Management of Impacted Canine Final / orthodontic courses by Indian dental academy
171
www.indiandentalacademy.com
-
Upload
indian-dental-academy -
Category
Documents
-
view
217 -
download
1
Transcript of Management of Impacted Canine Final / orthodontic courses by Indian dental academy

www.indiandentalacademy.com

INDIAN DENTAL ACADEMY
Leader in continuing dental education www.indiandentalacademy.com
www.indiandentalacademy.com

www.indiandentalacademy.com

contents
Introducton
Etiology
Frequency of impactions
Diagnosis
Treatment strategies
Impactions of incisors
Impaction of canines
Impactions of premolars
Impactions of molars
Conclusion
References.www.indiandentalacademy.com

INTRODUCTION The treatment of impacted teeth has caught the
imagination of many in dental profession. However, the
orthodontic / surgical modality has achieved the most
satisfactory result in long-term.
According to Shafer, Hine and Levy,Impacted teeth are
those which are prevented from erupting by some
physical barrier in the eruption path.
www.indiandentalacademy.com

A tooth which is completely or partially unerupted & is positioned against another tooth , bone or soft tissue, so that its further eruption is unlikely, described according to its anatomic position.
www.indiandentalacademy.com

CAUSES OF IMPACTIONS
-Local causes-Systemic causes
www.indiandentalacademy.com

Local causes Irregularity in the position and pressure of an
adjacent tooth. Density of overlying or surrounding bone. Long continued chronic inflammation with
resultant increase in the density of mucous membrane.
Lack of space due to underdeveloped jaws.
www.indiandentalacademy.com

Unduly long retention of primary teeth. Premature loss of primary teeth. Acquired diseases , such as necrosis due to
infection or abscesses. Inflammatory changes in the bone due to
exanthematous diseases.
www.indiandentalacademy.com

Systemic causes
PRE – NATAL - Heredity. POST – NATAL - Rickets. - Anemia. - Congenital Syphillis. - Tuberculosis. - Endocrine dysfunction. - Malnutrition.
www.indiandentalacademy.com

RARE CONDITIONS - Cleidocranial Dysplasia. - oxycephaly. - Progeria. - Achondroplasia. - Cleft palate.
www.indiandentalacademy.com

Normal eruption
www.indiandentalacademy.com

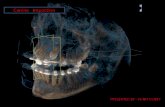
33rdrd molar impaction molar impaction
www.indiandentalacademy.com

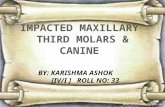
Canine impactionCanine impaction
www.indiandentalacademy.com

Premolar impactionPremolar impactionwww.indiandentalacademy.com

Mandibular 3rd molar. Maxillary 3rd molar. Maxillary canine. Mandibular bicuspid. Mandibular cuspid. Maxillary bicuspid. Maxillary central incisor. Maxillary lateral incisor.
FREQUENCY OF IMPACTION
www.indiandentalacademy.com

CLINICAL RADIOGRAPHIC
www.indiandentalacademy.com

CLINICAL METHOD FOR DIAGNOSISo Examination to assess facial form, arch form and symmetry.
o Relationship of maxillary dental midline to facial midline.
o CR and CO position should be carefully recorded.
o Overjet and Overbite should be carefully recorded.
o Delayed eruption of permanent teeth.
o Prolonged retention of deciduous teeth.
o Absence of normal labial canine bulge.
o Presence of palatal bulge (Abnormal).
o Delayed eruption, distal tipping or migration of lateral incisor.www.indiandentalacademy.com

RADIOGRAPHIC METHOD FOR DIAGNOSIS
In Orthodontic treatment planning, the exact localization of the position of an impacted teeth is necessary.
Periapical
Mandibular arch
Max. ant. occlusal True vertex/occlusal
OPG Lateral ceph
Extraoral
I. Qualitative radiographs
Maxillary arch Occlusal
PA view
www.indiandentalacademy.com

Parallax method
Radiographic views at right angle
II. 3-D diagnosis of the position
C T scanning
www.indiandentalacademy.com

PERIAPICAL RADIOGRAPH
www.indiandentalacademy.com

Periapical Radiography-
• Are the simplest and the most informative X-ray films.
• As this view passes through minimum of surrounding
tissues, it gives accuracy & quality of resolution.
• It is aimed to be perpendicular to an imaginary plane
bisecting the angle between the long axis of an erupted
tooth and the film plane to produce minimum distortion.www.indiandentalacademy.com

The periapical film gives the following information:
[1] Presence or absence of impacted tooth.
[2] Stage of development.
[3] Presence & size of follicle.
[4] Indicates crown or root resorption, resorption pattern
& integrity.
[5] Indicates presence or absence of supernumerary tooth.
[6] Indicates soft tissue lesions like cysts.www.indiandentalacademy.com

OCCLUSAL RADIOGRAPH
www.indiandentalacademy.com

Occlusal Radiography:
Mandibular arch:
• In mandibular arch occlusal view is taken by tipping the
patient’s head backwards & pointing the X-ray tube at
right angle to the film in the occlusal plane.
• In the canine or premolar region, this is a true oclusal
view.www.indiandentalacademy.com

• To get a true occlusal view in the anterior region, the
head is tipped back further & X-ray tube is angled at
110% to the horizontal plane at symphysis menti along
the long axis of the incisor teeth.
www.indiandentalacademy.com

Maxillary arch
1.Maxillary anterior occlusal
• In the maxillary arch, the nose and forehead interfere with
the positioning of x-ray tube close to the area to be viewed.
• The best that can be achieved by positioning the tube
close to the face,so that it becomes high and steeply angled
view. www.indiandentalacademy.com

