 1 3
ª 2 0 1 3 B Y T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N I S S N 1 9 3 6 - 8 7 8 X / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R I N C . h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j c m g . 2 0 1 3 . 0 7 . 0 0 8
iREVIEWSS T A T E - O F - T H E - A R T P A P E R S
Management of Mitral Stenosis Using2D and 3D Echo-Doppler Imaging
Nina C. Wunderlich, MD,*y Roy Beigel, MD,zx Robert J. Siegel, MDz Rostock and Darmstadt, Germany; Los Angeles, California; and Tel Hashomer and Tel Aviv, IsraelFrom the *University Hospital Rostock, Rostock, Germany; yCardiovascular Center Darmstadt, Darmstadt, Germany; zTheHeart Institute, Cedars-Sinai Medical Center, Los Angeles, California; and xThe Heart Institute, Sheba Medical Center,
Tel Hashomer, Sackler School of Medicine, Tel Aviv University, Tel Aviv, Israel. The authors have reported that they have
no relationships relevant to the contents of this paper to disclose.
Manuscript received May 10, 2013; revised manuscript received July 3, 2013, accepted July 18, 2013.
JACC: CARDIOVASCULAR IMAGING CME
CME Editor: Ragavendra R. Baliga, MD
This article has been selected as this issue’s CME ac-
tivity, available online at http://imaging.onlinejacc.org
by selecting the CME tab on the top navigation bar.
Accreditation and Designation Statement
The American College of Cardiology Foundation
(ACCF) is accredited by the Accreditation Council
for Continuing Medical Education (ACCME) to
provide continuing medical education for physicians.
The ACCF designates this Journal-based CME
activity for a maximum of 1 AMA PRA Category 1
Credit(s)™. Physicians should only claim credit
commensurate with the extent of their participation
in the activity.
Method of Participation and Receiptof CME Certificate
To obtain credit for this CME activity, you must:1. Be an ACC member or JACC: Cardiovascular
Imaging subscriber.2. Carefully read the CME-designated article
available online and in this issue of the journal.3. Answer the post-test questions. At least 2 out of
the 3 questions provided must be answeredcorrectly to obtain CME credit.
4. Complete a brief evaluation.
5. Claim your CME credit and receive your certifi-cate electronically by following the instructionsgiven at the conclusion of the activity.
CME Objective for This Article: At the end of this
activity the reader should be able to: 1) recognize
and identify the severity of mitral stenosis (mild,
moderate, severe) using various echocardiographic
methods; 2) recognize those patients who would
benefit and are amenable to treatment by percuta-
neous mitral balloon valvuloplasty (PMBV); and
3) utilize echocardiography to guide and assess the
result of PMBV.
CME Editor Disclosure: JACC: Cardiovascular ImagingCME Editor Ragavendra R. Baliga, MD, has re-
ported that he has no relationships to disclose.
Author Disclosure: The authors have reported that
they have no relationships relevant to the contents of
this paper to disclose.
Medium of Participation: Print (article only);
online (article and quiz).
CME Term of Approval:Issue Date: November 2013
Expiration Date: October 31, 2014

Wunderlich et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 6 , N O . 1 1 , 2 0 1 3
Echocardiography in Mitral Stenosis N O V E M B E R 2 0 1 3 : 1 1 9 1 – 2 0 5
1192
Management of Mitral Stenosis Using2D and 3D Echo-Doppler Imaging
Although the prevalence of rheumatic fever is decreasing in developed countries, it still affects numerous areas in
the nonindustrialized world. Untreated mitral stenosis (MS) contributes to a significant global morbidity and
mortality. Echocardiography is the main diagnostic imaging modality with which to evaluate mitral valve (MV)
obstruction and assess the severity and hemodynamic consequences of MS as well as valve morphology.
According to current guidelines and recommendations for clinical practice, the severity of MS should not be
defined by a single value but assessed by valve areas, mean Doppler gradients, and pulmonary pressures.
Transthoracic echocardiography is usually sufficient to grade MS severity and to define the morphology of the
valve. Transesophageal echocardiography is used when the valve cannot be adequately assessed with
transthoracic echocardiography and to exclude intracardiac thrombi before a percutaneous or surgical
intervention. Three-dimensional transthoracic and transesophageal echocardiographic assessment provide
more detailed physiological and morphological information. Current definitive treatment for severe MS
involves percutaneous mitral balloon valvuloplasty (PMBV) or surgery. The effectiveness of PMBV is related to
the etiology of MS, and certain anatomic characteristics tend to predict a more successful outcome for PMBV,
whereas other MV structural findings might suggest balloon valvuloplasty to be less likely successful or even
contraindicated. (J Am Coll Cardiol Img 2013;6:1191–205) ª 2013 by the American College of Cardiology
Foundation
Rheumatic fever (RF) is the major cause of mitralstenosis (MS), and although its prevalence has beensteadily decreasing in industrialized countries (1,2),rheumatic MS remains the most common heartdisease in developing countries (3–5). Globally,there are >15 million cases of rheumatic heartdisease, with 233,000 deaths each year and 282,000new cases per year (6).Surgical commissurotomy, first described in
1923 (7), became the standard treatment for pa-tients with MS in the late 1940s (8). Sincethe introduction of the Inoue balloon catheterin 1984 (9), percutaneous mitral balloon valvulo-plasty (PMBV) emerged as a safe and effectivetreatment for MS (10–18) and has evolved as thepreferred treatment option for selected symptom-atic patients with rheumatic MS (19–21).The focus of this review is on current
2-dimensional (2D) and 3-dimensional (3D)echocardiographic imaging for the selection ofsuitable patients for PMBV and on the periproce-dural aspects of PMBV.
Rheumatic MS
If the mitral valve (MV) orifice area exceeds1.5 cm2, patients are generally asymptomatic atrest (1). The clinical exacerbation of MS occurringwith pregnancy or complications such as atrial
fibrillation or embolic events (22) confer a poorprognosis if no intervention is performed to correctthe MS (1,2,23–25). Commissural fusion is therequisite lesion for PMBV to be effective (Fig. 1).Thus, the effectiveness of PMBV is related to theetiology of MS. RF, the major cause of MS (1,2),results in commissural fusion of the MV, whichleads to narrowing of the valve orifice and valveobstruction. In degenerative MS (Fig. 2), generallyseen in the elderly or in patients with severe renaldisease and secondary hyperparathyroidism,advanced mitral annular calcification is the mainlesion and commissural fusion is not present. Otherrare causes of MS include congenital MS, asdemonstrated in Figure 3, inflammatory diseases,infiltrative diseases, carcinoid heart disease, anddrug-induced MS. As with degenerative MS,commissural fusion is rare in these cases; mostcommonly, the leaflets are thickened and restricted,and, thus, these cases are generally not well suitedfor PMBV.
Echocardiographic assessment of MS
Echocardiography is the main diagnostic imagingmodality to evaluate MV obstruction and to assessthe severity and the hemodynamic consequences ofMS, as well as valve morphology and extent of thedisease (19,20).

A B B R E V I A T I O N S
A N D A C R O N YM S
2D = 2-dimensional
3D = 3-dimensional
IAS = interatrial septum
MR = mitral regurgitation
MS = mitral stenosis
MV = mitral valve
MVA = mitral valve area
PHT = pressure half-time
PISA = proximal isovelocity
surface area
PMBV = percutaneous mitral
balloon valvuloplasty
RF = rheumatic fever
RT-TT3DE = real-time
3-dimensional transthoracic
echocardiography
TEE = transesophageal
echocardiography
TTE = transthoracic
echocardiography
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 6 , N O . 1 1 , 2 0 1 3 Wunderlich et al.
N O V E M B E R 2 0 1 3 : 1 1 9 1 – 2 0 5 Echocardiography in Mitral Stenosis
1193
Transthoracic echocardiography (TTE) is usu-ally sufficient to grade MS severity and to definethe morphology of the MV. Transesophagealechocardiography (TEE) is used when the valvecannot be adequately assessed with TTE and toexclude intracardiac thrombi before a percutaneousor surgical intervention. A 3D TTE and TEEassessment should be incorporated into the routineevaluation of the MV because it provides moredetailed physiological and morphological infor-mation (26). A stress test should be consideredwhen there is a discrepancy between the restingDoppler echocardiographic measurements andsymptoms.
The decision for the method of treatment forthe patient and the timing of intervention shouldbe based on functional status, surgical risk, valveanatomy, concomitant diseases, and institutionalexpertise.Assessment of MS severity. According to currentguidelines and recommendations for clinical practice(19,20,27), the severity of MS should not be definedby a single value but rather be assessed by a multi-modality approach that determines valve areas,mean Doppler gradients, and pulmonary pressures(Table 1).MV AREA. Mitral valve area (MVA) can be assessedby planimetry using either 2D or 3D imaging,pressure half-time (PHT), the continuity equation,and the proximal isovelocity surface area (PISA)method.
