Management of adverse effects of cancer chemotherapy 1
70
MANAGEMENT OF ADVERSE EFFECTS OF CANCER CHEMOTHERAPY
-
Upload
dr-pooja -
Category
Health & Medicine
-
view
41 -
download
0
Transcript of Management of adverse effects of cancer chemotherapy 1

MANAGEMENT OF ADVERSE EFFECTS
OF CANCER CHEMOTHERAPY
CANCER
An abnormal growth of cells which tend
to proliferate in an uncontrolled way and,
in some cases, to metastasize (spread).
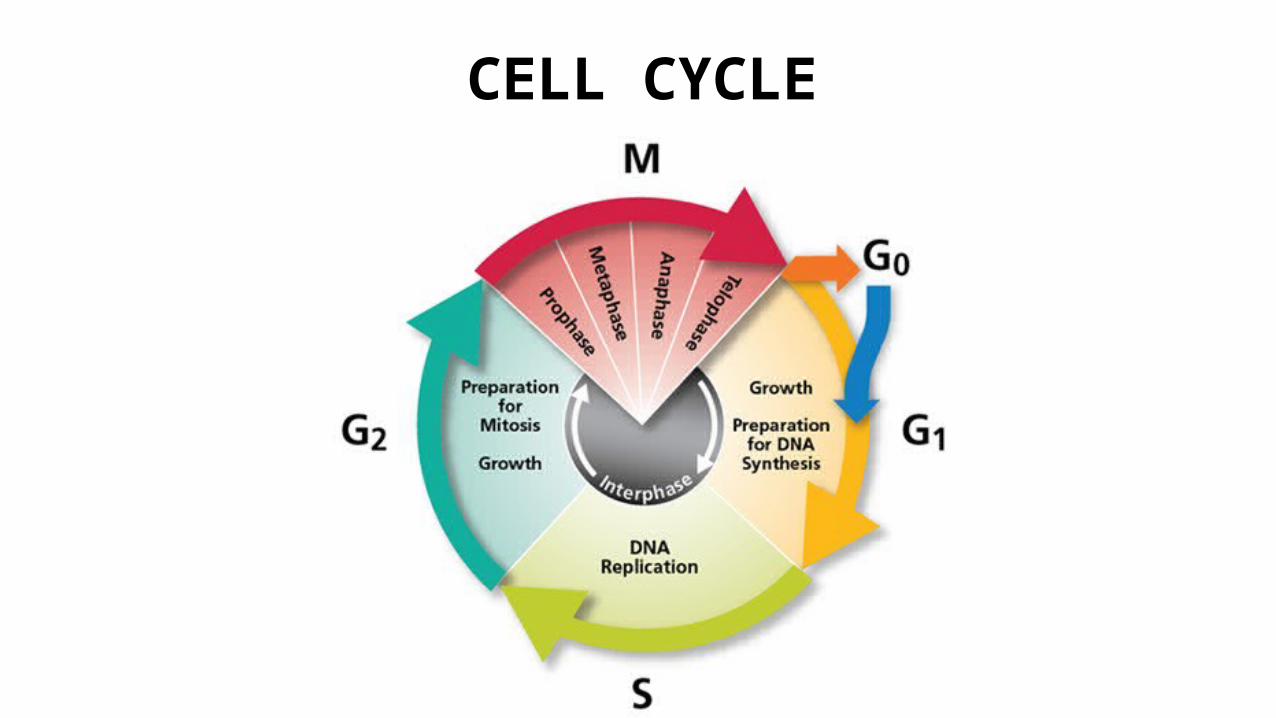
CELL CYCLE

