
Management of chronic pain in adults
84
Best Practice Statement ~ February 2006 Management of chronic pain in adults
Transcript of Management of chronic pain in adults

Best Practice Statement ~ February 2006
Management of chronic pain in adults

© NHS Quality Improvement Scotland 2006
ISBN 1-84404-385-1
First published February 2006
You can copy or reproduce the information in this document for use within NHSScotland and foreducational purposes. You must not make a profit using information in this document.Commercial organisations must get our written permission before reproducing this document.
www.nhshealthquality.org

i
Foreword
Chronic pain is a major health and social care challenge affecting asignificant number of people in Scotland, many of whom are cared bynurses and Allied Health Professionals (AHPs) working in primary careand in the community. In order to support these healthcare professionalsin their work, NHS Quality Improvement Scotland has, in partnershipwith patients, carers and clinical experts, developed a Best PracticeStatement for the Management of Chronic Pain in Adults.
This best practice statement is aimed at general nursing and AHP staffand does not cover Specialist Pain Services although it is acknowledgedthat they are a key element in the patient pathway for those withchronic pain.
We hope you find it of use and would welcome any comments you mayhave.
David R SteelChief ExecutiveNHS Quality Improvement Scotland

Management of chronic pain in adults
Acknowledgements
This best practice statement was developed in partnership with a numberof people who live with chronic pain, carers and clinical experts. A listof those involved can be found in Appendix 2.
There are also a number of individuals whose guidance and support hasbeen greatly appreciated. These include:
Dr. M. Basler, Consultant anaesthetistDr. Robin McKinlay, Consultant in anaesthesia and pain managementMr. Mick McMenemy, Physiotherapist, lead clinicianDr Mick Serpell, Consultant and senior lecturer in anaesthesiaMrs Rosemary Showell, District nurse and team leaderDr Nicola Stuckey, Consultant psychologist
We would also like to thank those who sent letters of inspiration andsupport throughout the development process.
ii

Contents
Foreword i
Acknowledgments ii
Introduction v
What is Chronic Pain? ix
Background x
Section 1: Initial assessment 1
Section 2: Pharmacological management of chronic pain 3
Section 3: Unconventional analgesics (Adjuvants) 5
Section 4: The use of opioids 7
Section 5: The multidisciplinary approach in primary care 8
Section 6: Pain management programmes 15
Section 7: Self management/support groups 16
Section 8: Chronic pain "flare-ups" 17
Section 9: Specific challenges 18
Section 10: The use of complementary therapies 24
Section 11: Culture and chronic pain 25
Section 12: Education for health professionals 26
Additional Information 27
Integration of pain services 27
Palliative care and chronic pain 28
Determining pain in people who have difficulty 29communicating
Examples of unconventional analgesics 30
The use of opioids in the management of chronic pain 31
Specialist Services: Pain management clinic 33
Common interventional procedures 34

Management of chronic pain in adults
Appendix 1: Examples of Assessment Tools 35
Doloplus-2 Scale 35
NoPain – Non-Communicative Patient’s Pain 38Assessment instrument
McCaffery & Pasero initial assessment 39
Patient comfort assessment guide 42
Short form McGill pain questionnaire 44
Brief pain inventory 45
Oswestry disability questionnaire 47
Appendix 2: Who was involved in developing the statement? 49
Glossary 52
References 54
iv

v
Introduction
NHS Quality Improvement Scotland (NHS QIS) was set up by the ScottishParliament in 2003 to take the lead in improving the quality of care andtreatment delivered by NHSScotland.
The purpose of NHS QIS is to improve the quality of healthcare inScotland by setting standards and monitoring performance, and byproviding NHSScotland with advice, guidance and support on effectiveclinical practice and service improvements.
A series of best practice statements has been produced within thePractice Development Unit of NHS QIS, designed to offer guidance onbest and achievable practice in a specific area of care. These statementsreflect the current emphasis on delivering care that is patient-centred,cost-effective and fair. They reflect the commitment of NHS QIS tosharing local excellence at a national level.
Best practice statements are produced by a systematic process, outlinedoverleaf, and underpinned by a number of key principles:
• They are intended to guide practice and promote a consistent,cohesive and achievable approach to care. Their aims are realistic butchallenging.
• They are primarily intended for use by registered nurses, midwives,allied health professionals, and the staff who support them.
• They are developed where variation in practice exists and seek toestablish an agreed approach for practitioners.
• Responsibility for implementation of these statements rests at locallevel.
Best practice statements are reviewed, and, if necessary, updated after 3years in order to ensure the statements continue to reflect currentthinking with regard to best practice.

Management of chronic pain in adults
vi
Key Stages in the development of best practice statements
Topic selection and Scoping Process
Establish working group.Review literature on topic.
Source grey literature.
Ascertain current policy and legislation.
Seek information from manufacturers,
voluntary groups and other relevant
sources.
Establish reference group to
advise on consultation drafts.
Determine focus and content
of statement.
Review evidence for
relevance to practice.
Determine process for
incorporating patients’ views.
Draft document sent to
reference group.
Wide consultation process.
Review and update process. Identify
new research/ findings affecting topic.
Consider challenges of using
statement in practice.
Review and revise statement
in light of consultation
comments.
Publish and disseminate
statement.
Feedback on impact
of statement is
sought/impact
evaluation.
▲
▲
▲
▲
▲
▲
▲
▲
▲
▲
▲

vii
Best practice statement on the management of chronicpain in adults
This best practice statement has been developed by a multidisciplinaryworking group of relevant specialists, which included people living withchronic pain and carers. A multi-professional reference group has advisedon and overseen the work of the working group.
Chronic pain is one of the most common reasons people seek medicalhelp and depending on the severity of their pain are thought to usehealth services up to five times more often than the rest of thepopulation (Von Korff 1991).
Pain is defined as an unpleasant sensory and emotional experienceassociated with actual or potential tissue damage, or described in terms ofsuch damage (IASP 1986). This definition suggests that chronic pain islinked with severe psychological, social and economic consequenceswhich impact upon the sufferer, their families and healthcare resources(Smith 2001).
Patients and families struggling with chronic pain have different needsthan those with acute healthcare problems (Matthews 2002). These needsare unlikely to be met within an acute care culture.
Traditionally chronic pain has been viewed as a symptom orcomplication of another condition rather than a medical problem in itsown right. Consequently, many approaches to pain management havebeen short-sighted reinforcing the problem of chronicity (Bonica andLoeser 2001).
Chronic pain varies in aetiology (the cause of a disease or condition) andpresentation therefore the effects on individuals are often particular tothem and can include disruption of employment, family and socialfunctioning. This can lead to depression, withdrawal from socialactivities, inability to cope and increasing disability. The Pain in EuropeSurvey (2004) suggested that the prevalence of chronic pain in Scotland islikely to be around 18.1% of the population, with only 3% of peopleaccessing specialist pain services.
Considering the number of people who live with chronic pain, this Bestpractice statement is intended as a resource to guide the practice ofnurses and allied health professionals (AHPs) in acute care and primarycare who will undoubtedly care for people with chronic pain.

Management of chronic pain in adults
This Best practice statement refers to the management of chronic pain in
adults; it does not address the needs of children who suffer chronic pain.
The IASP (International Association for the Study of Pain) taxonomy on
chronic pain lists over 600 individual clinical syndromes related to
chronic pain. It would be impractical to attempt to produce guidelines
on all these individual syndromes. Instead a more generalised approach
is taken. Further reference to individual disorders can and should be
sought elsewhere.
The analgesic medications referred to in this document are onlyillustrative examples. The prescription of medicines for the relief of painshould be carried out in accordance with information provided withinthe British National Formulary (BNF) and according to the Nursing andMidwifery Council (NMC) Guidelines for the Administration of Medicines(2004).
viii

ix
What is chronic pain?
Pain can be defined as "an unpleasant sensory and emotional experienceassociated with actual or potential tissue damage, or described in terms ofsuch damage" (International Association for the Study of Pain 1986). TheIASP further define Chronic Pain as "pain without apparent biologicalvalue that has persisted beyond normal tissue healing time" (usually takento be 3 months). When pain lasts longer than 3 months or beyond thetime when an acute injury would be expected to have healed, theperson’s presentation becomes more complex. There may bepsychological features, including complaints of poor or non-refreshingsleep, tiredness, depression and poor concentration.Apart from the time characteristics (acute or persistent), pain can beclassified clinically as either nociceptive or neuropathic, although inpractice these can co-exist. Psychosocial features may play a significantrole in the persistence of symptoms.Because of the complexity of persistent pain, it is essential to make abiopsychosocial assessment (Dysvik et al 2004). By viewing chronic painin a biopsychosocial manner it enables the practitioner to focus on theindividual area which is having the largest impact on the patient’ssymptoms.
Figure 1 Biopsychosocial model for pain courtesy of Medical IllustrationsDepartment, Glasgow Royal Infirmary, adapted from Waddell et al (1993)
Management of chronic pain in adults
x
The Scope of the Problem
Chronic pain is a complex, devastating and widespread problem affectingapproximately 18.1% of people in Scotland (Breivik et al 2005). It hasharmful effects on health, employment and daily life (Smith et al 2001). Itis often described as persistent and may not totally resolve even withtreatment (Elliott et al 2002).
Nevertheless, management is worth pursuing.
Resources:
www.neuropathy-trust.org/www.arc.org.uk/about-arth/astats.htm
Key points
• Chronic pain is most prevalent in middle aged people. It is more prevalent in women than men (Rustoen et al 2005, Verhaaket al 1998).
• At least 7 million adults in the UK have long-term health problemsdue to arthritis and related conditions (Arthritis ResearchCampaign).
• In the UK the prevalence of neuropathic pain is 2.4%-8% of thepopulation (Neuropathy Trust).
• Chronic pain is one of the most common reasons why peopleseek medical care (Haetzman et al 2003).
• Chronic pain is a major public health problem.
• Chronic pain inflicts tremendous personal suffering.
• Chronic pain can reduce quality of life.
• Chronic pain does not always lead to disability – different peoplewith the same condition or injury often respond differently.
• There are significant health and social economic consequencesassociated with chronic pain (Pizzi et al 2005, Thomsen 2002).

xi
Key Principles
The key to successful management is identification of chronic pain,accurate assessment, adequate intervention and frequent evaluation(McCaffery 1999). This will allow the professional to:
• explain the process to the patient
• offer empathy and support having clearly explained the possiblelimitations of the physical relief of symptoms
• support the patient in a holistic way, in terms of the social andenvironmental impact
• improve quality of life, where possible
• encourage continuance at work, or return to work, where appropriateand possible
• foster an understanding of these patients within their families andwithin the general population, including employers.
Factors to consider in patient assessment:
• clinical history
• general personality traits and dispositions
• current level of somatic concern, depression, anger
• report of pain and functional limitations
• preliminary behavioural analysis
• pain coping strategies
• beliefs about injury, pain and treatment outcome
• social, economic and occupational influences on symptom presentation(Keefe and Bonk 1999).

What are the most common causes of chronic pain?
For many people the source of pain is musculoskeletal. Commondiagnoses are back pain, arthritis and widespread joint pain. Headache,angina and neuropathic pain are other common causes of pain. It isimportant to recognise that a significant number of individuals (5-10%)will have chronic pain with no formal diagnosis. This does not mean theirpain is imaginary. Pain is what the person says it is and exists wheneverthe person says it does (McCaffery 1980).
Table 1 Common diagnostic subgroups of chronic pain in the community
(based on Elliott et al 1999)
Table 2 Anatomical Site of Pain (based on Gureje et al 1998)
Diagnosis Male (%) Female (%)
Back Pain 14.9 17
Arthritis 13.7 17.8
After Injury 7.6 4.3
Angina 4.9 4.1
Gynaecological 0 7.5
Unknown Cause 5.2 3.4
Management of chronic pain in adults
xii
Anatomical site Subjects reporting pain (%)
Backpain 47.8
Headache 45.2
Joint Pain 41.7
Arm or leg pain 34.3
Chest Pain 28.9
Abdominal Pain 24.9
Pain Elsewhere 11.7
Number of sites
1 32.1
2 27.5
3 22.8
>4 17.5

Working Model
In relation to Back Pain a set of "flags" have been produced to reflect thebiopsychosocial phenomenon.
Figure 2 Adapted from Main CJ, Spanswick CC. 2000
A number of psychosocial "yellow flags" can be used during acuteepisodes and have been found to be useful in predicting failure to returnto work after back injury, and also prove useful in predicting whichpatients will develop prolonged pain in other situations.
These include:
• presence of a belief that the pain is harmful or potentially severelydisabling
• fear-avoidance behaviour (avoiding a movement or activity because ofa misplaced anticipation of pain), and reduced activity levels
• tendency to low mood and withdrawal from social interaction
• an expectation that passive treatments rather than active participationwill help Kendall et al (1997).
Resource: www.nzgg.org.nz
xiii
Organic pathology
Concurrent medical problems
latrogenic factors
Beliefs
Coping strategies
Distress
Illness behaviour
Willingness to change
Family reinforcement
Work Status
Health benefits and insurance
Litigation
Work satisfaction
Working conditions
Work characteristics
Social Policy
Occupational blue flags
Socio-occupational
black Flags
Clinical yellow Flags
Clinical red Flags
Biomedical factors
Psychological or
behavioural factors
(predictors)
Social and Economical
factors
Occupational factors

Management of chronic pain in adults
Types of Pain
Nociceptive pain (tissue damage pain) arises from mechanical, chemicalor thermal stimulation of nociceptors (eg after surgery, trauma orassociated with degenerative processes such as osteoarthritis). It isimportant to realise that pain may persist long after the nociceptiveprocess has ended and that other factors eg psychosocial features mayneed to be considered.
Neuropathic pain (nerve damage pain) is initiated or caused by aprimary lesion or dysfunction in the nervous system (eg in conditionssuch as diabetic neuropathy or spinal cord injury). It has quite differentclinical features from nociceptive pain. It is less well localised and often isdescribed as burning or shooting. It can occur in areas that are numb andwhere there is no tissue damage.
Table 3 Types of pain adapted from Nicholson (2003)
xiv
Nociceptive (tissue damage) pain
• Well localised
• May be more diffuse ifvisceral structures involved
• Sharp
• Stabbing
• Ache
• Gripping
Examples of nociceptive pain
• Arthritis
• Trauma
• Acute Post Operative
Neuropathic (nerve damage) pain
• Persistent
• Burning
• Paroxsysmal/spontaneous
• "Electric Shocks"
• Pain in the absence ofongoing tissue damage
• Allodynia – painful responseto stimuli that would notnormally cause pain
• Hyperalgesia – increased painin response to pain stimulus
• Dysaesthesia – unpleasantabnormal sensations
Examples of neuropathic pain
• Trigeminal neuralgia
• Diabetic neuropathy
• Post-herpetic neuralgia
• Complex regional painsyndromes I & II
• Peripheral Neuropathy

xv
Key points
• The above characteristics are typical rather than definitive
• Not all the above characteristics will be present
• Both nociceptive and neuropathic pain may co-exist
Psychosocial Features have been shown to be predictors of incidence andduration of chronic pain. It is important to realise that this does not implythat the pain has a psychological basis, only that psychological and socialfactors may have an implication in the severity and maintenance of pain.This relationship has been firmly established by research.
Patients' fear of pain, their interpretation of what the pain means and itslikely effect on their lives, have become important targets for therapy.
Patient Assessment
Comprehensive assessment of pain requires protected time with the personand consideration of the following domains:
• Physical effects/manifestations
• Functional effects
• Interference with activities of daily living
o Weight gain/losso Sit from standing and vice versao Dress and undress unaidedo Walk with easeo Employment/unemploymento Unresolved litigation issues
• Psychosocial factors
o Level of anxietyo Moodo Cultural influenceso Fearso Effects on interpersonal relationshipso Factors affecting pain thresholds
• Spiritual aspects
o This relates to the meaning of purpose ie "why am I experiencingsuch pain"? It does not always include a religious component.(SIGN Guideline 44, 2000)

