M1013 a Cost-Effectiveness Analysis in Colorectal Cancer Screening Comparing Immunochemical Faecal...
1
4-part program (Discussion and Education, Documenting, Reporting and P4P) successfully improved WT and could likely be implemented in groups with strong governance and adequate EMR capabilities. We saw a trend toward increased AFR with increasing individual >6 minute WT, suggesting value in this compliance goal. M1013 a Cost-Effectiveness Analysis in Colorectal Cancer Screening Comparing Immunochemical Faecal Occult Blood Tests with Guaiac Faecal Occult Blood Tests and No Screening. Leo G. van Rossum, Anne Floortje van Rijn, Andre L. Verbeek, Martijn G. van Oijen, Robert J. Laheij, Paul Fockens, Jan B. Jansen, Eddy M. Adang, Evelien Dekker Introduction: The comparability of cost-effectiveness of colorectal cancer (CRC) screening strategies is limited if heterogeneous study data on tests, populations, and designs are combined. Furthermore cost-effectiveness studies frequently suffer from unrealistic assump- tions, e.g. concerning differences in screening participation and adherence to follow-up. Based on empirical data from a representative randomised controlled screening trial with FOBT in the Netherlands (Van Rossum, et al. Gastroenterology 2008), we aimed to compare cost-effectiveness of one round of immunochemical faecal-occult-blood-test (OC-Sensor®, I-FOBT) screening, with one round of guaiac based faecal-occult-blood-test (Hemoccult- II®, G-FOBT) screening and no screening. Methods: We designed a Markov model of the cost-effectiveness of CRC screening with FOBT and no screening in asymptomatic average risk individuals between 50 and 75 years. From a third-party payer perspective we analysed data with first and second order Monte Carlo simulation over 10 years of one year cycles. Empirical data were completed with cancer registry and literature data. Costs were presented in Euros using a discount rate of 4%. Effects were measured as life years gained using a discount rate of 1.5%. Results: I-FOBT resulted in more life years gained and costs saved (i.e. I-FOBT dominated) compared to G-FOBT and no screening. A hypothetical person invited for colorectal cancer screening with I-FOBT would on average save 0.003 life-years and €5 compared to G-FOBT and compared to no screening 0.006 life-years and €45. Ten years after a single round I-FOBT screening, in the Dutch population aged 50-75 years (n= 4,460,265), 25,200 life-years and €220 million would have been saved compared to no screening. I-FOBT remained the dominant screening strategy in sensitivity analyses when varying colorectal cancer incidence and major cost drivers. Conclusions: CRC screening with I-FOBT dominated G-FOBT and no screening. Accounting for uncertainty surrounding important parameters did not alter this conclusion. Table. Cost-effectiveness according to intention-to-screen analysis of one round immuno- chemical FOBT screening compared to one round guaiac FOBT screening or no screening *Difference in costs compared to I-FOBT †Average life-years per invited person for one round FOBT screening ‡Life-years gained compared to I-FOBT §Dominated i.e. costs and effects both favourable for I-FOBT M1014 For Patients with Colorectal Cancer, the Long-Term Use of Statins Is Associated with Better Clinical Outcomes Hector E. Nazario, Amar Mahgoub, Stuart J. Spechler, Ali Siddiqui Introduction: Statins, which have been used primarily to lower serum cholesterol levels and to protect against cardiovascular disease, have been shown to inhibit growth and to promote apoptosis in a variety of cancer cell types both In Vitro and In Vivo. For patients who develop cancers while taking statins, therefore, it is conceivable that the statins might favorably influence the biological behavior of the tumors. Aim: To explore the influence of the long-term use of statins on the presentation and prognosis of colorectal cancer (CRC). Methods: We conducted a retrospective, case-control study of male patients who were admitted to our hospital with a new diagnosis of CRC and who were followed for at least 5 years or until death. Patients were divided into two groups: 1) Statin Users who had taken statins continuously for at least 3 years prior to the diagnosis of CRC, and 2) Statin Non- Users who either had never taken statins or had not taken statins continuously during that same interval. We recorded the CRC location in the colon, tumor stage at presentation, the presence of metastases at presentation and deaths within 5-years of presentation. We also recorded demographic and