Magnetic resonance imaging of the functional anatomy of...
8
Magnetic Resonance Imaging of the Functional Anatomy of the Superior Oblique Muscle Joseph L. Demer*-\ and Joel M. Miller% Purpose. To study the size and contractile changes of the normal superior oblique (SO) muscle using high-resolution magnetic resonance imaging (MRI), and to evaluate the abnormalities in these characteristics produced by SO palsy. Methods. Multiple coronal MRI image planes were obtained using a surface coil to span the antero-posterior extent of each orbit and were repeated in multiple directions of gaze. Digital image analysis was used to measure muscle cross-sectional area for evaluation of size and contractility. Results. Data for 16 orbits of 11 subjects without SO palsies established norms for morphology and contractility. On SO contraction in down gaze, maximum cross sectional area was signifi- cantly (P < 0.001) greater than on relaxation in up gaze, and the point of maximum cross- section shifted posteriorly with contraction. In seven subjects with clinically unilateral chronic SO palsies, the affected muscle was significandy smaller than normal (P < 0.001) and lacked contractile changes; clinically normal fellow SO muscles exhibited normal cross-sections and contractile changes. Conclusion. High-resolution MRI, coupled with quantitative morphometric analysis, can dem- onstrate the size and contractility of the normal SO muscle. The technique, which can be employed using widely available clinical equipment, is also sensitive enough to detect anatomic and functional changes expected in chronic SO palsies. Invest Ophthalmol Vis Sci. 1995; 36:906-913. JL he actions of the oblique extraocular muscles are mechanically complex, 1 ' 2 and, in contrast with the recti muscles, oblique muscle dysfunction is often not clinically obvious from inspection of ocular ductions and versions. 3 One classical ambiguity in the diagnosis of hypertropia is determining the presence of superior oblique (SO) palsy. 4 A large body of clinical practice has evolved on the basis of clinical evidence, but the mechanical state of the SO muscle belly itself has been inaccessible to direct study. Thus, many inferences From the *Jules Stein Eye Institute and the ^Department of Neurology, UCLA School of Medicine, University of California, Los Angeles, and the XSmith-Kettlewell Eye Research Institute, San Francisco, California. Presented in part at the 1993 annual meeting of the Association for Research in Vision and Ophthalmology, Sarasota, Florida. Supported by grants from the United States Public Health Service, National Eye Institute, consortium grant EY0S313 (JD, JM), core grant EY00331 to the (/CM Department of Ophthalmology, and core grant EY06883 to Smith-Ketttaoell Eye Research Institute. JD was a Research to Prevent Blindness William and Mary Crevc International Research Scholar. Submitted for publication May 19, 1994; revised November 14, 1994; accepted November 15, 1994. Prof/rietary interest category: N. Reprint requests: Joseph L. Demer, Jules Stein Eye Institute, 100 Stein Plaza, UCI-A, Los Angeles, CA 90024-7002. concerning SO function remain presumptive. Recent advances in imaging now provide another means of evaluating SO function. Simonsz first used computed radiographic tomography for evaluation of extraocu- lar muscle paths during changes in gaze. 5 Miller used high-resolution, surface-coil magnetic resonance im- aging (MRI) along with three-dimensional reconstruc- tions and quantitative morphometry to demonstrate the functional anatomy of the recti muscles of normal subjects. 6 These studies revealed the following novel aspects of rectus muscle functional anatomy: The paths of the recti muscle bellies remain highly con- strained in the orbit despite the largest attainable duc- tions; during contraction, a muscle's cross-sectional area increases and the point of maximum cross-sec- tional area shifts posteriorly in the orbit; during relax- ation, a muscle's cross-sectional area decreases and the point of maximum cross-sectional area shifts ante- riorly in the orbit. This means that MRI can demon- strate the function and contractile state of recti extra- ocular muscles. There has been little application of MRI to the 906 Investigative Ophthalmology & Visual Science, April 1995, Vol. 36, No. 5 Copyright © Association for Research in Vision and Ophthalmology Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933185/ on 06/20/2018
-
Upload
dangnguyet -
Category
Documents
-
view
222 -
download
0
Transcript of Magnetic resonance imaging of the functional anatomy of...

Magnetic Resonance Imaging of the FunctionalAnatomy of the Superior Oblique Muscle
Joseph L. Demer*-\ and Joel M. Miller%
Purpose. To study the size and contractile changes of the normal superior oblique (SO) muscleusing high-resolution magnetic resonance imaging (MRI), and to evaluate the abnormalitiesin these characteristics produced by SO palsy.
Methods. Multiple coronal MRI image planes were obtained using a surface coil to span theantero-posterior extent of each orbit and were repeated in multiple directions of gaze. Digitalimage analysis was used to measure muscle cross-sectional area for evaluation of size andcontractility.