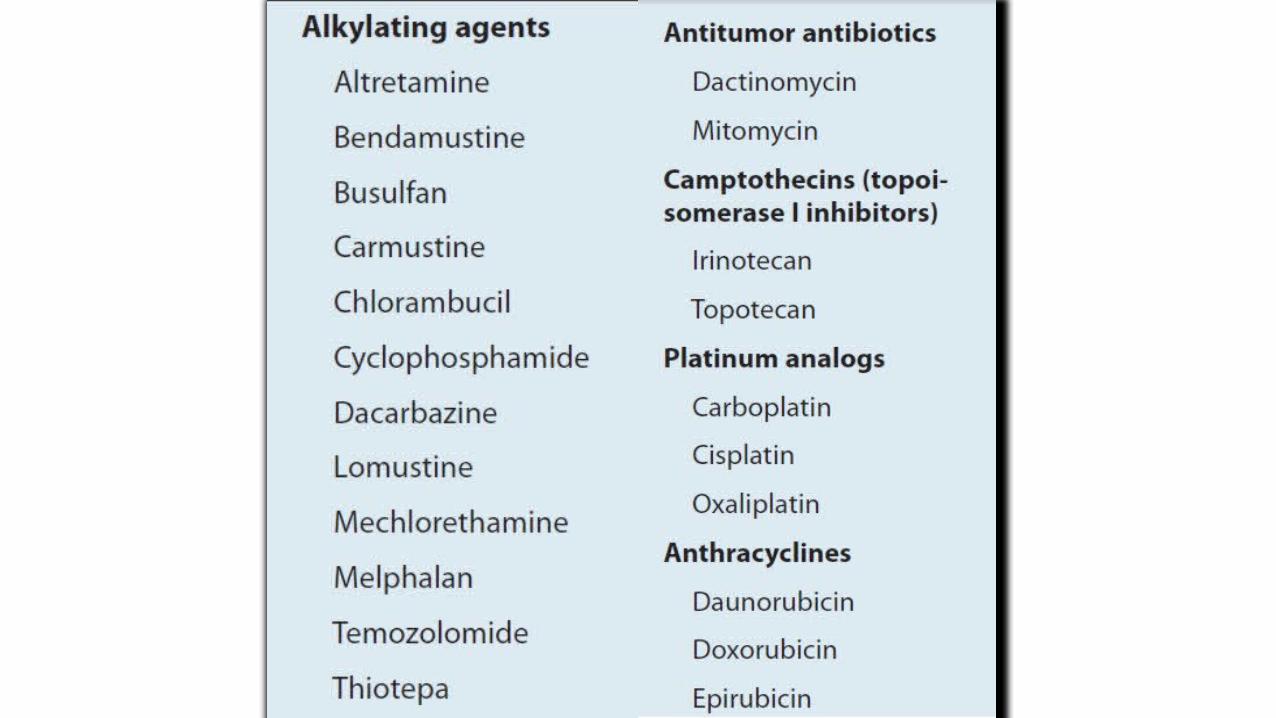
CLASSIFICATION OF ANTICANCER DRUGS
CELL CYCLE SPECIFIC AGENTS
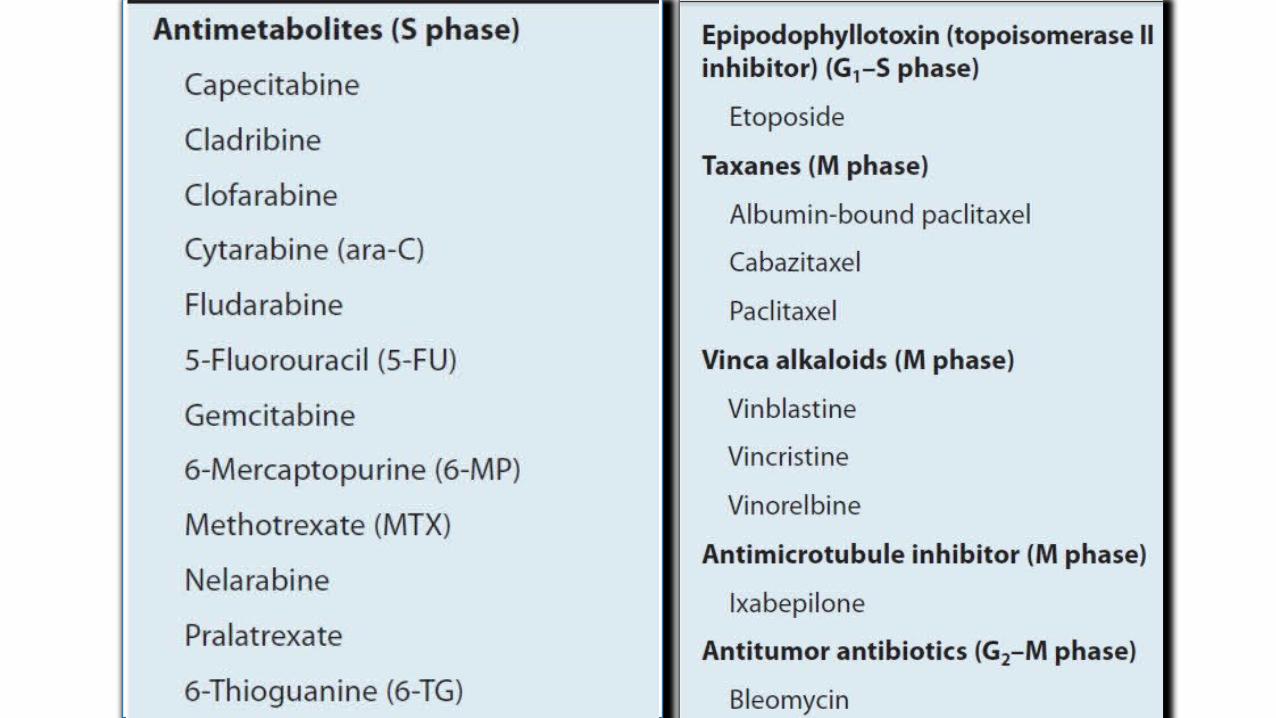
CELL CYCLE NON SPECIFIC AGENTS
GENERAL ADVERSE EFFECTS OF ANTICANCER DRUGS1. Immediate ADR: Nausea, Vomiting
2. Myelosuppression
3. Mucositis
4. Alopecia
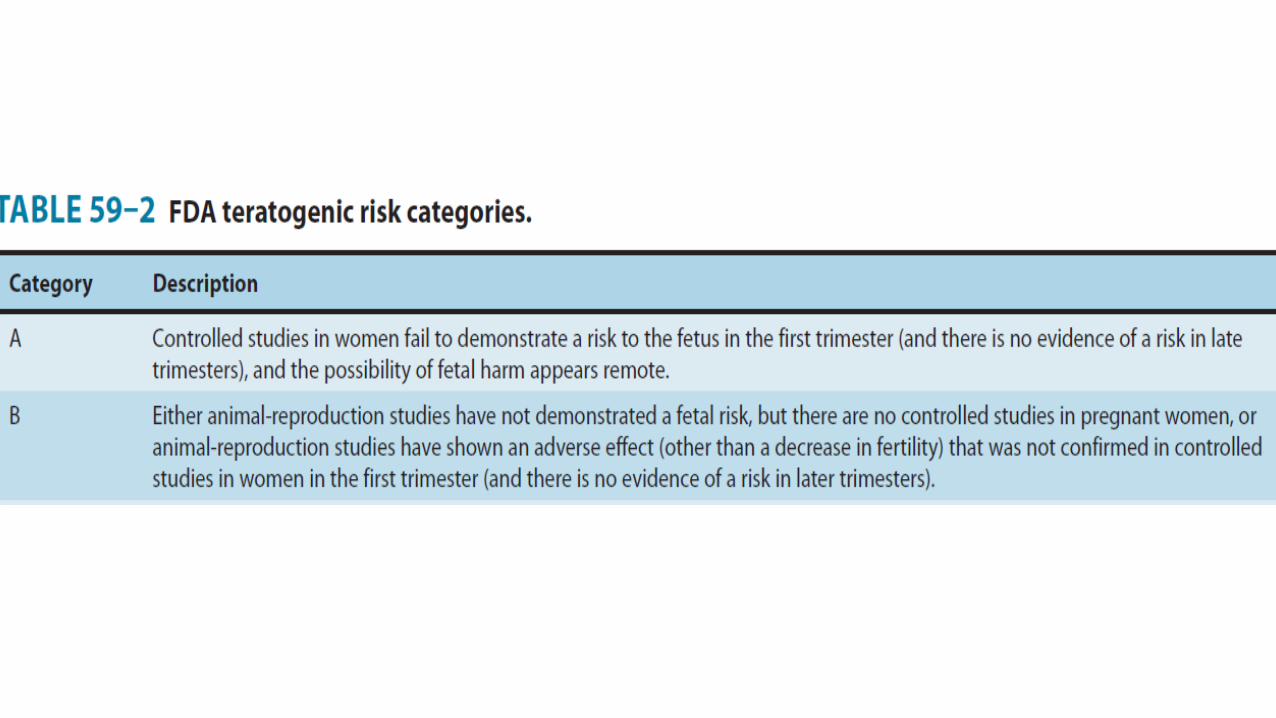
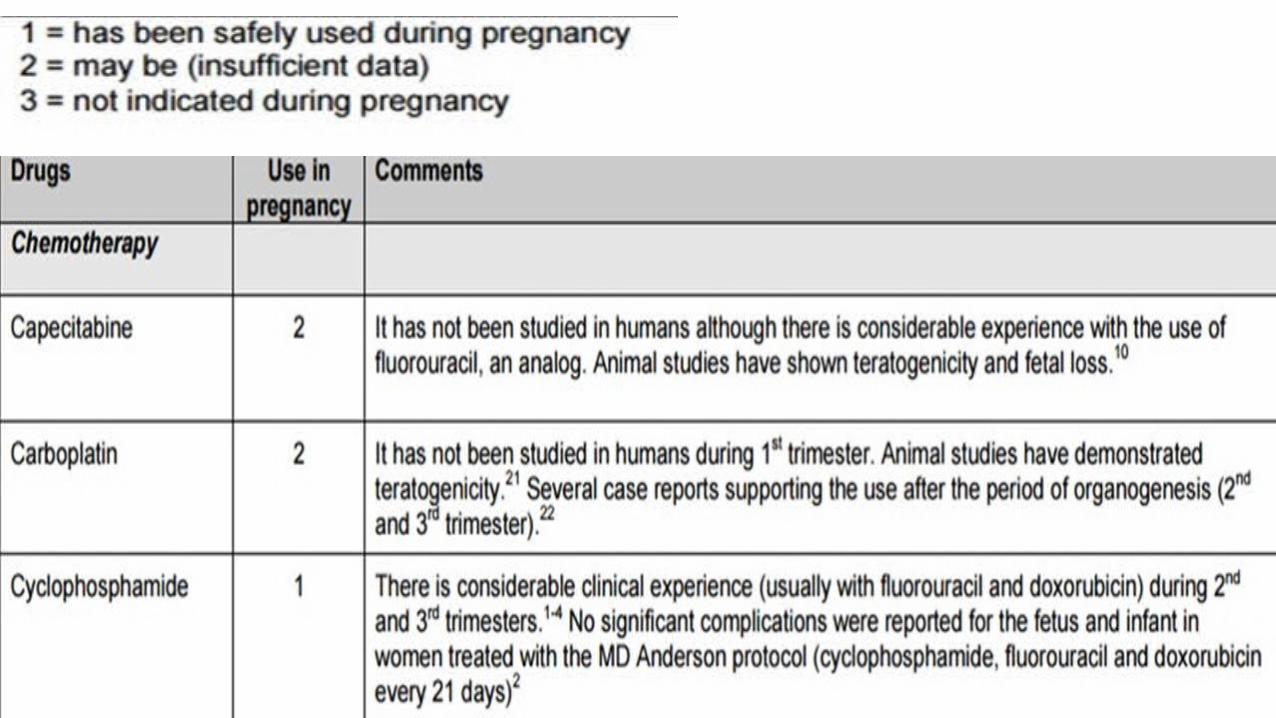
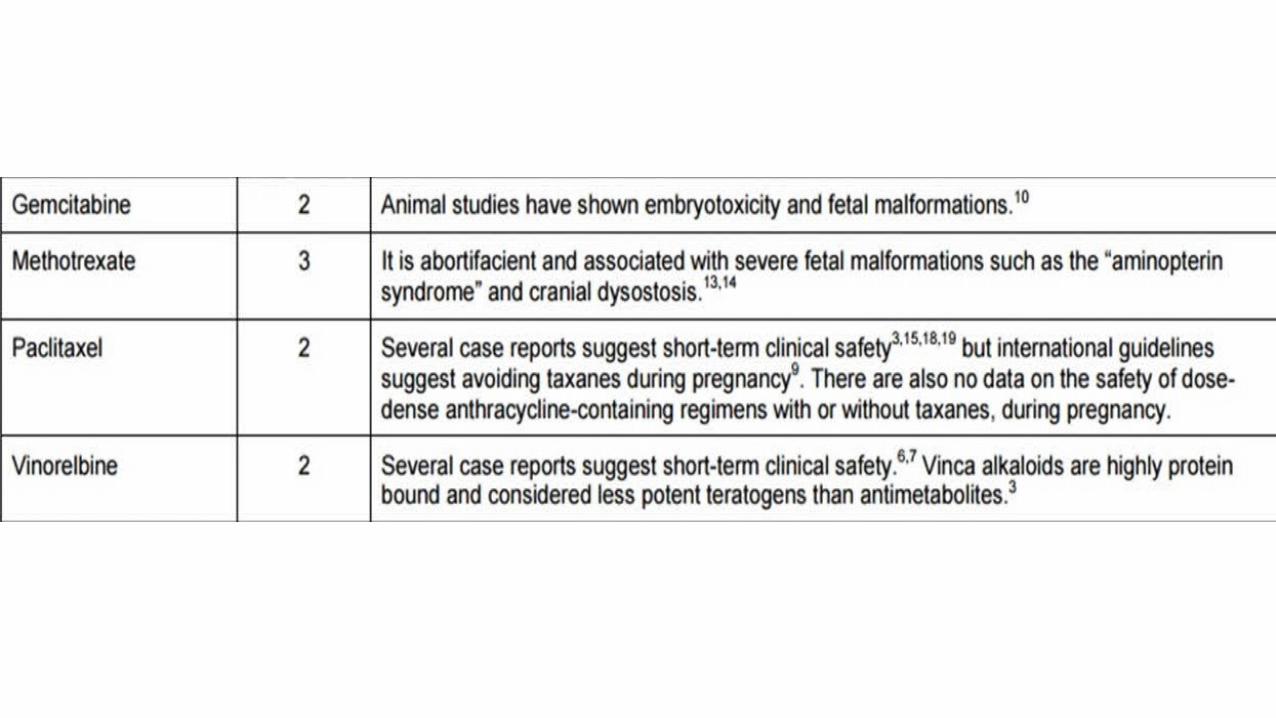
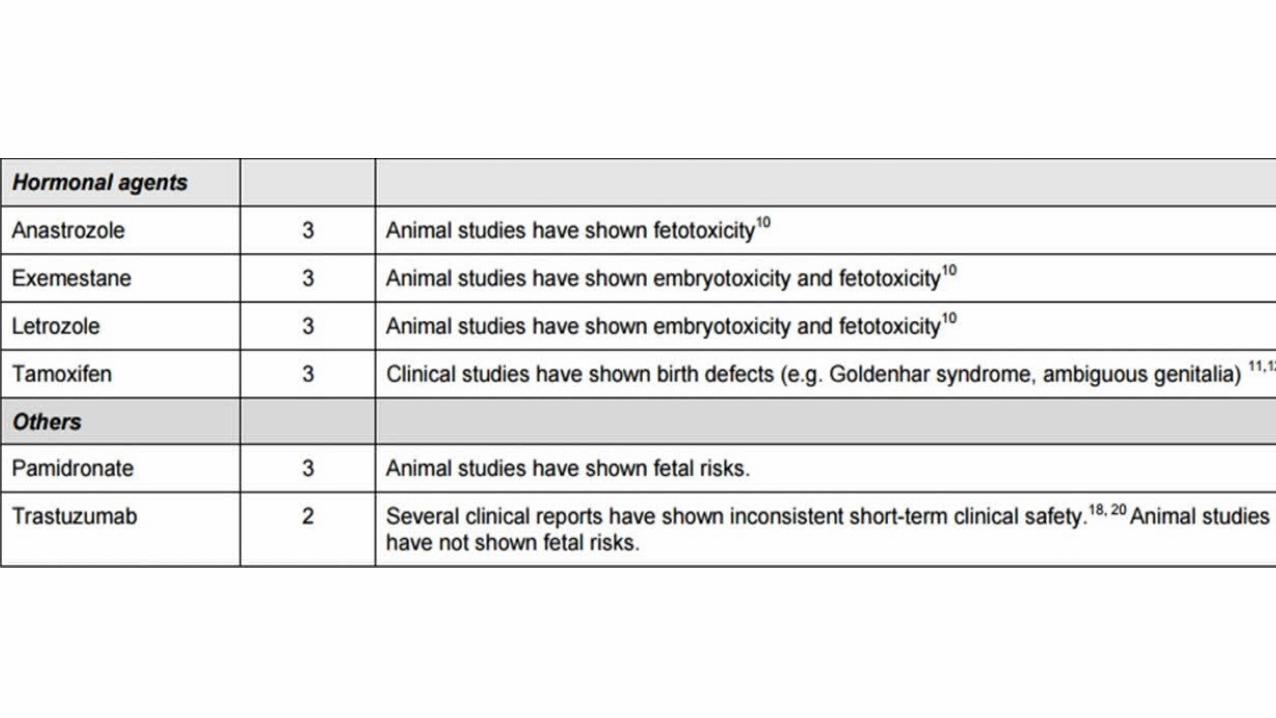
5. Teratogenicity