The 2D planimetry of the MVA is performed ina parasternal short-axis view at the tip of the leafletswhen maximal excursion of the leaflets is seen. Theinner edge of the MV orifice is traced in mid-diastole (Fig. 4A). The entire MV orifice shouldbe seen. High gain settings should be avoidedas they may lead to underestimation of the MVA.Planimetry has been shown to have the best corre-lation with anatomic MVA as assessed by explantedvalves (28). Two-dimensional planimetry tends tooverestimate MVA compared with 3D TEE mea-surements (Figs. 4B and 4C), especially in patientswith a large left atrium (29). As shown in Figure 5,3D echocardiography provides better alignment ofthe image plane at the mitral tips, rendering a moreaccurate and reproducible planimetric measurementwith excellent interobserver and intraobserveragreement (29–31).
Complementary to MV planimetry, the MVAcan also be derived from Doppler echocardiographyusing the diastolic PHT method (Fig. 4D) (32).PHT is obtained by tracing the decelerationslope of the E-wave on Doppler spectral display
of transmitral inflow. The MVA can be calculatedfrom the following simplified formula: 220/PHT.In case of a bimodal deceleration slope, as shownin Figure 6, it is preferable to trace the decelerationslope in mid-diastole rather than to trace the earlydeceleration slope (33). In patients with atrialfibrillation, the tracing should be performed in longdiastoles and average multiple cardiac cycles. Inpatients with a concave shape on the Dopplertracing, the method cannot be reliably used. Thomasand Weyman (32) demonstrated that the PHTshould vary inversely with the MVA, but also pro-portionally to net left atrial and ventricular compli-ance and to the square root of the peak transmitral
gradient. Limitations of the PHT methodtherefore include patients with abnormalleft atrial or left ventricular compliance aswell as patients with associated aorticregurgitation and atrial septal defects andthose who have undergone a previousmitral valvuloplasty (34–38). Sole relianceon PHT to determine the severity of MSshould be discouraged.MS severity can also be assessed by thecontinuity equation (35) based on theassumption that the filling volume of dia-stolic mitral flow is equal to aortic strokevolume. The following formula is used:
MVA ¼ p
�D2
4
��VTI aorta ðcmÞVTI mitral ðcmÞ
�
where D is the left ventricular outflow tractdiameter and VTI is the velocity timeintegral.
The accuracy and reproducibility of themethod are limited in that the number ofmeasurements needed for this calculationincrease the probability of measurementerrors. If more than mild mitral or aortic
regurgitation is present, the continuity equation willnot be accurate and should not be used.A fourth method for calculation of the MVA isthe PISA method, which enables the assessment ofmitral flow based on the hemispheric shape of theconvergence zone of mitral flow in diastole on theleft atrial side as seen by color Doppler. Subse-quently, the MVA is calculated by dividing themitral volume flow by the maximum velocity ofmitral flow in diastole, as assessed by continuous-wave Doppler: MVA¼ p (r2)(Valias)/peak Vmitral �a/180�, where r is the radius of the hemisphericconvergence zone (in centimeters), Valias is the ali-asing velocity (in centimeters per second), peakVmitral is the peak velocity of mitral inflow assessed

Figure 2. Example of a Degenerative Mitral Stenosis
Severe calcification of the mitral annulus is presented in a 4-chamber view with (A) andwithout (B) color Doppler. (B) The accelerated mitral inflow through the stenosis is shown.(C) A short axis view demonstrates severe calcification of the posterior mitral ring (whitearrows). (D) The measurement of the Doppler gradients reveals relevant mitral stenosis(mean gradient: 12 mm Hg). LA ¼ left atrium; LV ¼ left ventricle; MV ¼ mitral valve;RA ¼ right atrium; RV ¼ right ventricle.
Figure 1. Example of a Typical Rheumatic Mitral Stenosis
(A) Leaflet thickening at the edges is shown in a parasternal long axis transthoracic view.(B) The immobility of the posterior leaflet and the doming of the anterior leaflet as typicalmorphological characteristics of rheumatic mitral valve disease are shown in a 3-dimen-sional transesophageal image. The 3-dimensional transesophageal images (left atrial aspect[C]) and (left ventricular aspect [D]) show the fusion of both commissures (red arrows).AML ¼ anterior mitral leaflet; PML ¼ posterior mitral leaflet.
Wunderlich et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 6 , N O . 1 1 , 2 0 1 3
Echocardiography in Mitral Stenosis N O V E M B E R 2 0 1 3 : 1 1 9 1 – 2 0 5
1194
by continuous-wave Doppler (in centimeters persecond), and a is the opening angle of mitral leafletsrelative to flow direction.
The PISA method is technically demanding, butit can be used in the presence of severe mitralregurgitation (MR). The integration of colorM-mode, enabling simultaneous measurements ofvelocity and flow, improves the accuracy of thismethod (39).
According to Sugeng et al. (31), direct 3Dplanimetry from the left ventricular side is themost accurate method for MVA evaluation. ThePISA method was the most accurate of all 2Dtechniques, followed by the PHT method, and2D planimetry.
MEAN PRESSURE GRADIENT. Doppler measure-ments (transvalvular gradients) using the continuous-wave Doppler signal across the MV show goodcorrelation with invasive measurements using trans-septal catheterization (40). The Doppler diastolicmitral flow profile is traced, and the maximal andmean gradients are subsequently calculated automat-ically by integrated software (Fig. 4E). The maximalgradient is derived from peak mitral velocity and isstrongly influenced by left atrial compliance and leftventricular diastolic function (41). The mean gradientis the major hemodynamic determinant of MSseverity. Doppler measurements are highly heart rateand flow dependent because the transmitral gradientis a function of the square of the transvalvular flowrate and therefore dependent on the diastolic fillingof the left ventricle (42). Despite these limitations,transvalvular gradients are very useful for theassessment of MS severity, particularly in patients insinus rhythm.
PULMONARY ARTERY PRESSURE. The degree ofpulmonary hypertension is an indicator of theoverall hemodynamic consequences of MS, andsevere pulmonary hypertension is associated with adecrease in mean survival of <3 years (43). There-fore, pulmonary pressures should be serially evalu-ated and followed in all patients with significant MS(21). The presence of more than mild MR ($2þ) isassociated with worse outcomes (44) and is a relativecontraindication to PMBV (20,21). Consequently,MR severity should be precisely categorized before aPMBV according to current guidelines (19,20).Concomitant valve diseases are frequently associatedwith rheumatic MS. Because stroke volumes aredecreased in patients with MS, the severity of aorticstenosis may be underestimated. In patients withmore than mild aortic regurgitation, the PHTmethod is not accurate.
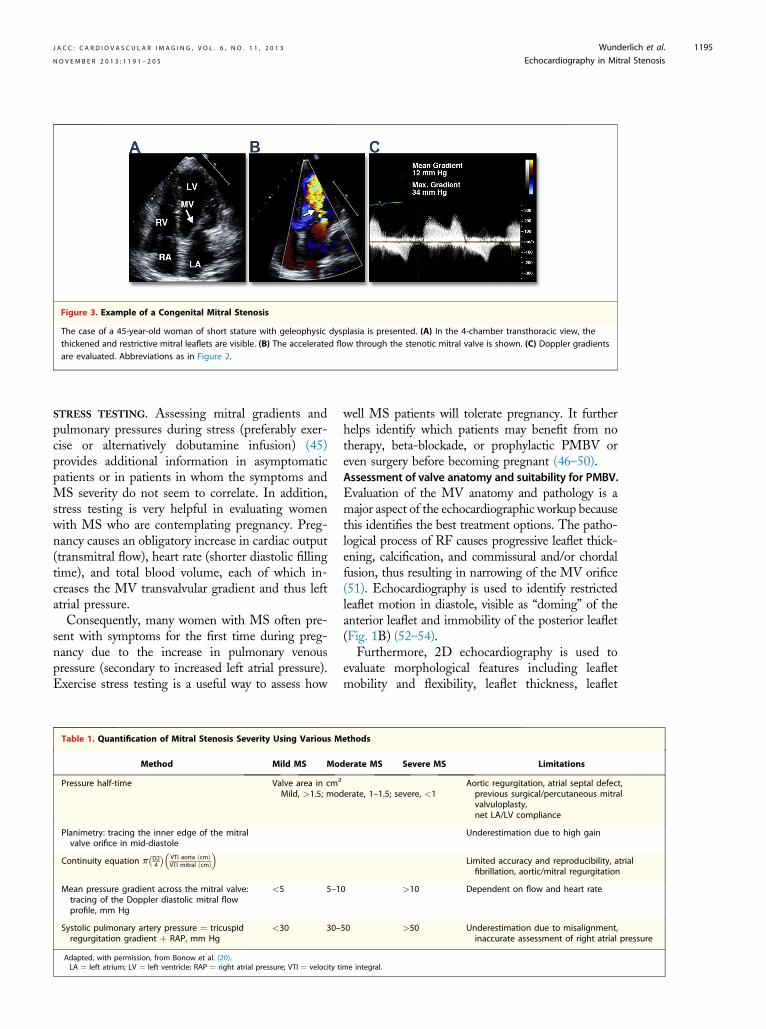
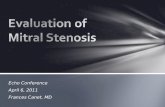
Figure 3. Example of a Congenital Mitral Stenosis
The case of a 45-year-old woman of short stature with geleophysic dysplasia is presented. (A) In the 4-chamber transthoracic view, thethickened and restrictive mitral leaflets are visible. (B) The accelerated flow through the stenotic mitral valve is shown. (C) Doppler gradientsare evaluated. Abbreviations as in Figure 2.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 6 , N O . 1 1 , 2 0 1 3 Wunderlich et al.
