Mammary Analogue Secretory Carcinoma of … › docs › 2013 Conf PDFs › 18 - Fri...
28
A Cutaneous Facial Mass Identified as the New Entity ‘Mammary Analogue Secretory Carcinoma’ of Probable Salivary Gland Origin Scott W. Binder, MD Professor and Senior Vice Chair Chief, Dermatopathology Geffen/UCLA Healthcare
Transcript of Mammary Analogue Secretory Carcinoma of … › docs › 2013 Conf PDFs › 18 - Fri...

A Cutaneous Facial Mass Identified as the New Entity ‘Mammary Analogue Secretory Carcinoma’ of Probable Salivary Gland Origin
Scott W. Binder, MD Professor and Senior Vice Chair
Chief, Dermatopathology Geffen/UCLA Healthcare

Case Presentation
A 50 year-old man presents with a 7 mm erythematous papule on the right face.
• Developed over a few months
• Asymptomatic
• No history of prior neoplasms including salivary glad tumors
Presenter
Presentation Notes
We have a 50-year-old man who presented with an asymptomatic, small erythematous papule on the R face, which had been present for 3 months.

Clinical Impression
“Rule out bug bite”
Presenter
Presentation Notes
The lesion was biopsied to “rule out a bug bite”

Differential Diagnoses
• Acinic cell carcinoma
• Apocrine or eccrine sweat duct tumor
• Mammary analogue secretory carcinoma
• Benign oncocytic neoplasms • Oncocytoma, Oncocytic cystadenoma, Warthin tumor
• Mucoepidermoid carcinoma
• Salivary duct carcinoma
Presenter
Presentation Notes
A tumor with this morphology has a limited differential. Until recently, the identification of a microcystic architecture within a primary salivary gland neoplasm would have been strong evidence in support of a diagnosis of acinic cell carcinoma. Serous acinar granules within the cytoplasm of tumor cells would carefully searched for, and if not apparent on routine H&E stains, a PAS plus diastase stain would be applied to aid in the search. Depending on the findings elsewhere, and assuming no acinar granules identified, the tumor in the past might have been termed low-grade adenocarcinoma (favor acinic cell carcinoma) or, if other features supported, simply acinic cell carcinoma. Now, with the description of the entity known as mammary analogue secretory carcinoma (MASC), further study is necessary to identify the presence of some of the characteristics of this lesions.

Diagnosis
Mammary Analogue Secretory Carcinoma (MASC)
? Primary salivary gland origin v. primary cutaneous tumor
Presenter
Presentation Notes
The constellation of histologic and immunologic features favors a low-grade carcinoma, suggestive of mammary analogue secretory carcinoma of salivary gland origin. The lesion appears quite cellular and demonstrates and infiltrative growth pattern, both atypical features. We want to emphasize some features of the immunologic staining pattern. Negative staining of this tumor with antibodies to p63 and cytokeratin 5/6 argue against a primary cutaneous sweat duct tumor and suggest the possibility of a metastasis from a visceral primary. The strong positive staining with mammaglobin may reflect a breast or salivary gland origin. So-called mammary analogue secretory carcinoma of the salivary gland may show positive immunostaining with S100, CK7, and mammaglobin, as seen in this tumor. Strong positive staining of tumor cells with antibodies to EMA is consistent with low grade carcinoma of MASC-type.

Background
• MASC first described in 2010 by Skalova et al.
• Morphologic overlap between acinic cell carcinoma and secretory carcinoma of the breast
• Tumors affect all ages (range 14-77), slightly male-predominant
Presenter
Presentation Notes
MASC was initially described in a series of 16 cases by Skalova et al in 2010. The authors had identified in their consultation practices a tumor that showed morphologic overlap between acinic cell carcinoma and secretory carcinoma of the breast. Since the initial description, there have been several additional reports describing small series of cases designated as MASC. The tumors affect patients over a wide age range, from 14 to 77, with an average age of 44 years. Males have been affected more frequently (21M:F14)

MASC
• Presents as slowly growing mass, often near parotid gland
• No evidence of primary cutaneous origin, as of yet
• Most treated with non-radical excision +/-radiotherapy
• Cases of lymph node metastases, local recurrences, low mortality Chiosea et al, Histopathology 2012
Presenter
Presentation Notes
Most presented with a slow growing mass. In 23 cases the parotid was the site of involvement, while oral sites made up the bulk of the remainder (lip, palate, and buccal mucosa). In 2 cases, the submandibular gland was involved. The tumors varied in size from 0.7-5.5cm. Most patients were treated with non-radical excision with or without radiotherapy. There is limited follow-up information, but 2 patients in the original series died of disease after 2 and 6 years, while 4 patients had local recurrences. Lymph node metastases have been identified in 3 patients – two at the time of diagnosis, and in another 86 months after initial treatment.

