Making Everyday Tasks Reachable
13
Making Everyday Tasks Reachable P.O. Box 9089, Saskatoon, Saskatchewan S7K 7E7 • Telephone (306) 956-7768 • Facsimile (306) 242-7941 November 27, 2013 Dear SSOT Member, Please be advised that your SSOT membership renewal is due February 15, 2014. This is the only notice that you will receive. ***For all members renewing as a practicing or restricted license, your completed 2013 Professional Development Plan and Outcomes Form (PDPO) and 2014 PDPO are required to be submitted with your renewal information. PDPOs for 2014 must state two goals and these goals must be updated annually to show progression. Go to www.ssot.sk.ca and look under the Continuing Competency Program page to find the PDPO form in a word format. Update your 2013 goal status and type your new 2014 goals into these forms and print them off to include in your renewal package. **** The Registrar must receive your renewal form (completed in full), PDPO and payment by 5:00 p.m. February 15, 2014 or you will receive an invoice for a late fee of $75.00. If your renewal is not received by 5:00 pm on February 28, 2014, you are not legally permitted to work as an Occupational Therapist. You and your employer will be notified by telephone stating that you are not permitted to work as an Occupational Therapist until your membership has been reinstated. In this package you will receive a copy of your SSOT file on the white sheets. Please refer to these sheets when completing the change only sections of the yellow renewal form. To ensure that your information is correct in the membership directory (e-mailed to you after renewals), make sure that all your information on the white sheets is correct. Please keep the white sheets for your personal records and return the completed yellow renewal form to SSOT. Please advise the Registrar in writing if you do not intend to renew your registration. SSOT grants an individual who is no longer a member a final standing. This final standing is important when you apply for registration in the future with SSOT, or with other regulatory organizations. If you voluntarily resign, your final standing is usually Member in good standing. Should you ignore the renewal package and not notify SSOT that you are not planning to renew your membership, your final standing will be recorded as Member not in good standing. Please send your renewal as soon as possible. Post-dated cheques for February 28, 2014 are acceptable. Cheques will be deposited the week of March 3rd, 2014. Please make cheques payable to the Saskatchewan Society of Occupational Therapists. Submit fees, PDPO and membership renewal forms with signature to: SSOT, Box 9089 Saskatoon, SK. S7K 7E7 Sincerely, Jesse Dziad, SSOT Registrar
Transcript of Making Everyday Tasks Reachable

Making Everyday Tasks Reachable
P.O. Box 9089, Saskatoon, Saskatchewan S7K 7E7 • Telephone (306) 956-7768 • Facsimile (306) 242-7941
November 27, 2013 Dear SSOT Member, Please be advised that your SSOT membership renewal is due February 15, 2014. This is the only notice that you will receive.
***For all members renewing as a practicing or restricted license, your completed 2013 Professional Development Plan and Outcomes Form (PDPO) and 2014 PDPO are required to be submitted with your renewal information. PDPOs for 2014 must state two goals and these goals must be updated annually to show progression. Go to www.ssot.sk.ca and look under the Continuing Competency Program page to find the PDPO form in a word format. Update your 2013 goal status and type your new 2014 goals into these forms and print them off to include in your renewal package. ****
The Registrar must receive your renewal form (completed in full), PDPO and payment by 5:00 p.m. February 15, 2014 or you will receive an invoice for a late fee of $75.00. If your renewal is not received by 5:00 pm on February 28, 2014, you are not legally permitted to work as an Occupational Therapist. You and your employer will be notified by telephone stating that you are not permitted to work as an Occupational Therapist until your membership has been reinstated. In this package you will receive a copy of your SSOT file on the white sheets. Please refer to these sheets when completing the change only sections of the yellow renewal form. To ensure that your information is correct in the membership directory (e-mailed to you after renewals), make sure that all your information on the white sheets is correct. Please keep the white sheets for your personal records and return the completed yellow renewal form to SSOT. Please advise the Registrar in writing if you do not intend to renew your registration. SSOT grants an individual who is no longer a member a final standing. This final standing is important when you apply for registration in the future with SSOT, or with other regulatory organizations. If you voluntarily resign, your final standing is usually Member in good standing. Should you ignore the renewal package and not notify SSOT that you are not planning to renew your membership, your final standing will be recorded as Member not in good standing.
