Making Meaning of “Meaningful Use”- EHR, Medicare and Texas Medicaid Funding Presented by Pamela...
30
Making Meaning of Making Meaning of “Meaningful Use”- “Meaningful Use”- EHR, Medicare and EHR, Medicare and Texas Medicaid Texas Medicaid Funding Funding Presented by Pamela Presented by Pamela McNutt McNutt Sr. VP & CIO Sr. VP & CIO Methodist Health System Methodist Health System 1
-
Upload
clyde-lambert -
Category
Documents
-
view
218 -
download
0
Transcript of Making Meaning of “Meaningful Use”- EHR, Medicare and Texas Medicaid Funding Presented by Pamela...

Making Meaning of Making Meaning of “Meaningful Use”- EHR, “Meaningful Use”- EHR,
Medicare and Texas Medicare and Texas Medicaid FundingMedicaid Funding
Presented by Pamela McNuttPresented by Pamela McNutt
Sr. VP & CIO Sr. VP & CIO
Methodist Health SystemMethodist Health System11

Acute care and critical access hospitalsAcute care and critical access hospitals Includes children’s hospitalsIncludes children’s hospitals Excludes Psychiatric, Rehab, Long Term Care and Cancer Excludes Psychiatric, Rehab, Long Term Care and Cancer
hospitalshospitals Must have at least 10% Medicaid volumeMust have at least 10% Medicaid volume May seek both Medicare or Medicaid incentivesMay seek both Medicare or Medicaid incentives
Eligible Providers Eligible Providers Physicians, pediatricians, dentists, certified nurse midwives Physicians, pediatricians, dentists, certified nurse midwives
nurse practitioners, physician assistants in special rural nurse practitioners, physician assistants in special rural programsprograms
Cannot be hospital based (ie. radiology, lab, ED) Cannot be hospital based (ie. radiology, lab, ED) Must have at least 30% Medicaid volume (20% for Pediatricians)Must have at least 30% Medicaid volume (20% for Pediatricians) Must choose either Medicare or Medicaid but can switch onceMust choose either Medicare or Medicaid but can switch once
Medicaid EHR Incentives – Eligibility
22

Medicaid EHR Incentives – How to Qualify
Possess a Certified Complete EHR system Report quality metrics Meet Meaningful Use by demonstrating functionality in
your EHR systems split into three increasingly difficult stages
First Fiscal Year
Payment Year
2011 2012 2013 2015 2015 +**
2011 Stage 1 Stage 1 Stage 2 Stage 2 Stage 3
2012 Stage 1 Stage 1 Stage 2 Stage 3
2013 Stage 1 Stage 2 Stage 3
2014 Stage 1 Stage 3
2015 +* Stage 3* Avoids payment adjustments only for EPs in the Medicare EHR Incentive Program.** Stage 3 criteria of meaningful use or a subsequent update to the criteria if one is established through rulemaking.
Progression of Meaningful Use Stages by Payment Year
33

Texas Medicaid EHR Incentives – How it is paidTexas Medicaid EHR Incentives – How it is paid
Incentive payments for use of electronic health records Incentive payments for use of electronic health records scaled over a scaled over a three-year periodthree-year period starting in CMS FY 2011 starting in CMS FY 2011
50%, 40%, 10% respectively50%, 40%, 10% respectively Year 1 payment is for adoption, implementation, upgrade Year 1 payment is for adoption, implementation, upgrade
or adoption of Certified EHR technology and or adoption of Certified EHR technology and does notdoes not require achievement of Meaningful Use require achievement of Meaningful Use
Year 2 – 3 requires demonstration of meaningful use of Year 2 – 3 requires demonstration of meaningful use of certified EHR technology and reporting of quality metricscertified EHR technology and reporting of quality metrics
Will be the same as the Medicare in TexasWill be the same as the Medicare in Texas
44

