Management of Hypertension after SPRINT
51
Management of Hypertension after SPRINT Richard J. Glassock, MD, MACP Professor Emeritus Geffen School of Medicine at UCLA
Transcript of Management of Hypertension after SPRINT

Management of Hypertensionafter SPRINT
Richard J. Glassock, MD, MACP
Professor Emeritus
Geffen School of Medicine at UCLA

Richard J. Glassock, MD, MACP, FRCP (Hon), FASN
◼ Dr. Glassock is currently Professor Emeritus at the Geffen School of Medicine at UCLA. He has had a long standing interest in clinical nephrology (glomerular diseases) and hypertension and has published over 750 papers, books chapters and monographs. He is a former President of the ASN and NKF

DISCLOSURES
◼ Nothing to Disclose

CASE and QUESTION
◼ An 83 year old woman is referred to you for advice concerning blood pressure control. She is active and has no symptoms, other than a painful hip from osteoarthritis. She is a life long non-smoker. Her BP taken in the office by the nurse using an anaeroidsphygmomanometer is 144/60mmHg, pulse 72 and regular. Other than cataracts and dry skin her examination is unremarkable. Her BMI is 24Kg/m2. The blood sugar (fasting) is 90mg/dL and a Hemoglobin A1c is 5.1%. A serum creatinine is 1.08mg/dL (eGFR= 55ml/min/1.73m2) and a urinalysis is negative for blood and protein (dipstick). The LDL-C is 96mg/dL and the HDL-C is 60mg/dL
CASE AND QUESTION
◼ Which ONE of the following would you now recommend?
A. Start a thiazide diuretic
B. Start an angiotensin receptor inhibitor
C. Initiate a DASH- style diet
D. Start a Beta-adrenergic blocker

OUTLINE
◼ Part I- Description of SPRINT
◼ Part II- Initial Guidelines built on SPRINT (AHA/ACC- 2017)
◼ Part III- Post-Hoc SPRINT Studies
◼ Part IV- Recent Guidelines based on Sprint (ISH- 2020; KDIGO- 2021)

PART I-
SPRINT 2015-2021:The gift that keeps on giving!


BP Measurement in SPRINT
◼ Mean of 3 measurements in office, seated position after 5 minutes of quite rest by an automated oscillo-metric system* (physician/or nurse not required to be present)
*Omron Healthcare (model 907)

AUTOMATED DEVICE (Omron-Model 907)
SPRINT
Primary End Point=
Composite of Myocardial Infarction, Acute Coronary Syndrome, Stroke, Congestive Heart Failure, or Death
from CVD (not a renal end point study!)


SPRINT(NEJM; November, 2015)
◼ 9361 patients Randomized (4678-Intensive; 4683-Standard)
◼ Non-Diabetic ; 91% already on anti-hypertensive treatment- mainly RASi
◼ CKD – 28% (eGFR >20ml/min/1.73m2; uPER <1gm/d; average uACR- 43mg/gm)
◼ Non-Hispanic Black- 30%
◼ Average Age- 68 years (28% ≥ 75 years)
◼ Pre-existing CVD- 22% (high risk population)
◼ Follow-Up -3.26 years- Stopped prematurely for Efficacy



SPRINT:Primary and Secondary Outcomes
Intensive(n=4678)
Standard(n=4683)
Hazard Ratio
Primary Composite Outcome
1.65%/yr 2.19%/yr 0.75 (p<0.001)
Myocardial Infarction
0.65%/yr 0.78%/yr 0.83 (ns)
Acute Coronary Syndrome
0.27%/yr 0.27%/yr 0.99 (ns)
Stroke 0.41%/yr 0.47%/yr 0.89 (ns)
Congestive Heart Failure 0.41%/yr 0.67%/yr 0.62 (p=0.002)
CVD Death 0.25%/yr 0.43%/yr 0.57 (p=0.003)
All Cause Death 1.03%/yr 1.40%/yr 0.78 (p<0.001)
SPRINT
Renal Outcomes-
For patients with CKD at baseline (n=2646)- first occurrence of
reduction of eGFR by 50% or more from BL, Dialysis or Transplantation

SPRINT:Renal Outcomes-
in patients with CKD at BL
Intensive (n=1330)
Standard(n =1316)
Hazard Ratio
Composite Renal Outcome
0.33%/yr 0.36%/yr 0.89 (ns)
≥50% decline in eGFR
0.23%/yr 0.26%/yr 0.87 (ns)
Dialysis 0.14%/yr 0.24%/yr 0.57 (ns)
Transplantation 0 0 NA
New OnsetAlbuminuria
3.02%/yr 3.90%/yr 0.72 (ns)

