Male Reproductive Disorders St
42
Disorders of Male Reproductive System NURS 304 – Adult Nursing 2 Lecturer: K. Mackey
-
Upload
estherthompson -
Category
Documents
-
view
7 -
download
2
description
Male Reproductive System
Transcript of Male Reproductive Disorders St

Disorders of Male Reproductive SystemNURS 304 – Adult Nursing 2Lecturer: K. Mackey

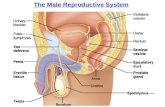
Structures of the Male Reproductive Tract

Assessment Sexual function
Diseases e.g. diabetes, multiple scerosis, CVA, cardiac disease
Medications e.g antihypertensives, psychotrophic agents, antihyperlipedemia
Alcohol use
stress
Urinary symptoms

Assessment
• Urinary function and symptoms
• Symptoms related to urinary obstruction– urinary frequency– Decreased force of stream– “Double” or “triple” voiding– Nocturia– Dysuria– Hematuria– hematospermia

Physical Assessment Digital rectal exam
Testicular exam
Assessment Digital rectal exam (DRE)
Used to screen for prostate CA
Recommended in men 40yrs and over
prostate gland is assessed
Inspect male genitalia Note any abnormalites
Palpate for masses
Discharges, inflammation

Assesment Scrotum
Palpated for nodules, masses, inflammation
Note abnormalities such as hydrocele, hernia, masses
Tumours of testes
Instruct pt. on TSE and purpose
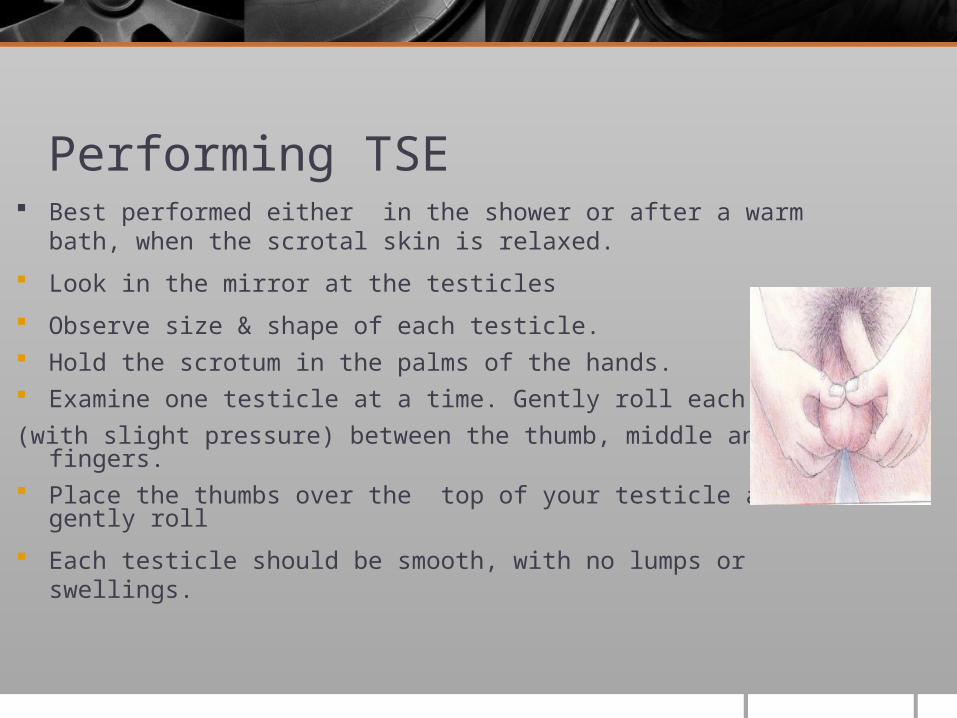
Performing TSE Best performed either in the shower or after a warm bath,
when the scrotal skin is relaxed.
Look in the mirror at the testicles
Observe size & shape of each testicle. Hold the scrotum in the palms of the hands. Examine one testicle at a time. Gently roll each testicle
(with slight pressure) between the thumb, middle and index fingers.
Place the thumbs over the top of your testicle and gently roll
Each testicle should be smooth, with no lumps or swellings.

