
a study on inventory control system practice in kuantan food ...
Upload
suhazeli-abdullahCategory
view
91download
3description

Balancing the cost and benefits of modern biphasic insulin
in primary care
Dr. Noor Lita Adam
Consultant Endocrinologist
Hospital tuanku Ja’afar

The diabetes epidemic Significant increases in prevalence projected by 2030
Adapted from IDF Diabetes Atlas 5th Ed. 2011
North America Europe
Middle East and North Africa
Africa
South and Central America
Western Pacific
Southeast Asia
Data shown for each region includes: Millions of people with diabetes 2011 → Global projections for 2030
Projected increase from 2011 to 2030
World 2011 = 366 million
2030 = 552 million
Increase 51%
37.7 → 51.2 36%
25.1→39.9 59%
14.7→28.0 90%
32.8→59.7 83%
52.6→64.0 22%
71.4→120.9 69%
131.9→187.9 42%
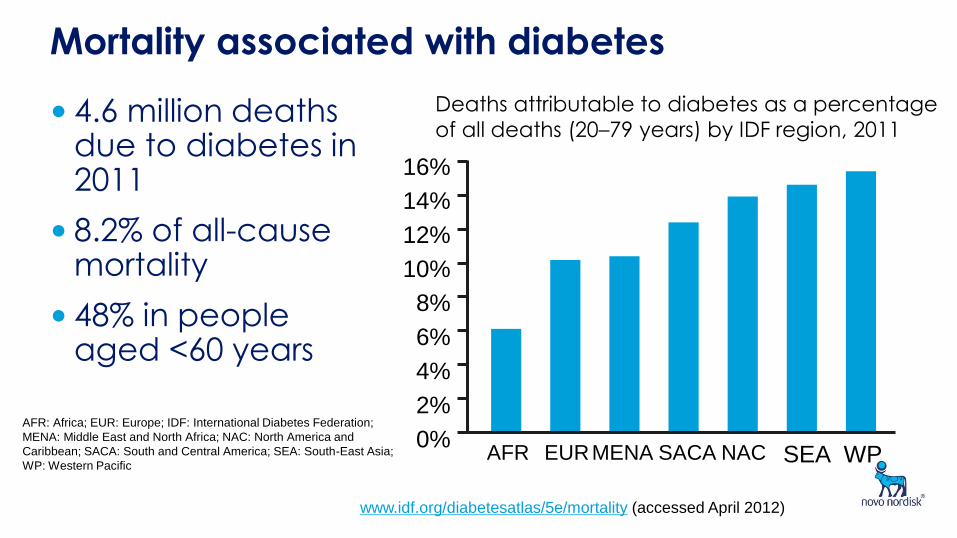
Mortality associated with diabetes
• 4.6 million deaths due to diabetes in 2011
• 8.2% of all-cause mortality
• 48% in people aged <60 years
16%
Deaths attributable to diabetes as a percentage
of all deaths (20–79 years) by IDF region, 2011
14%
12%
10%
8%
6%
4%
0%
2%
AFR EUR MENA SACA NAC SEA WP
www.idf.org/diabetesatlas/5e/mortality (accessed April 2012)
AFR: Africa; EUR: Europe; IDF: International Diabetes Federation;
MENA: Middle East and North Africa; NAC: North America and
Caribbean; SACA: South and Central America; SEA: South-East Asia;
WP: Western Pacific
4
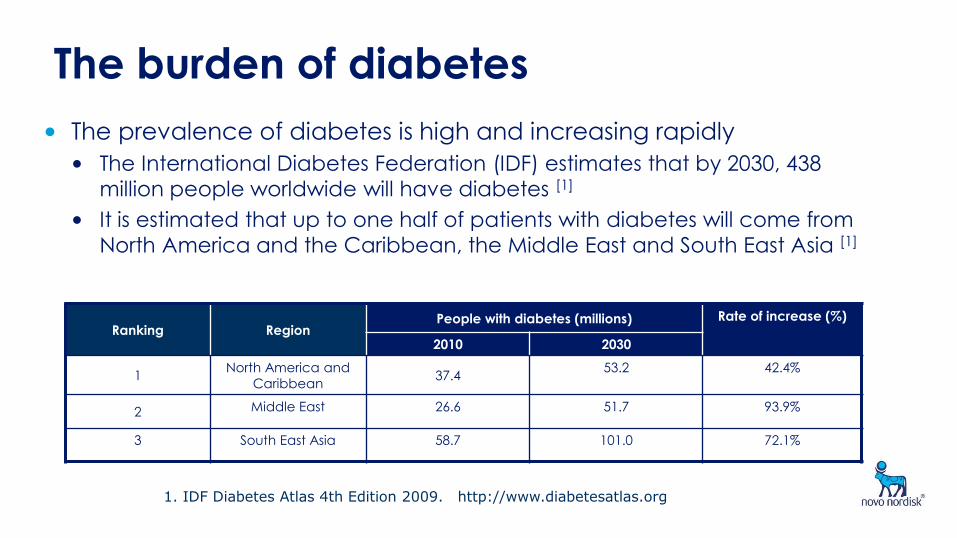
The burden of diabetes
• The prevalence of diabetes is high and increasing rapidly
• The International Diabetes Federation (IDF) estimates that by 2030, 438
million people worldwide will have diabetes [1]
• It is estimated that up to one half of patients with diabetes will come from
North America and the Caribbean, the Middle East and South East Asia [1]
Ranking Region People with diabetes (millions) Rate of increase (%)
2010 2030
1 North America and
Caribbean 37.4
53.2 42.4%
2 Middle East 26.6 51.7 93.9%
3 South East Asia 58.7 101.0 72.1%
1. IDF Diabetes Atlas 4th Edition 2009. http://www.diabetesatlas.org
5
The burden of diabetes
• Diabetes is among the top ten leading causes of death
• Worldwide, almost 4 million deaths are attributable to diabetes (6.8% of all deaths) [1]
• This is a 5.5% increase over 2007 estimates and diabetes deaths will continue to increase unless urgent action is taken to address the problem[1]
• Diabetes decreases life expectancy by >7 years in patients aged >50 years [2]
• The CDC estimated that the risk of death among people with diabetes is twice that of people without diabetes of the same age [3]
1. IDF Diabetes Atlas 4th Edition 2009. http://www.diabetesatlas.org 2. Franco OH et al.. Associations of Diabetes Mellitus With Total Life Expectancy and Life Expectancy With and Without Cardiovascular Disease. Arch Intern Med. 2007;167(11):1145-1151. 3. CDC http://www.cdc.gov/diabetes/pubs/pdf/ndfs_2007.pdf
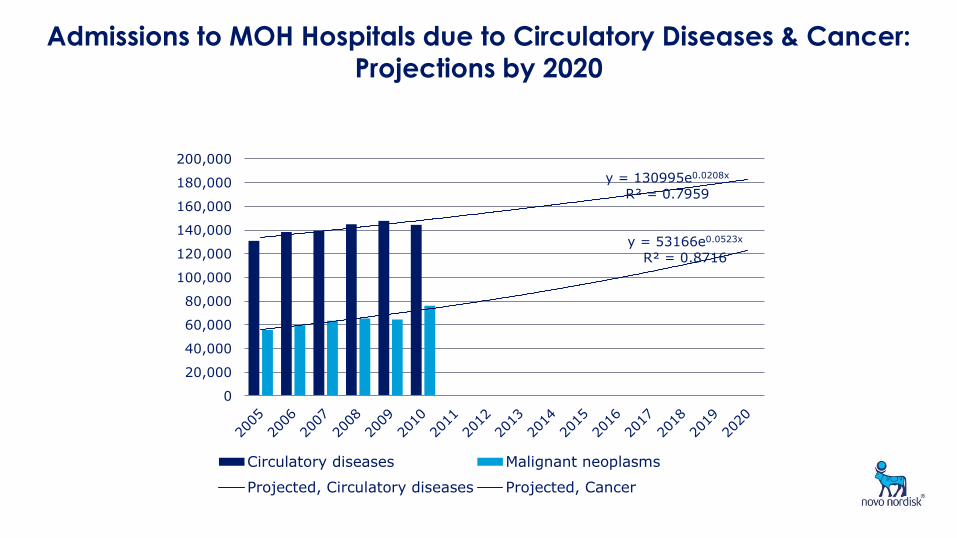
Admissions to MOH Hospitals due to Circulatory Diseases & Cancer:
Projections by 2020