Please send your renewal as soon as possible. Post-dated cheques for February 28, 2014 are acceptable. Cheques will be deposited the week of March 3rd, 2014. Please make cheques payable to the Saskatchewan Society of Occupational Therapists.
Submit fees, PDPO and membership renewal forms with signature to:
SSOT, Box 9089 Saskatoon, SK. S7K 7E7 Sincerely,
Jesse Dziad, SSOT Registrar

Revised April 2013
FEE SCHEDULE
Regular Licences:
New applications must include a non-refundable registration fee of $75.00.
Practicing $423.00 full year or
$159.00 for three months
Non-Practicing $107.00
Restricted License:
New applications must include a non-refundable registration fee of $125.00
Restricted Licence: $423.00 full year or
$159.00 for three months
Other Fees
NSF Cheque $20.00
LMSA (Labour Mobility Support Agreement) $40.00
Regulatory History No Charge
Late Fee $75.00
All funds for new applications must be received by a certified cheque or money order.
All fees payable to SSOT in Canadian Funds.

Making Everyday Tasks Reachable
P.O. Box 9089, Saskatoon, Saskatchewan S7K 7E7 • Telephone (306) 956-7768
Parental/Child Care Leave: Options for membership Option 1 – Practicing Membership
� You may choose to register as a practicing member for the upcoming year. This membership will run from March 1 to the end of February. You will retain all of your rights as a member of SSOT. As stated in the SSOT R#01 Processing New Applications and Granting Licenses Policy 1.5 All occupational therapists providing occupational therapy service (examples are: direct treatment, consultation, telehealth and telephone services) to a Saskatchewan resident must be licensed by SSOT.
� You will pay $423.00 to register and will not have to pay any other fees until it is time to renew your membership for March 1 next year.
� You will be required to participate in the SSOT Continuing Competency Program.
Option 2 – Non-Practicing Membership
� If, at the time of registration (March 1), you are on parental/child care leave and were registered as a practicing member last year, you may choose to register as a non-practicing member.
� You will pay $107.00 to register for this type of membership. � Please Note: You may not work in any capacity as an occupational therapist,
if you are registered as a non-practicing member. � If you return to work prior to end of February the following year, you will be required
to upgrade your membership to that of a practicing therapist and pay the difference from a practicing membership
� You will not be required to participate in the SSOT Continuing Competency Program.
Option 3 – Not Renew
� If you are on parental/child care leave as of March 1 you may choose to not renew your membership, thus letting it expire. Please note that if you choose this option, you must notify the Registrar in writing.
� If you let your membership expire you are unable to work as an occupational therapist in Saskatchewan until you reapply to SSOT.
� When you reapply you will be required to pay the application fee of $75.00 in addition to the fee for the membership category for which you are applying.
� You will not be required to participate in the SSOT Continuing Competency Program.
*** Remember you MUST be registered with SSOT if you are practicing Occupational Therapy in Saskatchewan***

November 2013
Dear SSOT Member,
The third annual audit was successfully completed this October. Members’ submissions have
progressively demonstrated improvement over the last three years in both SMART goal
comprehension as well as in the quality of evidence provided. The goal of the Continuing
Competency Program is to ensure SSOT members are meeting essential professional
competencies and engaging in professional development and ultimately improving the quality of
their practice. Therefore, it is reasonable that the content of the Professional Development Plan
and Outcomes advances to include the impact this process has on professional practice. While
you are completing the CCP requirements this year, begin to think critically about the
impact these goals and outcomes have on your practice and allow this to be reflected in
your Professional Development Plan and Outcomes.
As in the past, this year’s audit reflected that it is valuable to review the “SMART Goal Setting”
and the “CCP-What You Need to Know” power-point presentations on the SSOT website under
Continuing Competency Program. This will help to ensure SMART goals include the required
details and ensure quality evidence is provided.