SPRINTRenal Outcomes-
in Patients without CKD at BL
Intensive(n=3332)
Standard(n=3345)
Hazard Ratio
≥30% decline in eGFR to <60ml/min/1.73m2
1.21%/yr 0.35%/yr 3.49 (p<0.001)
New onset albuminuria
2.00%/yr 2.41%/yr 0.81 (ns)

SPRINT:Main Conclusions-I
◼ In elderly, non-diabetic subjects, without a prior history of Stroke but with increased CVD risk, intensive BP lowering improves CV and mortality outcomes, at least for up to 3.2 years
◼ In a subgroup analysis (hypothesis generating) no benefits were seen for the primary composite CV outcome in subjects with CKD at BL (?underpowered)
◼ No benefit observed on CKD progression in patients with CKD at BL and a potential harmful effect on eGFR seen in those without CKD at baseline. No clear effects on albuminuria was observed
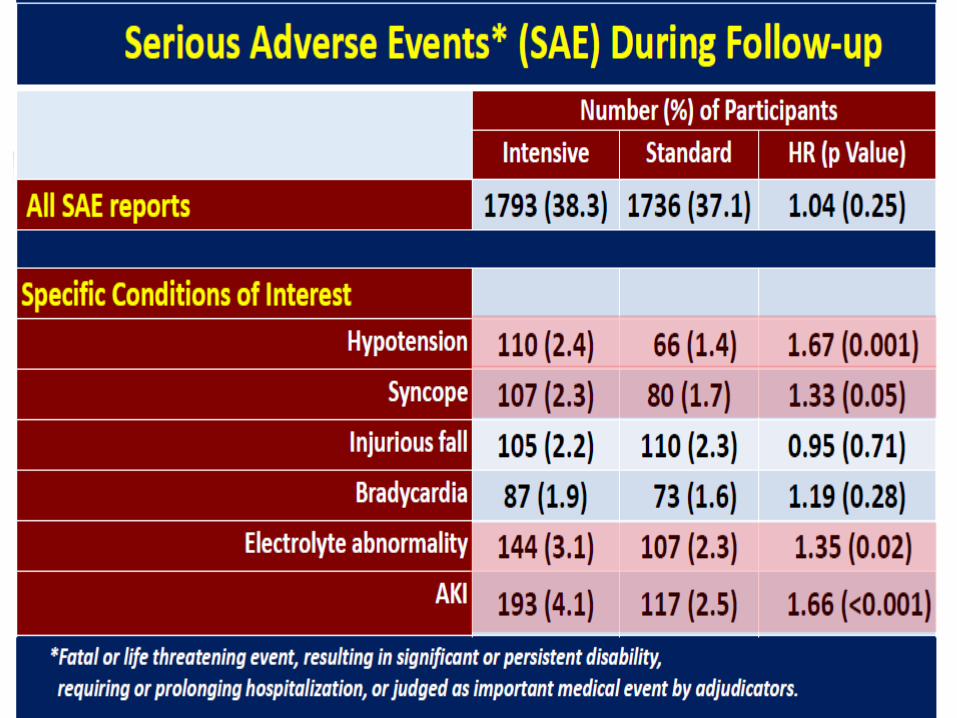
◼ Adverse events (hypotension, electrolyte abnormalities [hyperkalemia] and AKI) were “common” in the intensive arm
SPRINT:Main Conclusions-II
PART II-Translating SPRINT into
Practice (Guidelines)

ACC/AHA* Guideline for Prevention, Detection, Evaluation and Management of High Blood
Pressure in Adults (Whelton P, et al- 481 pages-Synopsis JAMA,
November 2017)
(ACC, AHA, AAPA, ABC, ACPM, AGS/APHA, ASH, ASPC, NMA/PCNA- No ASN, KDIGO, NKF, ACP or AAFP
participation in development- Consensus Driven)



Of 31 million “new” hypertensives the great majority will be
diagnosed and managed by PCP- 27million by lifestyle modifications
and 4 million by drugs
BP Measurement and Diagnosis of Hypertension
◼ Out-of-office measurement of BP using Automated (calibrated) devices (arm cuff preferred) is recommended for diagnosis and titration of therapy (evidence level high)-observed in office BP overestimates automated SBP by about 10mmHg
◼ Ambulatory BP monitoring required for accurate classification of subtypes


