
Mais le SIDA n’existe plus quand même..?!” [But AIDS has … · Lumbar puncture, even if no...
55
Klik om de ondertitelstijl van het model te bewerken “Mais le SIDA n’existe plus quand même..?!” [But AIDS has disappeared, not so…?!] Filip Moerman CHR Citadelle Lüttich, Belgium Institute of Tropical Medicine, Antwerp EUREGIO 2018 (Aachen, Germany)
Transcript of Mais le SIDA n’existe plus quand même..?!” [But AIDS has … · Lumbar puncture, even if no...

Klik om de ondertitelstijl van het model te bewerken
“Mais le SIDA n’existe plus quand même..?!”
[But AIDS has disappeared, not so…?!]
Filip MoermanCHR Citadelle Lüttich, BelgiumInstitute of Tropical Medicine, Antwerp
EUREGIO 2018 (Aachen, Germany)

Overview of the presentation 13 cases of clinical AIDS last 18 months in CHR
Liège! (9 Afr, 4 Europeans) So we may not forget the clinical spectrum of
AIDS (cfr in Africa still very prevalent) We’ll present 2 clinical cases of this year,
emphasizing on the Se / PPV (Prevalence!) of symptoms, AND a short summary on diagnosis and treatment of other AIDS-def. illnesses.

Renaud, 27yrs old (nurse). Never been tested, no relevant med history Emergencies June 2018 with longstanding
headache, loss of apetite and fever on and off Mother says: “becomes slow and bizarre and
can no longer concentrate” CLIN/LAB: cachectic (BMI=16), weak, pale,
tachycardia, tachypnoe, photophobia, HIV+ [CD4]=20/mm³, (SGOT/PT)↑, Hb = 8,2 g/dl with a HIV-1 VL of nearly 6 log

WHAT IS YOUR (D) DIAGNOSIS?

Cryptococcal meningitis Most common life-threatening fungal infection in
PLWHA CD4 < 50 Insidious onset: fever + headache (Se↑, NPV↑) Confusion, behavioral change (mother!) Papilledema,+/- neck stiffness, seizures, cranial
nerve paralysis
Lumbar puncture, even if no meningeal signs
Even when papiloedema, LP does not carry excessive risk of cerebral herniation

Diagnosis (clinical suspicion, Pre- test-Prob)
Microscopy, Culture, Antigen, PCR Se of India-ink-staining in CSF < 86% (CAVE low
fungal burden) CSF culture = gold standard (but takes 7 days!) (!): detection of Cryptococcal Ag in CSF and serum
both have high Se & Spe and are fast techniques. Additionally PCR
Usually several approaches result in quick diagnosis.

Cryptococcal meningitis
India ink preparation (85% sens.) : Cryptococcus neoformans


Treatment of cryptococcal meningitis
Induction phase Amphotericin B lip 3 mg/kg/24h, IV, 2 weeks + Flucytosine 25 mg/kg q6h p.o. for 2 weeks at least, followed byà Prolongation phase Fluconazole 800 mg 8-10
weeks, then 200 mg / day (2° prophyl)
Fungicidal rate decline about 0,4 log/day
Repeated LP as part of the therapyUp to 30 cc daily until ICP< 20 cm or 50% initial
P.

CAVE: wait with HAART!!Very intensive CRYPTO-IRIS

Smilnak, et al. Novel treatment of cryptococcal
meningitis via neurapheresis therapy JID 2018
designed as adjunctive treatment to standard care
The Journal of Infectious Diseases , Volume 218, Issue 7, 24 August 2018, Pages 1147–1154,
https://doi.org/10.1093/infdis/jiy286

Would result in a 5 log reduction of yeasts in 24h!

Follow-up of treatment success
Clinical
India Ink: capsula disappearing
Cryptococcal Ag: only useful when titers! And still…low evaluation power
Culture (probably ‘better’ than Ag)
How is Renaud? Hospitalized from June 10th – September 28th During the course of his crypto-treatment he
developped MAC characterised by fever+++ (possibly as IRIS since prompt VL-decrease to VL<20 copies/ml after 10 weeks!)
Developed severe AKI as well, now improved He is ‘relatively’ well now and followed-up
fortnightly.

Jane, 38 yrs old, Ivory Coast Slow loss of weight with diarrea Progressive increase of headache and apathy Vesperal fevers H. zoster recidivans Difficulties in walking with right hemiparesis Progressive dysphagia that forced Jane finally
to the hospital

Cerebral toxoplasmosis

Cerebral Toxo
Cerebral toxoplasmosisCause : T. Gondii (oocysts in cat stools and undercooked meat) – invasion of lungs, heart, retinitis, brainSYMPTOMS: Fever: 50% Headache: 50-70% Hemiparesis: 50% Seizures: 30% NO symptoms (!): MRI as screening in AIDS-
analyses!Diagnosis : IgG (IgG- = NPV↑), scan, MRI more Se than CT (CSF normal, exclude TB-meningitis, Lymphoma, Crypto, PMLE)à Response to empirical therapy in poor settingsà Go to brain biopsy if no improvement (TB-abcess of
brain!)

