M21-A Methodology for the Serum Bactericidal Test ...
51
M21-A Vol. 19 No. 17 Replaces M21-T September 1999 Vol. 12 No. 19 Methodology for the Serum Bactericidal Test; Approved Guideline This document provides a direct method of antimicrobial susceptibility testing using serum obtained from the patient to measure the activity of the serum against the bacterial pathogen isolated from the patient. ABC
Transcript of M21-A Methodology for the Serum Bactericidal Test ...
M21-AVol. 19 No. 17Replaces M21-T
September 1999 Vol. 12 No. 19
Methodology for the Serum Bactericidal Test;Approved Guideline
This document provides a direct method of antimicrobial susceptibility testing using serum obtainedfrom the patient to measure the activity of the serum against the bacterial pathogen isolated from thepatient.
ABC

NCCLS...Serving the World's Medical Science Community Through Voluntary Consensus
NCCLS is an international, interdisciplinary, nonprofit,standards-developing, and educational organization thatpromotes the development and use of voluntaryconsensus standards and guidelines within the healthcarecommunity. It is recognized worldwide for the applicationof its unique consensus process in the development ofstandards and guidelines for patient testing and relatedhealthcare issues. NCCLS is based on the principle thatconsensus is an effective and cost-effective way toimprove patient testing and healthcare services.
In addition to developing and promoting the use ofvoluntary consensus standards and guidelines, NCCLSprovides an open and unbiased forum to address criticalissues affecting the quality of patient testing and healthcare.
PUBLICATIONS
An NCCLS document is published as a standard,guideline, or committee report.
Standard A document developed through the consensusprocess that clearly identifies specific, essentialrequirements for materials, methods, or practices for usein an unmodified form. A standard may, in addition,contain discretionary elements, which are clearlyidentified.
Guideline A document developed through the consensusprocess describing criteria for a general operatingpractice, procedure, or material for voluntary use. Aguideline may be used as written or modified by the userto fit specific needs.
Report A document that has not been subjected toconsensus review and is released by the Board ofDirectors.
CONSENSUS PROCESS
The NCCLS voluntary consensus process is a protocolestablishing formal criteria for:
• the authorization of a project
• the development and open review of documents
• the revision of documents in response to commentsby users
• the acceptance of a document as a consensusstandard or guideline.
Most NCCLS documents are subject to two levels ofconsensus- "proposed" and "approved." Depending on
the need for field evaluation or data collection, documentsmay also be made available for review at an intermediate(i.e., "tentative") consensus level.
Proposed An NCCLS consensus document undergoes thefirst stage of review by the healthcare community as aproposed standard or guideline. The document should receivea wide and thorough technical review, including an overallreview of its scope, approach, and utility, and a line-by-linereview of its technical and editorial content.
Tentative A tentative standard or guideline is made availablefor review and comment only when a recommended methodhas a well-defined need for a field evaluation or when arecommended protocol requires that specific data becollected. It should be reviewed to ensure its utility.
Approved An approved standard or guideline has achievedconsensus within the healthcare community. It should bereviewed to assess the utility of the final document, toensure attainment of consensus (i.e., that comments onearlier versions have been satisfactorily addressed), and toidentify the need for additional consensus documents.
NCCLS standards and guidelines represent a consensusopinion on good practices and reflect the substantialagreement by materially affected, competent, and interestedparties obtained by following NCCLS’s establishedconsensus procedures. Provisions in NCCLS standards andguidelines may be more or less stringent than applicableregulations. Consequently, conformance to this voluntaryconsensus document does not relieve the user ofresponsibility for compliance with applicable regulations.
COMMENTS
The comments of users are essential to the consensusprocess. Anyone may submit a comment, and all commentsare addressed, according to the consensus process, by theNCCLS committee that wrote the document. All comments,including those that result in a change to the documentwhen published at the next consensus level and those thatdo not result in a change, are responded to by the committeein an appendix to the document. Readers are stronglyencouraged to comment in any form and at any time on anyNCCLS document. Address comments to the NCCLSExecutive Offices, 940 West Valley Road, Suite 1400,Wayne, PA 19087, USA.
VOLUNTEER PARTICIPATION
Healthcare professionals in all specialties are urged tovolunteer for participation in NCCLS projects. Pleasecontact the NCCLS Executive Offices for additionalinformation on committee participation.

Vol. 19 No. 17 M21-A
i
Methodology for the Serum Bactericidal Test;Approved Guideline
Abstract
Bactericidal testing methods occasionally are used because of the awareness of the need for lethalantimicrobial activity to treat certain deep-seated infections, e.g., bacterial endocarditis. There also isan increased awareness of the need to consider the pharmacodynamic and pharmacokinetic principlesof antimicrobial therapy. This often can be achieved by assessing both results of standardizedsusceptibility testing and of antimicrobial assays. The serum bactericidal test represents an alternativein vitro test that incorporates pharmacodynamic and pharmacokinetic principles. The test takes intoconsideration the susceptibility of the pathogen; measures the combined effect of absorption andelimination of the antibiotic; the binding of the drug to serum proteins; and the effect of the parentcompound as well as any metabolites against the infecting organism. This assay also measures theeffect of drug interactions. This includes both the synergistic or antagonistic effects of antibioticcombinations and the interactions of other drugs with antibiotics. Finally, the serum bactericidal test,by measuring the magnitude of antibiotic concentration relative to the MBC, allows a prediction of theaggregate time of bactericidal activity. Peak serum bactericidal titers of > 8, for example, assuremeasurable bactericidal activity in the serum for at least three half-lives of the drug being tested. Despite all of these potential advantages, the serum bactericidal test rarely is needed. Although the testprovides another predictive estimate of bacterial eradication, clinical cure depends largely upon hostfactors and other factors, e.g., postantibiotic effect and the growth-inhibitory effects of sub-MICconcentrations of antibiotics. When needed, however, established, reproducible methods should beavailable to the clinical, reference, and/or research laboratory.
(NCCLS. Methodology for the Serum Bactericidal Test; Approved Guideline. NCCLS document M21-A[ISBN 1-56238-383-3]. NCCLS, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 19087 USA,1999.)
THE NCCLS consensus process, which is the mechanism for moving a documentthrough two or more levels of review by the healthcare community, is an ongoingprocess. Users should expect revised editions of any given document. Becauserapid changes in technology may affect the procedures, methods, and protocols ina standard or guideline, users should replace outdated editions with the currenteditions of NCCLS documents. Current editions are listed in the NCCLS Catalog,which is distributed to member organizations, and to nonmembers on request. Ifyour organization is not a member and would like to become one, and to requesta copy of the NCCLS Catalog, contact the NCCLS Executive Offices. Telephone:610.688.0100; Fax: 610.688.0700; E-Mail: [email protected]

September 1999 NCCLS
ii

M21-AISBN 1-56238-383-3
September 1999 ISSN 0273-3099
Methodology for the Serum Bactericidal Test;Approved Guideline
Volume 19 Number 17
Arthur L. Barry, Ph.D.William A. Craig, M.D.Harriette Nadler, Ph.D.L. Barth Reller, M.D.Christine C. Sanders, Ph.D.Jana M. Swenson, M.M.Sc.
ABC

September 1999 NCCLS
iv
This publication is protected by copyright. No part of it may be reproduced, stored in a retrieval system,or transmitted in any form or by any means (electronic, mechanical, photocopying, recording, orotherwise) without written permission from NCCLS, except as stated below.
NCCLS hereby grants permission to reproduce limited portions of this publication for use in laboratoryprocedure manuals at a single site, for interlibrary loan, or for use in educational programs provided thatmultiple copies of such reproduction shall include the following notice, be distributed without charge,and, in no event, contain more than 20% of the document's text.
Reproduced with permission, from NCCLS publication M21-A— Methodology for theSerum Bactericidal Test; Approved Guideline. Copies of the current edition may beobtained from NCCLS, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 19087 USA.
Permission to reproduce or otherwise use the text of this document to an extent that exceeds theexemptions granted here or under the Copyright Law must be obtained from NCCLS by written request.To request such permission, address inquiries to the Executive Director, NCCLS, 940 West Valley Road,Suite 1400, Wayne, Pennsylvania 19087 USA.
Copyright ©1999. The National Committee for Clinical Laboratory Standards.
Suggested Citation
(NCCLS. Methodology for the Serum Bactericidal Test; Approved Guideline. NCCLS document M21-A[ISBN 1-56238-383-3]. NCCLS, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 19087 USA,1999.)
Proposed GuidelineJanuary 1987
Tentative GuidelineSeptember 1992
Approved GuidelineSeptember 1999
ISBN 1-56238-383-3ISSN 0273-3099

Vol. 19 No. 17 M21-A
v
Committee Membership
Area Committee on Microbiology
James H. Jorgensen, Ph.D. University of Texas Health Science BranchChairholder San Antonio, Texas
Melvin P. Weinstein, M.D. Robert Wood Johnson Medical SchoolVice-Chairholder New Brunswick, New Jersey
Arthur L. Barry, Ph.D. Clinical Microbiology InstituteWilsonville, Oregon
Sharon L. Hansen, Ph.D. Food and Drug AdministrationRockville, Maryland
Stephen G. Jenkins, Ph.D. Mt. Sinai Medical CenterNew York, New York
J. Michael Miller, Ph.D. Centers for Disease Control and PreventionAtlanta, Georgia
Jeffrey L. Watts, M.S., R.M.(AAM) Pharmacia & Upjohn Animal HealthKalamazoo, Michigan
Advisors
Ellen Jo Baron, Ph.D. Stanford Hospital & ClinicsStanford, California
Stanley Bauer, M.D. Beth Israel Medical CenterNew York, New York
Gary V. Doern, Ph.D. University of IowaIowa City, Iowa
George L. Evans, Ph.D. White Haven, Pennsylvania
Mary Jane Ferraro, Ph.D. Massachusetts General HospitalBoston, Massachusetts
John N. Galgiani, M.D. VA Medical CenterTuscon, Arizona
Lynne S. Garcia, M.S. UCLA Medical CenterLos Angeles, California
Richard L. Hodinka, Ph.D. Children’s Hospital of PhiladelphiaPhiladelphia, Pennsylvania
Michael A. Pfaller, M.D. University of Iowa College of MedicineIowa City, Iowa
Robert P. Rennie, Ph.D. University of Alberta HospitalEdmonton, Alberta

September 1999 NCCLS
vi
Thomas R. King, M(ASCP) NCCLSStaff Liaison Wayne, Pennsylvania
Patrice E. Polgar NCCLSEditor Wayne, Pennsylvania
Donna M. Wilhelm NCCLSAssistant Editor Wayne, Pennsylvania
Acknowledgments
Special recognition is given to the following persons whose help with the development of this documentwas extremely valuable:
William A. Craig, M.D. William S. Middleton VA HospitalMadison, Wisconsin
Harriette Nadler, Ph.D. Rhône-Poulenc RorerCollegeville, Pennsylvania
L. Barth Reller, M.D. Duke University Medical CenterDurham, North Carolina
Christine C. Sanders, Ph.D. Creighton University School of MedicineOmaha, Nebraska
Jana M. Swenson, M.M.Sc. Centers for Disease Control and PreventionAtlanta, Georgia

Vol. 19 No. 17 M21-A
vii
ACTIVE MEMBERSHIP (as of 1 July 1999)
Sustaining Members
Abbott LaboratoriesAmerican Association for Clinical ChemistryBayer CorporationBeckman Coulter, Inc.Becton Dickinson and CompanybioMérieux, Inc.College of American PathologistsDade Behring Inc.Nippon Becton Dickinson Co, Ltd.Ortho-Clinical Diagnostics, Inc.Pfizer IncRoche Diagnostics, Inc.
Professional Members
American Academy of Family PhysiciansAmerican Association of BioanalystsAmerican Association of Blood BanksAmerican Association for Clinical ChemistryAmerican Association for Respiratory CareAmerican Chemical SocietyAmerican Medical TechnologistsAmerican Public Health AssociationAmerican Society for Clinical Laboratory ScienceAmerican Society of HematologyAmerican Society for MicrobiologyAmerican Society of Parasitologists, Inc.American Type Culture Collection, Inc.Asociación Española Primera de Socorros (Uruguay)Asociacion Mexicana de Bioquimica Clinica A.C.Assn. of Public Health LaboratoriesAssoc. Micro. Clinici Italiani- A.M.C.L.I.Australasian Association of Clinical BiochemistsBritish Society for Antimicrobial ChemotherapyCanadian Society for Medical Laboratory ScienceCSociété Canadienne de Science de Laboratoire Médical
Canadian Society of Clinical ChemistsClinical Laboratory Management AssociationCollege of American PathologistsCollege of Medical Laboratory Technologists of OntarioCollege of Physicians and Surgeons of SaskatchewanCommission on Office Laboratory AccreditationDanish Society of Clinical ChemistryFundacion Bioquimica de la Provincia (Argentina)International Association of Medical Laboratory TechnologistsInternational Council for Standardization in HaematologyInternational Federation of Clinical ChemistryInternational Society for Analytical CytologyItalian Society of Clinical BiochemistryJapan Society of Clinical ChemistryJapanese Committee for Clinical Laboratory StandardsJoint Commission on Accreditation of Healthcare OrganizationsNational Academy of Clinical BiochemistryNational Society for Histotechnology, Inc.Ontario Medical Association Laboratory Proficiency Testing ProgramOrdre professionnel des technologistes médicaux du QuébecRCPA Quality Assurance Programs PTY LimitedSociedade Brasileira de Analises ClinicasSociedade Brasileira de Patologia ClinicaSociedad Espanola de Quimica ClinicaVKCN (The Netherlands)
Government Members
Armed Forces Institute of PathologyAssociation of Public Health Laboratory DirectorsBC Centre for Disease ControlCenters for Disease Control and PreventionChinese Committee for Clinical Laboratory StandardsCommonwealth of Pennsylvania Bureau of LaboratoriesDepartment of Veterans AffairsDeutsches Institut für Normung (DIN)FDA Center for Devices and Radiological HealthFDA Division of Anti-Infective Drug ProductsHealth Care Financing AdministrationIowa State Hygienic LaboratoryMassachusetts Department of Public Health LaboratoriesMichigan Department of Public HealthNational Association of Testing Authorities - AustraliaNational Center of Infectious and Parasitic Diseases (Bulgaria)National Institute of Standards and TechnologyOhio Department of HealthOklahoma State Department of HealthOntario Ministry of HealthSaskatchewan Health- Provincial LaboratorySouth African Institute for Medical ResearchSwedish Institute for Infectious Disease Control
Industry Members
AB BiodiskAbbott LaboratoriesAccuMed International, Inc.Accumetrics, Inc.Amersham Pharmacia BiotechAmmirati Regulatory ConsultingAsséssorAstraZenecaAvocet Medical, Inc.Bayer Corporation - Elkhart, INBayer Corporation - Middletown, VA