A 500 bed hospital with significant Medicaid and charity care volume showing timing of payments based on achievement of Meaningful Use (AIU = adopting, implementing or upgrading Certified EHRs)
Texas Medicaid EHR Incentives – Example of Payments
Calendar Calendar YearYear
Start in Start in 20112011
MU MU
StageStage
Start in Start in 2012 2012
MU MU StageStage
Start in Start in 20132013
MUMU
StageStage
Start inStart in
20142014
MUMU
StageStage
Start inStart in
20152015
MU MU StageStage
Start inStart in
20162016
MUMU
StageStage
20112011 $2,400,000$2,400,000 AIUAIU
20122012 $1,920,000$1,920,000 11 $2,400,000$2,400,000 AIUAIU
20132013 $ 480,000$ 480,000 22 $ 1,920,000$ 1,920,000 11 $2,400,000$2,400,000 AIUAIU
20142014 --------- --------- 22 $ 480,000$ 480,000 22 $ 1,920,000$ 1,920,000 22 $2,400,000$2,400,000 AIUAIU
20152015 -------------------- 33 ---------------------- 33 $ 490,000$ 490,000 33 $1,920,000$1,920,000 33 $2,400,000$2,400,000 AIUAIU
20162016 -------------------- 33 ---------------------- 33 -------------------------- 33 $ 490,000 $ 490,000 33 $1,920,000 $1,920,000 33 $2,400,000$2,400,000 AIUAIU
20172017 -------------------- 33 ---------------------- 33 -------------------------- 33 -------------------------- 33 $490,000$490,000 33 $1,920,000 $1,920,000 33
20182018 -------------------- 33 ---------------------- 33 -------------------------- 33 -------------------------- 33 ---------------------------- 33 $490,000$490,000 33
TotalTotal $4,800,000$4,800,000 $ 4,800,000$ 4,800,000 $ 4,800,000$ 4,800,000 $4,800,000$4,800,000 $4,800,000$4,800,000 $4,800,000$4,800,000
55

Texas Medicaid EHR Incentives – Physician Payments
“Allowable Costs” has been recently re-defined to be a flat rate rather than an accounting of actual expenses spent on EHR technology. The EHR product’s Certification # will be required for the attestation.
66

Texas Medicaid EHR Incentives – Important DatesTexas Medicaid EHR Incentives – Important Dates
CMS registration for the stimulus programs - January 3, CMS registration for the stimulus programs - January 3, 20112011
Must register for both Medicare and Medicare on CMS siteMust register for both Medicare and Medicare on CMS site Registration does not mean you have to attest to meaningful use Registration does not mean you have to attest to meaningful use
this yearthis year Texas registration and application for Year 1 funds – Texas registration and application for Year 1 funds –
opens February 14opens February 14 Year 1 payments start in May 2011Year 1 payments start in May 2011 Year 2 and 3 will required demonstration of Meaningful Year 2 and 3 will required demonstration of Meaningful
UseUse 90 contiguous days Year 2 90 contiguous days Year 2 Full year in Year 3Full year in Year 3
You can “sit out” a year between payment years then get You can “sit out” a year between payment years then get back in if needed for compliance to MUback in if needed for compliance to MU
77

Medicare Stimulus Medicare Stimulus FundingFunding
Presented by David S. MuntzPresented by David S. Muntz
Sr. VP & CIO Sr. VP & CIO
Baylor Health Care SystemBaylor Health Care System
Attribution: Much of the material presented is available at Attribution: Much of the material presented is available at http://healthit.hhs.gov
88