y = 130995e0.0208x
R² = 0.7959
y = 53166e0.0523x
R² = 0.8716
0
20,000
40,000
60,000
80,000
100,000
120,000
140,000
160,000
180,000
200,000
Circulatory diseases Malignant neoplasms
Projected, Circulatory diseases Projected, Cancer
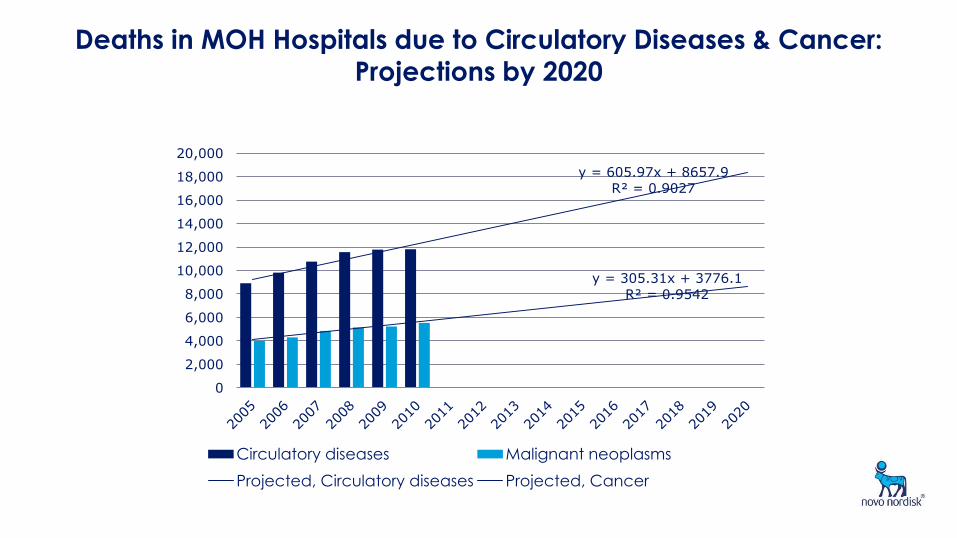
Deaths in MOH Hospitals due to Circulatory Diseases & Cancer: Projections by 2020
y = 605.97x + 8657.9
R² = 0.9027
y = 305.31x + 3776.1
R² = 0.9542
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
18,000
20,000
Circulatory diseases Malignant neoplasms
Projected, Circulatory diseases Projected, Cancer
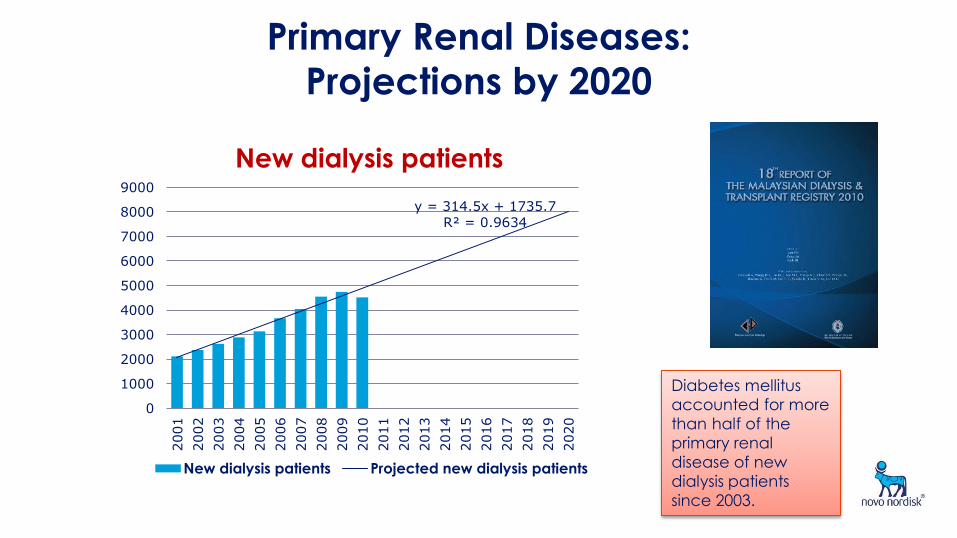
Primary Renal Diseases:
Projections by 2020
y = 314.5x + 1735.7 R² = 0.9634
0
1000
2000
3000
4000
5000
6000
7000
8000
90002001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
New dialysis patients
New dialysis patients Projected new dialysis patients
Diabetes mellitus
accounted for more
than half of the
primary renal
disease of new
dialysis patients
since 2003.
9
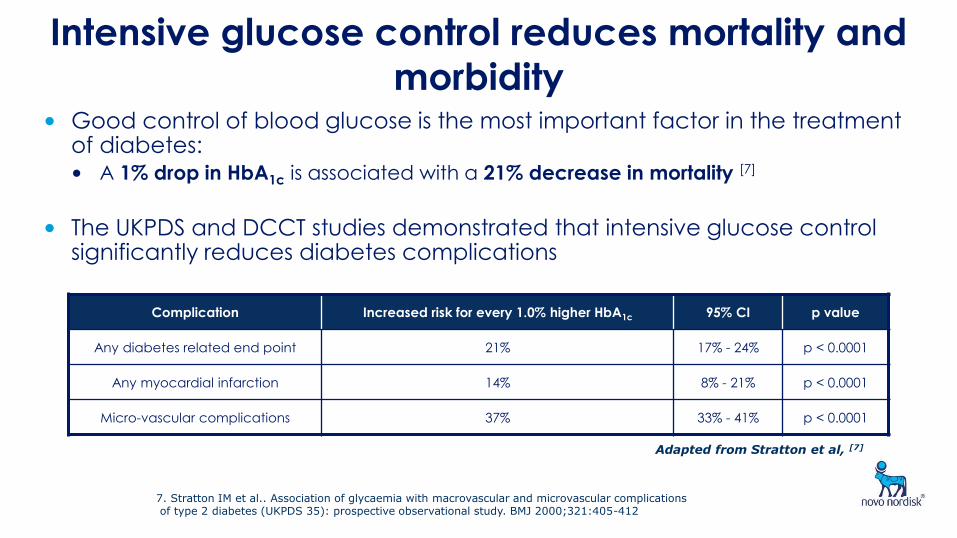
Intensive glucose control reduces mortality and
morbidity • Good control of blood glucose is the most important factor in the treatment
of diabetes: • A 1% drop in HbA1c is associated with a 21% decrease in mortality [7]
• The UKPDS and DCCT studies demonstrated that intensive glucose control significantly reduces diabetes complications
Complication Increased risk for every 1.0% higher HbA1c 95% CI p value
Any diabetes related end point 21% 17% - 24% p < 0.0001
Any myocardial infarction 14% 8% - 21% p < 0.0001
Micro-vascular complications 37% 33% - 41% p < 0.0001
Adapted from Stratton et al, [7]
7. Stratton IM et al.. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ 2000;321:405-412
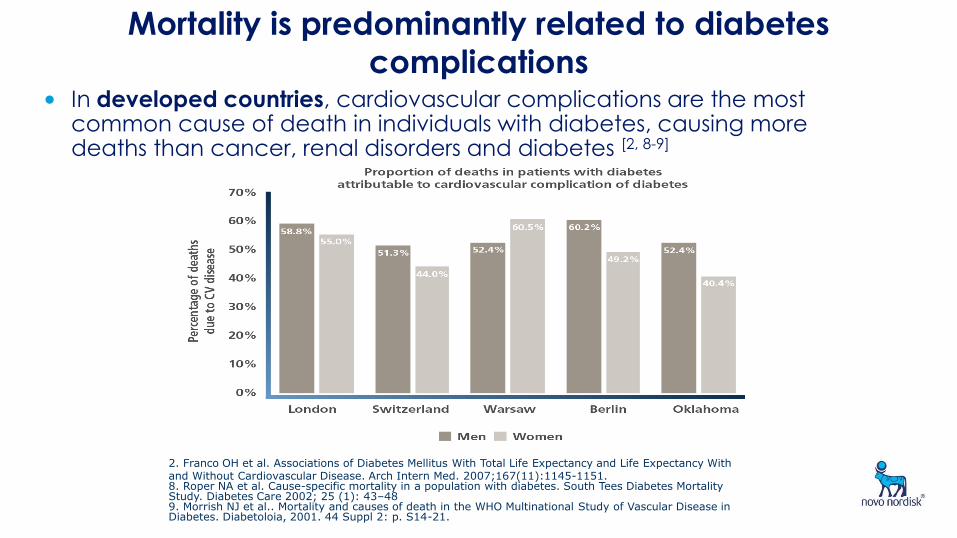
10 Mortality is predominantly related to diabetes
complications • In developed countries, cardiovascular complications are the most
common cause of death in individuals with diabetes, causing more deaths than cancer, renal disorders and diabetes [2, 8-9]
2. Franco OH et al. Associations of Diabetes Mellitus With Total Life Expectancy and Life Expectancy With and Without Cardiovascular Disease. Arch Intern Med. 2007;167(11):1145-1151. 8. Roper NA et al. Cause-specific mortality in a population with diabetes. South Tees Diabetes Mortality Study. Diabetes Care 2002; 25 (1): 43–48 9. Morrish NJ et al.. Mortality and causes of death in the WHO Multinational Study of Vascular Disease in Diabetes. Diabetoloia, 2001. 44 Suppl 2: p. S14-21.

11
Morbidity is predominantly related to diabetes
complications
• Diabetes related complications negatively impact on patient quality of life [11-13]
11. Wexler D et al.: Correlates of health-related quality of life in type 2 diabetes. Diabetologia 2006, 49:1489–1497. 12. Clarke P, Gray A, Holman R. Estimating utility values for health states of type 2 diabetic patients using the EQ-. 5D (UKPDS 62). Medical Decision Making, 22(4), 340–349. 13. Coffey JT et al.: Valuing health-related quality of life in diabetes. Diabetes Care 2002 , 25(12):2238-2243.