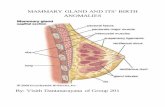
Histology of MASC
• Unencapsulated, lobulated
• Intercalated duct cells in tubular, microcystic, papillary patterns
• Lumina with ample “bubbly” secretions (mucicarmine +)
• Absence of serous acinar granules
Presenter
Presentation Notes
Microscopic descriptions of MASC have been generally uniform, with unencapsulated lobular tumor made of cuboidal cells arranged in ductal, papillary, microcystic patterns. Microcystic architecture is most common, with abundant secretions in the lumina that stain with mucicarmine and PASD. Unlike in AiCC, serous acinar granules tend to be absent, although this is not absolute. Staining is positive for S100, CK7, EMA, mammoglobin, GCDFP. Basal cell/ myoepithelial markers are negative (p63, calponin, CK5/6

Immunohistochemistry of MASC Staining • Usually positive
• S100
• CK7
• Vimentin • Often positive
• EMA
• GCDFP
• Mammoglobin
• Negative
• CK5/6, CK20
• P63, TTF-1, PSA, Thyroglobulin
9

Differentiating Features of MASC
Griffith et al, Cancer Cytopathology 2012
Presenter
Presentation Notes
Cytomorphology as well as immunostaining can help distinguish between these entities. For example, acinic cell carcinoma usually lacks mucin. Mucoepidermoid carcinoma has epidermoid differentation, which is not seen in MASC. S-100, p63, mammoglobin are all stains to help further distinguish these tumors. I won’t pause too much on this figure, but if you’re interested in specific stains, I would like to direct you to a paper published in Cancer Cytopathology in 2012 by Griffith et al.

Differentiating Features of MASC
Griffith et al, Cancer Cytopathology 2012
Presenter
Presentation Notes
Cytomorphology as well as immunostaining can help distinguish between these entities. For example, acinic cell carcinoma usually lacks mucin. Mucoepidermoid carcinoma has epidermoid differentation, which is not seen in MASC. S-100, p63, mammoglobin are all stains to help further distinguish these tumors. I won’t pause too much on this figure, but if you’re interested in specific stains, I would like to direct you to a paper published in Cancer Cytopathology in 2012 by Griffith et al.

Fusion Gene
• Almost all MASC had fusion gene ETV6-NTRK3
Normal Cells No ETV6 Split Signals Abnormal ETV6 split signals
Presenter
Presentation Notes
Lastly, all cases of MASC, except one have exhibited a t(12;15)(p13;q25) rearrangement leading to ETV6-NTRK3 fusion. We performed FISH studies in our case, which showed the 12p13 region involved as exhibited by the spilt signals of the ETV6 dual color breakpart probe. A normal cell would show both the red and green signals in close proximity while any rearrangement will show spilt or other signal pattern consistent with 12p13 abnormality. What you see is a fair amount of genomic heterogeneity suggestive of unbalanced rearrangement. The verdict is that there is indeed a ETV6 translocation in over 90% of the cells analyzed. This test is an extremely useful test to distinguish MASC from other tumors. And it was confirmed in our patient.

Clinical Course
• Patient had neoplasm completely excised by the ENT service
• Work-up for primary underlying neoplasm is on-going and imaging studies are negative for primary salivary gland tumor

Summary
• MASC is likely an under-recognized diagnosis and can present a diagnostic pitfall, easily being confused with a primary adnexal tumor given that it is a newly-described entity and too bland to be immediately interpreted as a metastasis or recurrence. The origin of this particular tumor is still uncertain, as no salivary gland primary has been detected in this patient.
• Immunohistochemical stains for S100, CK7, p63, vimentin, mammaglobin, GCDFP, and identification of the ETV6-NTRK3 fusion gene would be required to completely evaluate tumors of this type.
Presenter
Presentation Notes
First, one sees bland-appearing tumors which have resembled sweat duct tumors in the past which eventually were discovered to be metastases from occult visceral sites such as the salivary gland, breast, or lung. Therefore, keep MASC in mind. Second, cytologic features in combination with immunostaining and cytogenetic analysis can distinguish this entity from others in the differential diagnoses, such as acinic cell carcinoma.