September 1999 NCCLS
viii
Bayer Corporation - Tarrytown, NYBayer Corporation - West Haven, CTBayer Medical Ltd.Beckman Coulter, Inc.Beckman Coulter, Inc. Primary Care DiagnosticsBeckman Coulter K.K. (Japan)Becton Dickinson and CompanyBecton Dickinson BiosciencesBecton Dickinson Consumer ProductsBecton Dickinson Immunocytometry SystemsBecton Dickinson Italia S.P.A.Becton Dickinson VACUTAINER SystemsbioMérieux, Inc.Biometrology ConsultantsBio-Rad Laboratories, Inc.Biotest AGBristol-Myers Squibb CompanyCanadian Reference Laboratory Ltd.CASCO$NERL DiagnosticsCheckpoint Development Inc.Chiron Diagnostics Corporation - International OperationsChiron Diagnostics Corporation - Reagent SystemsClinical Lab EngineeringCOBE Laboratories, Inc.Combact Diagnostic Systems Ltd.Community Medical Center (NJ)Control Lab (Brazil)Cosmetic Ingredient ReviewCubist PharmaceuticalsCytometrics, Inc.Dade Behring Inc. - Deerfield, ILDade Behring Inc. - Glasgow, DEDade Behring Inc. - Marburg, GermanyDade Behring Inc. - Miami, FLDade Behring Inc. - Sacramento, CADade Behring Inc. - San Jose, CADAKO A/SDiagnostic Products CorporationDiaSorinEiken Chemical Company, Ltd.Enterprise Analysis CorporationFort Dodge Animal HealthGen-ProbeGlaxo-Wellcome, Inc.Greiner Meditech, Inc.Health Systems Concepts, Inc.Helena LaboratoriesHycor Biomedical Inc.I-STAT Corporation
Instrumentation LaboratoryInteg, Inc.International Technidyne CorporationJohnson City Medical CenterKendall Sherwood-Davis & GeckLabtest Diagnostica S.A.LifeScan, Inc. (a Johnson & Johnson Company)LifeSign, LLCLilly Research LaboratoriesMedical Device Consultants, Inc.Medical Laboratory Automation Inc.MediSense Products (Div. Of Abbott Laboratories)Medtronic Perfusion SystemsMerck & Company, Inc.NabiNeometrics Inc.Nichols Institute Diagnostics (Div. of Quest Diagnostics, Inc.)Nissui Pharmaceutical Co., Ltd.Nippon Becton Dickinson Co., Ltd.Norfolk Associates, Inc.OBC AssociatesOlympus CorporationOptical Sensors, Inc.Organon Teknika CorporationOrtho-Clinical Diagnostics, Inc. (England)Ortho-Clinical Diagnostics, Inc. (Raritan, NJ)Ortho-Clinical Diagnostics, Inc. (Rochester, NY)Oxoid Inc.Oxoid LTD (U.K.)Pfizer IncPharmacia & Upjohn Procter & Gamble Pharmaceuticals, Inc.The Product Development GroupQuintiles, Inc.Radiometer America, Inc.Radiometer Medical A/SDavid G. Rhoads Associates, Inc.Rhône-Poulenc RorerRoche Diagnostics GmbHRoche Diagnostics, Inc.Roche Diagnostic Systems (Div. Hoffmann-La Roche Inc.)Roche Laboratories (Div. Hoffmann-La Roche Inc.)The R.W. Johnson Pharmaceutical Research InstituteSanofi Diagnostics PasteurSarstedt, Inc.
SARL Laboratoire Carron (France)Schering CorporationSchleicher & Schuell, Inc.Second OpinionSenDx Medical, Inc.Showa Yakuhin Kako Company, Ltd.SmithKline Beecham CorporationSmithKline Beecham, S.A.Streck Laboratories, Inc.Sysmex Corporation (Japan)Sysmex Corporation (Long Grove, IL)The Toledo Hospital (OH)Vetoquinol S.A.Vysis, Inc.Wallac OyWarner-Lambert CompanyWyeth-AyerstXyletech Systems, Inc.YD Consultant
Trade Associations
Association of Medical Diagnostic ManufacturersHealth Industry Manufacturers AssociationJapan Association Clinical Reagents Ind. (Tokyo, Japan)Medical Industry Association of Australia
Associate Active Members
20th Medical Group (Shaw AFB, SC)67th CSH Wuerzburg, GE (NY)121st General Hospital (CA)Acadiana Medical Laboratories, LTD (LA)Advocate Laboratories (IL)The Aga Khan University Medical Center (Pakistan)Allegheny General Hospital (PA)Allegheny University of the Health Sciences (PA)Allina Laboratories (MN)Alton Ochsner Medical Foundation (LA)Anzac House (Australia)Associated Regional & University Pathologists (UT)Aurora Consolidated Laboratories (WI)Baptist St. Anthony=s Health Network (TX)Baystate Medical Center (MA)Brazileiro De Promocao (Brazil)
Vol. 19 No. 17 M21-A
ix
Bristol Regional Medical Center (TN)Brookdale Hospital Medical Center (NY)Brooke Army Medical Center (TX)Brooks Air Force Base (TX)Broward General Medical Center (FL)Calgary Laboratory Services (Calgary, AB, Canada)Cardinal Glennon Children=s Hospital (MO)Central Kansas Medical CenterChamplain Valley Physicians Hospital (NY)Children=s Hospital (LA)Children's Hospital Medical Center (Akron, OH)Clendo Lab (Puerto Rico)CLSI Laboratories (PA)Colorado Mental Health Institute at PuebloColumbia Tulsa Regional Medical Center (OK)Commonwealth of KentuckyCompuNet Clinical Laboratories (OH)Consolidated Laboratory Services (CA)Danville Regional Medical Center (VA)Dean Medical Center (WI)Detroit Health Department (MI)Duke University Medical Center (NC)Durham Regional Hospital (NC)Duzen Laboratories (Turkey)Dynacare Laboratories - Eastern Region (Ottawa, ON, Canada)E.A. Conway Medical Center (LA)East Texas Medical CenterElmhurst Memorial Hospital (IL)Emory University Hospital (GA)Fairfax Hospital (VA)Fairview-University Medical Center (MN)Foothills Hospital (Calgary, AB, Canada)Fox Chase Cancer Center (PA)Fresenius Medical Care/Life Chem (NJ)Fresno Community Hospital and Medical CenterGDS Technology, Inc (IN)Grady Memorial Hospital (GA)Greater Southeast Community Hospital (DC)Guthrie Clinic Laboratories (PA)Halifax Medical Center (FL)Harris Methodist Fort Worth (TX)
Harris Methodist Northwest (TX)Hartford Hospital (CT)Hays Pathology Laboratories, P.A. (KS)Headwaters Health Authority (High River, AB, Canada)Health Alliance Laboratory (OH)Health Network Lab (PA)Health Sciences Centre (Winnipeg, MB, Canada)Heartland Health System (MO)Hinsdale Hospital ((L)Hoag Memorial Hospital Presbyterian (CA)Holmes Regional Medical Center (FL)Holy Spirit Hospital (PA)Holzer Medical Center (OH)Hospital for Sick Children (Toronto, ON, Canada)Huddinge University Hospital (Sweden)Hunter Area Pathology Service (Australia)Hurley Medical Center (MI)Instituto Scientifico HS. Raffaele (Italy)International Health Management Associates, Inc. (IL)Intermountain Health Care Laboratory Services (UT)Jacobi Medical Center (NY)John Randolph Hospital (VA)Johns Hopkins Medical Institutions (MD)Johnson City Medical Center (IN)Kaiser Permanente (CA)Kenora-Rainy River Regional Laboratory Program (Dryden, Ontario, Canada)Klinicni Center (Slovenia)LabCorp (NC)Laboratoire de Santé Publique du Quebec (Canada)Laboratório Fleury S/C Ltda. (Brazil)Lancaster General Hospital (PA)Langley Air Force Base (VA)Lewis-Gale Medical Center (VA)Libero Instituto Univ. Campus BioMedico (Italy)Loma Linda University Medical Center (CA)Los Angeles County and USC Medical Center (CA)Louisiana State University Medical CenterLutheran Hospital (WI)Main Line Clinical Laboratories, Inc. (PA)
Massachusetts General HospitalMDS Metro Laboratory Services (Burnaby, BC, Canada)MDS-Sciex (Concord, ON, Canada)Medical College of Virginia HospitalMelrose-Wakefield Hospital (MA)Memorial Medical Center (LA)Memorial Medical Center (IL)Mercy Health System (PA)Mercy Hospital (NC)Methodist Hospital (TX)Methodist Hospital IndianaMethodist Hospitals of Memphis (TN)Mid Michigan Medical Center - MidlandMilton S. Hershey Medical Center (PA)Mississippi Baptist Medical CenterMonte Tabor-Centro Italo- Brazileiro De Promocao (Brazil)Montreal Children=s Hospital (Canada)Mount Sinai Hospital (NY)National University Hospital (Singapore)Naval Surface Warfare Center (IN)Nebraska Health SystemNew Britain General Hospital (CT)New England Medical Center Hospital (MA)The New York Blood CenterThe New York Hospital Medical Center of QueensNew York State Department of HealthNorDx (ME)North Carolina Laboratory of Public HealthNorth Coast Clinical Laboratory, Inc. (OH)Northridge Hospital Medical Center (CA)North Shore University Hospital (NY)Northwestern Memorial Hospital (IL)Ohio State University HospitalsOlin E. Teague Medical Center (TX)Our Lady of Lourdes Hospital (NJ)Our Lady of the Resurrection Medical Center (IL)Pathology and Cytology Laboratories, Inc. (KY)

September 1999 NCCLS
x
Permanente Medical Group (CA)Presbyterian Hospital of Dallas (TX)Providence Health System (OR)Providence Medical Center (WA)Queen Elizabeth Hospital (Prince Edward Island, Canada)Queensland Health Pathology Services (Australia)Quintiles Laboratories, Ltd. (GA)Regions HospitalResearch Medical Center (MO)Riyadh Armed Forces Hospital (Saudi Arabia)Robert F. Kennedy Medical Center (CA)Saint Mary=s Regional Medical Center (NV)Santa Clara Valley Medical Center (CA)St. Alexius Medical Center (ND)St. Anthony Hospital (CO)St. Boniface General Hospital (Winnipeg, Canada)St. Francis Medical Center (CA)St. John Hospital and Medical Center (MI)St. John Regional Hospital (St. John, NB, Canada)St. Joseph Hospital (NE)St. Joseph=s Hospital - Marshfield Clinic (WI)St. Luke=s Hospital (PA)St. Luke=s Regional Medical Center (IA)St. Luke=s-Roosevelt Hospital Center (NY)St. Mary Hospital (NJ)St. Mary Medical Center (CA)St. Mary Medical Center (IN)St. Mary of the Plains Hospital (TX)SARL Laboratoire Carron (France)San Francisco General Hospital (CA)Seoul Nat=l University Hospital (Korea)Shanghai Center for the Clinical Laboratory (China)Shands Healthcare (FL)SmithKline Beecham Clinical Laboratories (GA)SmithKline Beecham Clinical Laboratories (WA)South Bend Medical Foundation (IN)
Southern California Permanente Medical GroupSouth Western Area Pathology Service (Australia)Speciality Laboratories, Inc. (CA)Stanford Health Services (CA)Stormont-Vail Regional Medical Center (KS)Sun Health-Boswell Hospital (AZ)Sunrise Hospital and Medical Center (NV)Sutter Health (CA)Timmins & District Hospital (Timmons, ON, Canada)Tri-City Medical Center (CA)Tripler Army Medical Center (HI)Trumbull Memorial Hospital (OH)Tulane Medical Center Hospital & Clinic (LA)Twin Lake Regional Medical CenterUCSF Medical Center (CA)UNC Hospitals (NC)Unilab Clinical Laboratories (CA)University of Alabama - Birmingham HospitalUniversity of Alberta Hospitals (Canada)University of Chicago Hospitals (IL)University Hospital (IN)University Hospital (Gent) (Belgium)University Hospital (London, Ontario, Canada)University Hospital of Cleveland (OH)The University Hospitals (OK)University of Medicine & Dentistry, NJ University HospitalUniversity of MichiganUniversity of the Ryukyus (Japan)University of Texas Medical School at HoustonUniversity of Virginia Medical CenterUniversity of WashingtonUPMC Bedford Memorial (PA)USAF Medical Center (OH)UZ-KUL Medical Center (Belgium)VA (Dayton) Medical Center (OH)VA (Denver) Medical Center (CO)
VA (Kansas City) Medical Center (MO)VA Outpatient Clinic (OH)VA (San Diego) Medical Center (CA)VA (Tuskegee) Medical Center (AL)Vejle Hospital (Denmark)Viridae Clinical Sciences, Inc. (Vancouver, BC, Canada)ViroLogic, Inc. (CA)Waikato Hospital (New Zealand)Walter Reed Army Institute of Research (MD)Warde Medical Laboratory (MI)Warren Hospital (NJ)Washoe Medical Center (NV)Watson Clinic (FL)Williamsburg Community Hospital (VA)Wilford Hall Medical Center (TX)Wilson Memorial Hospital (NY)Winchester Hospital (MA)Winn Army Community Hospital (GA)Wishard Memorial Hospital (IN)Yonsei University College of Medicine (Korea)York Hospital (PA)Zale Lipshy University Hospital (TX)