Results. Data for 16 orbits of 11 subjects without SO palsies established norms for morphologyand contractility. On SO contraction in down gaze, maximum cross sectional area was signifi-cantly (P < 0.001) greater than on relaxation in up gaze, and the point of maximum cross-section shifted posteriorly with contraction. In seven subjects with clinically unilateral chronicSO palsies, the affected muscle was significandy smaller than normal (P < 0.001) and lackedcontractile changes; clinically normal fellow SO muscles exhibited normal cross-sections andcontractile changes.
Conclusion. High-resolution MRI, coupled with quantitative morphometric analysis, can dem-onstrate the size and contractility of the normal SO muscle. The technique, which can beemployed using widely available clinical equipment, is also sensitive enough to detect anatomicand functional changes expected in chronic SO palsies. Invest Ophthalmol Vis Sci.1995; 36:906-913.
JL he actions of the oblique extraocular muscles aremechanically complex,1'2 and, in contrast with therecti muscles, oblique muscle dysfunction is often notclinically obvious from inspection of ocular ductionsand versions.3 One classical ambiguity in the diagnosisof hypertropia is determining the presence of superioroblique (SO) palsy.4 A large body of clinical practicehas evolved on the basis of clinical evidence, but themechanical state of the SO muscle belly itself has beeninaccessible to direct study. Thus, many inferences
From the *Jules Stein Eye Institute and the ^Department of Neurology, UCLA Schoolof Medicine, University of California, Los Angeles, and the XSmith-Kettlewell EyeResearch Institute, San Francisco, California.Presented in part at the 1993 annual meeting of the Association for Research inVision and Ophthalmology, Sarasota, Florida.Supported by grants from the United States Public Health Service, National EyeInstitute, consortium grant EY0S313 (JD, JM), core grant EY00331 to the (/CMDepartment of Ophthalmology, and core grant EY06883 to Smith-Ketttaoell EyeResearch Institute. JD was a Research to Prevent Blindness William and MaryCrevc International Research Scholar.Submitted for publication May 19, 1994; revised November 14, 1994; acceptedNovember 15, 1994.Prof/rietary interest category: N.Reprint requests: Joseph L. Demer, Jules Stein Eye Institute, 100 Stein Plaza, UCI-A,Los Angeles, CA 90024-7002.
concerning SO function remain presumptive. Recentadvances in imaging now provide another means ofevaluating SO function. Simonsz first used computedradiographic tomography for evaluation of extraocu-lar muscle paths during changes in gaze.5 Miller usedhigh-resolution, surface-coil magnetic resonance im-aging (MRI) along with three-dimensional reconstruc-tions and quantitative morphometry to demonstratethe functional anatomy of the recti muscles of normalsubjects.6 These studies revealed the following novelaspects of rectus muscle functional anatomy: Thepaths of the recti muscle bellies remain highly con-strained in the orbit despite the largest attainable duc-tions; during contraction, a muscle's cross-sectionalarea increases and the point of maximum cross-sec-tional area shifts posteriorly in the orbit; during relax-ation, a muscle's cross-sectional area decreases andthe point of maximum cross-sectional area shifts ante-riorly in the orbit. This means that MRI can demon-strate the function and contractile state of recti extra-ocular muscles.
There has been little application of MRI to the
906Investigative Ophthalmology & Visual Science, April 1995, Vol. 36, No. 5Copyright © Association for Research in Vision and Ophthalmology
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933185/ on 06/20/2018

Superior Oblique Imaging 907
TABLE i. Characteristics of Subjects With Unilateral Superior Oblique Palsy
Subject
12340
67
Sex
MaleMaleMaleMaleMaleFemaleMale
Age(years)
29183263192221
Side
LeftLeftRightRightLeftRightLeft
Cause
TraumaticCongenitalPostviralCongenitalTraumaticCongenitalCongenital
Duration(years)
11181
631
2221
Primary PositionDeviation (Hyper A)
20104
30303040
Excyclodeviation f)
575364
10
ft-
study of abnormal extraocular muscles. Demer andMiller7 presented qualitative MRJ data in anecdotalcases of lateral rectus and SO atrophy in abducensand trochlear palsy, as well as congenital ectopy of thehorizontal rectus muscles in "A" pattern exotropia.Nishida and collaborators8 used MRI to demonstrateatrophy of involved muscles in abducens and oculo-motor paralysis. Horton and associates9 reported qual-itative evidence of SO atrophy in a patient with troch-lear palsy. However, the functional anatomy of thenormal SO muscle as it depends on gaze directionhas not been studied using MRI, and no quantitativestudies have been performed in SO palsy. The presentinvestigation was conducted to characterize the nor-mal quantitative morphology and contractility of theSO muscle and to determine the effects on these pa-rameters of SO palsy.
METHODS
Orbital MRI studies were prospectively performed involunteer subjects who, after receiving an explanationof the research, gave written informed consent ac-cording to a protocol approved by the institutionalreview board for the protection of human subjectsand conforming to the tenets of the Declaration ofHelsinki. Ten orbits were studied in seven subjectswho had no abnormalities of ocular motility. Six orbitswere studied in four subjects who had various formsof strabismus but no suspicion of SO abnormalities.The mean age of these control subjects was 38 ± 16years (mean ± SD). Fourteen orbits were studied inseven subjects who had clinically identified chronicunilateral SO palsies; clinical characteristics are de-scribed in Table 1. The mean age of subjects with SOpalsies was 29 ± 16 years.