All members who are registered as practicing or restricted license SSOT members despite
leave of absences or maternity/paternity leave are required to participate in the Continuing
Competency Program as part of the regular renewal process.
The SSOT Non-Clinical Self Assessment Tool and SSOT Clinical Assessment Tool were
adopted by SSOT in 2012. These documents can be found on the SSOT website under
Continuing Competency Program and are to be used as the foundation for developing the
Professional Development Plan and Outcomes. Therapists that have ANY amount of direct
contact with a client during the membership year are required to complete the Clinical
Assessment Tool.
Please be sure to review the Essential Competencies of Practice for Occupational Therapists in
Canada 3rd edition and complete the 2013 updated versions of either the Non-Clinical or the
Clinical Self Assessment Tool to guide your 2014 Professional Development Plan and
Outcomes. Please use only the new, updated PDPO format found on the SSOT website
under Continuing Competency Program.
If you have any questions please contact Natalie Bishop, SSOT Member at Large for
Professional Practice at [email protected] or Coralie Lennea, SSOT Executive Director at
Sincerely,
Natalie Bishop, SSOT Member at Large for Professional Practice

Name: __________________________________________
Renewal Application Form
Some sections of this form are for changes only, for these areas please refer to the white form which shows your current SSOT information
Please ensure that you use appropriate codes where an (*) is present.
YOU ARE REQUIRED TO NOTIFY THE REGISTRAR OF ANY CHANGES OR IT WILL AFFECT YOUR
STANDING.
PERSONAL DATA: Only put in CHANGES to personal data
Name: Mr. Mrs. Ms. Miss Last First Maiden (Please include confirmation of change of name)
If you were employed or educated under a different name, please list:
Home Address: City Province Country Postal Code
Home: Phone Number: ( ) Fax: ( ) e-mail:
Business: Ph. Number: ( ) Fax: ( ) e-mail:
Date of Birth: (d / m/ y) Gender: *Employment Status: Age Category: □ 20-24 □ 25-29 □ 30-34 □ 35-39 □ 40-44 □ 45-49 □ 50-54 □ 55-59 □ 60+
MEMBERSHIP DATA: Complete membership data section in full
Membership Category: □ Practicing □ Temporary (3 month term) □ Restricted License □ Life □ Student □ Non-Practicing (1 2 3) Have you ever been a previous member or student member of SSOT? Fees submitted (Please refer to enclosed Fee Schedule): Cheque #
POST-SECONDARY EDUCATION
Please state if you have completed any additional education in the last year
1. Basic Education Institution attended (for OT degree if applicable)
Name *ESIS Code
Address
City Province Country Postal Code
Year of Graduation *Degree or Diploma Attained
City Province Country Postal Code
Year of Graduation *Degree or Diploma Attained
Do you currently hold a membership with CAOT?
Do you currently hold a membership with any other professional association? If so, please list.
March 1, 2014 – February 28, 2015
P.O. Box 9089, Saskatoon, Saskatchewan S7K 7E7 • Telephone (306) 956-7768

EMPLOYMENT/EDUCATION/VOLUNTEER HISTORY
Dates
From
To
Employment Position/Education
Course/Volunteer Activity
Employer/Educational
Institution/Volunteer Organization
Hours
/Week
Total Hours
for year
01/03/2013
28/02/2014
Employment Position
Employer
Education Course Educational Institution
Volunteer Activity Volunteer Organization
01/03/2012
28/02/2013
Employment Position Employer
Education Course Educational Institution
Volunteer Activity Volunteer Organization
01/03/2011
28/02/2012
Employment Position Employer
Education Course Educational Institution
Volunteer Activity Volunteer Organization
01/03/2010
28/02/2011
Employment Position
Employer
Education Course Educational Institution
Volunteer Activity Volunteer Organization
01/03/2009
29/02/2010
Employment Position Employer
Education Course Educational Institution
Volunteer Activity Volunteer Organization
Please review the Practice Hours Policy on our website www.ssot.sk.ca under Information for Members prior to completing this page.