Vol. 19 No. 17 M21-A
xi
OFFICERS BOARD OF DIRECTORS
William F. Koch, Ph.D., PresidentNational Institute of Standards and Technology
F. Alan Andersen, Ph.D., President ElectCosmetic Ingredient Review
Robert F. Moran, Ph.D., FCCM, FAIC Secretarymvi Sciences
Donna M. Meyer, Ph.D., TreasurerCHRISTUS Health
A. Samuel Koenig, III, M.D., Past PresidentFamily Medical Care
John V. Bergen, Ph.D., Executive Director
Sharon S. Ehrmeyer, Ph.D.University of Wisconsin
Robert L. Habig, Ph.D.Becton Dickinson and Company
Thomas L. Hearn, Ph.D.Centers for Disease Control and Prevention
Gerald A. Hoeltge, M.D.The Cleveland Clinic Foundation
Elizabeth D. Jacobson, Ph.D.FDA Center for Devices and Radiological Health
Carolyn D. Jones, J.D., M.P.H.Health Industry Manufacturers Association
Hartmut Jung, Ph.D.Roche Diagnostics GmbH
Tadashi Kawai, M.D., Ph.D.International Clinical Pathology Center
Barbara G. Painter, Ph.D.Bayer Corporation
Marianne C. Watters, M.T.(ASCP)Parkland Health & Hospital System
Ann M. Willey, Ph.D.New York State Department of Health
Judith A. Yost, M.A., M.T. (ASCP)Health Care Financing Administration

September 1999 NCCLS
xii

Vol. 19 No. 17 M21-A
xiii
Contents
Abstract.............................................................................................................................. i
Committee Membership........................................................................................................ v
Active Membership .............................................................................................................vii
Foreword........................................................................................................................... xv
1 Introduction ............................................................................................................... 1
1.1 Principle ........................................................................................................... 11.2 Clinical Relevance .............................................................................................. 11.3 Clinical Use ....................................................................................................... 31.4 Interpretation .................................................................................................... 4
2 Collection of Patient's Serum........................................................................................ 5
2.1 Peak and Trough Levels ...................................................................................... 52.2 Sample Collection and Handling ........................................................................... 52.3 Patient’s Isolate ................................................................................................. 6
3 Serum Dilution Procedure ............................................................................................. 6
3.1 Broth Medium ................................................................................................... 73.2 Dilution Methods ............................................................................................... 83.3 Preparing Inoculum ............................................................................................ 93.4 Inoculating Broth ............................................................................................. 103.5 Incubation ...................................................................................................... 103.6 Determining Endpoints ...................................................................................... 103.7 Interpretation of Bactericidal Dilution Titers .......................................................... 11
4 Area Under the Bactericidal-Titer Curve ........................................................................ 11
5 Serum Bactericidal Rate ............................................................................................. 12
6 Antibiotic Carryover .................................................................................................. 13
7 Quality Control ......................................................................................................... 13
7.1 Purpose .......................................................................................................... 137.2 Selecting Reference Strains ............................................................................... 137.3 Suggested Quality Control Strains ...................................................................... 137.4 Batch or Lot Control ......................................................................................... 137.5 Other Control Procedures .................................................................................. 13
Table 1. Rejection Value and Calculated Sensitivityand Specificity for Each Initial Concentrationon the Basis of Duplicate 0.01-mL Samples ......................................................... 15
Table 2. Rejection Value and Calculated Sensitivity and Specificityfor Each Initial Concentration on the Basis of a Single0.01-mL Sample .............................................................................................. 16

September 1999 NCCLS
xiv
Contents (Continued)
Table 3. Suitable Quality Control Ranges for MICs and MBCs With andWithout Human Serum Using ATCC Strains ......................................................... 17
References ....................................................................................................................... 18
Additional References ......................................................................................................... 21
Summary of Comments and Subcommittee Responses ........................................................... 22
Related NCCLS Publications ................................................................................................ 25

Vol. 19 No. 17 M21-A
xv
Foreword
All of the susceptibility test methods commonly performed by clinical microbiology laboratories (i.e., diskdiffusion, broth dilution, and agar dilution) measure the inhibitory activity (MIC) of an antimicrobialagent.1-3 In most clinical situations, this is sufficient as the role of the antibiotic is to prevent the spreadof bacteria from the focus of infection by preventing microbial replication at new sites: the activeparticipation of the host's defense mechanisms finally achieves bacterial eradication and clinical cure.4
On occasion, it may be necessary to achieve bactericidal activity with an antimicrobial agent. This needhas been well documented for endocarditis5 and has been suggested by some for meningitis6 and forosteomyelitis7, as well as infections in immunocompromised patients.8
When assessment of bactericidal activity is deemed appropriate, an in vitro test method such as theMBC determination or the use of time-kill kinetic methodology may be useful. Bactericidal activityagainst the patient's isolate by the antibiotic tested allows eradication to be predicted based upon theusual dosing of this antibiotic or based upon the results of an antimicrobial assay. When clinicalexperience is lacking and assay methods are not readily available, the serum bactericidal test whichintegrates both pharmacodynamic and pharmacokinetic properties may be more useful. Depending oncertain modifications to the serum bactericidal test, the test can provide a quantitative assessment ofbactericidal activity relative to the MBC (the serum bactericidal titer), a dynamic assessment of rapidityof killing over time (the serum bactericidal rate), or both the magnitude of serum bactericidal activity andits duration (the area-under-the-bactericidal-titer-curve). In addition, methods using serum from persons(e.g., volunteers) receiving antibiotics (ex vivo) can be used to assess antimicrobial bactericidal activityacross drug classes or between members of a class against a wide variety of microorganisms.
Because of the complexity involved with the serum bactericidal test (including the particular methodused, the proper collection of timed serum specimens, and the interpretation of results), and the lackof clinical data clearly documenting the usefulness of this test for most infections, it is recommendedthat consultation with the microbiology laboratory be obtained as a prerequisite for this test. Theassistance of the laboratory's director is useful in (1) determining if such a test is needed; (2) selectingNCCLS recommended methodology for testing; and (3) interpreting the results.
The clinical relevance of the serum bactericidal test remains controversial, and there are relatively fewclinical situations in which the test is indicated. However, the serum bactericidal test is being used involunteers as a tool in the evaluation of new antimicrobial agents. Whatever the reason for performingthe serum bactericidal test, this document describes the details of the test and, in particular, describesthe methodologic variations. This information has been obtained largely from published data. Use ofthese techniques should result in uniform methodology that is practical enough to be used in the clinicalmicrobiology laboratory or in the research setting. The techniques are intended primarily for testingaerobic bacteria that grow well after overnight incubation in Mueller-Hinton broth.
In depth discussion of the factors influencing results of bactericidal tests and techniques for the conductof MBCs and timed-kill studies may be found in the most current edition of NCCLS documentM26SMethods for Determining Bactericidal Activity of Antimicrobial Agents.9
Standard Precautions
Because it is often impossible to know what might be infectious, all human blood specimens are to betreated as infectious and handled according to “standard precautions.” Standard precautions are newguidelines that combine the major features of “universal precautions and body substance isolation”practices. Standard precautions cover the transmission of any pathogen and thus are morecomprehensive than universal precautions which are intended to apply only to transmission of blood-

September 1999 NCCLS
xvi
Foreword (Continued)
borne pathogens. Standard precaution and universal precaution guidelines are available from the U.S.Centers for Disease Control and Prevention (Guideline for Isolation Precautions in Hospitals, InfectionControl and Hospital Epidemiology, CDC, Vol 17;1:53-80.), [MMWR 1987;36(suppl 2S):2S-18S] and(MMWR 1988;37:377-382, 387-388). For specific precautions for preventing the laboratorytransmission of blood-borne infection from laboratory instruments and materials; and recommendationsfor the management of blood-borne exposure, refer to NCCLS document M29—Protection of LaboratoryWorkers from Instrument Biohazards and Infectious Disease Transmitted by Blood, Body Fluids, andTissue.
Key Words
Schlichter test, serum bactericidal test, serum bactericidal titer, serum dilution test

Vol. 19 No. 17 M21-A
1
Methodology for the Serum Bactericidal Test; Approved Guideline
1 Introduction
1.1 Principle
Bacterial eradication by antimicrobial therapy isdetermined both by the pharmacodynamic andpharmacokinetic properties of the antimicrobialagent(s) used.10
The pharmacodynamic properties of anantimicrobial agent are defined as its activity(inhibitory and/or lethal) against microbialpathogens. When this activity is evaluated overa time-concentration continuum, the lethaleffect can be described either as concen-tration-dependent or time-dependent.
Concentration-dependent killing kinetics, asseen with aminoglycosides and fluoro-quinolones, are those in which the rate of killingincreases with increasing drug concen-trationsup to a point of maximum effect. In contrast,time-dependent killing kinetics, as seen with β-lactam agents and vancomycin, are those inwhich the rate of killing is relatively slow andcontinues only as long as the concentrations arein excess of the MIC.
Because both the magnitude and duration of theactivity of the antimicrobial agent can beimportant in determining its bactericidal effect,the pharmacokinetic properties of the agent aswell as the dosing parameters becomeimportant factors in determining the likelihoodof bacterial eradication.
The usual in vitro susceptibility test methodssuch as the MIC-MBC determination or brothtime-kill kinetic methodology do not considerthe pharmacokinetic properties of the agent, butinstead rely upon known pharmacokineticproperties with the usual dosing regimens.Often, an antimicrobial assay can provide thenecessary pharmacokinetic data which can becombined with the susceptibility test result toallow one to predict bacterial eradication. Forcertain infections (such as endocarditis)requiring bactericidal activity, the serumbactericidal test is a method that considers boththe pharmacodynamic and the pharma-cokineticproperties of an antimicrobial agent and can
provide another predictive estimate of bacterialeradication.
The serum bactericidal test can be used topredict the margin of bactericidal activityrelative to the MBC at the beginning and end ofthe dosing interval. It also can be used tomeasure duration of killing by seriallydetermining the level of bactericidal activity andthe area-under-the-bactericidal-titer-curve.11
Lastly it can effectively assess the rapidity ofkilling in serum by measuring the killing effectover time.12
In a clinical setting, the peak and trough serumbactericidal titers are most easily determinedand usually provide sufficient clinical in-formation. In a research setting, thearea-under-the-bactericidal-titer-curve and theserum bactericidal rate may be determined inaddition to the serum bactericidal titer in orderto provide a more comprehensive evaluation ofthe pharmacodynamics and pharmacokinetics ofa new antimicrobial agent.
1.2 Clinical Relevance
It must be understood that, like mostsusceptibility tests, there is very little publishedinformation documenting the clinical relevanceof the serum bactericidal tests.
The serum bactericidal test most often has beenused to evaluate the therapeutic effec-tivenessof antimicrobial agents in bacterialendocarditis.13,14 In a comprehensive review ofthe literature covering the years 1948 to 1980,Coleman et al. were unable to find evidencethat either the serum inhibitory or bactericidaltiters had any prognostic value in the treatmentof patients with endocarditis.15
However, evaluation of the serum bactericidaltest in bacterial endocarditis is complicated bythe fact that such patients receive four to sixweeks of parenteral antimicrobial therapy and,for the most part, are cured by this regimenregardless of their serum bactericidal titers. Forexample, a multicenter collaborative study ofinfective endocarditis16 required seven years toacquire enough patients in the study to havestatistically significant results, yet had only nineclinical failures. This same study found that

