Management Esophageal Foreign Body
10
Case Report Management Esophageal Foreign Body Haryanto Rahardjo*, Ari F Syam**, Marcel Simadibrata K** *Department of Internal Medicine , Panti Rapih Hospital, Yogyakarta ** Division of Gastroenterology, Departement of Internal Medicine, Faculty of Medicine University of Indonesia/Dr.Cipto Mangunkusumo General National Hospital Abstract Foreign body ingestion is a common clinical problem, objects such as coin, safety pin, bolus meat, bone, denture etc. They lodged in certain part of esophagus with clinical features was asymptomatic or symptoms from esophagus or respiratory tract. The plain radiography is indicated for every patients with known or suspected foreign body either radiopaque or non radiopaque. A variety of methods can be used to remove an esophageal foreign bodies; the chosen strategy depends on the type and location of foreign body such as: endoscopy, observation, rigid esophagoscopy, Foley catheter extraction, bougienage, sometimes used LES relaxant or surgery. Five cases have presented with different strategy, 2 cases success due to endoscopy, 1 case with observation, 1 case to push the object into the stomach by the endoscope, 1 case failed with Foley catheter but success with rigid esophagoscopy by ENT Dept., all of the cases without complications. Keywords : esophageal foreign body, foreign body ingestion, procedure removal Introduction In the United States, thousands of children per year have a foreign body in the esophagus and 1500 people die yearly of 1
-
Upload
haryantoay -
Category
Documents
-
view
133 -
download
0
description
Case Reports
Transcript of Management Esophageal Foreign Body

Case Report
Management Esophageal Foreign Body
Haryanto Rahardjo*, Ari F Syam**, Marcel Simadibrata K**
*Department of Internal Medicine , Panti Rapih Hospital, Yogyakarta
** Division of Gastroenterology, Departement of Internal Medicine, Faculty of Medicine University of Indonesia/Dr.Cipto Mangunkusumo General National Hospital
Abstract
Foreign body ingestion is a common clinical problem, objects such as coin, safety pin, bolus meat, bone, denture etc. They lodged in certain part of esophagus with clinical features was asymptomatic or symptoms from esophagus or respiratory tract. The plain radiography is indicated for every patients with known or suspected foreign body either radiopaque or non radiopaque. A variety of methods can be used to remove an esophageal foreign bodies; the chosen strategy depends on the type and location of foreign body such as: endoscopy, observation, rigid esophagoscopy, Foley catheter extraction, bougienage, sometimes used LES relaxant or surgery. Five cases have presented with different strategy, 2 cases success due to endoscopy, 1 case with observation, 1 case to push the object into the stomach by the endoscope, 1 case failed with Foley catheter but success with rigid esophagoscopy by ENT Dept., all of the cases without complications.
Keywords : esophageal foreign body, foreign body ingestion, procedure removal
Introduction
In the United States, thousands of children per year have a foreign body in the esophagus and 1500 people die yearly of ingested foreign body of upper gastrointestinal (1, 2).Most esophageal foreign bodies are radiopaque, frequently ingested items include small metal, plastic toys, coin, button batteries, fish bones, safety pin, thumbtacks, needles, wire, wood or glass objects, denture, bolus meat, razor blade (3,4,5). The most common locations of foreign body lodgment are the 3 areas of normal physiologic esophageal narrowing. The first and most common location is the proximal esophagus at the level of the junction between the neck and thorax, the second location is the mid esophagus at the level of carina and aortic arch, the third location is the distal esophagus, slightly proximal to gastroesophageal junction (6,7) The presenting symptoms varied with 20% of patients asymptomatic (4,5). Preferred examination begins with the radiographic evaluation. Current strategies for the removal of retained foreign bodies include endoscopy, observation (which allows the foreign body to pass into the stomach on its own), rigid esophagoscopy, Foley catheter extraction, bougienage, lower esophagus sphincter (LES) relaxant, or surgery (2,7) Button batteries do not usually cause problems unless they become lodged in the gastrointestinal, the esophageal damage can occur in an relative short period of time when disk battery is lodged in the esophagus.(2,4). This series case report of a boy 8th years old with ingestion a nail, a man 52nd years old accidentally swallowed a safety pin, a young man
1

30 years old with history of swallowed a denture during sleep, a female 53rd years old swallowed an onion and lodged, an old man 71st with bolus meat lodgment.
