
Man Ali
93
-
Upload
nakshatra1714 -
Category
Documents
-
view
217 -
download
0
Transcript of Man Ali

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 1/93

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 2/93
IMMUNOLOGICALDISEASES OF THE
ORAL CAVITYBY MISS MANALI NAGAONKAR
3RD
BDS
2

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 3/93
RECURRENT APTHOUS STOMATITIS
• RECURRENT APTHOUS MAJOR
• RECURRENT APTHOUS MINOR
•
RECURRENT APTHOUS HERPITIFORM
3

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 4/93
ETIOLOGY
• BACTERIAL INFECTION
• IMMUNOLOGICAL ABNORMALITIES
• IRON VIT B 12 DEFICIENCY ….FOLIC ACID
DEFICIENCY• ENDOCRINE
• TRAUMA
•PRECIPITATING FACTORS
• PSYCHIC FACTORS
• ALLERGIC FACTORS
4
8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 5/93
RECURRENT APTHOUS MINOR
(CANKER SORES)• MORE IN WOMEN
• BTWEEN 10 TO 30 YRS OF AGE SINGLE OR MULTIPLESOLITARY ,COVERED BY GREY MEMBRANE,NECROTICCENTRE ,ERYTHEMATOUS HALO
•
VERY PAINFUL,DIFFICULTY IN SPEECH AND EATING• 2 TO 3 MM IN DIAMETER MANIFESTATIONS …..BURNING
SENSATION ,PARASTHESIA ,MALAISE,EDEMA ,VESICLE LIKELESIONS CONTAINING MUCUS
• SITES …..BUCCAL AND LABIAL MUCOSA ,BUCCAL AND
LINGUAL SULCI ,SOFT PALATE ,PHARYNX• PERSISTS FOR 7 TO 14 DAYS
• NO EVIDENCE OF SCARRING
5

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 6/93
6

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 7/93
7

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 8/93
8

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 9/93
RECURRENT APTHOUS MAJOR
• LARGE,PAINFUL,1 TO 10 N NO ,MORE SEEN IN HIV
• SITE- LIPS ,CHEEK ,TONGUE,SOFT PALATE
• DYSPHAGIA AND PAIN
• 1 CM IN DIAMETER ,PERSISTS FOR UPTO 6 WEEKS
,LEAVE A SCRA UPON HEALING
• FEMALES MORE AFFECTED
• SEVERE FORM…..PENIS,VAGINA,RECTUM,LARYNX
,RHEUMATOID ARTHRITIS ,CONJUCTIVITIS
9

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 10/93
10

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 11/93
11

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 12/93
12

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 13/93
RECURRENT APTHOUS HERPITIFORM
• CROPS OF MULTIPLE,SMALL ,SHALLOW ULCERS ,UPTO 100IN NO
• SITE ….IN THE ORAL CAVITY
• LESIONS ON THE INTRA ORAL MUCOSAL SURFACE
• AS SMALL PIN HEAD EROSIONS THAT ENLARGE• MORE PAINFUL
• PRESENT CONTINOUSLY FOR ONE TO THREE YRS
• TEMPORARY RELIEF WITH 2% TETRACYCLINE MOUTHWASH
•
NON KERATINISED MOVABLE AREAS ARE MOSTLY• AFFECTED
• SIMILAR TO HSV INFECTION
13

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 14/93
HISTOLOGIC FEATURES
• MINOR APTHOUS SHOWS FIBRINOPURULENT
MEMBRANE
• INTENSE INFLAMMATION,LYMPHOCYTES ON
….PMNS ,LYMPHOCYTES ,EPITHELIAL
PROLIFERATION ,GRANULATION TISSUE
• TISSUE INVOLVEMENT GENERALLY
SUPERFICIAL
14

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 15/93
15
NON-SPECIFIC MICRSCOPIC PICTURE
• Early – central zone of ulceration covered byfibrinoprulent memberane
• Connective tissue – increased vascularity andmixed inflammatory cellular infiltrate
• Marginal epthelium – spongiosis and
numerous mononuclear cells• Presence of band of lymphocytes intermixed
with histocyte in superficial connective tissue.

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 16/93
DIFFERENTIAL DIAGNOSIS
16
• No defINitive lab. Diagnosis, depends on theclinical presentation
• Lesions can be mistaken for recurrent
aphthous stomatitis include herpecticstomatitis, herpangina, erythema multiforme,
erosive lichen planus, pemphigus and
pemphigoid.