NAUSEA AND VOMITING• Emesis; nausea- protective reflexes- to get rid of toxic
substances- prevents further ingestion.
• Central emesis center:• Chemoreceptor trigger zone in area postrema at bottom of 4th
ventricle• Solitary Tract nucleus.
NAUSEA AND VOMITING• Inputs to emesis center from- vagus nerve, splanchnic
afferents, cerebral cortex, vestibular apparatus.
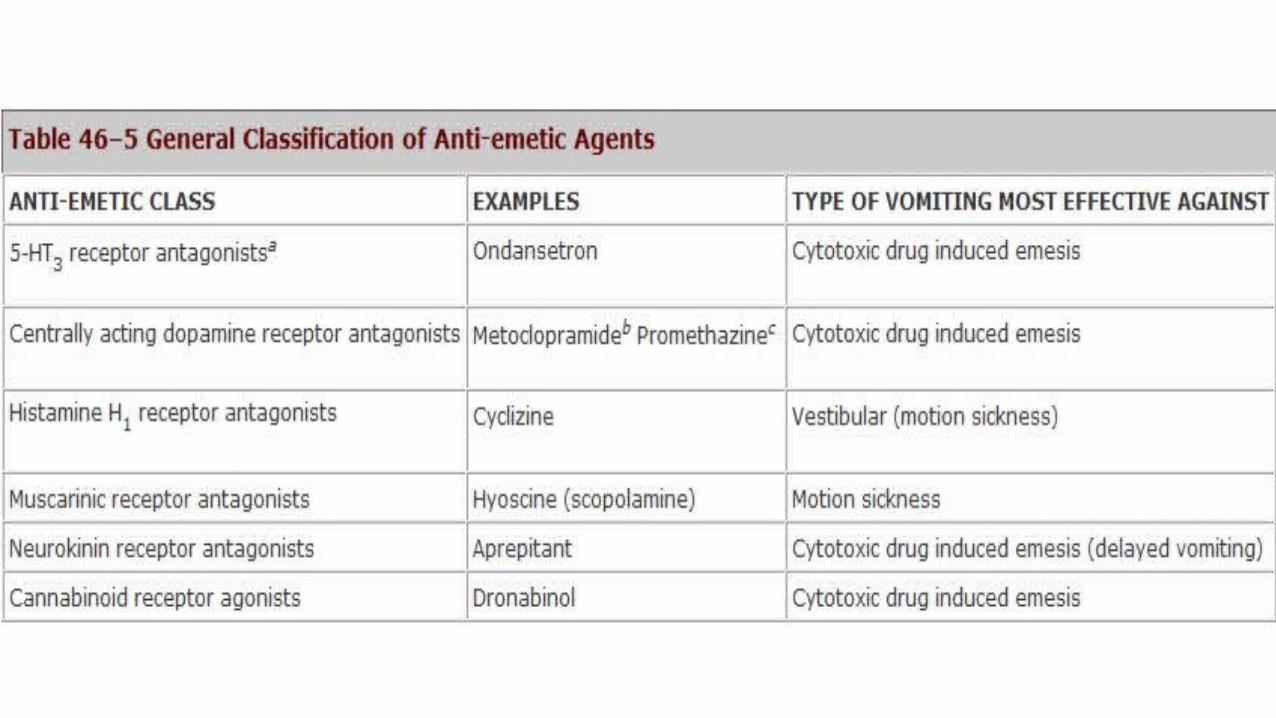
• Receptors on:• CTZ- Serotonin (5HT3), Dopamine (D2), Opioids.• STN- encephalin, histamine, ACh, 5HT3.