2. Ture vertex / occlusal
• A true vertex view is one which passes parallel to the long
axis of central incisors.This is possible if the cone is placed
over the vertex of the skull to produce vertex occlusal film.
• Since the beam has to travel a great distance there is loss of
clarity. www.indiandentalacademy.com

Extraoral Radiography:
• OPG has the advantage of simplicity & quickly
offering a good scan of the teeth & jaws from
Temporomandibular joint to Temporomandibular joint. www.indiandentalacademy.com

Parallax method:
By Clark & Richards
Principle:
• 2 periapical views of the same object are taken from
slightly different angles which can provide depth to
the flat 2-D picture depicted by each of the films
individually.
• Useful in distinguishing the buccal or lingual
displacement of the canine.www.indiandentalacademy.com

Procedure:
1. In the periapical film, the X-ray is taken in the area
of interest with the X-ray beam passing perpendicular
to a tangent to the line of arch at this point & at an
appropriate angle to horizontal plane.www.indiandentalacademy.com

2. In the second film, the X-ray tube is shifted mesially or
distally round the arch but held at the same angle to the
horizontal plane. The X-ray tube should describe between
30-450 of an arc of circle whose centre is somewhere in
the middle of the palate.www.indiandentalacademy.com

Result:
• It is based on the SLOB principle.
• If the object has moved on the same side as that
of the X-ray tube it is lingually placed & if it has
moved on the opposite side it is on the buccal side
www.indiandentalacademy.com

Radiographic views at right angles:
1. A true lateral view {e.g. Lateral
cephalograph} gives information
regarding the antero-posterior &
ventral location of an object . However,
it gives no information regarding
bucco-lingual {transverse} plane of an
object.www.indiandentalacademy.com

2. A true occlusal view will provide information in the
transverse & antero-posterior direction of an object .
www.indiandentalacademy.com

3. True postero-anterior view defines
the ventral plane & buccolingual
relationship of an object.
These views provide complete information regarding
3 planes of space of any impacted teeth .
www.indiandentalacademy.com

CT Scanning: By Ericson & Kurol
• Used to diagnose the exact
position of an impacted
tooth.
• Clear serial radiographs
may be taken at graduated
depth in any part of human
body in this method.www.indiandentalacademy.com

• This technique allows the
elimination of superimposition of
other structures.
• It is however rarely used in the
diagnosis of impacted teeth because
of
( 1) Large radiation dosage.
(2) High cost. www.indiandentalacademy.com

Rapid prototypingLimitations of CT Scan However even the 3D reconstruction is
obtained , the analysis by the orthodontist is still limited : 3D images are seen as 2 dimensional on film and computer screen.
This can be overcome with the use CT to make a model by means of rapid prototyping
This technique use data from computer aided design to produce physical models and devices by material addition .
www.indiandentalacademy.com

www.indiandentalacademy.com

Labial tooth impaction -
1% to 2% of orthodontic patients and is often difficult to manage. The most common methods of uncovering labial impactions
Excisional gingivectomy Apically positioned flap techniques. closed-eruption technique.
The esthetic and functional outcomes of these procedures, such as effects on gingival height, clinical crown length, width of attached gingiva, gingival scarring, relapse potential, and attachment levels need to be critically assessed in order to identify the optimal method of uncovering labial impactions.
www.indiandentalacademy.com

Vanarsdall and Corn evaluated more than 75 labially impacted teeth which had been uncovered using a split-thickness apically positioned flap. The authors found no marginal bone loss or gingival recession after orthodontic treatment.
They stressed the need to provide attached gingiva in order to prevent the muscles of the face from detaching the marginal periodontal tissue from the tooth, causing marginal bone loss and gingival recession.
The closed-eruption technique is believed by some to be the best method of uncovering labially impacted teeth, especially if the tooth is located high above the mucogingival junction or deep in the alveolus
www.indiandentalacademy.com

TYPES OF FLAPS FOR IMPACTED CANINE
• Exposure only
• Exposure with pack
Buccally accessible impacted teeth
• A circular incision
www.indiandentalacademy.com

• Apically repositioned surgical flap .Full flap closure
1.) Labially impacted maxillary anterior teeth uncovered with an apically positioned flap technique have more unesthetic sequalae than those uncovered with a closed-eruption technique.
2 )Negative esthetic effects, such as increased clinical crown length, increased width of attached tissue, gingival scarring, and intrusive relapse were evident in the teeth treated with an apically positioned flap.www.indiandentalacademy.com

Palatal Impaction
• Partial
• Full flap closure
www.indiandentalacademy.com

Anchor unit
• When dealing with a malocclusion that incorporates
an impacted tooth, modification must be made for anchor
unit.
• A fully multi-bracketed appliance should normally be
placed & the entire dentition treated through the stages of
leveling & opening of adequate space in the arch for impacted
tooth.
www.indiandentalacademy.com

• A heavy & more rigid arch wire is then placed into
the brackets on all the teeth of aligned & complete
dental arch, the aim is to provide solid anchor base that
will not allow distortion of arch wire to occur as a
result of force that will be applied to the impacted
tooth after exposure.
www.indiandentalacademy.com

Attachments: –
Lasso wires
Threaded pins
Orthodontic bands
Standard orthodontic bracket
A simple eyelet
Elastic ties and modules
Magnets
www.indiandentalacademy.com