Cutaneous Metastases v. Adnexal Primary Carcinoma: A Practical Approach
15

Cutaneous Metastases
• Clinical Considerations •Mean age at presentation is 62 •Most common primary tumors
• Lung 30% • Melanoma 18% • G.I. Tract 14% • Breast 5% • Lymphoma 5%
• In approximately 10% of cases, the primary is unknown • Histologic Types
• Adenocarcinoma 40% • Melanoma 15% • Squamous carcinoma 15% • Other 30%
16

Cutaneous Metastases
• Relative frequencies of involvement of different skin sites •Face & Scalp 22%
•Abdomen 18%
•Back 12%
•Chest 10%
17

Cutaneous Metastases v. Primary Adnexal Carcinoma
• Histopathologic Characteristics of Metastases •Tumor growth often concentrated in the deep dermis - “bottom heavy” appearance
• Sparing of epidermis common
•Ulceration and pagetoid spread rarely noted (colonic and melanoma)
•Tumor necrosis sometimes present
•Lymph/vascular invasion sometimes observed
•High grade tumor cells with numerous mitoses
18

Cutaneous Metastases v. Primary Adnexal Carcinoma
• Immunohistochemical Considerations • Battery may include
•Cytokeratin 7 •Cytokeratin 20 • S-100 •MART-1/Melan-A/MITF or SOX-10 •PSA •TTF-1 •ER/PR/Her-2-neu •CDX-2 •Cytokeratin 5/6, p63*
19

Cutaneous Metastases v. Primary Adnexal Carcinoma
• Most common patterns of staining: •Lung adenocarcinoma: CK7+/CK20-, S-100-, TTF-1+ •Melanoma: CK7-/CK20-/S-100+/MART-1+/MITF •Bladder (TCC): CK7+/CK20+/S-100- •Renal Cell CA: CK7+/CK20-/S-100-/EMA+/CA-9+ •Breast: CK7+/CK20-/ER/PR+/Her-2-neu+/- •Prostate: CK7-/CK20-/PSA+
20

Cutaneous Metastases v. Primary Adnexal Carcinoma
• Recent studies have shown that CK5/6 and p63 may help distinguish primary adnexal neoplasms (CK5/6+/p63+) from most metastatic carcinomas (CK5/6-/p63-)
• P63 especially helpful • D2-40 not been especially helpful in my lab
21

Cutaneous Metastases v. Primary Adnexal Carcinoma
• Impossible to reliably distinguish primary or metastatic eccrine/apocrine tumors from cutaneous metastases of breast carcinomas, especially apocrine or mucinous types
• Immunohistochemical Staining of Breast v. Metastases •ER (estrogen receptor) •PR (progesterone receptor) •GCDFP-15 (gross cystic disease fluid protein) •CEA •Her-2-neu
• None of these may reliably separate primary sweat duct from breast metastases
22

Cutaneous Metastases v. Primary Adnexal Carcinoma
• Of these, the best combination: •Her-2-neu: more commonly positive in metastatic breast CA than adnexal/sweat duct primaries
•Androgen receptor: more common in sebaceous tumors than breast metastases
23

24
Cutaneous Metastases v. Primary Adnexal Carcinoma
• Aberrant staining of metastases •Technical
•Antibody • Technique
•Therapeutic effect – chemo and/or radiation/immune modulators •Tumor metastases may have different immuno phenotypes than the primary •Tumors don’t always read the books •Another tumor/primary is responsible for the aberrant staining

25
Cutaneous Metastases v. Primary Adnexal Carcinoma
• Take Home •H&E considerations and clinical information most important for diagnostic purposes •Immunohistochemistry stains are useful ancillary studies, especially cytokeratin 5/6 and p63 but be careful as these may lead you astray •Be sure to eliminate the possibility of a basal cell carcinoma demonstrating unusual growth patterns •Always think of the possibility of a primary adnexal CA in the appropriate clinical and histologic context •Occasional inability to differentiate a primary adnexal CA from a visceral metastasis