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 17/93
TREATMENT AND PROGNOSIS
17
Immune enhancement
• Levimisole
• Vaccine
Immunosupression, inflammatory suppression
• Prednisone• Triamcicinolo acetonide
• Betamithasone-17-benzoate
• Antihistamine
Antibiotics• Suspension ,topical
• Chloramphenicol.
• Broad-spectrum antibiotics.

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 18/93
18
Diet supplementation.
• Vitamin B12,folic acid .
• Iron.
• Zinc sulfate.
Symptomatic treatment .
• Xylocaine/lidocaine.
• Silver nitrate .
• Benadryl ,topical.
• Camphor – phenol .

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 19/93
BEHCTES SYNDROME
19
• Disease of uncertain etiology .
• May resemble infectious diseases.
• National institute of health in 1977- humoral
antibodies and cell mediated immune responsesmay act either jointly or independently upon oralepithelium .
• Recurrent aphthous ulcer and Behcet ‘s syndromecan not be distinguished by antibodies and cellmediated immune responses .
• HLA MARKERS DIFFERENTIATE
8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 20/93
CLINICAL FEATURES
20
• More common in young adults (25 to 40 yrs).
• 5 to 10 times more common in males .
• Characterized by oral , genital ulcerations and ocular , skin lesions .
• First manifestation – appearance of oral and genital lesions witherythematous border .
• Genital ulcers are small located on scrotum, root of the penis ,orlabia majora .
• Ocular lesions – photophobia ,irritation , simple conjunctivitisuveitis
• Skin lesionssmall puspules or macules , erythema nodosum and
erythema multiform.• DISTINGUISHING FACTORS – CLASSIC TRIAD OF THE DISEASE
PRESENT

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 21/93

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 22/93
22

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 23/93
A common case of HLA B 27 UVEITIS
23
8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 24/93
Histologic features :
• Nonspecific remarkably similar to recurrentaphthous ulcer .
• Endothelial proliferation .
• Vasculitis .Laboratory findings .
• Hypergyamaglobulinemia .
•
Mucocytrosis• Eosinophilia .
• Elevated ESR .

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 25/93
TREATMENT AND PROGNOSIS
SYMPTOMATIC OR SUPPORTIVE MEASURES
25

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 26/93
REITERS SYNDROME
• TYPICAL TETRAD ….NON ONOCCAL URETHRITIS,ARTHRITISCONJUNCTIVITIS,MUCOCUTANEOUSLESIONS
•
MALE TO FEMALE RATIO ….9 : 1• URETHRITIS IS THE FIRST SIGN
• ARTHRITIS …BILATERAL POLYARTICULAR
• SKIN LESIONS – RED OR YELLOW KERATOTICMACULES OR PAPULES WHICH DESQUAMATE
• HLA B 27 IS THE FACTOR PRESENT ,SEEN IN HIV
26

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 27/93
SITES ….
27

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 28/93
28

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 29/93
ORAL MANIFESTATIONS
29
• Painless ,red,slightly elevated areas
,sometimes granular or even vesicular with
white circinate border on buccal mucosa ,lips
and gingiva .(pindborg etal)
• Palatal lesions – small bright red purpuric spot
which darken and coalesce .
• Geographic tongue appearance
• Circinate balanitis

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 30/93
GEOGRAPHIC TONGUE
30

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 31/93
Histologic features.
• No diagnostic findings .
• Parakeratosis ,acanthosis and
polymorphonuclear leukocyte infiltration of
epithelium .
• Microabscess formation .
• Connective tissue – lymphocyte and plasma
cell infiltrate .

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 32/93
Sarcoidosis (boeck’s sarcoid ,besnier-
boeck-schaumann disease)• Multi system granulomatious disease of unknown origin
characterized by the formation of uniform discrete compactnoncaseating epitheloid granulomas ,black>white .
• Etiology – infective and non infective .
•
Most favored infective (mycobacterium and propionibacterium).
• Associated with tuberculosis .(Gupta D et al)
• Most common in lungs ,skin , lymph nodes ,salivaryglands,spleen and bones.
DEPRESSION OF DELAYED TYPE HYPERSENSITIVITY,IMPAIREDCELL MEDIATED IMMUNITY ,INCREASE OR ABNORMALSERUM IMMUNOGLOBULINS ,LYMPHOPROLIFERATION
8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 33/93
Clinical features .
SITES …LUNGS,SKIN,LYMPH NODES,SALIVARY
GLANDS ,SPLEEN AND BONE
• Commonly seen in young and middle age.
• Mild malasise and cough – chief features .• Cutaneous lesions – 25 to 35 %.
• Multiple red patches that occur in group growslowly and do not tend to ulcerate .
• Hepatomegaly and splenomegaly .
• ERYTHEMA NODOSUM