Case report
Case 1 (No.MR 405752)
Boy 8 years old was suffering from heart burn, dysphagia and epigastric pain after swallowed a nail around 2 inch. The physical examination was normal; in the plain chest x-ray revealed a radiopaque look like a nail in slight upper diaphragm with vertical position and the part of sharp goes inside stomach. The endoscopy was performed and didn’t find a nail, but almost the entire stomach mucosal until the second part of duodenum revealed severe erosive without bleeding. Repeated the plain x-ray revealed the nail goes down into the intestine, a week later the nail find in patient’s stool
Case 2 (No.MR 180951)
Man 52 years old, was admitted to the emergency room with a history of dysphagia and sore of throat also heart burn after he was accidentally swallowed a safety pin due to scrape the dental several hours before reached the hospital. The physical exam was normal, the plain chest x-ray anteroposterior and lateral revealed a safety pin with open position, and sharp point was facing up (Fig1).
Fig 1 Open Safety Pin
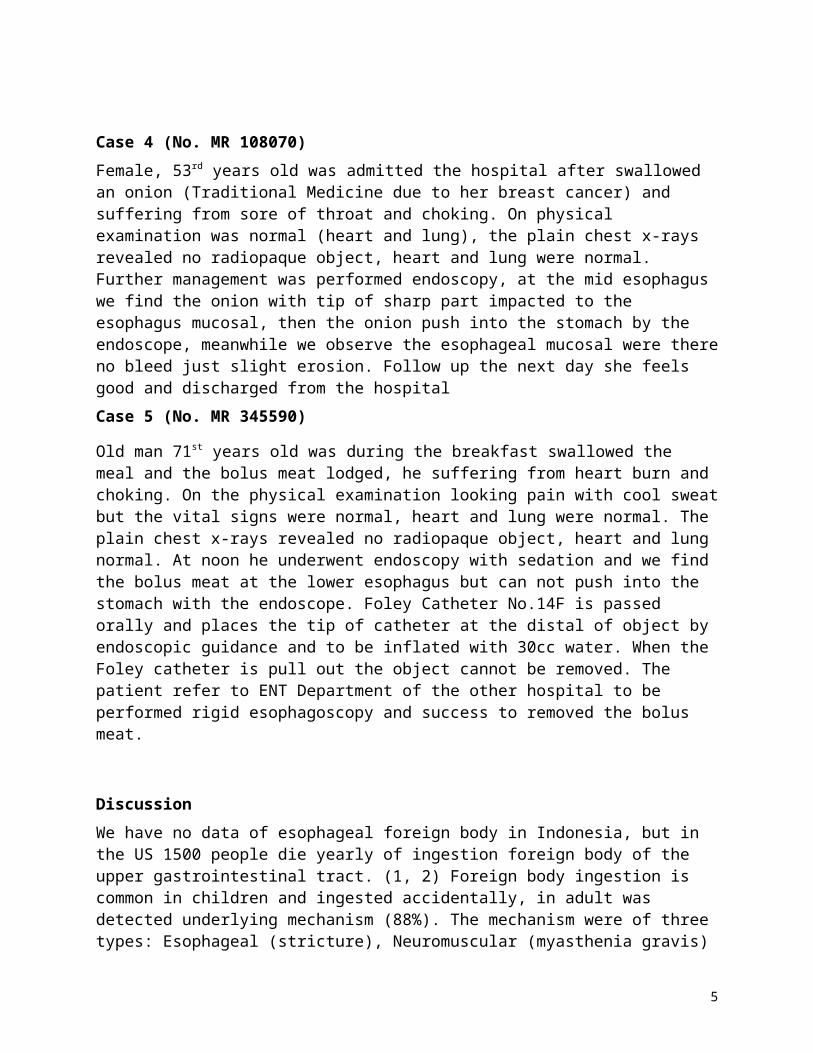
The endoscopy find the object in 25cm from teeth and grasp the sharp part of open safety pin by forceps biopsy and slowly pull together with the endoscope meanwhile looking for any impaction or bleed, the object success to extraction without complications (Fig2)
2
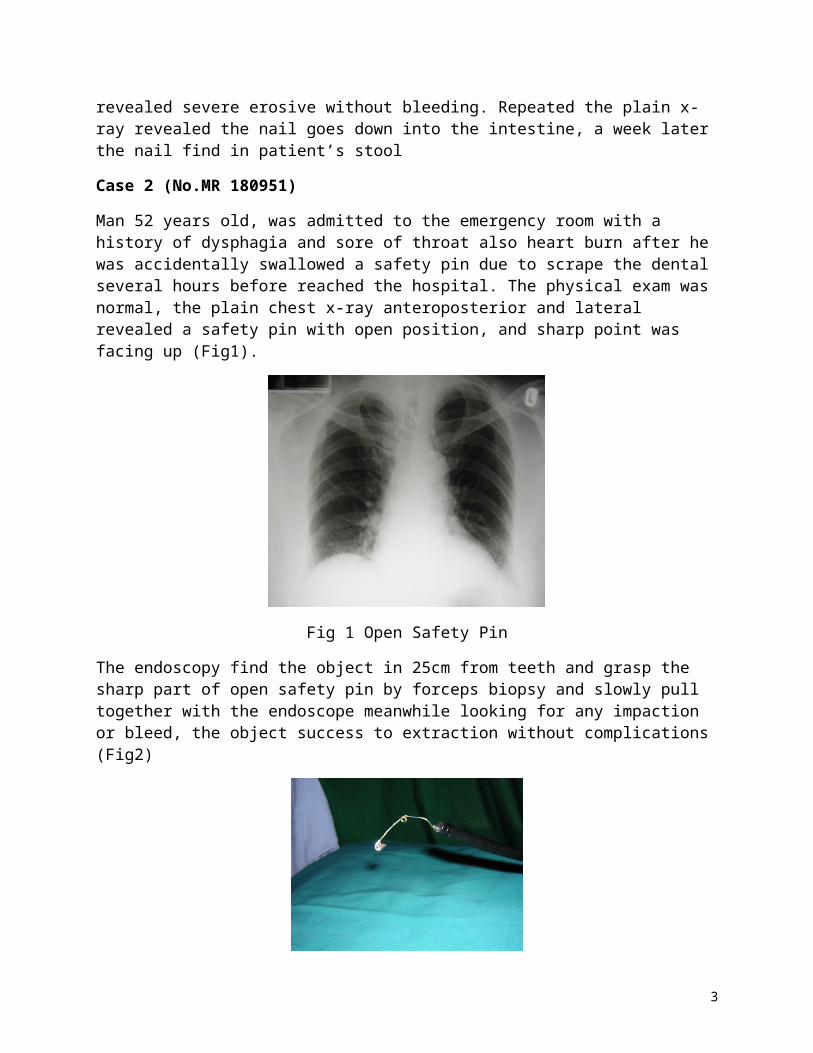
Fig2. The Object (Safety Pin)
Case 3 (No.MR 416492)
Man 30 years old, with history of swallowed a denture during sleep and suffering from odinophagia. He went to the hospital in hours; on clinical examination the patient had no problems. The plain chest x-ray revealed the radiopaque object (Fig3), the endoscopy was performed and revealed a denture in the endoscope 25cm from teeth, when we try to pull with forceps biopsy through the endoscope feel the obstacle then the denture push into the stomach with the endoscope. Inside the stomach forceps biopsy was direction to the wire part of the denture and we try again to pull the whole denture with the endoscope, the object was success pull by extraction (Fig.4)