Non-Pharmacologic Treatment of Hypertension
(“Life Style Modifications”)
Modification SBP Effect
in Hypertensives (mmHg)
Weight Loss -5
Heathy Diet (DASH) -11
Reduced NaCl (<3.5gms/d) -5
Increased K (3.5-5gm/d) -5
Exercise (Aerobic,Dynamic
Resistance or Isometric) -4/-8
Reduced Alcohol -4


Impact of SBP Control on Incident CKD with and without Diabetes:
ACCORD and SPRINT(Beddhu S, et al. Lancet Diab Endo, April, 2018; 3 yr FU)
Intensive Standard AbsoluteDifference
ACCORD (Diabetes)
10.0% 4.1% +5.9%
SPRINT (No Diabetes)
3.5% 1.0% +1.5%

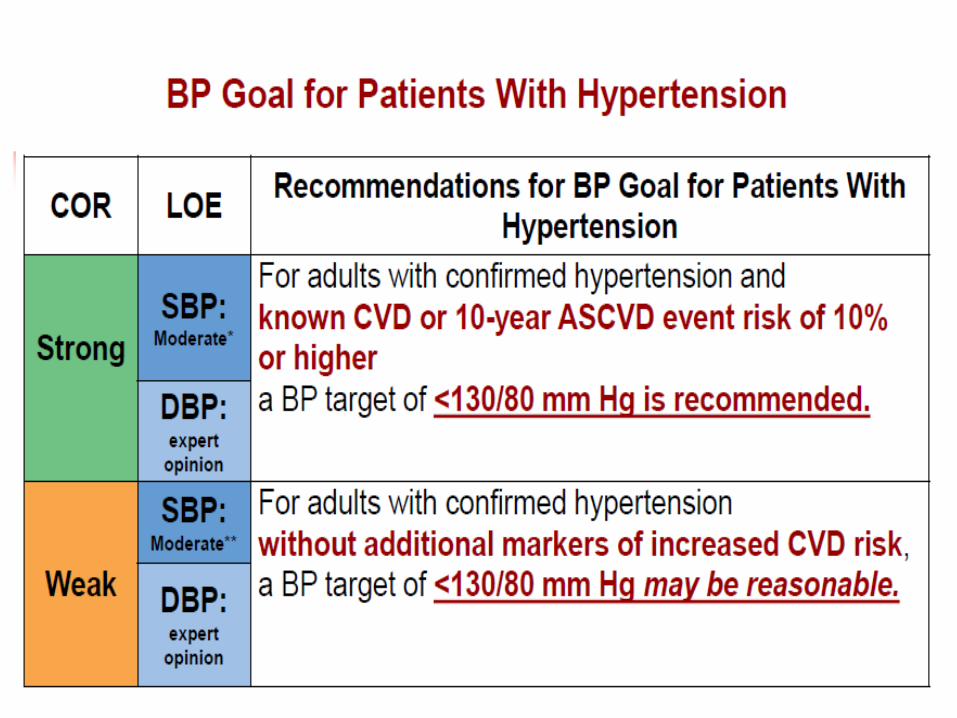
AHA/ACC Guidelines:Caveats
◼ Not endorsed by ACP or AAFP (yet)
◼ Not applicable to practices using Office Based non-automated BP measurements
◼ Largely based on Expert Opinion and Consensus
◼ Ignores dangers of DBP <60-65mmHg in DM and CVD
◼ In very low-risk subjects <140/90mmHg is a “reasonable” target
◼ Do not apply to eGFR <20-30ml/min/1.73m2 (CKD Category 4/5/5D)
◼ Creates 31 Million new “hypertensives” (in the USA)-$Billions of added costs and burden to PCP
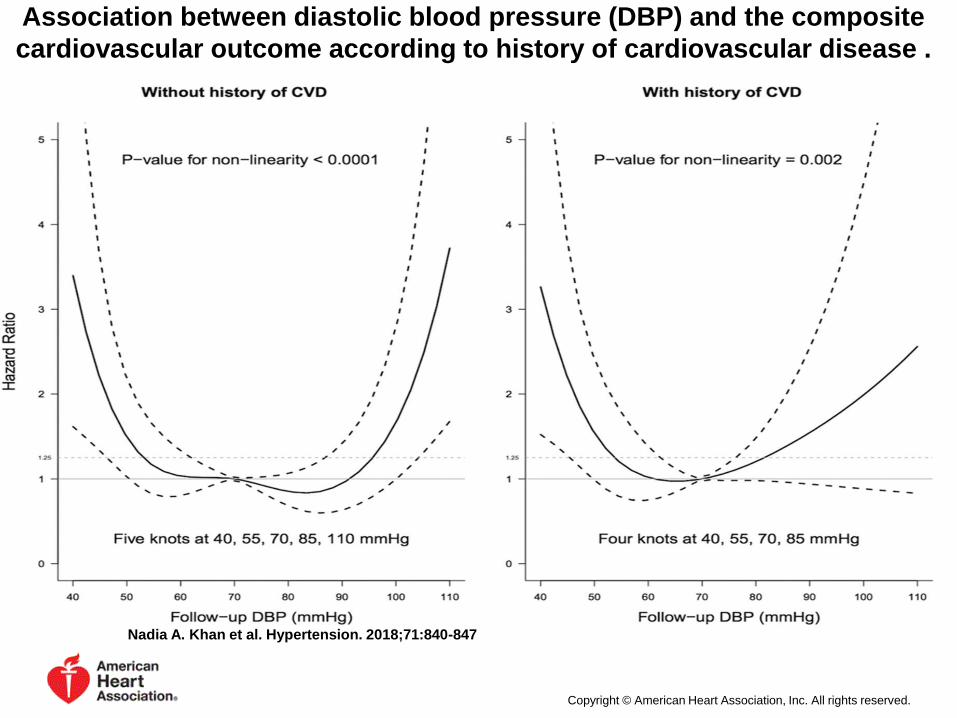
Association between diastolic blood pressure (DBP) and the composite
cardiovascular outcome according to history of cardiovascular disease .
Nadia A. Khan et al. Hypertension. 2018;71:840-847
Copyright © American Heart Association, Inc. All rights reserved.