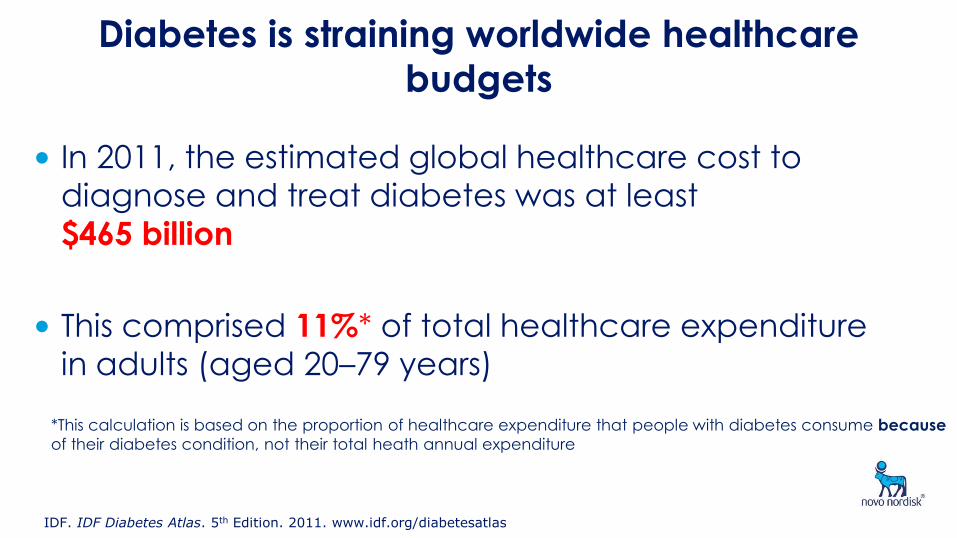
Diabetes is straining worldwide healthcare
budgets
• In 2011, the estimated global healthcare cost to
diagnose and treat diabetes was at least
$465 billion
• This comprised 11%* of total healthcare expenditure
in adults (aged 20–79 years)
*This calculation is based on the proportion of healthcare expenditure that people with diabetes consume because
of their diabetes condition, not their total heath annual expenditure
IDF. IDF Diabetes Atlas. 5th Edition. 2011. www.idf.org/diabetesatlas
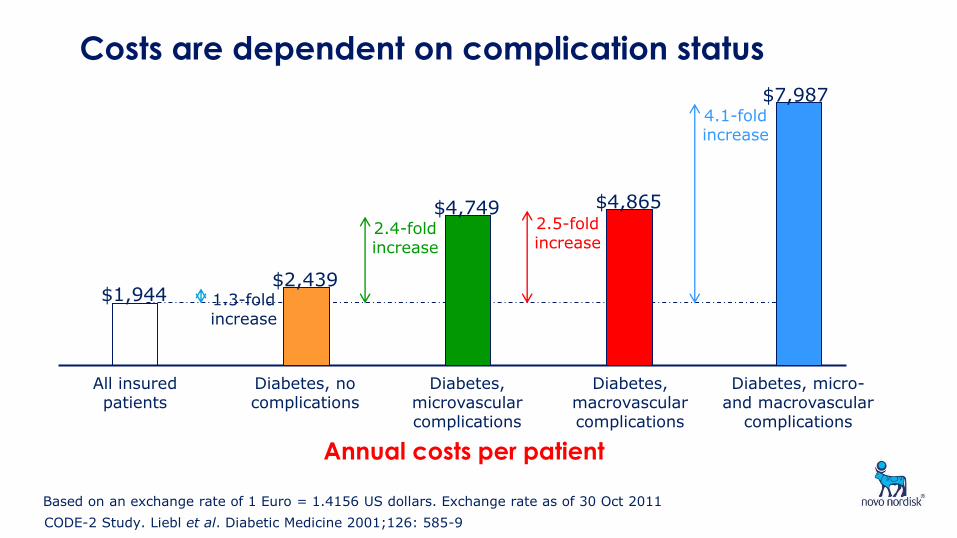
Costs are dependent on complication status
$1,944 1.3-fold increase
$2,439
$4,749 2.4-fold increase
$4,865 2.5-fold increase
$7,987 4.1-fold increase
All insured patients
Diabetes, no complications
Diabetes, microvascular complications
Diabetes, macrovascular complications
Diabetes, micro- and macrovascular
complications
CODE-2 Study. Liebl et al. Diabetic Medicine 2001;126: 585-9
Annual costs per patient
Based on an exchange rate of 1 Euro = 1.4156 US dollars. Exchange rate as of 30 Oct 2011
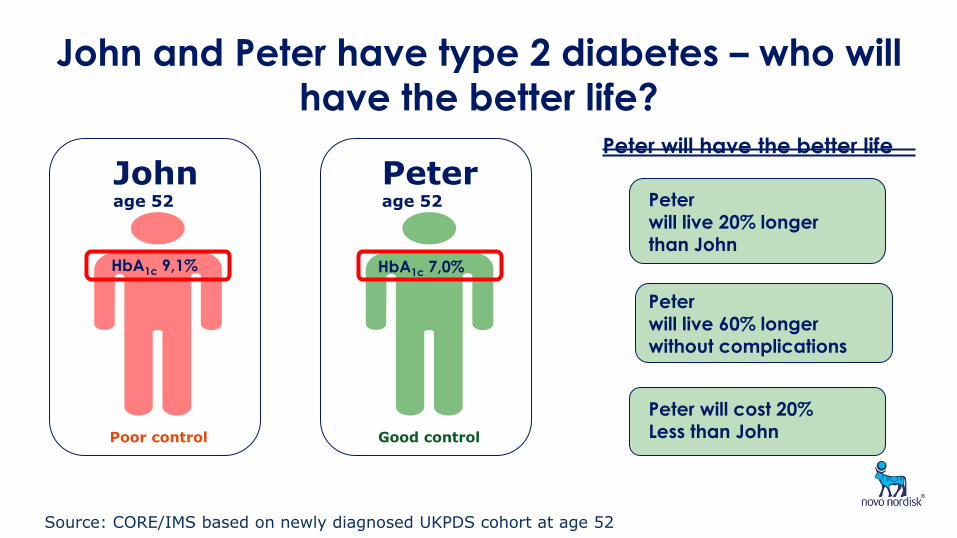
John and Peter have type 2 diabetes – who will
have the better life?
John age 52
Peter age 52
Poor control Good control
HbA1c 9,1% HbA1c 7,0%
Peter will have the better life
Peter will live 20% longer
than John
Peter will live 60% longer without complications
Peter will cost 20% Less than John
Source: CORE/IMS based on newly diagnosed UKPDS cohort at age 52
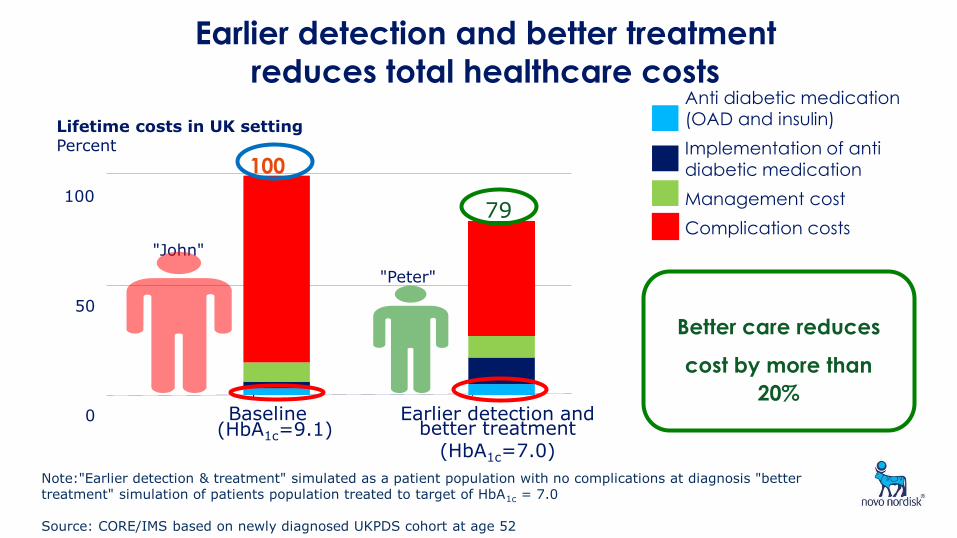
Lifetime costs in UK setting Percent
100
79
85
9 3 3
66
13
15
7
0
50
100
Baseline (HbA1c=9.1)
Earlier detection and better treatment
(HbA1c=7.0)
"John"
"Peter"
Earlier detection and better treatment
reduces total healthcare costs Anti diabetic medication
(OAD and insulin)
Implementation of anti
diabetic medication
Management cost
Complication costs
Note:"Earlier detection & treatment" simulated as a patient population with no complications at diagnosis "better treatment" simulation of patients population treated to target of HbA1c = 7.0 Source: CORE/IMS based on newly diagnosed UKPDS cohort at age 52
Better care reduces
cost by more than 20%
CO
ST R
ELA
TIV
E TO
20
10
BA
SE V
ALU
ES (
%)
2010 2015 2020 2025 2030 90
100
110
120
130
140
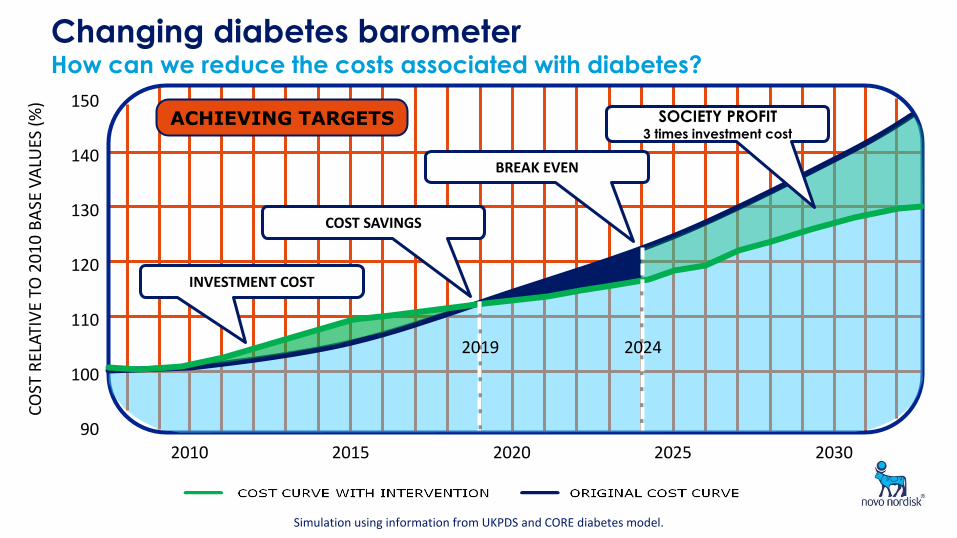
150 ACHIEVING TARGETS
2019 2024
INVESTMENT COST
COST SAVINGS
BREAK EVEN
SOCIETY PROFIT 3 times investment cost
Simulation using information from UKPDS and CORE diabetes model.