TSE contd. Locate and palpate the epididymis and spermatic cord
Check for any small irregularities, enlargements and: An increase in firmness of a testicle
Pain or discomfort in a testicle or in the scrotum
An unusual difference between one testicle and the other.
A heavy feeling in the scrotum
A dull ache in the lower stomach, groin or scrotum.
Normal for one testis to be slightly larger than the other

Diagnostic Tests
Prostate specific antigen (PSA) 0.2 – 4.0 ng/ml
Annual testing
Ultrasonography (TRUS)
Prostate fluid or tissue analysis
Tests of male sexual function

Common Conditions of Male Reproductive Organs
Crytorchidism
Orchitis
Epididymitis
Phimosis
Priaprism
Circumcision

Common Conditions of Male Reproductive System
• Hydrocele – collection of fluid in testes• Varicocele – abnormally dilated veins in the scrotum• Hypospadias – shortened urethra, urethral opening located on
ventral side of penis (congenital anomaly)• Epispadias – urethral opening is on dorsum of penis• peyronie’s disease – build up of fibrous plaque in corpus
cavernosum• urethral stricture – narrowing of urethra

Disorders of Male Sexual Function
• Erectile dysfunction• The inability to achieve/sustain an erection sufficient
to accomplish intercourse– Psychogenic and organic causes– Organic causes include vascular, endocrine, hematological,
and neurologic disorders, trauma, alcohol, medications, and drug abuse
– Medications associated with erectile dysfunction (pg. 1745; 49-1)

Erectile Dysfunction• Pharmacologic therapy–Oral medications—sildenafil (Viagra), cialis,
levitra• Side effects include headache, flushing,
dyspepsia• Use cautiously in pts. with retinopathy
Injected vasoactive agents Surgical implants
• Complications of erectile dysfunction include priapism (persistent abnormal erection)

Prostatitis
• Inflammation of prostate gland caused by an infectious agent
• Clinical manifestations– Fever, chills– Dysuria– Frequency– Urgency– Perineal pain– Nocturia– Rectal or lower back pain

ProstatitisPathophysiology
Inflammation of the prostate gland cause by infectious agents E. coli is the most common
Microorganisms are usually carried to the prostate from the urethra

Prostatitis Diagnosis (May be acute or chronic)
History
Culture of prostate gland
Urine for C & S
Histological examination of the tissue
D.R.E.
Swollen, tender & firm prostate gland
Prostatic massage Obtain prostatic fluid

Prostatitis Management
Antibiotic therapy broad-stectrum antibiotic
(rimethroprim sulfamethoxazole (Bactrim)Cirpfloxacin (Cipro) Analgesics for pain
Sitz bath (10-20mins)
Educate pt. on disease process
Stool softeners

Prosatitis1. AVOID Foods and liquids that have diuretic actions or that increase
Prostatic secretion should be avoided 1. Alcohol
2. Coffee
3. Tea
4. Chocolate
5. Cola
6. Spices
2. Avoid intercourse
3. Avoid sitting for long periods

Prostatitis Complications
Swelling of prostate gland
Urinary retention
Epididymitis
Bacteremia
pyelonephritis

Benign Prostatic Hypertrophy
• Non malignant enlargement of the prostate gland.• Characterized by formation of large nodular lesions in the periurethral region
of the prostate.
• Etiology– Unknown– Dihydrotestosterone (DHT) active metabolite in testosterone contibutes to
BPH– Free plasma testosterones enters prostatic cells where about 90% is converted
to DHT
• Predisposing factors– Men over the age of 50 years• Smoking• Heavy alcohol consumption• Diabtes, hypertension, heart disease• Race, ethnicity• Family history

Benign Prostatic Hypertrophy Clinical Manifestations
Signs of urinary obstruction Acute urinary retention Frequency Urgency Nocturia Abdominal straining with urination Hesitancy in passing urine Decrease in volume and force of urinary stream Dribbling urinary tract infections Sensation that bladder is not completely emptied General symptoms, fatigue, anorexia, pelvic discomfort
Renal failure can occur with chronic urinary retention

BPH: Pathophysiology• Pathophysiology not clearly understood
– Hormonal contribution in men with elevated testosterone levels – Develops over long period– Hypertrophied lobe of prostate obstruct the prostatic urethra– This causes the bladder to become over distended, urinary retention occurs with
incomplete emptying of the bladder– Frequency of urination occurs with constant desire to empty the bladder– Frequency becomes worse at nights Gradual dilation (hydroureter) of ureters and kidneys (hydronephrosis) occur
UTI may result from urinary stasis,
Urine remaining in the urinary tract serves as a medium for infectious organisms

BPH Diagnosis
History Digital rectal exam Urine analysis CBC’s Ultrasound scan (trans abdominal or rectal) PSA Serum creatinine levels

