Lupus and the heart
23
Lupus and the Heart Maryann Lee, MD UPG Rheumatology Staten Island, NY
-
Upload
lupusny -
Category
Health & Medicine
-
view
1.260 -
download
1
Transcript of Lupus and the heart

Lupus and the Heart
Maryann Lee, MDUPG Rheumatology
Staten Island, NY

What is Lupus?Systemic lupus erythematosus is a chronic inflammatory disease of unknown cause that can affect any organ in the body including the skin, joints, kidneys, lungs, nervous system, and the heart.

Lupus affects more women than men usually in their 20s and 30s during their child bearing years.
It is characterized by periods of remissions and chronic or acute relapses or “flares”
Common symptoms are fatigue, fever, weight loss, joint and muscle pain, sores in the mouth or nose, rashes the most common of which is the “butterfly” or malar rash after sun exposure, and Raynauds or microvasospasm of the small blood vessels especialy in the hands or feet.
Lupus can affect any organ especially the kidneys and heart so your Rheumatologist is always on the lookout for any signs of problems in these organ systems.

How does Lupus happen?Lupus can be like the game of telephone.
http://www.flickr.com/photos/fuffer2005/3006563299/lightbox/
The initial order from your body’s immune system may be protective but somewhere down the road the order gets changed and things take a wrong turn.

Something derails the normal message and the body attacks itself in lupus and makes antibodies that reacts with itself leading to the symptoms/disease of lupus. These antibodies seem to only be markers of lupus and an immune system problem . These antibodies have not been found to cause lupus on their own and so the cause of lupus is still unknown.

These antibodies can then travel throughout the body and trigger other chemical signals which leads to inflammation in different parts of the body and can cause damage in these different organs including the heart in various ways

Non Coronary Heart diseaseValvular diseaseThe heart has 4 valves that control the flow of blood circulating through your body
These valves can be injured by bacterial infection or by immune complexes of antibody/antigen reactions that occur during lupus activity.
More inflammation is then triggered and in the process of healing , fibrosis, scarring and calcification can occur, which can ultimately damage the valves
Often this is asymptomatic to the patient but over time valves can become stiff or floppy and not work as effectively leading to heart failure

These damaged valves are also more prone to bacterial infection or sometimes fragments of deposits on the valves caused by the lupus inflammatory process can break off and cause emboli leading to strokes
Patients with antiphospholipid antibodies are also at a higher risk for endocarditis perhaps from increased deposition of antibody complexes

What can we do about it?Antibiotic prophylaxis for lupus patients with valvular lesions is not an absolute recommendation by the AHA but is suggested especially when the patient is undergoing procedures that may cause transient bacteremia which include:
Invasive dental procedures/surgeriesSurgery of the respiratory tract such as tonsillectomy or bronchoscopyInvasive surgery/procedure of the GI tract

Steroids and other immunosuppressive therapy does not seem effective for these valve deposits.
Anticoagulation may be helpful for Antiphospholipid antibody associated valve deposits.
Patients with cardiac symptoms suggestive of valve disease should undergo echocardiogram testing however screening of asymptomatic patients is not recommended
What can we do about it?

Pericardial diseaseIt is usually asymptomatic and found incidentally but is the most frequent cause of symptomatic cardiac disease
Pericarditis refers to inflammation of the lining around the heart .
Symptoms include positional substernal chest pain with abnormal heart sounds on exam.
Pericardial effusion will occur at some point at least half of lupus patients
Pericarditis/pericardial effusion usually occurs when lupus is active

Usually it is a benign condition and is treated with NSAIDS/anti-inflammatories and sometimes steroids with success
If fluid has built up significantly around the heart surgical drainage would be required
Myocarditis occurs when the heart muscle is inflamed and is a much more serious condition but fortunately occurs rarely but can be treated with immunosupressant medications and would need be treated aggressively to prevent irreversible heart damage

Conduction defectsConduction defects where the electrical system of the heart is disrupted sometimes occurs as a result of myocarditis episode.
Usually it is a result of inflammation and fibrosis of the conduction system of the heart and can lead to arrythmias such as heart block.
Most often it is a first degree heart block and often short term and reverses with time. Higher degree heart block are not usually seen in adult lupus patients.