{a} Lasso wires:
It is twisted lightly around the neck of the canine.
Disadvantages: This results in irritation of the gingiva Prevents reattachments of the healing tissues in area of CEJ (cemento-enamel junction). May produce areas of external resorption & ankylosis in areas of CEJ.
So, it is rarely used now. www.indiandentalacademy.com

(b) Threaded Pins:
Provide the attachment for
an impacted tooth.
Disadvantages:
- Dentaly invasive.
- Requires a subsequent restoration.
- Difficult to place along the long axis of the tooth because of smaller surgical exposure.
- The drilled hole may inadvertently enter the pulp(unerupted teeth may have large pulp chambers).
So it is rarely used. www.indiandentalacademy.com

{c} Orthodontic bands:
They largely replace the
Lasso wires & threaded pins.
Advantage:
They are compatible with the health of periodontal tissues.
Disadvantage:
- Large surgical field required.
- Inadequate moisture control may hamper with the cement-band bond.
www.indiandentalacademy.com

{d}Standard orthodontic brackets:
Any edge-wise , Begg’s , PAE brackets can be used.
They are routinely used as direct attachments along with the composites.
www.indiandentalacademy.com

Disadvantages:
- As the bracket base is wide, it is difficult to adapt to
any other tooth surface except for the buccal surface.
- The bracket’s shear bulk creates irritation as the tooth
is drawn the soft tissues.
- Ligature wire or elastic thread tied to bring the
impacted tooth into arch.
www.indiandentalacademy.com

- Interferes with the investing tissues & leads to
inflammation & periodontal damage.
- As the impacted tooth advances into the arch
the exuberant gingival tissues bunches in front of it &
causes punching between the bracket & tissues.
www.indiandentalacademy.com

{e} A simple eyelet:
Advantages:
- An eyelet welded to band material with a mesh backing is
soft & easy to contour making its adaptation to bonding surface
more accurate which makes for superior retentive properties.
- Because of small size they can be placed in more awkwardly placed teeth.
- It is less irritating to the surrounding tissues. www.indiandentalacademy.com

(f) Elastic ties and modules
Advantages
- Application of light forces
- Good range of action
- Easier to tie
Disadvantages
- Tends to loosen
- High degree of force decay
www.indiandentalacademy.com

{f} Magnets:
It is made up of rare earth lanthanide alloys .
• It is rarely used.
Disadvantage:
- corrosion.
www.indiandentalacademy.com

Maxillary incisors impaction
The spectre of appearance of lateral incisors ,associated with non – appearance of one or both of central incisors ,should always deemed as abnormal ,whether or not a deciduous central incisor is still present .
www.indiandentalacademy.com

AetiologyObstructive causes supernumerary teeth Odontome Ectopoc position of tooth bud
Traumatic causesObstruction due to soft tissue repairDilacerationArrested root developmentAcute traumatic intrusion
www.indiandentalacademy.com

Treatment timing Obstructions should be removed early
before it causes delayed eruption.
Clinically – when both laterel incisors are erupted
Radio graphically – IOPA show atleast 2/3 rd of its root , the developmental landmark that tooth should be erupted .
Orthodontic and surgical intervention is indicated at this time.
www.indiandentalacademy.com

Attitudes of treatment Adequate space is created Obstructions are removed
1. Eruption - Battagel 1985, Houston 1986, mitchell and bennet 1992
2. Noneruption - Dibase 1971, Witsenburg 1981
3. Delayed eruption – 16 -20 months for eruption this is an unacceptable long period of time, 2 surgical episodes may be needed
Mitchell and Bennet 1992, Bodenham 1967.4.Alignment – Gardiner 1961 spontaneous
alignment occurs only minority of patients
www.indiandentalacademy.com

Treatment
1) An orthodontic appliance for the use in the early mixed dentition.
2) two by four appliance
3) Johnson’s twin - wire arch
www.indiandentalacademy.com

Prognosis1.Root length 2. Type and height of periodontal ligament – window created over the impacted canine over
attatched gingiva – poor prognosis full flap surgery – good prognosis
3. Relative height of the crestal alveolus – vertical movement of tooth is accompanied by
vertical increase in the alveolar bone When the impaction is resolved by natural
eruptive force - bone support is good when the excess extrusive forces – tooth will
erupt rapidlly without regeneration of alveolar bone
www.indiandentalacademy.com

4.preservation of vitality5.oral hygiene
www.indiandentalacademy.com

IMPACTION DUE TO TRAUMA
SOFT TISSUE OBSTRUCTION
Andreason and Andreason 1994
Removing of the fibrous mucosal covering or incising and resuturing it to leave the incisal edge exposed will generally lead to a fairly rapid eruption
www.indiandentalacademy.com

The dilacerated central incisor and arrested root development
long term prognosis of these teeth is poor and their extraction and replacement is a part of long term treatment strategy.
But it is always advisable to disimpact these teeth into arch for timely purpose and replace it later with prothesis depending upon its prognosis for following reasons.
www.indiandentalacademy.com

A permanent artificial solution can not considered in early childhoodFollowing extraction of the dilacerated teeth ,alveolar ridge is deficient ridge vertically and labio-lingually making the case unsuitable for an implantRetention of the short rooted and endodontically treated teeth will preserve the normal shape and architecture of alveolar ridge
www.indiandentalacademy.com

Apical root dilacerationThe more apical the dilaceration of root the better is the
prognosis.
Surgically expose
Attach an eyelet and a ligature is treaded to the eyelet and drawn towards the main arch wire
As crown moves down the root rotates labially towards the labial plate.
If the root is prominent and still more labial root movement is desirable - amputation of the labially projected part of the root and endodontic treatment is carried on
The prognosis is dependent on amount of root remaining after amputation.
www.indiandentalacademy.com