Cerebral toxoplasmosisTREATMENT: (steroids NOT systematically, but often later)
First choice: Sulphadiazine + pyrimethamine* 6w*inhibit folates synthesis
à hematologic toxicity (+ Sulphadiazine may cause crystaluria: hydration!)
+ Folinic acid
Cheap
Monitor Kidney
COTRIMOXAZOLE TMP/SMX 10/50 mg/kg daily divided over 2 dosesFor 4 weeks (patients 50 kg 3 tablets of TMP80/SMX400 twice daily)Followed by maintenance therapy

AFRICAN setting: If referral difficult
Focal neurological signs + fever + headache and CSF normal therapeutic trial with cotrimoxazole Response in 1-2 week if it is toxo
Altern treatments include: dara + Azithro 1000 OR ‘dara+dala’
Treat intracranial hypertension (prednisolone 40 mg 4x daily) and seizures (phenytoine 100 mg 2-3 daily) if necessary

Jane…(0 CD4)Jane denied her diagnosis established in Africa in 1998, she did not reveal it to her husband and 2 children. On admission, following active diagnoses were withheld: Cerebral Toxoplasmosis, H. zoster+++, slim disease with µ-sporidium, candida oesophagitis, CxCA in situ, PMLE (JC virus), probable AIDS-dementiaShe died of multipathology, drug-related toxicity and severe IRIS …

Diarrhea 50% of patients will develop diarrhea in the
course of their HIV disease Significant effect on quality of life
HAART / Paromomycin empirical to consider
In 50% of patients we can not identify a cause

Causes of diarrhea Infectious agents Other causes Bacteria
ProtozoaToxin inducedMycobacteriaHelminthicFungal Viral
AIDS enteropathyKaposi’s sarcomaLymphoma of the gutMedications

Isospora belli (‘cryptoisosporiasis’)
Direct stool exam Large oocysts (20-30
µm) R/ Cotri 1DS x 4/day
for 10 days Followed by 1 DS x
2/day for 3 weeks Secondary prophylaxis
with cotrimoxazole 1DS

Microsporidiosis Modified
trichrome stain Small spores: 1-3
µm: survive for years outs host
Usually faeco-oral
Albendazole 400 mg Bid 2-4w (relapse) HAART !!! (response in 1-15w, average 6w)

Case: chronic diarrhea Patient presents
with respiratory symptoms
Skin lesions ~ creeping eruption
Diarrhea, HIV+
Strongyloides hyperinfection syndromeR/ Ivermectin (Stromectol®) 200 µg/kg (+ repeat in 1 week)Poor setting: Albendazole 2 x 400 mg dd

PCP (Pneumocystis Carinii = Pneumocystis Jiroveci)
Symptoms: Sub-acute onset Dry cough Fever, first low & vesperal, later continuously DYSPNEA (on exertion): parabolic
deterioration at one point with desaturation. At this point, Steroids to add
Cfr LDH rather high NPV! Less frequent in Afr!

PCP, diagnosis ‘Typical’ chest X-ray – CT:
Bilateral interstitial infiltrates beginning in the perihilar regions/ ground glass appearance/ Butterfly wings
25% normal at initial presentation
Diagnosis mostly by clinical presentation
and chest X-ray/CT/BAL + PCR

Typical CT-scan

Bronchoalveolar ‘washing’

Treatment of PCP TMP-SMX: 20 mg/kg/day SMX and TMP 5 mg/kg/day
divided over 4 doses for 21 days, initially mostly IV (4 x 4 amp of Eusaprim IV/day)
In case of hypoxemia *(P02<70mmHg): Prednisone before Ǿ
40 mg 2x/day for 5 days40 mg 1x/day for 5 days20 mg for 11 days*Decomposition of many dead parasites aggravates inflammation worsening of hypoxemia
ALTERNATIVE TREATMENT: Atovaquone or DDS+TMP or Clinda+PQ
à Improvement in 7-10 daysà Secondary prophylaxis 1DS TMP/SMX
Average 4x3 tablets of CTX F per day

CMV retinitis (low CD4, CMV viraemia, Leucopenia, vision
disturbances)

Cerebral lymphoma

But don’t forget simpler diagnoses

S. Pneumoniae Pneumonia

Streptococcus pneumoniae Often positive blood
cultures Acutely ill, high
fever Productive cough Pleuritic type chest
pain Gram stain + culture
75% diagnostic
Vaccinate your patients!