Management of chronic pain in adults
1
Sect
ion
1:
Init
ial A
sses
smen
t
Key
Po
ints
~
1Peo
ple
wit
h ch
ron
ic p
ain
nee
d t
o ha
ve u
nder
gon
e a c
ompre
hen
sive
med
ical
ass
essm
ent
to e
nsu
re n
o u
nkn
own
un
der
lyin
g path
olog
ical
pro
cess
acc
oun
ts f
or t
heir
sym
pto
ms.
Thi
s is
ess
enti
al.
2Com
pre
hen
sive
ass
essm
ent
of t
he p
erso
n a
nd t
heir
pain
is
nec
essa
ry t
o in
crea
se t
he l
ikel
ihoo
d o
f su
cces
sfu
l m
an
age
men
t.
3Chr
onic
pain
is
a m
ultid
imen
sion
al
phe
nom
enon
an
d m
an
age
men
t m
ust
addre
ss a
ll a
spec
ts (
Ru
cker
et
al
1996).
4The
per
son
’s se
lf-r
epor
t of
pain
will
be c
onsi
der
ed a
n a
ccu
rate
acc
oun
t of
the
ir p
ain
(So
lom
on 2
001)
.
Nur
ses
& A
HPs
und
erst
and
the
mul
tidim
ensi
onal
nat
ure
ofch
roni
c p
ain
and
its c
omp
onen
t fe
atur
es.
Form
alis
ed a
sses
smen
t to
ols
that
are
ap
pro
pria
te f
or t
hein
divi
dual
are
use
d to
ass
ess
the
per
son
and
thei
r p
ain
(Bou
rbon
nais
et
al 2
004)
.
Onc
e p
ain
is r
epor
ted,
a c
omp
rehe
nsiv
e as
sess
men
t of
the
imp
act
of p
ain
on t
he p
erso
n is
und
erta
ken
and
am
anag
emen
t p
lan
deve
lop
ed.
Ther
e is
evi
denc
e of
loca
lly a
gree
d m
ulti
- di
men
sion
al p
ain
asse
ssm
ent
tool
s be
ing
used
to
dete
rmin
e m
anag
emen
tst
rate
gies
. To
ols
shou
ld b
e ap
pro
pria
te f
or e
ach
indi
vidu
alp
erso
n.
See
Ap
pen
dix
1 f
or
exam
ple
of
asse
ssm
ent
do
mai
ns
and
too
ls.
A p
ain
man
agem
ent
pla
n is
for
mul
ated
in p
artn
ersh
ip w
ithth
e p
erso
n.
A c
opy
of t
his
pla
n is
hel
d w
ithin
the
per
son’
sre
cord
s.
Stat
emen
tR
easo
ns
for
stat
emen
tH
ow
to
dem
on
stra
te s
tate
men
t is
bei
ng
ach
ieve
d
Acc
urat
e as
sess
men
t an
d in
divi
dual
man
agem
ent
of t
hep
erso
n w
ith c
hron
ic p
ain
(Tw
ycro
ss 2
000)
.
Mul
tidim
ensi
onal
ass
essm
ent
tool
s m
ust
refle
ct t
he h
olis
ticp
heno
men
on o
f ch
roni
c p
ain
(Dav
ies
& M
cVic
ar 2
000)
.
Ong
oing
ass
essm
ent
will
hel
p e
valu
ate
trea
tmen
tin
terv
entio
ns (
Turk
& B
urw
inkl
e 20
05).
Peop
le w
ith c
hron
ic p
ain
may
hav
e m
ultip
le n
eeds
.Su
cces
sful
man
agem
ent
dep
ends
on
com
pre
hens
ive
and
accu
rate
ass
essm
ent
and
reas
sess
men
t (d
eWit
et a
l 199
9).
Poin
ts t
o c
on
sid
er w
hen
tak
ing
a p
atie
nt’
s p
ain
his
tory
•Th
e si
te o
f p
ain
– W
here
do
you
feel
the
pai
n?
•W
here
doe
s it
radi
ate
to?
•N
atur
e of
pai
n –
Spee
d of
ons
et,
is it
inte
rmitt
ent
orp
ersi
sten
t?•
Cha
ract
eris
tics
of p
ain
– D
escr
ibe
wha
t th
e p
ain
feel
slik
e, e
g, is
the
pai
n bu
rnin
g, s
hoot
ing,
dul
l?•
His
tory
of
pai
n –
Ons
et a
nd d
urat
ion,
how
long
hav
eyo
u ha
d th
is p
ain?
•A
llevi
atin
g/ex
acer
batin
g fa
ctor
s –
Wha
t do
you
do
that
mak
es it
bet
ter
or w
orse
?
2
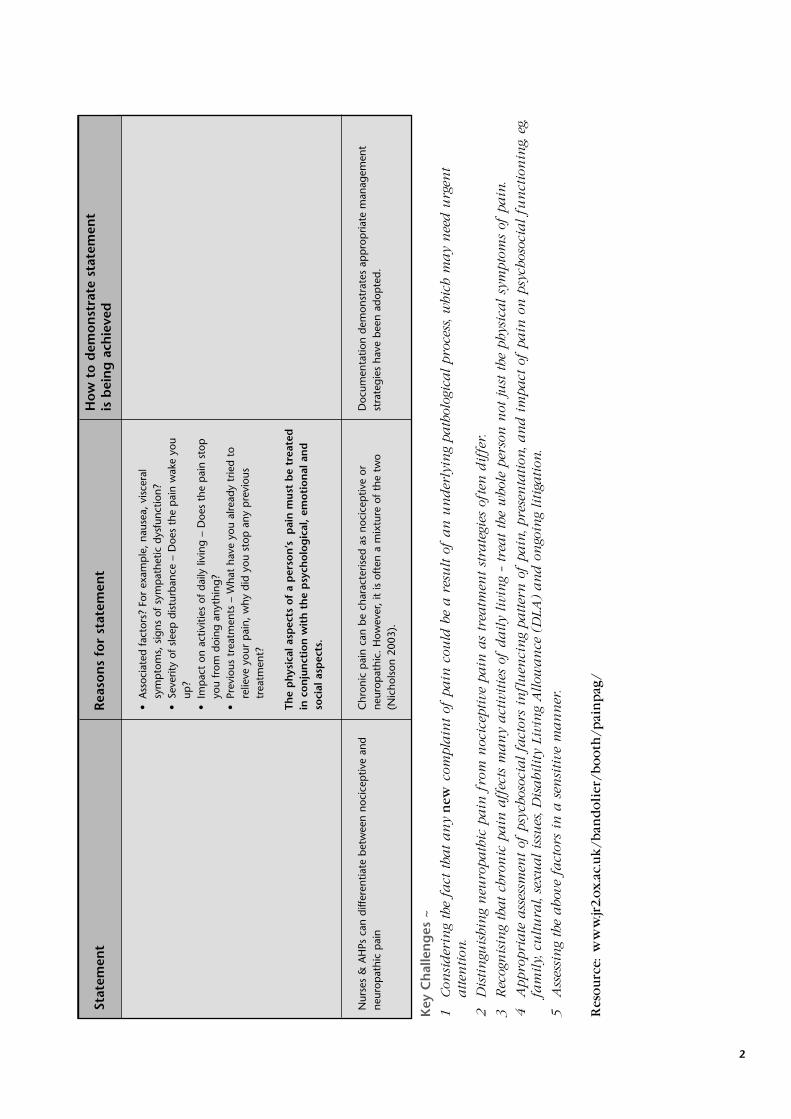
Nur
ses
& A
HPs
can
diff
eren
tiate
bet
wee
n no
cice
ptiv
e an
dne
urop
athi
c p
ain
Doc
umen
tatio
n de
mon
stra
tes
app
rop
riate
man
agem
ent
stra
tegi
es h
ave
been
ado
pte
d.
Stat
emen
tR
easo
ns
for
stat
emen
tH
ow
to
dem
on
stra
te s
tate
men
t is
bei
ng
ach
ieve
d
•A
ssoc
iate
d fa
ctor
s? F
or e
xam
ple
, na
usea
, vi
scer
alsy
mp
tom
s, s
igns
of
sym
pat
hetic
dys
func
tion?
•Se
verit
y of
sle
ep d
istu
rban
ce –
Doe
s th
e p
ain
wak
e yo
uup
?•
Imp
act
on a
ctiv
ities
of
daily
livi
ng –
Doe
s th
e p
ain
stop
you
from
doi
ng a
nyth
ing?
•Pr
evio
us t
reat
men
ts –
Wha
t ha
ve y
ou a
lread
y tr
ied
tore
lieve
you
r p
ain,
why
did
you
sto
p a
ny p
revi
ous
trea
tmen
t?
The
ph
ysic
al a
spec
ts o
f a
per
son
’s
pai
n m
ust
be
trea
ted
in c
on
jun
ctio
n w
ith
th
e p
sych
olo
gic
al,
emo
tio
nal
an
dso
cial
asp
ects
.
Chr
onic
pai
n ca
n be
cha
ract
eris
ed a
s no
cice
ptiv
e or
neur
opat
hic.
How
ever
, it
is o
ften
a m
ixtu
re o
f th
e tw
o(N
icho
lson
200
3).
Key
Ch
alle
ng
es ~
1Con
sider
ing
the
fact
tha
t an
y n
ew
com
pla
int
of p
ain
cou
ld b
e a r
esu
lt o
f an
un
der
lyin
g path
olog
ical
pro
cess
, whi
ch m
ay
nee
d u
rgen
tatten
tion
.
2 D
isti
ngu
ishi
ng
neu
ropath
ic p
ain
fro
m n
ocic
epti
ve p
ain
as
trea
tmen
t st
rate
gies
oft
en d
iffe
r.
3 R
ecog
nis
ing
that
chro
nic
pain
aff
ects
man
y act
ivit
ies
of d
aily
livi
ng
– tr
eat
the
who
le p
erso
n n
ot ju
st t
he p
hysi
cal
sym
pto
ms
of p
ain
.
4
Appro
pri
ate
ass
essm
ent
of p
sych
osoc
ial
fact
ors
infl
uen
cin
g patter
n o
f pain
, pre
sen
tati
on, a
nd i
mpact
of
pain
on
psy
chos
ocia
l fu
nct
ion
ing, e
g,fa
mily,
cu
ltu
ral,
sexu
al
issu
es, D
isabi
lity
Liv
ing
Allow
an
ce (
DLA
) an
d o
ngo
ing
liti
gati
on.
5 A
sses
sin
g th
e abo
ve f
act
ors
in a
sen
siti
ve m
an
ner
.
Re
sou
rce
: w
ww
.jr2
.ox
.ac
.uk
/b
an
do
lie
r/b
oo
th/
pa
inp
ag
/
Management of chronic pain in adults
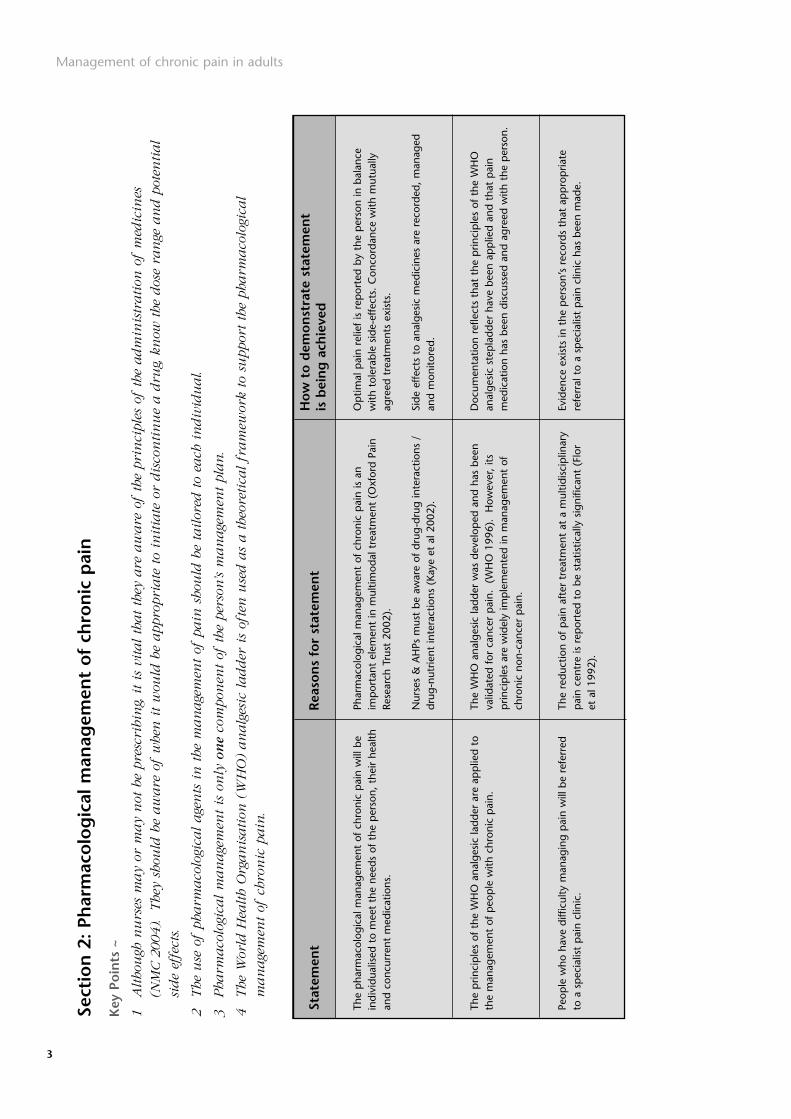
3
Sect
ion
2:
Phar
mac
olo
gic
al m
anag
emen
t o
f ch
ron
ic p
ain
Key
Po
ints
~
1A
ltho
ugh
nu
rses
may
or m
ay
not
be
pre
scri
bin
g, i
t is
vit
al
that
they
are
aw
are
of
the
pri
nci
ple
s of
the
adm
inis
trati
on o
f m
edic
ines
(N
MC 2
004).
The
y sh
ould
be
aw
are
of
whe
n i
t w
ould
be
appro
pri
ate
to
init
iate
or
dis
con
tin
ue
a d
rug, k
now
the
dos
e ra
nge
an
d p
oten
tial
side
effe
cts.
2The
use
of
pha
rmaco
logi
cal
age
nts
in
the
man
age
men
t of
pain
sho
uld
be
tailor
ed t
o ea
ch i
ndiv
idu
al.
3Pha
rmaco
logi
cal
man
age
men
t is
on
ly o
ne
com
pon
ent
of t
he p
erso
n’s
man
age
men
t pla
n.
4The
Wor
ld H
ealth
Org
an
isati
on (
WH
O)
an
alg
esic
ladder
is
ofte
n u
sed a
s a t
heor
etic
al
fram
ewor
k to
su
ppor
t th
e pha
rmaco
logi
cal
man
age
men
t of
chr
onic
pain
.
The
pha
rmac
olog
ical
man
agem
ent
of c
hron
ic p
ain
will
be
indi
vidu
alis
ed t
o m
eet
the
need
s of
the
per
son,
the
ir he
alth
and
conc
urre
nt m
edic
atio
ns.
The
prin
cip
les
of t
he W
HO
ana
lges
ic la
dder
are
ap
plie
d to
the
man
agem
ent
of p
eop
le w
ith c
hron
ic p
ain.
Peop
le w
ho h
ave
diffi
culty
man
agin
g p
ain
will
be
refe
rred
to a
sp
ecia
list
pai
n cl
inic
.
Op
timal
pai
n re
lief
is r
epor
ted
by t
he p
erso
n in
bal
ance
with
tol
erab
le s
ide-
effe
cts.
Con
cord
ance
with
mut
ually
agre
ed t
reat
men
ts e
xist
s.
Side
effe
cts
to a
nalg
esic
med
icin
es a
re r
ecor
ded,
man
aged
and
mon
itore
d.
Doc
umen
tatio
n re
flect
s th
at t
he p
rinci
ple
s of
the
WH
Oan
alge
sic
step
ladd
er h
ave
been
ap
plie
d an
d th
at p
ain
med
icat
ion
has
been
dis
cuss
ed a
nd a
gree
d w
ith t
he p
erso
n.
Evid
ence
exi
sts
in t
he p
erso
n’s
reco
rds
that
ap
pro
pria
tere
ferr
al t
o a
spec
ialis
t p
ain
clin
ic h
as b
een
mad
e.
Stat
emen
tR
easo
ns
for
stat
emen
tH
ow
to
dem
on
stra
te s
tate
men
t is
bei
ng
ach
ieve
d
Phar
mac
olog
ical
man
agem
ent
of c
hron
ic p
ain
is a
nim
por
tant
ele
men
t in
mul
timod
al t
reat
men
t (O
xfor
d Pa
inRe
sear
ch T
rust
200
2).
Nur
ses
& A
HPs
mus
t be
aw
are
of d
rug-
drug
inte
ract
ions
/dr
ug-n
utrie
nt in
tera
ctio
ns (
Kaye
et
al 2
002)
.
The
WH
O a
nalg
esic
ladd
er w
as d
evel
oped
and
has
bee
nva
lidat
ed f
or c
ance
r p
ain.
(W
HO
199
6).
How
ever
, its
prin
cip
les
are
wid
ely
imp
lem
ente
d in
man
agem
ent
ofch
roni
c no
n-ca
ncer
pai
n.
The
redu
ctio
n of
pai
n af
ter
trea
tmen
t at
a m
ultid
isci
plin
ary
pai
n ce
ntre
is r
epor
ted
to b
e st
atis
tical
ly s
igni
fican
t (F
lor
et a
l 199
2).

4
Key
Ch
alle
ng
es ~
1M
isco
nce
pti
ons
exis
t re
gard
ing
the
pha
rmaco
logi
cal
trea
tmen
ts o
f ch
ron
ic p
ain
, whi
ch c
an
be
a b
arr
ier
to s
ucc
essf
ul
man
age
men
t.
2In
form
ing
peo
ple
of
the
indic
ati
ons,
side
effe
cts
an
d b
enef
its
of t
heir
med
icati
on i
n a
way
that
is c
learl
y u
nder
stoo
d.
3A
na
lges
ic m
edic
ines
are
oft
en u
sed
ou
twit
h l
icen
sed
in
dic
ati
on
san
d a
ppro
pri
ate
in
form
ati
on a
bou
t ri
sks
an
d b
enef
its
for
pati
ents
an
dhe
althc
are
pro
fess
ion
als
req
uir
es t
o be
made
ava
ilabl
e.
Lice
nse
d p
rodu
cts
shou
ld b
e u
sed w
here
pos
sibl
e.
4To
en
sure
the
pati
ent
pro
gres
ses
up t
he l
adder
to
the
appro
pri
ate
lev
el. (
Bri
tish
Pain
Soc
iety
2004).
5R
ecog
nis
ing
that
othe
r in
terv
enti
ons
may
cau
se a
red
uct
ion
in
an
alg
esic
s n
eeded
.
INC
RE
AS
ING
PA
IN
No
no
pio
id
Ad
juva
nt
1
2
Op
ioid
fo
r M
od
era
te t
o S
eve
re P
ain
No
no
pio
id A
dju
va
nt
3
No
no
pio
id A
dju
va
nt
Op
ioid
fo
r M
ild t
o M
od
era
te P
ain
Figu
re 3
Adap
ted f
rom
WH
O 1
996

Management of chronic pain in adults
5
Sect
ion
3:
Un
con
ven
tio
nal
an
alg
esic
s (A
dju
van
ts)
Thes
e ar
e dr
ugs,
whi
ch a
re n
ot n
orm
ally
con
side
red
anal
gesi
cs,
but
they
hav
e a
prim
ary
role
in o
ther
con
ditio
ns.
The
y ar
e us
ed a
s ad
juva
nt t
reat
men
ts in
the
man
agem
ent
of p
ain
(McQ
uay
et a
l 199
6).
Key
Po
ints
~
1A
tri
al
of u
nco
nve
nti
onal
an
alg
esic
s sh
ould
be
con
sider
ed i
f th
e pati
ent
des
crib
es d
iffi
culty
in m
an
agi
ng
pain
.
2N
euro
path
ic p
ain
can
be
trea
ted b
y u
nco
nve
nti
onal
an
alg
esic
s eg
an
tidep
ress
an
ts, a
nti
con
vuls
an
ts a
s w
ell
as
con
ven
tion
al
med
icati
ons
egop
ioid
s.
3Tri
cycl
ic a
nti
dep
ress
an
ts a
re t
he p
refe
rred
in
itia
l th
erapy
in n
euro
path
ic p
ain
.
4U
nco
nve
nti
onal
an
alg
esic
s m
ay
be e
ffec
tive
at
dos
es w
hich
may
be l
ower
tha
n t
hose
use
d f
or t
heir
pri
mary
in
dic
ati
on.
Ta
ble
1
Fir
st-l
ine
me
dic
ati
on
s fo
r n
eu
rop
ath
ic p
ain
ad
ap
ted
fro
m D
wo
rkin
et
al
20
03
Tric
yclic
an
tid
epre
ssan
tssh
ould
be
cons
ider
ed f
orne
urop
athi
c p
ain.
An
tico
nvu
lsan
tssh
ould
be
cons
ider
ed f
or n
euro
pat
hic
pai
n.
Tram
ado
lsho
uld
be c
onsi
dere
d fo
r ne
urop
athi
c p
ain.
Star
ting
dose
10
– 25
mgs
eve
ry n
ight
.D
urat
ion
of a
deq
uate
tra
il 6
– 8
wee
ks a
t m
axim
umto
lera
ted
dosa
ge (
Dw
orki
n et
al 2
003)
.
Star
ting
dose
100
– 3
00m
gs e
very
nig
ht o
r 10
0 –
300m
gs 3
tim
es a
day
.In
crea
se b
y 10
0 –
300m
gs e
very
1 –
7 d
ays
as t
oler
ated
.D
urat
ion
of a
deq
uate
tria
l 3 –
8 w
eeks
for
titr
atio
n p
lus
1 –
2 w
eeks
at
max
imum
tol
erat
ed d
osag
e (D
wor
kin
et a
l 200
3).
Star
ting
dose
50m
gs o
nce
or t
wic
e da
ily.
Incr
ease
d by
50
– 1
00m
gs in
div
ided
dos
es e
very
3 –
7 d
ays
as t
oler
ated
.
Dur
atio
n of
ade
qua
te t
rial 4
wee
ks (
Dw
orki
n et
al 2
003)
.
Med
icat
ion
Evid
ence
Co
mm
ents
Tric
yclic
an
tid
epre
ssan
tsar
eth
ough
t to
be
effe
ctiv
etr
eatm
ent
for
neur
opat
hic
pai
n. T
he b
est
avai
labl
eev
iden
ce is
for
am
itrip
tylin
e (S
aart
o &
Wiff
en 2
005)
.
Gab
apen
tin
is t
houg
ht t
o be
effe
ctiv
e in
chr
onic
neur
opat
hic
pai
n (W
iffen
et
al 2
005)
.
Tram
ado
lis
thou
ght
to h
ave
a th
erap
eutic
effe
ct o
np
arae
sthe
siae
, al
lody
nia
and
touc
h ev
oked
pai
n.
It is
cons
ider
ed a
n ef
fect
ive
trea
tmen
t fo
r ne
urop
athi
c p
ain
(Duh
mke
et
al 2
005)
.

6
Un
con
ven
tio
nal
an
alg
esic
s (A
dju
van
ts)
Nur
ses
and
AH
Ps u
nder
stan
d th
e re
ason
s fo
r us
ing
unco
nven
tiona
l ana
lges
ic in
pai
n st
ates
eg
neur
opat
hic
pai
n.
Ther
e is
evi
denc
e in
the
per
son’
s re
cord
to
show
tha
t th
ese
unco
nven
tiona
l ana
lges
ics
have
bee
n co
nsid
ered
in a
syst
emat
ic w
ay.
Op
timal
pai
n re
lief
is r
epor
ted
by t
he p
erso
n in
bal
ance
with
tol
erab
le s
ide-
effe
cts.
Con
cord
ance
with
mut
ually
agre
ed t
reat
men
ts e
xist
s.
Side
effe
cts
to a
nalg
esic
med
icin
es a
re r
ecor
ded,
man
aged
and
mon
itore
d.
Stat
emen
tR
easo
ns
for
stat
emen
tH
ow
to
dem
on
stra
te s
tate
men
t is
bei
ng
ach
ieve
d
Ther
e is
str
ong
evid
ence
tha
t bo
th a
ntid
epre
ssan
ts a
ndan
ticon
vuls
ants
are
effe
ctiv
e in
pai
n st
ates
(Sa
arto
& W
iffen
2005
, W
iffen
et
al 2
005)
.
Key
Ch
alle
ng
es ~
1In
form
ing
pati
ents
of
the
indic
ati
ons,
side
effe
cts
an
d b
enef
its
of t
heir
med
icati
on i
n a
n a
cces
sibl
e fo
rmat.
2U
nder
stan
din
g th
e ri
sks
ben
efit
rati
os a
ssoc
iate
d w
ith
med
icati
ons
eg a
nti
con
vuls
an
ts.
3U
nco
nve
nti
onal
an
alg
esic
med
icin
es a
re o
ften
use
d o
utw
ith
lice
nse
d i
ndic
ati
ons,
an
d a
ppro
pri
ate
in
form
ati
on a
bou
t ri
sks
an
d b
enef
its
for
pati
ents
an
d h
ealthc
are
pro
fess
ion
als
req
uir
es t
o be
made
ava
ilabl
e.
Lice
nse
d p
rodu
cts
shou
ld b
e u
sed w
here
pos
sibl
e.
4
Chr
onic
pain
may
be a
n u
nlice
nse
d i
ndic
ati
on f
or m
ost
of t
hese
med
icin
es a
nd t
he p
ati
ent
info
rmati
on l
eafl
et, w
hich
is
issu
ed a
t th
e poi
nt
ofdis
pen
sin
g, m
ay
not
con
tain
rel
evan
t in
form
ati
on f
or t
he c
ondit
ion
bei
ng
trea
ted.
Th
e in
form
ati
on
pro
vid
ed m
ay
be
con
fusi
ng
.

Management of chronic pain in adults
7
Sect
ion
4:
The
use
of
op
ioid
s in
th
e m
anag
emen
t o
f ch
ron
ic n
on
-mal
ign
ant
pai
n
Key
Po
ints
~
1O
pio
id m
edic
ati
on m
ay
not
be
suit
abl
e or
eff
ecti
ve f
or s
ome
peo
ple
wit
h ch
ron
ic p
ain
.
2The
cho
ice
of o
pio
id m
edic
ati
on d
epen
ds
on c
lin
ical
circ
um
stan
ces.
A p
hysi
cal,
psy
chol
ogic
al a
nd s
ocia
l ass
essm
ent
isun
dert
aken
bef
ore
star
ting
the
per
son
on lo
ng-t
erm
op
ioid
med
icat
ion.
The
per
son
with
chr
onic
pai
n w
ill b
e fu
lly in
form
ed o
f th
eir
trea
tmen
t p
lan
befo
re c
omm
enci
ng o
pio
id t
hera
py.
Peop
le w
ith c
hron
ic p
ain
rece
ivin
g op
ioid
med
icat
ion
are
clos
ely
mon
itore
d du
ring
dose
titr
atio
n.
Doc
umen
tatio
n re
flect
s ap
pro
pria
te p
resc
ribin
g an
dev
alua
tion
of t
reat
men
t.
The
per
son
is c
onco
rdan
t w
ith t
reat
men
t.
Ther
e is
evi
denc
e th
at t
he u
se o
f op
ioid
s an
d p
oten
tial s
ide-
effe
cts
have
bee
n di
scus
sed
and
agre
ed b
etw
een
the
per
son
and
the
heat
h p
rofe
ssio
nal.
Stat
emen
tR
easo
ns
for
stat
emen
tH
ow
to
dem
on
stra
te s
tate
men
t is
bei
ng
ach
ieve
d
Som
e p
eop
le w
ith c
hron
ic p
ain
can
atta
in f
avou
rabl
eou
tcom
es f
or p
rolo
nged
per
iods
usi
ng o
pio
id m
edic
ines
(Por
teno
y 19
96).
To a
ssis
t th
e p
atie
nt t
o m
ake
as in
form
ed a
cho
ice
aspo
ssib
le a
bout
ben
efits
and
ris
ks (
Briti
sh P
ain
soci
ety
2005
).
Plea
se r
efer
to
th
e R
eco
mm
end
atio
ns
for
the
app
rop
riat
e us
e o
f o
pio
ids
for
per
sist
ent
no
n-c
ance
rp
ain
. T
he
Bri
tish
Pai
n S
oci
ety
2004
ww
w.b
riti
shp
ain
soci
ety.
org
/pd
f/Pu
b_F
inal
_op
ioid
_mar
ch
%20
2005
.pd
f
Key
Ch
alle
ng
es ~
1En
suri
ng
pati
ents
are
in
form
ed t
hat
inje
ctabl
e op
ioid
s are
rare
ly a
ppro
pri
ate
for
per
sist
ent
non
-can
cer
pain
(B
riti
sh P
ain
Soc
iety
2004).