Crown dilacerationIf the dilaceration is in the crown of the
tooth , prognosis improves the closer it is to the incisal edge
When the crown is surgically exposed , an attatchment is placed on the labial surface . In this way a continued downwards directed orhtodontic traction will bring the root portion of the tooth from more palatal position to its normal position ,this is due to lingual tipping effect
www.indiandentalacademy.com

The tooth will erupt with the incisal edge of the teeth more labially and post traumatic section in an acceptable position.
Retoration of the teeth indicated after grinding off the portion of the crown developed before pre trauma.
www.indiandentalacademy.com

Dilaceration of the crown near the CEJ junction , the progosis of aligned tooth is extremely poor
Since most of the root portion developed after post trauma period , will need to be amputated , leaving the tooth with a non –vaible coronal remanent of the teeth
www.indiandentalacademy.com

Treatment options1) Open up the space Dilacerated tooth is exposed Condition is evaluated – hopeless – extraction not hopeless – ampute the root portion , crown
pulp chamber is cleaned and filled with composite and used as space maintainer by bonding to the adj teeth
2) Crown is removed, immediate root filling is placed and treaded post is attatched and to this post a ligature wire is attatched and the prepared tooth is erupted in to the moth till the post becomes apparent at the gingival level and later a artificial crown is given.
www.indiandentalacademy.com

Acute traumatic intrusive luxation
Shapira in 1986 - following traumatic intrusive luxation tooth may erupt spontaneously and eventually erupt into its original position
in some cases orthodontic intervention may be required
www.indiandentalacademy.com

Individual tooth distraction Miniature tooth-borne distractor
www.indiandentalacademy.com

www.indiandentalacademy.com

www.indiandentalacademy.com

Canine impactions
www.indiandentalacademy.com

ERUPTION OF CANINE
• Dewel (1949) stated that “no tooth is more interesting
from the development point of view than the maxillary
canine”
• Canine develops in deepest area of maxilla, has
longest path of eruption, travels 22mm during its
course or eruption and has longest period of
development.www.indiandentalacademy.com

Reason for canine Impaction
Becker Concepts : Becker (1984) hypothesized two processes in the palatal impaction of the maxillary canine: I) Absence of initial early guidance from an anomalous lateral incisor. II) Failure of buccal movement of the canine at an unspecified age .
MC Bridge Concept Canine formed at high in the anterior wall at antrum, below the floor of orbit, long tortous path of eruption.
www.indiandentalacademy.com

Moyers Concept: Summarized by Bishara A)Primary cause: 1) Trauma to decidious tooth bud 2) Rate of Resorption of decidious tooth 3) Availability of space in the arch 4) Disturbance in tooth Eruption Sequence 5) Rotation of tooth buds 6) Canine Erupt in Cleft area in Person with Cleft 7) Premature root Closure B)Secondary cause: 1) Abnormal muscle pressure 2) Febrile diseases 3) Endocrine disturbances 4) Vitamin D deficency.
www.indiandentalacademy.com

Berger Concept :{Systemic cause of impaction} 1) Malnutrition 2) Tuberculosis 3) Syphilis 4) Rickets 5) Anemia 6) Progeria 7) Syndromes: a) Cleidocranial dysplasia b) Achondraplasia c) Down syndrome
www.indiandentalacademy.com

Vonder Heydt Concept Total arch length of permanent teeth is initially established very early in life at the time of eruption of first permanent molars. Canine is larger and later erupting and considering like a musical chair situation it may get impacted.
Guidance Theory - Miller Normal Eruption: Canine usually have a more mesial development path,which is guided downwards apparently along the distal aspect of the lateral incisor roots.
www.indiandentalacademy.com

Peck and Peck Concept:
1) Occurrence of other dental anomalies: Palatally impacted canine is an inherited trait occurs in combination with tooth agenesis,tooth size reduction,supernumery tooth and other ectopically positioned tooth. 2) Bilaterally occuring Phenomenon (17%) 3) Females affected more than males (1:3.2) 4) Familial occurence So they concluded palatally impacted canine as dental anomaly as GENETIC ORIGIN.
www.indiandentalacademy.com

INCIDENCE OF CANINE IMPACTION
• Dachi and Howell (1961) incidence of maxillary and mandibular canine impaction - 0.92% and 0.35% resp.
•Johnston et al (1982) – greater incidence of palatal impaction than the labial
• Of all patients with maxillary impacted canines, 8% have bilateral impactions.
www.indiandentalacademy.com

CLASSIFICATION OF IMPACTED CANINE
Impacted canine
Maxillary canine Mandibular canine
Buccal Palatal LingualBuccal
www.indiandentalacademy.com

Classification of palatally impacted canine The classification is based on two variables:
(1) Transverse relationship of the crown of the tooth to the line of dental arch which may be (a) Close (b) Distant ( nearer the midline)
(2) Height of the crown of the teeth in relation to the occlusal plane which may be (a) High (b) Low www.indiandentalacademy.com

Group 1 - Proximity to the line of arch – close.
- Position in the maxilla – low.
Group 2 - Proximity to the line of arch – close.
Position in the maxilla – forward , low &
mesial to the lateral incisor root.
www.indiandentalacademy.com

Group 3 - Proximity to the line of arch – close. - Position in the maxilla – high.
Group 4 - Proximity to the line of arch – distant. - Position in the maxilla – high.
www.indiandentalacademy.com