Fig3. The Object of radiopaque
Fig4. The Denture
3

Case 4 (No. MR 108070)
Female, 53rd years old was admitted the hospital after swallowed an onion (Traditional Medicine due to her breast cancer) and suffering from sore of throat and choking. On physical examination was normal (heart and lung), the plain chest x-rays revealed no radiopaque object, heart and lung were normal. Further management was performed endoscopy, at the mid esophagus we find the onion with tip of sharp part impacted to the esophagus mucosal, then the onion push into the stomach by the endoscope, meanwhile we observe the esophageal mucosal were there no bleed just slight erosion. Follow up the next day she feels good and discharged from the hospital
Case 5 (No. MR 345590)
Old man 71st years old was during the breakfast swallowed the meal and the bolus meat lodged, he suffering from heart burn and choking. On the physical examination looking pain with cool sweat but the vital signs were normal, heart and lung were normal. The plain chest x-rays revealed no radiopaque object, heart and lung normal. At noon he underwent endoscopy with sedation and we find the bolus meat at the lower esophagus but can not push into the stomach with the endoscope. Foley Catheter No.14F is passed orally and places the tip of catheter at the distal of object by endoscopic guidance and to be inflated with 30cc water. When the Foley catheter is pull out the object cannot be removed. The patient refer to ENT Department of the other hospital to be performed rigid esophagoscopy and success to removed the bolus meat.