Medical Management: BPH Treatment
Pharmacologic—alpha-adrenergic blockers, alpha- adrenergic antagonists, antiandrogen agents
Antiandrogen agents Relax smooth muscle of bladder, relieving urinary symptoms Catherization if unable to void
Prostate surgery TURP surgical resection Strinking of prostate
Prostate Cancer
Second most common cancer and the second most common cause of cancer death in men
Risk factors: increasing age familial predisposition African-American race
Early diagnosis is vital; health screening

Prostate Cancer• Clinical Manifestations
– Frequency of urination– urgency– hesitancy in starting urination– recurrent UTI– dribbling– interruption of urinary flow– sensation that bladder has not emptied– decrease in volume and force of urine stream
• Diagnosis– Digital rectal exam– PSA, Transrectal Ultrasound guided biopsy

Nursing Diagnoses Anxiety
Acute pain preoperatively
Acute pain postoperatively
Deficient knowledge

Nursing Management—Planning
Major goals preoperatively: adequate preparation and reduction of anxiety
Reduction of pain.
Major goals postoperatively: maintenance of fluid volume balance
relief of pain and discomfort
ability to perform self-care activities
absence of complications

Interventions• Routine preoperative management
– enema
• Reduction of anxiety– Be sensitive to potentially embarrassing and culturally charged issues – Establish a professional, trusting relationship – Provide privacy– Allow patient to verbalize concerns– Provide and reinforce information
• Provide patient teaching including explanations of anatomy and function, diagnostic tests and surgery, and the surgical experience.
• Preparation of pt. for actual surgery

Management Surgery
Transurethral resection of the prostate (TURP)
Chemotherapy
Radiation therapy

Prostate Cancer Surgical Management
Radical prostatectomy: removal of the prostate, seminal vesicles, tips of the vas deferens, surrounding fat, nerve and blood vessels may also be removed.
Radiation therapy If detected in the early stages radiation treatment can be used to destroy tumor
hormonal therapy Use of antiandrogen drugs to decrease growth of tumor
Chemotherapy Use of ketoconazole to lower testosterone levels

Post operative• Pain management• V/S• Fluid balance management• Irrigation of bladder
– Close monitoring of fluid intake, output– Amount of fluid used for irrigation– Irrigate according to Dr.’s order
• Ensure tubing is secured properly
• Monitor urinary drainage and keep catheter patent– Drainage is red then pink within 24hrs
• Cather care to prevent infection

Post operative care Observation of dressing site
Observe abdomen for distension Assessment of pain
Bladder spasms cause feelings of pressure and fullness urgency to void
bleeding from the urethra around the catheter. Educate pt. not to pull on catheter/tubing Advice re: feelings of urge to void is normal

Relief of Pain
Warm compresses or sitz baths to relieve spasms Administer analgesics and antispasmodics as ordered Encourage patient to walk, but to avoid sitting for prolonged
periods. Prevent constipation Ambulation begins 24hrs. post op Wound care using strict asepsis

Three-Way System for Bladder Irrigation

Collaborative Problems/Potential Complications
Hemorrhage and shock
Infection
DVT
Catheter obstruction
Sexual dysfunction

Rehabilitation and Home Care
Patient and family teaching for home care including care of urinary drainage devices and recognition and prevention of complications
Regain bladder continence Information that regaining control is a gradual process (dribbling may continue
for up to 1 year depending upon type of surgery) Perineal exercises
Avoidance of straining, heavy lifting, long car trips (6–8 weeks)
Diet: encourage fluids and avoid coffee, alcohol, and spicy foods
Assessment and referral of sexual issues

Testicular Cancer
• Most common cancer in men ages 15–40• Highly treatable and curable• Risk factors: undescended testicles, positive family history, cancer of one
testicle, Caucasian-American race• Manifestations: painless lump or mass in the testes• Early diagnosis: monthly testicular self-exam (TSE) and annual testicular exam • Treatment: orchidectomy, retroperitoneal lymph node dissection (open or
laparoscopic), radiation therapy, chemotherapy

Testicular cancer
Tumor markers that may be elevated in testicular cancer: Human chorionic gonadotropin
alpha fetoprotein.

Nursing Management Assessment of physical and psychological status
Support of coping
Address issues of body image and sexuality
Encourage a positive attitude
Patient teaching
TSE and follow-up care

References Salzano, C. (2008). Testicular Cancer
Bare, B., Cheever, K., Hinkle, J.L. & Smeltzer, S.C. (2008). Brunner, & Suddath’s textbook of medical-surgical nursing. (11th Ed.). Philidelphia: Lippincot Williams & Wilkins.