Changing diabetes barometer How can we reduce the costs associated with diabetes?
CO
ST R
ELA
TIV
E TO
20
10
BA
SE V
ALU
ES (
%)
2010 2015 2020 2025 2030 90
100
110
120
130
140
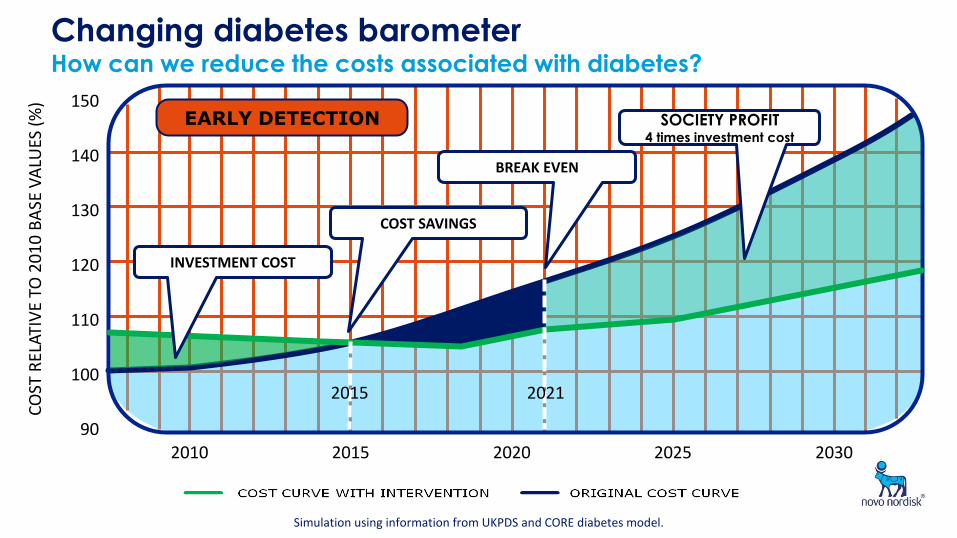
150 EARLY DETECTION
2015 2021
INVESTMENT COST
COST SAVINGS
BREAK EVEN
SOCIETY PROFIT 4 times investment cost
Simulation using information from UKPDS and CORE diabetes model.
Changing diabetes barometer How can we reduce the costs associated with diabetes?
CO
ST R
ELA
TIV
E TO
20
10
BA
SE V
ALU
ES (
%)
2010 2015 2020 2025 2030 90
100
110
120
130
140
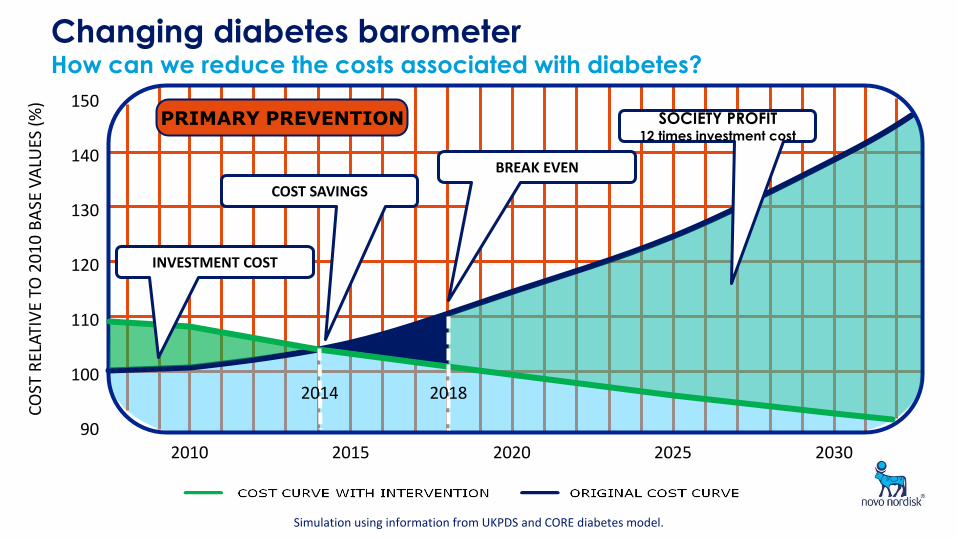
150 PRIMARY PREVENTION
2014 2018
INVESTMENT COST
COST SAVINGS
BREAK EVEN
SOCIETY PROFIT 12 times investment cost
Simulation using information from UKPDS and CORE diabetes model.
Changing diabetes barometer How can we reduce the costs associated with diabetes?
What are the limitations of older, traditional human
insulins?
• Hypoglycaemia – Relatively common side effect and the most feared complication of insulin therapy1
• Lack of flexibility – Having to inject at least 30 minutes prior to a meal, meaning meal times have to be planned2
• Weight gain – Consistent weight gain seen in both type 1 and type 2
diabetes3
• Variability/‘unpredictability’ – The same dose of insulin can have a different impact on glucose levels, making it harder to self-titrate treatment4
• Adherence – The possibility of hypoglycaemia and the lack of flexibility around mealtimes could impact on adherence5
Why are modern biphasic insulin superior to
biphasic human insulin?
Improved adherence to treatment
Patients are less likely to develop diabetic complications that are expensive to treat
Improved glycaemic control
Better safety profile
More dosing flexibility
Functional benefits
of Modern Insulins
References 1-10
Poor compliance to diabetes medication impairs blood glucose control, which results in expensive diabetic complications, such as blindness, amputations and kidney failure
Barriers to compliance with diabetes medication include patient fear of hypoglycaemia, weight gain and the inconvenience of planning mealtimes around treatment
Novo Nordisk’s portfolio of modern insulins are better at glycaemic control compared to human
insulin, and improve patient adherence as they reduce hypoglycaemic events, enable more flexible dosing and cause less weight gain
Modern insulins improve glycaemic control and adherence/compliance to treatment, making patients less likely to develop diabetic complications that are expensive to treat
Modern biphasic insulins provide better value than
biphasic human insulin
References 1-10
Modern biphasic insulin have a better safety profile than
biphasic human insulin
NovoMix® 30
Significantly
reduces the risk of
major
hypoglycaemic
events7
Patients have less fear of hypoglycaemia
Patients are more likely to comply with their treatment regimen and have better glycaemic control
Patients are less likely to develop diabetic complications that are expensive to treat
Modern biphasic insulin allow for more dosing flexibility than biphasic human insulin
NovoMix® 30
Provides more
predictable control
and option of simple
intensification of
dosing / injections.
Faster acting -
removes necessity to
plan mealtimes9 Patients find that their treatment regimen does not have as great an impact on their lifestyle
Patients are less likely to develop diabetic complications that are expensive to treat
Patients are more likely to comply with their treatment regimen and have better glycaemic control
NovoMix® 30
Better glycaemic control
without an increase in
hypoglycaemic events10
Modern biphasic insulin are better than biphasic human insulin in
controlling blood glucose levels with less hypoglycaemia
Patients’ blood glucose is better controlled throughout the day
HbA1c levels are reduced
Patients are less likely to develop diabetic complications that are
expensive to treat
Switch from biphasic human insulin
(BHI)
to BIAsp 30
Physicians Routine Evaluation of Safety and Efficacy of NovoMix 30 Therapy) PRESENT study
• Transferring type 2 diabetes patients with uncontrolled glycaemia from biphasic human insulin to biphasic insulin aspart 30
- to assess the safety and efficacy of biphasic insulin aspart (BIAsp30) used in routine clinical practice.
Shestakova, M. et al Current Medical Research and Opinion,
Volume 23, Number 12, Dec 2007 , pp. 3209-3214(6)
PRESENT study - results
Glycaemia improved significantly (mean ± SD):
• HbA1c by 1.58 ± 1.69% points (from 9.32 ± 1.64% to 7.70 ± 1.29%),
• FPG by 2.92 ± 3.71 mmol/L and PPPG by 4.75 ± 4.87 mmol/L.
• The incidence of hypoglycaemic episodes decreased over time, from 38.7% (baseline) to 20.8% (6 months).
