Malabsorption syndrome: pathophysiology and diagnosis. Teaching slides
24
Malabsorption syndrome Stefano Fiorucci, MD Department of Surgery and Biomedical Sciences University of Perugia
-
Upload
attivita-scientifica -
Category
Health & Medicine
-
view
204 -
download
6
Transcript of Malabsorption syndrome: pathophysiology and diagnosis. Teaching slides

Malabsorption syndrome
Stefano Fiorucci, MDDepartment of Surgery and Biomedical Sciences
University of Perugia

Malabsorption• Disorders of absorption constitute a broad spectrum of conditions with multiple
etiologies and varied clinical manifestations. Almost all of these clinical problems are associated with diminished intestinal absorption of one or more dietary nutrients and are often referred to as the malabsorption syndrome.
• Malabsorption is a clinical term that encompasses defects occurring during the digestion and absorption of food nutrients
• Impairment can be of single or multiple nutrients depending on the abnormality.
• Most, but not all, malabsorption syndromes are associated with steatorrhea, an increase in stool fat excretion of >6% of dietary fat intake. Some malabsorption disorders are not associated with steatorrhea: primary lactase deficiency, a congenital absence of the small intestinal brush border disaccharidase enzyme lactase, is associated with lactose "malabsorption," and pernicious anemia is associated with a marked decrease in intestinal absorption of cobalamin (vitamin B12) due to an absence of gastric parietal cell intrinsic factor required for cobalamin absorption

CLASSIFICATION OF MALABSORPTION SYNDROMESInadequate digestion
Postgastrectomy
Deficiency or inactivation of pancreatic lipaseExocrine pancreatic insufficiency, chronic pancreatitis, pancreatic cancer, cystic fibrosis, gastrinoma
Reduced intraduodenal bile acid concentration/impaired micelle formationCholestatic liver diseasesBacterial overgrowth in small intestine:
Afferent loop /stricture/fistulasInterrupted enterohepatic circulation of bile saltsIleal resection, Crohn diseaseDrugs (bind or precipitate bile salts)neomycin, cholestyramine, calcium carbonate Impaired mucosal absorption/mucosal loss or defectCrohn’s disease
Inflammation, infiltration, or infection:Crohn’s diseaase, amyloidosis, scleroderma Lymphoma, eophionolic gastroenteritis, celiac sprue, collagenous sprueWhipple disease, radiation enterits, infection includinggiardiasis, grapht vs hostGenetic disorders
Disaccharidase deficiency, agammaglobulinemia, abetalipoproteinemia, Hartnupdisease, cystinuriaImpaired nutrient delivery to and/or from intestine:L ymphomaa Lymphangiectasia Lymphatic obstruction Circulatory disordersEndocrine and metabolic disorders
Malabsorption:Causes
Exocrine pancreatic insufficiency chronic pancreatitispancreatic cancercystic fibrosis
Inactivation of pancreatic lipase – Gastrinoma(ZES)
drugs (orlistat)bile acid (impaired
micelle formation)parenchymal liver D.cholestatic liver D.
Bacterial overgrowthAnatomic stasis(blind loop, stricture, fistula)Functional stasis(DM, scleroderma)
Interrupted interohepatic circulation of bile acid(ileal resection, crohn’s D.)
Drugs(bind or precipitate bile salt)neomycin, chlestyramine
Impaired mucosal absorbtion/mucosal loss or defectintestinal resection or bypassinflammation/infiltration/infect.(celiac sprue, tropical sprue,whippl’s disease, lymphoma,mastocytosis, eosinophilic e.,scleroderma, crohn’s D., …)
Impaired nutrient transportlymphatic obstruction(lymphoma, lymphangectasia)CHF
Genetic disordersdisacharidase defficiencyAgamaglobulinemiaAbetalipoprotinemia
Endocrine/Metabolic disordersDM
Hyperthyroidismadrenal insufficiency
carcinoid syndrome
Malabsorptive disorders can be categorized into
1-Generalized mucosal abnormalities
resulting in multiple nutrient malabsorption
2-Specific nutrient disorder
(carbohydrate, fat, protein, vitamin and mineral
malabsorption)
Malabsorptive disorders with generalized mucosal defects
• Celiac disease
• Cow’s milk allergy
• Microvillous inclusion disease
• Tufting enteropathy
• Lymphangiectasia
• Short bowel syndrome
• Chronic malnutrition
• Congenital immunodeficiency disorders
• HIV
• Parasitic infections
• Tropical sprue
• Bacterial overgrowth

Specific nutrient malabsorptive disorder
Carbohydrate malabsorption
- lactase deficiency (congenital, secondary)
- Congenital sucrase-isomaltasedeficiency
- Glucose- galactose malabsorption
Protein malabsorption- Enterokinase deficiency
- Amino acid transport defect
(eg;Hartnup disease )
Fat malabsorption
-Pancreatic exocrine insufficiency
(cystic fibrosis, shwachman
diamond syndrome, chronic
pancreatitis)
-liver and biliary disorders
- abetalipoproteinemia