NAUSEA AND VOMITING
1. Anticipatory- conditioned reflex to sight and smell
2. Acute- within 24hrs of chemotherapy
3. Delayed- more than 24hrs

DRUGS CAUSING NAUSEA AND VOMITING
• Highly emetogenic- cisplatin, carmustine, cyclophosphamide,
dacarbazine, mechlorethamine, streptozocin
•Moderate emetogenic- doxorubicin, daunorubicin,
cytarabine, oxaliplatin, carboplatin, ifosfamide
DRUGS CAUSING NAUSEA AND VOMITING
• Low emetogenic- Etoposide, 5-FU, gemcitabine, MTX,
pemetrexed, mitomycin, paclitaxel
• Least emetogenic- Vinca alkaloids, cladarabine, bevacizumab.
ANTI-EMETIC AGENTS IN CANCER CHEMOTHERAPY
• LOW RISK OF EMESIS:• PRE- CHEMOTHERAPY• Dexamethasone• Metoclopramide± diphenhydramine• Prochlorperazine ± Lorazepam
• POST- CHEMOTHERAPY(delayed emesis)• None
ANTI-EMETIC AGENTS IN CANCER CHEMOTHERAPY
•MODERATE RISK OF EMESIS
• PRE-CHEMOTHERAPY
• 5HT3 antagonist+ dexamethasone
• 5HT3 antagonist+ dexamethasone+ aprepitant
ANTI-EMETIC AGENTS IN CANCER CHEMOTHERAPY
•POST- CHEMOTHERAPY (delayed emesis)
• Aprepitant (days 2 and 3)
• Dexamethasone or 5 HT3 antagonist (days 2-3 or 4)
• Aprepitant (days 2-3, if used pre-chemo) ±
dexamethasone (days 2-4) ± lorazepam (days 2-4)
ANTI-EMETIC AGENTS IN CANCER CHEMOTHERAPY
•HIGH RISK OF CHEMOTHERAPY
• PRE-CHEMOTHERAPY
• 5HT3 antagonist+ dexamethasone+ aprepitant ± lorazepam

ANTI-EMETIC AGENTS IN CANCER CHEMOTHERAPY
•POST- CHEMOTHERAPY (delayed emesis)
• Dexamethasone+ aprepitant
• Dexamethasone (days 2-4)+ aprepitant (days 2 and 3) ±
lorazepam (days 2-4)
MYELOSUPPRESSION• Chemotherapy induced myelosuppression drugs target
proliferating cells which includes both tumour cells and
hematopoietic cells.