In this observational study, in the type 2 diabetes mellitus patients who were poorly controlled on BHI, glycaemia improved when transferred to BIAsp30, and a lower incidence or rate of hypoglycaemia was observed in these patients.
A1chieve® global data
Home et al. Diabetes Res Clin Pract 2011;94:352–63
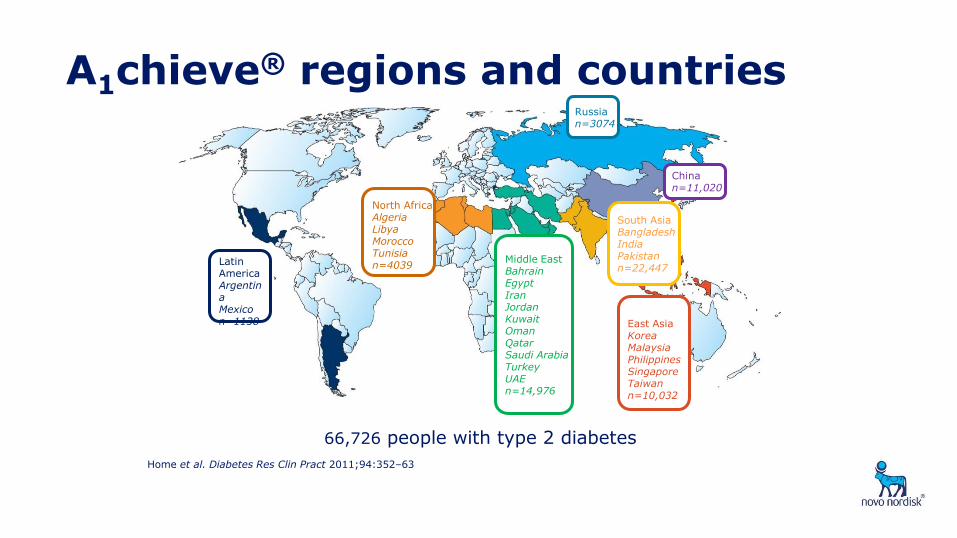
A1chieve® regions and countries
Home et al. Diabetes Res Clin Pract 2011;94:352–63
Latin America Argentina Mexico n=1138
South Asia Bangladesh India Pakistan n=22,447
North Africa Algeria Libya Morocco Tunisia n=4039
Middle East Bahrain Egypt Iran Jordan Kuwait Oman Qatar Saudi Arabia Turkey UAE n=14,976
China n=11,020
Russia n=3074
East Asia Korea Malaysia Philippines Singapore Taiwan n=10,032
66,726 people with type 2 diabetes
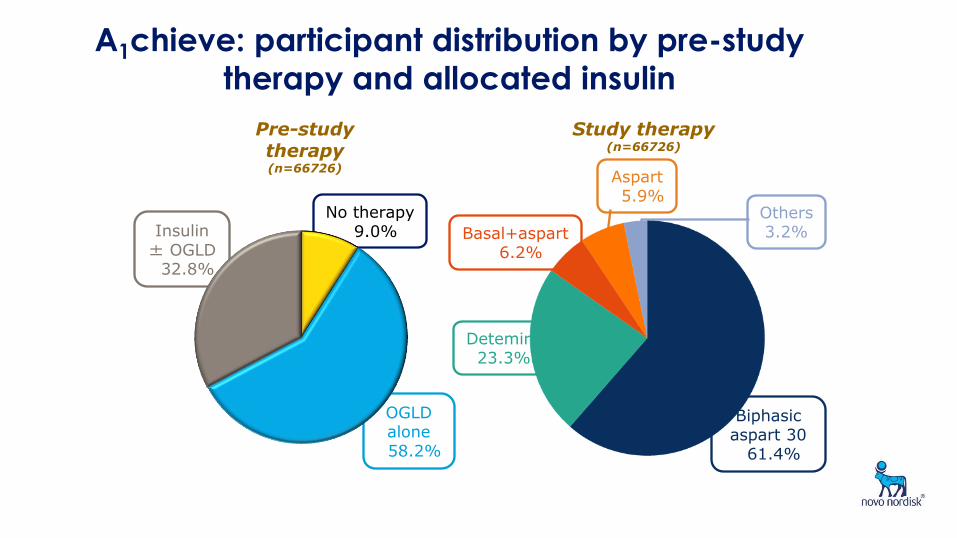
Detemir 23.3%
Insulin ± OGLD 32.8%
No therapy 9.0%
OGLD alone
58.2%
Basal+aspart 6.2%
Others 3.2%
Aspart 5.9%
A1chieve: participant distribution by pre-study
therapy and allocated insulin
Study therapy (n=66726)
Pre-study therapy (n=66726)
Biphasic aspart 30 61.4%

A1chieve subgroup: Change in HbA1c Participants switching from BHI to BIAsp 30
Hussein Z et al. J Diab Invest 2012; 3 (Suppl. 1): 200 (Abstract PCS-18-1)
Baseline to 24 weeks
Baseline HbA1c 9.4 n 465
p<0.001
-1.0
-1.5
0.0
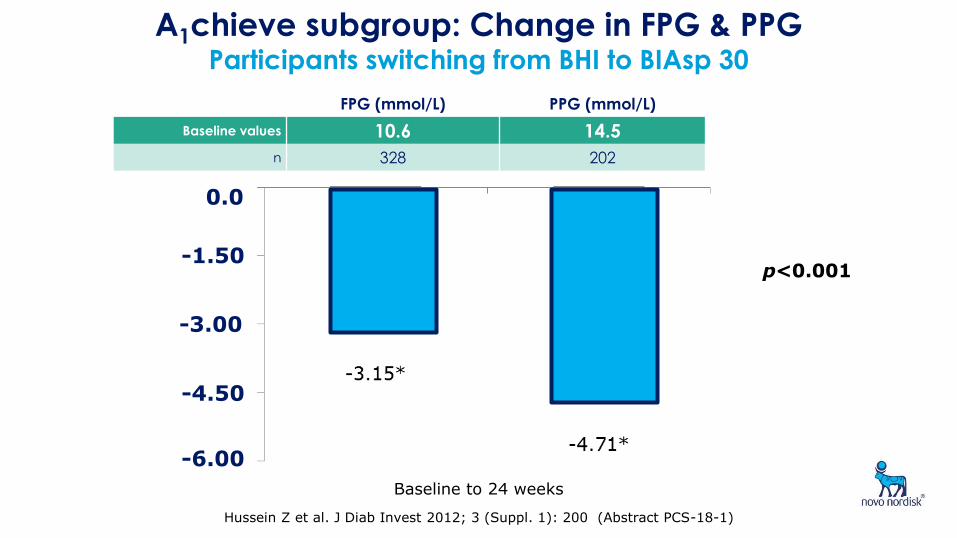
A1chieve subgroup: Change in FPG & PPG Participants switching from BHI to BIAsp 30
FPG (mmol/L) PPG (mmol/L)
Baseline values 10.6 14.5
n 328 202
-1.50
-4.50
-3.00
0.0
-6.00
Baseline to 24 weeks
p<0.001
Hussein Z et al. J Diab Invest 2012; 3 (Suppl. 1): 200 (Abstract PCS-18-1)
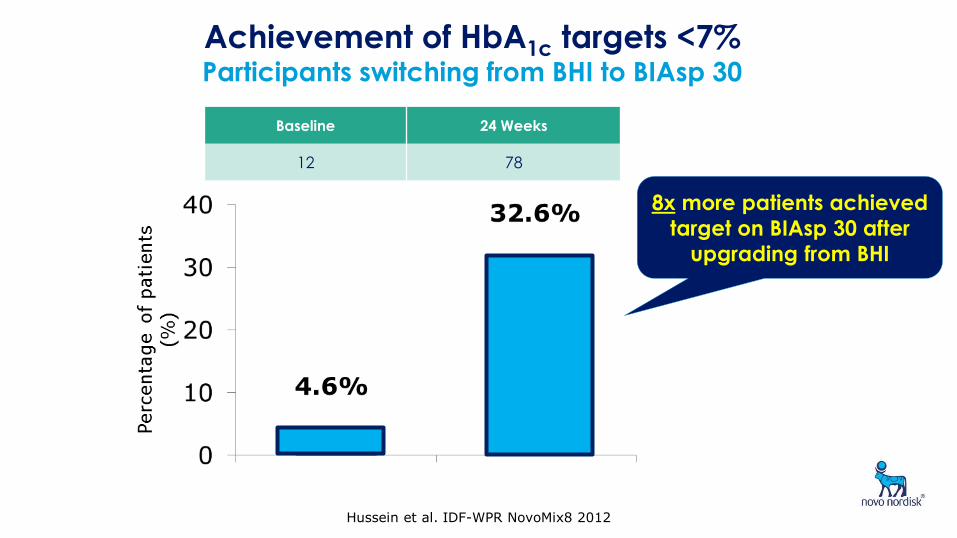
Achievement of HbA1c targets <7% Participants switching from BHI to BIAsp 30
Baseline 24 Weeks
12 78
8x more patients achieved
target on BIAsp 30 after
upgrading from BHI
Hussein et al. IDF-WPR NovoMix8 2012
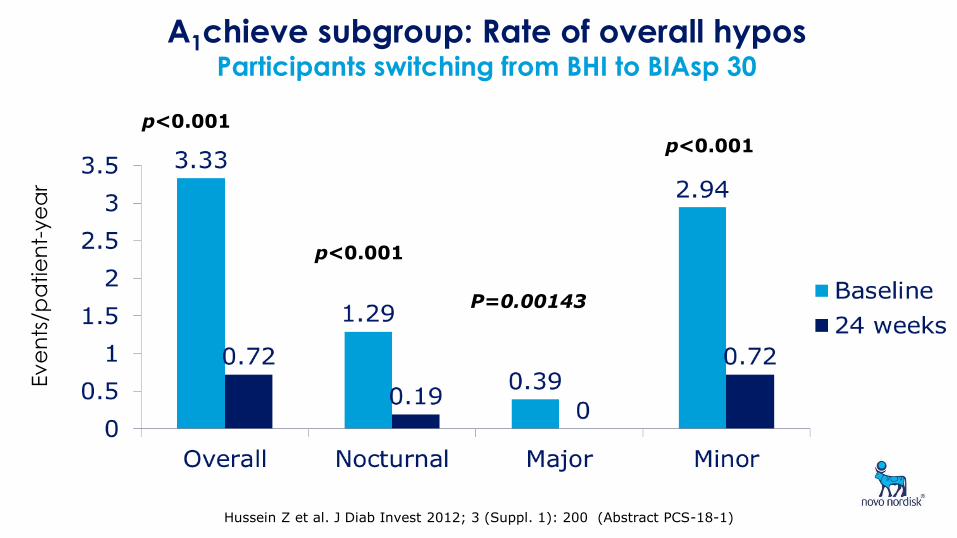
A1chieve subgroup: Rate of overall hypos Participants switching from BHI to BIAsp 30