N O V E M B E R 2 0 1 3 : 1 1 9 1 – 2 0 5 Echocardiography in Mitral Stenosis
1195
STRESS TESTING. Assessing mitral gradients andpulmonary pressures during stress (preferably exer-cise or alternatively dobutamine infusion) (45)provides additional information in asymptomaticpatients or in patients in whom the symptoms andMS severity do not seem to correlate. In addition,stress testing is very helpful in evaluating womenwith MS who are contemplating pregnancy. Preg-nancy causes an obligatory increase in cardiac output(transmitral flow), heart rate (shorter diastolic fillingtime), and total blood volume, each of which in-creases the MV transvalvular gradient and thus leftatrial pressure.
Consequently, many women with MS often pre-sent with symptoms for the first time during preg-nancy due to the increase in pulmonary venouspressure (secondary to increased left atrial pressure).Exercise stress testing is a useful way to assess how
Table 1. Quantification of Mitral Stenosis Severity Using Various M
Method Mild MS Mo
Pressure half-time Valve area in cm2
Mild, >1.5; mod
Planimetry: tracing the inner edge of the mitralvalve orifice in mid-diastole
Continuity equation p�D24
��VTI aorta ðcmÞVTI mitral ðcmÞ
�
Mean pressure gradient across the mitral valve:tracing of the Doppler diastolic mitral flowprofile, mm Hg
<5 5–1
Systolic pulmonary artery pressure ¼ tricuspidregurgitation gradient þ RAP, mm Hg
<30 30–
Adapted, with permission, from Bonow et al. (20).LA ¼ left atrium; LV ¼ left ventricle; RAP ¼ right atrial pressure; VTI ¼ velocity t
well MS patients will tolerate pregnancy. It furtherhelps identify which patients may benefit from notherapy, beta-blockade, or prophylactic PMBV oreven surgery before becoming pregnant (46–50).Assessment of valve anatomy and suitability for PMBV.Evaluation of the MV anatomy and pathology is amajor aspect of the echocardiographic workup becausethis identifies the best treatment options. The patho-logical process of RF causes progressive leaflet thick-ening, calcification, and commissural and/or chordalfusion, thus resulting in narrowing of the MV orifice(51). Echocardiography is used to identify restrictedleaflet motion in diastole, visible as “doming” of theanterior leaflet and immobility of the posterior leaflet(Fig. 1B) (52–54).
Furthermore, 2D echocardiography is used toevaluate morphological features including leafletmobility and flexibility, leaflet thickness, leaflet
ethods
derate MS Severe MS Limitations
erate, 1–1.5; severe, <1Aortic regurgitation, atrial septal defect,previous surgical/percutaneous mitralvalvuloplasty,net LA/LV compliance
Underestimation due to high gain
Limited accuracy and reproducibility, atrialfibrillation, aortic/mitral regurgitation
0 >10 Dependent on flow and heart rate
50 >50 Underestimation due to misalignment,inaccurate assessment of right atrial pressure
ime integral.

Figure 5.
The multiopening d
Figure 4. Different Methods to Evaluate the MVA and Assessment of Doppler Gradients
(A) A planimetric measurement in a transthoracic short-axis view is shown. (B) Using 3-dimensional (3D) transesophageal echocardiography(TEE), the planimetry is done in a post-processing step (Q-lab, Philips, Andover, Massachusetts). (C) The direct delineation of the MVA (mitralvalve area) in a 3D TEE image (left ventricular aspect) is demonstrated. (D) The MVA is assessed by using pressure half-time (PHT), which is 218ms (calculated valve area: 1.01 cm2). (E) Mean and maximal Doppler gradients are obtained by tracing the Doppler diastolic mitral flow profile.
Wunderlich et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 6 , N O . 1 1 , 2 0 1 3
Echocardiography in Mitral Stenosis N O V E M B E R 2 0 1 3 : 1 1 9 1 – 2 0 5
1196
calcification, subvalvular fusion, commissural fusion,and calcification. These morphological features are
3-Dimensional Transesophageal Measurement of the MVA
plane method allows for exact definition of the orifice area at maximaluring diastole. The calculated MVA (mitral valve area) is 1.05 cm2.
used by different scoring systems (10,55–59) todescribe the extent of the MV disease, to evaluatethe suitability for PMBV, and to predict the successor even contraindication to PMBV. The followingscoring systems have been validated in larger seriesand have been shown to be useful even thoughthe predictive values of post-PMBV results arelimited:
- Wilkins score (58). This most commonlyused 2D TTE assessment of the MV in-cludes severity and extent of leaflet thick-ening, calcification, and involvement of thesubvalvular apparatus. Each feature is gradedon a scale of 1 to 4, yielding a maximal scoreof 16. A score >8 does not preclude PMBV,but is associated with less optimal results.
- Assessment of commissural calcium (Fig. 7)(59). With this method, the extent of com-missural calcification is quantified by givingeach half commissure (anterolateral andposteromedial) a score of 1 with the detectionof high-intensity bright echoes. Commissuralcalcification can therefore range from grade0 to grade 4. The grade of intercomissural

Figure 7. Evaluation of Commissural Calcification Score
Commissural calcification is quantified by giving a half commissure each(anterolateral and posteromedial) with detection of high-intensity brightechoes a score of 1. Commissural calcification can therefore range from grade0 (no calcification) to grade 4. (A) Both commissures are completely calcified.(B) An example in which half a commissure is calcified on the left side and theentire commissure is calcified on the right side. The added score is therefore 3.(C) A 2-dimensional transthoracic short-axis view at the level of the mitralleaflets shows that only 1 commissure is completely calcified, whereas theother commissure shows no calcification. (D) The corresponding left atrial3-dimensional transesophageal echocardiographic aspect is presented. Thecalculated score in this example is 2. ALC ¼ anterolateral commissure; Ao ¼aorta; PMC ¼ posteromedial commissure.
T
M
Figure 6. Example of a Bimodal Deceleration Slope
It is preferable to trace the deceleration slope in mid-diastole (redline) than tracing the early deceleration slope (yellow line).
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 6 , N O . 1 1 , 2 0 1 3 Wunderlich et al.
N O V E M B E R 2 0 1 3 : 1 1 9 1 – 2 0 5 Echocardiography in Mitral Stenosis
1197
calcium is a predictor of achieving an MVApost-PMBV >1.5 cm2 without creating sig-nificant MR. The influence was most evidentin patients with a Wilkins score of #8 (i.e.,patients who are likely to be amenable toPMBV), whereas the influence was not sig-nificant in patients with a Wilkins score >8.Patients with a commissural calcificationgrade 0/1 had larger valve areas and a betterimprovement of symptoms than patientswith grade 2/3. Commissural calcification isa strong predictor of adverse outcomes ofPMBV (60) as well as of the occurrenceof severe MR as a major complication ofPMBV (61).
- Echocardiographic grouping (Table 2)(10). The echocardiographic grouping isbased on the echocardiographic and fluo-roscopic (calcification) assessment of thefollowing characteristics: valve mobility,fusion of the subvalvular apparatus, and theamount of leaflet calcification. It has been
able 2. Grouping of Mitral Anatomy as Assessed by 2-Dimensional E
Group 1
itral valveanatomy
Pliable, noncalcified anterior mitralleaflet and mild subvalvulardisease (thin chordae $10 mm long)
Pliable, noncalcifiesevere subvalvu<10 mm long)
shown in a subset of patients that a Wilkinsscore in the range of 7 to 9 correlated withthe echocardiographic group 1, a range of8 to 12 correlated with the echocardio-graphic group 2, and a range of 10 to 15with group 3 (62).