• For this last year, 01/03/2013 to 29/02/2014, please complete the table in full.
• Please refer to your work history on the white copy of the SSOT membership form. If there are any errors for the years 01/03/2009 to 28/02/2014, please make these corrections in the table on this page.
• Do not modify the date categories provided when recording practice hours.
• Remember that only actual worked hours are counted toward the practice hours to maintain a Practicing
License. Any type of leave of absence (vacation, maternity, illness, disability, etc.) cannot be included as practice hours.
• For those working in private practice settings, ensure that all actual worked hours are recorded not just billable
hours.

EMPLOYER DATA: Only put in changes to employer data
EMPLOYER PROFILE – PRIMARY EMPLOYER
Employer: *Employer Type
Employer Address City Prov Country Postal Code
Immediate Manager/Supervisor: Phone: ( ) Fax:( )
E-mail: Saskatchewan Health District (if applicable):
FACILITY NAME: *Postal Code same as Service Delivery Site (Yes / No / NA)
Address:
City Prov Country Postal Code
Phone No.: ( ) Fax No.: ( )
E-mail: Proposed Starting Date:
If you are doing any amount of private practice OT work (in the Primary, Secondary or Other Employer category)
you must provide SSOT with the name and contact number of your designate trustee (please go to page 7 for a
definition):
Name: ________________________________________________ Phone Number: ____________________
EMPLOYER PROFILE – SECONDARY EMPLOYER
Employer: *Employer Type
Employer Address City Prov Country Postal Code
Immediate Manager/Supervisor: Contact Phone: ( ) Fax:( )
E-mail: Saskatchewan Health District (if applicable):
FACILITY NAME: *Postal Code same as Service Delivery Site (Yes / No / NA)
Address: City Prov Country Postal Code
Phone No.: ( ) Fax No.: ( )
E-mail: Proposed Starting Date:
EMPLOYER PROFILE – OTHER EMPLOYER
Employer: *Employer Type
Employer Address City Prov Country Postal Code
Immediate Manager/Supervisor: Contact Phone: ( ) Fax:( )
E-mail: Saskatchewan Health District (if applicable):
FACILITY NAME: *Postal Code same as Service Delivery Site (Yes / No / NA)
Address: City Prov Country Postal Code
Phone No.: ( ) Fax No.: ( )
E-mail: Proposed Starting Date:
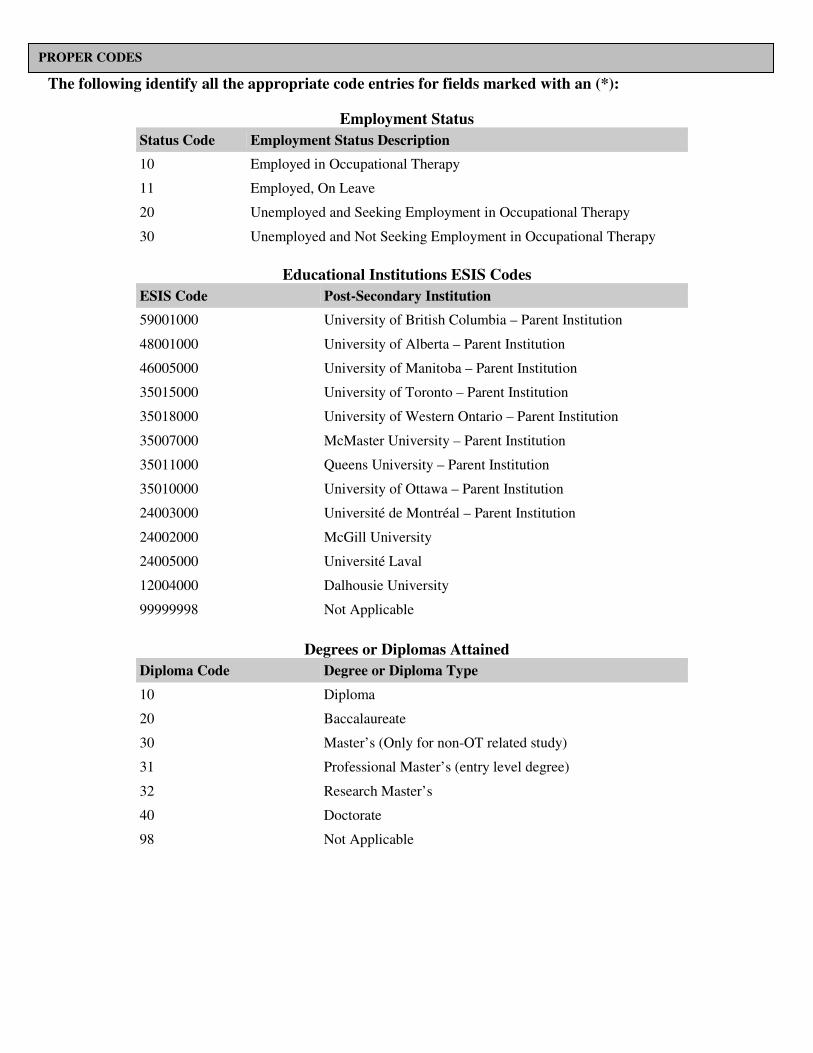
The following identify all the appropriate code entries for fields marked with an (*):
Employment Status
Status Code Employment Status Description