Ev
en
ts/p
atie
nt-
ye
ar
Hussein Z et al. J Diab Invest 2012; 3 (Suppl. 1): 200 (Abstract PCS-18-1)
P=0.00143
p<0.001
p<0.001
p<0.001
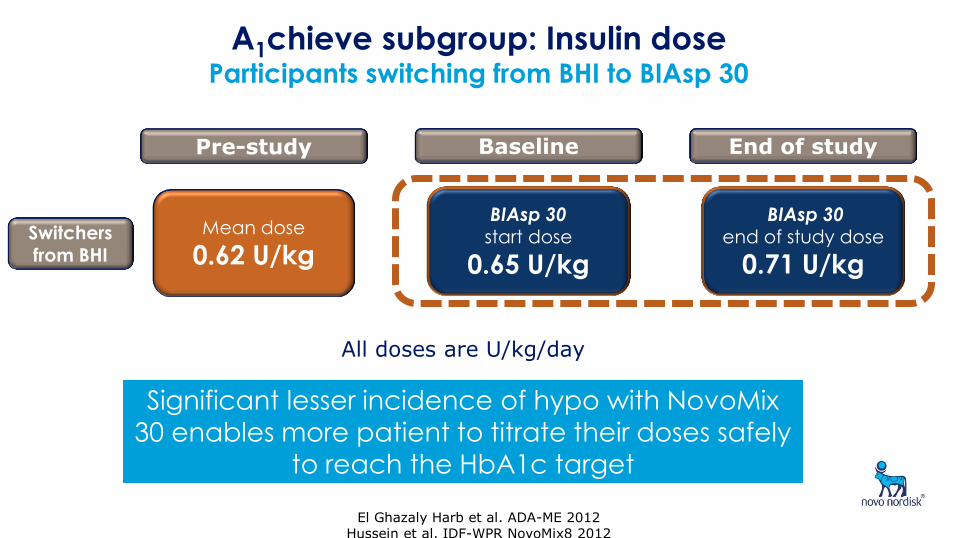
A1chieve subgroup: Insulin dose Participants switching from BHI to BIAsp 30
BIAsp 30 start dose
0.65 U/kg
BIAsp 30 end of study dose
0.71 U/kg
Baseline End of study
El Ghazaly Harb et al. ADA-ME 2012 Hussein et al. IDF-WPR NovoMix8 2012
Pre-study
Mean dose
0.62 U/kg Switchers
from BHI
All doses are U/kg/day
Significant lesser incidence of hypo with NovoMix
30 enables more patient to titrate their doses safely
to reach the HbA1c target
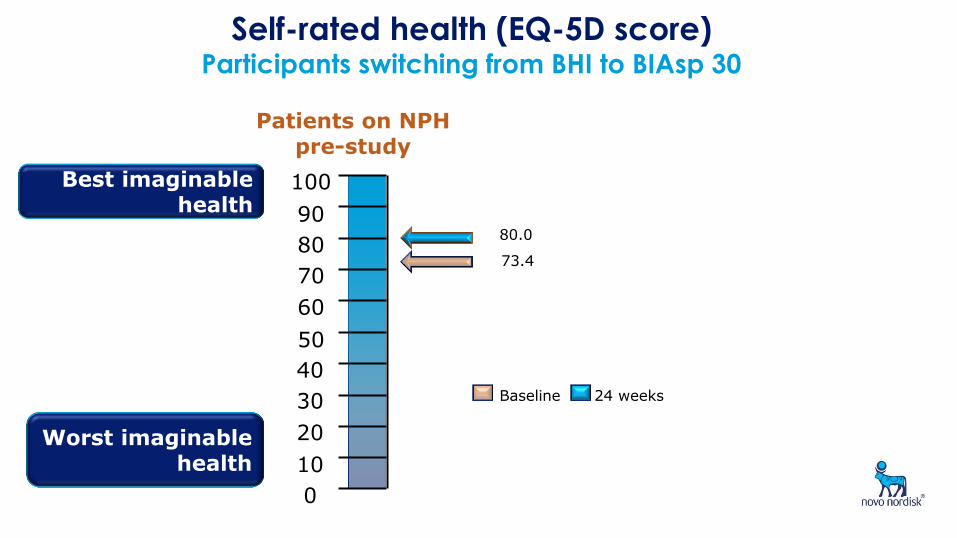
Self-rated health (EQ-5D score) Participants switching from BHI to BIAsp 30
0
10
20
30
40
50
60
70
80
90
100
Patients on NPH pre-study
Baseline 24 weeks
Best imaginable health
Worst imaginable health
73.4
80.0
APROM ID#1932;approval date:July 2010 37
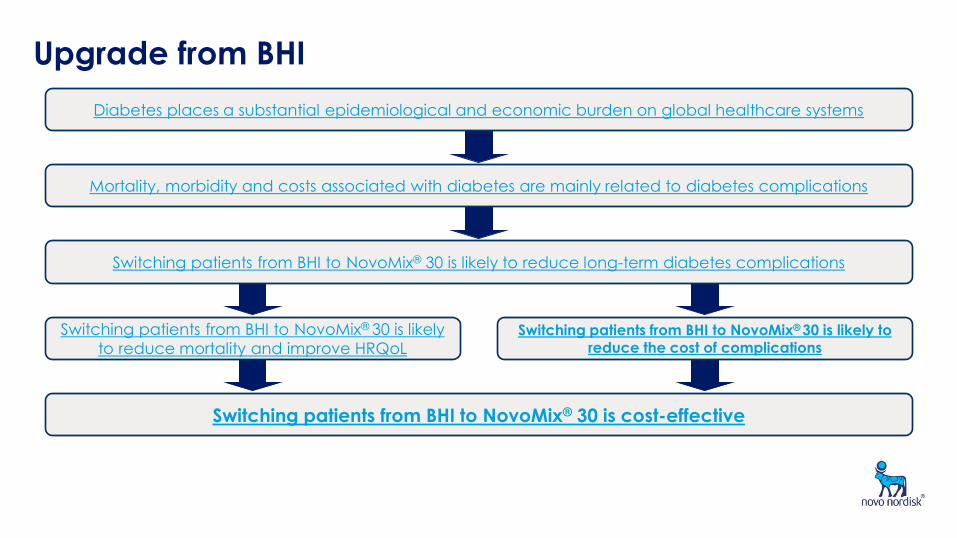
Upgrade from BHI
Switching patients from BHI to NovoMix® 30 is likely to reduce long-term diabetes complications
Switching patients from BHI to NovoMix® 30 is cost-effective
Switching patients from BHI to NovoMix® 30 is likely
to reduce mortality and improve HRQoL
Diabetes places a substantial epidemiological and economic burden on global healthcare systems
Mortality, morbidity and costs associated with diabetes are mainly related to diabetes complications
Switching patients from BHI to NovoMix® 30 is likely
to reduce the cost of complications
38
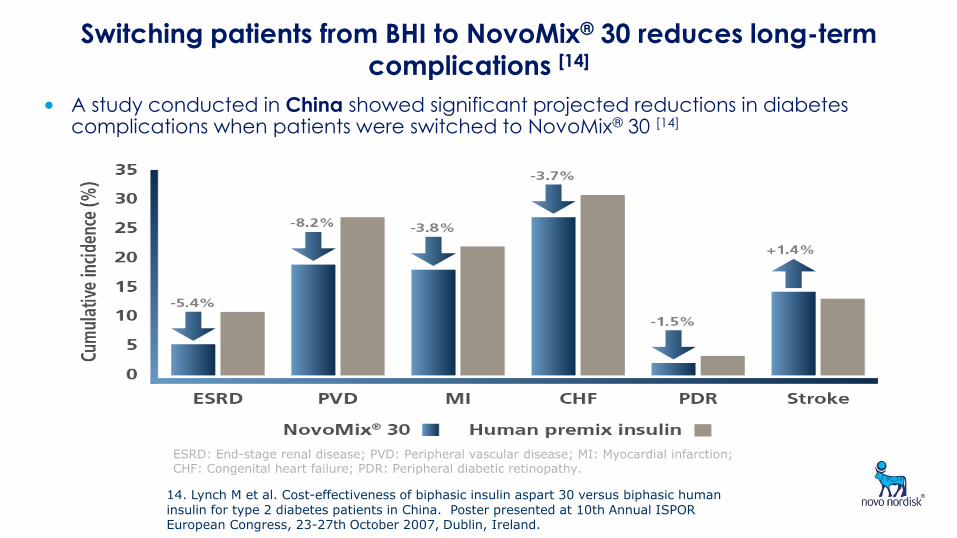
Switching patients from BHI to NovoMix® 30 reduces long-term complications [14]
• A study conducted in China showed significant projected reductions in diabetes complications when patients were switched to NovoMix® 30 [14]
ESRD: End-stage renal disease; PVD: Peripheral vascular disease; MI: Myocardial infarction; CHF: Congenital heart failure; PDR: Peripheral diabetic retinopathy.