clinical factors needed for tumor staging, and history of NSAID use. Those factors were examined by simple Chi-square and multivariate regression analysis models to determine independent predictors of advanced CRC after adjusting for age and NSAID use. Results: 1309 patients with a new diagnosis of CRC were identified (mean age 69 + 1.1(SE) years; 72% Caucasian, 24% African American and 4% Hispanic). There were 326 Statin Users and 983 Statin Non-Users. At the presentation of CRC, Statin Users had a less advanced tumor stage (2.2 vs. 2.6; p<0.01), a lesser prevalence of metastases (OR= A-331 AGA Abstracts 0.7 [0.4-0.9, 95%CI]; p<0.01), and more right-sided tumors (OR=1.6 [1.3-2.1], 95%CI]; p<0.01) than Statin Non-Users. The Statin Users also presented with CRC at an older age (68.7 vs. 66.7 years; p=0.001). Overall 5-year survival for the Statin Users was 56.4 % compared to 49.5% for the Statin Non-User group (OR=0.7 [0.6-0.9], 95%CI]; p=0.03). Kaplan-Meier analysis of survival revealed that Statin Users were significantly more likely to survive and to survive longer than Statin Non-Users (p=0.009), even when adjusted for stage at presentation. Conclusions: For patients who present to the hospital with a new diagnosis of CRC, those who use statins have less advanced tumor stages, a lesser prevalence of distant metastases and more right-sided tumors than non-users of statins. Statin use also is associated with better 5-year surviva M1015 The Yield of the First Surveillance Colonoscopy After Elective Resection of Colorectal Cancer Madelaine Plourde, Matthew Smith, Paul Johnson Colonoscopy plays central role in the diagnosis and surveillance of patients with colorectal cancer (CRC). Current guidelines vary in the recommended timing of the first surveillance colonoscopy after surgery (from 1-3 years). The purpose of this research was to examine the yield of the first surveillance colonoscopy after resection for CRC. All patients who underwent elective resection for CRC at a tertiary care referral center between January 2000 and June 2006 were identified for this retrospective cohort study. Data were collected regarding the pre-operative colon assessment and the first post-operative surveillance colon- oscopy. The primary outcome was the presence of advanced neoplasia (adenocarcinoma or adenoma > 1cm) at the time of surveillance colonoscopy. Elective resection of CRC was performed in 633 patients. Pre-operative colonoscopy was attempted in 539 patients and was successful in 399 (74%). Inability to pass the tumor was the most common reason for failure. Barium enema was the only pre-operative assessment in 94 patients. An additional 71 patients underwent barium enema after incomplete colonoscopy. Thus pre-operative assessment of the entire colon was performed in 567/633 (89%) patients. The first surveillance colonoscopy was completed within 1 year in 165 patients and within 3 years in 350 patients (165 + 185 patients). Advanced neoplasia was present in 7/165 patients (4.2% , 4 CRC and 3 adenomas >1cm) when colonoscopy was performed within one year of surgery and 11/ 350 patients (3.1% , 6 CRC and 5 adenomas >1cm) when colonoscopy was performed within 3 years of surgery. However, the rate of advanced neoplasia was significantly lower for patients who had a complete pre-operative colonoscopy as compared to patients who had a pre-operative barium enema (± incomplete colonoscopy) at both the 1 year and 3 year thresholds (1.7% versus 10% (p=0.04) and 1.6% versus 7% (p=0.01) respectively). Among the 252 patients who had pre-operative colonoscopy and post operative colonoscopy with 3 years of surgery, only 2 (0.8%) were found to have a CRC at the surveillance examination. These were identified 7 and 12 months after surgery and likely represent missed synchronous CRC. Complete colonoscopy was performed in only 63% of patients prior to elective resection for CRC. Patients who do undergo complete pre-oprerative colonos- copy have low rates of advanced neoplasia at the first surveillance colonoscopy performed within 3 years of surgery. Further data are needed to determine to optimal timing of the first surveillance examination. This has important implications for optimizing utilization of limited resources. M1016 Potential Savings for Federal Funding of a Colorectal Cancer Screening Program in Uninsured Patients: A Cost-Effectiveness Analysis Nison Badalov, Ian Wall, Jack Braha, Konstantin Vaizman, Rabin Rahmani, Jai Mirchandani, JianJun Li, Kadirawel Iswara, Scott M. Tenner Colorectal cancer is the second leading cause of cancer