Superior oblique palsy was diagnosed when thepatient's medical history indicated pathology of thetrochlear nerve and when the following clinical find-ings were present10"12: deficient depression of the ipsi-lateral eye in adduction; ipsilateral hypertropia in-creasing in adduction and with tilt of the head towardthe ipsilateral shoulder; presence of subjective ex-
cyclotorsion of one or both eyes; and ophthalmo-scopic evidence of excyclotorsion of the ipsilateralmacula. However, SO palsy was not diagnosed whenprior strabismus surgery or direct orbital traumamight have accounted for the above clinical findings.Binocular misalignment was determined using prismand cover testing and the Hess screen test.
Orbits were imaged using one of the followingscanners: MR-Max (0.5 tesla magnet) or Signa (1.5tesla) (General Electric, Milwaukee, WI) or Vista (1.5tesla) (Picker, Columbus, OH). General aspects of thescanning protocol have been described elsewhere.613
While using widely available clinical MRI hardwareand software, we used procedures optimized for extra-ocular muscles. The fundamental principle is to usescanner settings permitting the highest resolution im-ages of the orbit to be obtained in a time period suffi-ciently brief that subjects can maintain continuousfixation on a defined target. Control of fixation andavoidance of movement artifacts then permit quantita-tive analysis of images for determination of musclecontractility. There is necessarily a trade-off betweenimage acquisition time on the one hand and imagequality on the other. Smaller detector coils improveresolution but reduce the tissue volume that can beimaged. Use of 75-mm to 125-mm diameter surfacecoils, rather than the larger and more commonly usedcranial coil, provides higher resolution images limitedto the extent of the orbit.
Subjects' heads were oriented in the scanner sothat the axis of the scanned orbit was vertical, as illus-trated in Figure 1A. This permits acquisition of coro-nal plane images that are as close to perpendicular tothe axes of all of the extraocular muscles as possible.Data on the reed muscles are reported elsewhere.1'1
One eye was always occluded, and the fellow eyeviewed the fixation target. Fixation targets consistedof small black crosses in the center of 1.5-cm diameter,brightly colored adhesive disks affixed to the inside ofthe scanner magnet. Primary position was always used.In most subjects, scans were repeated in 20° elevationand in 20° depression. The eccentric position chosenwas the greatest that could be comfortably sustained
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933185/ on 06/20/2018

908 Investigative Ophthalmology & Visual Science, April 1995, Vol. 36, No. 5
FIGURE l. {left) An axial localizer magnetic resonance image of the rightorbit of a normal subject, illustrating the vertical orientation of the headin the scanner and levels of 12 contiguous coronal image planes usedfor analysis. Numerals indicate the designation of coronal image planes,with plane zero defined as that having the greatest SO cross-sectionalarea in primary gaze, (right) Coronal magnetic resonance images of theright orbit of a normal subject at an intermediate antero-posterior dis-tance, repeated in three directions of gaze. In down gaze, note the upward
displacement of the optic nerve (ON), large cross-section of the inferior rectus (IR) and superior oblique (SO) muscles, and smallcross-section of the superior rectus (SR) muscle. The cross-section of the SO has been digitally outlined in the image obtained inprimary gaze, in which all muscle cross sections are intermediate. In up gaze, note the downward displacement of the ON, thelarge cross-section of the SR, and the small cross-sections of the SO and IR muscles.
for the typically 3-minute, 38-second duration of eachscan. The actual position of the eye during scanningwas verified by measurement from the images of theposition of the globe-optic nerve junction, whichmoves in the opposite direction from the cornea.0
For each orbit, an axial localizer image (Fig. 1A)was taken at low resolution using settings in Table2 to select the optimal antero-posterior location ofsubsequent high-resolution coronal image acquisitionplanes. Scanning parameters were chosen to obtain aseries of 12 adjacent 2.5-mm to 3-mm thick imagesspanning the antero-posterior extent of each orbit.No gap was left between image planes. For most orbits,a set of 12 planes permits imaging from the annulusof Zinn in the orbital apex to a level just anterior tothe trochlea.
Settings for each of the MRI instruments usedare specified in Table 2. Subjects were instructed tomaintain steady fixation during scanning and to blinkas little as possible. The ventilator fan inside the scan-ner magnet was switched off during fixations becauseair flow produced by the fan causes rapid corneal des-iccation and induces frequent blinking, especially inup gaze. For images most commonly acquired in a 256(horizontal) X 192 (vertical) pixel matrix over a 10X 10 cm field of view, pixel resolution was 0.39 X 0.52mm in the image plane. Resolution between planeswas equal to the thickness of the image slice, 2.5 or 3mm.