Specific nutrient malabsorptive disorder
Mineral and vitamin malabsorption
-Congenital chloride diarrhea
-Congenital sodium absorption defect
-Acrodermatitis enteropathica
-Menke disease
-Vitamin D dependent rickets
-Vitamin B12 malabsorption
Mechanisms1. Luminal phase (processing defect)
– Digestive enzyme deficiency / inactivation– bile salt synthesis; Excretion; loss;
bile salt de-conjugation– gastric acid; intrinsic factor (p. anemia)– Bacterial consumption of nutrients
2. Mucosal phase– Epithelial transport defect – inflammations
infections– Brush border hydrolysis defect
congenital/acquired disacharidase deficiency
3. Post-absorptive phase– Enterocyte processing – Abetalipoproteinemia– Lymphocytic obstruction – intestinal
lymphangectasia

Clinical manifestations• History:
Diarrhea/steatorrhoea,Weight loss Symptoms of anaemia
• Diarrhoea – bulky, floating, malodorous stool –difficult to flush.
• Weight loss – may be profound, usually associated with anorexia.
• Anaemia – B12, iron, folate malabsorption.
• Patient may complain of dizziness, dyspnoea and fatigue

Symptom or Sign MechanismWeight loss/malnutrition Anorexia, malabsorption of nutrientsDiarrhea Impaired absorption or secretion of water and electrolytes; colonic fluid
secretion secondary to unabsorbed dihydroxy bile acids and fatty acids
Flatus Bacterial fermentation of unabsorbed carbohydrate
Glossitis, cheilosis, stomatitis Deficiency of iron, vitamin B12, folate, and vitamin A
Abdominal pain Bowel distention or inflammation, pancreatitisBone pain Calcium, vitamin D malabsorption, protein deficiency, osteoporosis
Tetany, paresthesia Calcium and magnesium malabsorptionWeakness Anemia, electrolyte depletion (particularly K+)
Azotemia, hypotension Fluid and electrolyte depletionAmenorrhea, decreased libido Protein depletion, decreased calories, secondary hypopituitarism
Anemia Impaired absorption of iron, folate, vitamin B12
Bleeding Vitamin K malabsorption, hypoprothrombinemia
Night blindness/xerophthalmia Vitamin A malabsorptionPeripheral neuropathy Vitamin B12 and thiamine deficiency
Dermatitis Deficiency of vitamin A, zinc, and essential fatty acid

Signs, symptomsCaloric Weight loss with normal appetite
Fat Pale,voluminous,greasy offensive diarrhea
Protein Edema, muscle atrophy, amenorrhea
carbohydrate Abdominal bloating, flatus, w. diarrhea
B12 Macrocytic anemia
Subacut combined degeneration of sp.cord
Folic acid Macrocytic anemia
Vit B (general) Cheliosis, glossitis,A.stomatitis, Acrodermatitis
Iron Microcytic anemia
Ca & Vit D Osteomalacea (bone pain,pathologic#), Tetany
Vit A Follicular hyperkeratosis, Night blindness
VIt K Bleeding diathesis, Hematoma