8
Sect
ion
5:
The
mul
tid
isci
plin
ary
app
roac
h t
o p
ain
man
agem
ent
in p
rim
ary
care
Key
Po
ints
~
1Peo
ple
wit
h ch
ron
ic p
ain
oft
en h
ave
mu
ltip
le f
act
ors
that
con
trib
ute
to
pain
.
2A
mu
ltid
isci
plin
ary
appro
ach
may
be n
eces
sary
for
peo
ple
wit
h co
mple
x n
eeds.
3N
ot a
ll p
ati
ents
wit
h ch
ron
ic p
ain
req
uir
e fu
ll m
ultid
isci
plin
ary
care
.
Med
ical
Pra
ctiti
oner
Nur
se
Phys
ioth
erap
ist
Psyc
holo
gist
Phar
mac
ist
Occ
upat
iona
l The
rap
ist
Psyc
hiat
ric S
ervi
ces
The
role
invo
lves
tak
ing
a de
taile
d hi
stor
y, m
edic
al e
xam
inat
ion,
ass
essi
ng,
co-o
rdin
atin
g th
e ap
pro
pria
te m
anag
emen
t st
rate
gy f
or p
atie
nts
with
ref
erra
l to
othe
r m
embe
rs o
f th
e te
am o
r ot
her
spec
ialis
ts;
agre
eing
and
rev
iew
ing
clin
ical
man
agem
ent
pla
ns.
The
nurs
e’s
role
invo
lves
a n
ursi
ng a
sses
smen
t, r
unni
ng n
urse
led
clin
ics,
TEN
S, a
cup
unct
ure,
sle
ep m
anag
emen
t, f
ollo
win
g up
on
med
icat
ion
regi
men
s, e
duca
tion,
cou
nsel
ling,
col
lect
ing
and
orga
nisi
ng p
atie
nt d
ata.
The
man
agem
ent
pla
n in
clud
es r
eass
essm
ent
and
educ
atio
n; a
dvic
e on
pac
ing
and
goal
set
ting;
and
fac
ilita
tion
of m
ovem
ent
and
exer
cise
with
the
aim
of
optim
isin
g p
hysi
cal f
itnes
s, a
ctiv
ity a
nd p
artic
ipat
ion.
Poor
ly m
anag
ed c
hron
ic p
ain
can
gene
rate
fee
lings
of
dist
ress
, ho
pel
essn
ess
and
desp
air,
psy
chol
ogic
al in
terv
entio
ns h
ave
been
dem
onst
rate
dto
be
effe
ctiv
e (M
orel
y et
al 1
999)
.
As
par
t of
the
mul
tidis
cip
linar
y te
am p
harm
acis
ts c
an e
valu
ate
med
icat
ion
regi
men
s to
gua
rd a
gain
st d
rug
inte
ract
ions
, ad
vers
e ef
fect
s an
ddu
plic
atio
n in
the
rap
y.
Phar
mac
ists
can
als
o di
scus
s p
reco
ncei
ved
fear
s as
soci
ated
with
ana
lges
ic,
asse
ssin
g co
mp
lianc
e an
d ad
visi
ng o
nap
pro
pria
te c
omp
lianc
e ai
ds.
Ass
essm
ent
and
trea
tmen
t is
foc
used
on
enab
ling
occu
pat
ion,
whi
ch in
tur
n ca
n le
ad t
o an
imp
rove
men
t in
qua
lity
of li
fe.
Anx
iety
and
dep
ress
ion
is c
omm
on in
chr
onic
pai
n p
atie
nts,
and
can
be
deal
t w
ith b
y p
sych
olog
y.
Psyc
hiat
ric o
pin
ion
shou
ld b
e so
ught
par
ticul
arly
in r
elat
ion
to m
anag
emen
t of
sui
cide
ris
k an
d re
sist
ant
seve
re m
edic
al d
epre
ssio
n.
Key
Ch
alle
ng
es ~
1The
re i
s n
o co
mm
only
acc
epte
d s
tan
dard
mu
ltid
isci
plin
ary
appro
ach
to
chro
nic
pain
.
2A
ll p
ract
ices
may
not
have
acc
ess
to a
ll d
isci
plin
es, t
here
fore
, altho
ugh
not
idea
l, so
me
role
s m
ay
be i
nte
rcha
nge
abl
e.
3En
suri
ng
a u
nif
ied a
ppro
ach
.
4U
nder
stan
din
g th
e lim
itati
ons
of e
ach
rol
e in
the
tea
m.

Management of chronic pain in adults
9
Sect
ion
5 (
i) R
ole
of
the
Nur
se
Key
Po
ints
~
1N
urs
es u
nder
take
a v
ari
ety
of r
oles
whi
ch s
hou
ld b
e vi
ewed
wit
hin
the
con
text
of t
he m
ultid
isci
plin
ary
tea
m. T
hese
can
vary
fro
m r
un
nin
g a
Tra
nsc
uta
neo
us
elec
tric
al
ner
ve s
tim
ula
tor
(TEN
S) c
lin
ic t
o cl
inic
al
ass
essm
ent,
med
icati
on r
evie
w a
nd c
ogn
itiv
e be
havi
oura
l th
erapy.
2N
urs
es r
equ
ire
know
ledge
of
both
pha
rmaco
logi
c an
d n
on-p
harm
aco
logi
c in
terv
enti
ons
an
d t
he a
pplica
tion
of
this
kn
owle
dge
thr
ough
su
chact
ivit
ies
as
ass
essm
ent,
teach
ing, m
onit
orin
g, p
ati
ent
self
–man
age
men
t an
d c
o-or
din
ati
ng
care
am
ong
health
care
pro
vider
s.
3N
urs
es a
re i
n a
n i
dea
l pos
itio
n t
o fo
cus
on i
nte
rven
tion
s th
at
help
the
per
son
take
an
act
ive
role
in
the
ir c
are
an
d m
ain
tain
as
mu
chin
dep
enden
ce a
s pos
sibl
e.
Nur
ses
unde
rsta
nd t
he n
eed
for
regu
lar
pai
n as
sess
men
tan
d re
asse
ssm
ent,
and
hav
e an
aw
aren
ess
of t
hep
rofe
ssio
nal/
lega
l res
pon
sibi
litie
s re
late
d to
pai
nm
anag
emen
t.
Nur
ses
can
imp
lem
ent
a cl
inic
al m
anag
emen
t p
lan/
care
pla
n fo
r th
e re
lief
of p
ain
in p
artn
ersh
ip w
ith t
he p
atie
ntan
d w
ithin
the
con
text
of
the
mul
tidis
cip
linar
y te
am.
Nur
ses
dem
onst
rate
an
abili
ty t
o lia
ise
succ
essf
ully
with
othe
r ag
enci
es.
The
nurs
e de
mon
stra
tes
clin
ical
and
inte
rper
sona
l ski
lls t
oas
sess
and
rel
ieve
pai
n an
d m
easu
res
outc
omes
by
clin
ical
audi
t.
Ther
e is
evi
denc
e th
at a
n ac
tion
pla
n/ca
re p
lan
has
been
form
ulat
ed,
imp
lem
ente
d an
d ev
alua
ted.
The
docu
men
tatio
n re
flect
s th
at t
he n
eces
sary
age
ncie
sha
ve b
een
invo
lved
.
Stat
emen
tR
easo
ns
for
stat
emen
tH
ow
to
dem
on
stra
te s
tate
men
t is
bei
ng
ach
ieve
d
Nur
ses
rout
inel
y p
erfo
rm a
sses
smen
t of
pai
n in
tens
ity a
ndad
min
istr
atio
n of
ana
lges
ics.
(M
cCaf
fery
et
al 2
000,
NM
C20
04).
Effe
ctiv
e p
ain
man
agem
ent
is in
extr
icab
ly li
nked
to
deci
sion
s nu
rses
are
req
uire
d to
mak
e in
dai
ly p
ract
ice
(Van
Nie
kerk
and
Mar
tin 2
003,
Pel
lino
et a
l 200
2).
Com
mun
icat
ion,
col
labo
ratio
n an
d p
atie
nt a
dvoc
acy
are
fund
amen
tal n
ursi
ng a
ctiv
ities
(N
MC
200
4).
Key
Ch
alle
ng
es ~
1U
nder
stan
din
g th
e br
eadth
an
d l
imit
ati
ons
of t
he s
kills
requ
ired
to
be a
n e
ffec
tive
pra
ctit
ion
er.
2Pro
vidin
g su
ffic
ien
t ti
me
to s
pen
d w
ith
the
per
son
to
un
der
take
com
pre
hen
sive
ass
essm
ent.

10
Sect
ion
5 (
ii) R
ole
of
ph
ysio
ther
apy
Key
Po
ints
~
1Peo
ple
wit
h ch
ron
ic p
ain
oft
en h
ave
pro
blem
s w
ith
phy
sica
l fi
tnes
s.
2A
ctiv
ity
lim
itati
on (
pro
blem
s w
ith
the
capaci
ty t
o ca
rry
out
task
s or
act
ion
s), i
s of
ten
a p
robl
em f
or p
eople
wit
h ch
ron
ic p
ain
.
3Part
icip
ati
on r
estr
icti
on (
pro
blem
s w
ith
per
form
an
ce o
r in
volv
emen
t in
soc
ial
situ
ati
ons)
, is
ofte
n a
pro
blem
for
peo
ple
wit
h ch
ron
ic p
ain
.
4Pro
mot
ion
of
mov
emen
t an
d e
xer
cise
can
main
tain
an
d i
mpro
ve p
hysi
cal
fitn
ess,
act
ivit
y an
d p
art
icip
ati
on f
or p
eople
wit
h ch
ron
ic p
ain
.
5A
s in
dep
enden
t pra
ctit
ion
ers,
phy
siot
hera
pis
ts h
ave
an
im
por
tan
t ro
le i
n a
sses
sin
g an
d m
an
agi
ng
pati
ents
wit
h pain
.
6Peo
ple
wit
h acu
te p
ain
or
chro
nic
pain
will
rou
tin
ely
be r
efer
red t
o ou
tpati
ent
phy
siot
hera
py
serv
ices
in
acu
te s
ites
an
d c
omm
un
ity
settin
gs.
Ass
essm
ent
of t
he im
pac
t of
pai
n on
fun
ctio
n (p
hysi
cal
fitne
ss,
activ
ity a
nd p
artic
ipat
ion)
is u
nder
take
n to
ass
ist
with
for
mul
atio
n of
a m
anag
emen
t p
lan.
The
man
agem
ent
pla
n in
clud
es r
eass
essm
ent
and
educ
atio
n; a
dvic
e on
pac
ing
and
goal
set
ting;
and
faci
litat
ion
of m
ovem
ent
and
exer
cise
with
the
aim
of
optim
isin
g p
hysi
cal f
itnes
s, a
ctiv
ity a
nd p
artic
ipat
ion.
The
per
son
with
chr
onic
pai
n is
invo
lved
in f
orm
ulat
ing
the
man
agem
ent
pla
n to
ens
ure
that
it is
rel
evan
t to
the
irne
eds.
Doc
umen
tatio
n re
flect
s th
at p
ain-
rela
ted
phy
sica
l dis
abili
tyha
s be
en m
easu
red
and
used
to
influ
ence
the
tre
atm
ent
pla
n.
Stat
emen
tR
easo
ns
for
stat
emen
tH
ow
to
dem
on
stra
te s
tate
men
t is
bei
ng
ach
ieve
d
Ass
essm
ent
of p
hysi
cal f
unct
ion
is a
cru
cial
ele
men
t in
the
form
ulat
ion
of a
n ac
cura
te d
iagn
osis
and
effe
ctiv
etr
eatm
ent
pla
n (S
trou
d et
al 2
004)
.
Key
Ch
alle
ng
es ~
1Phy
siot
hera
pis
ts n
eed t
o apply
a b
iopsy
chos
ocia
l appro
ach
to
the
man
age
men
t of
chr
onic
pain
.
"Incr
easi
ngl
y in S
cotlan
d, p
atie
nts
can
sel
f-re
fer
dir
ectly t
o p
hysi
oth
erap
y w
ithout
GP
refe
rral
. Se
lf-r
efer
ral bri
ngs
with it
a re
sponsi
bili
ty t
o t
riag
epat
ients
saf
ely a
nd e
ffic
iently.
A
key
res
ponsi
bili
ty is
to c
lass
ify t
he
nat
ure
of
the
pat
ient’s
pai
n a
nd inst
igat
e im
med
iate
appro
pri
ate
man
agem
ent.
For
exam
ple
, in G
lasg
ow, 7
00 n
ew p
atie
nts
pre
sent
to p
hysi
oth
erap
y e
ach m
onth
with low
bac
k p
ain.
Som
e of
thes
e pat
ients
will
hav
e neu
ropat
hic
pai
n w
hic
h r
equir
es s
pec
ific
med
icat
ion a
nd m
anag
emen
t. P
hysi
oth
erap
ists
can
iden
tify
this
conditio
n a
nd a
rran
geap
pro
pri
ate
med
icat
ion v
ia t
he
GP
oft
en r
esultin
g in
dra
mat
ic r
educt
ion in p
ain s
ym
pto
ms
and m
inim
isin
g th
e ch
ance
of
chro
nic
pai
ndev
elopin
g".
Mr.
M. M
cMen
emy,
Gla
sgow
Bac
kpai
n S
ervic
e

Management of chronic pain in adults
11
Sect
ion
5 (
iii):
Ro
le o
f p
sych
olo
gy
in t
he
man
agem
ent
of
chro
nic
pai
n
Key
Po
ints
~
1Psy
chol
ogic
al
fact
ors
aff
ect
the
neu
rophy
siol
ogic
al
an
d b
ioch
emic
al
asp
ects
of
the
pain
exper
ien
ce (
Pri
ce 1
999)
an
d c
an
adve
rsel
y aff
ect
the
effi
cacy
of
esta
blis
hed t
reatm
ents
(W
asa
n e
t al
2005)
.
2 Psy
chol
ogic
al
appro
ach
es t
o th
e m
an
age
men
t of
chr
onic
pain
in
clu
de
dif
fere
nt
inte
rven
tion
s aim
ed a
t en
abl
ing
an
in
div
idu
al
to d
evel
opst
rate
gies
to
man
age
the
ir t
hin
kin
g, b
ehavi
our
an
d e
mot
ion
in
res
pon
se t
o pain
.
3 Psy
chol
ogic
al
appro
ach
es c
an
be
on t
hree
lev
els
(Mow
bray
1989).
Lev
el o
ne
– (a
ll c
lin
icia
ns)
basi
c u
nder
stan
din
g of
psy
chol
ogic
al
pri
nci
ple
s, sk
ills
eg
good
the
rapeu
tic
rela
tion
ship
, lis
ten
ing
skills
.
Lev
el t
wo
(sp
ecif
ica
lly
tra
ined
cli
nic
ian
s)
applica
tion
of
psy
chol
ogic
al
tech
niq
ues
des
crib
ed b
y pro
toco
l (c
an
be
to h
igh
leve
l) e
g re
laxati
on, C
ogn
itiv
e B
ehavi
oura
l The
rapy
(CB
T)
pri
nci
ple
s, Pain
Man
age
men
t Pro
gram
me
(PM
P)
train
ing
to a
gree
d c
ompet
ency
ess
enti
al
an
d o
ngo
ing
super
visi
on f
rom
psy
chol
ogis
t to
en
sure
con
tin
uin
g co
mpet
ence
.
Lev
el t
hre
e (c
lin
ica
l a
nd
ap
pli
ed p
sych
olo
gis
ts)
applica
tion
of
psy
chol
ogic
al
pri
nci
ple
s an
d t
heor
ies.
Dis
cret
ion
ary
com
pon
ent
in d
ecis
ion
s as
to w
hat
to u
se a
nd w
hen
.Com
ple
x c
ase
s, in
div
idu
al,
grou
p a
nd g
rou
p p
roce
sses
, tra
inin
g ot
hers
.
Com
ple
x i
ssu
es s
uch
as
seve
re d
epre
ssio
n, p
ost-tr
au
mati
c st
ress
res
pon
se, v
uln
erabi
lity
du
e to
pre
viou
s life
exper
ien
ces,
will
infl
uen
ce p
ain
exper
ien
ce a
nd s
hou
ld o
nly
be
dea
lt w
ith
by
som
eon
e w
orki
ng
at
leve
l 3.
Psyc
holo
gica
l int
erve
ntio
ns c
an b
e p
rovi
ded
by in
divi
dual
sat
sp
ecifi
ed le
vels
of
com
pet
ence
with
ap
pro
pria
tesu
per
visi
on,
to e
nabl
e an
indi
vidu
al t
o de
velo
p t
heir
thin
king
, be
havi
our
and
emot
ion
in r
esp
onse
to
chro
nic
pai
n.
Patie
nts
rece
ive
cogn
itive
beh
avio
ural
tre
atm
ents
to
help
them
cop
e w
ith p
ain-
rela
ted
psy
chos
ocia
l pro
blem
s.
Ther
e is
doc
umen
ted
evid
ence
tha
t th
e p
atie
nt h
as b
een
offe
red
evid
ence
-bas
ed p
sych
olog
ical
inte
rven
tion.
Doc
umen
ted
evid
ence
sug
gest
s co
gniti
ve b
ehav
iour
alst
rate
gies
hav
e be
en c
onsi
dere
d.
Stat
emen
tR
easo
ns
for
stat
emen
tH
ow
to
dem
on
stra
te s
tate
men
t is
bei
ng
ach
ieve
d
Poor
ly m
anag
ed c
hron
ic p
ain
can
gene
rate
fee
lings
of
dist
ress
, ho
pel
essn
ess
and
desp
air,
psy
chol
ogic
alin
terv
entio
ns h
ave
been
dem
onst
rate
d to
be
effe
ctiv
e(M
orel
y et
al 1
999)
.
Cog
nitiv
e be
havi
oura
l str
ateg
ies
can
rest
ore
a se
nse
ofco
ntro
l and
imp
rove
cop
ing
abili
ty f
or p
eop
le w
ith c
hron
icp
ain
(Vla
eyen
& M
orle
y 20
05,
Mor
ley
et a
l 199
9).

12
Com
ple
x p
sych
olog
ical
pre
sent
atio
ns e
g su
icid
al id
eatio
n,p
ost
trau
mat
ic s
tres
s di
sord
er,
influ
ence
of
pre
viou
s ab
use,
is m
anag
ed b
y cl
inic
al p
sych
olog
ist
with
in p
ain
team
, or
refe
rred
to
app
rop
riate
men
tal h
ealth
ser
vice
.
Doc
umen
ted
evid
ence
of
refe
rral
to
app
rop
riate
ly q
ualif
ied
per
son/
serv
ice.
Stat
emen
tR
easo
ns
for
stat
emen
tH
ow
to
dem
on
stra
te s
tate
men
t is
bei
ng
ach
ieve
d
Thes
e fa
ctor
s w
ill h
ave
a si
gnifi
cant
imp
act
on o
utco
mes
and
pai
n ex
per
ienc
e, a
nd r
equi
re a
pp
rop
riate
tra
inin
g in
orde
r to
pro
vide
saf
e tr
eatm
ent.
(D
.O.H
. 20
01,
Trea
tmen
tch
oice
in p
sych
olog
ical
the
rap
ies
and
coun
selli
ng)
Key
Ch
alle
ng
es ~
1Pro
vidin
g appro
pri
ate
tra
inin
g an
d s
uper
visi
on f
or t
hose
wor
kin
g w
ith
psy
chol
ogic
al
pri
nci
ple
s (l
evel
2).
2A
cces
sin
g adeq
uate
res
ourc
es f
or p
sych
olog
ical
serv
ices
loc
ally
an
d t
imeo
usl
y (l
evel
3).
3A
dapti
ng
cogn
itiv
e be
havi
oura
l st
rate
gies
to
mee
t th
e n
eeds
of p
eople
wit
h co
gnit
ive
impair
men
ts.
4D
ealin
g w
ith
pati
ents
who
are
not
rea
dy
to e
mbr
ace
a p
sych
olog
ical
appro
ach
to
pain
man
age
men
t.

