Lymphoma 101
43
LYMPHOMA 101 Armaan Khalid
description
Lymphoma 101. Armaan Khalid. What is Lymphoma?. Cancer of the lymph nodes Lymphoma > Leukaemia Commonly manifest by the development of lymphadenopathy at single/multiple sites Classified on basis of histological appearance Hodgkin’s lymphoma (HL) Non-Hodgkin’s lymphoma (NHL). - PowerPoint PPT Presentation
Transcript of Lymphoma 101

LYMPHOMA 101Armaan Khalid

WHAT IS LYMPHOMA? Cancer of the lymph nodes Lymphoma > Leukaemia Commonly manifest by the development of
lymphadenopathy at single/multiple sites Classified on basis of histological appearance
Hodgkin’s lymphoma (HL) Non-Hodgkin’s lymphoma (NHL)

HODGKIN’S LYMPHOMA (HL) Involves primarily the lymph nodes ♂:♀ is 1.3:1 Peak incidence is in 3rd decade Tumour of B Cell origin Presence of Reed-Sternberg Cells on
pathology Often presents @ a single site & spreads in a
predictable fashion

AETIOLOGY OF HL ?Link with EBV Evidence linking previous infectious
mononucleosis with HL 40% of patients ↑ EBV titres @ time of
diagnosis

IT’S ALL ABOUT THE REED-STERNBERG’S Hallmark of HL is Reed-Sternberg cells Large cell w enlarged multilobulated nucleus,
prominent nucleoli & abundant eosinophilic cytoplasm
RS cell variants exist in HL subtypes Staging based on the Ann Arbor Classification
Used to stage both HL & NHL

CLASSIFICATION OF HL Nodular Sclerosing HL (70%)
Typically seen in young adults/adolescents & involving Mediastinal & neck LN
Characteristic cell is the lacunar type RS cells Overall prognosis is good
Mixed Cellularity HL (25%) Most common HL in pt > 50y/o, ♂ predominance Classical RS cells abundant Assoc with B symptoms Commonly affects abdominal LN & spleen Most common HL subtype in HIV +ve population

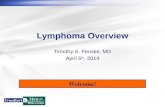
‘CLASSIC’ REED-STERNBERG CELLS
*Common in mixed-cellular subtype HL

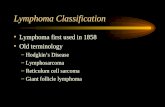
‘LACUNAR-TYPE’ RS CELLS
*Common in nodular sclerosis subtype HL

CLASSIFICATION OF HL Lymphocyte-rich HL (5%)
Characterised by an inflitrate of many small lymphocytes & RS cells; often an indolent disease
Lymphocyte-depleted HL (1%) Rare & lacks cellular infiltrate with numerous RS
cells Seen in HL assoc with HIV Patients usually w advanced stage disease
Nodular Lymphocyte-predominant HL (5%) Characterised by large number of small resting
lymphocytes admixed with benign histiocytes Classical RS cells difficult to find
Lympho-histiocytic (L&H) variant RS cell (popcorn cell)

PATHOGENESIS OF HL ??? Central issue: Lymphocytes of the B-cell
lineage not expressing immunoglobulins escape apoptosis
?Role of EBV Interferes w normal immune regulatory
mechanisms Often localised to single site & spreads in
pedictable fashion

CLINICAL FEATURES LN enlargement, esp. Cervical LN
Painless & of rubbery consistency Supra-diaphragmatic LNs affected in 80%
Hepatosplenomegaly B symptoms (40%)
Fever, drenching night sweats, weight loss > 10% in 6/12
Pruritis, fatigue, anorexia, lethargy, malaise Sg/Sx due to organ involvement
Due to mass effect (Bone, Lung, Cardiac, Gut) SVC Syndrome
Due to biochemical derangement

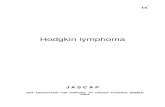
BEFORE & AFTER

WHAT IS CAUSING THE BLOCKAGE?