Group 5 - canine root apex
mesial to that of lateral incisor or
distal to that of first premolar.
Group 6 - Erupting in the line of
arch in place and resorbing the
roots of incisors.
www.indiandentalacademy.com

TREATMENT ALTERNATIVES
1. No treatment, if the patient does not desire it. Since the
long term prognosis of deciduous canine is poor as its root
may eventually resorb , it should be periodically evaluated.
2. Auto transplantation of the canine.
3. Extraction of impacted canine and moving premolar in its position.
4. Extraction of the canine & posterior segmental
osteotomy to move the buccal segment mesially to close the
residual space. www.indiandentalacademy.com

5. Prosthetic replacement of the canine, not amendable
for juvenile cases.
6. Most desirable approach is surgical exposure of the
canine followed by orthodontic treatment .
www.indiandentalacademy.com

PALATAL VERSES LABIAL IMPACTIONS
• Incidence - Palatal : Labial is 2:1 or 3:1.
• Ectopic labially positioned canines may erupt on their own without surgical exposure.
• Palatally impacted canine seldom erupt without surgical
intervention due to thick palatal cortical bone & dense &
resistant palatal mucosa.
• Palatally impacted canines are more often inclined in a horizontal / oblique direction .
• Labial impactions are more often vertically inclined. www.indiandentalacademy.com

FORCE GENERATING DEVICES
Various methods have been used for moving the canine in to
proper alignment with following considerations:
• Creation of sufficient space.
• Maintenance of the space.
• Arch wire of sufficient stiffness.
•The use of light force (not more than 60 gms).
www.indiandentalacademy.com

TMA BOX LOOP
• TMA .017 X .025 wire used.
• Produce sagittal and horizontal corrections while continuing vertical eruption.
Surendra Patel J C O 1999www.indiandentalacademy.com

NICKEL TITANIUM CLOSED-COIL SPRING
Loring L.Ross (1999)
• 0.009”X 0.041” spring
• Provides 80 gm of force when stretched to twice its resting length
JCO Feb 1999www.indiandentalacademy.com

Procedure
JCO Feb 1999www.indiandentalacademy.com

CANTILEVER SPRING
• Lindauer and Isaacson (1995)
• TMA .017 X .025 wire used
• Force generated was measured
by dontrix guage.
• It should not exceed 70gms.
JCO Feb 1999www.indiandentalacademy.com

THE MONKEY HOOK
S.Jay Bowman (2002)
• It is a simple auxiliary with an open loop on each
end for the attachment of intra oral elastic or
elastomeric chain or for connecting to a bondable
loop button. JCO July 2002www.indiandentalacademy.com

A combination of monkey hooks and bondable loop-buttons
I. Vertical intermaxillay eruptive forces
JCO July 2002www.indiandentalacademy.com

II. Lateral directional forces
JCO July 2002www.indiandentalacademy.com

AUSTRALIAN HELICAL ARCHWIRE
• Christine Hauser (2000)
• Made in special plus .016” arch wire
• Force should not exceed 200 gm
• Activation by twisting the steel ligature wire every two weeks
JCO Sep 2000www.indiandentalacademy.com

Palatally impacted canine: When crown of canine is more palatally displaced,surgery on the buccal side needs to become more radical,rendering a palatal; approach preferable. Usually palatally impacted tooth is guided to occlusion in two stages.
I) Guiding tooth to oral enviroment II) Guiding tooth to line of arch
www.indiandentalacademy.com

Guiding tooth to oral enviroment
I) Active palatal arch (Becker1978)
It consist of fine 0.020 inch removable palatal arch wire carrying an omega loop on each side. End of the wire is doubled for Frictionless fit in lingual sheath.It is activated by elevating downward activated palatal arch wire and hooking the pigtail ligature around it
www.indiandentalacademy.com

2) Ballista Spring (Jacoby 1979)
It is made of rectangular wires. It proceeds forward untill it is opposite to canine space and bent vertically downwards and terminate into a small loop.With slight finger pressure ,spring is tied to pigtail ligature. By this it provide an extrusive force for the canine to erupt.
www.indiandentalacademy.com

3) Light Auxiliary Labial Arch (Kornhauser1996)
It is made up of 0.014 inch round SS wire with vertical loops in the area of impacted canine on both sides.This loop has a small helix.This wire is tied with the basal arch wire in piggyback fashion.If basal arch wire is not used it will leads to extrusion of adjacent tooth and cause alteration of occlusal plane .
www.indiandentalacademy.com

THE K- 9 SPRING
•Varun Kalra (2000)
• Made in 0.017”X 0.025”TMA wire
Adv:
• Simple in design
• Low cost
• No patient compliance
• Light continuous eruptive and distalizing forces
JCO Oct 2000www.indiandentalacademy.com

Fabrication and Activation
JCO Oct 2000 www.indiandentalacademy.com

JCO Oct 2000 www.indiandentalacademy.com

JCO Oct 2000www.indiandentalacademy.com

JCO Oct 2000 www.indiandentalacademy.com

MANDIBULAR ACHORAGE
• Pramod K.Sinha (1999)
• Lingual arch is fabricated with 0.036 inch SS wire
• Vertical hooks (5-6mm in length)
• Elastic force should not exceed 40-60 gm AJO March 1999www.indiandentalacademy.com

Advantages
• Simplicity in appliance
design and application
• Reduced overall treatment
time
AJO March 1999www.indiandentalacademy.com