Part III-Post-Hoc SPRINT Studies
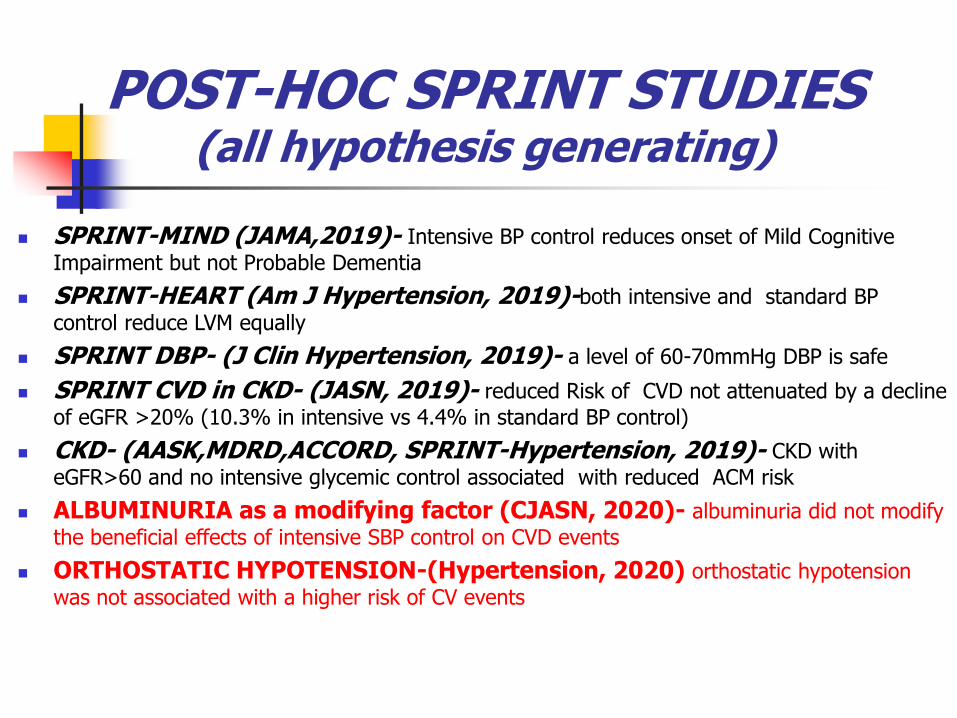
POST-HOC SPRINT STUDIES(all hypothesis generating)
◼ SPRINT-MIND (JAMA,2019)- Intensive BP control reduces onset of Mild Cognitive
Impairment but not Probable Dementia
◼ SPRINT-HEART (Am J Hypertension, 2019)-both intensive and standard BP
control reduce LVM equally
◼ SPRINT DBP- (J Clin Hypertension, 2019)- a level of 60-70mmHg DBP is safe
◼ SPRINT CVD in CKD- (JASN, 2019)- reduced Risk of CVD not attenuated by a decline
of eGFR >20% (10.3% in intensive vs 4.4% in standard BP control)
◼ CKD- (AASK,MDRD,ACCORD, SPRINT-Hypertension, 2019)- CKD with
eGFR>60 and no intensive glycemic control associated with reduced ACM risk
◼ ALBUMINURIA as a modifying factor (CJASN, 2020)- albuminuria did not modify
the beneficial effects of intensive SBP control on CVD events
◼ ORTHOSTATIC HYPOTENSION-(Hypertension, 2020) orthostatic hypotension
was not associated with a higher risk of CV events