September 1999 NCCLS
2
peak bactericidal titers of 64 or greater with themicrodilution method were associated with100% bacteriologic cure. The often-recommended peak serum bactericidal titer of 8was not associated with predictive accuracyand had no statistically significant associationwith clinical cure. Finally, the results of theserum bactericidal test in this study wereunable to accurately predict the failure ofbacterial eradication.
The serum bactericidal test also has been usedto monitor intravenous therapy followed by oralantimicrobial therapy for infective endocarditis,and the clinical outcome of these patients wasexcellent.17 The serum bactericidal test (boththe serum bactericidal titers18 and the serumbactericidal rate19) have proven useful in animalmodels and in human therapy for assessingcombination therapy of bacterial endocarditis.
The serum bactericidal test also has been usedto monitor antimicrobial therapy in cancerpatients. Klastersky et al.20 measured the peakand trough levels of bacteriostatic andbactericidal activity of the serum and urine of317 patients with cancer and a bacterio-logically proven infection. When the serumbactericidal test had a peak titer of > 8, theinfection was cured in 80% of cases.
Similarly, Sculier and Klastersky8 analyzed theclinical significance of the serum bactericidalactivity in cancer patients who presented withbacteremia caused by gram-negative bacilli.These investigators noted that the clinicalresponse to antibiotic therapy in these patientsstrongly correlated with the peak serumbactericidal activity. Ninety-eight percent ofnongranulocytopenic patients with a serumbactericidal titer of 8 or more had a favorableclinical response.
In contrast, patients with severe neutropenia(granulocyte count below 100/mm3) had an87% rate of cure only with titers of 16 or more.The higher titers needed with neutro-penicpatients may be related to the need forbactericidal activity over a longer time span. A16-peak serum bactericidal titer guaranteessome bactericidal activity in the serum for fourhalf-lives of the drugs being tested. Drusano etal.21 have found that four of five neutropenicpatients with gram-negative bacteremia inwhom empiric combination therapy failed hadno bactericidal titers at trough levels.21 This is
in distinct contrast to the 21 patients whosurvived, all having measurable serumbactericidal titers at trough levels.
The serum bactericidal test appears to haveutility in some cases for predicting bacterialeradication in patients with skeletal infections.Osteomyelitis and suppurative arthritis remaindifficult to treat successfully despite theavailability of effective antimicrobial agents.Dich et al.,22 for example, found that 19% ofchildren whose antibiotic regimen was changedfrom parenteral to oral during the first threeweeks of treatment had relapses or theirinfection took on a chronic course.
This is in contrast to the cumulative experienceof other investigators who have used the resultsof the serum bactericidal test to adjust thetherapy of children receiving parenteral followedby oral antimicrobial therapy. Tetzlaff andcolleagues23 treated 30 children with acutehematogenous skeletal infections (19 osteo-myelitis, 3 osteoarthritis, and 8 suppurativearthritis) with a brief (1 to 13 days) period ofparenteral antibiotic therapy followed by oraltherapy to complete a usual 4-week course. Adjustments in dosage were made whennecessary to insure a peak serum bactericidaltiter of at least 8. Twenty-nine of thirty weresuccessfully treated.
Kolyvas et al.24 also used the serum bactericidaltest to monitor parenteral/oral therapy inchildren, adjusting doses of antibiotics toachieve peak titers of 1:8. All of 10 childrenstudied remained cured after follow-up of oneyear. Prober and Yeager25 reported the resultsof 22 children treated with sequential therapy ofintravenous followed by oral agents. Peakserum bactericidal titers of 8 were achieved in21 of the 22 patients; trough titers of 2 in 20of 22 patients. The authors had no recurrencesin 21 of 22 patients.
Finally, Syrogiannopoulous and Nelson26
reviewed ten years of experience with childrenwho had acute suppurative osteoarthritis. Therewere 180 children who received large doses oforal antibiotics following clinical stabilizationwith intravenous antibiotics; the medianduration of intravenous therapy was about oneweek. Serum bactericidal titers were usedroutinely to monitor absorption and determinean adequate dose. These investigators used apeak serum bactericidal titer of 1:8 when the

Vol. 19 No. 17 M21-A
3
pathogen was a gram-negative bacillus, S.aureus, or H. influenzae and at least 1:32 whenthe etiologic agent was a streptococcus. If thetiters were suboptimal, the dosage of theantibiotic was increased. The dosages of oralantibiotics used under these guidelines weretwo-to-three times those normally used.
Over this ten-year period, no patient withsuppurative arthritis was readmitted withrecurrence. Four patients with acuteosteomyelitis were readmitted with recurrence,representing 3.8% of the 106 patients withbone infection. In two of these recurrences,noncompliance with the oral therapy (one caseproven and one suspected) were felt to be thereason for antimicrobial failure.
In a retrospective report of 18 adults withosteomyelitis, Black et al.27 assessed theplausibility of sequential parenteral-peroralantimicrobial therapy, adjusting the trough titeron peroral therapy to >1:8. There were 16 outof 18 patients who were cured.
In another study with mostly adults, Weinsteinet al.7 prospectively assessed the value ofserum bactericidal titers to predict outcome ofpatients with acute and chronic osteomyelitis.These investigators analyzed 51 patients withosteomyelitis, 30 acute and 21 chronic, whowere monitored at multiple medical centers withthe same serum bactericidal test methodology.
In this series, trough serum bactericidal titers of1:2 or greater predicted medical cure in 23 of25 patients successfully treated for acuteosteomyelitis. There were 13 successfullytreated episodes out of 21 cases of chronicosteomyelitis. In these 13 patients, peak serumbactericidal titers of 1:16 or greater and thetrough titers of 1:4 or greater were achievedand accurately predicted a cure. In contrast,peak titers of less than 1:16 and trough titers ofless than 1:2 in the 8 patients in whom therapyfailed accurately predicted this failure.
Other investigators reported that one should aimfor trough values of 1:2 or greater, wheneverpossible.28 However, if the patient response isfavorable, dosage should not be altered.
1.3 Clinical Use
It must be recognized that the number ofclinical situations in which a serum bactericidal
test is needed is very limited. There are,however, theoretical situations in which theserum bactericidal test might be useful.
The serum bactericidal titer, for example, can beused to determine the magnitude of serumbactericidal activity in relation to the MBC. Thisparameter can be important for antimicrobialagents that exhibit concentration-dependentkilling kinetics as shown by Moore andcolleagues29 who have reviewed the clinicalcourse of 236 patients with gram-negativebacillary infections that were treated withaminoglycosides. The clinical response toaminoglycosides in these patients was 80%(188 patients). Elevated maximal and meanpeak aminoglycoside concentration/MIC ratioswere strongly associated with clinical response(P<0.0001 and P<0.00001, respectively). Bylogistic regression the peak concentration/MICratios were associated significantly with clinicalresponse after adjustment for underlyingseverity of disease and other factors correlatedwith response. The serum bactericidal test,conceptually, measures no more than the serumlevel of the antimicrobial agent divided by theMIC or MBC of the infecting organism.30
NOTE: This statement is generally trueproviding there is no chemical, ionic binding, orpharmacologic interference with drug activity.
There are some conditions where drugconcentration does not reflect drug activity.Although for aminoglycosides the availability ofassay methods for determining the peak levelsprecludes the need for the serum bactericidaltest, the serum inhibitory activity for peak levelsof aminoglycosides, in theory, should be usefulin predicting clinical response in patients withgram-negative bacillary infections who aretreated with aminoglycosides. There are nocurrently available assay methods similar tothose available for aminoglycosides forfluoroquinolones. Fluoroquinolones are alsoconcentration-dependent agents. Determinationof serum bactericidal titers therefore may beuseful in intravenous therapy with ciprofloxacinso as to avoid clinical failure as has beenreported for seven of ten patients withnosocomial pneumonia caused by P. aeruginosawho were treated with intravenous cipro-floxacin.31
Moore and colleagues also noted that highplasma levels of aminoglycosides are associated

September 1999 NCCLS
4
with decreased mortality in patients withgram-negative bacillary pneumonia.32
For antimicrobial agents that exhibittime-dependent killing kinetics, a trough serumbactericidal titer would, in theory, be useful todemonstrate that the serum concentration-timeprofile has free drug levels always remainingabove the MIC (e.g., four-to-eight times theMIC) for the duration of time prior to the nextdose. The clinical relevance of such anapproach can be seen in the study of Warren etal. who found that the efficacy ofcefoperazone correlated best with the troughconcentration of free drug being above the MICof the infecting isolate.
The serum bactericidal test can also be used tomeasure not only the magnitude of serumbactericidal activity but also its duration. Thisis done by plotting serum bactericidal titersmeasured over time and calculating the areaunder the curves. The largest area under thebactericidal-titer curve will be found for theantimicrobial agent(s) with the best combinationof three factors: antibacterial activity,achievable free drug concentrations, andhalf-life.
Barriere et al. serially determined the serumbactericidal activity of three new cephalo-sporins and found prolonged bactericidalactivity against E. coli for cefotaxime despitethe half-life of this agent being only 1 hour. The authors postulated that the unexpectedprolonged bactericidal activity was likely due tothe presence of the active metabolite,desacetylcefotaxime, and suggested that adosage of 1 g of cefotaxime every 8 to 12hours should be sufficient for infections causedby susceptible gram-negative bacilli. Theefficacy of this dosing schedule subsequentlyhas been confirmed by the clinical study byGoodpasteure et al.35 The area under thebactericidal-titer curve provides anotherdimension to the evaluation of investigationalantibiotics.
The serum bactericidal titer, like the MBC,determines bactericidal activity after 24 hoursof incubation and separates the bacteria intotwo populations, a segregation that might nothave biological relevance. The serumbactericidal rate, however, evaluates therapidity of bacterial killing and has been shownin an experimental animal model to correlate
better with the rapidity of sterilization ofvegetations and to reflect the concentrationdependency of the synergy of nafcillin plus anaminoglycoside against S. aureus.
In human volunteers, Van der Auwera et al.compared the serum bactericidal rates forimipenem and vancomycin against methicillin-susceptible and methicillin-resistant S. aureus.These investigators found that againstmethicillin-susceptible S. aureus isolates,imipenem and vancomycin provided anequivalent rate of killing. Against methicillin-resistant isolates, imipenem was almostequivalent to vancomycin. The relevance ofthese findings is suggested by Fan et al. whostudied the clinical efficacy of imipenem against methicillin-susceptible and methicillin-resistant S. aureus. Eleven of 12 methicillin-susceptible and 10 of 11 methicillin-resistant S.aureus infections were clinically cured. Thismethod for evaluating the serum bactericidalrate is worthy of further investigation as a toolfor the evaluation of new antimicrobial agents.
1.4 Interpretation
The relation of the test results of the serumbactericidal test to the clinical outcome is notsuch that cure or failure can be predictedeasily.40
in the treatment of infected patients. It isimportant to understand the difference betweenbacterial eradication and clinical cure.Obviously, the ultimate clinical cure cannot bepredicted accurately solely by an in vitro test ofantimicrobial activity. Clinical cure dependslargely upon host factors and other factors,e.g., postantibiotic effect and the growth-inhibitory effects of sub-MIC concentrations ofantibiotics may also impact bacteriologicresponse of patients.41
Most immunocompetent hosts with bacterialinfections, moreover, do not requireantimicrobial therapeutic programs in whichthere is bactericidal activity. Strict adherence tothe achievement of an arbitrary serumbactericidal activity in the absence ofsupporting data may create an increased risk forthe patient. For example, drug toxicity mightensue due to an unnecessary increase in dosagein a clinically stable patient with a low titer.
Conversely, an effective dose may be loweredinappropriately. It is also important to realize
19,36,37
38
33
39
11
34
Bactericidal activity is only one factor

Vol. 19 No. 17 M21-A
5
that the final result of the serum bactericidaltest can be greatly influenced by methodology.Many factors must be carefully controlled ifreproducible results (intralaboratory andinterlaboratory) are to be achieved. Because ofthe specialized nature, the variations ofmethodology, the need for timed specimens,the complexity of technical factors, and thepotential difficulty for interpretation, it isrecommended that the serum bactericidal testbe done in consultation with the director of theclinical microbiology laboratory (i.e., this testshould be performed in reference or researchlaboratories or those laboratories with highly-trained medical technologists).
With such assistance, the clinician can moreeasily determine if the serum bactericidal test isthe appropriate test for assessing bactericidalactivity for his patient, determine whichvariation is most appropriate, assure that theserum specimens are collected properly, andproperly interpret the results.
2 Collection of Patient's Serum
2.1 Peak and Trough Levels
Generally, both a peak and trough level areobtained with the serum bactericidal test. Theoptimal timing of samples and most appropriatestorage conditions for collecting and obtainingpeak levels varies by drug and by route ofadministration; therefore, the product labelingshould be consulted to select the optimalsampling times.
This timing attempts to ensure that the peaklevel is obtained approximately 30 to 60minutes after the antimicrobial agent isabsorbed and distributed. The trough level isthat level obtained immediately before the nextdose.
These definitions are useful for singleantimicrobial agent therapy and are based onthe usual pharmacokinetic properties ofantimicrobial agents. If more than oneantibiotic is being used, the peak sample shouldbe obtained 1 hour after administration of thesecond antibiotic. If one of the agents isadministered infrequently (e.g., every 12 hours)and the other is administered more frequently(e.g., every 4 hours), peak levels should beobtained 1 hour after completion of the infusionof the second antimicrobial agent at a time
when the administration of both antimicrobialagents coincides. Though levels may beobtained based on the timing of the lessfrequently administered agent, the assumptionis made that the agent administered every 4hours will have a more constant level.
2.2 Sample Collection and Handling
The serum specimen must be collectedaseptically. Any bacterial contamination fromthe skin may interfere with the results. Also,because of short half-lives of some antibiotics,the timing of the serum collection is critical, andthe time the antimicrobial agent was givenshould be confirmed. This should include:
• The time that the previous dose was given.
• The time that the current dose was given orwill be given.
• The duration of the infusion when obtainingpeak levels for intravenously administeredagents.
Antimicrobial agents may not be given at theexact times ordered on a busy nursing unit, andcare must be taken to ensure that peak andtrough specimens are obtained accurately.Some hospitals designate one person to collectall samples for any type of drug assay.Specimens should be clearly marked with thefollowing:
• Patient's name and hospital number.
• Antimicrobial agent(s) and dose(s) beingused.
• Time of antimicrobial dose (start andcompletion of infusion) and initials ofmedication nurse.
• Time and date of specimen collection andinitials of collector.
One method to ensure compliance with propercollection is to require that the above materialbe completed on a requisition slip by theappropriate persons (medication nurse andblood collector) and initialed. If the requisitionslip is not properly completed (with initials), thespecimen is not processed. After the specimenhas been collected, serum should be separatedfrom red blood cells as soon as possible. Rapid

September 1999 NCCLS
6
transportation to the laboratory is necessary; ifany delay is expected, the specimen (blood orserum) should be transported on ice. (Serummust be frozen if the tests are to be delayedmore than 2 hours; blood cells must beseparated first because freezing hemolyzes thered blood cells.) Adhere to the pharmaceuticalmanufacturer’s guidelines for stability of theantibiotic in frozen human serum prior totesting. If serum is submitted frozen to areference laboratory for SBT testing, send in asterile plastic vial. Do not use glass.
2.3 Patient’s Isolate
The patient's isolate must be saved to serve asthe inoculum. The isolate may be kept frozenat –70ºC in tryptic soy broth or in a glycerolsuspension of a subculture on a tryptic soy agarslant. It is advisable to subculture the isolatethree times before testing to ensure that theorganism has an optimal growth and metabolicstatus before the drug exposure.
Since variations in density of inoculum mayalter the endpoints by one or more dilutions, thecorrect preparation of a standardized inoculumis critical. The rate of loss of viability of
bacterial cells following exposure to mostantibiotics is a direct function of bacterialgrowth prior to the addition of the agent withespecially marked effect shown for cell-wall-active agents. The use of stationary phasecultures, such as recently inoculated culturesgrowing for periods >8 hours, will include anincreased number of dormant cells which arenot susceptible to the agent and, therefore,cause diminished killing rates. See referencesand text in the most current edition of NCCLSdocument M26—Methods for DeterminingBactericidal Activity of Antimicrobial Agents.
In addition, the use of a lag phase cultures, i.e.,cultures which have recently undergone achange in test condition (e.g., temperature shiftor change from agar to broth medium), will alsoinclude cells less reactive to the agent and,therefore, cause less reliable killing endpoints(see Figure 1). A higher inoculum size, even inlog phase cultures, will approach the stationarygrowth phase and such organisms may be killedmore slowly.
Figure 1. Bacterial Growth Curve. Growth curve of typical bacterial culture as measured by viablecount (a: Lag phase; b: logarithmic phase; c: stationary phase; d: death phase).
3 Serum Dilution Procedure
The method for determining serum bactericidaltiters is a variation of the broth dilution test,and many of the methods used to control thevariables in the broth dilution test are applicableto the serum dilution procedure. Hence, it is
advisable to refer to extensive discussions,particularly of biological and technical factorsinfluencing test interpretation in NCCLSdocument M26—Methods for DeterminingBactericidal Activity of Antimicrobial Agents.

