Main points to be covered Rate ratios Relationship between the type of ratio measure of association...
47
Main points to be covered • Rate ratios • Relationship between the type of ratio measure of association and study design • How the odds ratio estimates other ratio measures depending on the type of sampling in a case-control study • Strengths and weaknesses of case- control studies
-
date post
21-Dec-2015 -
Category
Documents
-
view
219 -
download
3
Transcript of Main points to be covered Rate ratios Relationship between the type of ratio measure of association...

Main points to be covered
• Rate ratios
• Relationship between the type of ratio measure of association and study design
• How the odds ratio estimates other ratio measures depending on the type of sampling in a case-control study
• Strengths and weaknesses of case-control studies

Comparison of two person-time rates with a ratio
• Ratio of two person-time rates– NB: denominators of two person-time rates must be in the same units
• Rate NSAID use = 12.02 per 1000 person-years• Rate for non use = 11.86 per 1000 person-years
Rate ratio = 1.01
• Described as “rate ratio” in the articleRay, Lancet, 2002

Rate Ratio described as Relative Risk
• CA mortality rate ratio by BMI group:
841.6 per 100,000 person-years (BMI 40+) 578.3 per 100,000 person-years (BMI < 40) Rate ratio = 1.46 (Calle, NEJM, April 2003)
• Described as “relative risk” in the article (very common practice)

Rate ratio vs. Risk ratio• Risk must be between 0 and 1
– Thus in comparing 2 groups high risk in unexposed group limits how large ratio can be
– Eg, risk in unexposed group = 0.7 means maximum risk ratio = 1.0/0.7 = 1.42
• Rates are not restricted between 0 and 1– If exposed rate = 10/100 person-years and
unexposed rate = 5/100 person-years, risk (cumulative incidence) in 2 groups after 20 years = 0.88 and 0.64.
– Risk ratio would be 0.88/0.64 = 1.38 – but rate ratio = 10/5 = 2.0.

Ratio measures of association and Study Design
• Cross-sectional study– Prevalence ratio– (Prevalence) odds ratio
• Cohort Study– Risk ratio– Rate ratio– Odds ratio
• Case-control study– Odds ratio
Measure of Association in Case-Control Studies
• Odds ratio (OR) of exposure in cases and controls is the measure of association in case-control studies
• OR of exposure = OR of disease
• OR of exposure estimates different measures of association depending on the type of sampling used for the case-control designs

To understand what OR in a case-control study
estimates, we return to the setting of a cohort
Some abbreviations: 1= exposed and 0 = not exposed
E1 = Events = diagnoses in exposed group
E0 = Events = diagnoses in unexposed group
N1 = number of persons in exposed group
N0 = number of persons in unexposed group
1
0
0
1
0
0
1
1
0
0
1
1
N
N
E
E
E
N
N
E
NENE
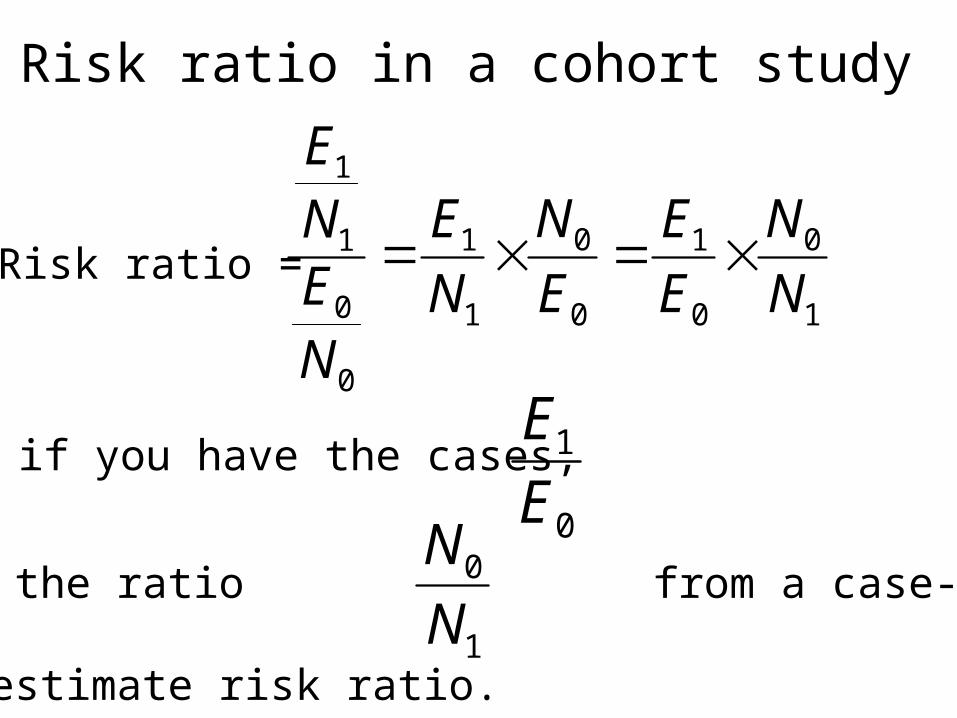
Risk ratio in a cohort study
Risk ratio =
So if you have the cases,
0
1
E
E
Only need the ratio from a case-control
study to estimate risk ratio. 1
0
N
N