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 34/93
34

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 35/93
MULTIPLE RED PATCHES
35

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 36/93
Oral manifestation .
• Sarcoid granulomas – labial glands – 58%.
• Lesions on lip – small papular nodules or
plaques resemble fever blisters .
• Palate and buccul mucosa- bleblike ,
containing clear yellowish fluid OR SOLID
NODULES

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 37/93
37

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 38/93
Histologic features .
• No acid fast organisms can be demonstrated .
• Nest of epithelioid cells with multinucleated
giant
• cells-chief feature .
• Also contains T and B cells, various
immunoglobulins .
• Caseation and necrosisn do not occour .

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 39/93
39

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 40/93
Uveoparotid fever .
• Form of sarcoidosis .• Firm painless usually bilateral .Enlargement of parotid gland
• Inflammation of uveal tracts of the eye , cranial nerve involvement,submandibular sublingual and lacrimal gland involvement .
• Often presence of chronic low grade fever .
• Symptoms :• Lassitude
• Malaise
• Vague GI disturbances , nausea , vomiting .
• Xerostomia
• Patchy erythema on skin.

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 41/93
• Enlargement of cervical lymph nodes .
• Lesions – uveoparotitis,conjunctivitis,uveitis , keratitis ,CORNEAL HERPES
• Signs and symptoms disappears in time
while parotid swelling and visualdisturbance may persist
• SEVENTH NERVE PARALYSIS .

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 42/93
MIDLINE LETHAL GRANULOMA
• IDIOPATHIC PROGRESSIVE DESTRUCTION OF THENOSE ,PARANASAL SINUS ,PALATE ,FACE ANDPHARYNX
• DYSFUNCTION OF IMMUNE MECHANISM
…..GRANULOMA FORMATION • AFFECTED PERSON LACKS RESISTANT TO THE
PROGRESS OF THE DISEASE
• ASSOCIATD WITH NEOPLASTIC ANDINFLAMMATORY DISEASE
• MOST UNUSUAL CONDITION
42

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 43/93
CLINICAL FEATURES
• ULCERATION OF PALATE AND NASAL SEPTUM ,STUFFINESS IN
THE NOSE
• PALATAL AND NASAL AND MALAR BONES INVOLVES
• PURULENT DISCHARGE ,PERFORATING SINUS TRACTS
,SLOUGHING OF THE SOFT TISSUES LEAVING A DIRECT
OPENING INTO THE NASOPHARYNX AND ORAL CAVITY
• VASCULAR ALLERGY ,ARTHUS PHENOMENON,PERIARTERITIS
NODOSA ,
• PATIENT ULTIMATELY DIES OF EXHAUSTION OR OF
HAEMORRHAGE IF A LARGE BLOOD VESSE BECOMES ERODED
43

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 44/93
44

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 45/93
45

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 46/93
Histologic features:
• Extensive necrosis with infiltration of some inflammatory cells
• the formation of occasional new capillaries .
• TREATMENT:
•
Usually fatal diseases .• Corticosteriod therapy .
• Coupled with antibiotics for secondary infection .
• Some authorities believe that the disease is best treated with
high dose of radaition therapy.

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 47/93
WEGENER’S GRANULOMATOSIS
• CLINICAL FEATURES
• INFANTS TO ELDERLY ,MAJORITY IN 4 TH OR 5 TH DECADE OF
THE LIFE
• MALE PREDOMINANCE
• RHINITIS,OTITIS,SINUSITIS
• COUGH,HEMOPTYSIS,FEVER,JOINT PAINS,HAEMORRHAGIC OR
VESICULAR SKIN LESIONS
•
GRANULOMATOUS LESIONS OF THE LUNG• GLOMERULONEHRITIS …..UREMIA…..TERMINAL RENAL
FAILURE
47

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 48/93
Oral manifestations
• Involvement of gingiva strawberrygingivitisulcerations
• Starts from interdental papilla-spreads toperiodontal structures and lead to bone loss ,
tooth mobility .• Hyperplastic gingivitis(Israelson et al)
• Ulceration of palate due to extension of diseasefrom nose.
• Spontaneous exfoliation of teeth and failure of healing after removal of tooth.