Magnetic resonance images in the early phase ofthis study were printed on conventional radiographicfilm at approximately X2 magnification with centeringon the orbit, and they were digitized using a ScanJet
II flatbed optical scanner (Hewlett-Packard, Palo Alto,CA) at 150 dots per inch and 256 levels of gray scale.Later images were directly converted from scannermagnetic tape data files using locally written softwarethat also optimized contrast and brightness. In eithercase, images were converted to standard 8-bit taggedimage file format (TIFF) for quantitative analysis onMacintosh II or Quadra (Apple Computer, Cupertino,CA) computers using the public domain NIH Imageprogram obtained from the National Institutes ofHealth (W. Rasband). Spatial calibration was per-formed through the NIH Image program. The SOmuscle was identified near the antero-posterior centerof the orbit and traced anteriorly and posteriorly insequential images. The border of the SO was manuallytraced using a cursor (Fig. IB), and the cross-sectionalarea of the muscle was automatically computed. Thisprocedure was replicated for each orbit and each di-rection of gaze.
As a consequence of head positioning, the pathof the SO muscle was angled from the normal to thecoronal plane. Using measurements from the axiallocalizer images, the mean angle in the axial planewas found to be 24.1° ± 4.5° (mean ± SD). Usingmeasurements from reconstructed sagittal images, themean angle in the sagittal plane was found to be 19.5°± 6.5°. Measured cross-sectional areas were trigono-metrically corrected for these angles so that reportedareas represent true perpendicular cross-sections.
Superior oblique cross-sectional areas were plot-ted against image plane number, as registered to thenumber zero assigned by convention to the imageplane having the greatest cross-sectional area in pri-
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933185/ on 06/20/2018
Superior Oblique Imaging
TABLE 2. Magnetic Resonance Scanner Parameters
909
Model
GE SignaGE SignaGE MR-MaxGE MR-MaxPicker VistaPicker Vista
Field(tesla)
1.51.50.50.51.51.5
Plane
AxialCoronalAxialCoronalAxialCoronal
Thickness(mm)
43332.53
Gap(mm)
201000
Matrix
256 X 128256 X 192192 X 192128 X 128192 X 128256 X 256
Field ofView (cm)
161015151610
RepeatTime(msec)
400550400750300817
EchoTime(msec)
161530302020
Excitations
121211
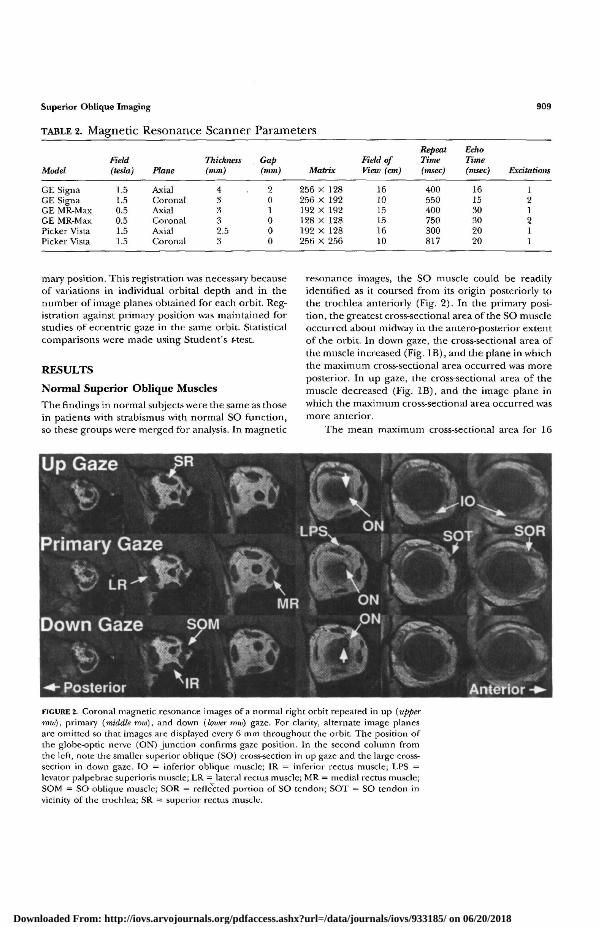
mary position. This registration was necessary becauseof variations in individual orbital depth and in thenumber of image planes obtained for each orbit. Reg-istration against primary position was maintained forstudies of eccentric gaze in the same orbit. Statisticalcomparisons were made using Student's t-test.
RESULTS
Normal Superior Oblique Muscles
The findings in normal subjects were the same as thosein patients with strabismus with normal SO function,so these groups were merged for analysis. In magnetic
resonance images, the SO muscle could be readilyidentified as it coursed from its origin posteriorly tothe trochlea anteriorly (Fig. 2). In the primary posi-tion, the greatest cross-sectional area of the SO muscleoccurred about midway in the antero-posterior extentof the orbit. In down gaze, the cross-sectional area ofthe muscle increased (Fig. IB), and the plane in whichthe maximum cross-sectional area occurred was moreposterior. In up gaze, the cross-sectional area of themuscle decreased (Fig. IB), and the image plane inwhich the maximum cross-sectional area occurred wasmore anterior.