SUPERIOR VENA CAVA SYNDROME Obstruction of the SVC by an upper
mediastinal mass Sg/Sx
Difficulty breathing/swallowing Stridor, swollen, oedematous facies Venous congestion
Ix Imaging (CXR, CT chest, Invasive contrast
venogram) Rx
Based on what is causing the obstruction Steroids, diuretics, stenting, chemo/radioRx

DIFFERENTIALS Infectious Mononucleosis Lung Ca (Small Cell) HL NHL Rheumatoid Arthritis Sarcoidosis SLE

INVESTIGATIONS FBE ESR LFT Serum LDH (Correlates with ‘bulk’ of disease) CXR HIV screening CT scan PET scan Bone marrow aspirate & trephine (BMAT) LN biopsy

ANN ARBOR STAGING CLASSIFICATIONAnn Arbor Staging SystemStage I Involvement of 1 LN region or single extra-
lymphatic siteStage II Involvement of >1 LN region on the same side of
the diaphragmStage III Involvement of LN regions on both sides of the
diaphragmStage IV Diffuse/disseminated involvement of >1 extranodal
organs/tissue

FURTHER DESIGNATIONS TO ANN ARBORFurther Applicable Designation to the Ann ArborA No symptomsB B symptoms (Fever, night sweats, weight loss)X Bulky disease (Widening of mediastinum > 1/3)E Involvement of single extranodal site that is
contiguous/proximal to known nodal site

MANAGEMENT Rx taken with curative intent Rx based on:
Anatomical distribution of disease ‘Bulk’ Presence/Absence of ‘B’ symptoms

EARLY STAGE (IA, IIA, NO BULK) Brief chemotherapy + radiotherapy Example: ABVD or BEACOPP
A = Adriamycin (Doxorubicin) B = Bleomycin V = Vinblastine D = Dacarbazine

ADVANCED DISEASE Cyclical combination chemoRx w or w/o
radioRx Gold standard: ABVD Pt w bulk disease receive radioRx Curative 50-60% Risk of myelosuppression, infertility, 2°
malignancy & organ damage

NON-HODGKIN’S LYMPHOMA (NHL) Classified separately from HL 70% - 80% are of B Cell origin Incidence 15/100 000 per year in devt
countries Slight ♂ predominance Median age of presentation 55-75y/o Can be classified on the basis of origin
Tumours of B cells Tumours of T cells Tumours of NK cells

AETIOLOGY NHL Unknown cause; wide geographical variation ?Envt factors
EBV (Burkitt’s lymphoma) ↑% of lymphoma in pts with AIDS H. Pylori in gastric MALT lymphoma

BURKITT LYMPHOMA (AFRICAN SUBTYPE)

PATHOGENESIS NHL Malignant clonal expansion of lymphocytes
Due to errors in gene rearrangements or recombinations
Translocation errors with specific genes Burkitt’s (c-myc)


CLINICAL FEATURES Same as HL*
Same as HL
INVESTIGATIONS

CLINICAL DIFFERENCES B/W HL & NHLHodgkin’s Lymphoma Non-Hodgkin’s LymphomaOften localised to a single axial group of nodes (cervical, mediastinal, para-aortic)
More frequent involvement of multiple peripheral nodes
Orderly spread by contiguity Non-contiguous spreadMesenteric nodes & Waldeyer ring rarely involved
Mesenteric nodes & Waldeyer ring commonly involved
Extranodal involvement uncommon
Extranodal involvement common

FOLLICULAR B CELL LYMPHOMA HOPC Asymptomatic w painless generalised
lymphadenopathy Occurs ↓% in Asian population &
predominantly in older people (>20-30y/o) Ix indicates multiple site involvement (Bone
marrow infiltration is common) Runs a remitting & recurring clinical course Death due to:
Rx resistant disease Transformation to Diffuse Large B Cell Lymphoma
Bad prognostic factor, less curable Effects of Rx