- Anwar et al. (63) (Table 3) introduced a scorebased on real-time 3-dimensional trans-thoracic echocardiography (RT-TT3DE) forthe assessment of patients with MS beforePMBV. This score includes the evaluation ofboth mitral leaflets and the subvalvularapparatus. The new RT-TT3DE score isfeasible and highly reproducible with good
chocardiography and Fluoroscopy
Group 2 Group 3
d anterior mitral leaflet andlar disease (thickened chordae
Calcification of mitral valve of any extent,as assessed by fluoroscopy, no matter thestate of the subvalvular apparatus

Table 3. Real-Time Transthoracic 3-Dimensional Echocardiographic Score for the Evaluation of Mitral Stenosis BeforePercutaneous Mitral Balloon Valvuloplasty
Anterior Mitral Leaflet Posterior Mitral Leaflet
A1 A2 A3 P1 P2 P3
Thickness* 0–1 0–1 0–1 0–1 0–1 0–1
Mobility* 0–1 0–1 0–1 0–1 0–1 0–1
Calcificationy 0–2 0–1 0–2 0–2 0–1 0–2
Subvalvular ApparatuszProximal Third Middle Third Distal Third
Thickness 0–1 0–1 0–1
Separation 0–2 0–2 0–2
The anterior and posterior leaflets are each divided into 3 segments (anterior leaflet: A1 [lateral segment], A2 [middle segment], A3 [medial segment]; posterior leaflet:P1 [lateral], P2 [middle], P3 [lateral]).*Each segment receives a separate score (either 0 for normal or 1 for abnormal) for thickness, mobility, and calcification. Normalscore ¼ 0, mild ¼ 1 to 2, moderate ¼ 3 to 4, severe ¼ $5. yAbsence of calcification is scored as 0, calcification in A2 or P2 (middle segments) is scored as 1, andcalcification of commissural segments of both leaflets (A1, A3 and P1 and P3) is scored as 2. For calcifications: normal score ¼ 0, mild ¼ 1 to 2, moderate ¼ 3 to 5,severe ¼$6. zThe anterior and posterior chordae are scored at proximal (mitral valve level), middle, and distal (papillary muscle level) levels. At each level, the anteriorand the posterior leaflet is scored for thickness and separation in between. Normal thickness is scored as 0, and abnormal thickness is scored as 1. Normal chordalseparation (defined as distance >5 mm) is scored as 0, partial separation (defined as distance <5 mm) is scored as 1, and absence of separation is scored 2. Theindividual points are added, with the total score ranging from 0 to 31 points. Mild MV involvement is defined as <8 points, moderate MV involvement is 8 to 13, andsevere MV involvement is >14 points. Adapted, with permission, from Anwar et al. (63).
Figure 8. Transseptal Puncture
(A) Determination of the puncture site is shown in a transesophageal echo-cardiography (TEE) x-plane view. A short-axis view (left side) and a long-axisview (right side) are presented simultaneously. The “tenting” of the interatrialseptum (caused by the transseptal needle) is marked with white arrows (A, B).(B) A 4-chamber view (TEE 0�) without (left) and with (right) color Dopplerdemonstrates the evaluation of the height above the mitral valve. SVC ¼superior vena cava; other abbreviations as in Figures 2 and 7.
Wunderlich et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 6 , N O . 1 1 , 2 0 1 3
Echocardiography in Mitral Stenosis N O V E M B E R 2 0 1 3 : 1 1 9 1 – 2 0 5
1198
interobserver and intraobserver agreement inthe assessment of MV morphology in pa-tients with MS. RT-TT3DE is better able todetect calcification and commissural splitting.Predictors of optimal PMBV results by the3D scoring system are leaflet mobility and theinvolvement of the subvalvular apparatus.The incidence and severity of post-proceduralMR are associated with a high RT-TT3DEcalcification score.
No individual scoring system is clearly superior toanother. Thus, the scoring systems should be usedin a complementary fashion, as a part of thecomprehensive echocardiographic assessment of theMV pathology and function.
Unfortunately all scoring systems are limitedby variable reproducibility because all scores aresemiquantitative; lesions may be underestimated,particularly with regard to the extension of thesubvalvular disease, and scores that describe theoverall degree of MV pathology may not adequatelyidentify localized abnormalities in specific partsof the MV and the MV apparatus, which may in-crease the risk of MR.
Many interventionalists consider or even recom-mend PMBV in patients with a high overall echo-cardiographic score, when commissural fusion ispresent, and when other clinical features arefavorable.
Contraindications to PMBV should be excluded(MVA >1.5 cm2, left atrial/left atrial appendagethrombus, MR that is more than mild, severe or
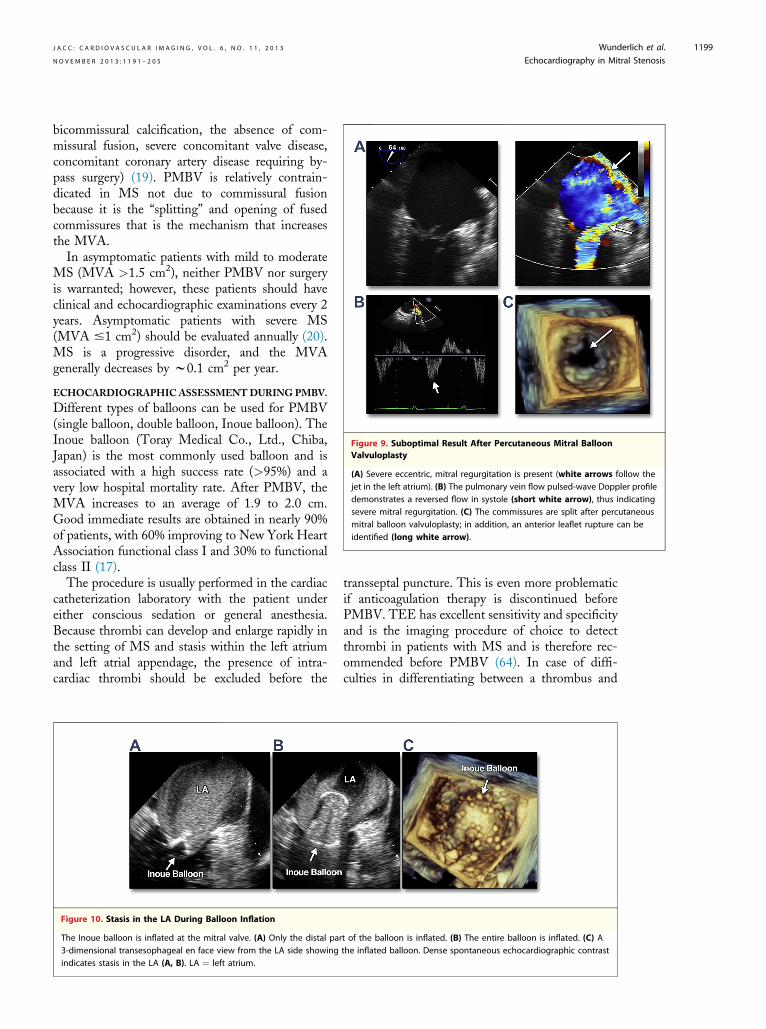
Figure 9. Suboptimal Result After Percutaneous Mitral BalloonValvuloplasty
(A) Severe eccentric, mitral regurgitation is present (white arrows follow thejet in the left atrium). (B) The pulmonary vein flow pulsed-wave Doppler profiledemonstrates a reversed flow in systole (short white arrow), thus indicatingsevere mitral regurgitation. (C) The commissures are split after percutaneousmitral balloon valvuloplasty; in addition, an anterior leaflet rupture can beidentified (long white arrow).
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 6 , N O . 1 1 , 2 0 1 3 Wunderlich et al.
N O V E M B E R 2 0 1 3 : 1 1 9 1 – 2 0 5 Echocardiography in Mitral Stenosis
1199
bicommissural calcification, the absence of com-missural fusion, severe concomitant valve disease,concomitant coronary artery disease requiring by-pass surgery) (19). PMBV is relatively contrain-dicated in MS not due to commissural fusionbecause it is the “splitting” and opening of fusedcommissures that is the mechanism that increasesthe MVA.
In asymptomatic patients with mild to moderateMS (MVA >1.5 cm2), neither PMBV nor surgeryis warranted; however, these patients should haveclinical and echocardiographic examinations every 2years. Asymptomatic patients with severe MS(MVA #1 cm2) should be evaluated annually (20).MS is a progressive disorder, and the MVAgenerally decreases by w0.1 cm2 per year.
ECHOCARDIOGRAPHIC ASSESSMENTDURING PMBV.