The mean maximum cross-sectional area for 16
FIGURE 2. Coronal magnetic resonance images of a normal right orbit repeated in up (upperroiv), primary (middle row), and down (loioer roxu) gaze. For clarity, alternate image planesare omitted so that images are displayed ever)' 6 mm throughout the orbit. The position ofthe globe-optic nerve (ON) junction confirms gaze position. In the second column fromthe left, note the smaller superior oblique (SO) cross-section in up gaze and the large cross-section in down gaze. IO = inferior oblique muscle; IR = inferior rectus muscle; LPS =levator palpebrae superioris muscle; LR = lateral rectus muscle; MR = medial rectus muscle;SOM = SO oblique muscle; SOR = reflected portion of SO tendon; SOT = SO tendon invicinity of the trochlea; SR = superior rectus muscle.
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933185/ on 06/20/2018

910 Investigative Ophthalmology & Visual Science, April 1995, Vol. 36, No. 5
TABLE 3. Maximum Superior Oblique Cross-Sectional Area in Normal Subjects
Gaze
UpPrimaryDown
Mean (cm2)
0.170*0.1900.217*
Cross-Sectional AreaFrom Primary Gaze(within subjects)
Standarddeviation (cm2)
0.0540.0400.043
Orbits
111611
Mean (cm2)
-0.055f
0.076f
Area Change
Standarddeviation (cm2)
0.032
0.041
Orbits
11
11
* Up area significantly different from down, P < 0.025.t Change significantly different from zero, P < 0.0005.
normal SO muscles was 0.190 cm2 ± 0.040 cm2, witha range of 0.126 to 0.269 cm2. Pooled mean cross-sectional areas for all normal SO muscles, averagedfor each direction of gaze, are plotted in Figure 3.Between up and primary gaze, the maximum pooledmean cross-sectional area increased and shifted about3 mm posteriorly. Between primary and down gaze,there was a broadening of the peak in cross-sectionalarea, with an increase in cross-sectional area for themost posterior image planes. From primary to downgaze, the maximum pooled mean maximum cross-sec-tional area did not increase. Table 3 indicates meanvalues for maximum individual cross-sectional areasobserved in each subject for the SO muscle in downgaze, primary position, and up gaze. It should benoted that these values were obtained by averagingthe maximum values for each subject and thus aregreater than the maximum values of the mean alignedareas. Mean SO cross-sectional area in down gaze wassignificantly greater than in up gaze (P < 0.025).Pooled areas for up gaze and down gaze did not differ
£ 0.20
W O
o
Up GazePrimary GazeDown Gaze
Mean ± Standard Error of Mean
<- Posterior MRI Image Plane Anterior ->
FIGURE 3. Cross-sectional area of normal superior obliquemuscles in three directions of gaze obtained by 3-mm coro-nal plane magnetic resonance imaging. The cross-sectionalarea decreased in up gaze, and the plane of maximum cross-sectional area moved anteriorly. In down gaze, cross-sectionsincreased posteriorly.
significantly from those for primary position (P >0.05). However, when interindividual differences werecontrolled by computing for each individual thechange in SO cross-sectional area from primary posi-tion to eccentric gaze, the differences were significant(Table 3, P < 0.0005). The mean change in SO cross-sectional area during gaze changes is plotted as a func-tion of antero-posterior location in the orbit in Figure4. This plot shows that contraction and relaxation ofthe SO muscle during gaze changes occurs primarilyin the posterior half of the muscle, deep in the orbit.
With these basic data available on the normalfunctional anatomy of the SO, similar investigationswere made in seven subjects with unilateral SO palsies(Table 1). Three patterns of abnormality were foundin the palsied muscles, as illustrated, for representativesubjects in Figure 5. In subject 1, only the posteriorhalf of the affected left SO muscle belly was smallerthan normal (Fig. 5A); the maximum cross-section ofthis muscle did not occur in its normal mid-antero-posterior orbital position. Instead of being maximalin image plane 0, the maximum cross-section for theleft SO of subject 1 occurred in image plane 3, where
Normal Muscles
o j
—4r-- Up Gaze
— • — Down Gaze
Mean ± Standard Error of Mean
<- Posterior MRI Image Plane Anterior ->
FIGURE 4. Change in cross-sectional area of the superioroblique muscle of normal subjects during gaze change fromprimary to up and primary to down. Consistent contractilechanges occurred only in the posterior muscle, correspond-ing to negative image plane numbers.