Malasportion syndrome
Diagnosis

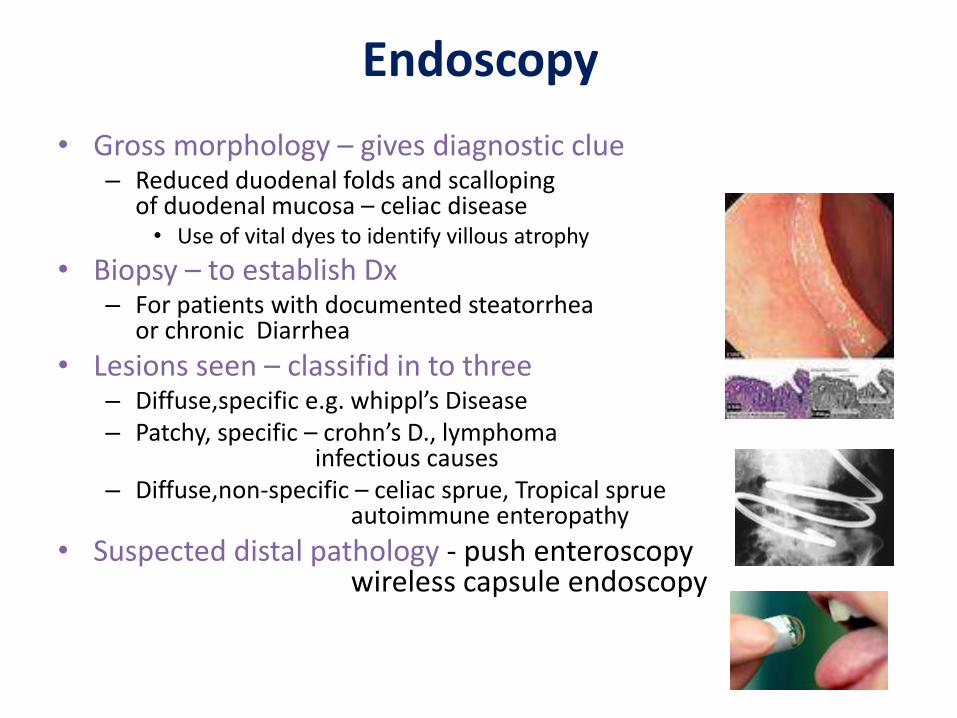
Endoscopy
• Gross morphology – gives diagnostic clue– Reduced duodenal folds and scalloping
of duodenal mucosa – celiac disease• Use of vital dyes to identify villous atrophy
• Biopsy – to establish Dx– For patients with documented steatorrhea
or chronic Diarrhea
• Lesions seen – classifid in to three– Diffuse,specific e.g. whippl’s Disease– Patchy, specific – crohn’s D., lymphoma
infectious causes– Diffuse,non-specific – celiac sprue, Tropical sprue
autoimmune enteropathy
• Suspected distal pathology - push enteroscopywireless capsule endoscopy
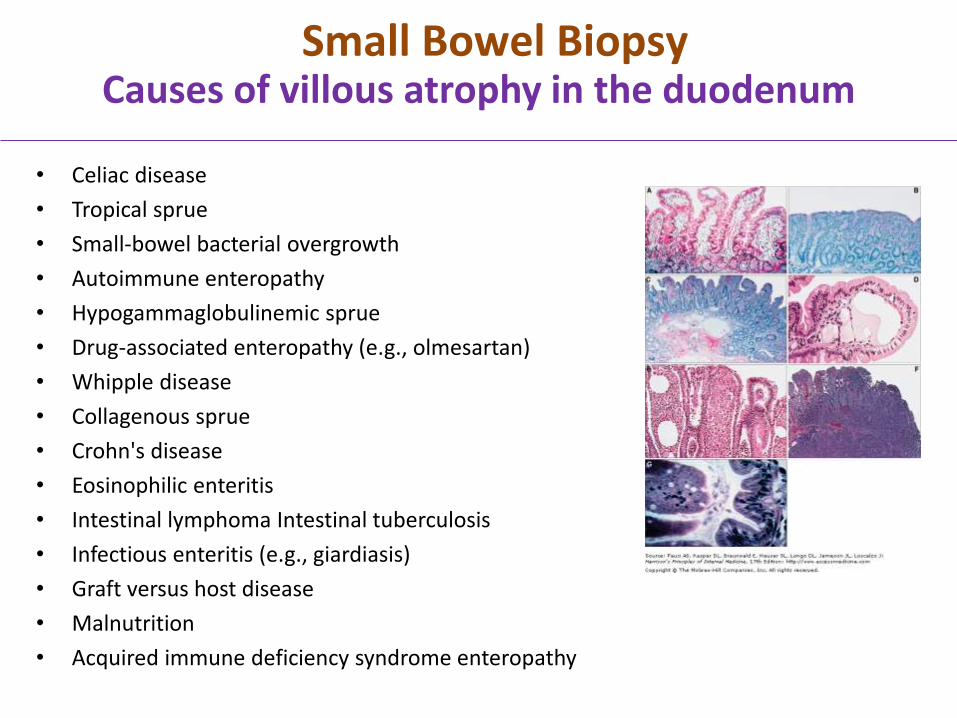
Causes of villous atrophy in the duodenum
• Celiac disease
• Tropical sprue
• Small-bowel bacterial overgrowth
• Autoimmune enteropathy
• Hypogammaglobulinemic sprue
• Drug-associated enteropathy (e.g., olmesartan)
• Whipple disease
• Collagenous sprue
• Crohn's disease
• Eosinophilic enteritis
• Intestinal lymphoma Intestinal tuberculosis
• Infectious enteritis (e.g., giardiasis)
• Graft versus host disease
• Malnutrition
• Acquired immune deficiency syndrome enteropathy
Small Bowel Biopsy
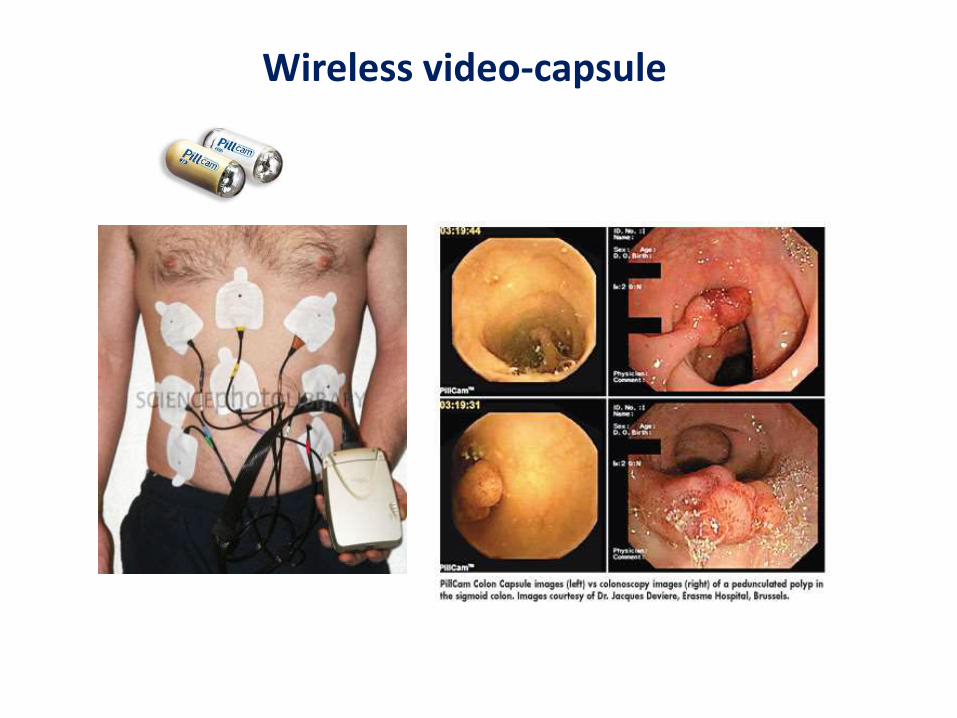
Wireless video-capsule