Vol. 19 No. 17 M21-A
7
3.1 Broth Medium
3.1.1 Human Serum as Diluent
In the serum bactericidal test, a broth is used todilute the patient's serum. Many differentbroths have been used as diluents, includingtrypticase soy, brain heart infusion, Columbia,dextrose phosphate, and (most commonly)Mueller-Hinton.41 The use of salt-containingdiluents must be avoided when testingstaphylococci and β-lactam agents. Humanserum in a 1:1 ratio (CAMHB/HS) has also beenrecommended as the diluent.42 The mainrationale for human serum as a diluent is toassess the role of protein-binding in theresults.protein-binding are well known,44,45 there hasbeen debate as to the clinical relevance of thisphenomenon. There is information available,however, as to the importance of protein-binding in determining clinical cure.
Chambers et al.46 found that cefonicid, a highlyprotein-bound cephalosporin, failed to clear theblood of bacteria or to produce a resolution ofclinical findings by day five of therapy in threeof four patients with staphylococcalendocarditis. This was despite peak concen-trations that were assayed in two patients andfound to be 20 to 40 times the MIC for theinfecting isolate. However, when protein wasadded to the medium, MICs for the isolates rosefour-to-eightfold and bactericidal titers were <1:8 at peak for all three patients.
In another study evaluating a highlyprotein-bound antimicrobial agent (teicoplanin),Calain and colleagues described six failuresdespite measured trough concentrations of totalteicoplanin which exceeded the MIC for theinfecting pathogen by 5 to 35 times in four ofthese patients. Because teicoplanin is veryhighly protein-bound, free antimicrobial agentwas noted to be less than the MIC even at peakconcentrations. Bolivar et al. evaluatedcefoperazone (12 g/day) as single agent therapyin cancer patients. These investigators wereable to achieve success in 80% (44 of 55) ofcases where the MIC of cefoperazone was ≤ 25µg/mL for the infecting organism.
Based on these clinical observations, Petersonet al.49 have used pharmacokinetic concepts topredict what a 12-g/day dose of cefoperazonewould produce in terms of extravascular levels
of cefoperazone. They predicted that such adose would result in extravascular levels of freecefoperazone in the range of 15 to 25 µg/mL.(Total mean levels in serum would be expectedto range from 75 to 250 µg/mL.) Thiscorrelates very nicely with the clinicalobservations of Bolivar. Clearly, the clinicalimportance of protein-binding can bedemonstrated for both gram-positive andgram-negative organisms.
Despite the theoretical and proven importanceof using human serum as the diluent, there is amultitude of problems associated with the useof pooled human serum in the clinicalmicrobiology laboratory. This problem can beavoided simply by using an ultrafiltrate of thepatient's serum.50 This separates the freeantimicrobial agent present and allows the useof Mueller-Hinton broth as the diluent. The useof an ultrafiltrate in the measurement of serumbactericidal activity avoids the disadvantagesassociated with the use of normal pooledhuman serum for the diluent. Ultrafiltration ofserum is easily accomplished by centrifugationat 25 ºC for 30 minutes at 1000 x g using acommercially available filtration device.Sterilization of the ultrafiltrate is done byfiltration through a 0.2-micron filter.
For antimicrobial agents that are known to haverelatively little protein binding (<90%, e.g.,gentamicin and vancomycin), Mueller-Hintonbroth can be used as the diluent. If there isappreciable protein-binding (>90%, e.g.,ceftriaxone and nafcillin), then either anultrafiltrate of the patient's serum or the use ofpooled human serum as the diluent isrecommended. Minimum inhibitory concen-trations (MICs) and minimum bactericidalconcentrations (MBCs) of most antimicrobialagents determined with and without humanserum against strains of bacteria commonlyused as quality controls in susceptibility testingcan be useful for quality control measures (see
3.1.2 Broth Monitoring
The performance and chemical characteristics ofboth Mueller-Hinton broth and human serummust be routinely monitored.
• The pH of each batch of Mueller-Hintonbroth should be checked with a pH meter
Although the in vitro effects of30,42,43
47
51Table 3).48

September 1999 NCCLS
8
when the medium is prepared; pH should bebetween 7.2 and 7.4.
• The MIC characteristics of broth should beevaluated periodically with a standard set ofquality control microorganisms and with anantibiotic from each major class. Thefrequency of such testing will depend onthe overall quality control program and thevolume of serum bactericidal tests done.
MICs for aminoglycosides and fluoroquinolonestested in Mueller-Hinton (MH) broth may belower than MICs obtained on MH agar(particularly when Pseudomonas aeruginosa istested) unless the MH broth is adjusted tocontain the recommended concentrations ofCa+2 and Mg.+2
Pooled human serum can be obtained fromcommercial sources or from volunteers. It mustbe quality controlled as rigorously as any otherreagent used in a clinical microbiologylaboratory. For the safety of laboratorypersonnel, it should be screened for hepatitis Bvirus antigen and for antibodies to HIV-1. (Thepooled human serum may be heated to 56 ºCfor 1 hour upon receipt to inactivate HIV-1 andcomplement.) Next, the serum should beadjusted with 0.1 N NaOH or 0.1 N HCl to pH7.2 to 7.4. After adjustment of pH, the serumshould be clarified by prefiltering with a 0.80-micron filter. Finally, the serum should befiltered using a 0.22-micron filter.
Pooled human serum may contain substancesto neutralize antibiotic agents, e.g.,β-lactamases. For this reason, pooled humanserum should be tested for the presence ofβ-lactamase activity especially when β-lacta-mases are to be tested. There are severalcommercially available rapid β-lactamase tests.Any of these, except those utilizing PADAC52
can be used by dropping some of the sera onthe test strip and observing for a color changeover 30 minutes. The serum should be screenedfor nonspecific antimicrobial activity by putting20 µL of the pooled human serum on blankpaper disks, placing the disks onto nutrient agarthat has been seeded with a spore suspension(5 x 108) of Bacillus subtilis ATCC® 6633, andlooking for zones of inhibition after incubationat 35 ºC for 24 hours.
A final quality control measure is to periodicallydetermine MICs and MBCs of various
antimicrobial agents for control strains ofbacteria in media supplemented with the serum. Use one antibiotic from each major class(penicillins, cephalosporins, and amino-glycosides) against an appropriate ATCC strain(see Section 7.3). MICs and MBCs of manyantimicrobial agents have been determined withand without human serum against strains ofbacteria commonly used as quality controls insusceptibility testing.51 The pooled humanserum should be heated to 56 ºC for 1 hour justbefore use in order to inactivate HIV-1 and anycomplement. The serum may be stored at -20ºC or less until needed.
3.2 Dilution Methods
Inhibitory activity is determined by dilutionmethods similar to those used to determine anMIC. Dilutions having no visible growth canthen be sampled with a calibrated device todetermine the concentration at which 99.9% ofthe final inoculum is killed.
Serum bactericidal titers can be determinedwith:
• A macrodilution method (1 to 2 mL in eachtest tube).
• A microdilution method (100 µL in eachwell).
It can be difficult to determine 99.9% killing ofthe final inoculum with the microdilutionmethod. However, the microdilution methodhas been found to be more reproducible thanthe macrodilution method for bactericidaltesting.51,53-60 Clinical studies suggest,moreover, that the microdilution method isuseful.7,8,10 It also is better suited for researchpurposes when testing serum from volunteersreceiving antibiotics against large numbers ofdifferent isolates. Therefore, the microdilutionmethod is recommended for the serumbactericidal test.
3.2.1 Macrodilution Method
The macrodilution method, if done, should beperformed in sterile 13- x 100-mm acid-treatedborosilicate glass test tubes. (Bacteria adhereto the walls of plastic tubes.) The followingprocedure is similar to that for MIC deter-minations.
Vol. 19 No. 17 M21-A
9
(1) Add 1.0 mL of the patient's serum to eachof the first two tubes. Alternatively, use1.0 mL of an ultrafiltrate of the patient'sserum.
(2) Add 1.0 mL of heat-inactivated pooledhuman serum to tubes 2 through 10.Alternatively, use cation-adjusted Mueller-Hinton broth (CAMHB).
(3) Make serial two-fold dilutions beginningwith the second tube and continuingthrough the ninth tube, leaving anintermediate volume of 1.0 mL in eachtube (use a separate pipette for each tube). Make the dilutions by withdrawing 1.0 mLfrom the tube containing 2.0 mL andtransferring this to the next tube which isthen mixed on a vortex mixer before thenext step is repeated.
(4) After the dilutions have been completed,add 1.0 mL of CAMHB, or other broth (ifnecessary) to each tube in order to yield afinal volume of 2.0 mL in each tube,ending with a 1:1 ratio of pooled humanserum to broth.
(5) Use the tenth tube as a control for growthof the organism.
3.2.2 Microdilution Method
The preferred microdilution method is performedin sterile plastic microdilution trays that haveround or conical bottom wells, each containinga final volume of 0.1 mL of broth. Adherence ofbacteria to the sides of the wells has not beenfound to be a problem as has been found withthe use of plastic test tubes for themacrodilution method. The micro-dilutionmethod is simple and more efficient, andrequires less broth. The following proce-dure issimilar to that for MIC determinations.
(1) Add 0.05 mL of pooled human serum orCAMHB to each well of columns 2 through10 in each row.
(2) Add 0.05 mL of the patient's serum orserum ultrafiltrate to each of the first twowells.
(3) Make serial two-fold dilutions of the serumfrom column 2 through column 9 with a
semiautomatic microdiluting device em-ploying 0.05-mL microdiluters.
(4) Use the tenth well as a positive growthcontrol.
3.3 Preparing Inoculum
The patient's isolate is used to prepare theinoculum. Variations in density of inoculummay alter the endpoints by one or moredilutions, and therefore, the preparation of astandardized inoculum is critical.
(1) To address the possibility of hetero-geneously distributed resistance amongcolonies, prepare the standardized finalinoculum by using 5 to 10 colonies of asingle type from a 16- to 24-hour agarplate containing nonselective culturemedium; inoculate them into a tubecontaining 5.0 mL of prewarmed (35 oC)broth (i.e., CAMHB or trypticase soybroth).
(2) Incubate this bacterial suspension at 35 oCuntil it is visibly turbid (up to six hours forstaphylococci; gram-negative rods mayrequire < six hours). Log-phase inoculashould be prepared in a shaker-incubatorand flask or beaker, whenever possible, topromote uniformity and optimization ofgrowth.
(3) Adjust the turbidity of the actively growingbroth culture (logarithmic phase) to obtaina turbidity visually comparable to that of a0.5 McFarland turbidity standard.
(4) Dilute the adjusted culture in broth(macrodilution method) or 0.9% bufferedsaline (microdilution method) so that afterinoculation of drug-containing broths, eachtube or well contains 5 x 105 CFU/mL.
The number of CFU/mL in the broth mediumjust before incubation is known as the finalinoculum. The inoculum size of the finalinoculum must be determined by serial dilutionin saline and subculture to solid media for usethe next day to interpret killing endpoints. Theexact inoculum volume delivered to the tubes orwells must be known before this calculation canbe done. For example, if the volume of mediumin the tubes is 2.0 mL, and the inoculum is 0.1mL, the adjusted culture (1.5 x 108 CFU/mL)