Medicare EHR Incentives – Medicare EHR Incentives – EligibilityEligibility
Eligible HospitalsEligible Hospitals "Subsection (d) hospitals" in the 50 states or DC that are paid under the Inpatient Prospective Payment System (IPPS) "Subsection (d) hospitals" in the 50 states or DC that are paid under the Inpatient Prospective Payment System (IPPS) Critical Access Hospitals (CAHs) Critical Access Hospitals (CAHs)
• Qualifying CAHs may receive incentive payments for up to four payment years beginning with cost reporting periods that begin in Qualifying CAHs may receive incentive payments for up to four payment years beginning with cost reporting periods that begin in FY 2011. The year with a cost reporting period that begins in FY 2015 is the last payment year for which a qualifying CAH can FY 2011. The year with a cost reporting period that begins in FY 2015 is the last payment year for which a qualifying CAH can receive incentive payments as a meaningful EHR user. receive incentive payments as a meaningful EHR user.
• CAHs can qualify to receive payments from both the Medicare and Medicaid EHR Incentive Programs.CAHs can qualify to receive payments from both the Medicare and Medicaid EHR Incentive Programs. Medicare Advantage (MA-Affiliated) HospitalsMedicare Advantage (MA-Affiliated) Hospitals A payment year is the federal fiscal year (October 1 - September 30) starting in fiscal year 2011 (i.e. October 1, 2010)A payment year is the federal fiscal year (October 1 - September 30) starting in fiscal year 2011 (i.e. October 1, 2010)
Eligible Providers Eligible Providers Doctor of Medicine, Doctor of Osteopathy, Dental surgeon, Doctor of Dental Medicine, Podiatrist, Optometrist, Doctor of Medicine, Doctor of Osteopathy, Dental surgeon, Doctor of Dental Medicine, Podiatrist, Optometrist,
ChiropractorChiropractor Cannot be hospital based (e.g. radiology, lab, ED) Cannot be hospital based (e.g. radiology, lab, ED) Must choose either Medicare or Medicaid but can switch onceMust choose either Medicare or Medicaid but can switch once A payment year is a calendar year starting in 2011A payment year is a calendar year starting in 2011 Additional incentive for eligible professionals who provide services in a Health Professional Shortage Area (HSPA)Additional incentive for eligible professionals who provide services in a Health Professional Shortage Area (HSPA)
BothBoth For the first payment year, any continuous 90-day period within a calendar yearFor the first payment year, any continuous 90-day period within a calendar year For the second, third, and fourth payment year, the calendar yearFor the second, third, and fourth payment year, the calendar year If you skip a year, you cannot make it upIf you skip a year, you cannot make it up To get the maximum payment, you must begin activities in 2012To get the maximum payment, you must begin activities in 2012
99

Medicare EHR Incentives – Medicare EHR Incentives – How to QualifyHow to Qualify
Possess a Certified Complete EHR system. Possess a Certified Complete EHR system. Report quality metrics.Report quality metrics. Meet Meaningful Use by demonstrating Meet Meaningful Use by demonstrating
functionality in your EHR systems split into functionality in your EHR systems split into three increasingly difficult stages.three increasingly difficult stages.
Important! For 2015 and later, Medicare Important! For 2015 and later, Medicare eligible professionals, eligible hospitals, and eligible professionals, eligible hospitals, and CAHs that do not successfully demonstrate CAHs that do not successfully demonstrate meaningful use will have a payment meaningful use will have a payment adjustment in their Medicare reimbursement.adjustment in their Medicare reimbursement.
1010

Progression of Meaningful Use Stages Progression of Meaningful Use Stages by Payment Yearby Payment Year
1111
First Fiscal Year
Payment Year
2011 2012 2013 2015 2015 +**
2011 Stage 1 Stage 1 Stage 2 Stage 2 Stage 3
2012 Stage 1 Stage 1 Stage 2 Stage 3
2013 Stage 1 Stage 2 Stage 3
2014 Stage 1 Stage 3
2015 +* Stage 3* Avoids payment adjustments only for EPs in the Medicare EHR Incentive Program.** Stage 3 criteria of meaningful use or a subsequent update to the criteria if one is established through rulemaking.