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933185/ on 06/20/2018
Superior Oblique Imaging 911
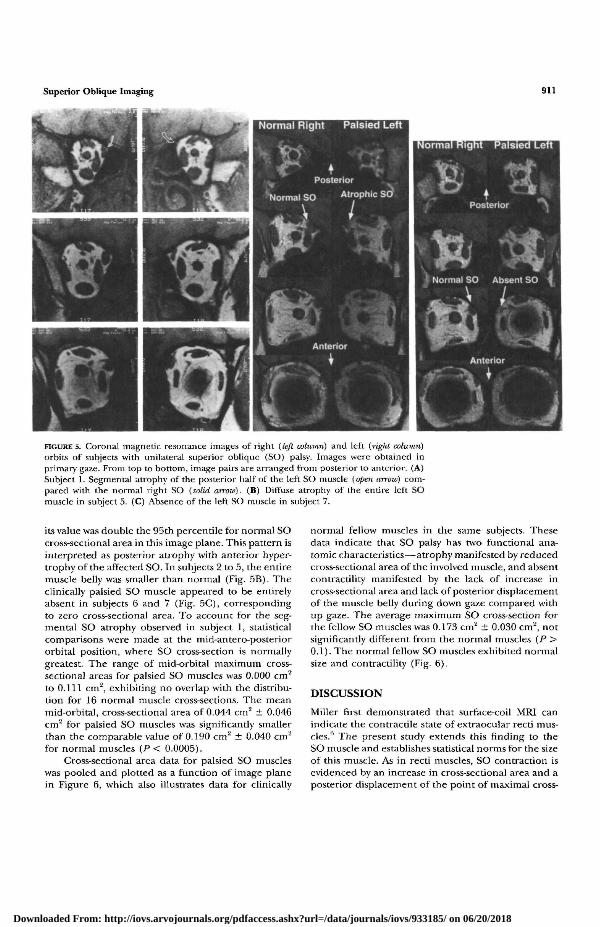
FIGURE 5. Coronal magnetic resonance images of right {left column) and left {light column)orbits of subjects with unilateral superior oblique (SO) palsy. Images were obtained inprimary gaze. From top to bottom, image pairs are arranged from posterior to anterior. (A)Subject 1. Segmental atrophy of the posterior half of the left SO muscle {open arrow) com-pared with the normal right SO {solid arroio). (B) Diffuse atrophy of the entire left SOmuscle in subject 5. (C) Absence of the left SO muscle in subject 7.
its value was double the 95th percentile for normal SOcross-sectional area in this image plane. This pattern isinterpreted as posterior atrophy with anterior hyper-trophy of the affected SO. In subjects 2 to 5, the entiremuscle belly was smaller than normal (Fig. 5B). Theclinically palsied SO muscle appeared to be entirelyabsent in subjects 6 and 7 (Fig. 5C), correspondingto zero cross-sectional area. To account for the seg-mental SO atrophy observed in subject 1, statisticalcomparisons were made at the mid-antero-posteriororbital position, where SO cross-section is normallygreatest. The range of mid-orbital maximum cross-sectional areas for palsied SO muscles was 0.000 cm2
to 0.111 cm2, exhibiting no overlap with the distribu-tion for 16 normal muscle cross-sections. The meanmid-orbital, cross-sectional area of 0.044 cm3 ± 0.046cm2 for palsied SO muscles was significantly smallerthan the comparable value of 0.190 cm2 ± 0.040 cm2
for normal muscles (P < 0.0005).Cross-sectional area data for palsied SO muscles
was pooled and plotted as a function of image planein Figure 6, which also illustrates data for clinically
normal fellow muscles in the same subjects. Thesedata indicate that SO palsy has two functional ana-tomic characteristics—atrophy manifested by reducedcross-sectional area of the involved muscle, and absentcontractility manifested by the lack of increase incross-sectional area and lack of posterior displacementof the muscle belly during down gaze compared withup gaze. The average maximum SO cross-section forthe fellow SO muscles was 0.173 cm2 ± 0.030 cm'2, notsignificantly different from the normal muscles (P >0.1). The normal fellow SO muscles exhibited normalsize and contractility (Fig. 6).
DISCUSSION
Miller first demonstrated that surface-coil MRI canindicate the contractile state of extraocular recti mus-cles.6 The present study extends this rinding to theSO muscle and establishes statistical norms for the sizeof this muscle. As in recti muscles, SO contraction isevidenced by an increase in cross-sectional area and aposterior displacement of the point of maximal cross-
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933185/ on 06/20/2018

912 Investigative Ophthalmology & Visual Science, April 1995, Vol. 36, No. 5
Fellow
— * - Up Gaze
—•— Primary Gaze
—•— Down Gaze
Palsy—••&—• up Q a z e
—O— Primary Gaze
--O— Down Gaze
<- Posterior MR| Image Plane Anterior ->
FIGURE 6. Mean cross-sectional area of SO muscles in threedirections of gaze in the palsied and normal orbits of sevensubjects with unilateral SO palsy. The cross-sectional area ofthe normal SO muscle decreased in up gaze, and the planeof maximum cross-sectional area moved anteriorly. In downgaze, the plane of maximum cross-sectional area moved pos-teriorly. For palsied muscles, the cross-sectional area wassignificantly smaller (P < 0.005).
sectional area. In addition, as in recti muscles, thecontractile changes in the SO occurred in the poste-rior extent of the muscle, deep in the orbit. This lastfinding was not surprising because the anterior por-tion of the SO is tendinous.