MYELOSUPPRESSION•Manifestations- anemia; thrombocytopenia; neutropenia.
• Often managed with delay/ reduction in dose to allow hematopoietic activity to recover.
• Results in low relative dose intensity.

ANTICANCER DRUGS CAUSING MYELOSUPPRESSION
• Highest- • Alkylating agents;• Antimetabolites;• Anthracyclines- doxorubicin; daunorubicin
• Lowest-• Asparginase• Bleomycin• Vinca alkaloids• Hormonal antagonists
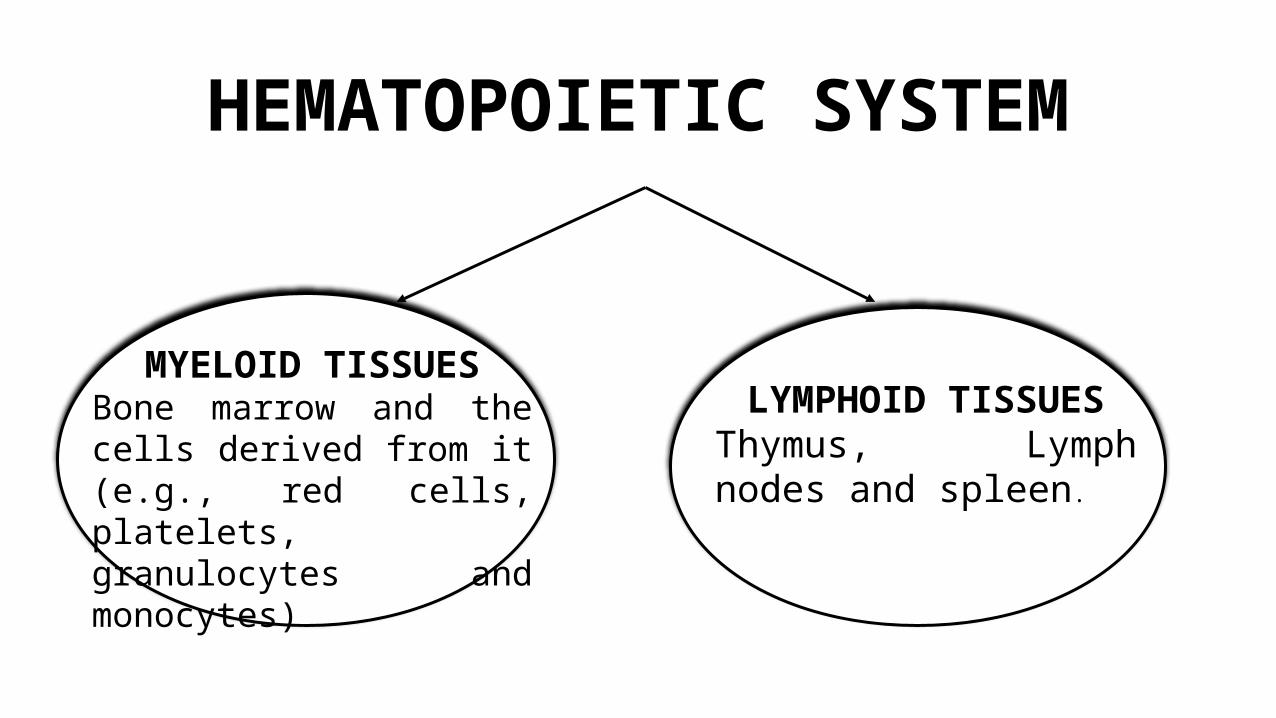
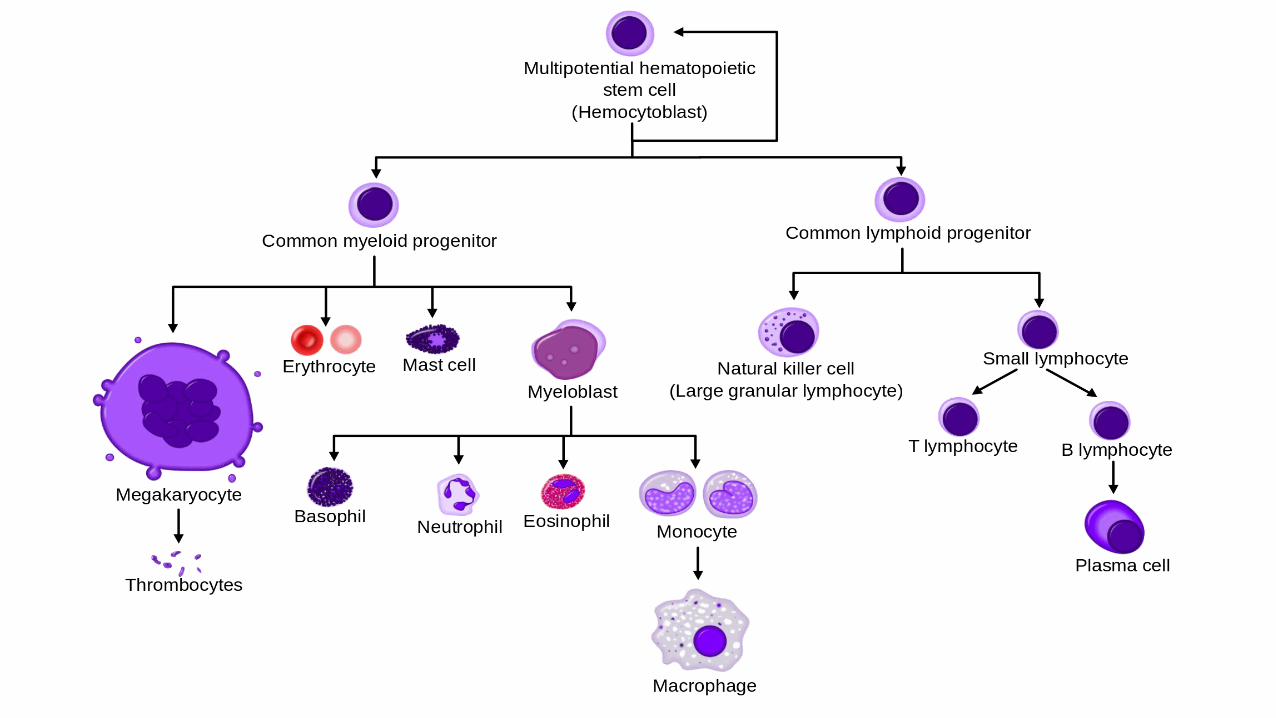
HEMATOPOIETIC SYSTEM
MYELOID TISSUESBone marrow and the cells derived from it (e.g., red cells, platelets, granulocytes and monocytes)
LYMPHOID TISSUESThymus, Lymph nodes and spleen.
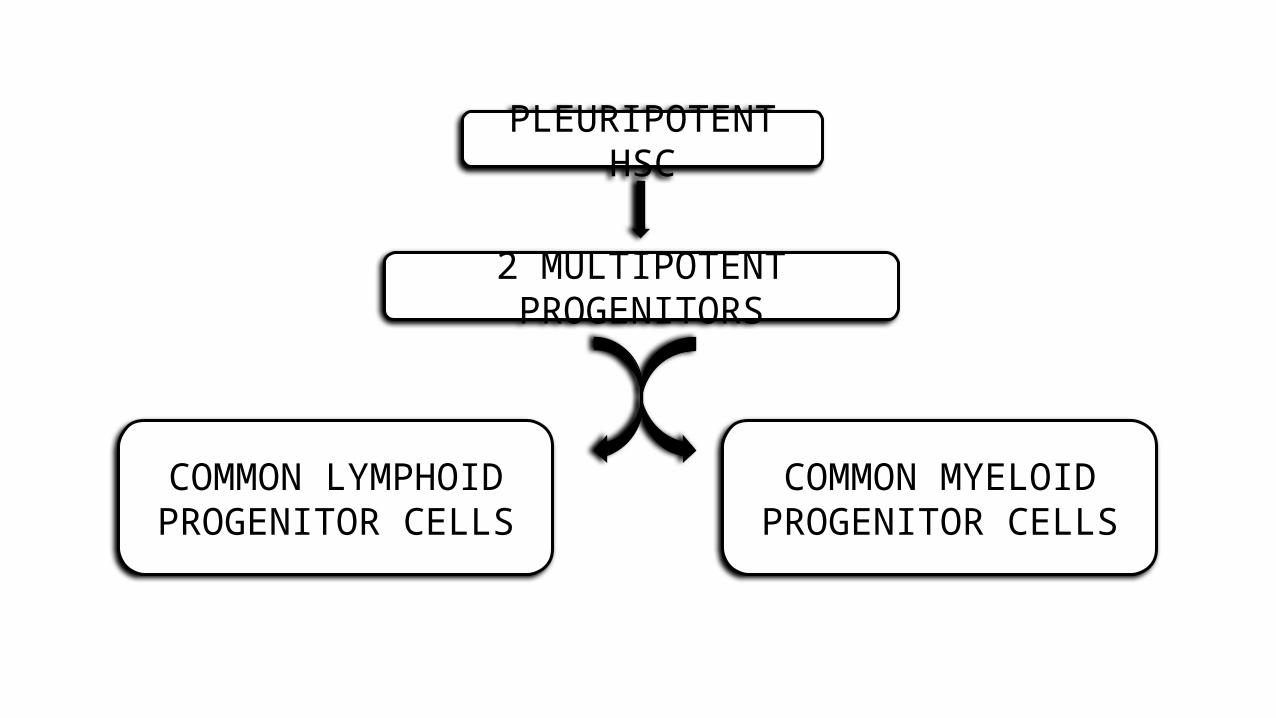
PLEURIPOTENT HSC
2 MULTIPOTENT PROGENITORS
COMMON LYMPHOID PROGENITOR CELLS
COMMON MYELOID PROGENITOR CELLS