Different types of balloons can be used for PMBV(single balloon, double balloon, Inoue balloon). TheInoue balloon (Toray Medical Co., Ltd., Chiba,Japan) is the most commonly used balloon and isassociated with a high success rate (>95%) and avery low hospital mortality rate. After PMBV, theMVA increases to an average of 1.9 to 2.0 cm.Good immediate results are obtained in nearly 90%of patients, with 60% improving to New York HeartAssociation functional class I and 30% to functionalclass II (17).
The procedure is usually performed in the cardiaccatheterization laboratory with the patient undereither conscious sedation or general anesthesia.Because thrombi can develop and enlarge rapidly inthe setting of MS and stasis within the left atriumand left atrial appendage, the presence of intra-cardiac thrombi should be excluded before the
Figure 10. Stasis in the LA During Balloon Inflation
The Inoue balloon is inflated at the mitral valve. (A) Only the distal par3-dimensional transesophageal en face view from the LA side showingindicates stasis in the LA (A, B). LA ¼ left atrium.
transseptal puncture. This is even more problematicif anticoagulation therapy is discontinued beforePMBV. TEE has excellent sensitivity and specificityand is the imaging procedure of choice to detectthrombi in patients with MS and is therefore rec-ommended before PMBV (64). In case of diffi-culties in differentiating between a thrombus and
t of the balloon is inflated. (B) The entire balloon is inflated. (C) Athe inflated balloon. Dense spontaneous echocardiographic contrast

Figure 11. Mitral Commissurotomy Technique With the Inoue Balloon
(A) The inflation of the distal portion of the balloon is seen fluoroscopically. Thereafter, the balloon is pulled back at the mitral valve. (B) Asubsequent inflation of the proximal and middle portions of the balloon follows. A waist in the mid-portion of the balloon on both sides (redarrows) indicates that both commissures are still fused. (C) The balloon is fully inflated. The disappearance of the waist on one side (yellowarrow) indicates that this commissure is split, whereas the opposite commissure remains fused (red arrow). The asterisks mark the trans-esophageal echocardiography probe.
Wunderlich et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 6 , N O . 1 1 , 2 0 1 3
Echocardiography in Mitral Stenosis N O V E M B E R 2 0 1 3 : 1 1 9 1 – 2 0 5
1200
dense spontaneous echocardiographic contrast, theuse of contrast agents may be useful. Whether thisdistinction affects a patient’s management and/orprognosis has not been studied. The presence of athrombus in either the left atrium or left atrialappendage is considered as a relative contraindica-tion to PMBV. If a thrombus is detected, the pro-cedure should be postponed until the thrombusresolves on future TEE evaluation. If the thrombusdoes not resolve, surgery is considered the preferredtreatment option. However, some intervention-alists have shown that it is feasible to performPMBV using a modified Inoue technique in se-lected patients with laminar thrombus confined tothe left atrial appendage, particularly after 4 to 6
Table 4. Predictors of Outcome After Percutaneous Mitral Balloon
Predictors of Good Outcome
Commissural calcium grade 0/1 (60,61)Wilkins score <8 (12,49,58,72,73)Sinus rhythm (15,72,74)Good leaflet mobility (63)No involvement of the subvalvular apparatus (63)Age #65 yrs (70,73)Larger pre-procedural MVA (72)Normal mean pulmonary artery pressure (70)MR grade post-procedure #2 (15,72)Complete commissural opening (75)Larger MVA post procedure (72,73,75)Absence of calcium at fluoroscopy (74)Reduction in left atrial pressures post procedure (72)Lower MV gradient pressures post procedure (70,72)Echocardiographic grouping score <3 (59,70)
MR ¼ mitral regurgitation; MV ¼ mitral valve; MVA ¼ mitral valve area.
weeks of effective anticoagulation treatment (65).Nonetheless, our recommended approach is to avoidPMBV in the setting of thrombi due to the po-tential risk of iatrogenic catastrophic stroke.
For most PMBV cases, the preferred puncturesite for transseptal access to the left atrium is inthe posterior, more inferior region of the fossaovalis. Many operators rely primarily on fluoro-scopic guidance, but TEE or, alternatively, in-tracardiac echocardiographic guidance is helpful,especially in patients with a large atrium or un-usual morphology of the interatrial septum (IAS).The IAS morphology may be altered in the settingof a large atrial septum aneurysm, previous cardiacsurgery, or percutaneous procedures involving the
Valvuloplasty
Predictors of Poor Outcome
Age >65 yrs (10,62,70,71)Wilkins score >8 (12,50,58,71,73)Smaller initial MVA (10,62)Use of the double-balloon technique (62)High echocardiographic group (62)Commissural calcium grade 2/3 (59,60)Valvular calcification and severe subvalvular lesions (12)Previous commissurotomy (10)Baseline mitral regurgitation (10)Lower MVA post-procedure (63,70)Elevated post-procedural pulmonary artery pressure (71,76)Post-procedural MR $3þ (71)Previous surgical commissurotomy (62,71)New York Heart Association functional class IV (71)Echocardiographic grouping score of 3 (59,70)
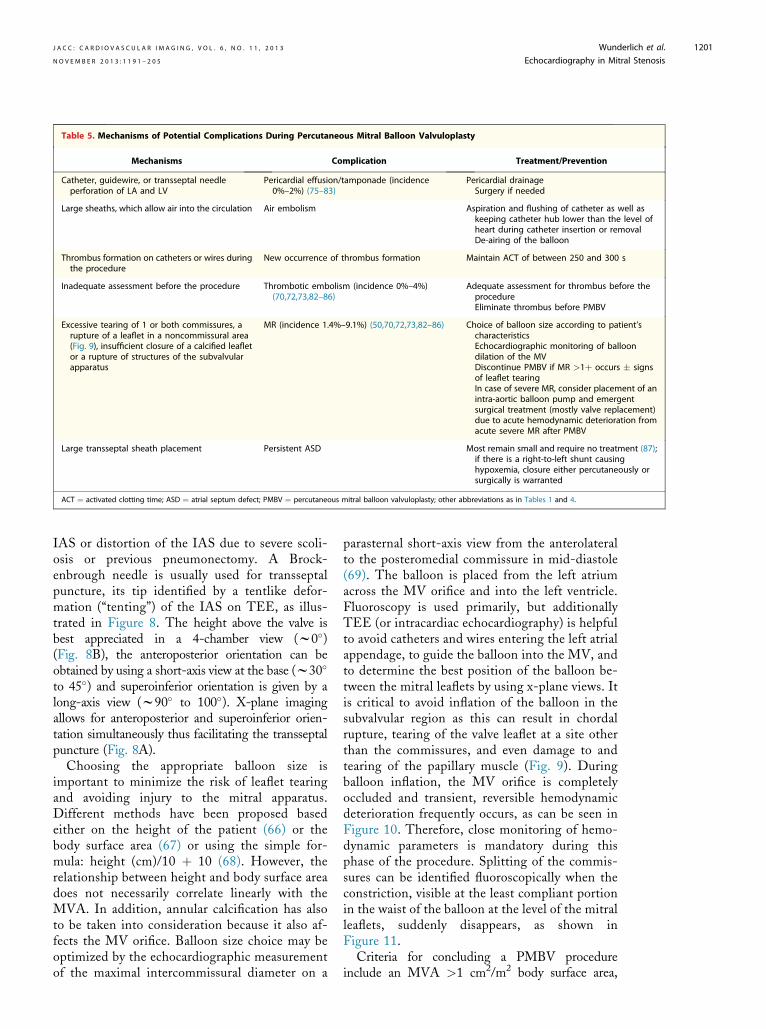
Table 5. Mechanisms of Potential Complications During Percutaneous Mitral Balloon Valvuloplasty
Mechanisms Complication Treatment/Prevention
Catheter, guidewire, or transseptal needleperforation of LA and LV
Pericardial effusion/tamponade (incidence0%–2%) (75–83)
Pericardial drainageSurgery if needed
Large sheaths, which allow air into the circulation Air embolism Aspiration and flushing of catheter as well askeeping catheter hub lower than the level ofheart during catheter insertion or removalDe-airing of the balloon
Thrombus formation on catheters or wires duringthe procedure
New occurrence of thrombus formation Maintain ACT of between 250 and 300 s
Inadequate assessment before the procedure Thrombotic embolism (incidence 0%–4%)(70,72,73,82–86)
Adequate assessment for thrombus before theprocedureEliminate thrombus before PMBV
Excessive tearing of 1 or both commissures, arupture of a leaflet in a noncommissural area(Fig. 9), insufficient closure of a calcified leafletor a rupture of structures of the subvalvularapparatus
MR (incidence 1.4%–9.1%) (50,70,72,73,82–86) Choice of balloon size according to patient’scharacteristicsEchocardiographic monitoring of balloondilation of the MVDiscontinue PMBV if MR >1þ occurs � signsof leaflet tearingIn case of severe MR, consider placement of anintra-aortic balloon pump and emergentsurgical treatment (mostly valve replacement)due to acute hemodynamic deterioration fromacute severe MR after PMBV
Large transseptal sheath placement Persistent ASD Most remain small and require no treatment (87);if there is a right-to-left shunt causinghypoxemia, closure either percutaneously orsurgically is warranted
ACT ¼ activated clotting time; ASD ¼ atrial septum defect; PMBV ¼ percutaneous mitral balloon valvuloplasty; other abbreviations as in Tables 1 and 4.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 6 , N O . 1 1 , 2 0 1 3 Wunderlich et al.