14. Lynch M et al. Cost-effectiveness of biphasic insulin aspart 30 versus biphasic human insulin for type 2 diabetes patients in China. Poster presented at 10th Annual ISPOR European Congress, 23-27th October 2007, Dublin, Ireland.
39
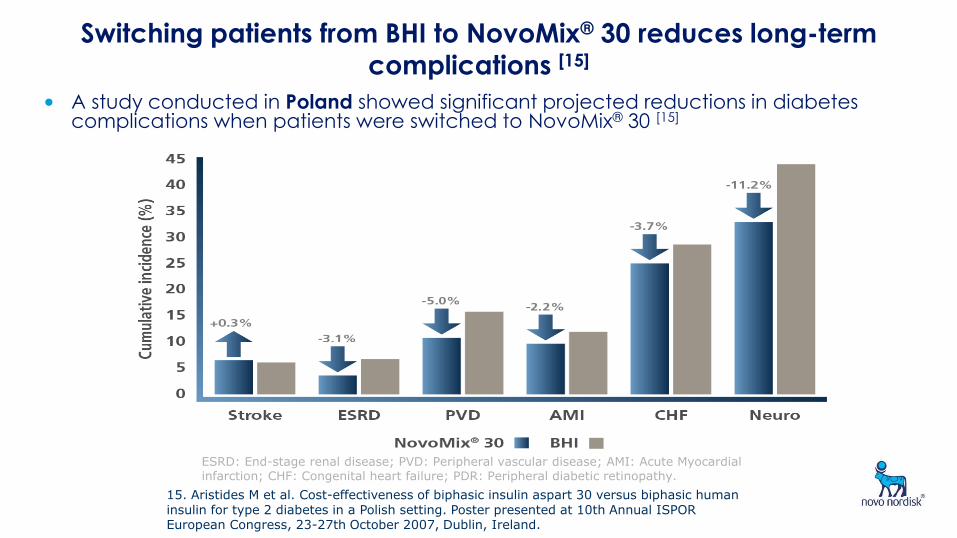
Switching patients from BHI to NovoMix® 30 reduces long-term complications [15]
• A study conducted in Poland showed significant projected reductions in diabetes complications when patients were switched to NovoMix® 30 [15]
ESRD: End-stage renal disease; PVD: Peripheral vascular disease; AMI: Acute Myocardial infarction; CHF: Congenital heart failure; PDR: Peripheral diabetic retinopathy.
15. Aristides M et al. Cost-effectiveness of biphasic insulin aspart 30 versus biphasic human insulin for type 2 diabetes in a Polish setting. Poster presented at 10th Annual ISPOR European Congress, 23-27th October 2007, Dublin, Ireland.
40
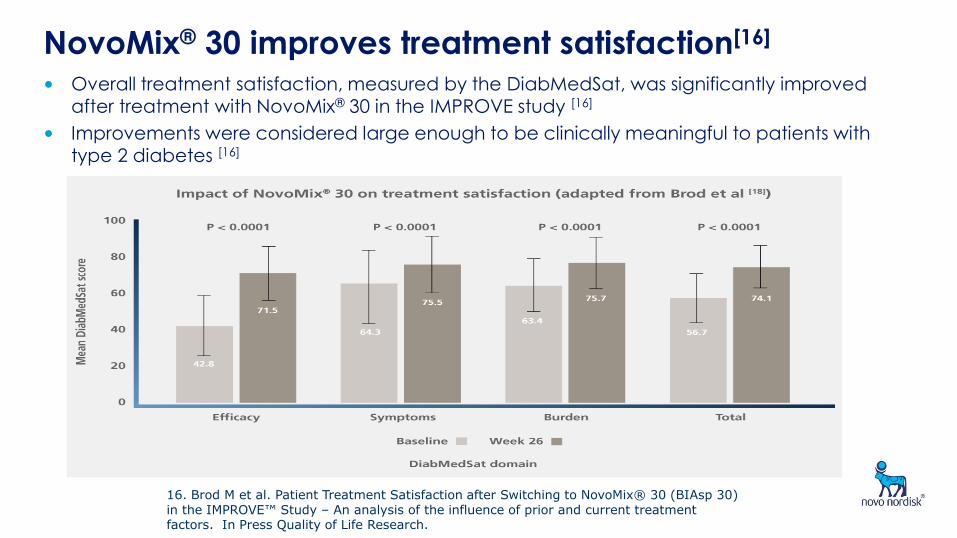
NovoMix® 30 improves treatment satisfaction[16]
• Overall treatment satisfaction, measured by the DiabMedSat, was significantly improved after treatment with NovoMix® 30 in the IMPROVE study [16]
• Improvements were considered large enough to be clinically meaningful to patients with type 2 diabetes [16]
16. Brod M et al. Patient Treatment Satisfaction after Switching to NovoMix® 30 (BIAsp 30) in the IMPROVE™ Study – An analysis of the influence of prior and current treatment factors. In Press Quality of Life Research.

41
Some studies have shown that switching patients from BHI to
NovoMix® 30 reduces mortality and improves HRQoL [21]
• Switching patients to NovoMix® 30 is expected to increase life expectancy and quality-adjusted life expectancy [21]
21. Valentine WJ et al. Systematic review of the cost-effectiveness of biphasic insulin aspart 30 in type 2 diabetes. Curr Med Res Opin 2010.
42
Upgrade from BHI
Switching patients from BHI to NovoMix® 30 is likely to reduce long-term diabetes complications
Switching patients from BHI to NovoMix® 30 is cost-effective
Switching patients from BHI to NovoMix® 30 is likely
to reduce mortality and improve HRQoL
Diabetes places a substantial epidemiological and economic burden on global healthcare systems
Mortality, morbidity and costs associated with diabetes are mainly related to diabetes complications
Switching patients from BHI to NovoMix® 30 is likely to
reduce the cost of complications
43
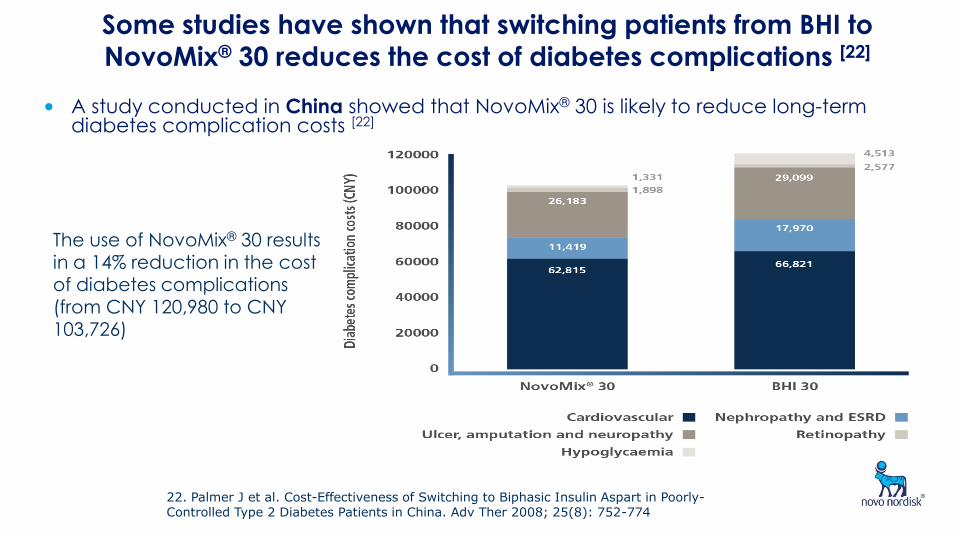
Some studies have shown that switching patients from BHI to
NovoMix® 30 reduces the cost of diabetes complications [22]
• A study conducted in China showed that NovoMix® 30 is likely to reduce long-term diabetes complication costs [22]
The use of NovoMix® 30 results in a 14% reduction in the cost of diabetes complications
(from CNY 120,980 to CNY 103,726)
22. Palmer J et al. Cost-Effectiveness of Switching to Biphasic Insulin Aspart in Poorly- Controlled Type 2 Diabetes Patients in China. Adv Ther 2008; 25(8): 752-774
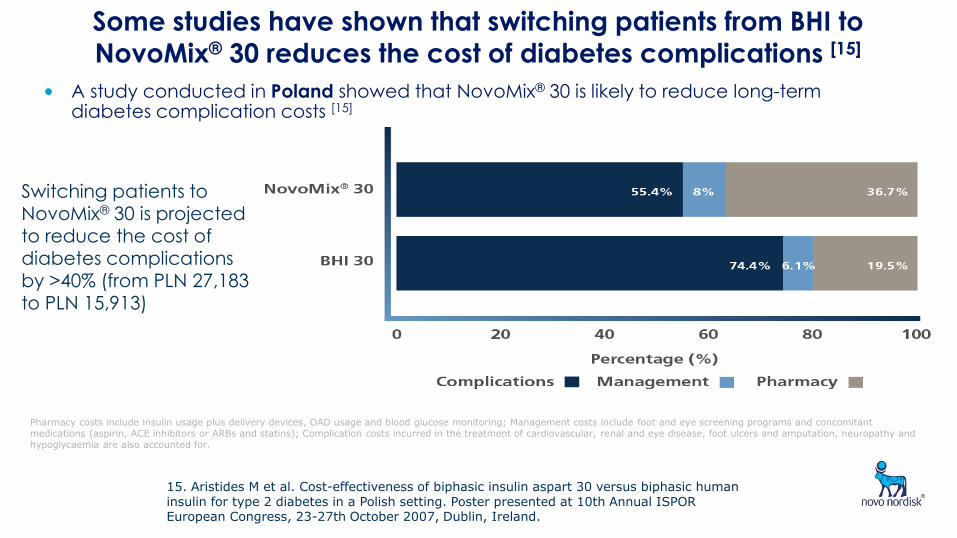
44 Some studies have shown that switching patients from BHI to
NovoMix® 30 reduces the cost of diabetes complications [15]
• A study conducted in Poland showed that NovoMix® 30 is likely to reduce long-term diabetes complication costs [15]
Switching patients to NovoMix® 30 is projected to reduce the cost of diabetes complications by >40% (from PLN 27,183
to PLN 15,913)
Pharmacy costs include insulin usage plus delivery devices, OAD usage and blood glucose monitoring; Management costs include foot and eye screening programs and concomitant medications (aspirin, ACE inhibitors or ARBs and statins); Complication costs incurred in the treatment of cardiovascular, renal and eye disease, foot ulcers and amputation, neuropathy and hypoglycaemia are also accounted for.