References
• Saliva A, Vanecek T, Sima R, Laco J, Weinreb I, Perez-Ordonez B, Starek I, Geierova M, Simpson RH, Passador-Santos F, Ryska A, Leivo I, Kinkor Z, Michal M. Mammary analogue secretory carcinoma of salivary glands, containing the ETV6-NTRK3 fusion gene: a hitherto undescribed salivary gland tumor entity. Am J Surg Pathol. 2010 May;34(5):599-608. • Griffith C, Seethala R, Chiosea SI. Mammary analogue secretory carcinoma: a new twist to the
diagnostic dilemma of zymogen granule poor acinic cell carcinoma. Virchows Arch. 2011 Jul;459(1):117-8. • Fehr A, Löning T, Stenman G. Mammary analogue secretory carcinoma of the salivary glands with
ETV6-NTRK3 gene fusion. Am J Surg Pathol. 2011 Oct;35(10):1600-2. • Rastatter JC, Jatana KR, Jennings LJ, Melin-Aldana H. Mammary analogue secretory carcinoma of the
parotid gland in a pediatric patient. Otolaryngol Head Neck Surg. 2012 Mar;146(3):514-5. • Connor A, Perez-Ordoñez B, Shago M, Skálová A, Weinreb I. Mammary analog secretory carcinoma
of salivary gland origin with the ETV6 gene rearrangement by FISH: expanded morphologic and immunohistochemical spectrum of a recently described entity. Am J Surg Pathol. 2012 Jan;36(1):27-34. • Chiosea SI, Griffith C, Assaad A, Seethala RR. Clinicopathological characterization of mammary
analogue secretory carcinoma of salivary glands. Histopathology. 2012 Sep;61(3):387-94. • Griffith CC, Stelow EB, Saqi A, Khalbuss WE, Schneider F, Chiosea SI, Seethala RR. The cytological
features of mammary analogue secretory carcinoma: a series of 6 molecularly confirmed cases. Cancer Cytopathol. 2013 May;121(5):234-41. • Bishop JA. Unmasking MASC: bringing to light the unique morphologic, immunohistochemical and
genetic features of the newly recognized mammary analogue secretory carcinoma of salivary glands. Head Neck Pathol. 2013 Mar;7(1):35-9.

References
• Jung MJ, Song JS, Kim SY, Nam SY, Roh JL, Choi SH, Kim SB, Cho KJ. Finding and characterizing mammary analogue secretory carcinoma of the salivary gland. Korean J Pathol. 2013 Feb;47(1):36-43. • Hwang MJ, Wu PR, Chen CM, Chen CY, Chen CJ. A rare malignancy of the parotid gland in a
13-year-old Taiwanese boy: case report of a mammary analogue secretory carcinoma of the salivary gland with molecular study. Med Mol Morphol. 2013 Aug 18. • Knezevich SR, Garnett MJ, Pysher TJ, et al. ETV6-NTRK3 gene fusions and trisomy 11
establish a histogenetic link between mesoblastic nephroma and congenital fibrosarcoma. Cancer Res. 1998;15:5046–5048. • Makretsov N, He M, Hayes M, et al. A fluorescence in situ hybridization study of ETV6-
NTRK3 fusion gene in secretory breast carcinoma. Genes Chromosomes Cancer. 2004;40:152–157. • Rastatter JC, Jatana KR, Jennings LJ, Melin-Aldana H. Mammary analogue secretory carcinoma
of the parotid gland in a pediatric patient. Otolaryngol Head Neck Surg. 2012 Mar;146(3):514-5. • Connor A, Perez-Ordoñez B, Shago M, Skálová A, Weinreb I. Mammary analog secretory
carcinoma of salivary gland origin with the ETV6 gene rearrangement by FISH: expanded morphologic and immunohistochemical spectrum of a recently described entity. Am J Surg Pathol. 2012 Jan;36(1):27-34. • Chiosea SI, Griffith C, Assaad A, Seethala RR. Clinicopathological characterization of
mammary analogue secretory carcinoma of salivary glands. Histopathology. 2012 Sep;61(3):387-94.

References
•Griffith CC, Stelow EB, Saqi A, Khalbuss WE, Schneider F, Chiosea SI, Seethala RR. The cytological features of mammary analogue secretory carcinoma: a series of 6 molecularly confirmed cases. Cancer Cytopathol. 2013 May;121(5):234-41. • Bishop JA. Unmasking MASC: bringing to light the unique morphologic,
immunohistochemical and genetic features of the newly recognized mammary analogue secretory carcinoma of salivary glands. Head Neck Pathol. 2013 Mar;7(1):35-9. • Jung MJ, Song JS, Kim SY, Nam SY, Roh JL, Choi SH, Kim SB, Cho KJ. Finding and
characterizing mammary analogue secretory carcinoma of the salivary gland. Korean J Pathol. 2013 Feb;47(1):36-43. • Hwang MJ, Wu PR, Chen CM, Chen CY, Chen CJ. A rare malignancy of the parotid
gland in a 13-year-old Taiwanese boy: case report of a mammary analogue secretory carcinoma of the salivary gland with molecular study. Med Mol Morphol. 2013 Aug 18. •Knezevich SR, Garnett MJ, Pysher TJ, et al. ETV6-NTRK3 gene fusions and trisomy 11
establish a histogenetic link between mesoblastic nephroma and congenital fibrosarcoma. Cancer Res. 1998;15:5046–5048. •Makretsov N, He M, Hayes M, et al. A fluorescence in situ hybridization study of ETV6-
NTRK3 fusion gene in secretory breast carcinoma. Genes Chromosomes Cancer. 2004;40:152–157.