September 1999 NCCLS
10
must be diluted 1:20 with broth to yield 7.5 x106 CFU/mL. When 0.1 mL of this suspensionis inoculated into 2.0 mL of the broth, the finalinoculum of bacteria will be approximately 4 x105 CFU/mL.
Count the viable colonies in the inoculum toverify the final inoculum size. (This can easilybe done by using the growth control test tubeor by using a second growth control well in themicrodilution plate.) This is accomplished byusing a micropipettor to drop a 10-2, 10-3, and10-4 saline dilution of the inoculum onto thesurfaces of agar plates and then spreading thisover the surface. (The micropipettor volumeshould be ≤ 0.1 mL.) After overnight incu-bation, the plate showing 20 to 200 colonies isused to calculate the initial inoculum size. Forexample, if there are 40 colonies on the plateinoculated with the 1:1000 dilution, then thefinal inoculum contained 4 x 105 CFU/mL.
3.4 Inoculating Broth
3.4.1 Macrodilution Method
Prepare the dilutions of the patient's serumbefore adjusting the actively growing inoculum.Within 15 minutes after the inoculum has beenstandardized, add 0.1 mL of the adjustedinoculum to each tube in the dilution series witha micropipettor to release the inocula beneaththe surface of antimicrobial-containing solution. Mix by flushing two or three times withoutcreating air bubbles or splashing the sides ofthe tubes. Do not vortex or agitate the tubes.
3.4.2 Microdilution Method
As in the macrodilution method, make thedilutions before adjusting the actively growinginoculum. Then, dilute the inoculum and use toinoculate the solution within 15 minutes afterthe inoculum is standardized. If the volume ofthe inoculum exceeds 10% of the well volume,the diluting effect of the inoculum on theantimicrobial agent must be taken into account.If a 0.05-mL pipette dropper is used to addinoculum to the wells, the resulting dilution is1:2 which results in a final range of dilutions ofthe patient's serum of 1:2 to 1:512.
An alternative way to inoculate the wells is tofirst add 0.05 mL of broth to each well after thedilutions of the serum have been made and thenadd 0.0015 mL of inoculum with a multipoint
inoculator and a seed tray. In this case, thenumber of organisms in the seed tray should bedetermined and must be at least 5 x 107
CFU/mL. To prevent evaporation duringincubation, seal each tray in a plastic bag, withplastic tape or with a tight-fitting plastic coverbefore incubation.
3.5 Incubation
For all test methods, incubate the tubes or traysat 35 ºC in air or CO2, if required for growth ofthe patient’s isolate. Macrodilution tubesshould be incubated for 20 hours, vortexed,reincubated, and then vortexed again beforesampling at 24 hours. Microdilution trays shouldbe incubated for 24 hours and should be shakenat 20 hours but not before sampling at 24hours. To maintain the same incubationtemperature for all cultures, do not stackmicrodilution trays more than four high.
3.6 Determining Endpoints
The commonly used definition of serumbactericidal activity is 99.9% killing (� 3 log10
drop in CFU/mL) of the original inoculum. Thefinal inoculum size must be known. Thevolume subcultured must be based on this finalinoculum size and must be done quantitatively.Because of inaccuracy due to random variationin the number of cells in a small-volume sample,this subculture volume should be large enoughto provide an endpoint of at least ten colonies,but not so large that the antimicrobial agent iscarried over in a concentration high enough tocontinue inhibition of viable cells. Methods fordetermining MBCs which take into accountpipetting error and intrinsic sampling variabilitydue to the Poisson distribution of sampleresponse have been described.50-57
In these techniques, the final inoculum size canbe determined by a method such as thesurface-drop count58 or by a quantitativesubculture using a calibrated pipettor.50
Rejection values are determined by a chart thatconsiders the final inoculum size, single ordouble sampling, pipetting error, and thePoisson distribution of sample responses(Tables 1 and 2 contain the rejection values,i.e., the threshold for assessing lethal activity,for single and duplicate 0.01-mL sampling witha 5% pipette error50). The calculated sensitivityand specificity for these rejection values are
Vol. 19 No. 17 M21-A
11
provided for the sake of completeness. (Seefootnote (a) in Table 2.)
3.6.1 Macrodilution Endpoints
Determine macrodilution endpoints as follows:
(1) Use a logarithmic-phase culture for thefinal inoculum.
(2) The final inoculum should be 5 x 105
CFU/mL (range ≥ 1 x 105 CFU/mL to ≤ 1x 106 CFU/mL).
(3) Confirm the final inoculum (5 x 105
CFU/mL) by actual count of CFUs.
(4) Add the final inoculum to the tubes insmall volume (0.1 mL) below the surface,with no shaking.
(5) Gently mix by hand (or vortex at a lowspeed) at 20 hours and again at 24 hoursbefore sampling.
(6) Use a 0.01-mL calibrated pipettor tosubculture each clear test tube; duplicatesubcultures should be done.
(7) Streak the broth subcultured on an agarplate. The number of colonies subse-quently grown after 48 hours of incu-bation is used to determine the lethalendpoint based on the final inoculum andthe rejection values. For example, if thefinal inoculum is 5 x 105 and a singlesample is used, the dilution having fewerthan 11 colonies is the lethal endpoint(Table 2).
(8) The dilution which demonstrates 99.9%killing of the final inoculum is thebactericidal dilution titer.
3.6.2 Microdilution Endpoints
(1) Use a logarithmic-phase culture for thefinal inoculum.
(2) The final inoculum should be 5 x 105
CFU/mL (5 x 104 CFU/well) (range: 1 x105 to 1 x 106 CFU/mL).
(3) Confirm the final inoculum (5 x 105
CFU/mL) by actual count of CFUs.
(4) The final inoculum can be added to thewells in a volume equal to half the finalvolume or can be added using amultipoint inoculator (0.0015 mL). Do notshake.
(5) A multipoint inoculator or a pipettor canbe used to remove 10 µL; duplicatesubcultures should be done.
(6) Spot the broth subcultured with themultipoint inoculator on an agar platewith the first no growth after 48 hours ofincubation being considered the lethalendpoint. Alternatively, streak the brothsubcultured on an agar plate and after 48hours of incubation, count the coloniesand use the rejection values in Tables 1and 2. Colonies should not be countedwhen the 10 µL is spotted on an agarplate due to the tendency for the coloniesto run together.
(7) The dilution which demonstrates 99.9%killing of the final inoculum is thebactericidal dilution titer.
3.7 Interpretation of Bactericidal DilutionTiters
Although interpretation of the bactericidaldilution titers is controversial based on thelimited number of clinical evaluations, thefollowing are “approximate” guidelines for theclinical laboratory that uses the microdilutionmethodology delineated herein. As a generalguideline, SBTs of 16 to 32 were frequentlyassociated with more favorable clinicaloutcomes in patients with endocarditis.7,8,28 Thepeak SBT has been predictive of favorableoutcome for some patients with skeletalinfections although some investigators haveindicated that trough SBTs of 2 or greater maybe more predictive.
Inability to achieve a specific titer without toxiclevels of the antimicrobial agent(s) may indicatethe need for alternative agents. Lastly, themedical literature should be followed for otherapplications and validations.
4 Area Under the Bactericidal-TiterCurve
The area under the bactericidal-titer curve isdetermined by plotting bactericidal titers

September 1999 NCCLS
12
measured over time and calculating the areaunder the curve. The resulting area under thebactericidal-titer curve serves as a unifyingvalue to measure not only the magnitude ofserum bactericidal activity but also its duration.The largest area under the bactericidal-titercurve is found for the antimicrobial agent withthe best combination of three factors:antimicrobial activity, achievable free-drugconcentration, and half-life. The individualserum bactericidal tests which are performedover time are done as described in Section 3.This technique is generally reserved for researchas a means of comparing different antimicrobialagents or combinations of agents.
5 Serum Bactericidal Rate
The serum bactericidal rate evaluates therapidity of bacterial killing over time. The serumbactericidal rate is performed by first obtainingpeak and trough serum samples which are thenprocessed to yield ultrafiltrate. The ultrafiltrateis filter-sterilized and then mixed with an equalvolume of CAMHB to yield a 1:2 dilution. Atotal volume of 10 mL is used with a glass testtube. The inoculum is added in a small volumebelow the surface with a micropipettor in orderto avoid splashing on the inside of the test tubeabove the meniscus. The final inoculum shouldbe approximately 5 x 105 CFU/mL andconfirmed by a colony count. Test tubes shouldnot be agitated during incubation, but should bevortexed after each sampling.
One test tube is used as a growth control andconsists of the same inoculum added toCAMHB. The final inoculum is confirmed attime 0; subsequent colony counts are done at4 hours, between 6 and 12 hours, and at 24hours. Sampling for colony counts is done byremoving 0.5-mL samples of the broth at thespecified times. The 0.5-mL sample is seriallydiluted in test tubes containing 4.5 mL ofbuffered sterile saline (0.9% NaCl) to producetenfold dilutions (10-1, 10-2, 10-3, 10-4). Anumber of different colony count methods canbe used to determine the CFU/mL from thesedilutions. One-milliliter samples of the serialdilutions can be added to a tube of molten agar(48 ºC) for the preparation of a pour plate.
Alternatively, 0.1-mL samples of the serialdilutions can be pipetted onto prewarmed (35ºC for 1 hour) agar plates and distributed evenlyusing sterile, bent glass rods. Yet another
method uses 20 to 50 mL samples which aredropped on each of five spots onto prewarmedagar plates and allowed to absorb withoutstreaking.
Whichever method is used, the minimal,accurately detectable number of CFU/mL mustbe determined by serial dilutions with a knowninoculum. Potential drug carryover (Section 6)must be evaluated and, if a problem, stepstaken to eliminate these effects. Colonies arecounted after 24 to 48 hours of incubation. Amagnifying lens can facilitate colony countswhen plates are incubated for 24 hours.Prolonged incubation (48 hours) facilitatescounting colonies as the colonies are larger.With certain organism/ antibiotic combinations,the resultant colonies may be changed (i.e.,dwarf size and not readily detected). Prolongedincubation of plates before colonies are countedmay be more accurate. The kill-kineticdeterminations are shown graphically byplotting log10 CFU against time. A bactericidaleffect can be seen by a ≥ 3 log10 CFU decrease(99.9% killing of the final inoculum) at the timespecified.
During the performance of these studies, colonycounts may show a final increase in numberafter an initial decrease. This can be due to theselection of resistant isolates (most oftenphenotypic resistance61), inactivation of theantimicrobial agent (most likely after 24 hours),or regrowth of susceptible bacteria which haveescaped the antimicrobial activity by adhering tothe wall of the test tube.57,62,63 When regrowthoccurs, it is useful to determine the MICs ofsurvivors in order to see if a resistant organismwas selected from the population tested.
For comparisons of serum bactericidal rates,linear regression analysis can be done12 with theserum bactericidal rate being defined as theslope of the regression line, and its units beingthe change in the log10 CFU per milliliter perhour of exposure to the agent. The morenegative the slope, the faster the rate ofbacterial killing. A positive slope (e.g., incontrols) indicates growth. Alternatively, thearea-under-the-killing-curve64 can be deter-mined. Unlike linear regression analysis, thelatter method allows for nonlinear segments inthe curves. The serum bactericidal rate hasmainly been used as a research tool, but haspotential usefulness in clinical situations.19,36
Vol. 19 No. 17 M21-A
13
6 Antibiotic Carryover
The transfer of a quantitated volume of brothfrom the serum inhibitory titers or from akill-kinetic determination in order to assess thenumber of survivors can be complicated byantibiotic carryover.65 This problem occursmainly when higher concentrations of antibioticare present and is especially common whentesting β-lactam agents and staphylococci.Antibiotic carryover can be detected bystreaking the sample subcultured across thesurface of a prewarmed agar plate, allowing 20minutes for antimicrobial absorption into theagar, then cross-streaking the test organismover the entire surface of the plate, and after 24hours of incubation looking for inhibition ofcolonial growth at the site of the initial streak.60
This effect can be minimized by allowinginoculum to dry on the agar surface beforespreading.
7 Quality Control
7.1 Purpose
The quality control program monitors:
• The precision and accuracy of thesusceptibility test procedure, including theinoculum size and the growth of themicroorganism.
• The performance of reagents.
• The individuals who perform the test andread the results.
This goal is best realized through the use ofreference strains selected for their geneticstability and for their usefulness in the particularmethod being controlled.
7.2 Selecting Reference Strains
Ideal reference strains for quality control ofdilution susceptibility methods have MICs (andMBCs) that fall near the midrange of theconcentration for all antimicrobials tested. Anideal control strain is inhibited at the fourthdilution of a seven dilution log2 series, butstrains with MICs (and MBCs) at either the thirdor fifth dilution are acceptable. The referencestrains will be used primarily as quality controlmeasures for occasional testing of the media
used in bactericidal testing and for occasionaltesting of individuals who perform the test.
7.3 Suggested Quality Control Strains
A full set of quality control strains that haveadequate or optimal endpoints for all thecommonly used antimicrobial agents is not yetavailable. Some strains with useful endpoints,however, have been tested repeatedly and haveproven to be stable. We currently recommendthe following reference strains for controllingdilution tests:
• Escherichia coli ATCC® 25922
• Pseudomonas aeruginosa ATCC® 27853
• Staphylococcus aureus ATCC® 25923
• Enterococcus faecalis ATCC® 29212.For suitable quality control ranges, see Table 3.
7.4 Batch or Lot Control
Records should be kept of the lot numbers of allmaterials and reagents used in these tests.
7.5 Other Control Procedures
7.5.1 Growth Control
Each macrodilution series and eachmicrodilution tray should include a positivegrowth control of basal medium withoutantimicrobial agent to assess viability of the testorganisms. The growth control also serves asa turbidity control for reading endpoints.
7.5.2 Purity Control
A sample of the inoculum should be streaked ona suitable agar plate and incubated overnight todetect mixed cultures and to provide freshlyisolated colonies in case retesting provesnecessary. Also, the growth control can besubcultured at the same time that the serumbactericidal test is performed in order to assesspurity.
7.5.3 Reproducibility
If serum dilution titers are determined by themicrodilution method, the reproducibility caneasily be determined by performing the test induplicate.

September 1999 NCCLS
14
7.5.4 Paradoxical Effect
The paradoxical effect is defined as theoccurrence of progressively increasing platecounts for at least three consecutiveconcentrations above the serum inhibitory titer.If this occurs, the concentrations exhibiting theparadoxical effect are usually ignored for S.aureus but are reported when dealing with
those gram-negative bacteria which can beinducible/constitutive producers of Class C(Group 1) β-lactamase (e.g., Enterobacter, P.aeruginosa). Paradoxical effect can also beseen with quinolones once the maximumbactericidal concentration has been exceeded.