Management of chronic pain in adults
13
Sect
ion
5 (
iv):
Ro
le o
f O
ccup
atio
nal
Th
erap
y
Key
Po
ints
~
1The
foc
us
of i
nte
rven
tion
is
the
pro
mot
ion
of
occu
pati
on.
Occ
upati
on i
s def
ined
as
"daily
act
ivit
ies
that
refl
ect
cultu
ral
valu
es, p
rovi
de
stru
ctu
re t
o livi
ng
an
d m
ean
ing
to i
ndiv
idu
als
; the
se a
ctiv
itie
s m
eet
hum
an
nee
ds
for
self
-care
, en
joym
ent
an
d p
art
icip
ati
on i
n s
ocie
ty" (C
OT2
2004).
2A
sses
smen
t of
the
per
son
’s oc
cupati
onal
per
form
an
ce s
hou
ld b
e u
nder
take
n w
ithi
n a
ny
ass
essm
ent.
3A
tre
atm
ent
pla
n s
hou
ld b
e id
enti
fied
wit
h jo
int
goal-s
etti
ng.
4The
per
son
sho
uld
be
edu
cate
d o
n g
oal-s
etti
ng
pri
nci
ple
s an
d p
aci
ng
tech
niq
ues
as
tool
s to
part
icip
ati
on i
n o
ccu
pati
ons
rele
van
t to
his
/her
lif
e.
Ass
essm
ent
and
trea
tmen
t is
foc
used
on
enab
ling
occu
pat
ion,
whi
ch c
an le
ad t
o an
imp
rove
men
t in
qua
lity
of li
fe.
Inte
rven
tion
is u
nder
take
n w
ithin
the
fra
mew
ork
of a
mul
tidis
cip
linar
y ap
pro
ach
to p
ain
man
agem
ent.
The
per
son’
s p
rogr
ess
is d
ocum
ente
d an
d p
erfo
rman
cem
onito
red
with
reg
ular
rev
iew
.
Ap
pro
pria
te o
utco
me
mea
sure
s ar
e co
mp
lete
d be
fore
and
afte
r oc
cup
atio
nal t
hera
py
(Law
et
al 1
991)
.
The
occu
pat
iona
l the
rap
ist
has
read
and
com
plie
s w
ith t
heN
atio
nal O
ccup
atio
nal T
hera
py
Pain
Ass
ocia
tion
Gui
delin
eson
the
Rol
e of
Occ
upat
iona
l The
rap
y an
d M
inim
umRe
qui
rem
ents
for
Pra
ctic
e (P
ain
Soci
ety,
200
1).
Stat
emen
tR
easo
ns
for
stat
emen
tH
ow
to
dem
on
stra
te s
tate
men
t is
bei
ng
ach
ieve
d
An
occu
pat
iona
l beh
avio
ural
mod
el p
rovi
des
a ho
listic
pic
ture
of
the
per
son
with
chr
onic
pai
n. A
reh
abili
tativ
eap
pro
ach
to b
e ta
ken
with
em
pha
sis
on r
e-es
tabl
ishi
ngor
der
in t
he o
ccup
atio
nal f
unct
ioni
ng o
f th
e in
divi
dual
pat
ient
(St
rong
199
6).
A m
ultid
isci
plin
ary
team
ap
pro
ach
to c
hron
ic p
ain
is c
ost
effe
ctiv
e (W
adde
ll 19
96).
Key
Ch
alle
ng
es ~
1The
pro
visi
on o
f eq
uip
men
t an
d a
dapta
tion
s m
ust
pro
mot
e fu
nct
ion
al
abi
lity
an
d n
ot r
ein
forc
e fu
nct
ion
al
dis
abi
lity
.
2A
ddre
ssin
g so
cial
barr
iers
(phy
sica
l, or
gan
isati
onal,
cultu
ral
an
d a
ttit
udin
al)
to
occu
pati
onal
per
form
an
ce.
3Con
sider
ing
the
man
age
men
t of
ris
k w
hen
pro
mot
ing
occu
pati
onal
per
form
an
ce.

14
Sect
ion
5 (
v):
Psyc
hia
tric
Ser
vice
s
Key
Po
ints
~
1A
nxie
ty a
nd d
epre
ssio
n a
re c
omm
on i
n c
hron
ic p
ain
pati
ents
, an
d c
an
be
addre
ssed
by
psy
chol
ogy
serv
ices
. Psy
chia
tric
opin
ion
sho
uld
be
sou
ght,
part
icu
larl
y, i
n r
elati
on t
o m
an
age
men
t of
su
icid
e ri
sk a
nd r
esis
tan
t se
vere
med
ical
dep
ress
ion
.
2Illn
ess
beha
viou
r ca
n a
ffec
t pain
pati
ents
’ clin
ical
pre
sen
tati
on.
3So
mato
form
Dis
order
can
pre
sen
t in
a p
ain
clin
ic.
Key
Ch
alle
ng
es ~
1A
sses
sin
g pati
ents
in
a s
ensi
tive
an
d n
on-c
onfr
onta
tion
al
man
ner
whe
re p
ati
ents
may
be d
efen
sive
abo
ut
psy
chia
tric
con
tact
.

Management of chronic pain in adults
15
Sect
ion
6:
Pain
man
agem
ent
pro
gra
mm
es
Key
Po
ints
~
1Peo
ple
wit
h ch
ron
ic p
ain
nee
d t
he k
now
ledge
an
d s
kills
to b
e act
ivel
y in
volv
ed i
n s
elf-
man
age
men
t of
the
ir c
ondit
ion
.
2Fa
mily
suppor
t ca
n b
e an
im
por
tan
t fa
ctor
in
the
reh
abi
lita
tion
of
peo
ple
wit
h ch
ron
ic p
ain
.
3Pain
man
age
men
t pro
gram
mes
req
uir
e cl
ose
inte
rdis
ciplin
ary
wor
kin
g w
ith
all s
taff
en
gagi
ng
the
pri
nci
ple
s of
cog
nit
ive
beha
viou
ral
ther
apy.
4The
aim
s of
pain
man
age
men
t pro
gram
mes
are
to:
•im
pro
ve p
eople
’s u
nder
stan
din
g of
chr
onic
pain
an
d t
he r
elati
onsh
ip b
etw
een
pain
, em
otio
n a
nd b
ehavi
our
•im
pro
ve p
eople
’s le
vel
of p
hysi
cal,
soci
al,
pra
ctic
al
an
d e
mot
ion
al
fun
ctio
nin
g an
d c
onfi
den
ce
•re
du
ce f
ear
of m
ovem
ent
•pro
vide
copin
g st
rate
gies
for
dea
lin
g w
ith
thei
r dis
abi
lity
an
d d
istr
ess
•pro
mot
e au
ton
omy
an
d i
ndep
enden
ce
•re
du
ce o
r m
odif
y th
e per
son
’s fu
ture
use
of
healthc
are
res
ourc
es e
g, G
P a
ppoi
ntm
ents
, med
icati
on.
Pain
man
agem
ent
pro
gram
mes
incl
ude
all a
spec
ts o
f p
ain,
the
trea
tmen
t of
pai
n, p
ain
per
cep
tion,
psy
chol
ogic
al a
ndso
cial
fac
tors
.
Car
ers
or f
amily
mem
bers
are
act
ivel
y in
volv
ed in
the
man
agem
ent
of c
hron
ic p
ain
and
the
per
son’
sre
habi
litat
ion.
Pre
and
pos
t-p
rogr
amm
e as
sess
men
ts a
re c
omp
lete
d.
The
pat
ient
and
the
fam
ily/c
arer
rep
ort
imp
rove
d q
ualit
y of
life.
Stat
emen
tR
easo
ns
for
stat
emen
tH
ow
to
dem
on
stra
te s
tate
men
t is
bei
ng
ach
ieve
d
Pain
man
agem
ent
educ
atio
n p
rogr
amm
es h
ave
been
show
n to
red
uce
pai
n, a
nxie
ty,
dep
ress
ion,
imp
rove
trea
tmen
t ad
here
nce
and
faci
litat
e re
turn
to
wor
k (O
laso
n20
04).
Chr
onic
pai
n af
fect
s im
por
tant
bas
ic r
elat
ions
hip
s in
clud
ing
emot
iona
l and
phy
sica
l int
imac
y (S
mith
200
3).
Key
Ch
alle
ng
es ~
1En
suri
ng
pain
man
age
men
t pro
gram
mes
mee
t th
e des
irabl
e cr
iter
ia s
et b
y th
e B
riti
sh P
ain
Soc
iety
, (19
97,
cu
rren
tly
un
der
rev
iew
), in
clu
din
gm
inim
um
sta
ffin
g.
2En
suri
ng
pain
man
age
men
t pro
gram
mes
are
acc
essi
ble
to a
ll w
ho r
equ
ire
them
via
ref
erra
l to
spec
ialist
pain
man
age
men
t cl
inic
(M
cEw
enR
epor
t 20
04).
3En
suri
ng
appro
pri
ate
pati
ent
sele
ctio
n.
4A
cces
sin
g pain
man
age
men
t pro
gram
mes
.
Re
sou
rce
: ww
w.b
riti
shp
ain
soc
iety
.org
/p
df/
de
sira
ble
.pd
f

16
Sect
ion
7:
Self
-man
agem
ent/
sup
po
rt g
roup
s
Key
Po
ints
~
1So
me
self
-man
age
men
t gr
oups
offe
rin
g se
lf-m
an
age
men
t an
d t
rain
ing
can
pro
mot
e w
ays
of
copin
g w
ith
chro
nic
pain
an
d i
mpro
ve s
elf-
effi
cacy
(Lo
rig
et a
l 19
99).
2M
utu
al
suppor
t an
d g
rou
p e
nco
ura
gem
ent
can
im
pro
ve t
he p
erso
n’s
copin
g abi
liti
es.
3Se
lf-m
an
age
men
t/su
ppor
t gr
oups
can
red
uce
soc
ial
isol
ati
on.
4Se
lf-m
an
age
men
t/su
ppor
t gr
oups
can
com
ple
men
t st
atu
tory
ser
vice
s by
offe
rin
g su
ppor
t be
twee
n a
ppoi
ntm
ents
an
d b
y of
feri
ng
lon
g-te
rmfo
llow
-up s
uppor
t.
Peop
le w
ith c
hron
ic p
ain
will
be
info
rmed
of
any
loca
l sel
f-m
anag
emen
t/su
pp
ort
grou
ps
or o
rgan
isat
ions
to
faci
litat
eth
eir
cop
ing
skill
s an
d ac
cess
ong
oing
sup
por
t.
Ther
e is
evi
denc
e th
at t
he p
atie
nt a
nd t
he c
arer
hav
ere
ceiv
ed in
form
atio
n on
how
to
acce
ss s
elf-
man
agem
ent
/sup
por
t gr
oup
s.
Ther
e is
evi
denc
e of
an
up t
o da
te d
irect
ory
of s
elf
man
agem
ent
grou
ps/
sup
por
t gr
oup
s av
aila
ble
in t
he a
rea.
Stat
emen
tR
easo
ns
for
stat
emen
tH
ow
to
dem
on
stra
te s
tate
men
t is
bei
ng
ach
ieve
d
Peop
le w
ith c
hron
ic p
ain
who
cho
ose
to jo
in
self-
man
agem
ent/
sup
por
t gr
oup
s re
por
t th
e be
nefit
s as
: •
an o
pp
ortu
nity
to
rece
ive
info
rmat
ion
•an
op
por
tuni
ty t
o ge
t a
deep
er,
diffe
rent
sor
t of
unde
rsta
ndin
g th
at c
an b
e ob
tain
ed f
rom
frie
nds,
fam
ilyan
d he
alth
pro
fess
iona
ls•
over
com
ing
a se
nse
of is
olat
ion
•le
arni
ng f
rom
oth
ers
with
chr
onic
pai
n•
help
ing
othe
rs a
nd s
ocia
lisin
g (S
ubra
man
iam
et
al 1
999)
.
Key
Ch
alle
ng
es ~
1Se
lf-m
an
age
men
t/su
ppor
t gr
oups
requ
ire
act
ive
leader
ship
.
2H
ealth
pro
fess
ion
al
invo
lvem
ent
in s
elf-
man
age
men
t/su
ppor
t gr
oups
can
in
flu
ence
the
dir
ecti
on o
f th
e gr
oup.
3En
suri
ng
succ
essf
ul
inte
grati
on w
ith
the
health
care
tea
m.
Re
sou
rce
s:
ww
w.p
ain
ass
oc
iati
on
.co
m
ww
w.p
ain
co
nc
ern
.org
.uk

Management of chronic pain in adults
17
Sect
ion
8:
Ch
ron
ic p
ain
‘fla
re-u
ps’
/exa
cerb
atio
ns
Key
Po
ints
~
1Peo
ple
wit
h ch
ron
ic p
ain
will
exper
ien
ce f
luct
uati
ons
in t
heir
pain
in
ten
sity
.
2Chr
onic
pain
‘fla
re-u
ps’
can
last
for
vary
ing
per
iods
of t
ime
from
a f
ew s
econ
ds
to s
ever
al
hou
rs.
Peop
le w
ith c
hron
ic p
ain
are
awar
e th
at t
hey
may
exp
erie
nce
occa
sion
al p
erio
ds o
f flu
ctua
tion
in p
ain
inte
nsity
.
The
pos
sibi
lity
of’ ‘
flare
-up
s’ is
incl
uded
in p
atie
nted
ucat
ion
sess
ions
.
Peop
le w
ith c
hron
ic p
ain
have
suf
ficie
nt k
now
ledg
e to
man
age
thei
r an
alge
sic
med
icin
es a
nd e
mp
loy
per
sona
lco
pin
g st
rate
gies
to
man
age
fluct
uatio
ns o
f p
ain
inte
nsity
.
Peop
le w
ith c
hron
ic p
ain
dem
onst
rate
effe
ctiv
e co
pin
gm
echa
nism
s du
ring
fluct
uatio
ns in
pai
n in
tens
ity.
Peop
le w
ith c
hron
ic p
ain
are
awar
e of
the
ir ow
n p
ain-
activ
atin
g tr
igge
rs.
Stat
emen
tR
easo
ns
for
stat
emen
tH
ow
to
dem
on
stra
te s
tate
men
t is
bei
ng
ach
ieve
d
Patie
nts
with
per
sist
ent
non-
canc
er p
ain
may
pre
sent
with
acut
e ex
acer
batio
ns o
f p
ain
(Brit
ish
Pain
Soc
iety
200
4).
Perip
hera
l and
/or
cent
ral s
ensi
tisat
ion
may
pla
y a
role
inm
any
case
s of
bre
akth
roug
h p
ain
in c
hron
ic
non-
mal
igna
nt p
ain
(Sve
ndse
n et
al 2
005)
.
Key
Ch
alle
ng
es ~
1R
ecog
nis
ing
an
d d
iagn
osis
of
an
epis
ode
of ‘f
lare
-up’.
2Peo
ple
wit
h ch
ron
ic p
ain
who
exper
ien
ce a
‘fla
re-u
p’ m
ay
avo
id p
hysi
cal
act
ivit
y.
3Peo
ple
who
are
exper
ien
cin
g a ‘f
lare
-up’ m
ay
adop
t n
egati
ve t
hou
ghts
.
4En
suri
ng
aw
are
nes
s th
at
‘fla
re-u
ps’
may
be i
nfl
uen
ced b
y be
havi
oura
l act
ivit
y patter
ns.
5The
re i
s pati
ent-le
d d
eman
d f
or a
n a
ctio
n p
lan
for
the
man
age
men
t of
‘fla
re-u
ps’.
6The
re i
s a n
eed f
or r
esea
rch
into
the
valu
e of
an
act
ion
pla
n i
n t
he m
an
age
men
t of
‘fla
re-u
ps’
of p
ain
.

18
Sect
ion
9:
Spec
ific
ch
alle
ng
es (
i):
chro
nic
pai
n a
nd
th
e o
lder
ad
ult
Key
Po
ints
~
1 Chr
onic
pain
is
high
ly p
reva
len
t in
old
er p
eople
(G
agl
iese
& M
elza
ck 2
003,
Ellio
tt e
t al
1999).
2 Pain
is
poo
rly
man
age
d i
n o
lder
peo
ple
(Pro
ctor
& H
irdes
2001,
Ber
nabe
i et
al
1998, C
loss
1994).
3Pain
is
ofte
n a
part
of
a c
omple
x p
ictu
re i
ncl
udin
g co
ncu
rren
t m
edic
al
con
dit
ion
s.
Old
er p
eop
le w
ho r
epor
t p
ain
are
rout
inel
y as
sess
ed u
sing
a fo
rmal
ised
pai
n as
sess
men
t to
ol a
s p
art
of in
itial
eval
uatio
n fo
llow
ing
refe
rral
to
any
heal
thca
re p
rofe
ssio
nal.
Any
pai
n re
por
ted
is r
ecog
nise
d as
a p
robl
em.
Form
alis
ed p
ain
asse
ssm
ent
tool
s ar
e av
aila
ble
for
use
by a
llhe
alth
pro
fess
iona
ls.
Ther
e is
evi
denc
e of
pai
n as
sess
men
t w
ithin
the
pat
ient
s’re
cord
s.
Stat
emen
tR
easo
ns
for
stat
emen
tH
ow
to
dem
on
stra
te s
tate
men
t is
bei
ng
ach
ieve
d
Chr
onic
pai
n is
not
an
inev
itabl
e co
nseq
uenc
e of
age
ing,
how
ever
, p
ain
may
be
a co
nseq
uenc
e of
oth
er c
hron
icco
nditi
ons
(Am
eric
an G
eria
tric
Soc
iety
199
8).
Pain
in t
he o
lder
adu
lt is
poo
rly a
sses
sed
and
man
aged
(Pro
ctor
& H
irdes
200
1, C
loss
199
4).
Key
Ch
alle
ng
es ~
1En
suri
ng
suff
icie
nt
tim
e to
un
der
take
acc
ura
te a
sses
smen
t.
2A
n o
lder
per
son
may
be u
nw
illin
g to
ack
now
ledge
pain
du
e to
mis
con
cepti
ons
that
pain
is
a p
art
of
age
ing
(Clo
ss 2
004).
3O
verc
omin
g co
mm
un
icati
on d
iffi
cultie
s. R
epea
tin
g or
rep
hrasi
ng
ques
tion
s ca
n i
mpro
ve r
espon
se (
Clo
ss e
t al
2004).
4U
nqu
alifi
ed s
taff
pro
vide
dir
ect
care
to
elder
ly r
esid
ents
in
nu
rsin
g ho
mes
. The
y m
ay
not
be
edu
cati
onally
pre
pare
d t
o u
nder
take
man
yco
mple
x t
ask
s in
clu
din
g th
ose
invo
lved
in
pain
man
age
men
t (H
orga
s &
Du
nn
2001, H
iggi
ns
et a
l 20
04).

Management of chronic pain in adults
19
Spec
ific
chal
len
ges
(ii)
: ch
ron
ic p
ain
an
d t
he
per
son
wit
h le
arn
ing
dis
abili
ties
incl
udin
g c
ogn
itiv
e im
pai
rmen
t
Key
Po
ints
~
1Peo
ple
wit
h pro
fou
nd l
earn
ing
dis
abi
liti
es m
ay
be u
nabl
e to
com
mu
nic
ate
ver
bally
ther
efor
e pain
ass
essm
ent
tool
s th
at
rely
on
sel
f-re
por
t u
sin
gla
ngu
age
are
in
adeq
uate
(D
avi
s &
Eva
ns
2001)
.
2Psy
chol
ogic
al
dis
tres
s ca
n o
ccu
r if
pain
is
not
ack
now
ledge
d.
3The
cari
ng
rela
tion
ship
wit
h th
e cl
ien
t is
im
por
tan
t fo
r th
e id
enti
fica
tion
of
beha
viou
ral
chan
ges
ass
ocia
ted w
ith
pain
(D
onov
an
2002)
.
4U
se o
f n
on-v
erba
l co
mm
un
icati
on m
etho
ds
an
d n
on-tra
dit
ion
al
met
hods
requ
ire
spec
ialist
ski
lls,
pati
ence
an
d i
nte
rpre
tati
on.
Peop
le w
ith le
arni
ng d
isab
ilitie
s ha
ve t
he r
ight
to
have
thei
r p
ain
man
aged
.
Loca
lly a
gree
d to
ols
to a
ssis
t in
the
ass
essm
ent
of p
ain
inp
eop
le w
ith le
arni
ng d
isab
ilitie
s ar
e av
aila
ble
and
used
.
Loca
l pra
ctic
e gu
idel
ines
for
the
man
agem
ent
of p
ain
inp
eop
le w
ith le
arni
ng d
isab
ilitie
s ex
ist.
Ther
e is
evi
denc
e th
at r
efer
ral a
dvic
e ha
s be
en s
ough
t fr
omle
arni
ng d
isab
ilitie
s se
rvic
es.
Stat
emen
tR
easo
ns
for
stat
emen
tH
ow
to
dem
on
stra
te s
tate
men
t is
bei
ng
ach
ieve
d
Def
icie
ncie
s ha
ve b
een
high
light
ed in
the
tre
atm
ent
ofp
ain
in p
eop
le w
ith le
arni
ng d
isab
ilitie
s (C
SAG
199
9).
Pain
ass
essm
ent
for
this
car
e gr
oup
rel
ies
on b
ehav
iour
alin
dica
tors
and
fac
ial e
xpre
ssio
n (M
cGra
th e
t al
199
8).
Key
Ch
alle
ng
es ~
1B
ehavi
our
that
indic
ate
s pain
in
the
gen
eral
pop
ula
tion
may
be i
nco
nsi
sten
t an
d d
iffi
cult t
o in
terp
ret
in t
hose
wit
h pro
fou
nd l
earn
ing
dis
abi
liti
es (
McG
rath
et
al
1998).
2En
suri
ng
pra
ctit
ion
ers
do
not
make
ass
um
pti
ons
abo
ut
the
cau
ses
of p
ain
.
3A
ckn
owle
dgi
ng
that
peo
ple
wit
h le
arn
ing
dis
abi
liti
es o
ften
exper
ien
ce o
ngo
ing
pain
fro
m a
vari
ety
of o
ther
dis
abi
liti
es.

20
Spec
ific
ch
alle
ng
es (
iii):
man
agem
ent
of
slee
p in
peo
ple
wit
h c
hro
nic
pai
n
Key
Po
ints
~
170
% o
f peo
ple
wit
h ch
ron
ic p
ain
rep
ort
impair
ed s
leep
(M
orin
et
al
1998).
2Pain
cau
ses
ligh
ter/
dis
turb
ed s
leep
an
d c
an
in
terf
ere
wit
h th
e abi
lity
to
init
iate
or
main
tain
sle
ep.
3Poo
r sl
eep m
ay
be a
con
trib
uti
ng
fact
or t
o th
e per
cepti
on o
f pain
in
ten
sity
.
Patie
nts
with
chr
onic
pai
n w
ho r
epor
t sl
eep
dis
turb
ance
unde
rgo
accu
rate
eva
luat
ion
of t
he r
epor
ted
sym
pto
ms.
Adv
ice
is g
iven
to
peo
ple
with
chr
onic
pai
n on
how
to
addr
ess
pro
blem
s w
ith s
leep
dis
turb
ance
.
The
pat
ient
dem
onst
rate
s sk
ill in
tec
hniq
ues
that
enh
ance
rest
ful s
leep
.
Stat
emen
tR
easo
ns
for
stat
emen
tH
ow
to
dem
on
stra
te s
tate
men
t is
bei
ng
ach
ieve
d
25%
of
peo
ple
with
chr
onic
pai
n re
por
t th
at p
ain
disr
upts
thei
r sl
eep
at
leas
t 10
nig
hts
per
mon
th (
Lam
berg
199
9).
Key
Ch
alle
ng
es ~
1M
an
agi
ng
slee
p d
istu
rban
ce w
hich
may
be a
con
sequ
ence
of
an
d a
con
trib
uti
ng
fact
or t
o ch
ron
ic p
ain
.
2Tre
ati
ng
dep
ress
ion
whi
ch c
an
be
ass
ocia
ted w
ith
slee
p d
istu
rban
ce.
3O
pti
mis
ing
an
alg
esic
med
icati
on a
nd m
an
agi
ng
side-
effe
cts
that
can
in
terf
ere
wit
h sl
eep.
4A
cces
sin
g co
gnit
ive
beha
viou
ral
inte
rven
tion
s th
at
spec
ific
ally
targ
et i
nso
mn
ia (
Smit
h et
al
2000).