Discussion
We have no data of esophageal foreign body in Indonesia, but in the US 1500 people die yearly of ingestion foreign body of the upper gastrointestinal tract. (1, 2) Foreign body ingestion is common in children and ingested accidentally, in adult was detected underlying mechanism (88%). The mechanism were of three types: Esophageal (stricture), Neuromuscular (myasthenia gravis) and Extrinsic and Mechanical (ankylosing spondylitis) (3) Most esophageal foreign bodies are radiopaque, frequently ingested items include small metal, plastic toys, coin, buttons, fish bones, batteries, safety pin, thumbtacks, needles, wire, wood or glass objects, denture, bolus meat, razor blade (3, 4, 5) Button batteries lodged in the esophagus represent emergency and should be removed without delay. Esophageal damage can occur in relatively short period of time, liquefaction necrosis may occur because by direct corrosive action, low voltage burns, and pressure necrosis. (2, 4)
The most common locations of foreign body lodgment are the 3 areas of normal physiologic esophageal narrowing. The first and most common location is the proximal esophagus at the level of the junction between the neck and thorax, the second location is the mid esophagus at the level of carina and aortic arch, the third location is the distal esophagus, slightly proximal to gastroesophageal junction ( 6, 7). In our series all cases presenting with the same these location.
The presenting symptoms varied, with 20% of patients asymptomatic. Dysphagia and odinophagia are the usual symptoms of foreign body impaction in the esophagus, associated respiratory symptoms such as coughing, choking and stidor. (2, 4, 6,)
4
Complications were more frequently in adults, mainly owing to the underlying condition; the others complication such as abrasions, lacerations, and punctures, with associated abscesses, perforation and soft tissue infections, pneumothorax, peritonitis, cardiac tamponade (2,3,4)
Early recognition and treatment of esophageal foreign bodies is important because the complications are serious and can be life-threatening. Radiology plays an important role in the initial diagnosis, in recognition of complications, and treatment. Chest radiography may detect a radiopaque object or suggest soft tissue swelling with a radiolucent foreign body, upper endoscopy usually provides the diagnosis. The goal standard of diagnosis is rigid or flexible oesophagoscopy as it allows visualization and retrieval of the foreign body (2, 4, 7)
Over 80% of ingested foreign bodies pass through the gastrointestinal tract without incident. Sharp (bones, pins, needles, wire) or long (greater than 6.5cm) foreign bodies are most commonly impacted in perforation. Foreign bodies less than 2.5cm in diameter usually pass through gastrointestinal tract without difficulty. Once a foreign body has reached the stomach, it has an 80-90% change of passage. Objects longer than 6 cm may become entrapped by either the pylorus of the duodenal sweep, and objects larger than 2 cm in diameter also may fail to pass the pylorus. When a foreign body has reached the small bowel the only structural impediment to passage is the ileocecal valve. (4, 6, 8) In our series Case 1 and Case 4 the objects reached into the stomach, the nail of Case 1 passed the pylorus then observation was suitable for him; a week later the nail find in the patient’s stool and Case 4 after the onion push with the endoscope into the stomach she has no problem.