N O V E M B E R 2 0 1 3 : 1 1 9 1 – 2 0 5 Echocardiography in Mitral Stenosis
1201
IAS or distortion of the IAS due to severe scoli-osis or previous pneumonectomy. A Brock-enbrough needle is usually used for transseptalpuncture, its tip identified by a tentlike defor-mation (“tenting”) of the IAS on TEE, as illus-trated in Figure 8. The height above the valve isbest appreciated in a 4-chamber view (w0�)(Fig. 8B), the anteroposterior orientation can beobtained by using a short-axis view at the base (w30�
to 45�) and superoinferior orientation is given by along-axis view (w90� to 100�). X-plane imagingallows for anteroposterior and superoinferior orien-tation simultaneously thus facilitating the transseptalpuncture (Fig. 8A).
Choosing the appropriate balloon size isimportant to minimize the risk of leaflet tearingand avoiding injury to the mitral apparatus.Different methods have been proposed basedeither on the height of the patient (66) or thebody surface area (67) or using the simple for-mula: height (cm)/10 þ 10 (68). However, therelationship between height and body surface areadoes not necessarily correlate linearly with theMVA. In addition, annular calcification has alsoto be taken into consideration because it also af-fects the MV orifice. Balloon size choice may beoptimized by the echocardiographic measurementof the maximal intercommissural diameter on a
parasternal short-axis view from the anterolateralto the posteromedial commissure in mid-diastole(69). The balloon is placed from the left atriumacross the MV orifice and into the left ventricle.Fluoroscopy is used primarily, but additionallyTEE (or intracardiac echocardiography) is helpfulto avoid catheters and wires entering the left atrialappendage, to guide the balloon into the MV, andto determine the best position of the balloon be-tween the mitral leaflets by using x-plane views. Itis critical to avoid inflation of the balloon in thesubvalvular region as this can result in chordalrupture, tearing of the valve leaflet at a site otherthan the commissures, and even damage to andtearing of the papillary muscle (Fig. 9). Duringballoon inflation, the MV orifice is completelyoccluded and transient, reversible hemodynamicdeterioration frequently occurs, as can be seen inFigure 10. Therefore, close monitoring of hemo-dynamic parameters is mandatory during thisphase of the procedure. Splitting of the commis-sures can be identified fluoroscopically when theconstriction, visible at the least compliant portionin the waist of the balloon at the level of the mitralleaflets, suddenly disappears, as shown inFigure 11.
Criteria for concluding a PMBV procedureinclude an MVA >1 cm2/m2 body surface area,

Wunderlich et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 6 , N O . 1 1 , 2 0 1 3
Echocardiography in Mitral Stenosis N O V E M B E R 2 0 1 3 : 1 1 9 1 – 2 0 5
1202
complete commissural opening in at least 1 com-missure, and occurrence of or increase in MR>1þ. Meticulous attention to procedural detailsis important in high-risk patients such as theelderly patients, pregnant patients, and patientswith severe MS, extensive subvalvular involve-ment, nodular commissural calcification as well asin patients in whom the MV opens asymmetrically.According to theAmericanCollege ofCardiology/
American Heart Association guidelines, successfulPMBV is usually defined as an MVA $1.5 cm2
and absence of complications (includingMR> grade2/4) (20).In cases with suboptimal results, balloon inflation
is repeated by increasing the balloon size in 1-mmincrements until a satisfactory MV opening is ach-ieved or a relevant worsening of MR occurs.The prediction of results after PMBV is multi-
factorial and includes a variety of clinical, morpho-logical, and hemodynamic parameters. Table 4provides an overview of predictors of good andpoor immediate and long-term results (70–76).
ASSESSMENT AFTER PMBV. Immediately after bal-loon inflation, left atrial pressure should be obtainedand echocardiography is used to evaluate a post-PMBV MVA using mean Doppler gradients and2D and 3D MV planimetry, reassess commissuralopening, evaluate MV leaflet mobility, determinethe severity and location of MR, and assesscomplications.In the post-procedural evaluation of MVA
planimetry, using real-time 3D echocardiographyhas been shown to be more accurate and to have thebest agreement with invasively determined MVAcompared with conventional 2D planimetry (77). Inaddition, the opening of the commissures is shownmore clearly by real-time 3D echocardiography.
Commissural opening is a significant predictor oflong-term outcome and is associated with a largerMVA, smaller gradients, and better functionaloutcomes (75). After PMBV, the PHT method forMVA assessment should not be used because it isoften inaccurate (36,78) due to the newly createdatrial septal defect in many patients, the changes inhemodynamic variables that influence the mea-surement, and the alteration in the complianceof the left ventricle and left atrium after PMBV.Moreover, there is poor agreement betweenPHT with invasive measurements after PMBV(14,79,80).
COMPLICATIONS DURING PMBV. Complicationsmay occur at any time during the procedure, andtheir detection by echocardiographic monitoring isimportant. Table 5 summarizes potential compli-cations during PMBV, their mechanisms and pre-vention, and treatment options (70,72,73,81–87).
Conclusions
Although the incidence of RF and the prevalence ofrheumatic heart disease is decreasing in industrial-ized countries, a substantial occurrence of rheumaticMV disease exists worldwide, especially in devel-oping countries. PMBV is an important treatmentoption for this condition. Therefore, adequate un-derstanding of the indications, patient selection,PMBV procedures, and assessment of results is ofparamount importance.
Reprint requests and correspondence: Dr. Robert J. Siegel,Cedars-Sinai Medical Center, 127 South San VicenteBoulevard, Los Angeles, California 90048. E-mail: [email protected].
R E F E R E N C E S
1. Wood P. An appreciation of mitralstenosis. I: Clinical features. Br Med J1954;4870:1051.
2. Rowe JC, Bland EF, Sprague HB,White PD. The course of mitral ste-nosis without surgery: ten- andtwenty-year perspectives. Ann InternMed 1960;52:741–9.
3. Iung B, Baron G, Butchart EG,et al. A prospective survey of pa-tients with valvular heart disease inEurope: the Euro Heart Survey onValvular Heart Disease. Eur Heart J2003;24:1231–43.
4. Carapetis JR,SteerAC,MulhollandEK,Weber M. The global burden of groupA streptococcal diseases: a population-based study. Lancet Infect Dis 2005;5:685–94.
5. Marijon E, Ou P, Celermajer DS,et al. Prevalence of rheumatic heartdisease detected by echocardiographicscreening. N Engl J Med 2007;357:470–6.
6. Seckeler MD, Hoke TR. The world-wide epidemiology of acute rheumaticfever and rheumatic heart disease. ClinEpidemiol 2011;3:67–84.
7. Cohn LH. The first successful surgicaltreatment of mitral stenosis: the 70thanniversary of Elliot Cutler’s mitralcommissurotomy. Ann Thorac Surg1993;56:1187–90.
8. Harken DE, Dexter L, Ellis LB, et al.The surgery of mitral stenosis: III:Finger-fracture valvuloplasty. AnnSurg 1951;134:722–42.
9. Inoue K, Owaki T, Nakamura T, et al.Clinical application of transvenousmitral commissurotomy by a newballoon catheter. J Thorac CardiovascSurg 1984;87:394–402.

J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 6 , N O . 1 1 , 2 0 1 3 Wunderlich et al.
N O V E M B E R 2 0 1 3 : 1 1 9 1 – 2 0 5 Echocardiography in Mitral Stenosis
1203
10. Iung B, Cormier B, Ducimetiere P,et al. Immediate results of percutaneousmitral commissurotomy. A predictivemodel on a series of 1514 patients.Circulation 1996;94:2124–30.
11. Palacios IF. Farewell to surgical mitralcommissurotomy for many patients.Circulation 1998;97:223–6.
12. Hung JS, Chern MS, Wu JJ, et al.Short and long-term results of catheterballoon percutaneous transvenousmitral commissurotomy. Am J Cardiol1991;67:854–62.