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 49/93
STRAWBERRY GINGIVITIS
49

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 50/93
HISTOLOGIC FEATURES
• MIXED INFLAMMATION AROUND THE BLOOD
VESSELS
• VASCULITIS
• ORAL BIOPSY ….PSEUDOEPITHELIOMATOUS
HYPERPLASIA AND SUBEPITHELIAL ABSCESS
• GINGIVAL LESIONS …SCATTERED GIANT CELLS
50

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 51/93
Laboratory findings
• Anemia
• Leukocytosis
• Elevated E.S.R.
• Hyperglobinemia
• Hematuria
•
Some patients- circulating immune complex.

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 52/93
TREATMENT
• PREDNISONE
• CYCLOPHOSPHAMIDE
52

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 53/93
Chronic granulomatous disease
• Uncommon herediatary CONDITION caused due x
linked mode of tranmission.
• Majority patients are males
• Characterised by severe reccurent infection as aresult of defect of intracellular leukocyte enzyme
formation
• Failure to destroy catalase positive organism.
A VARIANT TRANSMITTED AS AN AUTOSOMAL
RECESSIVE CHARACTERISTIC

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 54/93
CLINICAL FEATURES
CLINICAL FEATURES
INFECTION FROM INFANCY …..LUNG
,LIVER,SPEEN,BONE,ECZEMATOUS LESIONS ON
THE FACE ,LEADING TO NECROSIS AND
GRANULOMA FORMATION
ABSCESS ,SEPTICAEMIA
,PNEUMONIA,PERICARDITIS ,MENINGITIS,OSTEOMYLELITIS
54

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 55/93
Oral manifestation
• Diffused stomatitis with or without solitary or
multiple ulcerations.
• benign migratory glossitis
• Enamel hyperplasia in very rare cases

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 56/93
Histologic features
• Small granulomas with mononuclear
histocytes
• Multiple inulated giant cells
• Central necrosis with polymorphonuclear
leukocyte may also be present.

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 57/93
Diagnosis and treatment
• Diagnosis:- neutrophil function test
• Treatment :- vigorous treatment of infection
Angioedema (angioneurotic edema

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 58/93
Angioedema (angioneurotic edema,
Quincke’s edema)
• Diffused erythematous swelling of skin mucosa and submucosal connective tissue.,
• Results in death due to GI or respiratory tractinvolvement.
• Pathogenesis:-
1] allergic angioedema (due to mast cell degradation)
2] associated with use of ACE inhibitors
3]activation of complement pathway• Presence of high level of antigen antibody complex
• Grossly elevated peripheral blood eosinophillic count.

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 59/93
Clinical features
• Soft,non tender,diffuse edematous,solitary ormultiple
• Lips ,chin,eyes,tongue,pharynx,larynx,hands,arms,legs,genitals
and buttocks• Enlargement usually resloves within 24 to 72 hrs
• Git symptons include pain ,vomitting,waterydiarrhoea
• Perioral or periorbital oedema
• Skin colour normal or slightly pink
59

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 60/93
60

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 61/93
TREATMENT
Antihisatmines
Laryngeal involvement ….intramuscular
epinephrine
Iv corticosteroids
C1 – inh deficiency respond to intubation and
tracheotomy
Androgens such as danazol ,stanazol for
hereditary and acquired form
61

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 62/93
Drug allergy
• IGE MEDIATED REACTIONS …ANTIBODY BINDS
TO THE DRUG THAT IS ALREADY ATTACHED TO
THE CELL SURFACE
• IN NON IMMUNOLOGIC DRUG REACTIONS,DRUGS DIRECTLY AFFECT THE MAST CELLS
WHICH CAUSES RELEASE OF CHEMICAL
MEDIATORS
62

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 63/93
Clinical features :
• Skin lesions , arthralgia ,fever,
lymphadenopathy and rarely agranulocytosis .
• Common drugs aspirin , barbiturates ,
chloromphenicol, tetracycline ,penicillin ,streptomycin and sulphonamides .

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 64/93
treatment
• Antihistamines (cortisone)
• Adrenaline
• Corticosteroids
64
8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 65/93
Oral manifestation .
• Stomatitis medicamentosa .
• Ulceration, necrosis, hemorrhage , gingivalhyperplasia.
• Altered salivary function .
• Altered taste sensation.
• Allergic reactions erythema multiforme ,
• Negative patch taste .
•Localized erythema and edema .
• Gingiva – necrotizing gingivitis or vincent’s diseases .
• Hairy tongue .