MANAGEMENT Treat the symptoms, not the numbers
Leave the asymptomatic pt alone Watchful waiting & repeat biopsies
ChemoRx + RadioRx rCHOP
r = Rituximab C = Cyclophosphamide H = Hydroxydaunorubicin (Doxorubicin) O = Oncovin (Vincristine) P = Prednisolone

WHAT IS RITUXIMAB? Trade name: Rituxan or Mabthera Chimeric monoclonal antibody against CD20,
found primarily on the surface of B cells CD20 widely expressed on B cells, but is
absent on terminally differentiated plasma cells
Basically, it induces apoptosis of CD20+ cells

DIFFUSE LARGE B CELL LYMPHOMA Commonest NHL (50% adults) & invariably
fatal w/o Rx Treat to cure, expectant management
inappropriate >50% of young pts are cured Contra: Co-morbidities & pt’s will
HOPC Rapidly progressive lymphadenopathy,
symptomatic Infiltration of extranodal organs
Morphology Nuclei of neoplastic B cells are huge (x3-4 of
resting lymphocytes)

DIFFUSE LARGE B CELL LYMPHOMA

MANAGEMENT Rx decision based on staging Cyclical chemoRx + radioRx
rCHOP Bad prognostic factors
Disease progression during Rx Failure to achieve complete remission during
initial Rx

BURKITT’S LYMPHOMA Uncommon in the Western world
Endemic to Africa Close assoc w EBV Rapidly fatal w/o Rx HOPC lymphadenopathy, abdo mass, BM &
CNS infiltration (leukaemia & meningitis) Morphology
Starry sky pattern Assoc w translocations involving MYC gene

BURKITT’S LYMPHOMA

MANAGEMENT Supportive Rx
Hydration Prevent Tumour Lysis Syndrome!
Cyclical chemoRx + radioRx rEPOCH
r = Rituximab E = Etoposide P = Prednisolone O = Oncovin (Vincristine) C = Cyclophosphamide H = Hydroxydaunorubicin (Doxorubicin)
?African setting

PERIPHERAL T CELL LYMPHOMA (UNSPECIFIED) Most common type of adult T-cell lymphoma
Most common subtype of peripheral T Cell lymphoma
Often disseminated & aggressive

MANAGEMENT Treated similarly to B Cell lymphomas
Cyclical chemoRx + RadioRx Refer to haematologist
In general, overall Rx strategies are similar but success of complete remission is ↓ than B Cell lymphomas

TUMOUR LYSIS SYNDROME Iatrogenic cause, Rx causes massive
breakdown of tumour cells Intracellular contents released into
circulation Metabolic derangement
Uric acid, potassium & phosphate Complications
Can precipitate Acute Renal Failure Mgmt
Identify high-risk pts Allopurinol given prophylactically Close monitor of electrolytes Baseline ECGs & follow-ups

CASE STUDY #1 62 y/o woman referred for Ix of neck mass
HOPC Enlarging L neck lump over last 6/52, no pain Fatigue, unwell & LOW 3kg
O/E Afebrile, no pallor/jaundice & peripheral oedema BP 170/105 & prominent but undisplaced apex beat L supraclavicular LN (firm, non-tender) Abdo NAD, soft, tender X2 enlarged LN in L groin Urinalysis +1 protein
Other Info Hx of HTN (felodipine 5mg bd) Non-smoker & social drinker

QUESTION TIME What further info should be elicited from
Hx/Ex? DDx? Ix? Staging the pt? Mgmt & considerations?

INTERESTING FACT OF THE DAY: BREAST IMPLANTATION & LYMPHOMA Epidemiological studies indicate link b/w
silicone breast implants & anaplastic large cell lymphoma (ALCL) ALCL devt in at least 60 women
2/3 occurred in silicone implants 1/3 occurred in saline implants
Considered to be related because ALCL occurred uniformly in breast tissue
FDA labelled silicone as inert, Grade 2 Later relabelled to Grade 3 (somewhat
dangerous)