The findings in SO palsy were consistent: The pal-sied muscle was either absent altogether or was sig-nificantly smaller than normal and did not exhibitnormal contractile changes in up and down gaze. Inevery case, the cross-sectional areas in primary gaze ofclinically palsied SO muscles were below the normalrange when assessed at the antero-posterior positionin the orbit where the normal maximum occurs. Thesmall size of palsied SO muscles is perhaps due tochronic denervation atrophy15"17 and is consistentwith findings by Horton and collaborators9 of anatrophic SO muscle demonstrated by conventionalMRI. In monkeys subjected to experimental intracra-nial oculomotor nerve section by Porter and associ-ates,17 the mean cross-sectional area of the orbital sin-gly and multiply innervated fibers of the medial rectusmuscle reached a nadir of approximately 50% of con-trol at 4 months from the time of lesion, whereasglobal multiply innervated fibers were virtually unaf-fected by denervation. In the monkey denervationstudy, the mean cross-sectional area for all fiber typesreached asymptote of 75% to 80% of control in ani-mals in which only limited reinnervation occurred.
In the small sample of cases of SO palsy studiedhere, the functional anatomy of the muscles exhibitedthree patterns: complete absence, diffuse atrophy, andsegmental posterior atrophy with anterior hypertro-phy. The anterior hypertrophy observed in subject 1
is consistent with dynamic damage or denervation ofthe SO muscle. Porter and colleagues17 observed thatthere was hypertrophy to 156% of control cross-sec-tional area following spontaneous reinnervation afterexperimental oculomotor nerve section. This suggeststhat trauma in subject 1 may have permanently dener-vated only the most posterior part of the muscle andthat the anterior part may have become reinnervatedand hypertrophic. Extraocular muscle hypertrophyalso occurs in the acute phase of denervation as aconsequence of vacuolization and organelle disper-sion, but in experimental denervation in the primate,this resolved within 2 months of denervation.17 In theother patients with SO palsy reported here, the in-volved muscle was uniformly small or absent. Presum-ably, the variation in degree of binocular misalign-ments observed in these subjects resulted from factorsin addition to simple SO weakness, most likely innerva-tional factors,18"20 and secondary mechanical changesin SO connective tissues21 and the other extraocularmuscles.22
Surface-coil MRI, as described here, is sufficientlysensitive to demonstrate the normal pattern of SOcontractility. It is thus easy to demonstrate atrophyand absence of contractility in SO palsy. It is proposedthat such objective findings provide direct proof ofthe diagnosis of SO palsy. We report elsewhere thatsometimes hypertropia simulates many of the classicalclinical findings of SO palsy, but MRI confirms normalSO size and contractility.23 This observation shouldnot be surprising because it is likely that after transienttraumatic or ischemic denervation of the SO muscle,hypertropia may be perpetuated by mechanical or in-nervational factors despite recovery of SO contractil-ity. Indeed, biomechanical modeling indicates thatchanges of <10% in resting lengths of certain rectiand oblique muscles, each contracting normally, canproduce patterns of binocular misalignment clinicallytypical of SO palsy.23
There are some intriguing implications for the diag-nosis and management of acute, traumatic SO palsies.Although contractility can be expected to be lost immedi-ately after traumatic denervation, it is unclear how quicklymuscle atrophy develops in the human SO muscle. Datain the medial rectus muscles of monkeys subjected tooculomotor section suggest that the initial phase of dener-vation hypertrophy observed at 1 month gives way to sig-nificant atrophy by 2 months, although atrophy was muchmore profound by 4 months.17 Further, recovery of SOsize and contractility is expected with die common sponta-neous reinnervation of the SO muscle. In the monkeydenervation study, reinnervation was associated widi sig-nificant medial rectus hypertrophy at 6 months,17 al-though resolution of this hypertrophy at later times seemsa possibility. It is unknown if the human SO muscle re-sponds to denervation in the same manner as the primate
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933185/ on 06/20/2018

Superior Oblique Imaging 913
V
medial rectus. Adequate evaluation of the time course ofrecovery of SO size and contractility would require serialimaging studies that have not yet been performed, al-though normal SO contractility and size have been ob-served in one patient 3 months after spontaneous recov-ery from a traumatic SO palsy (Demer, unpublished data,1993). Further study is required to determine if MRI canbe useful in ascertaining die likelihood and completionof spontaneous recovery from SO palsy.
Key Words
extraocular muscle, magnetic resonance imaging, neuro-ophthalmology, strabismus, superior oblique muscle
Acknowledgments
The authors thank Laura Hovis and Mary Johnstone forassistance with magnetic resonance imaging. The public do-main NIH Image program was written by Wayne Rasbandat the U.S. National Institutes of Health and is available fromthe Internet by anonymous ftp from zippy.nimh.nih.gov oron floppy disk from NTIS, 5285 Port Royal Road, Spring-field, VA 22161, part number PB93-504868.