Capturing the events with a case-control design
• From a well-defined study base:– All new cases in the study base will be the same
cases as in a cohort study of the base (E1 and E0 )
– Or a random sample of the cases will give the same ratio
0
1
E
E

Sampling in a case-control study• Given all the cases (or a random sample), goal of case-
control design is to sample the study base to get an unbiased estimate of the exposure distribution in the controls
• The exposure distribution in the controls is given by the ratio
• Thus if this ratio can be obtained in a case-control study, the risk ratio is obtained with a case-control design
1
0
N
N

Case Control Sampling and the Risk Ratio
• How can the study base be sampled to get an unbiased estimate of the risk ratio?
• Question can be rephrased as “How can the study base be sampled to get an unbiased estimate of ?”
1
0
N
N
Three Case-Control Designs
1) Case-cohort design: controls sampled from baseline of a cohort or study base
2) Incidence-density controls: controls sampled from risk sets of cohort or study base each time a case is diagnosed
3) Prevalent controls: controls sampled from non-cases at one point in time during follow-up of the cohort or study base

Case-cohort: sample baseline of cohort N0 / N1 is sampled randomly from baseline

Case-cohort Sampling• Control group is random sample of cohort at
baseline
• Estimates the odds of exposure in the study base (i.e., estimates N0 / N1)
• Control group can be used for >1 outcome
• Can use same controls later for more follow-up
• Relatively new design: first described by Prentice (1986); now being extended from cohorts to other primary study bases
• Odds ratio estimates the risk ratio

How OR = Risk ratio in a Case-Cohort design
Cases Controls
Exp
osur
e
Yes
No
a = E1 b ≈ N1
c = E0
exposure oddsin cases = a/cand odds in controls = b/dSo OR = E1
E0
N1
N0
d ≈ N0

1
0
0
1
0
0
1
1
0
0
1
1
N
N
E
E
E
N
N
E
NENE
Risk ratio in a cohort study
Risk ratio =
So if you have the cases,
0
1
E
E
Only need the ratio
1
0
N
N

Example of case-cohort studyIn the Netherlands Cohort Study among 120,852 subjects aged 55-69 years at baseline (1986), the association between vitamins and carotenoids intake, vitamin supplement use, and bladder cancer incidence was examined. . . . After 6.3 years of follow-up, data from 569 cases and 3123 subcohort members were available for case-cohort analyses. The age-, sex-, and smoking-adjusted relative risks (RRs)for retinol, vitamin E, folate, a-carotene, b-carotene, lutein and zeaxanthin, and lycopene were 1.04, 0.98, 1.03, 0.99, 1.16, 1.11, and1.08, respectively, comparing highest to lowest quintile of intake. Onlyvitamin C (RR: 0.81, 95% CI: 0.61-1.07, P-trend = 0.08), and b-cryptoxanthin intake (RR: 0.74, 95% CI: 0.53-1.03, P-trend =0.01) were inversely associated with bladder cancer risk.
Zeegers MP, Goldbohm RA, Brandt PA. Are retinol, vitamin C, vitamin E, folate and carotenoids intake associated withbladder cancer risk? Results from the Netherlands Cohort Study. Br J Cancer 2001 Sep;85(7):977-83

Case-cohort within Netherlands Cohort Cohort baseline = 120,852 subjects
3123 subjectsrandomly sampled
569 incidentcases of bladdercancer

Estimating the rate ratio in a case-control study
• For calculating a rate ratio, what is analogous to estimating the proportion of exposed and unexposed persons?
• Answer: the proportion of exposed and unexposed person-time