Medicare EHR Incentives For Eligible Hospitals – Medicare EHR Incentives For Eligible Hospitals – How it is paid How it is paid
1212
The payment formula for a hospital (payment year) is equal The payment formula for a hospital (payment year) is equal to the product of the following (to the product of the following (get your CFO involvedget your CFO involved):):
1)1) Initial amount – The sum of the base amountInitial amount – The sum of the base amount* specified plus the * specified plus the discharge related** amount for a 12 month period selected by the discharge related** amount for a 12 month period selected by the Secretary with respect to such payment yearSecretary with respect to such payment year
2)2) The Medicare share*** for the hospital for a period selected by The Medicare share*** for the hospital for a period selected by the Secretary with respect to such payment yearthe Secretary with respect to such payment year
3)3) The transition factor**** for the hospital for the payment yearThe transition factor**** for the hospital for the payment year
*The base amount specified in the subparagraph is $2 million
** The discharge related amount is as follows: 1 - 1,149th discharge, $0; 1,150th through the 23,000th discharge, $200; any discharge greater than the 23,000th, $0.
*** The Medicare share specified is equal to a fraction determined by the number of Medicare inpatient bed days and other specific factors
**** The transition factor is determined by multiplying first payment year by: 1 for year 1; .75 for year 2; .5 for year 3; .25 for year 4; and 0 for any following payment year

Medicare EHR Incentives For Eligible Hospitals – Medicare EHR Incentives For Eligible Hospitals – How it is paid How it is paid
1313

CRITICAL ACCESS HOSPITALS CRITICAL ACCESS HOSPITALS (CAHs) – How it is paid(CAHs) – How it is paid
Qualifying CAHs may receive incentive payments for up to four payment Qualifying CAHs may receive incentive payments for up to four payment years beginning with cost reporting periods that begin in FY 2011. The years beginning with cost reporting periods that begin in FY 2011. The year with a cost reporting period that begins in FY 2015 is the last payment year with a cost reporting period that begins in FY 2015 is the last payment year for which a qualifying CAH can receive incentive payments as a year for which a qualifying CAH can receive incentive payments as a meaningful EHR user. meaningful EHR user.
Qualifying CAHs can receive incentive payments for the reasonable costs Qualifying CAHs can receive incentive payments for the reasonable costs incurred for the purchase of depreciable assets like computers and incurred for the purchase of depreciable assets like computers and associated hardware and software, necessary to administer certified EHR associated hardware and software, necessary to administer certified EHR technology, excluding any depreciation and interest expenses associated technology, excluding any depreciation and interest expenses associated with the acquisition.with the acquisition.
A qualifying CAH will receive an incentive payment amount equal to the A qualifying CAH will receive an incentive payment amount equal to the product of its reasonable costs incurred for the purchase of certified EHR product of its reasonable costs incurred for the purchase of certified EHR technology and its Medicare share percentage. The Medicare share technology and its Medicare share percentage. The Medicare share percentage equals the lesser of (1) 100 percent; or (2) the sum of the percentage equals the lesser of (1) 100 percent; or (2) the sum of the Medicare share fraction for the CAH and 20 percentage points.Medicare share fraction for the CAH and 20 percentage points.
1414

Medicare EHR Incentives For Eligible Providers Medicare EHR Incentives For Eligible Providers – How it is paid– How it is paid
1515

Limiting FactorsLimiting Factors A qualifying EP will receive an incentive payment equal to 75 A qualifying EP will receive an incentive payment equal to 75
percent of Medicare allowable charges for covered percent of Medicare allowable charges for covered professional services furnished by the EP in a payment year, professional services furnished by the EP in a payment year, subject to maximum payments.subject to maximum payments.
Physicians who report using an EHR that is also capable of e-Physicians who report using an EHR that is also capable of e-prescribing would be eligible for EHR incentives only, and will prescribing would be eligible for EHR incentives only, and will no longer be eligible for the e-prescribing bonuses. no longer be eligible for the e-prescribing bonuses.
Hospital-based EPs who furnish substantially all their services Hospital-based EPs who furnish substantially all their services in a “hospital setting” are not eligible for incentive payments. in a “hospital setting” are not eligible for incentive payments. Hospital-based EPs are now defined as EPs who furnish 90 Hospital-based EPs are now defined as EPs who furnish 90 percent or more of their allowed services in a hospital percent or more of their allowed services in a hospital inpatient setting, or hospital emergency department.inpatient setting, or hospital emergency department.
1616