MAGNETS
• M.Ali Darendeliler (1994)
• Samarium cobalt magnet coated
with thermoplastic material
(Eurcodur).
• Initial force of attraction is 10gmJCO 1994www.indiandentalacademy.com

Procedure
JCO 1994
www.indiandentalacademy.com

Tunnel traction of infraosseous impacted canines
A.crescini et al(1994)
Adv:• No attachment loss
• No recession
AJO 1994www.indiandentalacademy.com

surgical approach for the orthodontic treatment of deep infraosseous impacted canines. This technique allows for orthodontic traction of the impacted tooth to the center of the alveolar ridge.
Its creates the natural path of eruption.
www.indiandentalacademy.com

Full gingival flap is raised , with some cortical bone removal to expose the canine, deciduous teeth is extracted, a tunnel is made with a bur through socket of deciduous canine till the tip of the impacted canine www.indiandentalacademy.com

Attatchments used
www.indiandentalacademy.com

Flap is sutured back and canine is disimpacted through the socket of deciduous teeth
www.indiandentalacademy.com

Impacted canine erupts at center of alveolar ridge.
www.indiandentalacademy.com

Guiding tooth to line of arch Once the tooth is moved to the oral enviroment,bonding attachment is placed on the midbuccal aspect to prevent iatrogenic rotation of canine and guided to the line of arch.
www.indiandentalacademy.com

If the root apex mesial to lateral incisor or distal to premolar , tooth is considered as TRANSPOSED.
I) Incomplete transposition: Roots will be in line of arch in its position and crown tipped due to path of eruption.(uprighting of tooth will align the tooth in arch).
II) Complete transposition: Both crown and root together will be completely interchanged.In these sutiation its better to align tooth to their respective position ,i.e canine between premolars or mesial to lateral incisors depends on type of transposition..
Canine transposition
www.indiandentalacademy.com

If we tried to align this tooth to their respective position,following will occur, I) If canine is palatal to line of arch,secondary effect of root contact will rotate the root apex both mesially and palatally across the palate in a wide sweeping motion.the tooth will be laid down beneath the periosteum with huge dehiscence.
II) If canine is buccal to the line of arch ,secondary effect of root contact will cause further buccal displacement of root with gross dehiscence of buccal periodontium.
www.indiandentalacademy.com

Dentigerous Cyst: Dentigerous cyst inhibit the eruption of the involved tooth. Treatment: Marsupialization is the procedure consists of fenestrating the outer wall of the cyst, and relieving the intracystic pressure. With this early decompression, the size of the cavity slowly decreases, enabling the surrounding bone to regenerate around the impacted tooth, which eventually erupt the tooth into the dental arch. time to erupt after Marsupialization is 109 days,without any traction. Orthodontic traction is necessary if it delays later..
www.indiandentalacademy.com

Impacted tooth and Periodontium In 1984 Becker showed Exposure of the crown should be sufficient to bond attachment rather than exposing upto CEJ When these tooth erupt in to occlusion,these tooth will have longer clinical crown and reduced alveolar height.
www.indiandentalacademy.com

Kokich and Mathew showed that bone removal should not be more than 2/3rd of the impacted tooth crown.
Light orthodontic movement like tipping , extrusion, and rotation have less periodontal breakdown than Heavy orthodontic movement like root uprighting and torquing.
In 2002 Charles and Frank showed periodontal condition depends on the type of surgery.Closed approach seems to be preferable than open approach and apically repositioned flap.
www.indiandentalacademy.com

COMPLICATION OF UNTREATED IMPACTED CANINE
1) Crown Resorption: 2) Labial or lingual malposition of impacted tooth
3 ) Migration of neighboring teeth and loss of arch length 4) Internal resorption of impacted tooth 5) Cyst formation {Dentigerous cyst}
www.indiandentalacademy.com

RETENTION CONSIDERATIONS
Evaluation of post treatment alignment by Becker et al
• Incidence of rotations and spacings
1. Impacted side- 17.4%
2. Control side 8.7%
• Ideal alignment on control side is twice as often as the impacted side.
www.indiandentalacademy.com

To minimize rotational relapse, options available are
1. Fiberotomy
2. Bonded fixed retainer
This can be done during or after the treatment.
Clark’s suggestion for palatally impacted canine: Lingual
drifting can be prevented by removal of halfmoon- shaped
wedge of tissue from lingual aspect of canine.
www.indiandentalacademy.com

WHEN TO EXTRACT AN
IMPACTED CANINE
* If it is ankylosed & cannot be transplanted.
* If it is undergoing external or internal root
resorption.
* If the root is severely dilacerated. www.indiandentalacademy.com

If the impaction is severe on central & lateral
incisors & orthodontic movement will jeopardize these
teeth.
If the occlusion is acceptable, with first premolar in
canine position.
If there are pathologic changes {cystic formation,
infection}.www.indiandentalacademy.com

Other single teeth
Mandibular and maxillary second premolars
Crowding and space lossEarly extraction of second
deciduous molarDistal tipping of 1 deciduous molar
teeth is blocked from eruptionTipping of adj permanent teeth
www.indiandentalacademy.com

Treatment alternativesExtraction of the first premolar – to
resolve crowding and disimpaction Uprighting of adj teeth with coil
compressed b/w 1 molar and I premolar
Extraction of impacted teeth along with other tooth rxtraction in other quadrants.
www.indiandentalacademy.com