COMMITTED PROGENITORS(COLONY FORMING UNITS)
PRECURSORS- MYELOBLASTS, PROERYTHROBLASTS, MEGAKARYOBLASTS.
MATURE GRANULOCYTES, RED CELLS AND PLATELETS.
CHEMOTHERAPY INDUCED ANAEMIA
• Recombinant human erythropoietin- epoetin alfa.
• Stimulates proliferation and maturation of committed erythroid progenitors to increase red cell production.
• 150 units/kg thrice a week or 450-600 units/kg once a week.
• Used when Hb levels fall below 10g/dl.
CHEMOTHERAPY INDUCED ANAEMIA
• Erythropoiesis stimulating protein, darbepoetin alfa.
• Genetically modified erythropoietin.
• 4 mutated amino acids with additional carbohydrates side chains prolongs the circulatory survival of the drug to 24-26 h.
CHEMOTHERAPY INDUCED NEUTROPENIA
•Myeloid growth factors.
•Glycoproteins.
• Stimulate proliferation and differentiation of one or
more myeloid cell lines.
• Enhance the function of mature granulocytes and
monocytes.

• Recombinant forms are:• Granulocyte Colony Stimulating Factor (G-CSF)
• Granulocyte Macrophage Colony Stimulating Factor (GM-CSF)

• Recombinant human G-CSF- Filgrastim• Produced in a bacterial expression.
• Non glycosylated peptide of 175 amino acids.
• Molecular weight 18kDa.
• Pegfilgrastim-
• Covalent conjugation product of filgrastim and a form of
polyethylene glycol.
• Lenograstim-
• Glycosylated form of recombinant G-CSF.
• Recombinant human GM-CSF- Sargramostim
• Produced in a yeast expression.
• Partially glycosylated peptide of 127 amino acids.
• 3 molecular species with molecular weights of 15,500; 15,800;
19,500.
• These preparations have serum half-lives of 2-7 hours.
• May be administered Intravenously or subcutaneously.
CHEMOTHERAPY INDUCED NEUTROPENIA
• Accelerates rate of neutrophil recovery after dose intensive myelosuppressive chemotherapy.
• Reduces the duration of neutropenia
• Raises the nadir count following a cycle of chemotherapy.

Clinical guidelines for the use of G-CSF after cytotoxic chemotherapy recommend reserving G-CSF for :
• Patients at high risk for febrile neutropenia based on age, medical history, and disease characteristics.
• Patients receiving dose-intensive chemotherapy regimens that carry a greater than 40% risk of causing febrile neutropenia.

• Patients with a prior episode of febrile neutropenia after cytotoxic chemotherapy.
• Patients at high risk for febrile neutropenia.
• Patients who are unlikely to survive an episode of febrile neutropenia.
• Doses:• G-CSF: 5mcg/kg/d
• GM-CSF: 250mcg/m2/d
• Started within 24-72 hours after completing chemotherapy.
• Completed until absolute neutrophil count is greater than 10,000cells/µl
• Pegfilgrastim is given as a single dose of 6mg.

CHEMOTHERAPY INDUCED THROMBOCYTOPENIA
• Thrombopoietic growth factors- Interleukin 11; Thrombopoietin.
• Interleukin 11-• Cytokine; Stimulates hematopoiesis, intestinal epithelial cell
growth, osteoclastogenesis; inhibits adipogenesis.
• Enhances megakaryocyte maturation invitro.
CHEMOTHERAPY INDUCED THROMBOCYTOPENIA
• Recombinant human IL-11: Oprelvekin.• Thrombopoietic response in 5-9 days.
• 25-50 µg/kg per day subcutaneously.
• Used in patients undergoing chemotherapy for nonmyeloid malignancy with severe thrombocytopenia (platelet count <20,000/µl)
• Administered till platelet count >1,00,000 µl.