Observation for up to 24 hours is probably safe, and the proper method of therapy must be carefully selected according to the age of patient, the type of the impacted foreign body, the location of impaction, the duration of impaction, and available medical resources and skills (9)A variety of method can be used to remove an esophageal foreign body. The chosen strategy depends on the type and location of foreign body, the length of time it has been in the esophagus, and the relative degree of experience with different techniques at given facility. The success rate for the removal of foreign bodies from the esophagus is 95-100% regardless of the technique used. Current strategies for removal of retained foreign bodies include endoscopy; observation, which allows the foreign body to pass into the stomach on its own; rigid or flexible esophagoscopy; balloon catheter extraction with radiographic guidance; and bougienage technique to push the foreign body into the stomach, the last technique is appropriate only when the object is lodged in the distal portion of the esophagus and smooth object and surgery. An overtube should be use to prevent tracheal aspiration. (2, 7) Foreign bodies lodged at the LES can be managed by relaxation of the LES. The most often used medication is glucagons, a smooth muscle relaxant that significantly reduces lower esophageal sphincter pressure with doses as low as 0.25 mg. Glucagon has reported successes of 12% to 58% in treating esophageal food impactions. Glucagon does not work with a fixed obstruction present, which is often found with esophageal foreign bodies and food impactions. Finally, glucagons may help when used with endoscopy by lowering lower esophageal sphincter pressure and facilitating the endoscope pushing a food impaction into the stomach. Nitrate such as sublingual nitroglycerin and nifedipine have been used less widely because a risk of hypotension and does not work in patients with structural abnormalities (2, 7) Success rate for rigid esophagoscopy (100%) and
5
flexible endoscopy (76-98.5%). Overall rigid esophagoscopy had higher complication rate than flexible endoscopy (10% versus 5.1%). Endoscopic removal of foreign bodies in the upper gastrointestinal tract is an effective and safe procedure. The Foley catheter technique is suited only for proximally located blunt object, and its routine use is not recommended, success rate 87%. (10, 11, 12)Meat impaction resulting obstructed esophagus is an urgent problem and the bolus should be removed within hours (8). In our series Case 5 when failed extraction either endoscopies or Foley catheter, he refer to Department of ENT of the others hospital to be performed rigid esophagoscopy and success removed the bolus meat.Sharp object can also be removed safely by endoscopic technique avoiding open surgical method, there are different techniques described for removal of open safety pin with pointed edge facing up, like rotating it in the stomach, engaging pointed edge into endoscope and the withdrawing it. (2) In our series Case 2, success removed by forceps biopsy endoscopic with grasp the sharp part of the safety pin and pull extraction carefully all of the forceps biopsy, the endoscope and the object, but in Case 3 the denture must push into the stomach with the endoscope and forceps biopsy grasps the wire part of the denture then extraction, meanwhile observe for any impaction or bleed. In our series, all of the cases without complications and discharged from the hospital the next day after removal the object.
References
1. Webb WA. Management of foreign bodies of the upper gastrointestinal tract. Gastroenterology 1988;94(1):204-16
2. Pfau P. IngestedForeign Objects and Food Bolus Impactions. In: Guisberg GG, et al. Clinical Gastrointestinal Endoscopy. Elsevier Saunders 2005.p.291-303
3. Baraka A, Bhikazi G. Oesophageal foreign bodies.BMJ 1975;1:561-563.
4. Macpherson RI, et al. Esophageal foreign bodies in children: diagnosis, treatment, and complications. AJR Am J Roentgenol. 1996;166:919-924.
5. Sanowski RA, et al. Foreign body extraction. In: Sivak, Gastroenterologic Endoscopy. 2nd
Eds. WB Saunders Company Philadelphia 2000. p.801-812
6. Shivakumar AM,Naik AS, Prashanth KB. Yogesh BS, Hongal GF. Foreign body in upper digestive tract. Indian J Pediatr 2004;71:689-693.
7. Bozymski EM, Isaacs KL. Miscellaneous Diseases of the Esophagus. In: Yamada T, et al. Textbook of Gastroenterology Vol.One. 2nd Eds. JB Lippincott Company Philadelphia, 1995.p.1283-1302
8. Webb WA. Management of foreign bodies of the upper gastrointestinal tract: update Gastrointest Endosc.1995;41:39-51.
6

9. Chaikhouni A, Kratz JM, Crawford FA. Foreign bodies of the esophagus. Am Surg 1985;51:173-179.
10. Taylor RB. Esophageal foreign bodies. Emerg Med Clin North Am.1987;5:301-311.
11. Faigel DO. Miscellaneus Diseases of The Esophagus: Systemic and Dermatologic Disease, Foreign Bodies, Physical Injury. In: Yamada T,et al. Atlas of Gastroenterology. 3rd Eds. Lipincott Williams & Wilkins 2003.p.209-217
12. Berggreen PJ, et al. Techniques and complications of esophageal foreign body extraction in children and adults. Gastrointest Endosc. 1993;39:626-630
7