11
00
0
1
00
0
11
1
TN
TN
E
E
TN
ETN
E
11
00
TN
TN
Rate ratio in cohort where = exposedand = unexposed person-time
So analogous to estimating risk ratio, need to estimate the proportion
If we can estimate that proportion in a case-control study, we can estimate the rate ratio
Rate Ratio =
11TN00TN
Second type of case-control sampling
Incidence density sampling
• Controls are sampled from the risk set at the time each case is diagnosed– Samples person-time experience of the study
base
• Odds ratio estimates the rate ratio

Incidence density sampling in a fixed cohort study base
• Controls are matched to cases on time at risk (same amount of follow-up time)
• Sampling non-cases at each time case occurs samples person-time
• Someone who is a control at one time can later be a case and/or a control again
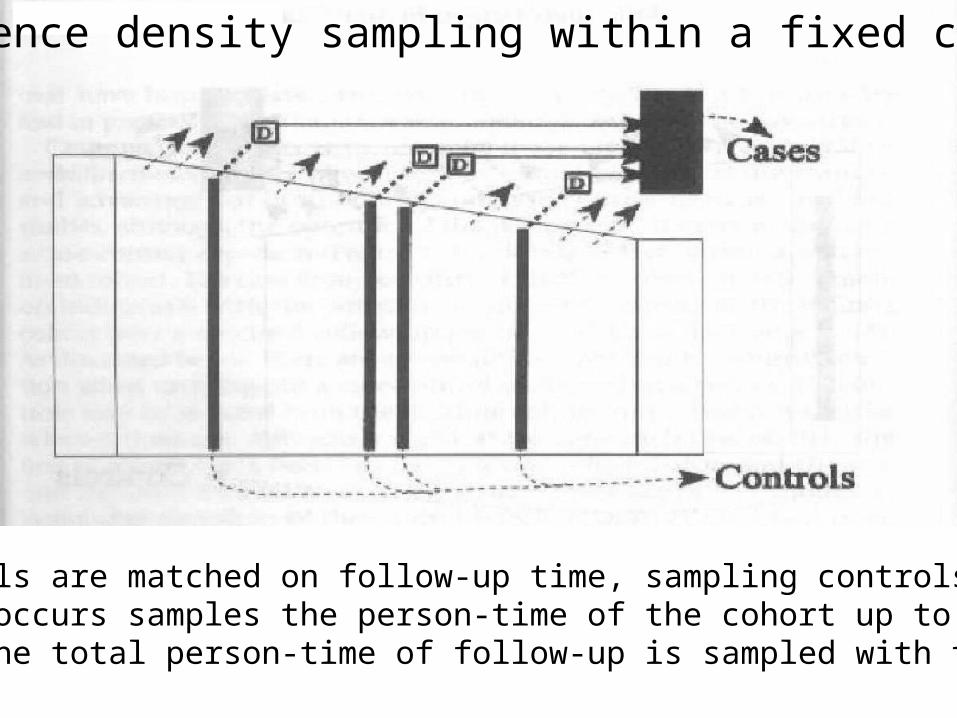
Incidence density sampling within a fixed cohort
Since controls are matched on follow-up time, sampling controls eachtime a case occurs samples the person-time of the cohort up to that point. So the total person-time of follow-up is sampled with this design.

Incidence density sampling in a dynamic cohort(e.g., Kaiser Permanente membership)
New members
Sampling in a dynamic cohort gives unbiased estimate ofperson-time in the same way as sampling in a closed cohort
PrimaryStudyBase

How OR = Rate ratio in a case-control studywith incidence density sampling
Cases Controls
Exp
osur
e
Yes
No
a = E1 b ≈ N1 T1
c = E0
exposure oddsin cases = a/cand odds in controls = b/dSo OR = E1
E0
N1T1
N0T0
d ≈ N0 T0