CHEMOTHERAPY INDUCED ALOPECIA
• Incidence- 65%
•Most traumatic factor in cancer patient care.
• Negative impact on individual perceptions of appearance, body image, sexuality and self esteem.
DRUGS CAUSING ALOPECIA
• Taxanes; Antimicrotubule inhibitors- >80%
• Topoisomerase inhibitors; Anthracyclines- 60-100%
• Alkylating agents- >60%
• Antimetabolites- 10-50%
• Higher incidence in combination therapy than monotherapy.

CHEMOTHERAPY INDUCED ALOPECIA
• Dystrophic anagen effluvium.
• In anagen proliferation of epithelial cells greatest activity in matrix cells of hair bulb building up hair shaft.
• Chemotherapy abrupt cessation of mitotic activity weakening of partially keratinized proximal portion of hair shaft narrowing and breakage.

CHEMOTHERAPY INDUCED ALOPECIA
• Begins 1-3 weeks after initiation.
• Scalp- common location
• Hair of beard, eyebrows, eyelashes, axillary and pubic region may be affected.
• Hair loss is reversible. Occurs after 3-6 months.
• Permanent alopecia- Rx with busulfan and cyclophosphamide.
TREATMENT- PHYSICAL PREVENTION
• SCALP TORNIQUES• Application of bands around head occludes superficial blood
flow to scalp reduces amount of drug delivered to hair follicles.
• Pressure- 10mmHg more than SBP to 300 mmHg.
• 5-10 min before or at the time of chemotherapy upto 30 min later.

TREATMENT- PHYSICAL PREVENTION
• SCALP COOLING• Application of cold to scalp using cap (pre-cooled or
exchanges coolant with reservoir)
• 5 min before treatment till an hour later.
• Vasoconstriction reduces blood flow to scalp reduces amount of drug available for hair follicle.