References
1. Miller JM, Robinson DA. A model of the mechanicsof binocular alignment. Compul Biomed Res. 1984; 17:436-470.
2. Neetens A, Janssens M. The superior oblique: A chal-lenging extraocular muscle. Doc Ophthalmol. 1979;46:295-303.
3. Burgerman RS, Wolf AL, Kelman SE, et al. Traumatictrochlear nerve palsy diagnosed by magnetic reso-nance imaging: Case report and review of the litera-ture. Neurosurgery. 1989; 25:978-981.
4. Adler FH. Physiologic factors in differential diagnosisof paralysis of superior rectus and superior obliquemuscles. Arch Ophthalmol. 1946; 36:661-673.
5. Simonsz HJ, Harting F, de Waal BJ, Verbeeten BWJM.Sideways displacement and curved path of the rectieye muscle. Arch Ophthalmol. 1985; 103:124-128.
6. Miller JM. Functional anatomy of normal human rec-tus muscles. Vision Res. 1989;29:223-240.
7. Demer JL, Miller JM, Rosenbaum AL. Clinical correla-tions of models of orbital statics. In: Scott AB, ed.Mechanics of Strabismus. San Francisco: Smith-Ket-tlewell Eye Research Institute; 1992:141-161.
8. Nishida Y, Hayashi O, Nishida E, et al. [Volume mea-surement of the horizontal extraocular muscles usingmagnetic resonance imaging]. Act Soc OphthalmolJa-ponicae. 1993;97:827-833. In Japanese, with Englishabstract.
9. Horton JC, Tsai RK, Truwit CL, Hoyt WF. Magneticresonance imaging of superior oblique muscle atro-
phy in acquired trochlear nerve palsy [letter]. Am JOphthalmol. 1990; 110:315-316.
10. Ellis FD, Helveston EM. Superior oblique palsy: Diag-nosis and classification. Int Ophthalmol Clin. 1976;16:127-135.
11. Flanders M, Draper J. Superior oblique palsy: Diagno-sis and treatment. Can J Ophthalmol. 1990; 25:17-24.
12. Parks MM, Mitchel PR. Cranial nerve palsies. In: Tas-man EW, Jaeger EA, eds. Duane's Clinical Ophthalmol-ogy- Vol. 1. Philadelphia: Lippincott; 1991:5-12.
13. Miller JM, Demer JL, Rosenbaum AL. Effect of trans-position surgery on rectus muscle paths by magneticresonance imaging. Ophthalmology. 1993; 100:475-487.
14. Koo EY, Miller JM, Demer JL. MRI demonstrates nor-mal contractility of superior rectus (SR) and inferiorrectus (IR) in orbits with hypertropia. Ophthalmology.1993;100(9A):119.
15. Baker RS, Milieu AJ, Young AB, Marksberry WR. Ef-fects of chronic denervation on the histology of canineextraocular muscle. Invest Ophthalmol Vis Sci. 1982;22:701-705.
16. Engel AG, Stonnington HH. Morphological effects ofdenervation of muscle: A quantitative ultrastructuralstudy. Ann NY A cad Sci. 1974; 228:68-88.
17. Porter JD, Burns LA, McMahon EJ. Denervation ofprimate extraocular muscle: A unique pattern of struc-tural alteractions. Invest Ophthalmol Vis Sci. 1989;30:1894-1908.
18. Ohtsuki H, Kishimoto F, Kobashi R, et al. [Motor ad-aptation in the Bielschowsky head-tilt test in cases ofsuperior oblique palsy]. Ada Soc OphthalmolJaponicae.1992;96:1055-1060.
19. Robinson DA. Bielschowsky head-tilt test: II: Quantita-tive mechanics of the Bielschowsky head-tilt test. VisionRes. 1985;25:1983-1988.
20. Simonsz HJ, Crone RA, van der Meer J, et al.Bielschowsky head-tilt test: I: Ocular counterrollingand Bielschowsky head-tilt test in twenty-three casesof superior oblique palsy. Vision Res. 1985; 25:1977-1982.
21. Goldspink G, Williams P. Cellular mechanisms in-volved in the determination of muscle length andmass during growth: Problems arising from imbalancebetween antagonist muscle groups. In: Scott AB, ed.Proceedings of the Mechanics of Strabismus Symposium. SanFrancisco: Smith-Ketdewell Eye Research Institute:1992; 195-206.
22. Scott AB, Kraft SP. Botulinum toxin injection in themanagement of lateral rectus paresis. Ophthalmology.1985;92:676-683.
23. Demer JL, Miller JM, Koo EY, et al. True versus masqu-erading superior oblique palsies: Muscle mechanismsrevealed by magnetic resonance imaging. In: Lenner-strand G, ed. Update on Strabismus andPediatric Ophthal-mology. Boca Raton: CRC Press; 1995:in press.
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933185/ on 06/20/2018