13. Dean LS, Mickel M, Bonan R, et al.Four-year follow-up of patients un-dergoing percutaneous balloon mitralcommissurotomy: a report from theNational Heart, Lung, and BloodInstitute Balloon Valvuloplasty Reg-istry. J Am Coll Cardiol 1996;28:1452–7.
14. Abascal VM,Wilkins GT, Choong CY,et al. Echocardiographic evaluation ofmitral valve structure and function inpatients followed for at least 6 monthsafter percutaneous balloon mitral valvu-loplasty. J Am Coll Cardiol 1988;12:606–15.
15. Post JR, Feldman T, Isner J, et al.Inoue balloon mitral valvotomy in pa-tients with severe valvular and sub-valvular deformity. J Am Coll Cardiol1995;25:1129–36.
16. Hernandez R, Banuelos C, Alfonso F,et al. Long-term clinical and echocar-diographic follow-up after percuta-neous mitral valvuloplasty with theInoue balloon. Circulation 1999;99:1580–6.
17. Iung BL, Garbarz E, Michaud P, et al.Late results of percutaneous mitralcommissurotomy in a series of 1024patients: analysis of late clinical dete-rioration: frequency, anatomic findingsand predictive factors. Circulation1999;99:3272–8.
18. Chen C-R, Cheng TO, Chen J-Y,et al. Long-term results of percuta-neous balloon mitral valvuloplasty formitral stenosis: a follow-up study to 11years in 202 patients. Cathet Car-diovasc Diagn 1998;43:132–9.
19. Borger MA, Carrel TP, DeBonis M,et al. The Joint Task Force on theManagement of Valvular Heart Dis-ease of the European Society of Car-diology (ESC) and the EuropeanAssociation for Cardio-Thoracic Sur-gery (EACTS). Guidelines on themanagement of valvular heart disease(version 2012). Eur Heart J 2012;33:2451–96.
20. Bonow RO, Carabello BA,Chatterjee K, et al., American Collegeof Cardiology/American Heart Asso-ciation Task Force on PracticeGuidelines. 2008 Focused updateincorporated into the ACC/ACC2006 guidelines for the management
of patients with valvular heart disease.J Am Coll Cardiol 2008;52:e1–142.
21. Vahanian A, Baumgartner H, Bax J,et al. Guidelines on the managementof Valvular Heart Disease of the Eu-ropean Society of Cardiology. EurHeart J 2007;28:230–68.
22. Chiang CW, Lo SK, Ko YS, Cheng NJ,Lin PJ, Chang CH. Predictors of sys-temic embolism in patients with mitralstenosis. A prospective study. Ann InternMed 1998;128:885–9.
23. Olesen KH. The natural history of 271patients with mitral stenosis undermedical treatment. Br Heart J 1962;24:349–57.
24. Selzer A, Cohn KE. Natural history ofmitral stenosis: a review. Circulation1972;45:878–90.
25. Munoz S, Gallardo J, Diaz-Gorrin JR,Medina O. Influence of surgery on thenatural history of rheumatic mitral andaortic valve disease. Am J Cardiol1975;35:234–42.
26. Lang RM, Badano LP, Tsang W,et al. EAE/ASE recommendations forimage acquisition and display usingthree-dimensional echocardiography.J Am Soc Echocardiogr 2012;25:3–46.
27. Baumgartner H, Hung J, Bermejo J,et al. Echocardiographic assessment ofvalve stenosis: EAE/ASE Recom-mendations for Clinical Practice. J AmSoc Echocardiogr 2009;22:1–23.
28. Faletra F, Pezzano A Jr., Fusco R,et al. Measurement of mitral valve areain mitral stenosis: four echocardio-graphic measurements compared withdirect measurements of anatomic ori-fices. J Am Coll Cardiol 1996;28:1190–7.
29. Min SY, Song JM, Kim YJ, et al.Discrepancy between mitral valve areasmeasured by two-dimensional planim-etry and three dimensional trans-esophageal echocardiography inpatients with mitral stenosis. Heart2013;99:253–8.
30. Schlosshan D, Aggarwal G,Mathur G, et al. Real-time 3D trans-esophageal echocardiography for theevaluation of rheumatic mitral valvestenosis. J Am Coll Cardiol 2011;4:580–8.
31. Sugeng L, Weinert L, Lammertin G,et al. Accuracy of mitral valve areameasurements using transthoracicrapid freehand 3-dimensional scan-ning: comparison with noninvasiveand invasive measurements. J Am SocEchocardiogr 2003;16:1292–300.
32. Thomas JD, Weyman AE. Dopplermitral pressure half-time: a clinical toolin search of theoretical justification.J Am Coll Cardiol 1987;10:923–9.
33. GonzalesMA,Child JS, Krivokapich J.Comparison of two-dimensional andDoppler echocardiography and
intracardiac hemodynamics for quanti-fication of mitral stenosis. Am JCardiol1987;60:327–32.
34. Hatle L, Angelsen B, Tromsdal A.Noninvasive assessment of atrioven-tricular pressure half-time by Dopplerultrasound. Circulation 1979;60:1096–104.
35. Nakatani S, Masuyama T, Kodama K,et al. Value and limitations of Dopplerechocardiography in the quantificationof stenotic mitral valve area: compari-son of the pressure half-time and thecontinuity equation methods. Circu-lation 1988;77:78–85.
36. Thomas JD, Wilkins GT,Choong CY, et al. Inaccuracy of mitralpressure half-time immediately afterpercutaneous mitral valvotomy.Dependence on transmitral gradientand left atrial and ventricular compli-ance. Circulation 1988;78:980–93.
37. Flachskampf FA, Weyman AE,Guerrero JL, Thomas JD. Influence oforifice geometry and flow rate oneffective valve area: an in vitro study.J Am Coll Cardiol 1990;15:1173–80.
38. Karp K, Teien D, Bjerle P,Eriksson P. Reassessment of valve areadeterminations in mitral stenosis bythe pressure half-time method: impactof left ventricular stiffness and peakdiastolic pressure difference. J Am CollCardiol 1989;13:594–9.
39. Messika-Zeitoun D, Fung Yiu S,Cormier B, et al. Sequential assess-ment of mitral valve area during dias-tole using color M-mode flowconvergence analysis: new insights inmitral stenosis physiology. Eur Heart J2003;24:1244–53.
40. Nishimura RA, Rihal CS, Tajik AJ,Holmes DR Jr. Accurate measurementof the transmitral gradient in patientswith mitral stenosis: a simultaneouscatheterization and Doppler echocar-diographic study. J Am Coll Cardiol1994;24:152–8.
41. Thomas JD, Newell JB, Choong CY,Weyman AE. Physical and physiologicaldeterminants of transmitral velocity: nu-merical analysis. Am J Physiol 1991;260:H1718–31.
42. Gorlin R, Gorlin SG. Hydraulic for-mula for calculation of the area of thestenotic mitral valve, other cardiacvalves, and central circulatory shunts.Am Heart J 1951;41:1–29.
43. Ward C, Hancock BW. Extremepulmonary hypertension caused bymitral valve disease: natural history andresults of surgery. Br Heart J 1975;37:74–8.
44. Palacios IF, Sanchez PL, Harrell LC,et al. Which patients benefit from percu-taneous mitral balloon valvuloplasty?Prevalvuloplasty and postvalvuloplastyvariables that predict longterm outcome.Circulation 2002;105:1465–71.

Wunderlich et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 6 , N O . 1 1 , 2 0 1 3
Echocardiography in Mitral Stenosis N O V E M B E R 2 0 1 3 : 1 1 9 1 – 2 0 5
1204
45. Lancelotti P, Moura L, Pierard LA,et al. European Association of Echo-cardiography recommendations for theassessment of valvular regurgitation.Part 2: mitral and tricuspid regurgita-tion (native valve disease). Eur JEchocardiogr 2010;11:307–32.
46. Picano E, Pibarot P, Lancelotti P,et al. The emerging role of exercisetesting and stress echocardiography invalvular heart disease. J Am CollCardiol 2009;54:2251–60.
47. Himelman RB, Stulbarg M,Kircher B, et al. Noninvasive evalua-tion of pulmonary artery pressureduring exercise by saline-enhancedDoppler echocardiography in chronicpulmonary disease. Circulation 1989;79:863–71.
48. Tamai J, Nagata S, Akaike M, et al.Improvement in mitral flow dynamicsduring exercise after percutaneoustransvenous mitral commissurotomy:noninvasive evaluation using contin-uous wave Doppler technique. Circu-lation 1990;81:46–51.
49. Leavitt JI, Coats MH, Falk RH. Ef-fects of exercise on transmitral gradientand pulmonary artery pressure in pa-tients with mitral stenosis or a pros-thetic mitral valve: a Dopplerechocardiographic study. J Am CollCardiol 1991;17:1520–6.