• Practically ineffective if drug administered as continuous infusion for long time.
• Increases risk of scalp metastasis.
• Hence contraindicated in hematological malignancies and cutaneous T cell lymphoma.
TREATMENT- PHARMACOLOGICAL
PREVENTION•Minoxidil- a vasodilator• Prolongs duration of anagen phase.
• Fails to induce significant regrowth of hair in permanent alopecia caused by busulfan and cyclophosphamide.
TREATMENT- PHARMACOLOGICAL
PREVENTION• Cyclosporine A• Immunosuppressive immunophilin ligand.
• Use in alopecia side effect of excess hair growth
• Induces anagen and inhibits catagen of hair cycle promotion of hair growth.
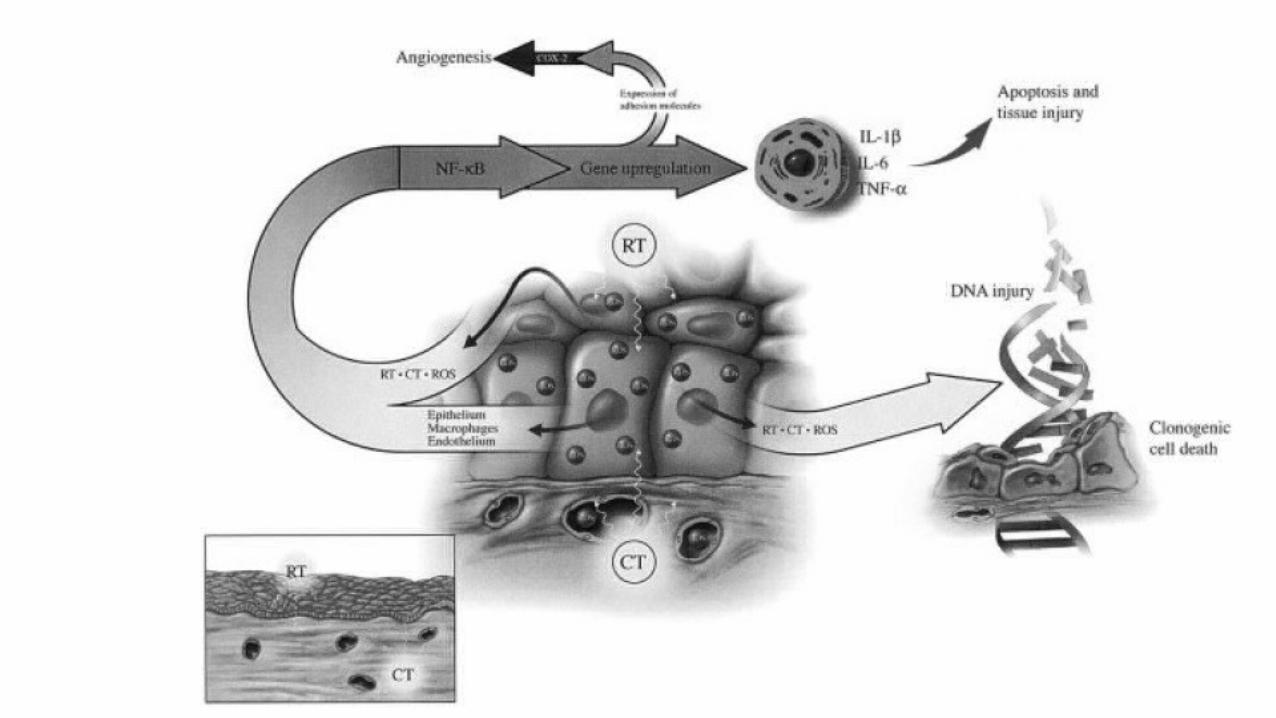
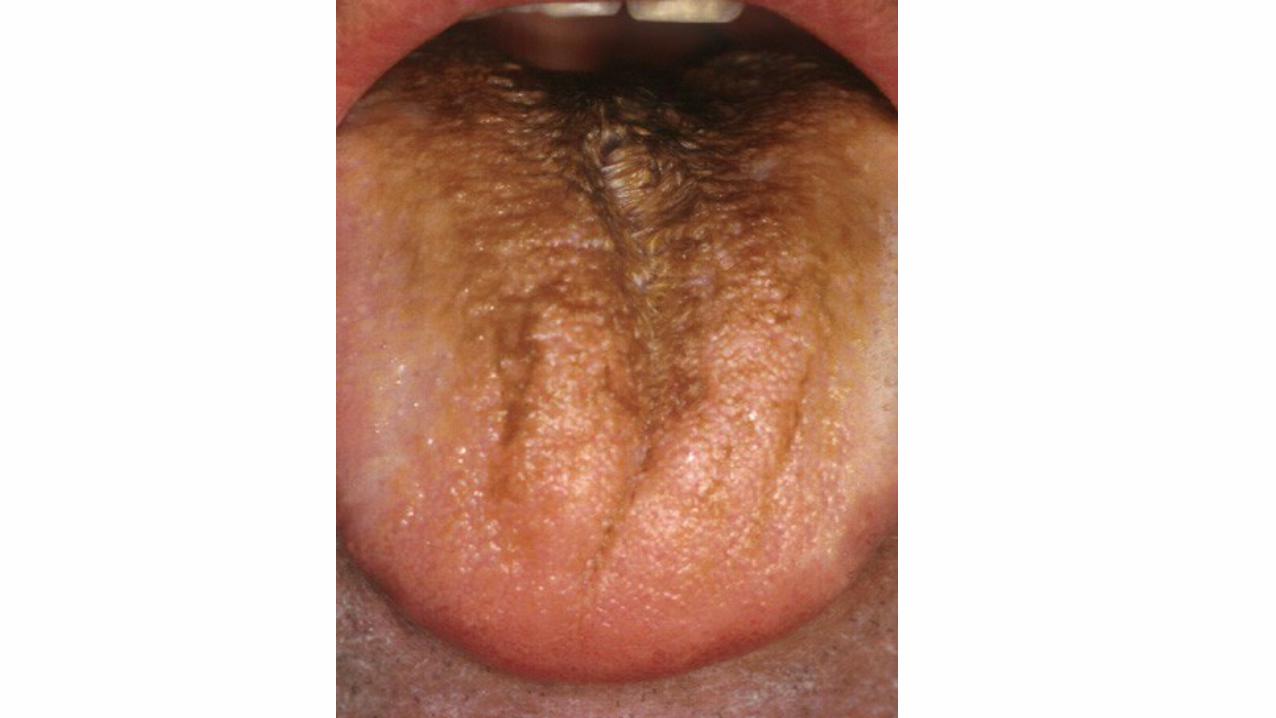
MUCOSITIS• Threatens effectiveness of therapy dose reduction;
increases health care cost; impairs patients quality of life.
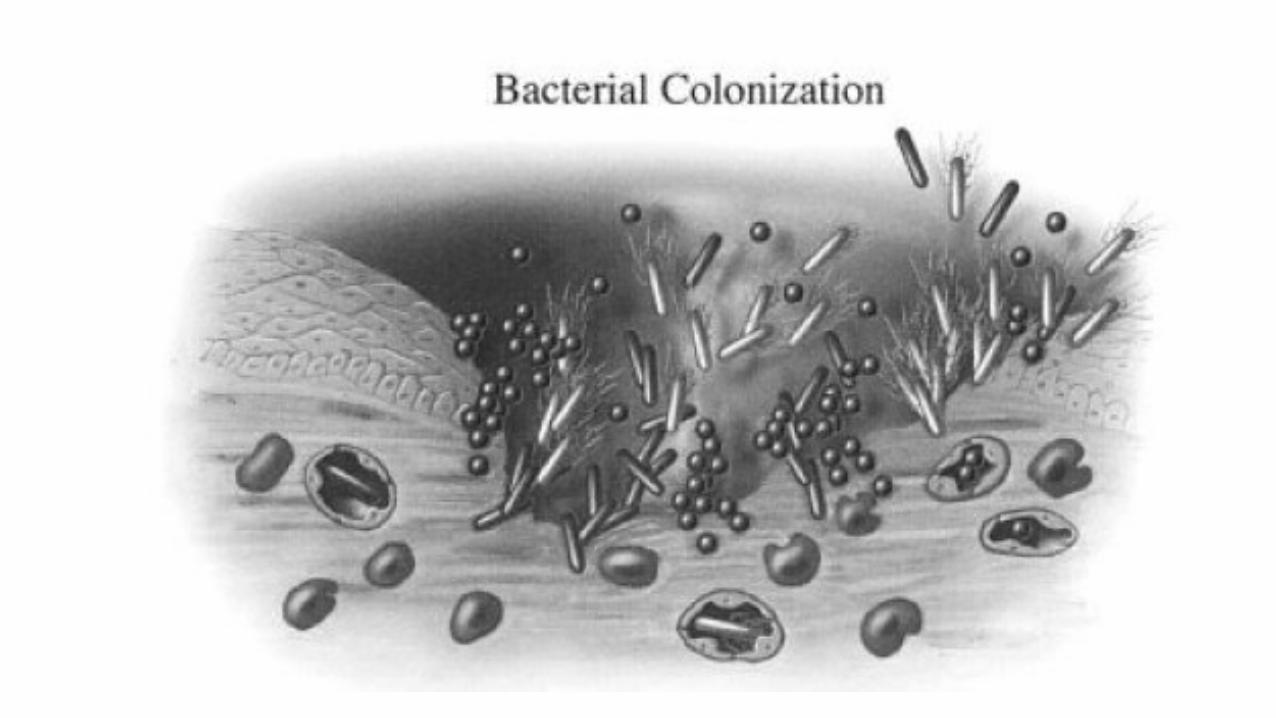
• Oral mucositis- a frequent complication of cytoreductive cancer chemotherapy.
• Associated with pain; in neutropenic pts with cancer risk factor for sepsis.
• Gastrointestinal mucositis injury of rest of alimentary tract.
•Most prominent in small intestine.
• Followed by esophagus, stomach, large intestine.


MANAGEMENT OF ORAL MUCOSITIS
• Oral decontamination- antifungal and antibacterial rinses.
• Topical and systemic pain management-• Topical- 2% lidocaine; morphine solution.
• Frequent rinsing with NaCl mucosa moist; decreases caking of secretions; soothes inflamed or ulcerated mucosa.

MANAGEMENT OF ORAL MUCOSITIS
• Cryotherapy with ice chips.
• Palifermin- Keratinocyte Growth Factor.• 60 µg/kg/day for 3 days before and after chemotherapy.
• Control of bleeding:• Topical thrombin packs.• Topical antifibrinolytic agents- tranexamic acid.
CHEMOTHERAPY AND TERATOGENICITY



THANK YOU

REFERENCES• Goodman and Gillman Manual of Pharmacology and therapeutics.• Katzung- Basic and clinical pharmacology- 12th edition• Medscape• Luanpitpong S, Rojanasakul Y. Chemotherapy induced Alopecia. Available from:
http://intechopen.com• Sonis S, Elting L, Keefe D, Peterson D, Schubert M, Hauer-Jensen M et al.
Perspectives on cancer therapy-induced mucosal injury. Cancer. 2004;100(S9):1995-2025. • 3. Naidu M, Ramana G, Rani P, Mohan l, Suman A, Roy P. Chemotherapy-Induced
and/or Radiation Therapy-Induced Oral Mucositis-Complicating the Treatment of Cancer. Neoplasia. 2004;6(5):423-431.