Improper orientation of premolarDistal tipped premolars causes only
resorption of distal root of deciduous molar ,leaving mesial root unresorbed and overretention of deciduous molar.
extract the deciduous molar Hold the space Surgically expose the mesial and
occlusal aspects of impacted teeth and attatch an eyelet and tie a piggy tail and attach it to hook of the rigid bar used for maintaining space.
www.indiandentalacademy.com

www.indiandentalacademy.com

Infraocclusion of deciduous second molar
Due to infraocclusion - premolar is impacted more apically
treatment extract the infraoccluded teethHold the spaceWait and check for spontaneous
eruption of teeth – vertical bone height is also developed.
www.indiandentalacademy.com

www.indiandentalacademy.com

Maxillary first molars In early mixed dentition - common to see that erupting
maxillary molars caught by distal tuberosity of adj deciduous second molar.
Clinically - marginal ridges of 2 teeth are not at same level or present beneath the distal CEJ of deciduous teeth
Radiological - distal root of deciduous 2 molar is resorbed path of eruption of permanent molar is mesially tilted.Treatment - donot extract the deciduous molar - mesial
tilt the permanent molar and occupy the spaceMild cases - elastic separator can be used - relapse may
occur after removalFixed appliance - banding E of both sides and soldering a
palatal arch with soldered spring on the deep occlusal pit of I st permanent molar.
Removal appliance-
www.indiandentalacademy.com

www.indiandentalacademy.com

Third molar impactions Archer defined an impacted third molar as ‘One
which was completely or partly erupted and positioned against another tooth,bone or soft tissue, so that its further eruption was unlikely.
Dachi and Howell in their study found that the incidence of patients with atleast one impacted tooth was 16.7%.
www.indiandentalacademy.com

Bjork and colleagues identified 3 skeletal factors that are separately influencing third molar impaction– Reduced mandibular length,measured as
the distance from the chin point to the condylar head.
– Vertical direction of condylar growth as indicated by the mandibular base angle.
– Backward directed eruption of mandibular dentition determined by the degree of alveolar prognathism of lower jaw.
www.indiandentalacademy.com

TYPES OF IMPACTIONRichardson suggested five categories of
impaction Type A : The tooth can follow the pattern of an
ideally developing third molar, by decreasing its angle to the mandibular plane and becoming more upright, but the uprighting may not be enough to allow full eruption.
www.indiandentalacademy.com

Type B : The angular developmental position relative to the mandibular plane may remain unchanged
Type C : The tooth can increase its angulation to the mandibular plane ,and become more mesially inclined .There is at present no reliable way of predicting which teeth will follow this unfavourable pattern,which sometimes occurs unilaterally and leads to horizontal impaction
www.indiandentalacademy.com

Type D :The tooth can be seen to make favourable changes in angulation ,but fail to erupt owing to lack of space.These are so called vertical impactions.
Type E :The tooth can continue to change its angulation beyond the ideal occlusal position,and show disto angular impaction
www.indiandentalacademy.com

MECHANISM FOR ERUPTION AND IMPACTION
Differential root elongation might explain differences in eruptive behaviour among lower third molars.
Richardson offered a theoretical explanation for favorable or unfavorable rotational movement.
www.indiandentalacademy.com

Favorable change in angulation ,to a more upright position ,seemed to occur in teeth where the mesial root developed ahead of the distal crown surface and root and a mesial root which was curved in a distal direction and was slightly longer than the distal root.
www.indiandentalacademy.com

Unfavorable mesial tipping, leading to horizontal impaction, seemed to occur when the distal root became the same length, and then longer than the mesial root.
The distal root on such teeth was seen to appear to have a mesial
curvature.
www.indiandentalacademy.com

FACTORS INFLUENCING AVAILABILITY OF SPACE GROWTH
Bjork et al measured the distance from the anterior border of the ramus to the second molar,and concluded that the bigger the space,the better the chance of eruption.Richardson measured an average of 11.4 mm of growth between the age of 10 and 15 years.
www.indiandentalacademy.com

BONE RESORPTION In 1987 Richardson examined the
creation of space for third molars in 51 subjects.
She found that increased space was obtained from both the mesial movement of the dentition and bone remodeling along the anterior border of the ramus.
On average 2 mm of posterior space was created by bone remodeling
www.indiandentalacademy.com

SPACE RELEASED BY ATTRITION In so-called primitive dentitions, where considerable attrition takes place,
the third molars erupt to take up the space released. Begg felt that lack of this attrition,due to highly refined diets,was a
major cause of third molar impaction. Other authors, such as Profitt,have questioned this hypothesis.
Early and extensive interproximal caries could also reduce the size of erupted teeth, owing to disappearance of proximal contacts.
www.indiandentalacademy.com

SECOND MOLAR EXTRACTION Richardson and Richardson in AJO 93
investigated 63 patients after extraction of lower second molars and found that all the lower third molars erupted more or less successfully after an average observation period of 5.8 years.
www.indiandentalacademy.com

Bonham Magness in JCO 86 suggests that upper third molars has a much more predictable eruption pattern than lower third molars.
He suggested the extraction of upper second molars in some cases to assist first molar positioning and increase space for upper third molars.
www.indiandentalacademy.com

Tae-Woo Kim et al in AJO 2003 impaction of mandibular third molars occurs about twice as often in non-extraction patients than in extraction patients.
The mechanism may be that premolar extraction therapy is associated with an increase in the amount of mesial movement of the maxillary and mandibular molars and an increase in the eruption space for the third molars.
www.indiandentalacademy.com