10 Employed in Occupational Therapy
11 Employed, On Leave
20 Unemployed and Seeking Employment in Occupational Therapy
30 Unemployed and Not Seeking Employment in Occupational Therapy
Educational Institutions ESIS Codes
ESIS Code Post-Secondary Institution
59001000 University of British Columbia – Parent Institution
48001000 University of Alberta – Parent Institution
46005000 University of Manitoba – Parent Institution
35015000 University of Toronto – Parent Institution
35018000 University of Western Ontario – Parent Institution
35007000 McMaster University – Parent Institution
35011000 Queens University – Parent Institution
35010000 University of Ottawa – Parent Institution
24003000 Université de Montréal – Parent Institution
24002000 McGill University
24005000 Université Laval
12004000 Dalhousie University
99999998 Not Applicable
Degrees or Diplomas Attained
Diploma Code Degree or Diploma Type
10 Diploma
20 Baccalaureate
30 Master’s (Only for non-OT related study)
31 Professional Master’s (entry level degree)
32 Research Master’s
40 Doctorate
98 Not Applicable
PROPER CODES

Fields of Study
Field Code Field Name
010 General Rehabilitation Science
020 Health Administration/Management
030 Public Administration
040 Public Health
050 Kinesiology and Exercise Science
060 Gerontology
070 Psychology
080 Health Professions and Related Clinical Sciences
090 Biological and Biomedical Sciences and Physical Sciences
100 Social Sciences, Arts and Humanities
110 Education
120 Law
130 Business, Management, Marketing and Related
140 Other Field of Study
998 Not Applicable
Employer Types
Employer Code Employer Description
010 General Hospital
020 Rehabilitation Hospital/Facility
030 Mental Health Hospital/Facility
040 Residential Care Facility
050 Assisted Living Residence
060 Community Health Centre
070 Visiting Agency/Business
080 Group Professional Practice/Clinic
090 Solo Professional Practice/Clinic
100 Post-Secondary Educational Institution
110 School or School Board
120 Association/Government/Para-Governmental
130 Industry, Manufacturing and Commercial
140 Other
998 Not Applicable
Postal Code Same as Service Delivery Site
Yes – Postal code reflects a site where service is delivered. No – Postal code does not reflect a site where service is delivered. The postal code provided refers to an employer or business office that is different than the site where service is delivered.