11
00
0
1
00
0
11
1
TN
TN
E
E
TNE
TNE
Rate ratio in cohort where = exposedand = unexposed person-time
Rate Ratio =
11TN00TN
So inverting and multiplying the OR on the previous slidegives the right-hand term on this slide which equals theleft-hand term, the rate ratio.
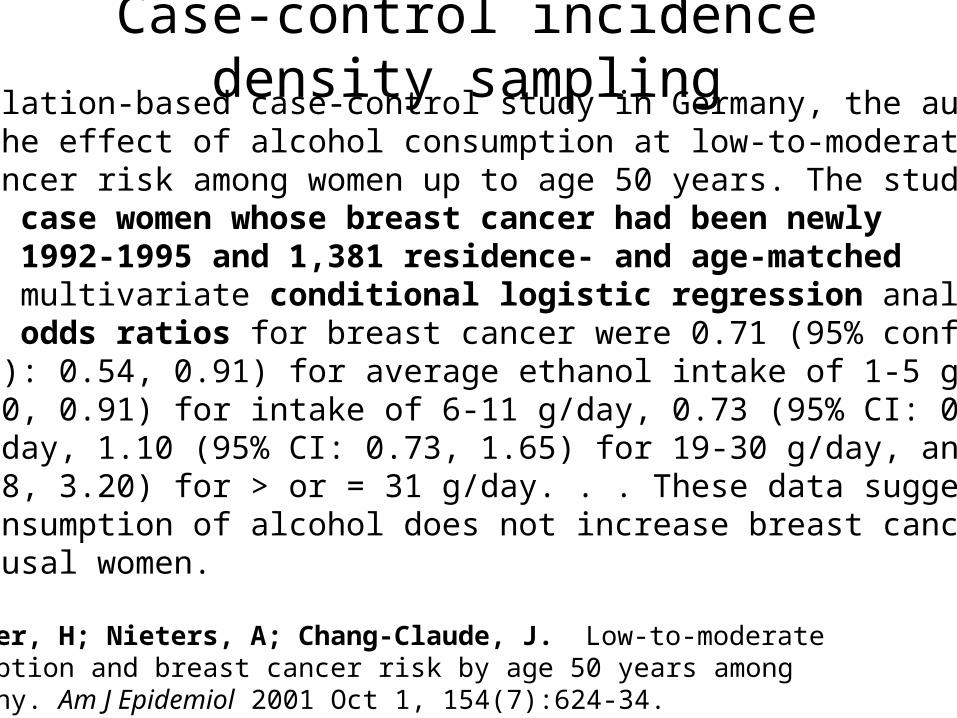
Case-control incidence density sampling...In a population-based case-control study in Germany, the authors determined the effect of alcohol consumption at low-to-moderate levels on breast cancer risk among women up to age 50 years. The study included 706 case women whose breast cancer had been newlydiagnosed in 1992-1995 and 1,381 residence- and age-matchedcontrols. In multivariate conditional logistic regression analysis, the adjusted odds ratios for breast cancer were 0.71 (95% confidence interval (CI): 0.54, 0.91) for average ethanol intake of 1-5 g/day, 0.67 (95% CI: 0.50, 0.91) for intake of 6-11 g/day, 0.73 (95% CI: 0.51, 1.05)for 12-18 g/day, 1.10 (95% CI: 0.73, 1.65) for 19-30 g/day, and 1.94 (95% CI: 1.18, 3.20) for > or = 31 g/day. . . These data suggest that low-level consumption of alcohol does not increase breast cancer risk in premenopausal women.
Kropp, S; Becher, H; Nieters, A; Chang-Claude, J. Low-to-moderate alcohol consumption and breast cancer risk by age 50 years among women in Germany. Am J Epidemiol 2001 Oct 1, 154(7):624-34.

New residents
Random sample of population each time breast cancer diagnosed
PrimaryStudyBase
Incidence density sampling within a dynamic cohort (German population 1992-1995)
706 incidentcases of breast cancer
1,381 age & residencematched

Third type of case-control sampling
• Sampling only non-cases in a primary or secondary study base
• Prevalent controls because controls are sampled from those without disease with a cross-sectional sample of the study base
• Odds ratio approximates risk ratio only if disease occurrence is rare

Text example of case-control design showing sampling prevalent controls from non-casesStudy
Base
Only non-casesare eligible to becontrols in thisdesign

Inability to calculate risk ratio if controls sampled from non-cases
ratio is known in all case-control designs
But sampling only non-cases cannot get unbiased estimate of 1
0
N
N
0
1
E
E

Inability to calculate risk ratio if controls sampled from non-cases
Example:
Cohort of 200 with prevalence of exposure = 50%
100 exposed-----40 cases occur--leaves 60 non-cases100 unexposed--10 cases occur--leaves 90 non-cases
Total: 50 cases 150 non-cases

Inability to calculate risk ratio if controls sampled from non-cases
• So in this example:
• And:
• Risk ratio = 4.0
410
40
0
1 E
E
1100
100
1
0 N
N