death in the United States. Screening for, detecting and removing precancerous adenomas or early colon cancers can decrease morbidity and mortality. Current guidelines recommend a screening colonoscopy for average risk individuals by age 50. Despite the widespread availability of colonoscopy, barriers exist in performing this potentially lifesaving procedure, including lack of insurance coverage. The Federal Government covers screening colonoscopy for Medicare beneficiaries, typically beginning at age 65. Unfortunately, this time period is 15 years later for those at average risk for colorectal cancer screening. In order to determine the effect of lack of coverage on screening, and determine the cost effectiveness of screening uninsured patients, the following cost effective analysis was performed. The number of uninsured patients eligible for colorectal cancer screening and the projected population for medicare eligibility was determined (www.census.gov/population/projections). The prevalence of colorectal polyps in this cohort including histology, number of polyps, incidence of carcinomas, and outcomes of screening, including number of cancers prevented was determined. The cost of performing a colonos- copy in an HOPD, including costs of biopsy, snare, and pathology was calculated.(www.cms/ feeschedule.2008). Projected costs of surveillance, complications of screening and treating expected colorectal cancers were included in the final analysis. Assuming all at risk, uninsured patients underwent a screening colonoscopy, the total cost of the program would be 242 million dollars, preventing 216,000 deaths. Despite this initial cost, by preventing the development of colon cancer in the uninsured population by age 65 (Medicare eligible), the Federal Government would save 814 million dollars. If we assume that the screening rate would be only 60% of the uninsured population (based on observed compliance), the cost would be 145 million dollars, preventing 130,032 deaths. This would still result in a cost savings to the Federal Government of 454 million dollars. We conclude that a federally funded colorectal cancer screening program would be cost effective to the government, saving 2 dollars for every dollar spent while avoiding unnecessary suffering from this preventable disease. AGA Abstracts
Transcript of M1013 a Cost-Effectiveness Analysis in Colorectal Cancer Screening Comparing Immunochemical Faecal...

4-part program (Discussion and Education, Documenting, Reporting and P4P) successfullyimproved WT and could likely be implemented in groups with strong governance andadequate EMR capabilities. We saw a trend toward increased AFR with increasing individual>6 minute WT, suggesting value in this compliance goal.
M1013
a Cost-Effectiveness Analysis in Colorectal Cancer Screening ComparingImmunochemical Faecal Occult Blood Tests with Guaiac Faecal Occult BloodTests and No Screening.Leo G. van Rossum, Anne Floortje van Rijn, Andre L. Verbeek, Martijn G. van Oijen,Robert J. Laheij, Paul Fockens, Jan B. Jansen, Eddy M. Adang, Evelien Dekker
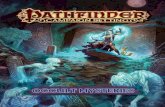
Introduction: The comparability of cost-effectiveness of colorectal cancer (CRC) screeningstrategies is limited if heterogeneous study data on tests, populations, and designs arecombined. Furthermore cost-effectiveness studies frequently suffer from unrealistic assump-tions, e.g. concerning differences in screening participation and adherence to follow-up.Based on empirical data from a representative randomised controlled screening trial withFOBT in the Netherlands (Van Rossum, et al. Gastroenterology 2008), we aimed to comparecost-effectiveness of one round of immunochemical faecal-occult-blood-test (OC-Sensor®,I-FOBT) screening, with one round of guaiac based faecal-occult-blood-test (Hemoccult-II®, G-FOBT) screening and no screening. Methods: We designed a Markov model of thecost-effectiveness of CRC screening with FOBT and no screening in asymptomatic averagerisk individuals between 50 and 75 years. From a third-party payer perspective we analyseddata with first and second order Monte Carlo simulation over 10 years of one year cycles.Empirical data were completed with cancer registry and literature data. Costs were presentedin Euros using a discount rate of 4%. Effects were measured as life years gained using adiscount rate of 1.5%. Results: I-FOBT resulted in more life years gained and costs saved(i.e. I-FOBT dominated) compared to G-FOBT and no screening. A hypothetical personinvited for colorectal cancer screening with I-FOBT would