Neonatal lupusNeonatal lupus is observed in 1-2 % of babies born to mothers with autoimmune disease. There seems to be an association with Ro and La antibodies carried by the mother being transferred the the fetus
There is an increased incidence up to 17% in mothers with Ro and La antibodies who already had a previous child with heart block. Still this is a minority of births.
Symptoms include a facial/body rash that can occur up to 4 months old
Cardiac manifestations such has heart block usually occurs in utero or in the neonatal period. It is less common after birth ( a Toronto based study reported an incidence after birth of only 5%) This heart block is irreversible and life threatening and requires aggressive fetal monitoring during pregnancy.

Coronary heart disease and lupusPatients with SLE have been found to have an increased risk of accelerated atherosclerosis leading to coronary heart disease and heart attack
Several studies have given reports of up to double the risk of heart disease in young women with SLE in their 30s and 40s as opposed to other women at that age without SLE

Coronary heart disease and lupusWith improvements in treatments of other life-threatening organ disease caused by lupus such as kidney failure coronary artery disease is emerging as the leading cause of morbidity and premature death in patients with SLE
Reasons for this are likely multifactorial:Traditional risk factors such as diabetes, high cholesterol, hypertension, family history, obesity, sedentary lifestyle, cigarette smoking are still important modifiable risk factors
Other factors special to lupus include steroid use and lupus itself are factors as well

We know now that atherosclerosis itself is an inflammatory process with activation of the immue system and inflammation driven processes that lead to the plaques that causes blockages in the arteries of the heart
Image from medscape.org

We also know that Lupus specific factors likely play a role here.Certain antibodies associated with lupus stimulates the production and storage of cholesterol
Lupus also affects your blood vessels and how they respond to stress and injury and affect their inherent repair mechanisms
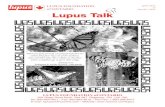
Standard Risk Factors
AgeHypertensionHyperlipidemiaHyperglycemiaSmokingGenetic factors
Systemic inflammationAutoantibodies to endothelium,HDL, phospholipidsCirculating immune complexesActivated complement productsNephritisDyslipidemia
SLE-Related Risk Factors
HDL
Smooth-muscle cells
OxidizedLDL
Foam cellCalcium
MonocyteMacrophage
Endothelium
Image from Hahn, B. n engl j med349;25, december18, 2003

Traditional risk factorsNumerous studies have shown an increased prevalence in Lupus patients of certain risk factors for heart disease including
HypertensionDiabetesPremature menopauseSedentary lifestyleAt risk body habitusMetabolic syndrome (central obesity, high cholesterol, diabetes)

Lupus related risk factorsSteroid use- can cause or worsen traditional risk factors like high cholesterol, diabetes, and obesity
- dose and duration of steroid use may be an important factor with higher dose and longer use may also be a maker of more active SLE
Active SLE which indicates an active inflammatory state may also in itself be a risk factor for accelerated atherosclerosis and heart disease

Screening ToolsCholesterol screening
Stress test and echocardiograms
CT of the heart looking for calcification
Carotid artery ultrasound
Cardiac mri

Prevention and treatmentCheck your cholesterol levels regularlyCurrent recommendations suggest treating SLE patients as having a cardiac equivalent which means treating to goals of a LDL cholesterol less than 100 with cholesterol lowering drugs
Certain trials have shown statins which are effective cholesterol lowering drugs also have an anti-inflammatory effect
Plaquenil which is a useful medication in the treatment of several manifestations of lupus has also been shown to have lipid lowering effects – C. Tang, T. Gofrey, et. al, Int Med Journal, July 2012; 968-978.

Controlling risk factors- things you can doDiabetes – control glucose with medications and diet and lifestyle changes
Hypertension control with medications, diet and lifestyle changes
IF possible reduce steroid dose as much as possible
Stop smoking
Weight control and reducing obesity
Healthy well balanced diet – low fat, high fiber diet incorporating fresh fruits and vegetables and lean proteins is the way to go. there is no proven “anti-inflammatory diet”
Exercise regularly – improves blood pressure, lowers cholesterol, improves fatigue, aids weight loss