OR using controls from prevalent non-cases
Disease No disease
Exposed 40
10 90 Unexposed
Disease
60
No disease
time
cases controls
A random sample from cells b (60) and d (90) will give a ratio equal to 60/90 and therefore an OR = 6.0 vs. the true risk ratio = 4.0
Using all prevalent non-cases in cohort, the OR would be: OR = 40/10 over 60/90 = 6.0
Case-Control with prevalent controls
• If controls are selected among those without disease at time of study (+ prevalent cases), the
OR approximates risk ratio only with the
rare disease assumption
• Rare disease assumption: if disease incidence low in unexposed and exposed (<10%), OR RR– Exposure in controls exposure in whole cohort

Case-Control with prevalent controls
• Sampling only non-cases means sampling from N1 – E1, so if E1 is small, N1 isn’t changed much (and similarly for N0)
• Older texts describe case-control design as always requiring rare disease assumption to estimate risk ratio -- not the case

OR using controls from prevalent non-caseswhen incidence low
Disease No disease
Exposed 4
1 99 Unexposed
Disease
96
No disease
time
cases controls
A random sample from cells b (60) and d (90) will give a ratio equal to 96/99 and therefore an OR = 4.13 close to true risk ratio = 4.0If the incidence had been 10% overall, OR = 4.57.
Using all prevalent non-cases in cohort would be OR = 4/1 over 96/99 = 4.13
Caveat: Sampling non-cases may introduce bias even if disease is rare
• Disease may remove few from study base sampled for controls, but other sources of loss to follow-up can bias control group
• Losses to follow-up and deaths among potential controls from the study base giving rise to the cases affect who is available at one point in time

Surveillance for toxic-shock syndrome (TSS) in Wisconsin detected cases with onsets from September 1975 through June 1980… 35 patients were matched for age and menstruation to 105 controls: 34 of 35 cases (versus 80 of 105 controls) used tampons during every menstrual period (OR = 10.6, p < 0.01)… In Wisconsin the minimum incidence of TSS as defined by clinical criteria is 6.2 cases per 100,000 menstruating women per year.
Davis JP et al. N Engl J Med 1980 Dec 18;303(25):1429-35
Case-Control study with prevalent sampling of rare disease
An example of an extremely rare disease: only 6 per 100,000 person-years. The odds ratio of 10.6 is a very good approximation of the risk ratio in this instance.
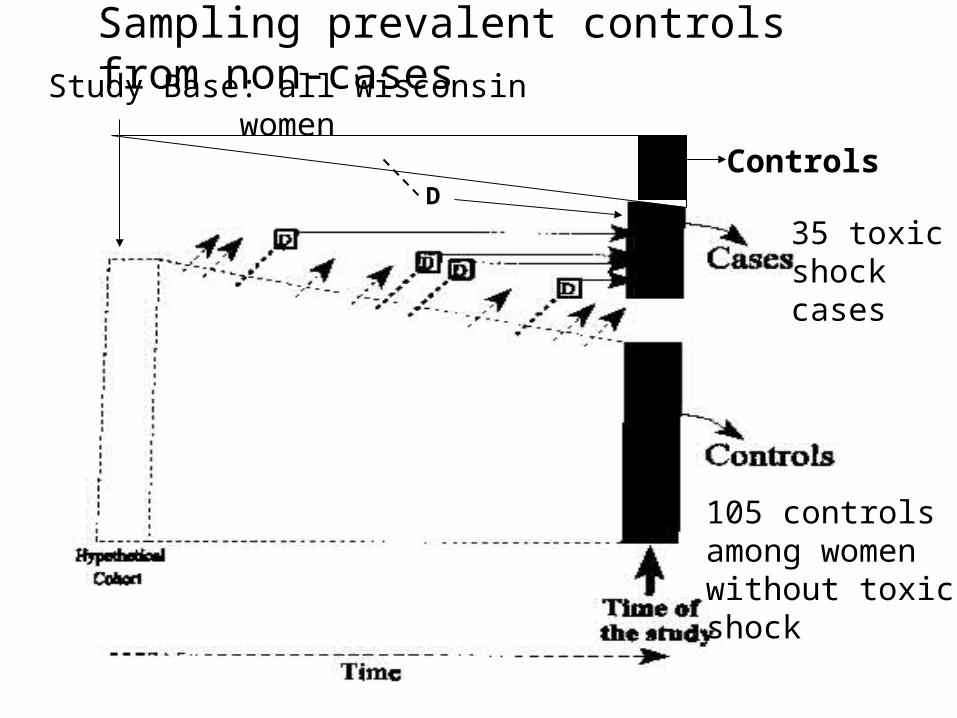
Sampling prevalent controls from non-casesStudy Base: all Wisconsin women
105 controlsamong womenwithout toxicshock
35 toxicshockcases
ControlsD