UPRIGHTING IMPACTED MOLARS
Third molar retention may be beneficial in many situations.
Some investigators maintain that third molars could be used at a later date as replacements or for prosthetic abutments in case of loss of first and second molars.
Third molars could also be used as transplants
www.indiandentalacademy.com

In shallow mesio-angular impactions Richardson used a one stage method.
A second molar tube can normally be bonded onto the buccal aspect of a partly erupted lower third molar, if enough enamel is visible.
www.indiandentalacademy.com

In deep mesio-angular impactions,a two-stage method is used.
The first stage involves bonding a second molar tube onto the occusal surface of the lower third molar.After some uprighting using this method, it is
normally possible to bond a tube buccally for the second stage.
www.indiandentalacademy.com

Ike Slodov et al in AJO 89 describes an orthodontic uprighting
Modified impaction related surgical procedures provide easy application of techniques to facilitate exposure of unerupted and partially erupted third molars and allow orthodontic manipulation
www.indiandentalacademy.com

After surgical exposure a cleat is bonded in center of mesial marginal ridge.
The wire portion of the appliance is fabricated from 0.032 inch stainless steel wire and adapted closely to the mucosa.
The mesial hook is placed 3 mm distal to the distal portion of the third molar.
www.indiandentalacademy.com

Standard soldering techniques are used to attach the wire to the buccal (or lingual) surface of the band. Appliance is cemented in place and is activated with elastic modules
www.indiandentalacademy.com

Orton and Jones in JCO 87 described a simple whip spring.
It is used for disimpacting , mild to severe mesially impacted lower terminal molars (LTM).
If the impacted molar has not sufficiently erupted then surgically expose distobuccal surface and bond an attachment.
The whip spring is fabricated with 0.018X 0.025 wire for 0.022 slot and 0.017X0.022 wire for 0.018 slot. A circular loop is placed mesial to the tube to prevent posterior displacement of the wire and to provide attachment of an elastic module that anchors the wire in the tube.
www.indiandentalacademy.com

www.indiandentalacademy.com

REPLACEMENT OF THIRD MOLARS FOR SECOND MOLARS
www.indiandentalacademy.com

According to Malcolm.R.Chipman in AJO 1961 the third molars can be substituted for the second molars in certain situations and solve some of the problems of maxillary tuberosity area.
The indications for eliminating maxillary second molar and replacing it with third molars are1.Maxillary third molars of fair size and shape with the possibility of good root development2.Small,restricted maxillary tuberosities and the possibility of interference with distal movement in maxillary posterior region.3.Second molars erupted buccally.
www.indiandentalacademy.com

4.Second molars decayed ,badly decalcified or having large restorations.
5.Maxillary third molars in favourable position and angulation relative to second molars and maxillary tuberosity.
6.Maxillary third molars in favourable relation to mandibular second molars.
www.indiandentalacademy.com

Orton-Gibbs et al in AJO 2001 described the eruptive path of maxillary and mandibular third molars after extraction of second molars with the use of radiograph and assessed the final position from study models.
They showed that the angulation of the mandibular third molar crown long axis showed progressive uprighting from a mean of 55 to the occlusal plane at the start of active treatment (SAT).
Uprighting of mandibular third molars from SAT to end of active treatment (EAT) was limited (mean 6). However the third molars continued to upright thereafter on average a further 13.
www.indiandentalacademy.com

Approximately 50% of the space closure occurs by EAT. Interestingly space closure is not a result of mesial tipping but is due to significant horizontal translation.
The relationship of the first and the
third molar crown should be the
most important indicator of successful outcome, not
angulation of the whole tooth.
www.indiandentalacademy.com

In contrast to the mandibular third molars, the maxillary third molars upright rapidly by 14 degree on average from SAT to EAT.
Angular changes is minimal as the maxillary molars settle into occlusion.
The rate of vertical change is rapid, with almost 7 mm of
eruption occurring by the completion of active treatment and a further 6 mm after active treatment
www.indiandentalacademy.com

The results showed that relief of crowding by removal of second molar is a realistic option in appropriate cases with mild to moderate crowding, particularly in patients in whom third molar impaction is predicted and in reducing the likelihood of increasing crowding through the teenage years
www.indiandentalacademy.com

conclusion
Orthodontic treatment can be very rewarding if we are ready to accept the challenge of anticipating the changes , on the basis of a sound problem list and treatment goals.
Thus management of the impacted teeth is one of the greatest challenge for orthodontist. Success of the treatment depends upon patient cooperation, Age of patient, Proper diagnosis, Level of impaction, Inclination and Depth of impaction, Amount of root formation, Type of exposure of tooth, Amount of bone removal, Type of attachment, Orthodontic traction. All these parameter plays important role when managing impacted teeth to achieve good alignment in the arch, Gingival level, and Integrity of periodontium.
www.indiandentalacademy.com

References1) Orthodontic treatment of impacted teeth - Ardian Becker2) AJO 1983 Aug 125 – 132 The etiology of maxillary canine impactions - Jacoby3) AJO 1994 Jan 61 – 72 Tunnel traction of infraosseous impacted maxillary canines - Crescini, Clauser, Giorgetti, Cortellini, and Prato4)AJO 1982 Mar 236 - 239 Txt Orthodontic considerations in the treatment of maxillary impacted canines - Fournier, Turcotte, and Bernard5) AJO1991 Dec 494 - 512 Txt Rare earth magnets and impaction - Vardimon, Graber, Drescher, and Bourauel.5) Seminar in orthodontics - management of impacted teeth.
www.indiandentalacademy.com

www.indiandentalacademy.com
For more details please visit www.indiandentalacademy.com