SPRINT-Albuminuria and CVD outcomes
(Chang A, et al CJASN, 2020)

SPRINT-Orthostatic Hypotension
(Juraschek SP, et al Hypertension 2020; 75:660-667)

PART IV-Recent Guidelines
International Society of Hypertension (ISH)-
(Unger T, et al. Hypertension 2020; 75:1334-1357
◼ Normal SBP= <130mmHg; DBP= <85mmHg; High-normal BP= 130-139mmHg; DBP= 85-89mmHg; Hypertension=SBP≥ 140 mmHg and or DBP≥ 90mmHg- confirmed X2-3
◼ Office Based BP measurement; quiet room, seated 3-5 min, no smoking, caffeine or exercise; automated oscillo-metric (calibrated) upper arm device preferred
◼ 3 measurements, last 2 averaged

Hypertension and CKD-(ISH- 2020)
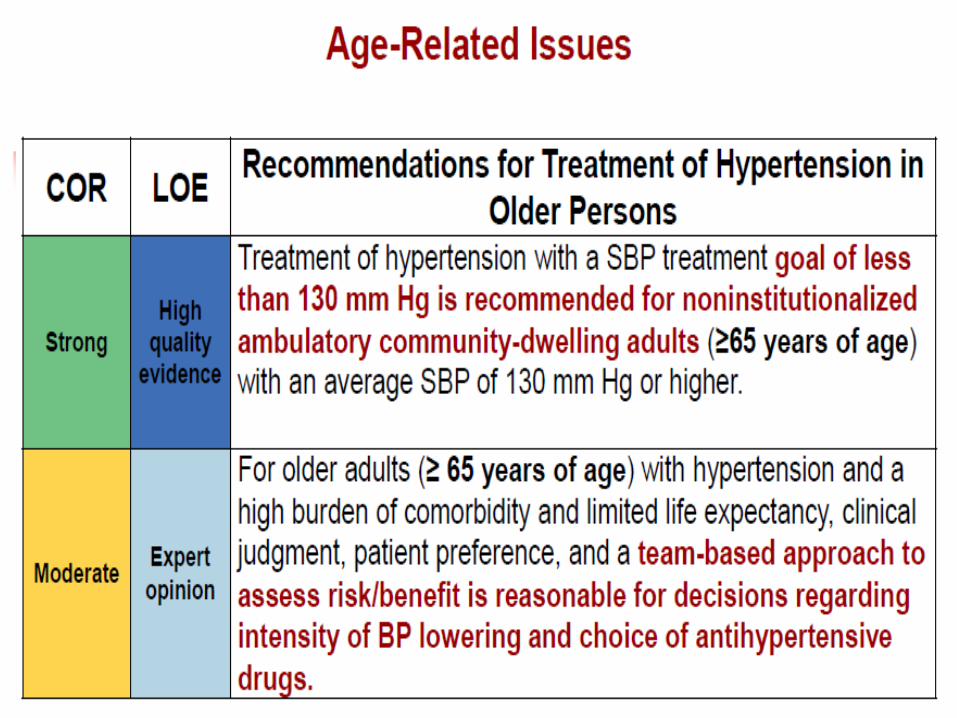
◼ BP should be lowered if ≥ 140/90mmHg and treated to a target of <130/80mmHg, in both Diabetic and non-Diabetic subjects (<140/90mmHg in elderly subjects)
◼ RASi first-line agents. CCB and diuretics can be added. Loop diuretics preferred if eGFR <30ml/min/1.73m2