Vol. 19 No. 17 M21-A
15
Table 1. Rejection Value and Calculated Sensitivity and Specificity for Each Initial Concentration on theBasis of Duplicate 0.01-mL Samplesa
5% Error (Pipette error plus full samplingerror) for Determination of Final Inoculumb
Final Inoculum Rejection Sensitivity Specificity(CFU/mL) Value (%) (%)
1 x 105 4 77 972 x 105 8 89 993 x 105 15 99 994 x 105 20 99 995 x 105 25 99 996 x 105 29 99 997 x 105 33 99 998 x 105 38 99 999 x 105 42 99 991 x 106 47 99 992 x 106 91 99 993 x 106 136 99 994 x 106 182 99 995 x 106 227 99 996 x 106 273 99 997 x 106 318 99 998 x 106 364 99 999 x 106 409 99 991 x 107 455 99 99
a
antibiotic was declared lethal (a 0.999 or greater reduction in the final inoculum).
bBased on duplicate samples for the determination of the final inoculum size.
cNumber of colonies.
dSensitivity and specificity calculated for each specific final inoculum concentration and rejection value.
d
c
d
When the sum of colonies from duplicate samples was equal to or less than the rejection value, the
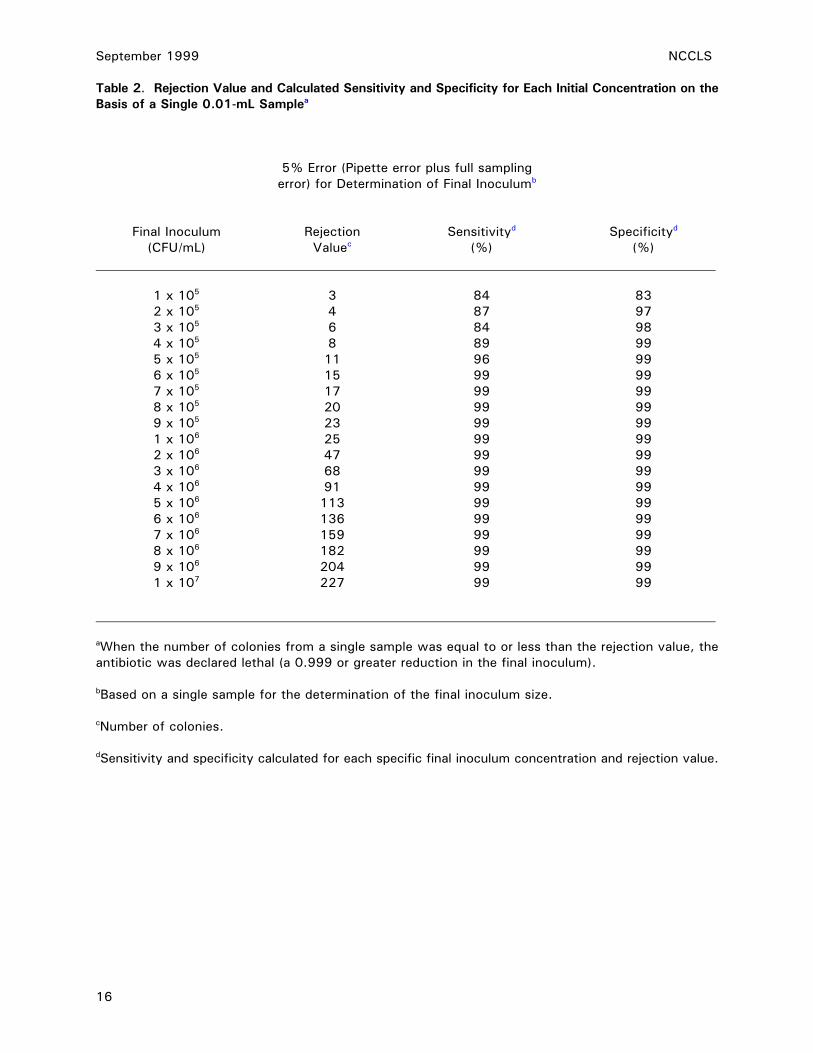
September 1999 NCCLS
16
Table 2. Rejection Value and Calculated Sensitivity and Specificity for Each Initial Concentration on theBasis of a Single 0.01-mL Samplea
5% Error (Pipette error plus full samplingerror) for Determination of Final Inoculumb
Specificityd
(CFU/mL)
c (%) (%)
1 x 105 3 84 832 x 105 4 87 973 x 105 6 84 984 x 105 8 89 995 x 105 11 96 996 x 105 15 99 997 x 105 17 99 998 x 105 20 99 999 x 105 23 99 991 x 106 25 99 992 x 106 47 99 993 x 106 68 99 994 x 106 91 99 995 x 106 113 99 996 x 106 136 99 997 x 106 159 99 998 x 106 182 99 999 x 106 204 99 991 x 107 227 99 99
aWhen the number of colonies from a single sample was equal to or less than the rejection value, theantibiotic was declared lethal (a 0.999 or greater reduction in the final inoculum).
bBased on a single sample for the determination of the final inoculum size.
cNumber of colonies.
dSensitivity and specificity calculated for each specific final inoculum concentration and rejection value.
d Final Inoculum Rejection SensitivityValue

Vol. 19 No. 17 M21-A
17
Table 3. Suitable Quality Control Ranges for MICs and MBCs With and Without Human Serum UsingATCC Strainsa
Staphylococcus aureus ATCC® 25923
MIC in MBC in
Drug CAMHBb CAMHB/HSc CAMHBb CAMHB/HSc
Methicillin 1-4 1-4 1-4 1-4
Oxacillin 0.125-0.5 0.5-2 0.25-1 1-4
Nafcillin 0.125-0.5 0.5-2 0.25-1 1-4
Cephalothin 0.0625-0.25 0.25-1 0.125-0.5 0.5-2
Cefazolin 0.125-0.5 0.5-2 0.125-0.5 1-4
Vancomycin 0.5-2 0.5-2 1-4 1-4
Escherichia coli ATCC® 25922
MIC in MBC in
Drug CAMHBb CAMHB/HSc CAMHBb CAMHB/HSc
Ampicillin 2-8 2-8 4-16 4-16
Piperacillin 1-4 1-4 2-8 2-8
Cephalothin 8-32 16-64 16-64 32-128
Imipenem 0.0625-0.25 0.25-1 0.125-0.5 0.25-1
Gentamicin 0.25-1 1-4 0.25-1 1-4
Amikacin 0.5-2 2-8 0.5-2 2-8
Pseudomonas aeruginosa ATCC® 27853
MIC in MBC in
Drug CAMHBb CAMHB/HSc CAMHBb CAMHB/HSc
Piperacillin 4-16 2-8 8-32 4-16
Ticarcillin 32-128 16-64 32-128 16-64
Imipenem 1-4 2-8 4-16 8-32
Gentamicin 2-8 2-8 4.0-16 4-16
Tobramycin 0.5-2 0.5-2 1-4 1-4
Amikacin 2-8 2-8 4-16 4-16
aAlthough these quality control ranges are derived from a published study, it should be noted that thisstudy was performed before NCCLS document M23—Development of In Vitro Susceptibility TestingCriteria and Quality Control Parameters defined the parameters for such studies.
bCAMHB = cation-adjusted Mueller-Hinton broth.
cCAMHB/HS = cation-adjusted Mueller-Hintonbroth mixed with pooled human serum in a 1:1 ratio.

September 1999 NCCLS
18
References
1 NCCLS. Performance Standards forAntimicrobial Disk Susceptibility Tests—Sixth Edition; Approved Standard. NCCLSdocument M2-A6. Wayne, Pennsylvania:NCCLS;1997.
2 NCCLS. Methods for Dilution Anti-microbial Susceptibility Tests for Bacteriathat Grow Aerobically—Fourth Edition;Approved Standard. NCCLS documentM7-A4. Wayne, Pennsylvania: NCCLS;1997.
3 NCCLS. Methods for Antimicrobial Sus-ceptibility Testing of Anaerobic Bacteria—Fourth Edition; Approved Standard. NCCLSdocument M11-A4. Wayne, Pennsylvania:NCCLS;1997.
4 Isenberg HD. Clinical evaluation oflaboratory guidance to antibiotic therapy.Health Lab Science. 1967;4:166-180.
5 Hunter TH. Speculations on the mech-anism of cure of bacterial endocarditis. JAm Med Assoc. 1950;144:524-527.
6 Scheld WM, Sande MA. Bactericidalversus bacteriostatic antibiotic therapy ofexperimental pneumococcal meningitis inrabbits. J Clin Invest. 1983;71:411-419.
7 Weinstein MP, et al. Multicenter collab-orative evaluation of a standardized serumbactericidal test as a predictor oftherapeutic osteomyelitis. Am J Med.1987;83:218-222.
8 Sculier JP, Klastersky J. Significance ofserum bactericidal activity in gram-negative bacillary bacteremia in patientswith and without granulocytopenia. Am JMed. 1984;76:429-435.
9 NCCLS. Methods for Determining Bacte-ricidal Activity of Antimicrobial Agents;Tentative Guideline. NCCLS documentM26-A. Wayne, Pennsylvania: NCCLS;1999.
10 Vogelman B, Craig WA. Kinetics ofantimicrobial activity. J Pediatr. 1986;108:835-840.
11 Barriere SL, et al. Analysis of a new
method for assessing activity of com-binations of antimicrobials: area under thebactericidal titer curve. J AntimicrobChemother. 1985;16:49-59.
12 Briceland LL, Pasko MT, Mylotte JM.Serum bactericidal rate as a measure ofantibiotic interactions. Antimicrob AgentsChemother. 1987;31:679-685.
13 Wolfson JS, Swartz MN. Serum bacte-ricidal activity as a monitor of antibiotictherapy. N Engl J Med. 1985;213:968-975.
14 Stratton CW. The serum bactericidal test.Clin Microbiol Rev. 1988;1:19-26.
15 Coleman DL, Horwitz RI, Andriole VT.Association between serum inhibitory andbactericidal concentrations and therapeuticoutcome in bacterial endocarditis. Am JMed. 1982; 73:260-267.
16 Weinstein MP, et al. Multicenter collab-orative evaluation of a standardized serumbactericidal test as a prognostic indicatorin infective endocarditis. Am J Med.1985;78:262-269.
17 Parker RH, Fossieck BE Jr. Intravenousfollowed by oral antimicrobial therapy forstaphylococcal endocarditis. Ann InternMed. 1980;93:832-834.
18 Sande MA, Sheld WM. Combinationtherapy of bacterial endocarditis. AnnIntern Med. 1980;92:390-395.
19 Drake TA, Hackbarth CJ, Sande MA. Valueof serum tests in combined drug therapy ofendocarditis. Antimicrob AgentsChemother. 1983;24:653-657.
20 Klastersky J, Daneau D, Swings G, WeertsD. Antibacterial activity in serum and urineas a therapeutic guide in bacterialinfections. J Infect Dis. 1974;129:187-193.
21 Drusano G, et al. Correlation of predictedserum bactericidal activities and valuesmeasured in volunteers. Eur J Clin Mi-crobiol. 1986;5:88-92.
Vol. 19 No. 17 M21-A
19
22 Dich VQ, Nelson JD, Hatalin KC.Osteomyelitis in infants and children. AmJ Dis Child. 1975;129:1273-1278.
23 Tetzlaff TR, McCracken GH. Oral anti-biotic therapy for skeletal infections inchildren. II. Therapy of osteomyelitis andsupprative arthritis. J Pediatr. 1978;92:485-490.
24 Kolyvas E, et al. Oral antibiotic therapy ofskeletal infections in children. Pediatrics.1980;65:867-871.
25 Prober CG, Yeager AS. Use of the serumbactericidal titer to assess the adequacy oforal antibiotic therapy in the treatment ofacute hematogenous osteomyelitis. JPediatr. 1979;95:131-135.
26 Syrogiannopoulos GA, Nelson JD. Durationof antimicrobial therapy for acutesuppurative osteoarticular infections. Lancet. 1988;I:37-40.
27 Black J, Hunt TL, Godley PJ, et al. Oralantimicrobial therapy for adults withosteomyelitis or septic arthritis. J InfectDis. 1987;155:963-972.
28 Norden C, Gillespie WJ, Nade S. Infectionsin Bones and Joints. Blackwell ScientificPublications; 1994.
29 Moore RD, Lietman PS, Smith CR. Clinicalresponse to aminoglycoside therapy:importance of peak concentration tominimal inhibitory concentration. J InfectDis. 1987;155:93-99.
30 Stratton CW, Weinstein MP, Reller LB.Correlation of serum bactericidal activitywith antimicrobial agent level and minimalbactericidal concentration. J Infect Dis.1982; 145:160-168.
31 Peloquin CA, et al. Evaluation ofintravenous ciprofloxacin in patients withnosocomial lower respiratory tractinfections. Arch Intern Med. 1989;149:2269-2273.
32 Moore RD, Smith CR, Lietman PD.
Association of aminoglycoside plasmalevels with therapeutic outcome in gram-negative pneumonia. Am J Med. 1984;77:657-662.
33 Warren JW, Miller Jr EH, Fitzpatrick B,DiFranco DE, Caplan ES, Tenney JH,Anthony WC. A randomized, controlledtrial of cefoperazone vs cefamandole-tobramycin in the treatment of putative,severe infections with gram-negativebacilli. Rev Infect Dis. 1983;5:173.
34 Barriere SL, Ozasa DC, Mordenti J.Assessment of serum bactericidal activityafter administration of cefoperazone,cefotaxime, ceftizoxime and moxalactamto healthy subjects. Antimicrob AgentsChemother. 1985;28:55-57.
35 Goodpasture HC, et al. Optimalcefotaxime dosing for gram-negative bac-teremia: effective trough serum bacte-ricidal titers and drug concentrations 8 and12 hr after 1- or 2-g infusions. DiagnMicrobiol Infect Dis. 1988;9:97-103.
36 Drake TA, Sande MA. Studies of thechemotherapy of endocarditis: correlationof in vitro, animal model, and clinicalstudies. Rev Infect Dis. 1983;5(Suppl2):S345-S354.
37 Zak D, Sande MA. In: Sabath LD, ed.Correlation of in vitro antimicrobial activityof antibiotics with results of treatment inexperimenal animal models and humaninfection. Action of Antibiotics in Patients. Bern, Switzerland: Han Huber Publishers;1982:55-67.
38 Van der Auwera P, Van Laethem Y,Klastersky J. Bactericidal activity andkilling rate of serum against gram-positivecocci in volunteers receiving imipenem,oxacillin, vancomycin, or ampicillin plusgentamicin. J Antimicrob Chemother.1987;20:239-249.
39 Fan W, et al. Imipenem-cilastin in thetreatment of methicillin-sensitive andmethicillin-resistant Staphylococcus au-reus infections. Antimicrob Agents Che-mother. 1986;29:26-29.