Nocardiosis Rare in immune
competent DD TB Gram stain + AFB

Histoplasmosis (published)

Deep fungal infection Rare Histoplasmosis, coccidiomycosis, aspergillosis,
cryptococcosis, Penicillium Marneffei (OI frequent in Thailand)
Diagnosis: blood and sputum culture, BAwashing
Amphotericin B during 14 days, followed by itraconazole 200 mg twice daily (10 weeks), followed by secondary prophylaxis with itraconazole once daily

ORAL HAIRY LEUKOPLAKIA Vertical folds Non-removable Not painful
No treatment (HAART)
Sign of immune suppression
WHO stage III
Caused by EBV replication in the epithelium of the surface of the tongue

Severe forms of OHL
Disturbance of taste
Difficulties to eat Regression is seen
when treated with Acyclovir and HAART

Ulcers of unkown origin

Solitary big ulcers
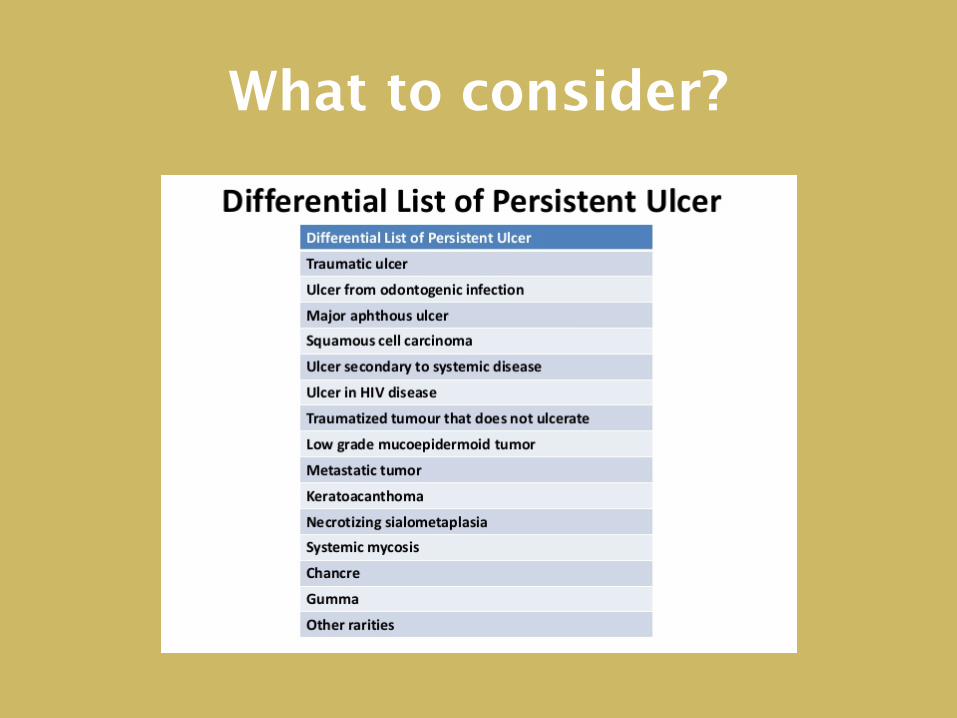
What to consider?

Clinical approach

Histoplasma

Necrotising gingivitis Inflammation of the
gums Extensive and
necrotic Tooth loss
Anaerobic infection R/ metronidazole
3x500 mg

Kaposi’s Sarcoma

Solitary big ulcers CMV Deep mycosis: histoplasma, cryptococcosis
In single big ulcers:Before prednisone 40 mg daily
èTrial with fluconazole or itraconazoleèRule out treatables (clinical approach)èDon’t forget SYPHILIS !

TB meningitis 10% of AIDS patients who present with TB will
show involvement of the meninges. Symptoms: sub-acute meningitisü Gradual onset of headacheü Low grade feverü Neck stiffness
Cranial nerve palsies Seizures, focal neurological deficits, altered consciousness

Diagnosis of TB meningitis: difficult!
IMAGING: MRI/CT may show leptomeningeal enhancement, hydrocephalus, tuberculoma, abcess
LAB: hypoNa+, QFR (CAVE AIDS), VS +/- CSF microbiology: smear, culture, PCR
(multiple [>3] samples required to increase Se) CSF analysis: lympho pleio preceded by PMN
predominance in early infection, high proteinorachia, low glucose: consider when glu low, prot high and negative bact cultures AND ‘pre-test’ high (HIV, Afr origin, Epidemiol context, …)

TB brain abcess (DD: biopsy!)


Tuberculous granuloma of the brain

Treatment of TB meningitis TB treatment according to protocol
(INH+PZA+RIF+EMB), prolonged: 2 + 7-10 months.
Furthermore, Prednisolone 1 mg/kg for 2-4 weeks in case of severe neurological signs (always if IRIS)*
Timing to introduction of HAART depends on CD4 count; if possible (> 100 CD4/mm³), wait until end of initial phase.
Steroids in TB-HIV: pericarditis, meningitis *early mortality decrease: Marx G, et al. Tuberc Res Treat 2014


