PRACTICE PROFILE – PRIMARY PRACTICE Only put in changes to practice profile Job Title ___________________________________________ Province _______________________________________________
Hours ___________________________ hours per week Country ________________________________________________
STATUS: CATEGORY – Must check ONE only. .................Permanent .................Temporary .................Casual .................Self Employed .................Not Applicable
STATUS: HOURS – Must check ONE only. .................Full Time .................Part Time ................Not Applicable ROLE: Please check the category that best represent the MAIN component of your work ................Manager ................Professional Leader/Coordinator ................Direct Service Provider ................Educator ................Researcher ................Other(specify) __________________________________ ................Not Applicable SYSTEM IN WHICH YOU WORK: Please check the ONE that BEST describes the area of the area of practice ...............Mental Health ...............Neurological System ............... Musculoskeletal System ...............Cardiovascular and Respiratory System ............... Digestive/Metabolic/Endocrine System ...............General Physical Health ............... Vocational Rehabilitation ...............Palliative Care ...............Client Service Management ...............Medical/Legal Related Client Service Management ...............Service Administrator ...............Teaching ............... Other Areas of Direct Service(specify) _____________ ...............Health Promotion & Wellness ...............Research ...............Other(specify)_____________________________________________________________________________ ...............Not Applicable FUNDING SOURCES FOR THIS POSITION: Please check the major source of funding for this position (Must check ONE only) ...............Public/Government ...............Private Sector or Individual Client(s) ...............Public/Private Mix ............... Other (Specify) _____________________________________ ...............Not Applicable CLIENT AGE RANGE: Please Check the age category that BEST represents the MAJORITY of your clients (Must check ONE only) ...............Preschool Age ............... School Age ............... Mixed Pediatrics ............... Adults ............... Seniors ............... Mixed Adults ............... All Ages ............... Not Applicable ............... Other
PRACTICE PROFILE – SECONDARY PRACTICE
Job Title ___________________________________________ Province_________________________________________
Hours __________________ hours per week Country _________________________________________
STATUS: CATEGORY – Must check ONE only. .................Permanent .................Temporary .................Casual .................Self Employed .................Not Applicable STATUS: HOURS – Must check ONE only. .................Full Time .................Part Time ................Not Collected ................Not Applicable ROLE: Please check the category that best represent the MAIN component of your work ................Manager ................Professional Leader/Coordinator ................Direct Service Provider ................Educator ................Researcher ................Other(specify) __________________________________ ................Not Applicable SYSTEM IN WHICH YOU WORK: Please check the ONE that BEST describes the area of the area of practice ...............Mental Health ...............Neurological System ............... Musculoskeletal System ...............Cardiovascular and Respiratory System ............... Digestive/Metabolic/Endocrine System ...............General Physical Health ............... Vocational Rehabilitation ...............Palliative Care ...............Client Service Management ...............Medical/Legal Related Client Service Management ...............Service Administrator ...............Teaching ............... Other Areas of Direct Service(specify) _____________ ...............Health Promotion & Wellness ...............Research ...............Other(specify)_____________________________________________________________________________ ...............Not Applicable FUNDING SOURCES FOR THIS POSITION: Please check the major source of funding for this position (Must check ONE only) ...............Public/Government ...............Private Sector or Individual Client(s) ...............Public/Private Mix ...............Other (Specify) _____________________________________ ...............Not Applicable CLIENT AGE RANGE: Please Check the age category that BEST represents the MAJORITY of your clients (Must check ONE only) ...............Preschool Age ............... School Age ............... Mixed Pediatrics ............... Adults ............... Seniors ............... Mixed Adults ............... All Ages ............... Not Applicable ............... Other

PRACTICE PROFILE – OTHER PRACTICE
Job Title ___________________________________________ Province_________________________________________
Hours __________________ hours per week Country _________________________________________
STATUS: CATEGORY – Must check ONE only. .................Permanent .................Temporary .................Casual .................Self Employed .................Not Applicable STATUS: HOURS – Must check ONE only. .................Full Time .................Part Time ................Not Collected ................Not Applicable ROLE: Please check the category that best represent the MAIN component of your work ................Manager ................Professional Leader/Coordinator ................Direct Service Provider ................Educator ................Researcher ................Other(specify) __________________________________ ................Not Applicable SYSTEM IN WHICH YOU WORK: Please check the ONE that BEST describes the area of the area of practice ...............Mental Health ...............Neurological System ............... Musculoskeletal System ...............Cardiovascular and Respiratory System ............... Digestive/Metabolic/Endocrine System ...............General Physical Health ............... Vocational Rehabilitation ...............Palliative Care ...............Client Service Management ...............Medical/Legal Related Client Service Management ...............Service Administrator ...............Teaching ............... Other Areas of Direct Service(specify) _____________ ...............Health Promotion & Wellness ...............Research ...............Other(specify)_____________________________________________________________________________ ...............Not Applicable FUNDING SOURCES FOR THIS POSITION: Please check the major source of funding for this position (Must check ONE only) ...............Public/Government ...............Private Sector or Individual Client(s) ...............Public/Private Mix ...............Other (Specify) _____________________________________ ...............Not Applicable CLIENT AGE RANGE: Please Check the age category that BEST represents the MAJORITY of your clients (Must check ONE only) ...............Preschool Age ............... School Age ............... Mixed Pediatrics ............... Adults ............... Seniors ............... Mixed Adults ............... All Ages ............... Not Applicable ............... Other
PRACTICE HOURS POLICY
Please see G#10 – Practice Hour Policy on the website under Information for Members (www.ssot.sk.ca) for which hours can be counted on your renewal.