Penalties Based on Medicare Penalties Based on Medicare ReimbursementReimbursement
1717
YEARPENALTY -
REDUCTION
2015 1%
2016 2%
2017 & beyond 3%

Useful Information For All in Useful Information For All in Pursuit of Meaning Use Pursuit of Meaning Use
Incentive$Incentive$
1818

Caveat Based on Re-Estimation of Participation Caveat Based on Re-Estimation of Participation and Budget for Incentive Programand Budget for Incentive Program
The government may distribute less money than anticipatedThe government may distribute less money than anticipated CBO estimated that total federal incentive payouts could reach $34 billionCBO estimated that total federal incentive payouts could reach $34 billion Officials have now stated that outlays are likely to range from $14.1 to $27.3 billionOfficials have now stated that outlays are likely to range from $14.1 to $27.3 billion
Budget revisions may be reviewed after evaluating the popularity of the incentive Budget revisions may be reviewed after evaluating the popularity of the incentive payment program.payment program.
Source: Congressional Budget Office year-by-year estimate of the economic effects of the American Recovery and Reinvestment Act of 2009, dated March 2, 2009
Link: http://www.cbo.gov/ftpdocs/100xx/doc10008/03-02-Macro_Effects_of_ARRA.pdf
1919

2020

EHR Incentives – Important DatesEHR Incentives – Important Dates
October 1, 2010 – Reporting year begins for eligible hospitals and CAHs. October 1, 2010 – Reporting year begins for eligible hospitals and CAHs. January 1, 2011 – Reporting year begins for eligible professionals. January 1, 2011 – Reporting year begins for eligible professionals. January 3, 2011 – Registration for the Medicare EHR Incentive Program begins. January 3, 2011 – Registration for the Medicare EHR Incentive Program begins. January 3, 2011 – For Medicaid providers, states may launch their programs if they so January 3, 2011 – For Medicaid providers, states may launch their programs if they so
choose. choose. April 2011 – Attestation for the Medicare EHR Incentive Program begins. April 2011 – Attestation for the Medicare EHR Incentive Program begins. May 2011 – EHR Incentive Payments expected to begin. May 2011 – EHR Incentive Payments expected to begin. July 3, 2011 – Last day for eligible hospitals to begin their 90-day reporting period to July 3, 2011 – Last day for eligible hospitals to begin their 90-day reporting period to
demonstrate meaningful use for the Medicare EHR Incentive Program. demonstrate meaningful use for the Medicare EHR Incentive Program. September 30, 2011 – Last day of the federal fiscal year. Reporting year ends for eligible September 30, 2011 – Last day of the federal fiscal year. Reporting year ends for eligible
hospitals and CAHs. hospitals and CAHs. October 1, 2011 – Last day for eligible professionals to begin their 90-day reporting period October 1, 2011 – Last day for eligible professionals to begin their 90-day reporting period
for calendar year 2011 for the Medicare EHR Incentive Program. for calendar year 2011 for the Medicare EHR Incentive Program. November 30, 2011 – Last day for eligible hospitals and critical access hospitals to register November 30, 2011 – Last day for eligible hospitals and critical access hospitals to register
and attest to receive an Incentive Payment for Federal fiscal year (FY) 2011. and attest to receive an Incentive Payment for Federal fiscal year (FY) 2011. December 31, 2011 – Reporting year ends for eligible professionals. December 31, 2011 – Reporting year ends for eligible professionals. February 29, 2012 – Last day for eligible professionals to register and attest to receive an February 29, 2012 – Last day for eligible professionals to register and attest to receive an
Incentive Payment for calendar year (CY) 2011.Incentive Payment for calendar year (CY) 2011.
2121