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 66/93
HAIRY TONGUE
66

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 67/93
CONTD
• Intraoral fixed drug reactions
• Lichenoid drug reactions
• Elongation and staining of filiform papillae
,producing a heavy coating of the tongue
• Anaphylactic stomatitis
67

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 68/93
Histologic features.
• Non specific patterns .
• Admixture of lymphocytes ,eosinophils and
neutrophils .
• Vacuolar changes of basal layer and individual
necrotic epithelial cells .
• Distinctive annular fluorescence
pattern.(string of pearl’s ).
• Basal cell cytoplasmic antibody .

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 69/93
Treatment
• Antihistamines ( cortisone )
• Adrenaline
• Corticosteroids
• Anaphlactic stomatitis …antihistamines
69

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 70/93
Contact stomatitis and dermatitis
• Causative agent chemical in nature
• Haptens
• Require conjugation with proteins to become
effective
• Process occurs with the aid of intra epithelial
langerhans cells
70
• DENTAL OR COSMETIC PREPARATIONS .
8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 71/93
1. Dentrifrices .
2. Mouth washes .
3. Denture powder .
4. Lipsticks , candy ,cough drops, chewing gum .
• DENTAL MATERIALS :
1. Rubber dam .
2. Vulcanite .
3. Alcrylic .
4. Metal alloy base .
•
DENTAL THERAUPATIC AGENTS :1. Alcohols
2. Antibiotics
3. Iodides ,phenols
4. Procaine .

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 72/93
Clinical features
• Stomatitis venenata
• Itching and burning sensation
• Skin becomes rough and dry
• Appearance of erythema
• Vesicle formation
•
Vesicle rupture …it becomes more severe
72

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 73/93
Oral manifestations .
• Mucosa – remarkably inflamed and edematous .
• Bright red gingiva in all quadrants .
• Buccal mucosa – puffy , dark red , revealing ,engorged and
ejected superficial capillaries on closure examination .
• Zone of ulceration – lips .
• Chronic cases – mucosaerythematous , hyperkeratotic
• Scaling , fissuring , or cracking of vermillion lip border.
•
Contact stomatitis .
8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 74/93
Histologic features
• Intra and inter cellular edema of the
epithelium along with the vesicle formation
within the epithelium or at the basement
membrane• Increased eosinophils
• Lymphocytes and plasma cells
• Engorged and dilated blood vessels
• Connective tissue – edema
74
8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 75/93
Diagnosis and treatment .
• Diagnosis – patch test
• Treatment- removal of offending material
Contact stomatitis with cinnamon

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 76/93
Contact stomatitis with cinnamon
flavouring
• Toothpaste –plasma cell gingivitis ,edema
,erythema
• Erythematous mucositis of the buccal mucosa
and tongue ,exfoliative chilitis ,circumoraldermatitis
• Lingual keratosis
• Buccal mucosa – oblong,hyper keratotic
lesions with an erythematous base
76

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 77/93
Contact stomatitis .
• Cinnamon oils –flavoring agent .
• Used in ice-cream , soft drinks alcoholic
beverages processed meats ,gum , candy
,tooth paste and mouth washes .

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 78/93
78
l f
8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 79/93
Histologic features .
• Acanthotic epithelium with elongated reteridges thinned suprapapillary palates .
• Hyperkeratosis and neutrophil exocytosis is
observed .• Connective tissue exhibits a diffuse chronic
inflammatory infiltrate predominantlyconsisting of lymphocytes .
• Characteristic perivascular infiltration of lymphocytes .
d
8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 80/93
Treatment and prognosis
• Reaction disappears within a week of
discontinuance of cinnamon products
• Reappears with use of cinnamon products
80
Contact stomatitis from chronic oral
8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 81/93
Contact stomatitis from chronic oral
mucosal contact with dental amalgam
• neurotoxicity ,kidney dysfunction, reduced
incompetence, alterations of oral and
intestinal flora , birth defects ,
• Contact lichenoid reactions to amalgam
81