Effect of control sampling on measure of association estimated by OR
Design Sampling Measure of Association
Prevalent non-cases at case-control single point in time odds ratio
Case-cohort entire cohort at baseline risk ratio
Incidence- non-cases at timedensity each case diagnosed rate ratio

Statistical penalties for sampling the study base
• Case-control design obtains a sample of the denominator rather than entire denominator
• Introduces some sampling error
• Reduces precision of the risk ratio or rate ratio or odds ratio estimate because sample N is smaller than full study base N
• Loss of precision offset by large gain in cost and time of study

OR misuse in presenting results• Language like “X times as likely to” implies a
comparison of probabilities, not odds– acceptable only if incidence is low
• Language like “7% more likely” suggests an absolute risk difference, not a ratio (also a misuse of risk ratios)
• With high incidence of outcome, OR misrepresents the relative probabilities, so language should not imply probability
• Abstracts and press releases determine how results are received by public

Summary: Common misunderstandings about case-
control studies
• They can only study one disease outcome
• Inference is not as valid as from a cohort
• “Rare disease assumption” is required for OR from case-control to estimate risk ratio
• Retrospective measurement is necessary in case-control studies

Summary: What is true about case-control studies
• There are typically more opportunities for bias and misclassification in case-control studies than in cohort studies
• Relative ease with which they can be done has encouraged a lot of badly designed studies
• Low cost and shorter time should be an incentive to better, not worse, design

Case-control design recommendations
• Look for a primary study base that can be clearly defined and has good case ascertainment
• Use incidence density or case-cohort sampling whenever possible– incidence density more often possible
• Use measurements recorded prior to the diagnosis when possible (medical records, etc.) or perform biological measurements on stored specimens
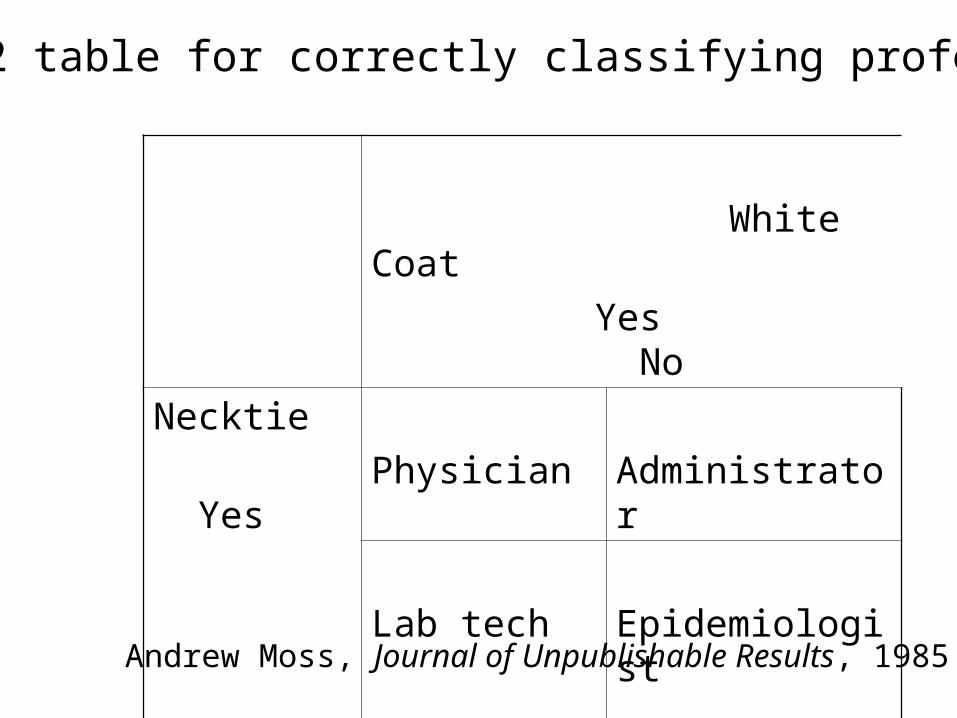
White Coat
Yes No
Necktie
Yes
No
Physician Administrator
Lab tech Epidemiologist
2 x 2 table for correctly classifying professions
Andrew Moss, Journal of Unpublishable Results, 1985