Barium studies
• Important information about the gross anatomy and morphology of SB– Upper GI series with small
bowell follow through
– Duodenal tube
• double contrast study by passing a tube into proximal SB and injecting barium+ methylcellulose
• Normal study doesn’t exclude small bowell disease

Functional tests for malabsorption(excluding pancreatic causes)
• Steatorrhea
• Shilling test
• Lactose test
• Xylose test
• Hydrogen breath test

Tests for steatorrhea• Quantitative test
– 72hr stool fat collection – gold standard• > 6gm/day – pathologic• P’ts with steatorrhea - >20gm/day• Modest elevation in diarrheal disease
(may not necessarily indicate Malabsorption)
• Qualitative tests– Sudan lll stain
• Detect clinically significant steatorrhea in>90% of cases
– Acid steatocrit – a gravimetric assay• Sensitivity – 100%, specificity – 95% , PPV – 90%
– NIRA (near infra reflectance analysis)• Equally accurate with 72hr stool fat test• Allows simultaneous measurement of fecal fat,
nitrogen, CHO
Schilling test
– To determine the cause of cobalamine(B12) malabsorbtion
– Helps to asses the integrity of gastric, pancreatic and ilealfunctions.
• Abnormal cobalamine absorbtion in:pernicious anemia, ch. Pancreatitis, Achlorohydria, Bacterial overgrowth, ileal dysfunction
– The test • Administering 58Co-labeled cobalamine p.o.
– Cobalamine 1mg i.m. 1 hr after ingestion to saturate hepaticbinding sites
• Collecting urine for 24 hr(dependant on normal renal & bladder function)
• Abnormal - <10% excretion in 24 hrs

D-xylose test• D-xylose
– A Pentose monosacharide absorbed exclusively at the proximal SB
– Used to asses proximal SB mucosal function
• The test
– After overnight fast, 25 gm D-xylose p.o.
– Urine collected for next 5 hrs
– Abnormal test - <4.5 gm excretionshow duodenal / jejunal mucosal D.
– False +ve results:
Renal dysfunction
Inadequate urine sample
Impaired gastric empyting,
Ascites
Drugs(ASA, indometacin, Neomycin)

Steatorrhea and D-Xylose Test Discriminate Maldigestionfrom Malabsorption
MALDIGESTION
(pancreatic insufficiency)
MALABSORPTION
(celiac sprue)
Fecal Fat
D-Xylose
Excretion Normal
Jejunal BiopsyNormal Abnormal “flat”

• Carbohydrate malabsorbtion– Lactose tolerance test
• P.o. 50 gm lactose• Blood glucose at 0,60,120 min.• BG <20mg/l + dev’t of Sxs – diagnostic
• Breath tests hydrogen (also detects bacterial overgrowth)
The hydrogen breath tests and lactose tolerance tests have Sensitivity and Specificity >95% in detecting in lactose intolerancei-
H2 breath test is easier