KDIGO Practice Guidelines for Management of Blood Pressure in CKD
(KDIGO- 2021; KI Supplements 99:#35; s1-s85; abbreviated summary)
◼ “Standardized” office BP measurement
recommended: ➢ Sitting, feet on floor, “relaxed” for 5 minutes
➢ Empty bladder
➢ No talking
➢ Clothing on upper arm removed
➢ Calibrated oscillo-metric device preferred; but calibrated auscultatory (Korotkoff sounds), anaeroid device acceptable
➢ Cuff size appropriate to arm circumference
➢ At first visit, measure BP in both arms; use highest value
➢ Average of ≥2 readings on ≥2 visits

KDIGO Practice Guidelines for Management of Blood Pressure in CKD (2021)
(KDIGO- KI Supplements 99:#35; s1-s85; abbreviated summary)
◼ Suggests that out-of-office BP measurements (Either ambulatory or home monitoring) be used to complement standardized office-based BP readings for management (2B).
◼ Patients should be classified as White Coat Hypertension, Masked Hypertension, Sustained Hypertensioin or Normotension based on the office and out-of-office recordings.

KDIGO Practice Guidelines for Management of Blood Pressure in CKD (2021)
(KDIGO- KI Supplements 99:#35; s1-s85; abbreviated summary)
◼ Suggests that adult subjects (age above 18 years) with high BP (SBP=≥130mmHg ) be treated to a target SBP of <120mmHg, when tolerated using standardized office BP measurement (2B)
◼ This suggestion is not dependent on etiology of CKD. Except patients with ADPCKD who may derive benefits of SBP <120mmHg

KDIGO-CKD-Uncertainties concerning the balance of
benefits and harms
◼ Applicability to CKD Categories G4/G5 (G5D)
◼ Diabetic vs Non-Diabetic CKD
◼ Patients with SBP of 120-129mmHG
◼ Patients with very low DBP (<50mmHg)
◼ Etiology of CKD not important; except ADPCKD who may derive renal benefits at SBP of 95-110mmHg
◼ Older age, frailty
◼ Patients at low risk of CVD
◼ “White –Coat” hypertension; Multi-drug resistant Hypertension
◼ Severe hypertension (SBP ≥180mmHg)

KDIGO- CKDTreatment modalities
◼ RASi strongly preferred for non-diabetic subjects with G1-4/A3 CKD (1B)
◼ RASi strongly preferred for Diabetic subjects with G1-4/A2 or A3 CKD (1B)
◼ RASi weakly preferred for non- diabetic subjects with G1-4/A2 (2C)

CASE and QUESTION
◼ An 87 year old woman is referred to you for advice concerning blood pressure control. She is active and has no symptoms. Her BP taken in the office by a nurse is 142/60mmHg, pulse 72 and regular. Other than cataracts and dry skin her examination is unremarkable. Her BMI is 24Kg/m2. The blood sugar (fasting) is 95mg/dL and a Hemoglobin A1c is 5.1%. A serum creatinine is 1.08mg/dL (eGFR by CKD-EPI= 55ml/min/1.73m2) and a urinalysis is negative for blood and protein (dipstick). The LDL-C is 96mg/dL and the HDL-C is 60mg/dL
CASE AND QUESTION
◼ Which ONE of the following would you now recommend?
A. Start a thiazide diuretic
B. Start an angiotensin receptor inhibitor
C. Initiate a DASH- style diet
D. Start a Beta-adrenergic blocker
The correct answer (in my opinion) is C

References◼ SPRINT Research Group, Wright JT Jr, Williamson JD, Whelton PK, et al. A Randomized
Trial of Intensive versus Standard Blood-Pressure Control. N Engl J Med. 2015;373:2103-16
◼ Whelton PK,2, Carey RM. The 2017 Clinical Practice Guideline for High Blood Pressure. JAMA. 2017;318:2073-2074.
◼ Whelton PK, Williams B. The 2018 European Society of Cardiology/European Society of Hypertension and 2017 American College of Cardiology/American Heart Association Blood Pressure Guidelines: More Similar Than Different. JAMA. 2018;320:1749-1750.
◼ Chang AR, et al Effects of intensive blood pressure control in patients with and without albuminuria. CJASN 2020; 15
◼ Unger T, et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension 2020; 75: 1334-1357
◼ KDIGO 2021 Clinical Practice Guidelines for Management of Blood Pressure in Chronic Kidney Disease. Kidney Int Supplements. 2021; 35: s1-s85