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 82/93
8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 83/93
83
B f l
8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 84/93
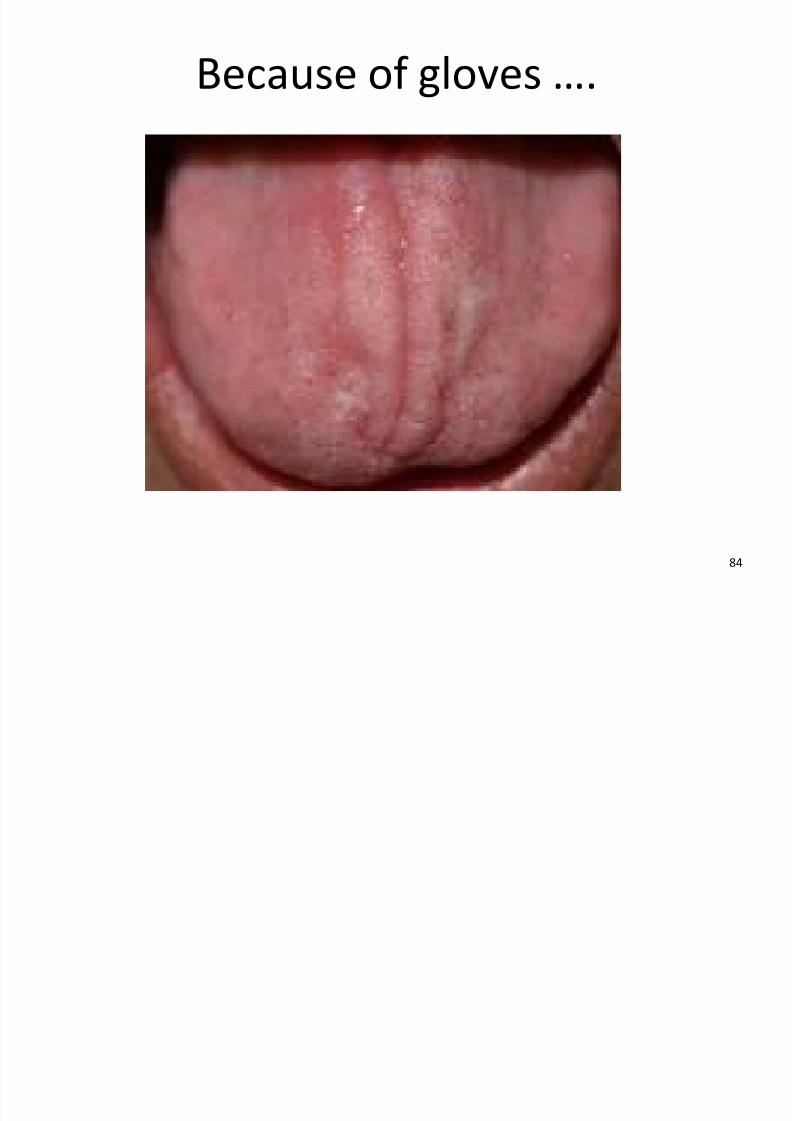
Because of gloves ….
84
Cli i l d hi t l i l f t

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 85/93
Clinical and histological features .
• Commonly seen in posterior buccal mucosa,ventral borders of the tongue and gingival cuffsadjacent to subgingival amalgam restorations.
•
White or ertythematous with or without striae .• Histologically features similar to lichen planus like
hydropic degeneration of basal cell layer .
• Hyperkeratotic or atropic epithelium ,and dense
band- like chronic inflammatory infiltrateconsisting predominantly of lymphocytes areobserved
T t t d i

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 86/93
Treatment and prognosis .
• Improving oral hygienic ,smoothening,polishing ,and recontouring of the restoration
before adopting aggressive measures .
• Amalgam replaced with a non-metallicrestoration .
P i l d titi

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 87/93
Perioral dermatitis
• Skin disease of the circum oral area due totartar control,bubble gum ,night creams
,toothpaste, moisturizers
• Topical corticosteroids is inciting agents
87
Cli i l f t

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 88/93
Clinical features
• Pruritis
• Female predominance
• Lesions as papules or papulopustules
• Surface surrounding the vermillion border of
the lip ,with zone of spared skin immediately
adjacent to the vermillion border .
88

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 89/93
89
Hi t l i f t

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 90/93
Histologic features
• Rosacea like pattern
• Chronic lymphohistiocytic dermatitis
• Mimicking sarcoidosis
90
T t t d i

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 91/93
Treatment and prognosis .
• topical corticosteroid and prescribing topicalmetronidsazole
• With out topical tetracycline .
• Recurrences are uncommon.
Bibliography

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 92/93
Bibliography
• Shafer’s textbook of oral pathology
92

8/4/2019 Man Ali
http://slidepdf.com/reader/full/man-ali 93/93


