50. Cheriex EC, Pieters FA, Janssen JH,et al. Value of exercise Doppler-echocardiography in patients withmitral stenosis. Int J Cardiol 1994;45:219–26.
51. Roberts WC, Perloff JK. Mitralvalvular disease: a clinicopathologicsurvey of the conditions causing themitral valve to function abnormally.Ann Intern Med 1972;77:939–75.
52. Henry WL, Griffith JM, Michaelis LL,et al.Measurement of mitral orifice areain patients with mitral valve disease byreal-time, two-dimensional echocardi-ography. Circulation 1975;51:827–31.
53. Nichol PM, Gilbert BW, Kisslo JA.Two-dimensional echocardiographicassessment of mitral stenosis. Circu-lation 1977;55:120–8.
54. Martin RP, Rakowski H, Kleiman JH,et al. Reliability and reproducibility oftwo dimensional echocardiographmeasurement of the stenotic mitralvalve orifice area. Am J Cardiol 1979;43:560–8.
55. Chen CG, Wang X, Wang Y,Lan YF. Value of two-dimensionalechocardiography in selecting patientsand balloon sizes for percutaneousballoon mitral valvuloplasty. J Am CollCardiol 1989;14:1651–8.
56. Reid CL, Chandraratna PA,Kawanishi DT, Kotlewski A,Rahimtoola SH. Influence of mitralvalve morphology on double-ballooncatheter balloon valvuloplasty in
patients with mitral stenosis. Analysisof factors predicting immediate and3-month results. Circulation 1989;80:515–24.
57. Nobuyoshi M, Hamasaki N,Kimura T, et al. Indications, compli-cations, and short-term clinicaloutcome of percutaneous transvenousmitral commissurotomy. Circulation1989;80:782–92.
58. Wilkins GT, Weyman AE,Abascal VM, et al. Percutaneousballoon dilatation of the mitral valve:an analysis of echocardiographic vari-ables related to outcome and themechanism of dilatation. Br Heart J1988;60:299–308.
59. Cannan CR, Nishimura RA,Reeder GS, et al. Echocardiographicassessment of commissural calcium: asimple predictor of outcome afterpercutaneous mitral balloon valvotomy.J Am Coll Cardiol 1997;29:175–80.
60. Sutaria N, Northridge DB,Shaw TRD. Significance of commis-sural calcification on outcome of mitralballoon valvotomy. Heart 2000;84:398–402.
61. Padial LR, Freitas N, Sagie A, et al.Echocardiography can predict whichpatients will develop severe mitralregurgitation after percutaneous mitralvalvotomy. J Am Coll Cardiol 1996;27:1225–31.
62. Iung B, Cormier B, Ducimetiere P,et al. Functional results 5 years aftersuccessful percutaneous mitral com-missurotomy in a series of 528 patientsand analysis of predictive factors. J AmColl Cardiol 1996;27:407–14.
63. Anwar AM, Attia WM, Nosir YF,et al. Validation of a new score for theassessment of mitral stenosis usingreal-time three-dimensional echocar-diography. J Am Soc Echocardiogr2010;23:13–22.
64. Rao AS, Murthy RS, Naidu PB, et al.Transesophageal echocardiography forthe detection of left atrial thrombus.Indian Heart J 1994;46:37–40.
65. Hung J-S. Mitral stenosis with leftatrial thrombi: Inoue balloon cathetertechnique. In: Cheng TO, editor.Percutaneous Balloon Valvuloplasty.New York, NY: Igaku-Shoin, 1992:280–93.
66. Lau KW, Gao W, Ding ZP, Hung JS.Immediate and long-term results ofpercutaneous Inoue balloon mitralcommissurotomy with use of a simpleheight-derived balloon sizing methodfor the stepwise dilatation technique.Mayo Clin Proc 1996;71:556–63.
67. Hernandez R, Macaya C, Banuelos C,et al. Predictors, mechanisms andoutcome of severe mitral regurgitationcomplicating percutaneous mitral val-vulotomy with the Inoue balloon. AmJ Cardiol 1992;70:1169–74.
68. Lau KW, Hung JS. A simple balloon-sizing method in Inoue-balloonpercutaneous transvenous mitral com-missurotomy. Cathet CardiovascDiagn 1994;33:120–9.
69. Sanati HR, Zahemehr A, Shakerian F,et al. Percutaneous mitral valvuloplastyusing echocardiographic inter-commissural diameter as reference forballoon sizing: a randomizedcontrolled trial. Clin Cardiol 2012;35:749–54.
70. Meneveau N, Schiele F, Seronde MF,et al. Predictors of event free survivalafter percutaneous mitral commissur-otomy. Heart 1998;80:359–64.
71. Zhang HP, Yen GS, Allen JW, et al.Comparison of late results of balloonvalvotomy in mitral stenosis withversus without mitral regurgitation.Am J Cardiol 1998;81:51–5.
72. Ben-Farhat M, Betbout F, Gamra H,et al. Predictors of long-term eventfree survival and of freedom fromrestenosis after percutaneous balloonmitral commissurotomy. Am Heart J2001;142:1072–9.
73. Fawzy ME, Shoukri M, Al Buraiki J,et al. Seventeen years’ clinical echo-cardiographic follow-up of mitralballoon valvuloplasty in 520 patients,and predictors of long-term outcome.J Heart Valve Dis 2007;16:454–60.
74. Pan M, Medina A, Suarez de Lezo J,et al. Factors determining late successafter mitral balloon valvulotomy. Am JCardiol 1993;71:1181–5.
75. Messika-Zeitoun D, Blanc J, Iung B,et al. Impact of degree of commissuralopening after percutaneous mitralcommissurotomy on long-termoutcome. J Am Coll Cardiol Img2009;2:1–7.
76. Jorge E, Baptista R, Faria H, et al.Mean pulmonary arterial pressure afterpercutaneous mitral valvuloplasty pre-dicts long-term adverse outcomes. RevPort Cardiol 2012;31:19–25.
77. Zamorano J, Perez de Isal L, Sugeng L,et al. Non-invasive assessment of mitralvalve area during percutaneous balloonmitral valvuloplasty: role of real-time3D echocardiography. Eur Heart J2004;25:2086–91.
78. Otto CM, Davis KB, Holmes DR, et al.Methodologic issues in clinical evaluationof stenosis severity in adults undergoingaortic ormitral balloon valvuloplasty. AmJ Cardiol 1992;69:1607–16.
79. Reid CL, Rahimtoola SH. The role ofechocardiography/Doppler in catheterballoon treatment of adults with aorticand mitral stenosis. Circulation 1991;84:240–9.
80. Vahanian A, Michel PL, Cormier B,et al. Results of percutaneous mitralcommissurotomy in 200 patients. AmJ Cardiol 1989;63:847–52.

J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 6 , N O . 1 1 , 2 0 1 3 Wunderlich et al.
N O V E M B E R 2 0 1 3 : 1 1 9 1 – 2 0 5 Echocardiography in Mitral Stenosis
1205
81. Martinez-Rios MA, Tovar S, Luna J,Eid-Lidt G. Percutaneous mitralcommissurotomy. Cardiol Rev 1999;7:108–16.
82. Chen CR, Cheng TO. Percutaneousballoon mitral valvuloplasty by theInoue technique: a multicenter studyof 4832 patients in China. Am Heart J1995;129:1197–203.
83. Arora R, Kalra GS, Singh S, et al.Percutaneous transvenous mitral com-missurotomy: immediate and long-termfollow-up results. Catheter CardiovascInterv 2002;55:450–6.
84. Iung B, Nicoud-Houel A, Fondard O,et al. Temporal trends in percutaneous
mitral commissurotomy over a15-year period. Eur Heart J 2004;25:701–7.
85. Neumayer U, Schmidt HK,Fassbender D, et al. Early (threemonth) results of percutaneous mitralvalvuloplasty with the Inoue balloon in1123 consecutive patients comparingvarious age groups. Am J Cardiol2002;90:190–3.
86. Jneid H, Cruz-Gonzalez I, Sanchez-Ledesma M, et al. Impact of pre- andpostprocedural mitral regurgitation onoutcomes after percutaneous mitralvalvuloplasty for mitral stenosis. Am JCardiol 2009;104:1122–7.
87. Cequier A, Bonan R, Serra A, et al.Left-to-right atrial shunting afterpercutaneous mitral valvuloplasty.Incidence and long-term hemody-namic follow-up. Circulation 1990;81:1190–7.
Key Words:echocardiography - mitralstenosis - percutaneousintervention - percutaneousmitral balloon valvuloplasty -
rheumatic heart disease.
To participate in this CME activity by taking the quiz
and claiming your CME credit certificate, please goto
www.imaging.onlinejacc.organd select the CME tab on the top navigation bar.