Definitions
Designate Trustee – an eligible trustee who is willing to take on the responsibility for care and security of the personal health information of another trustee, in case on an unplanned cessation of practice.

ADDITIONAL INFORMATION Complete In Full
1. Do you wish to have your name included on the list of Private Practice OT’s Yes No
that is released to the public?
Please indicate the practice areas you would like included on the list:
______________________________________________________________________________
Please indicate the contact information you would like on the list if it is different from your primary work
information:
______________________________________________________________________________
2. For regular SSOT e-mails do you prefer: � Work Address � Home Address
3. Do you wish to volunteer in SSOT activities (e.g. committees, public relations, Council)? Yes No
List areas of interest: _____________________________________________________
4. In the previous year, have you been previously registered/licensed to practice as an OT
in any other province/country? Yes No
If so, where? ___________________________________________________________________
5. Are you currently registered/licensed to practice as an OT in any other province or country? Yes No
If so, list the current provinces/countries of registration? ________________________________
______________________________________________________________________________
6. Have you been refused registration in any OT regulatory body? Yes No
7. Have you had a find of, or are currently facing a proceeding for, professional misconduct,
incompetence or incapacity in any jurisdiction? Yes No
8. Have you been found guilty of a criminal offense or an offense related to the
regulation of practice of OT? Yes No
9. Have you ever been suspended, disqualified, censured, reprimanded or had disciplinary
action instituted against you as a member of the profession? Yes No
10. Have you ever been denied any membership, license or permit by any profession
or governmental authority, the procurement of which required proof of good
moral character? Yes No
11. Have you ever been suspended or expelled from any post-secondary educational institution? Yes No
12. Do you currently have 5 million personal liability/malpractice insurance? Yes No
13. Have you successfully completed the CAOT National Certification examination? Yes No
14. Are you an approved Worker’s Compensation Board (WCB) provider? Yes No
15. Self-Declaration (optional)
Are you part of the First Nations (Status or Non-Status), Metis or Inuit peoples? Yes No

16. Self-Declaration (optional)
Do you consent to the sharing of this information with others who declare for the
purpose of developing a network? Yes No
DECLARATION I am aware that SSOT has formally adopted the Essential Competencies of Practice for Occupational Therapists in Canada –
3rd
Edition as its definition of the standards of competency for its members and I have incorporated them into my practice of
Occupational Therapy.
I hereby certify that the statements made by me in this application are complete and correct to the best of my knowledge and
belief. I understand that a false or misleading statement may disqualify me from registration or may cause from revocation or
any registration which may be granted me.
Signature _____________________________________________ Date _________________________________________________
ADMINISTRATION USE ONLY
Date Application Received: _______________________ Date Renewal Package mailed: November 27, 2013
Date Fees received: ______________________________
Employer contacted if renewal not received by February 28, 2013: ____________________________________ Date PDPO received: _________________________ E-mail confirmation of receipt of complete renewal form and PDPO: ____________________