http://healthit.hhs.gov
2222

2323

2424

Visit the CHPL: Visit the CHPL: http://onc-chpl.force.com/ehrcert
2525

Regional Extension CentersRegional Extension CentersOverarching objective:Overarching objective: The RECs will support and serve health care providers to help them quickly The RECs will support and serve health care providers to help them quickly
become adept and meaningful users of electronic health records (EHRs). become adept and meaningful users of electronic health records (EHRs). RECs are designed to make sure that primary care clinicians get the help RECs are designed to make sure that primary care clinicians get the help they need to use EHRs. they need to use EHRs.
RECs will:RECs will: Provide training and support services to assist doctors and other providers Provide training and support services to assist doctors and other providers
in adopting EHRs in adopting EHRs Offer information and guidance to help with EHR implementation Offer information and guidance to help with EHR implementation Give technical assistance as needed Give technical assistance as needed The goal of the program is to provide outreach and support services to at The goal of the program is to provide outreach and support services to at
least 100,000 priority primary care providers within two years.least 100,000 priority primary care providers within two years.
Under HITECH, $677 million is allocated to support a nationwide system of Under HITECH, $677 million is allocated to support a nationwide system of RECs that cover every geographic region of the United States to ensure RECs that cover every geographic region of the United States to ensure plenty of support to health care providers in communities across the plenty of support to health care providers in communities across the country. country. There are 4 RECs in Texas.There are 4 RECs in Texas.
2626

Certification Certification ComplicationsComplications
Presented by Pamela McNuttPresented by Pamela McNutt
Sr. VP & CIO Sr. VP & CIO
Methodist Health SystemMethodist Health System
2727

An eligible hospital or provider must possess a Certified An eligible hospital or provider must possess a Certified EHR through:EHR through:
A Certified Complete EHR orA Certified Complete EHR or A combination of Certified Modules orA combination of Certified Modules or Self certification of home grown or non-certified modulesSelf certification of home grown or non-certified modules
You must own all the modules even if not using them for You must own all the modules even if not using them for “meaningful use”“meaningful use”
There are complications with mixing and matching There are complications with mixing and matching systems since most major vendors certified as a systems since most major vendors certified as a Complete EHRComplete EHR
Modules do not inherit the certification of a Complete EHR Modules do not inherit the certification of a Complete EHR
Issues that have arisen with CertificationIssues that have arisen with Certification
2828

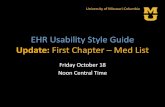
Quality Reporting and Data Repository
Clinical
Documentation
Emergency
Dept
PortalPublic Health
ReportingQuality MetricsCPOE
Primary Vendor A – Certified Complete EHR
Data exchange
CCD record
Clinical
Documentation
Emergency
Dept
PortalPublic Health
ReportingQuality MetricsCPOE
Vendor B – Certified Complete EHR
Data exchange
CCD record
Emergency
Dept
X
X
X X
XX XVendor D – Certified Module
X
Vendor C – Certified Module
The organization would have to “possess” every component listed on this diagram regardless of whether they are used
Illustration of Certification IssuesIllustration of Certification Issues
2929

ONC’s proposed solution to certification issuesONC’s proposed solution to certification issues
Put market pressure on your vendors to go back and Put market pressure on your vendors to go back and get permutations of the Complete EHRs certified as get permutations of the Complete EHRs certified as modulesmodules
Leverage the “loop hole” that you don’t have to Leverage the “loop hole” that you don’t have to implement all modules of a Certified Complete EHRimplement all modules of a Certified Complete EHR
Get vendors to agree to let you load the software but not pay Get vendors to agree to let you load the software but not pay until you begin using ituntil you begin using it
Contract with vendors for the right to use, at any time and at Contract with vendors for the right to use, at any time and at one’s discretion, all the software but not pay until it is used one’s discretion, all the software but not pay until it is used
If “mixing and matching” assure yourself that the If “mixing and matching” assure yourself that the combination:combination:
Has not adversely impacted the calculation of any meaningful Has not adversely impacted the calculation of any meaningful use measuresuse measures
Includes all meaningful use measures Includes all meaningful use measures
3030