Management of chronic pain in adults
21
Spec
ific
ch
alle
ng
es (
iv):
sp
irit
ual n
eed
s as
soci
ated
wit
h c
hro
nic
pai
n
Key
Po
ints
~
1Sp
irit
uality
is
a b
asi
c hu
man
phe
nom
enon
tha
t allow
s th
e cr
eati
on o
f a m
ean
ing
an
d p
urp
ose
in l
ife.
2Chr
onic
pain
may
be a
ssoc
iate
d w
ith
endle
ss, m
ean
ingl
ess
suff
erin
g.
3The
per
son
’s sp
irit
ual
belief
s ca
n i
nfl
uen
ce t
heir
hea
lth
belief
s an
d s
ense
of
wel
l-bei
ng.
Emot
iona
l, p
sych
olog
ical
, so
cial
and
sp
iritu
al a
spec
ts o
fch
roni
c p
ain
are
addr
esse
d.
Spiri
tual
car
e is
giv
en in
a o
ne-t
o-on
e re
latio
nshi
p,
isco
mp
lete
ly p
erso
n-ce
ntre
d an
d m
akes
no
assu
mp
tions
abou
t p
erso
nal c
onvi
ctio
n or
life
orie
ntat
ion
(NH
S H
DL
2002
76)
.
The
per
son’
s sp
iritu
al n
eeds
for
m p
art
of t
he o
vera
llm
anag
emen
t p
lan
and
are
asse
ssed
sen
sitiv
ely.
Loca
l res
ourc
es f
or s
piri
tual
sup
por
t ar
e ac
cess
ed w
ith t
hep
erso
n’s
per
mis
sion
.
The
pers
on d
ispl
ays
the
desi
re a
nd a
bilit
y to
get
on
with
life
.
Stat
emen
tR
easo
ns
for
stat
emen
tH
ow
to
dem
on
stra
te s
tate
men
t is
bei
ng
ach
ieve
d
Unc
ontr
olle
d p
ain
can
caus
e su
fferin
g an
d lo
ss o
f se
lf-es
teem
(C
hap
man
& G
avrin
199
9, B
ullin
gton
et
al 2
003)
.
Spiri
tual
issu
es r
elat
ed t
o th
e su
fferin
g of
chr
onic
pai
n ca
nin
volv
e a
reac
tion
betw
een
emot
ions
suc
h as
fea
r, gu
ilt,
ange
r, lo
ss a
nd d
esp
air.
It m
ay a
pp
ear
inse
par
able
fro
mp
hysi
cal p
ain
and
can
influ
ence
the
way
pai
n is
exp
ress
ed.
The
NH
S m
ust
offe
r bo
th s
piri
tual
and
rel
igio
us c
are
with
equa
l ski
ll an
d en
thus
iasm
(N
HS
HD
L 20
02 7
6).
Key
Ch
alle
ng
es ~
1The
con
cept
of s
pir
itu
al
pain
req
uir
es p
ract
itio
ner
s to
go
beyo
nd t
he b
oun
ds
of c
lin
ical
trea
tmen
ts a
nd b
e pre
pare
d t
o dev
ote
the
tim
ere
quir
ed t
o gi
ve s
uppor
tive
an
d u
nder
stan
din
g ca
re.
2In
clu
din
g th
e sp
irit
ual
asp
ects
of
pain
in
the
hol
isti
c ass
essm
ent.
3 Sp
irit
ual
care
is
not
nec
essa
rily
rel
igio
us.
Rel
igio
us
care
, at
its
best
, sho
uld
alw
ays
be
spir
itu
al
(NH
S H
DL
2002
76).
Re
sou
rce
: htt
p:/
/w
ww
.sh
ow
.sc
ot.
nh
s.u
k/
seh
d/
me
ls/
HD
L2
00
2_
76
.pd
f

22
Spec
ific
Ch
alle
ng
es (
v):
chro
nic
pai
n a
nd
sex
ualit
y
Key
Po
ints
~
1Peo
ple
who
exper
ien
ce c
hron
ic p
ain
may
repor
t a d
eter
iora
tion
or
cess
ati
on o
f se
xu
al
act
ivit
y.
2Peo
ple
wit
h ch
ron
ic p
ain
may
fear
an
exace
rbati
on o
f pain
du
rin
g se
xu
al
act
ivit
y.
3Pha
rmaco
logi
cal
age
nts
com
mon
ly u
sed i
n t
he t
reatm
ent
of p
ain
can
dim
inis
h libi
do
an
d i
nhi
bit
sexu
al
fun
ctio
n.
4D
epre
ssio
n c
omm
only
lin
ked w
ith
chro
nic
pain
can
con
trib
ute
to
loss
of
libi
do.
5Tim
e sh
ould
be
alloc
ate
d t
o dis
cuss
thi
s asp
ect
of c
are
in
pri
vate
.
Ass
essm
ent
of s
exua
l fun
ctio
n is
incl
uded
in t
hem
ultid
imen
sion
al a
sses
smen
t of
peo
ple
with
chr
onic
pai
n.
Whe
n st
artin
g ne
w p
harm
acol
ogic
al a
gent
s fo
r th
etr
eatm
ent
of c
hron
ic p
ain
the
pat
ient
is in
form
ed o
fp
oten
tial e
ffect
s of
the
med
icin
es.
Mul
tidim
ensi
onal
ass
essm
ent
incl
udin
g se
xual
fun
ctio
n ha
sbe
en c
arrie
d ou
t if
nece
ssar
y.
Peop
le w
ith c
hron
ic p
ain
rece
ive
info
rmat
ion
on t
he d
rug
trea
tmen
ts in
itiat
ed a
nd a
re e
duca
ted
on t
he p
oten
tial s
ide-
effe
cts.
Ther
e is
evi
denc
e to
sho
w t
hat
any
sexu
al d
ysfu
nctio
n ha
sbe
en a
ddre
ssed
.
Stat
emen
tR
easo
ns
for
stat
emen
tH
ow
to
dem
on
stra
te s
tate
men
t is
bei
ng
ach
ieve
d
Ther
e is
a h
igh
inci
denc
e of
sex
ual d
ysfu
nctio
n re
por
ted
byp
eop
le li
ving
with
chr
onic
pai
n (A
mbl
er e
t al
200
1).
Man
y m
edic
ines
use
d to
tre
at c
hron
ic p
ain
are
know
n to
inhi
bit
sexu
al f
unct
ion
(Pai
ce 2
003)
.
Key
Ch
alle
ng
es ~
1A
void
ing
the
ass
um
pti
on t
hat
the
iden
tifi
cati
on o
f se
xu
al
dif
ficu
ltie
s m
ean
s th
at
the
indiv
idu
al
wis
hes
to a
cces
s he
lp.
2R
ecog
nis
ing
that
phy
siol
ogic
al
chan
ges
can
alter
sex
uality
in
peo
ple
wit
h ch
ron
ic p
ain
.
3A
ckn
owle
dgi
ng
pati
ents
an
d p
rofe
ssio
nals
are
oft
en u
nco
mfo
rtabl
e dis
cuss
ing
sexu
al
issu
es.

Management of chronic pain in adults
23
Spec
ific
Ch
alle
ng
es (
vi):
ch
ron
ic p
ain
an
d t
he
wo
rkp
lace
Key
Po
ints
~
1Peo
ple
wit
h ch
ron
ic p
ain
are
at
incr
ease
d r
isk
of w
ork
loss
an
d d
isabi
lity
, an
d t
he l
onge
r th
ey a
re a
bsen
t fr
om w
ork,
the
les
s like
ly t
hey
are
to
retu
rn (
Waddel
l 19
98).
2Peo
ple
liv
ing
in a
reas
of s
ocia
l dep
riva
tion
, whe
re u
nem
plo
ymen
t m
ay
be h
ighe
r, a
re m
ore
like
ly t
o su
ffer
chr
onic
pain
.
3In
form
ati
on o
n t
he D
isabi
lity
Dis
crim
inati
on A
ct (
2005)
can
be
obta
ined
fro
m h
ttp://
ww
w.d
isabi
lity
.gov
.uk/
dda/e
mplo
yers
/em
plo
yers
.asp
Key
Ch
alle
ng
es ~
1If
chr
onic
pain
is
lin
ked t
o a w
ork-
rela
ted i
nju
ry t
here
may
be o
ngo
ing
com
pen
sati
on i
ssu
es.
2Peo
ple
may
be r
elu
ctan
t to
ret
urn
to
wor
k as
they
may
lose
fin
an
cial
suppor
t.
3A
sta
ged a
ppro
ach
for
ret
urn
to
wor
k m
ay
nee
d t
o be
neg
otia
ted w
ith
the
emplo
yer.
4To
lia
ise
wit
h oc
cupati
onal
health
dep
art
men
ts t
o fa
cilita
te r
etu
rn t
o w
ork.

24
Sect
ion
10:
Use
of
com
ple
men
tary
th
erap
ies
in t
he
man
agem
ent
of
chro
nic
pai
n
Key
Po
ints
~
1M
an
y peo
ple
wit
h ch
ron
ic p
ain
sou
rce
com
ple
men
tary
the
rapie
s.
2Vari
ous
def
init
ion
s of
com
ple
men
tary
the
rapie
s ex
ist.
3The
re h
as
been
an
in
crea
se i
n t
he u
se o
f co
mple
men
tary
the
rapie
s fo
r pain
-rel
ate
d p
robl
ems
(Rao
et a
l 19
99, H
aet
zman
n e
t al
2003)
.
4N
on-p
harm
aco
logi
cal
inte
rven
tion
s m
ust
not
be
seen
as
a s
ubs
titu
te f
or p
harm
aco
logi
cal
age
nts
.
5The
in
tera
ctio
n b
etw
een
the
pati
ent
an
d h
ealthc
are
pro
fess
ion
al
may
be a
n i
mpor
tan
t m
edia
tor
in t
reatm
ent
outc
ome.
6Tra
nsc
uta
neo
us
Ele
ctri
cal
Ner
ve S
tim
ula
tion
(TEN
S) a
nd a
cupu
nct
ure
are
com
mon
ly u
sed f
or t
he r
elie
f of
chr
onic
pain
.
Ass
essm
ent
of p
atie
nts’
use
of
com
ple
men
tary
the
rap
ies
isin
clud
ed in
the
com
pre
hens
ive
asse
ssm
ent.
Ass
essm
ent
of t
he p
atie
nt’s
sui
tabi
lity
and
a tr
ial o
f TE
NS
shou
ld b
e co
nsid
ered
in m
anag
ing
chro
nic
pai
n.
Doc
umen
tatio
n re
flect
s th
at c
onsi
dera
tion
ofco
mp
lem
enta
ry t
hera
pie
s ha
s be
en in
clud
ed in
the
pat
ient
’sas
sess
men
t.
A t
rial o
f TE
NS
is o
ffere
d to
the
pat
ient
.
The
pat
ient
dem
onst
rate
s an
und
erst
andi
ng o
f th
e TE
NS
mac
hine
.
Stat
emen
tR
easo
ns
for
stat
emen
tH
ow
to
dem
on
stra
te s
tate
men
t is
bei
ng
ach
ieve
d
Ther
e is
evi
denc
e to
sug
gest
tha
t so
me
com
ple
men
tary
ther
apie
s ha
ve a
pos
itive
effe
ct o
n ch
roni
c p
ain
(Sny
der
&W
iela
nd 2
003,
Ste
phe
nson
& D
alto
n 20
03).
The
use
of T
ENS
has
been
sho
wn
to b
e ef
fect
ive
in t
hem
anag
emen
t of
chr
onic
pai
n if
used
cor
rect
ly a
nd f
or a
suffi
cien
t du
ratio
n (J
ohns
on 2
000)
.
Patie
nt e
duca
tion
can
influ
ence
the
suc
cess
of
TEN
Sth
erap
y (M
itche
ll &
Kaf
ai 1
997)
.
Key
Ch
alle
ng
es ~
1En
suri
ng
a b
ala
nce
d a
ttit
ude
tow
ard
s th
e u
se o
f co
mple
men
tary
the
rapie
s is
con
veye
d.
2R
ecog
nis
ing
that
som
e co
mple
men
tary
the
rapie
s m
ay
be u
nsu
itabl
e fo
r peo
ple
wit
h ch
ron
ic p
ain
who
are
con
sider
ed p
sych
olog
ically
un
stabl
e.
3En
suri
ng
pati
ents
un
der
stan
d h
ow a
TEN
S m
ach
ine
wor
ks t
o m
axim
ise
the
ben
efit
.
NB
: TE
NS
an
d a
cu
pu
nc
ture
ca
n b
e p
rov
ide
d b
y h
ea
lth
ca
re p
rofe
ssio
na
ls b
ut
it m
ust
be
ac
kn
ow
led
ge
d t
ha
t p
eo
ple
ma
y a
cc
ess
th
ese
tre
atm
en
ts f
rom
oth
er
sou
rce
s.

Management of chronic pain in adults
25
Sect
ion
11:
Ch
ron
ic p
ain
an
d c
ultu
re
Key
Po
ints
~
1Pain
has
both
per
son
al
an
d c
ultu
ral
inte
rpre
tati
ons.
2Ver
bal
an
d n
on-v
erba
l co
mm
un
icati
ons
dif
fer
betw
een
cu
ltu
res.
Hea
lth p
rofe
ssio
nals
dem
onst
rate
sen
sitiv
ity t
o th
ein
fluen
ce o
f cu
lture
on
pai
n p
erce
ptio
ns a
nd p
ain
beha
viou
rs.
Patie
nt a
sses
smen
t an
d m
anag
emen
t re
flect
s cu
ltura
llyap
pro
pria
te c
are.
Stat
emen
tR
easo
ns
for
stat
emen
tH
ow
to
dem
on
stra
te s
tate
men
t is
bei
ng
ach
ieve
d
Cro
ss-c
ultu
ral d
iffer
ence
s in
the
mea
ning
of
and
cop
ing
with
pai
n ha
ve b
een
rep
orte
d (C
lela
nd e
t al
200
5, C
allis
ter
2003
, L
asch
200
0).
Key
Ch
alle
ng
es ~
1En
suri
ng
health
pro
fess
ion
als
are
sen
siti
ve t
o th
e in
flu
ence
of
a p
erso
n’s
cultu
ral
back
grou
nd o
n p
ain
per
cepti
ons
an
d b
ehavi
ours
, an
d a
reaw
are
tha
t th
ere
are
dif
fere
nce
s in
the
pain
exper
ien
ce b
etw
een
in
div
idu
als
in
cu
ltu
ral
grou
ps.

26
Sect
ion
12:
Ed
ucat
ion
fo
r H
ealt
hca
re P
rofe
ssio
nal
s
Key
Po
ints
~
1H
ealthc
are
pro
fess
ion
als
sho
uld
be
pre
pare
d t
o m
eet
pati
ents
’ des
ire
for
info
rmati
on a
bou
t ch
ron
ic p
ain
an
d i
ts m
an
age
men
t.
2La
ck o
f kn
owle
dge
by
healthc
are
pro
fess
ion
als
is
one
reaso
n f
or t
he i
nappro
pri
ate
tre
atm
ent
of c
hron
ic p
ain
.
3Edu
cati
on s
hou
ld r
efle
ct t
hat
chro
nic
pain
is
a m
ultid
imen
sion
al
phe
nom
enon
, whi
ch c
uts
acr
oss
pro
fess
ion
al
bou
ndari
es.
The
prin
cip
les
of c
hron
ic p
ain
asse
ssm
ent
and
man
agem
ent
are
incl
uded
in e
duca
tiona
l pro
gram
mes
for
heal
th p
rofe
ssio
nals
at
pre
and
pos
t re
gist
ratio
n le
vels
.
Educ
atio
n p
rogr
amm
es r
efle
ct t
he m
ultid
imen
sion
al n
atur
eof
chr
onic
pai
n.
A r
ecor
d of
hea
lthca
re p
rofe
ssio
nals
who
att
end
pai
nm
anag
emen
t ed
ucat
ion
is a
vaila
ble.
Hea
lthca
re p
rofe
ssio
nals
are
eq
uip
ped
with
the
kno
wle
dge
to c
are
for
peo
ple
with
chr
onic
pai
n.
As
a m
inim
um r
equi
rem
ent
chan
ges
in k
now
ledg
e an
d/or
skill
s ar
e as
sess
ed;
atte
mp
ts a
re m
ade
to a
sses
s ch
ange
s in
attit
udes
and
bel
iefs
; id
eally
cha
nges
in p
atie
nt/c
lient
outc
omes
are
add
ress
ed.
Stat
emen
tR
easo
ns
for
stat
emen
tH
ow
to
dem
on
stra
te s
tate
men
t is
bei
ng
ach
ieve
d
Chr
onic
pai
n is
a m
ultid
imen
sion
al p
heno
men
on,
whi
chcu
ts a
cros
s al
l pro
fess
iona
l bou
ndar
ies.
Ther
e is
an
educ
atio
nal g
ap r
elat
ing
to c
are
for
peo
ple
with
chr
onic
pai
n (J
ones
et
al 2
001)
.
Hea
lthca
re p
rofe
ssio
nals
mus
t be
pre
par
ed f
or p
ract
ice
(Soh
n &
Coo
k 20
02).
Key
Ch
alle
ng
es ~
1En
suri
ng
edu
cati
on a
ddre
sses
the
kn
owle
dge
, ski
lls
an
d c
onfi
den
ce r
equ
ired
to
del
iver
eff
ecti
ve p
ain
man
age
men
t in
a m
ultip
rofe
ssio
nal
envi
ron
men
t.
2Pro
fess
ion
als
’ attit
udes
an
d b
elie
fs, a
nd o
rgan
isati
onal
barr
iers
may
ham
per
pain
man
age
men
t pra
ctic
e in
dep
enden
tly
of p
rofe
ssio
nals
’kn
owle
dge
.
3En
suri
ng
the
edu
cati
onal
nee
ds
of s
ocia
l ca
re p
rofe
ssio
nals
who
com
e in
to c
onta
ct w
ith
peo
ple
wit
h ch
ron
ic p
ain
are
addre
ssed
.

Management of chronic pain in adults
27
Ad
dit
ion
al I
nfo
rmat
ion
Inte
gra
tio
n o
f Pa
in S
ervi
ces
Situ
ati
ons
whe
re a
cute
pa
in s
erv
ices
an
d c
hro
nic
pa
in m
an
ag
emen
t se
rvic
esw
ill
over
lap
Key
Po
ints
~
1Sp
ecif
ic a
nalg
esic
in
terv
enti
ons
may
redu
ce t
he i
nci
den
ts o
f ch
ron
ic p
ain
aft
er s
urg
ery.
2Chr
onic
pos
t–su
rgic
al
pain
is
com
mon
, may
be s
ever
e an
d l
ead t
o si
gnif
ican
t dis
abi
lity
.
3R
isk
fact
ors
whi
ch a
re p
redis
pos
ed t
o ch
ron
ic p
ost-su
rgic
al
pain
in
clu
de
the
seve
rity
of
pre
or
pos
t-op
erati
ve p
ain
, in
traop
erati
ve n
erve
in
jury
an
d p
sych
olog
ical
vuln
erabi
lity
.
4M
an
y pati
ents
su
ffer
ing
from
chr
onic
pain
rel
ate
thi
s to
an
acu
te i
nci
den
t.
5Chr
onic
sev
ere
pain
is
com
mon
aft
er s
urg
ery
(Macr
ae
2001)
. Su
ch p
ain
may
have
a n
euro
path
ic e
lem
ent
whi
ch m
ay
appea
r ea
rly
in t
hepos
t–op
erati
ve p
erio
d.
6Chr
onic
pain
pati
ents
req
uir
ing
trea
tmen
t fo
r acu
te p
ain
pre
sen
t a s
pec
ial
challen
ge.
Inci
den
ce o
f C
hro
nic
Pai
n a
fter
Surg
ery
Typ
e o
f o
per
atio
nIn
cid
ence
%
Am
puta
tion
30 - 8
5
Thora
coto
my
5 - 67
Mas
tect
om
y11
- 5
7
Chole
cyst
ecto
my
3 - 56
Ingu
inal
her
nia
0
- 63
Vas
ecto
my
0 - 37
Adap
ted f
rom
Mac
rae
2001
, Per
kin
s an
d K
ehle
t 20
00