on average save 0.003 life-yearsand €5 compared to G-FOBT and compared to no screening 0.006 life-years and €45. Tenyears after a single round I-FOBT screening, in the Dutch population aged 50-75 years (n=4,460,265), 25,200 life-years and €220 million would have been saved compared to noscreening. I-FOBT remained the dominant screening strategy in sensitivity analyses whenvarying colorectal cancer incidence and major cost drivers. Conclusions: CRC screeningwith I-FOBT dominated G-FOBT and no screening. Accounting for uncertainty surroundingimportant parameters did not alter this conclusion.Table. Cost-effectiveness according to intention-to-screen analysis of one round immuno-chemical FOBT screening compared to one round guaiac FOBT screening or noscreening
*Difference in costs compared to I-FOBT †Average life-years per invited person for oneround FOBT screening ‡Life-years gained compared to I-FOBT §Dominated i.e. costs andeffects both favourable for I-FOBT
M1014
For Patients with Colorectal Cancer, the Long-Term Use of Statins IsAssociated with Better Clinical OutcomesHector E. Nazario, Amar Mahgoub, Stuart J. Spechler, Ali Siddiqui
Introduction: Statins, which have been used primarily to lower serum cholesterol levelsand to protect against cardiovascular disease, have been shown to inhibit growth and topromote apoptosis in a variety of cancer cell types both In Vitro and In Vivo. For patientswho develop cancers while taking statins, therefore, it is conceivable that the statins mightfavorably influence the biological behavior of the tumors. Aim: To explore the influence ofthe long-term use of statins on the presentation and prognosis of colorectal cancer (CRC).Methods: We conducted a retrospective, case-control study of male patients who wereadmitted to our hospital with a new diagnosis of CRC and who were followed for at least5 years or until death. Patients were divided into two groups: 1) Statin Users who had takenstatins continuously for at least 3 years prior to the diagnosis of CRC, and 2) Statin Non-Users who either had never taken statins or had not taken statins continuously during thatsame interval. We recorded the CRC location in the colon, tumor stage at presentation, thepresence of metastases at presentation and deaths within 5-years of presentation. We alsorecorded demographic and clinical factors needed for tumor staging, and history of NSAIDuse. Those factors were examined by simple Chi-square and multivariate regression analysismodels to determine independent predictors of advanced CRC after adjusting for age andNSAID use. Results: 1309 patients with a new diagnosis of CRC were identified (mean age69 + 1.1(SE) years; 72% Caucasian, 24% African American and 4% Hispanic). There were326 Statin Users and 983 Statin Non-Users. At the presentation of CRC, Statin Users hada less advanced tumor stage (2.2 vs. 2.6; p<0.01), a lesser prevalence of metastases (OR=
A-331 AGA Abstracts
0.7 [0.4-0.9, 95%CI]; p<0.01), and more right-sided tumors (OR=1.6 [1.3-2.1], 95%CI];p<0.01) than Statin Non-Users. The Statin Users also presented with CRC at an older age(68.7 vs. 66.7 years; p=0.001). Overall 5-year survival for the Statin Users was 56.4 %compared to 49.5% for the Statin Non-User group (OR=0.7 [0.6-0.9], 95%CI]; p=0.03).Kaplan-Meier analysis of survival revealed that Statin Users were significantly more likelyto survive and to survive longer than Statin Non-Users (p=0.009), even when adjusted forstage at presentation. Conclusions: For patients who present to the hospital with a newdiagnosis of CRC, those who use statins have less advanced tumor stages, a lesser prevalenceof distant metastases and more right-sided tumors than non-users of statins. Statin use alsois associated with better 5-year surviva
M1015
The Yield of the First Surveillance Colonoscopy After Elective Resection ofColorectal CancerMadelaine Plourde, Matthew Smith, Paul Johnson