September 1999 NCCLS
20
40 Greenwood D. In vitro veritas? Anti-microbial susceptibility tests and theirclinical relevance. J Infect Dis. 1981;144:380-385.
41 Pien FD, Vosti KL. Variation in per-formance of the serum bactericidal test. Antimicrob Agents Chemother. 1974;6:330-333.
42 Stratton CW, Reller LB. Serum dilutiontest for bactericidal activity. I. Selection ofa physiologic diluent. J Infect Dis.1977;136:187-195.
43 Kunin CM. Protein binding of antibioticsdoes affect their antistaphylococcalactivity. J Antimicrob Chemother. 1986;17:263.
44 Bergan T, Engeset A, Olszewski W. Doesserum protein binding inhibit tissuepenetration of antibiotics? Rev Infect Dis.1987;9:713-718.
45 Rolinson GN. The significance of proteinbinding of antibiotics in antibiotic activityin vivo. J Antimicrob Chemother. 1980;6:311-317.
46 Chambers HF, et al. Failure of a once-dailyregimen of cefonicid for treatment ofendocarditis due to Staphylococcusaureus. Rev Infect Dis. 1984;6(Suppl4):S870-S874.
47 Calain P, et al. Early termination of aprospective, randomized trial comparingteicoplanin and flucloxacillin for treatingsevere staphylococcal infections. J InfectDis. 1987;155:187-191.
48 Bolivar R, Fainstein D, Elting K, Bodey GP.Cefoperazone for treatment of infections inpatients with cancer. Rev Infect Dis.1983;5(Suppl 1):181-187.
49 Peterson LR, et al. Influence of proteinbinding on therapeutic efficacy ofcefoperazone. Antimicrob Agents Chemo-ther. 1989;33:566-568.
50 Leggett JE, Wolz SA, Craig WA. Use of
serum ultrafiltrate in the serum bactericidaltest. J Infect Dis. 1989;160:616-623.
51 Reimer LG, Stratton CW, Reller LB. Mini-mal inhibitory and bactericidal concen-trations of 44 antimicrobial agents againstthree standard control strains in broth withand without human serum. AntimicrobAgents Chemother. 1981;19:1050-1055.
52 Anhalt JP, Nelson R. Failure of PADACtest strips to detect staphylococcalß-lactamase. Antimicrob Agents Chemo-ther. 1982;21:993-999.
53 Woolfrey BF, Lally RT, Tait KR. Influenceon technical factor variations on seruminhibitions and bactericidal titers. J ClinMicrobiol. 1986;23:997-1000.
54 Pearson RD, Steigbigel RT, Davis HT,Chapman SW. Method for reliabledetermination of minimal lethal antibioticconcentrations. Antimicrob Agents Che-mother. 1980;18:699-708.
55 Shanholtzer CJ, Peterson LR, Mohn ML.MBCs for Staphylococcus aureus asdetermined by macrodilution andmicrodilution techniques. AntimicrobAgents Chemother. 1984;26:214-219.
56 Sherris JC. Problems in vitro deter-mination of antibiotic tolerance in clinicalisolates. Antimicrob Agents Chemother.1986;30:633-637.
57 Taylor PC, et al. Determination of mini-mum bactericidal concentrations ofoxacillin for Staphylococcus aureus:influence and significance of technicalfactors. Antimicrob Agents Chemother.1983;23:142-150.
58 Miles AA, Misra SS. The estimation of thebactericidal power of the blood. J Hyq(Lond). 1938;38:732-748.
59 Peletier LL. Lack of reproducibility ofmacrodilution MBCs for Staphylococcusaureus. Antimicrob Agents Chemother.1984;26:815-818.

Vol. 19 No. 17 M21-A
21
60 Pelletier Jr LL, Baker CB. Oxacillin,
cephalothin, and vancomycin tubemacrodilution MBC result reproducibilityand equivalence to MIC results formethicillin-susceptible and reputedlytolerant Staphylococcus aureus isolates. Antimicrob Agents Chemother. 1988;32:374-377.
61 Greenwood D. Phenotypic resistance toantimicrobial agents. J AntimicrobChemother. 1985;15:653-658.
62 Gwynn MN, Webb LT, Rolinson GN. Regrowth of Pseudomonas aeruginosa andother bacteria after the bactericidal action ofcarbenicillin and other beta-lactam antibiotics.J Infect Dis. 1981;144:263-269.
63 Layte S, Harris P, Rolinson GN. Factors
affecting the apparent regrowth ofPseudomonas aeruginosa followingexposure to bactericidal concentrations ofcarbenicillin. Chemotherapy. 1983;30:26-30.
64 Tisdale JE, Pasko MT, Mylotte JM.Antipseudomonal activity of simulatedinfusions of gentamicin alone or withpiperacillin assessed by serum bactericidalrate and area under the killing curve. Antimicrob Agents Chemother. 1989;33:1500-1505.
65 Dankert J, Holloway Y, Joldersma W, HessJ. Importance of minimizing carry-overeffect at subculture in the detection ofpenicillin-tolerant viridans groupstreptococci. Antimicrob Agents Che-mother. 1983;23:614-616.
Additional References
Craig WA, Gudmundsson S. Postantibioticeffect. In: Antibiotics in Laboratory Medicine.4th ed. Williams and Wilkins Co.;1996:2.
Odenholt-Tornqvist I, Lowdin E, Cars O.Postantibiotic sub-MIC effects of vancomycin,roxithromycin, sparfloxacin, and amikacin.Antimicrob. Ag Chemother. 1992;36:1852-1858.

September 1999 NCCLS
22
Summary of Comments and Subcommittee Responses
M21-T: Methodology for the Serum Bactericidal Test; Tentative Guideline
General Comments
1. I would argue that a critical review of the clinical relevance of the serum bactericidal test to theclinical setting be a part of the document.
! Serum bactericidal tests by different methods have been used for 50 years; however, criticalassessments of clinical utility are few and not sufficient. A principal goal of an approvedNCCLS serum bactericidal testing guideline is to foster the very studies that could becomereferences in future documents.
2. While I have many concerns about the use of this test in most clinical laboratories, I believe itis possible to obtain reproducible answers depending on the technology that is employed inperforming the test.
! Ensuring reproducibility of results with this testing methodology is the main objective of thisserum bactericidal testing guideline.
3. We avoid the use of serum additive because it introduces a major, uncontrolled variable to thetest, and the direct effects of serum on antimicrobial agent performance due to protein bindingduring patient treatment can be estimated easily. Because of the poor reproducibility of theMBC test, it should always be run in duplicate. When the macrodilution method is used, thesubculture should be repeated after 48 hours of incubation if the results at 24 hours show skipsor are discrepant. Also, we do not recommend any agitation before sampling.
! Using the microdilution methodology in this document should enable a reproducible result. Anultrafiltrate of the patient’s serum is an acceptable alternative to dilution with pooled humanserum as noted.
4. Since this test has quite limited scientific evidence correlating a single or specific titer totherapeutic outcome, I would strongly encourage NCCLS in the next revision of this documentto not publish specific interpretive criteria.
! This comment is duly noted. The importance of keeping abreast of the medical literature on thistopic has been emphasized in this version.
5. Many viridans streptococci are capable of growing in broth with chain lengths exceeding 100cells. These chains are not easily disrupted; placing the culture (in a glass container) in anultrasonic waterbath has little effect on chain length. I believe that this is a major technicalfactor in the irreproducibility of time-kill and associate methodology, particularly for viridansstreptococci. The time period for which the organism is grown in broth prior to standardizationof the inoculum using a McFarland standard will affect the initial chain length obtained (factorssuch as the length of the lab phase resulting in a change of media formulation from agar-plateto broth, the degree of metabolic shutdown relating the age of the culture on the plate whichthe broth was inoculated and the time taken to reach opacity all affect the chain length oforganisms in broth). Sonication of the sample used to assess the initial inoculum in such testsdoes go some way to addressing this technical factor, and if properly controlled should resultin more reproducible methods.
! The relevance of this comment has been noted.

Vol. 19 No. 17 M21-A
23
Foreword
6. Last sentence - Should this read “The assistance of the laboratory’s director is useful in (1)determining if such a test is needed, (2) selecting NCCLS recommended methodology for testingand (3) interpreting the results”?
! The wording in the Foreword has been revised accordingly.
Section 1.1
7. Is “integrates” the appropriate word, or would something like “incorporate” be more accurate?The word “integrate” is used repeatedly throughout the document in this same sense.
! The indicated wording has been revised accordingly.
8. The serum bactericidal test which can determine the magnitude of bacterial activity. . .The word“magnitude” does not read well and is repeated.
! This comment has been noted and the text revised.
Section 2.2
9. Add a sentence for those physicians submitting to referral laboratories. We suggest. . .”Ifsubmitted frozen to a referral laboratory for testing, submit in a sterile plastic vial. Do not useglass.”
! This comment has been noted and the text revised.
Section 3.1
10. The sentence “The greatest effect. . .” is awkward; suggest rewording.
! This comment has been noted and the text revised.
11. Could a list of such agents affected by protein binding be provided (recognizing that new agentsare always being released)?
! This comment has been noted and the text revised.
Section 3.1.2
12. With the emphasis on use of the ultrafiltrate, could these details be deleted or relegated to anappendix?
! Details on the use of the ultrafiltrate should be in the text itself for laboratories that use pooledhuman serum.
Section 3.3
13. It is not necessary to prepare the inoculum by using 20 to 30 colonies. We suggest that 5 to10 colonies would work as well.

September 1999 NCCLS
24
! This comment has been noted and the text revised.
14. It is suggested, when attempting to count viable colonies from the growth control well inoculumand using a micropipettor to drop dilutions, that this be done in duplicate and the numbers ofcolonies be counted and averaged to give a better representation of initial inoculum size.
! This comment has been noted and the text revised.
Section 3.5
15. Specify atmospheric conditions of incubation, i.e., ambient, CO2, or other.
! The atmospheric conditions have been added to the text.
Section 3.6
16. The term “rejection values” is not clear. Define the term and how it should be used.
! A working definition of this term has been incorporated into the text of Section 3.6.
Section 6.0
17. There are no instructions for preparing a diluted sample.
! Detailed instructions regarding diluted sample preparation have been added to Section 6.

Vol. 19 No. 17 M21-A
25
Related NCCLS Publications*
M2-A6 Performance Standards for Antimicrobial Disk Susceptibility Test—Sixth Edition;Approved Standard (1997). This document provides current recommended techniquesfor disk susceptibility testing, new frequency criteria for quality control testing, andupdated tables for interpretive zone diameters.
M7-A4 Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria That GrowAerobically— Fourth Edition; Approved Standard (1997). This document providesreference methods for the determination of minimum inhibitory concentrations (MIC) ofaerobic bacteria by broth macrodilution, broth microdilution, and agar dilution.
M11-A4 Methods for Antimicrobial Susceptibility Testing of Anaerobic Bacteria; ApprovedStandard— Fourth Edition (1997). This document provides methods for susceptibilitytesting of anaerobic bacteria; description of reference agar dilution method, alternativeagar methods (Wadsworth and limited dilutions), broth microdilution, and broth (macro)dilution procedures, and quality control criteria for each procedure.
M26-A Methods for Determining Bactericidal Activity of Antimicrobial Agents; ApprovedGuideline (1999). This document provides procedures for determining the lethal activityof antimicrobial agents.
M29-A Protection of Laboratory Workers from Instrument Biohazards and Infectious DiseaseTransmitted by Blood, Body Fluids, and Tissue; Approved Guideline (1997). Thisdocument provides guidance on the risk of transmission of hepatitis viruses and humanimmunodeficiency viruses in any laboratory setting; specific precautions for preventingthe laboratory transmission of blood-borne infection from laboratory instruments andmaterials; and recommendations for the management of blood-borne exposure.
* Proposed- and tentative-level documents are being advanced through the NCCLS consensus process; therefore, readers should refer to the most recent editions.

September 1999 NCCLS
26
NOTES

Vol. 19 No. 17 M21-A
27
NOTES

September 1999 NCCLS
28
NOTES

Vol. 19 No. 17 M21-A
29
NOTES

September 1999 NCCLS
30
NOTES

Vol. 19 No. 17 M21-A
31
NOTES

September 1999 NCCLS
32
NOTES

NCCLS�940 West Valley Road � Suite 1400 � Wayne, PA 19087� USA �PHONE 610.688.0100 FAX 610.688.0700 � E-Mail: [email protected]. ISBN 1-56238-383-3
ABC