28
Palli
ativ
e ca
re a
nd
ch
ron
ic p
ain
Situ
ati
ons
whe
re c
hro
nic
pa
in a
nd
pa
llia
tiv
e ca
re w
ill
over
lap
Key
Po
ints
~
1The
pri
nci
ple
s u
nder
lyin
g th
e m
an
age
men
t of
chr
onic
pain
an
d t
he p
allia
tive
care
of
pati
ents
wit
h ca
nce
r ha
ve m
uch
in
com
mon
(S
IGN
Gu
idel
ine
44, N
HS
QIS
2000).
2Thi
s in
clu
des
the
pallia
tive
man
age
men
t of
non
-malign
an
t dis
ease
whe
re p
ain
may
be a
majo
r is
sue
eg
HIV
, mu
ltip
le s
cler
osis
.
3The
bes
t re
sults
are
lik
ely
to b
e ach
ieve
d w
here
the
re a
re g
ood l
ocal
lin
ks b
etw
een
pallia
tive
care
, pain
man
age
men
t se
rvic
es a
nd t
he l
ocal
com
mu
nit
y.
4A
sig
nif
ican
t n
um
ber
of c
an
cer
pati
ents
will
not
ach
ieve
opti
mal
pain
rel
ief
wit
h th
e W
HO
gu
idel
ines
eit
her
du
e to
the
dru
g or
un
acc
epta
ble
side-
effe
cts.
5Fo
r pati
ents
whe
re s
tan
dard
tre
atm
ents
have
failed
, in
terv
enti
onal
tech
niq
ues
may
be r
equ
ired
an
d r
efer
ral
to a
pain
man
age
men
t se
rvic
efo
r advi
ce w
ould
be
appro
pri
ate
(SI
GN
Gu
idel
ine
44).
Key
Ch
alle
ng
es ~
1To
en
sure
tha
t he
alth
pro
fess
ion
als
loo
kin
g aft
er s
uch
pati
ents
are
aw
are
of
the
ran
ge o
f te
chn
iqu
es a
vailabl
e an
d w
hen
the
se a
re a
ppro
pri
ate
.
2To
ach
ieve
adeq
uate
rapid
acc
ess
to s
pec
ialist
pain
ser
vice
s (M
cEw
en 2
004).
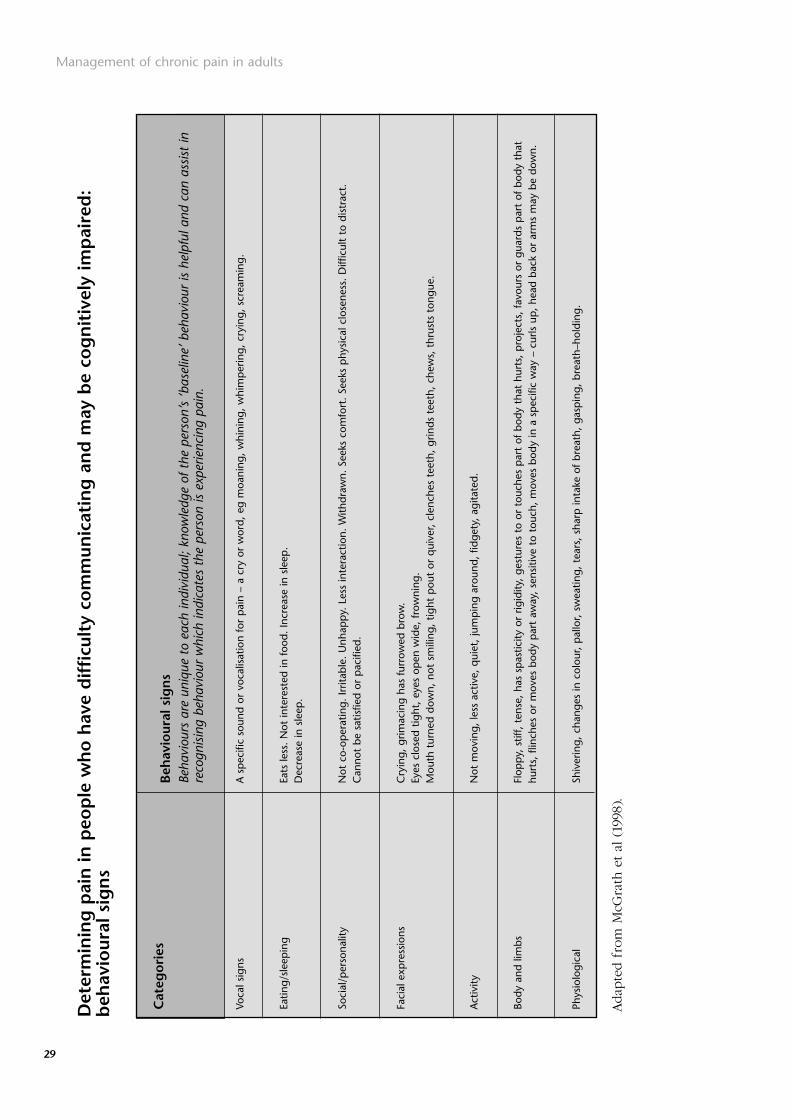
Management of chronic pain in adults
29
Det
erm
inin
g p
ain
in p
eop
le w
ho
hav
e d
iffi
cult
y co
mm
unic
atin
g a
nd
may
be
cog
nit
ivel
y im
pai
red
:b
ehav
iour
al s
ign
s
Voca
l sig
ns
Eatin
g/sl
eep
ing
Soci
al/p
erso
nalit
y
Faci
al e
xpre
ssio
ns
Act
ivity
Body
and
lim
bs
Phys
iolo
gica
l
Cat
ego
ries
Beh
avio
ural
sig
ns
Beha
viou
rs a
re u
niqu
e to
eac
h in
divi
dual
; kno
wle
dge
of t
he p
erso
n’s
‘bas
elin
e’ b
ehav
iour
is h
elpf
ul a
nd c
an a
ssis
t in
reco
gnis
ing
beha
viou
r w
hich
indi
cate
s th
e pe
rson
is e
xper
ienc
ing
pain
.
A s
pec
ific
soun
d or
voc
alis
atio
n fo
r p
ain
– a
cry
or w
ord,
eg
moa
ning
, w
hini
ng,
whi
mp
erin
g, c
ryin
g, s
crea
min
g.
Eats
less
. N
ot in
tere
sted
in f
ood.
Incr
ease
in s
leep
. D
ecre
ase
in s
leep
.
Not
co-
oper
atin
g. Ir
ritab
le.
Unh
app
y. L
ess
inte
ract
ion.
With
draw
n. S
eeks
com
fort
. Se
eks
phy
sica
l clo
sene
ss.
Diff
icul
t to
dis
trac
t.C
anno
t be
sat
isfie
d or
pac
ified
.
Cry
ing,
grim
acin
g ha
s fu
rrow
ed b
row
. Ey
es c
lose
d tig
ht,
eyes
op
en w
ide,
fro
wni
ng.
Mou
th t
urne
d do
wn,
not
sm
iling
, tig
ht p
out
or q
uive
r, cl
ench
es t
eeth
, gr
inds
tee
th,
chew
s, t
hrus
ts t
ongu
e.
Not
mov
ing,
less
act
ive,
qui
et,
jum
pin
g ar
ound
, fid
gety
, ag
itate
d.
Flop
py,
stif
f, te
nse,
has
sp
astic
ity o
r rig
idity
, ge
stur
es t
o or
tou
ches
par
t of
bod
y th
at h
urts
, p
roje
cts,
fav
ours
or
guar
ds p
art
of b
ody
that
hurt
s, f
linch
es o
r m
oves
bod
y p
art
away
, se
nsiti
ve t
o to
uch,
mov
es b
ody
in a
sp
ecifi
c w
ay –
cur
ls u
p,
head
bac
k or
arm
s m
ay b
e do
wn.
Shiv
erin
g, c
hang
es in
col
our,
pal
lor,
swea
ting,
tea
rs,
shar
p in
take
of
brea
th,
gasp
ing,
bre
ath–
hold
ing.
Adap
ted f
rom
McG
rath
et
al (
1998
).

30
Exam
ple
s o
f un
con
ven
tio
nal
an
alg
esic
s (
Ad
juva
nts
)
Tric
yclic
ant
idep
ress
ants
shou
ld b
e co
nsid
ered
for
Neu
rop
athi
c p
ain.
Sele
ctiv
e Se
roto
nin
Re-u
pta
ke in
hibi
tors
(SS
RIs)
Sero
toni
n N
orad
rena
line
Re-u
pta
ke in
hibi
tors
(SN
RIs)
Ant
icon
vuls
ants
sho
uld
be c
onsi
dere
d fo
rne
urop
athi
c p
ain.
Am
itryp
tylin
eIm
ipra
min
eN
ortr
ypty
line
Cita
lop
ram
Venl
afax
ine
Car
bam
azep
ine
Gab
apen
tin
Ther
e m
ay b
e a
redu
ctio
n in
op
ioid
req
uire
men
tre
por
ted.
Whe
n th
e p
atie
nt h
as s
usta
ined
pai
n re
lief
for
3 m
onth
s, a
slo
w d
ose
redu
ctio
n sh
ould
be
atte
mp
ted
to s
ee if
the
ant
icon
vuls
ant
coul
d be
disc
ontin
ued.
Live
r fu
nctio
n sh
ould
rem
ain
with
in n
orm
al li
mits
whi
lst
rece
ivin
g an
ticon
vuls
ant
ther
apy.
Typ
e o
f D
rug
Pres
crib
ing
no
tes/
Pati
ent
info
rmat
ion
Mo
nit
ori
ng
no
tes
❏St
art
with
a lo
w d
ose
and
grad
ually
incr
ease
.
❏Th
e an
alge
sic
effe
ct a
pp
ears
with
in t
he f
irst
few
day
s of
the
rap
y.
❏Th
ere
is a
dos
e-re
spon
se c
urve
to
anal
gesi
c ef
fect
s of
tric
yclic
antid
epre
ssan
ts.
❏C
hron
ic p
ain
may
be
an u
nlic
ense
d in
dica
tion
for
mos
t of
the
sem
edic
ines
and
the
pat
ient
info
rmat
ion
leaf
let,
whi
ch is
issu
ed a
tth
e p
oint
of
disp
ensi
ng,
may
not
con
tain
rel
evan
t in
form
atio
nfo
r th
e co
nditi
on b
eing
tre
ated
.
The
info
rmat
ion
pro
vid
ed m
ay b
e co
nfu
sin
g.
❏A
ntid
epre
ssan
ts a
nd a
ntic
onvu
lsan
ts h
ave
a si
mila
r ef
ficac
y in
the
trea
tmen
t of
neu
rop
athi
c p
ain.
C
hoic
e is
bas
ed o
n p
atie
ntfa
ctor
s an
d co
ncur
rent
med
icat
ion.
❏D
iffer
ent
antic
onvu
lsan
ts h
ave
diffe
rent
mec
hani
sms
of a
ctio
n.
If on
e is
inef
fect
ive
it m
ay b
e w
orth
con
side
ring
tria
l of
anot
her.
Exam
ple
SSR
Is a
re t
hough
t to
be
less
eff
ective
for
the
relie
f of
neu
ropat
hic
pai
n t
han
tri
cycl
ic a
ntidep
ress
ants
or
SNR
Is
(Sin
dru
p e
t al
200
5).

Management of chronic pain in adults
31
Use
of
op
ioid
s in
th
e m
anag
emen
t o
f ch
ron
ic n
on
-mal
ign
ant
pai
n
Key
Iss
ues
~
1St
ron
g op
ioid
s sh
ould
no
tbe
con
sider
ed a
s fi
rst
lin
e tr
eatm
ents
for
chr
onic
pain
.
2So
me
peo
ple
wit
h ch
ron
ic n
on-m
align
an
t pain
can
ben
efit
fro
m t
he u
se o
f or
al
opio
ids.
3Tho
rou
gh a
tten
tion
to
dia
gnos
is a
nd p
ati
ent
hist
ory
mu
st p
rece
de
an
y dec
isio
n t
o pre
scri
be o
pio
ids.
4Pati
ents
sho
uld
be
dee
med
psy
chol
ogic
ally
stabl
e w
ith
spec
ific
reg
ard
to
addic
tion
iss
ues
.
5The
per
son
wit
h ch
ron
ic p
ain
an
d t
heir
doc
tor
shou
ld a
gree
bef
oreh
an
d o
n h
ow t
o ass
ess
the
outc
ome
of t
hera
py.
6Su
stain
ed r
elea
se o
pio
id p
repara
tion
s are
the
dru
g of
cho
ice
7A
n i
mm
edia
te r
elea
se p
repara
tion
may
be r
equ
ired
to
man
age
bre
akt
hrou
gh/’f
lare
-up’ p
ain
.
8A
tri
al
of t
hera
py,
wit
h go
als
an
d e
ndpoi
nt
agr
eed b
etw
een
the
per
son
wit
h ch
ron
ic p
ain
an
d t
heir
doc
tor, s
hou
ld p
rece
de
an
y dec
isio
n t
opre
scri
be o
pio
ids
in t
he l
ong
term
.
Info
rmed
co
nse
nt
sho
uld
:
•st
ress
tha
t or
al
opio
ids
are
on
ly o
ne
part
of
the
trea
tmen
t pla
n, a
nd t
hat
data
is
lack
ing
on t
he l
ong-
term
eff
ects
of
med
ically
pre
scri
bed
opio
ids.
•cl
earl
y def
ine
spec
ific
goa
ls o
f th
e tr
eatm
ent
pro
gram
.
•w
arn
of
the
pot
enti
al
for
cogn
itiv
e im
pair
men
t w
hich
may
aff
ect
dri
vin
g abi
lity
, esp
ecia
lly
whi
le c
omm
enci
ng
opio
id t
hera
py
an
d a
rou
nd
the
tim
e of
dos
e es
cala
tion
.
•poi
nt
out
the
incr
ease
d l
ikel
ihoo
d o
f se
dati
on i
f be
nzo
dia
zepin
es a
nd/o
r alc
ohol
are
use
d i
n c
onju
nct
ion
wit
h op
ioid
the
rapy.
•st
ress
tha
t pati
ents
mu
st a
ccep
t re
spon
sibi
lity
for
:
oen
suri
ng
thei
r su
pply
of
med
icati
on d
oes
not
ru
n o
ut
aft
er h
ours
;
ose
curi
ty o
f th
eir
med
icati
on;
oke
epin
g re
view
appoi
ntm
ents
;
ou
sin
g on
ly o
ne
doc
tor
to s
upply
thi
s m
edic
ati
on.

32
•ex
pla
inth
e co
nse
quen
ces
of a
berr
an
t be
havi
our
as
clea
rly
as
pos
sibl
e.
•ex
pla
in t
he i
ndic
ati
ons
for
ceasi
ng
trea
tmen
t w
ith
opio
ids:
ola
ck o
f im
pro
vem
ent
in f
un
ctio
n, o
r ev
iden
ce o
f det
erio
rati
on i
n f
un
ctio
n;
ou
nsa
nct
ion
ed d
ose
esca
lati
on a
nd r
equ
ests
for
earl
y re
pea
t pre
scri
pti
ons;
olo
sin
g pre
scri
pti
ons;
ou
nappro
ved u
se o
f th
e dru
g to
tre
at
othe
r sy
mpto
ms.
•dis
cuss
sid
e-ef
fect
s an
d t
heir
man
age
men
t (e
g, c
onst
ipati
on, n
au
sea, s
edati
on, d
ry m
outh
, uri
nary
hes
itan
cy, a
nd d
epre
ssio
n o
f se
xho
rmon
es, w
ith
ass
ocia
ted r
isk
of o
steo
por
osis
wit
h lo
ng-
term
use
).
•th
e pos
sibi
lity
(fo
r w
omen
) of
phy
sica
l dep
enden
ce i
n c
hild
ren
bor
n t
o th
em i
f th
ey c
onti
nu
e to
take
opio
ids
in l
ate
pre
gnan
cy.

Management of chronic pain in adults
33
Spec
ialis
t Se
rvic
es:
The
Pain
Man
agem
ent
Clin
ic
Key
Po
ints
~
1R
efer
ral
to a
pain
clin
ic s
hou
ld b
e co
nsi
der
ed a
fter
appro
pri
ate
tre
atm
ent
stra
tegi
es h
ave
pro
ved u
nsu
cces
sfu
l.
2W
hen
the
pati
ent
has
dif
ficu
lt-to-
con
trol
pain
.
3W
hen
the
re a
re c
omple
x p
sych
osoc
ial
infl
uen
ces
in t
he p
ain
pre
sen
tati
on.
4Pro
fess
ion
al
role
s in
pain
man
age
men
t cl
inic
s m
ay
vary
.
At
a pai
n c
linic
, pat
ients
will
usu
ally
be
seen
by a
pai
n m
edic
ine
spec
ialis
t an
d b
e off
ered
a m
ore
com
pre
hen
sive
and s
pec
ialis
ed a
sses
smen
t th
at is
likel
y t
o b
e m
ulti-d
isci
plin
ary.
Dis
ciplin
es r
epre
sente
d v
ary,
but
may
incl
ude
spec
ialis
t nurs
ing,
spec
ialis
t pai
n p
hysi
oth
erap
ist,
pai
n m
edic
ine
spec
ialis
t, occ
upat
ional
ther
apis
t, phar
mac
ist
and c
linic
al p
ain p
sych
olo
gist
(le
vel 3)
. Pr
ofe
ssio
nal
role
s in
thes
e cl
inic
s m
ay v
ary.
The
key
to e
ffec
tive
man
agem
ent,
nam
ely a
ppro
pri
ate
asse
ssm
ent,
funct
ional
res
tora
tion a
nd a
bio
psy
choso
cial
appro
ach, u
nder
pin
any
phar
mac
olo
gica
l or
inva
sive
ther
apie
s under
taken
. T
he
ke
y t
o s
uc
ce
ss i
s p
ati
en
t in
vo
lve
me
nt.
A m
ultid
isci
plin
ary m
anag
emen
t pla
n s
hould
be
dev
eloped
for
appro
pri
ate
pat
ients
. M
edic
atio
n r
evie
w is
an im
port
ant
par
t, co
nsi
der
ing
the
appro
pri
aten
ess
of
exis
ting
med
icin
es, w
ithdra
win
g or
reduci
ng
or
intr
oduci
ng
new
med
icin
es.
This
may
be
com
ple
men
ted w
ith n
on-in
vasi
veth
erap
ies.
The
man
agem
ent
pla
n m
ay incl
ude
inte
rven
tional
ther
apie
s, but
rare
ly in iso
lation.
Good r
esourc
es f
or
info
rmat
ion a
bout
thes
e in
clude:
•A
n e
vid
ence
bas
ed r
esourc
e fo
r in
terv
entional
pai
n m
anag
emen
t w
ww
.acc
.co.n
z/ip
m
•T
he
Bri
tish
Pai
n S
oci
ety
ww
w.b
ritish
pai
nso
ciet
y.org
Key
Ch
alle
ng
es ~
1The
pati
ent
un
der
stan
ds
why
the
y are
bei
ng
refe
rred
to
the
pain
clin
ic.
2A
n a
ppro
pri
ate
med
ical
ass
essm
ent
shou
ld h
ave
take
n p
lace
.
3A
co
mp
lete
refe
rral
letter
sho
uld
be
sen
t (S
IGN
Gu
idel
ine
31).
4R
ealist
ic e
xpec
tati
ons
shou
ld b
e en
cou
rage
d.
5Tre
atm
ent
at
a p
ain
clin
ic s
hou
ld b
e lim
ited
wit
h dis
charg
e ba
ck t
o pri
mary
care
wit
h co
mm
un
ity
suppor
t w
here
appro
pri
ate
.
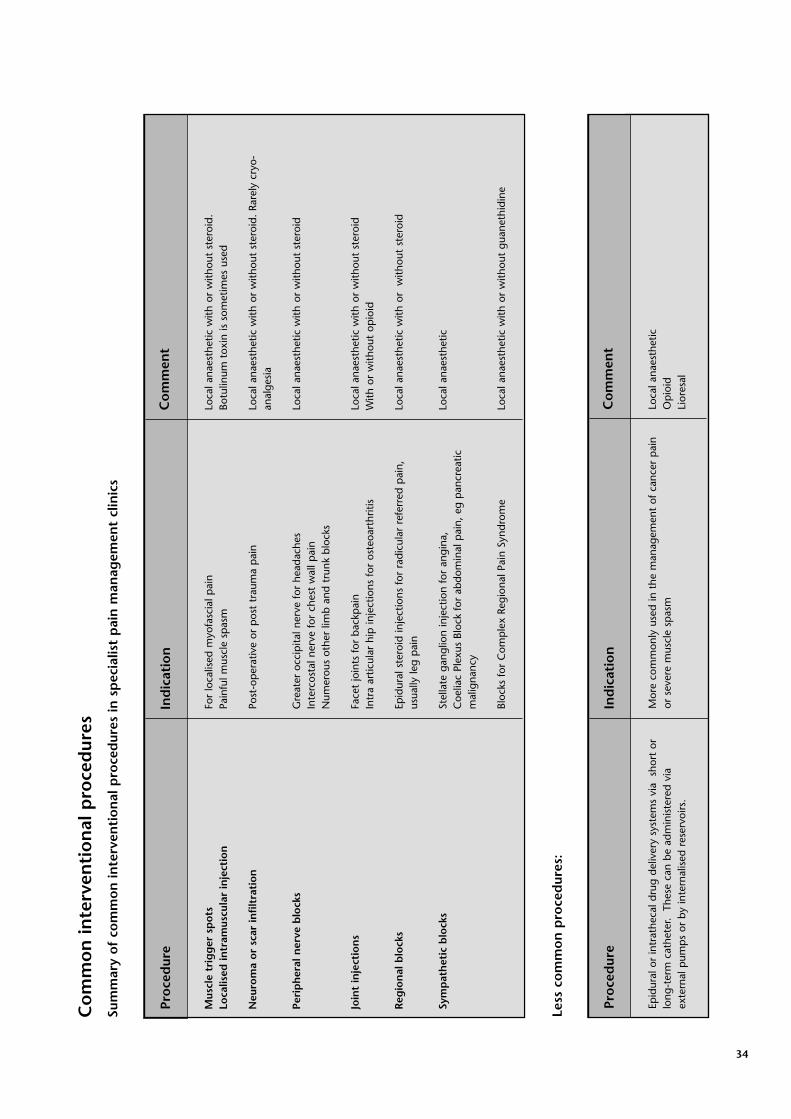
34
Co
mm
on
inte
rven
tio
nal
pro
ced
ures
Su
mm
ary
of
com
mo
n in
terv
enti
on
al p
roce
dur
es in
sp
ecia
list
pai
n m
anag
emen
t cl
inic
s
Mus
cle
trig
ger
sp
ots
Loca
lised
intr
amus
cula
r in
ject
ion
Neu
rom
a o
r sc
ar in
filt
rati
on
Peri
ph
eral
ner
ve b
lock
s
Join
t in
ject
ion
s
Reg
ion
al b
lock
s
Sym
pat
het
ic b
lock
s
Loca
l ana
esth
etic
with
or
with
out
ster
oid.
Botu
linum
tox
in is
som
etim
es u
sed
Loca
l ana
esth
etic
with
or
with
out
ster
oid.
Rar
ely
cryo
-an
alge
sia
Loca
l ana
esth
etic
with
or
with
out
ster
oid
Loca
l ana
esth
etic
with
or
with
out
ster
oid
With
or
with
out
opio
id
Loca
l ana
esth
etic
with
or
with
out
ster
oid
Loca
l ana
esth
etic
Loca
l ana
esth
etic
with
or
with
out
guan
ethi
dine
Pro
ced
ure
Ind
icat
ion
Co
mm
ent
For
loca
lised
myo
fasc
ial p
ain
Pain
ful m
uscl
e sp
asm
Post
-op
erat
ive
or p
ost
trau
ma
pai
n
Gre
ater
occ
ipita
l ner
ve f
or h
eada
ches
Inte
rcos
tal n
erve
for
che
st w
all p
ain
Num
erou
s ot
her
limb
and
trun
k bl
ocks
Face
t jo
ints
for
bac
kpai
nIn
tra
artic
ular
hip
inje
ctio
ns f
or o
steo
arth
ritis
Epid
ural
ste
roid
inje
ctio
ns f
or r
adic
ular
ref
erre
d p
ain,
usua
lly le
g p
ain
Stel
late
gan
glio
n in
ject
ion
for
angi
na,
Coe
liac
Plex
us B
lock
for
abd
omin
al p
ain,
eg
pan
crea
ticm
alig
nanc
y
Bloc
ks f
or C
omp
lex
Regi
onal
Pai
n Sy
ndro
me
Less
co
mm
on
pro
ced
ures
:
Epid
ural
or
intr
athe
cal d
rug
deliv
ery
syst
ems
via
sho
rt o
rlo
ng-t
erm
cat
hete
r. T
hese
can
be
adm
inis
tere
d vi
aex
tern
al p
ump
s or
by
inte
rnal
ised
res
ervo
irs.
Loca
l ana
esth
etic
O
pio
idLi
ores
al
Pro
ced
ure
Ind
icat
ion
Co
mm
ent
Mor
e co
mm
only
use
d in
the
man
agem
ent
of c
ance
r p
ain
or s
ever
e m
uscl
e sp
asm