Colonoscopy plays central role in the diagnosis and surveillance of patients with colorectalcancer (CRC). Current guidelines vary in the recommended timing of the first surveillancecolonoscopy after surgery (from 1-3 years). The purpose of this research was to examinethe yield of the first surveillance colonoscopy after resection for CRC. All patients whounderwent elective resection for CRC at a tertiary care referral center between January 2000and June 2006 were identified for this retrospective cohort study. Data were collectedregarding the pre-operative colon assessment and the first post-operative surveillance colon-oscopy. The primary outcome was the presence of advanced neoplasia (adenocarcinoma oradenoma > 1cm) at the time of surveillance colonoscopy. Elective resection of CRC wasperformed in 633 patients. Pre-operative colonoscopy was attempted in 539 patients andwas successful in 399 (74%). Inability to pass the tumor was the most common reason forfailure. Barium enema was the only pre-operative assessment in 94 patients. An additional71 patients underwent barium enema after incomplete colonoscopy. Thus pre-operativeassessment of the entire colon was performed in 567/633 (89%) patients. The first surveillancecolonoscopy was completed within 1 year in 165 patients and within 3 years in 350 patients(165 + 185 patients). Advanced neoplasia was present in 7/165 patients (4.2% , 4 CRC and3 adenomas >1cm) when colonoscopy was performed within one year of surgery and 11/350 patients (3.1% , 6 CRC and 5 adenomas >1cm) when colonoscopy was performedwithin 3 years of surgery. However, the rate of advanced neoplasia was significantly lowerfor patients who had a complete pre-operative colonoscopy as compared to patients whohad a pre-operative barium enema (± incomplete colonoscopy) at both the 1 year and 3year thresholds (1.7% versus 10% (p=0.04) and 1.6% versus 7% (p=0.01) respectively).Among the 252 patients who had pre-operative colonoscopy and post operative colonoscopywith 3 years of surgery, only 2 (0.8%) were found to have a CRC at the surveillanceexamination. These were identified 7 and 12 months after surgery and likely representmissed synchronous CRC. Complete colonoscopy was performed in only 63% of patientsprior to elective resection for CRC. Patients who do undergo complete pre-oprerative colonos-copy have low rates of advanced neoplasia at the first surveillance colonoscopy performedwithin 3 years of surgery. Further data are needed to determine to optimal timing of thefirst surveillance examination. This has important implications for optimizing utilization oflimited resources.
M1016
Potential Savings for Federal Funding of a Colorectal Cancer ScreeningProgram in Uninsured Patients: A Cost-Effectiveness AnalysisNison Badalov, Ian Wall, Jack Braha, Konstantin Vaizman, Rabin Rahmani, JaiMirchandani, JianJun Li, Kadirawel Iswara, Scott M. Tenner
Colorectal cancer is the second leading cause of cancer death in the United States. Screeningfor, detecting and removing precancerous adenomas or early colon cancers can decreasemorbidity and mortality. Current guidelines recommend a screening colonoscopy for averagerisk individuals by age 50. Despite the widespread availability of colonoscopy, barriers existin performing this potentially lifesaving procedure, including lack of insurance coverage.The Federal Government covers screening colonoscopy for Medicare beneficiaries, typicallybeginning at age 65. Unfortunately, this time period is 15 years later for those at averagerisk for colorectal cancer screening. In order to determine the effect of lack of coverage onscreening, and determine the cost effectiveness of screening uninsured patients, the followingcost effective analysis was performed. The number of uninsured patients eligible for colorectalcancer screening and the projected population for medicare eligibility was determined(www.census.gov/population/projections). The prevalence of colorectal polyps in this cohortincluding histology, number of polyps, incidence of carcinomas, and outcomes of screening,including number of cancers prevented was determined. The cost of performing a colonos-copy in an HOPD, including costs of biopsy, snare, and pathology was calculated.(www.cms/feeschedule.2008). Projected costs of surveillance, complications of screening and treatingexpected colorectal cancers were included in the final analysis. Assuming all at risk, uninsuredpatients underwent a screening colonoscopy, the total cost of the program would be 242million dollars, preventing 216,000 deaths. Despite this initial cost, by preventing thedevelopment of colon cancer in the uninsured population by age 65 (Medicare eligible),the Federal Government would save 814 million dollars. If we assume that the screeningrate would be only 60% of the uninsured population (based on observed compliance), thecost would be 145 million dollars, preventing 130,032 deaths. This would still result in acost savings to the Federal Government of 454 million dollars. We conclude that a federallyfunded colorectal cancer screening program would be cost effective to the government,saving 2 dollars for every dollar spent while avoiding unnecessary suffering from thispreventable disease.
AG
AA
bst
ract
s