Management of chronic pain in adults
35
COPYRIGHT
DOLOPLUS-2 SCALE BEHAVIOURAL PAIN ASSESSMENT IN THE ELDERLY
Behavioural RecordsNAME : Christian Name : Unit :
1• Somatic complaints
2• Protective body posturesadopted at rest
3• Protection ofsore areas
4• Expression
5• Sleep pattern
6• washing &/or dressing
7• Mobility
8• Communication
9• Social life
10• Problems ofbehaviour
SCORE
DATES
SOMATIC REACTIONS
PSYCHOMOTOR REACTIONS
PSYCHOSOCIAL REACTIONS
• no complaints . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0 0 0 0• complaints expressed upon inquiry only . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 1 1 1• occasionnal involuntary complaints . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 2 2 2• continuous involontary complaints . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 3 3 3
• no protective body posture . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0 0 0 0• the patient occasionally avoids certain positions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 1 1 1• protective postures continuously and effectively sought . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 2 2 2• protective postures continuously sought, without success . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 3 3 3
• no protective action taken . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0 0 0 0• protective actions attempted without interfering against any investigation or nursing . . . . . . . . . . . . . . 1 1 1 1• protective actions against any investigation or nursing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 2 2 2• protective actions taken at rest, even when not approached . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 3 3 3
• usual expression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0 0 0 0• expression showing pain when approached . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 1 1 1• expression showing pain even without being approached . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 2 2 2• permanent and unusually blank look (voiceless,staring, looking blank) . . . . . . . . . . . . . . . . . . . . . . . 3 3 3 3
• normal sleep . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0 0 0 0• difficult to go to sleep . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 1 1 1• frequent waking (restlessness) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 2 2 2• insomnia affecting waking times . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 3 3 3
• usual abilities unaffected . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0 0 0 0• usual abilities slightly affected (careful but thorough) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 1 1 1• usual abilities highly impaired, washing &/or dressing is laborious and incomplete . . . . . . . . . . . . . . 2 2 2 2• washing &/or dressing rendered impossible as the patient resists any attempt . . . . . . . . . . . . . . . . . . 3 3 3 3
• usual abilities & activities remain unaffected . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0 0 0 0• usual activities are reduced (the patient avoids certain movements and reduces his/her walking distance) . 1 1 1 1• usual activities and abilities reduced (even with help, the patient cuts down on his/her movements) . . . . 2 2 2 2• any movement is impossible, the patient resists all persuasion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 3 3 3
• unchanged . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0 0 0 0• heightened (the patient demands attention in an unusual manner) . . . . . . . . . . . . . . . . . . . . . . . . . . 1 1 1 1• lessened (the patient cuts him/herself off) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 2 2 2• absence or refusal of any form of communication . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 3 3 3
• participates normally in every activity (meals, entertainment, therapy workshop) . . . . . . . . . . . . . . . . . 0 0 0 0• participates in activities when asked to do so only . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 1 1 1• sometimes refuses to participate in any activity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 2 2 2• refuses to participate in anything . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 3 3 3
• normal behaviour . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0 0 0 0• problems of repetitive reactive behaviour . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 1 1 1• problems of permanent reactive behaviour . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 2 2 2• permanent behaviour problems (without any external stimulus) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 3 3 3
Appendix 1 Examples of tools and assessment domains
Sample 1: Doloplus-2 Scale

36
Somatic complaintsThe patients expresses pain by word, gesture, cries, tears or moans.
Protective body postures adopted at restUnusual body positions intended to avoid or relieve pain.
Protection of sore areasThe patient protects one or several areas of his/her body by a defensive attitude or gestures.
ExpressionThe facial expression appears to express pain (grimaces, drawn, atonic) as does the gaze (fixedgaze, empty gaze, absent, tears).
InvestigationAny investigation whatsoever (approach of a caregiver, mobilization, care procedure, etc.).
Washing/dressingPain assessment during washing and/or dressing, alone or with assistance.
MobilityEvaluation of pain in movement: change of position, transfer, walking alone or with assistance.
CommunicationVerbal or non-verbal.
Social lifeMeals, events, activities, therapeutic workshops, visits, etc.
Problems of behaviourAggressiveness, agitation, confusion, indifference, lapsing, regression, asking for euthanasia, etc.
DOLOPLUS-2 SCALE : LEXICON

Management of chronic pain in adults
37
1 • Scale use requires learningAs is the case with any new instrument, it is judicious to test it before circulating it. Scale scoring timedecreases with experience (at most a few minutes). Where possible, it is of value to appoint a referenceperson in a given care structure.
2 • Pluridisciplinary team scoringIrrespective of the health-care, social-care or home structure, scoring by several caregivers is preferable(physician, nurse, nursing assistant, etc.). At home, the family and other persons can contribute using a liaison notebook, telephone or even a bedside meeting. The scale should be included in the 'care' or 'liaison notebook' file.
3 • Do not score if the item is inappropriateIt is not necessary to have a response for all the items on the scale, particularly given an unknown patienton whom one does not yet have all the data, particularly at psychosocial level. Similarly, in the event ofcoma, scoring will be mainly based on the somatic items.
4 • Compile score kineticsRe-assessment should be twice daily until the pain is sedated, then at longer intervals, depending on thesituation. Compile score kinetics and show the kinetics on the care chart (like temperature or blood pressure).The scale will thus become an essential argument in the management of the symptom and in treatment initiation.
5 • Do not compare scores on different patientsPain is a subjective and personal sensation and emotion. It is therefore of no value to compare scoresbetween patients. Only the time course of the scores in a given patient is of interest.
6 • If in doubt, do not hesitate to conduct a test treatment with an appropriate analgesicIt is now accepted that a score greater than or equal to 5/30 is a sign of pain. However, for borderlinescores, the patient should be given the benefit of the doubt. If the patient's behavior changes followinganalgesic administration, pain is indeed involved.
7 • The scale scores pain and not depression, dependence or cognitive functionsNumerous instruments are available for each situation. It is of primary importance to understand that thescale is used to detect changes in behavior related to potential pain.Thus, for items 6 and 7, we are not evaluating dependence or independence but pain.
8 • Do not use the DOLOPLUS 2 scale systematicallyWhen the elderly patient is communicative and cooperative, it is logical to use the self-assessment instruments.When pain is patent, it is more urgent to relieve it than to assess it ... However, if there is the slightestdoubt, hetero-assessment will avoid underestimation.
DOLOPLUS-2 SCALE : INSTRUCTIONS FOR USE
Reproduced with permission
http://www.doloplus.com

38
Sample 2: NoPain - Non-Communicative Patient’s Pain Assessment Instrument
Snow et al 2003

Management of chronic pain in adults
39
Initial Pain Assessment Tool
Date: _________________________________
Patient's name: ____________________________________________ Age: ________
Diagnosis: ____________________________________________________________________
____________________________________________________________________
Physician: _______________________________________________
Nurse: __________________________________________________
I. Location: Patient or nurse marks drawing
II. Intensity: Patient rates the pain. Scale used: ___________
Present:__________________________________________________
Worst pain gets:___________________________________________
Best pain gets:____________________________________________
Acceptable level of pain:_____________________________________
Sample 3: McCaffery and Pasero Initial Assessment Tool

40
III. Quality: (Use patient's own words, e.g., prick, ache, burn, throb, pull, sharp)
____________________________________________________________________________
____________________________________________________________________________
IV. Onset, duration, variations, rhythms:
____________________________________________________________________________
____________________________________________________________________________
V. Manner of expressing pain:
____________________________________________________________________________
___________________________________________________________________________
VI. What relieves the pain?
____________________________________________________________________________
____________________________________________________________________________
VII. What causes or increases the pain?
____________________________________________________________________________
____________________________________________________________________________
VIII. Effects of pain: (Note decreased function, decreased quality of life.)
Accompanying symptoms (e.g., nausea)_____________________________________________
Sleep_________________________________________________________________________
Appetite_______________________________________________________________________
Physical activity________________________________________________________________
Relationship with others (e.g., irritability)_____________________________________________
Emotions (e.g., anger, suididal, crying)______________________________________________
Concentration__________________________________________________________________
Other_________________________________________________________________________

Management of chronic pain in adults
41
IX. Other comments: _________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
X. Plan:_____________________________________________________
____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
___________________________________________________________________________
____________________________________________________________________________
Note: May be duplicated and used in clinical practice Source: McCaffery and Beebe, 1989. Usedwith permission.

42
Sample 4: Patient Comfort Assessment Guide

Management of chronic pain in adults
43

44
Appendix IV (i)
SHORT FORM McGILL PAIN QUESTIONNAIRE and PAINDIAGRAM
(Reproduced with permission of author © Dr. Ron Melzack, for publication and
distribution)
Date: ______________________________________
Name: _____________________________________
Check the column to indicate the level of yourpain for each word, or leave blank if it does notapply to you.
Mild Moderate Severe
1 Throbbing _____ _____ _____
2 Shooting _____ _____ _____
3 Stabbing _____ _____ _____
4 Sharp _____ _____ _____
5 Cramping _____ _____ _____
6 Gnawing _____ _____ _____
7 Hot-burning _____ _____ _____
8 Aching _____ _____ _____
9 Heavy _____ _____ _____
10 Tender _____ _____ _____
11 Splitting _____ _____ _____
12 Tiring-Exhausting_____ _____ _____
13 Sickening _____ _____ _____
14 Fearful _____ _____ _____
15 Cruel-Punishing _____ _____
Indicate on this line how bad your pain is—at the left end of line means no pain at all, at right endmeans worst pain possible.
No ________________________________________________ Worst PossiblePain Pain
S /33 A /12 VAS /10
Sample 5: Short Form McGill Pain Questionnaire

Management of chronic pain in adults
45
Brief pain inventory goes here
����������������� ������
�� ����������������� ���� ������ ������������������������������� ����� ������������� �� ���� ��������������� ����������������������������������� ��������������� ��������������
� � ! " # $ % & ' ��(� )���� �*���� )�� �������������
�������+� ������(�
���������� �������� ���������
������ � ��������������� ����� �� ��
���� ��������������� �������������������������������
�� ,�������������� ��������������� �-�������������������)������.��������������������� ������� ��
� � ! " # $ % & ' ��(� )���� �*���� )�� �������������
� � ! " # $ % & ' ��(� )���� �*���� )�� �������������
� � ! " # $ % & ' ��(� )���� �*���� )�� �������������
�� )�� ����������������*�������������������*��������*� ���� ��*� �������������� -�� ��������� �� "����� �
�� )�� ����������������*�������������������*��������*� ���� ��*� ������������������������
�� )�� ����������������*�������������������*��������*� ���� ��*� �������������� �� ��������� �� "����� �
�� )�� ����������������*�������������������*���������� ���-�������������������������-�
������������� ������ ���� ���
Sample 6: Brief Pain Inventory

46
%� /������������� ������������ ������������������������������
�������������� ����������� ������� ������ ����������� ����� ���������
�0 ��0 �0 !�0 "�0 #�0 $�0 %�0 &�0 '�0 ���0(� ����������1������2��� ����������2���
� � ! " # $ % & ' ��3�� ���� �������1�������4�������� �������4��������
5� 6������5�����
� � ! " # $ % & ' ��3�� ���� �������1�������4�������� �������4��������
7� 8���
� � ! " # $ % & ' ��3�� ���� �������1�������4�������� �������4��������
1� /�����5*��
� � ! " # $ % & ' ��3�� ���� �������1�������4�������� �������4��������
3� (�����/���������� �*����-������� ������������������� �-����
� � ! " # $ % & ' ��3�� ���� �������1�������4�������� �������4��������
9� 2����� �-��������������
� � ! " # $ % & ' ��3�� ���� �������1�������4�������� �������4��������
:� ;���
� � ! " # $ % & ' ��3�� ���� �������1�������4�������� �������4��������
6� 9�<������������
'� 1���������������*���������� ��*� ���-�������������� �� "����� �������� ����������-�������=
&� 4������� �� "����� ����-����������������������������� ������������ ����������)�� ��������������������������������� �� ��- ���-���������������������������
Used by permission.

Management of chronic pain in adults
47
Oswestry Disability Questionnaire This questionnaire has been designed to give us information as to how your back or leg pain is affecting your ability to manage in everyday life. Please answer by checking one box in each section for the statement which best applies to you. We realise you may consider that two or more statements in any one section apply but please just shade out the spot that indicates the statement which most clearly describes your problem.
Section 1: Pain Intensity
� I have no pain at the moment
� The pain is very mild at the moment � The pain is moderate at the moment � The pain is fairly severe at the moment � The pain is very severe at the moment � The pain is the worst imaginable at the moment
Section 2: Personal Care (eg. washing, dressing)
� I can look after myself normally without causing extra pain
� I can look after myself normally but it causes extra pain
� It is painful to look after myself and I am slow and careful
� I need some help but can manage most of my personal care
� I need help every day in most aspects of self-care
� I do not get dressed, wash with difficulty and stay in bed
Section 3: Lifting
� I can lift heavy weights without extra pain
� I can lift heavy weights but it gives me extra pain
� Pain prevents me lifting heavy weights off the floor but I can manage if they are conveniently placed eg. on a table
� Pain prevents me lifting heavy weights but I can manage light to medium weights if they are conveniently positioned
� I can only lift very light weights
� I cannot lift or carry anything
Section 4: Walking*
� Pain does not prevent me walking any distance � Pain prevents me from walking more than 2 kilometres � Pain prevents me from walking more than 1 kilometre � Pain prevents me from walking more than 500 metres � I can only walk using a stick or crutches
� I am in bed most of the time
Section 5: Sitting
� I can sit in any chair as long as I like
� I can only sit in my favourite chair as long as I like � Pain prevents me sitting more than one hour � Pain prevents me from sitting more than 30 minutes � Pain prevents me from sitting more than 10 minutes � Pain prevents me from sitting at all
Section 6: Standing
� I can stand as long as I want without extra pain
� I can stand as long as I want but it gives me extra pain � Pain prevents me from standing for more than 1 hour � Pain prevents me from standing for more than 30
minutes
� Pain prevents me from standing for more than 10 minutes
� Pain prevents me from standing at all
Section 7: Sleeping
� My sleep is never disturbed by pain
� My sleep is occasionally disturbed by pain
� Because of pain I have less than 6 hours sleep � Because of pain I have less than 4 hours sleep
� Because of pain I have less than 2 hours sleep
� Pain prevents me from sleeping at all
Section 8: Sex Life (if applicable)
� My sex life is normal and causes no extra pain
� My sex life is normal but causes some extra pain
� My sex life is nearly normal but is very painful
� My sex life is severely restricted by pain
� My sex life is nearly absent because of pain
� Pain prevents any sex life at all
Section 9: Social Life
� My social life is normal and gives me no extra pain
� My social life is normal but increases the degree of pain
� Pain has no significant effect on my social l ife apart from limiting my more energetic interests e.g. sport
� Pain has restricted my social life and I do not go out as often
� Pain has restricted my social life to my home
� I have no social life because of pain
Section 10: Travelling
� I can travel anywhere without pain
� I can travel anywhere but it gives me extra pain
� Pain is bad but I manage journeys over two hours
� Pain restricts me to journeys of less than one hour
� Pain restricts me to short necessary journeys under 30 minutes
� Pain prevents me from travelling except to receive treatment
Sample 7: Oswestry Disability Questionnaire

48
Score: / x 100 = % Scoring: For each section the total possible score is 5: if the first statement is marked the section score = 0, if the last statement is marked it = 5. If all ten sections are completed the score is calculated as follows: Example: 16 (total scored) 50 (total possible score) x 100 = 32% If one section is missed or not applicable the score is calculated: 16 (total scored) 45 (total possible score) x 100 = 35.5% Minimum Detectable Change (90% confidence): 10%points (Change of less than this may be attributable to error in the measurement) Source: Fairbank JCT & Pynsent, PB (2000) The Oswestry Disability Index. Spine, 25(22):2940-2953.
Davidson M & Keating J (2001) A comparison of five low back disability questionnaires: reliability and responsiveness. Physical Therapy 2002;82:8-24.
*Note: Distances of 1mile, ½ mile and 100 yards have been replaced by metric distances in the Walking section.

Management of chronic pain in adults
Appendix 2
Who was Involved in Developing the Statement?
Working Group
Janette Barrie Practice Development NHS QISProject Co-ordinator
Helen Cadden Lay Representative Glasgow
David Carroll General Practitioner NHS Grampian
David Craig Psychologist NHS Glasgow
Sandra Fyfe Lay Representative Pain Association Scotland
Mairi Harvey Lay Representative Argyll
Kathleen Henderson Occupational Therapist NHS Borders
Jennifer Hogg District Nurse NHS Ayrshire & Arran
Rhona Hotchkiss Head of Practice Development NHS QISChair of Working Group
Derek Jones Lecturer in Occupational Therapy Queen Margaret University College
Alison MacRobbie Pharmacist Inverness
Robin McKinlay Consultant in Anaesthesia NHS Forth Valleyand Pain Management
Fiona McPherson Clinical Nurse Specialist NHS Lothian
Mary Maghee Care Home Manager Glasgow
Gail Monteith Lay Representative Pain Association Scotland
Blair Robertson Hospital Chaplain NHS Glasgow
Mick Serpell Consultant and Senior Lecturer University of Glasgow,in Anaesthesia NHS Glasgow
Rosemary Showell District Nurse NHS Lanarkshire
Michael Souter Lay Representative Pain Association Scotland
Drummond Taylor Carer Pain Association Scotland
Jenny Williamson Clinical Nurse Specialist NHS LothianPain Management
49

50
Reference Group
Ms Dorothy Armstrong Programme Director NHS Education ScotlandDr. Clare Blackburn Chairperson National Occupational
Therapist Pain AssociationMs Ruth Clark Operations Manager Princess Royal Trust for
CarersDr. Beverly Collett President The British Pain Society
Consultant AnaesthetistMr. David Falconer Director Pain Association ScotlandMrs Aileen Hamilton Lecturer in Holistic Therapies Telford College, EdinburghMr Brian Jappy Chief Pharmacist NHS GrampianDr Pete Mackenzie Consultant Anaesthetist Royal College of
AnaesthetistsDr. Bill Macrae Consultant in Pain Medicine NHS TaysideDr. John McGarrity General Practitioner NHS LanarkshireDr. Danny McGhee General Practitioner NHS GlasgowDr. Denis Martin Research Fellow with special Sheffield Hallum
interest in Chronic Pain University Chairman, Pain Association, Scotland
Ms Tracey Nairn Dietician Care CommissionMr John Norden Lecturer in Nursing Studies Bell College, LanarkshireProfessor Ian Power Head of Anaesthesia, Critical Care The University of Edinburgh
and Pain Medicine NHS LothianDr David Reilly Medical Director Homeopathic Hospital,
GlasgowDr. Blair Smith General Practitioner The University of Aberdeen
Senior LecturerDr. Nicola Stuckey Head of Clinical Psychology NHS LothianDr Tun Than Consultant Anaesthetist NHS Western Isles Mrs. Heather Wallace National Organiser Pain ConcernDr Asad Zoma Consultant in Rheumatology NHS Lanarkshire

Management of chronic pain in adults
NHS Quality Improvement Scotland Support Team
Paula Carson Unit Secretary
Louise Foster Information Scientist
Rosemary Hector Practice Development Project Coordinator
Annie Wright Communication and Publication Officer
Further Information
For further information about NHS QIS, or to obtain additional copies ofthis best practice statement, please contact:
NHS Quality Improvement Scotland
Edinburgh Office
Elliott House
8-10 Hillside Crescent
Edinburgh
EH7 5EA
Tel: 0131 623 4300
Fax: 0131 623 4299
[email protected]@nhshealthquality.org
Copies of all NHS QIS publications can also be downloaded from the
website (www.nhshealthquality.org).
51

52
Glossary of Terms
AHP Allied Health Professions
acute pain Related to injury and resolves during an appropriate
healing period.
addiction The compulsive use of opioids or other agent to the
detriment of the user’s physical and/or psychological
health and/or social function. Signs of compulsive use
include preoccupation with obtaining opioids,
apparently impaired control over their use, and reports
of craving. These signs of compulsive use are well
established where opioids are taken not primarily for
pain relief but for effects on mood and thinking (The
Pain Society 2004).
allodynia Pain due to a stimulus which does not normally
provoke pain (IASP)
analgesia Absence of pain or suppression of pain
analgesic Substance or technique that reduces pain
BNF British National Formulary
chronic pain Pain that persists for more than 3 months or that
outlasts the healing process.
complementary Any range of medical treatments that fall beyond the
therapy scope of scientific medicine
dysaesthesia An unpleasant abnormal sensation, whether
spontaneous or evoked (IASP)
hyperalgeisa Increased sensitivity to pain or noxious stimulation
hyperaesthesia Increased sensitivity to stimulation
IASP International Association for the Study of Pain
NMC Nursing and Midwifery Council
neuralgia Pain in the distribution of a nerve
neuropathic pain Pain initiated or caused by a primary lesion or
dysfunction in the nervous system (IASP)
NHS QIS NHS Quality Improvement Scotland
nociceptive Pain Pain due to tissue damage i.e. skin, muscle, bone,
viscera
opioid A broad term that applies to any substance which
produces its effects by binding opioid receptors and
which is stereospecifically antagonised by naloxone
(Shug & Cardwell 2003)

Management of chronic pain in adults
pain An unpleasant sensory and emotional experience
associated with actual or potential tissue damage or
described in terms of such damage (IASP 1994)
paraesthesia An abnormal sensation, whether spontaneous or
evoked.
physical Is the physiological adaptation of the body to the
dependence presence of an opioid
pruritis Where irritation of sensory nerve endings leads to
localised or more general itching
sensitisation Elevated spontaneous activity in neurones, lowered
activation thresholds, and increased response to stimuli
tolerance State of adaptation in which exposure to a drug
induces changes that result in a diminution of one or
more of the drug’s effects over time. Increased doses
are then needed to get the same effect.
unconventional/ Diverse group of drugs that have a primary indication
adjuvant other than pain, but are used to enhance analgesia in
analgesics specific circumstances (WHO 2002)
WHO World Health Organization
withdrawal usually occurs when pharmacological agents eg opioids
are stopped suddenly, or an antagonist such as
naloxone or naltrexone is administered. Withdrawal is
easily avoided by gradual reduction of opioid dose
(The Pain Society 2004).
53

54
References
Ambler N., de C Willaims A., Hill P., Gunary R., Cratchley G. (2001) Sexualdifficulties of chronic pain patients. Clinical Journal of Pain. 17 (2) 138–145
American Geriatric Society Panel on Persistent Pain in Older Persons(2002) The Management of persistent pain in older persons. Journal of theAmerican Geriatrics Society. (2002) 50 (6): S205–S224
Arthritis Research Campaign. Retrieved URL: http://www.arc.org.uk/about-arth/astats.htm Accessed 15 November 2005
Bernabei R, Gambassi G., Lapane K., Landi F.,Gatsonis C., Dunlop r., LipsitzL., Steel K.,Mor V. (1998) Management of pain in elderly patients withcancer. JAMA. 279 (23): 1877–1882
Blomqvist K., Edberg A (2002) Living with persistent pain: experiences of older people receiving home care. Journal of Advanced Nursing. 40 (3): 297–306
Bonica J.J., Loeser J.D. (2001) History of pain concepts and therapies.In: Loeser J.D., Butler S.H., Chapman C. R., Turk D. (eds) Bonica’sManagement of pain (third edition) Philadelphia Lippincott, Williams andWilkins: p3
Bourbonnais F.F., Perreault A., Bouvette M. (2004) Introduction of a painand symptom assessment tool in the clinical setting – lessons learned.Journal of Nursing Management. 12 (3) 194–200
Breivik H., Collett B., Ventafridda V., Cohen R., Gallacher D (2005) Surveyof chronic pain in Europe: Prevalence, impact on daily life, and treatment.European Journal of Pain. Article in Press.
British Association/College of Occupational Therapists UK, Definition ofOccupational Therpay. COT2 2004
British Pain Society, (2005) Recommendations for the appropriate use ofopioids for persistent non cancer pain. London
British Pain Society, (2004) Spinal cord stimulation for the management ofpain: provisional recommendations for best clinical practice. London
Bullington J., Nordemar R., Nordermar K Sjostrom- Flanagan C. (2003)Meaning out of chaos: a way to understand chronic pain. ScandinavianJournal of Caring Sciences 17 (4): 325–331

Management of chronic pain in adults
Callister LC., (2003) Cultural influences on pain perceptions andbehaviours. Home Health Care Management & Practice 15 (3): 207–211
Cancer Pain Relief: (1996) With a guide to opioid availability World HealthOrganization, Geneva, Switzerland
Chapman CR., Garvin J (1999) Suffering: the contributions of persistentpain. The Lancet 353 (9171): 2233–2237
Cleland JA., Palmer JA., Venzke JW. (2005) Ethnic differences in painperception. Physical Therapy Reviews 10 (2): 113–122
Clinical Standards Advisory Group (CSAG) (1999) Services for patientswith pain Department of Health, London
Closs SJ. (1994) Pain in elderly patients: a neglected phenomenon? Journalof Advanced Nursing. 19 (6): 1072–1081
Closs SJ., Barr B., Briggs M. (2004) A comparison of five pain assessmentscales for nursing home residents with varying degrees of cognitiveimpairment. Journal of Pain & Symptom Management. 27 (3): 196–205
Davies J., McVicar A. (2000) Issues in effective pain control 1: assessmentand education. International Journal of Palliative Care. 6 (2): 58–65
Davis D., Evans L. (2001) Assessing pain in people with learningdisabilities British Journal of Nursing. 10 (8) 513–516
DeWit R., vanDam F., Vielvoye-Kerkmeer A, Mattern C., Abu-Saad HH.(1999) The treatment of chronic pain in a cancer hospital in theNetherlands. Journal of Pain and Symptom Management. 17 (5): 333–350
Donovan J. (2002) Learning disability nurses’ experiences of being with clients who may be in pain. Journal of Advanced Nursing. 38 (5): 458–466.
Duhmke RM., Cornblath DD., Hollingshead JRF.(2005)Tramadol for neuropathic pain. The Cochrane Database of SystematicReviews 2005; issue (3): (ID CD003726)
Dworkin RH., Backonja M., Rowbotham MC., Allen RR., Argoff CR., BennettGJ., Bushnell MC., Farrar JT., Galer BS., Haythornwaite JA., Hewitt DJ.,Loeser JD., Max MB., Saltarelli M., Schmader KE., Stein C., Thomson D.,Turk DC., Wallace MS., Watkins LR., Weinstein SM. (2003) Advances inNeuropathic Pain: Diagnosis, Mechanisms and TreatmentRecommendations. Archives of Neurology 60: 1524–1534
55

56
Dysvik E., Lindstrom T.C., Eikeland O., Natvig G K. (2004) Health relatedquality of life and pain beliefs among people suffering from chronic pain.Pain Management Nursing. 5 (2): 66–74
Elliott AM., Smith BBH., Penny KI., Smith WC., Chambers WA. (1999) The epidemiology of chronic pain in the community. Lancet. 354 (9186:) 1248–1253
Elliott AM., Smith BH., Hannaford PC., Smith WC., Chambers WA. (2002)The course of chronic pain in the community: results of a 4-year follow-up study. Pain. 99 (1-2): 299–307
Ferrell B A., Ferrell BR., Rivera L. (1995) Pain in cognitively impairednursing home patients. Journal of Pain & Symptom Management. 10 (8): 591–598
Flor H., Fydrich T., Turk DC (1992) Efficacy of multidisciplinary paintreatment centres: a meta-analytic review. Pain. 49 (2): 221–230
Gagliese L., Melzack R. (2003) Age-related differences in the quality butnot the intensity of chronic pain. Pain. 104 (3): 597–608
Gureje O., Von Korff M., Simon G., Gater R. (1998) Persistent pain andwell being: A World Health Organization Study in Primary Care. JAMA.280 (2): 147–151
Haetzman M., Elliott AM., Smith BH., Hannaford P, Chambers WA. (2003)Chronic pain and the use of conventional and alternative therapy. FamilyPractice. 20 (2) 147–154
Higgins I., Madjar I., Walton J.A. (2004) Chronic pain in elderly nursinghome residents: the need for nursing leadership. Journal of NursingManagement. 12 (3): 167–173
Horgas A.L., Dunn K.D. (2001) Pain in Nursing Home Resident: acomparison of resident’s self-report and nursing assistant’s perceptions.Journal of Gerontological Nursing 27 (3): 44–53
International Association for the Study of Pain (IASP) (1986) Pain. Suppl 3 S1–S225
Johnson I. (2000) The Clinical Effectiveness of TENS in Pain Management.Physical and Rehabilitation Medicine 12: 131–149
Jones D. (2003) Pain management and people with learning disabilities: acomplex challenge. Journal of Learning Disabilities. 7 (4): 291–295

Management of chronic pain in adults
Jones D., Martin D., Steedman WM., Ravery J. (2001) A survey of primaryand social care professionals attitudes and beliefs about chronic non-cancer pain. Poster presentation. Pain Society Annual Scientific Meeting,University of York
Kaye A.D., Akye A.M., Hegazi A., Sabar R., Deaton B., Powel J., Hofbauer R.(2002) Natraceuticals: Potential roles and potential risk for painmanagement. Pain Practice 2 (2): 122–128
Keefe FJ., Bonk V. (1999) Psychosocial assessment of pain in patientshaving rheumatic diseases. Rheumatic Disease Clinics of North America.25 (1): 81–103
Kehlet H., Holte K. (2001) Effect of post operative analgesia on surgicaloutcome. British Journal of Anaesthesia. 87 (1): 62–72
Kendall NAS., Linton SJ., Main CJ. (1997) Guide to assessing psychologicalyellow flags in acute low back pain: risk factors for long term disabilityand work loss. Accident Rehabilitation and Compensation InsuranceCorporation of New Zealand and the National Health Committee.Wellington, New Zealand
Lamberg L. (1999) Chronic pain linked with poor sleep: exploration ofcauses and treatment. JAMA. 281 (8): 691–692
Lasch KE. (2000) Culture, pain and culturally sensitive pain care. PainManagement Nursing 1 (3) 2: 16–22
Lorig K R., Sobel DS., Stewart AL., Brown BW., Bandura A., Ritter P.,Gonzalez VM., Laurent DD., Holman HR. (1999) Evidence suggesting that a chronic disease self management programme can improve healthstatus while reducing hospitalization: A randomized trial. Medical Care. 37 (1): 5–14
McCaffery M. (1980) Understanding your patient’s pain. Nursing. 10 (9):26–31
McCaffery M.(1999) In: McCaffery M and Paesero C, Pain: Clinical Manual.2nd Ed Moseby. St Louis
McCaffery M., Ferrell BR., Paesero C. (2000) Nurses’ personal opinionsabout patients’ pain and their effect on recorded assessments and titrationof opioid doses. Pain Management Nursing. 1(3): 79–87McEwen J (2004) Chronic Pain Services in Scotland, Scottish ExecutiveHealth Department
57

58
McGrath PJ., Rosmus C., Campbell MA., Hennigar AW. (1998) Behaviourscaregivers use to determine pain in nonverbal cognitively impairedindividuals. Developmental Medicine and Child Neurology. 40: 340–343
McQuay, HJ., Tramer M., Nye BA., Carroll D., Wiffen PJ., Moore RA.(1996) A systematic review of antidepressants in neuropathic pain. Pain.68 (2-3): 217–227
McQuay HJ., Moore RA., Eccleston C., Morley S., Williams AC. (1997)Systematic review of outpatient services for chronic pain control. HealthTechnology Assessment. 1 (6): 1–135, Winchester, England
Macrae W A. (2001) Chronic pain after surgery. British Journal ofAnaesthesia. 87 (1): 88–98
Main CJ, Spanswick CC. (2000) Pain Management: an interdisciplinaryapproach, Edinburgh: Churchill–Livingstone, 2000
Mannion AF., Muntener M., Taimela S., Dvorak J. (2001) Comparison ofthree active therapies for chronic low back pain: results of a randomisedclinical trial with one-year follow up. British Journal of Rheumatology. 40 (7): 772–778
Matthews E. (2002) A snapshot view of the impact of chronic pain onadolescents. British Journal of Nursing. 11 (11): 735–744
Mitchell A., Kafai S. (1997) Patient education in TENS pain management.Professional Nurse. 12 (11): 804–807
Management Advisory Service. (1989) Review of Clinical PsychologyServices; activities and possible models. Cheltenham
Morin CM., Gibson D., Wade J. (1998) Self reported sleep and mooddisturbance in chronic pain patients. Clinical Journal of Pain. 14 (4): 311–314
Morley S., Eccleston C., Williams A. (1999) A systematic review and meta-analysis of randomised controlled trials of cognitive behaviour therapyand behaviour therapy for chronic pain in adults excluding headache.Pain. 80 (1–2) 1–13
National Institute of Health Technology Assessment Panel on integrationof behavioural and relaxation approaches into the treatment of chronicpain and insomnia. (1996). Integration of behavioural and relaxationapproaches into the treatment of chronic pain and insomnia. JAMA 276 (4): 313–318
Management of chronic pain in adults
Nueropathy Trust. Retrieved URL http://www.neuropathy-trust.org/Accessed 15 November 2005
Nicholson BD. (2003) Diagnosis and management of neuropathic pain: abalanced approach to treatment. Journal of the American Academy ofNurse Practitioners (Supplement). 15 (12): 3–9
Nursing and Midwifery Council (2004) Guidelines for the Administrationof Medicines NMC London.
Olason M. (2004) Outcome of an interdisciplinary pain managementprogramme in a rehabilitation clinic. Work 22 (1): 9–15
Oxford Pain Research Trust, Oxford League Table of Analgesic EfficacyRetrieved URLhttp://www.jr2.ox.ac.uk/bandolier/painpag/Acuterev/analgesics/leagtab.html Accessed 15 November 2005
Paice J. (2003) Sexuality and chronic pain: what your patients may notbe telling you. American Journal of Nursing. 103 (1): 87–89
Pain in Europe. (2003) A 2003 Report. Research project by NFOWorldgroup funded by an educational grant from MundipharmaInternational Limited., Cambridge, England.
Pellino TA., Willens J., Polomano RC., Heye M. (2002) The AmericanSociety of Pain Management Nurses practice analysis: role delineationstudy . Pain Management Nursing. 3 (1): 2–15
Perkins FM., Kehlet H. (2000) Chronic pain as an outcome of surgery: areview of predictive factors. Anaesthesiology. 93 (4):1123–1133
Pizzi LT., carter CT., Howell JB., Vallow SM., Crawford AG., Frank ED.(2005) Work loss, healthcare utilisation, and costs among US employeeswith chronic pain Disease Management Health Outcomes. 13 (3) 201–208
Price DD (1999) Psychological mechanisms of pain and analgesia. Progressin pain research and management. IASP Press, Seattle USA
Proctor WR. Hirdes JP. (2001) Pain and cognitive status among nursinghome residents in Canada. Pain Research and Management 6 (3): 119–125
Portenoy R.K. (1994) Opioid therapy for chronic non malignant pain:current status. In: Fields HL., Liebskind JC, Eds., Progress in Pain Researchand Management IASP Press Seattle, USA p247–287.
59

60
Portenoy RK. (1996) Opioid therapy for chronic non malignant pain:Clinicians perspective. Journal of Law, Medicine and Ethics. 24 (4) 296–309
Rao JK., Mihaliak K., Kroenke K., Bradley J., Tierney W., Weinberger M.(1999) Use of complimentary therapies for arthritis among patients ofRheumatologists Annals of Internal Medicine. 131 (6): 409–416
Recommendations for the appropriate use of opioids for persistent non-cancer pain The British Pain Society (2004) London.
Rucker KS., Metzler HM., Kregel J. (1996) Standardisation of Chronic PainAssessment: A multiperspective approach. Clinical Journal of Pain. 12 (2): 94–110
Rusteon T., Wahl AK., Hanestad BR., Lerdal A., Paul S., Miaskowski C.(2005) Age and the experience of chronic pain: differences in health and quality of life among younger, middle-aged and older adults. ClinicalJournal of Pain. 21 (6) 513–523
Saarto T., Wiffen PJ. (2005) Antidepressants for neuropathic pain TheCochrane Database of Systematic Reviews (2005) Issue 3 Art No:CD005454. DOI:10.1002/14651858.CD005454
Savage S.R. (1996) Long-term opioid therapy: assessment of consequencesand risks. Journal of Pain and Symptom Management. 11 (5) 274–286
Scottish Intercollegiate Guidelines Network. SIGN Guideline No. 31 (1998)Report on a Recommended Referral Document. NHS QualityImprovement Scotland Edinburgh.
Scottish Intercollegiate Guidelines Network. SIGN Guideline No.44 (2000)Control of pain in patients with cancer. NHS Quality ImprovementScotland Edinburgh.
Sindrup SH., Otto M., Finnerup NB. Jensen TS (2005) antidepressants in thetreatment of neuropathic pain. Basic and Clinical Pharmacology &Toxology 96 (6): 399–409
Smith AA (2003) Intimacy and family relationships of women withchronic pain. Pain Management Nursing. ) 4 (3): 134–142
Smith BH., Elliott AM., Chambers WA., Smith WC., Hannaford PC., Penny K(2001) The impact of chronic pain in the community. Family Practice. 18 (3): 292–299

Management of chronic pain in adults
Smith MT., Perlis ML., Giles DE., Carmody TP. (2000) Sleep quality and presleep arousal in chronic pain. Journal of Behavioural Medicine. 23 (1): 1–13
Snyder M., Wieland J. (2003) Complimentary and alternative therapies:what is their place in the management of chronic pain? The NursingClinics of North America 38 (3): 495–508
Snow AL., Weber JB., O’Malley CM., Beck C., Bruera E., Ashton C., KunikME. (2003) NOPAIN: a nursing assistant-administered pain assessmentinstrument for use in dementia. Dementia and Geriatric CognitiveDisorders. 921: 1–8
Sohn P.M., Cook C.A.L. (2002) Nurse practitioner knowledge ofcomplementary alternative healthcare; foundation for practice. Journal ofAdvanced Nursing) 39 (1): 9–16
Solomon P. (2001) Congruence between health professionals and patientspain ratings; a review of the literature. Scandinavian Journal of CaringSciences. 15 (2): 174–180
Stephenson NLN., Dalton JA. (2003) Using reflexology for painmanagement. Journal of Holistic Nursing. 21 (2): 179–91
Strong J (1996) Chronic Pain an occupational therapist perspective.Churchill Livingston. Melbourne Australia : p54
Stroud MW., McKnight PE., Jensen MP. (2004) Assessment of self reportedphysical activity inpatients with chronic pain: Development of anabbreviated Roland Morris disability scale. The Journal of Pain. 5 (5): 257–263
Subramaniam V., Stewart MW., Smith JF. (1999) The development andimpact of a chronic pain support group: a qualitative and quantitativestudy. Journal of Pain and Symptom Management. 17 (5) 376–383
Svendsen KB., Andersen S., Arnason S., Arner S., Breivik H., Heiskanen T.,Kalso E., Kongsgaard UE., Sjogren P., Strang P., Bach FW., Jensen TS. (2005)Breakthrough pain in malignant and non-malignant diseases: a review ofprevalence, characteristics and mechanisms. European Journal of Pain. 9 (2): 195–206
Thomsen AB., Sorensen J., Sjogren P., Eriksen J. (2002) Chronic nonmalignant pain patients and health economic consequences. EuropeanJournal of Pain (6): 341–352
61

62
Treatment Choice in Psychological Therapies and Counselling (2001)Evidence based clinical guidelines. Department of Health. England.
Turk DC., Burwinkle TM. (2005) Assessment of chronic pain inrehabilitation: Outcomes measures in clinical trials and clinical practice.Rehabilitation Psychology. 50 (1): 56–64
Twycross A. (2000) Education about pain: a neglected area? NurseEducation Today. 20: 244–253
Van Niekerk LM., Martin F. (2003) The impact of the nurse – physicianrelationship on barriers encountered by nurses during pain management.Pain Management Nursing. 4 (1): 3–10
Verhaak PFM., Kerssens JJ., Dekker J., Sorbi MJ., Bensing JM. (1998)Prevalence of chronic benign pain disorder among adults: a review ofthe literature. Pain. 77: 231–239
Vlaeyen JWS., Morley S. (2005) Cognitive Behavioural Treatments forChronic Pain: What works for whom? Clinical Journal of Pain. 21 (1): 1–8
Von Korff M., Wagner EH., Dworkin SF., Saunders KW. (1991) Chronic painand the use of ambulatory healthcare. Psychosomatic Medicine. 53 (1): 61–79
Waddell G. (1996) Low Back Pain: a twentieth century healthcare enigma.Spine 21 (24) 2820–2825
Waddell G. Newton M,m Henderson I., Somerville D., Main CJ. (1993) aFear-Avoidance Beliefs Questionnaire and the role of fear-avoidancebeliefs in chronic low back pain and disability. Pain 52 (2) 157–168
Waddell G. (1998) The Back Pain Revolution. Churchill Livingston.Edinburgh
Wasan AD., Davar G., Jamieson R. (2005) The association betweennegative affect and opioid analgesia in patients with discogenic low backpain. Pain. 117: 450–461
Wiffen PJ., McQuay HJ., Edwards JE., Moore RA. (2005) Gabapentin foracute and chronic pain. The Cochrane Database of Systematic Reviews(2005) Issue 3 Art No: CD005452.DOI10.1002/14651858.CD005452
World Health Organization (WHO) (2002) The essential adjuvantanalgesics for neuropathic pain. Cancer Pain Release 15 (2), Geneva,Switzerland.




NHS Quality Improvement ScotlandEdinburgh Office Glasgow OfficeElliott House Delta House8-10 Hillside Crescent 50 West Nile StreetEdinburgh EH7 5EA Glasgow G1 2NP
Phone: 0131 623 4300 Phone: 0141 225 6999Textphone: 0131 623 4383 Textphone: 0141 241 6316
Email: [email protected]: www.nhshealthquality.org
This document is produced from elemental chlorine-free material and is sourced from sustainable forests
You can read and download this document from our website.We can also provide this information:
• by email• in large print• on audio tape or CD• in Braille, and• in community languages.













![Psychological therapies for the management of chronic … · [Intervention Review] Psychological therapies for the management of chronic pain (excluding headache) in adults Christopher](https://static.fdocuments.us/doc/165x107/5b0880497f8b9a93738c7862/psychological-therapies-for-the-management-of-chronic-intervention-review-psychological.jpg)