15. Aristides M et al. Cost-effectiveness of biphasic insulin aspart 30 versus biphasic human insulin for type 2 diabetes in a Polish setting. Poster presented at 10th Annual ISPOR European Congress, 23-27th October 2007, Dublin, Ireland.
45
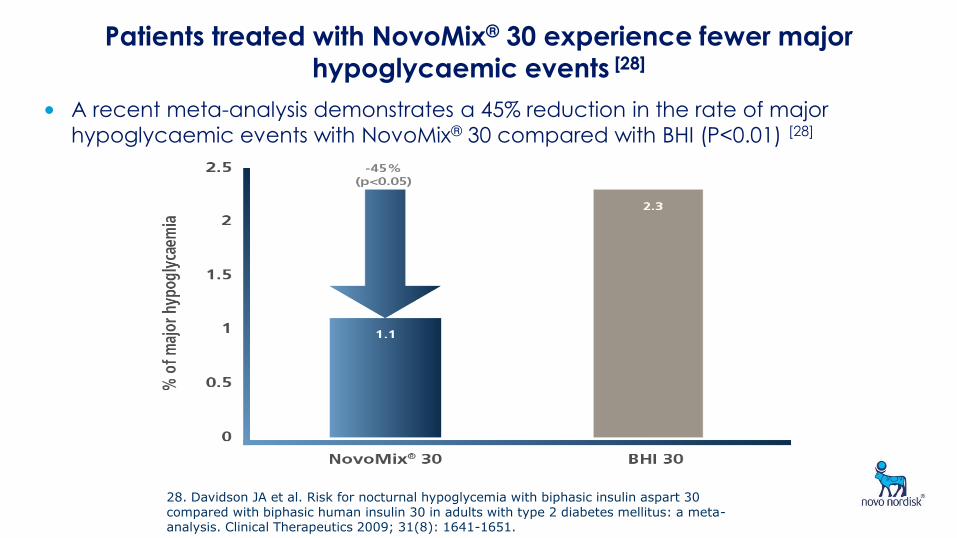
Patients treated with NovoMix® 30 experience fewer major
hypoglycaemic events [28]
• A recent meta-analysis demonstrates a 45% reduction in the rate of major
hypoglycaemic events with NovoMix® 30 compared with BHI (P<0.01) [28]
28. Davidson JA et al. Risk for nocturnal hypoglycemia with biphasic insulin aspart 30 compared with biphasic human insulin 30 in adults with type 2 diabetes mellitus: a meta-analysis. Clinical Therapeutics 2009; 31(8): 1641-1651.
46
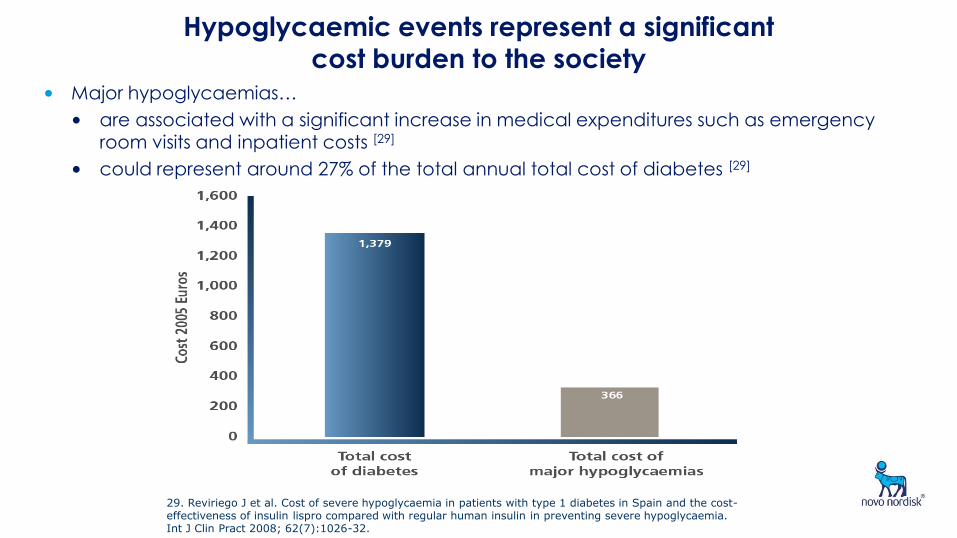
Hypoglycaemic events represent a significant cost burden to the society
• Major hypoglycaemias…
• are associated with a significant increase in medical expenditures such as emergency room visits and inpatient costs [29]
• could represent around 27% of the total annual total cost of diabetes [29]
29. Reviriego J et al. Cost of severe hypoglycaemia in patients with type 1 diabetes in Spain and the cost-effectiveness of insulin lispro compared with regular human insulin in preventing severe hypoglycaemia. Int J Clin Pract 2008; 62(7):1026-32.
47
Switching patients from BHI to NovoMix® 30
is cost-effective in many countries
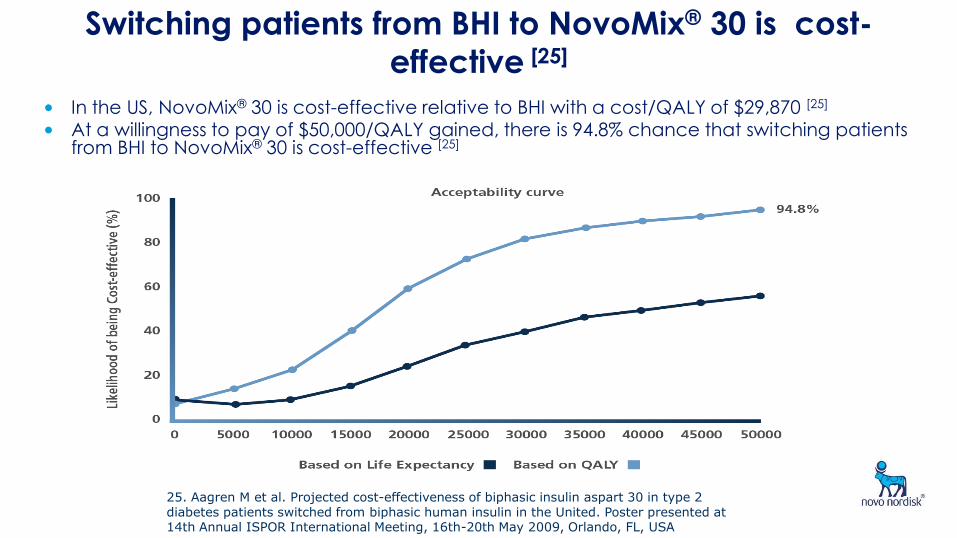
48 Switching patients from BHI to NovoMix® 30 is cost-
effective [25]
• In the US, NovoMix® 30 is cost-effective relative to BHI with a cost/QALY of $29,870 [25]
• At a willingness to pay of $50,000/QALY gained, there is 94.8% chance that switching patients from BHI to NovoMix® 30 is cost-effective [25]
25. Aagren M et al. Projected cost-effectiveness of biphasic insulin aspart 30 in type 2 diabetes patients switched from biphasic human insulin in the United. Poster presented at 14th Annual ISPOR International Meeting, 16th-20th May 2009, Orlando, FL, USA
49
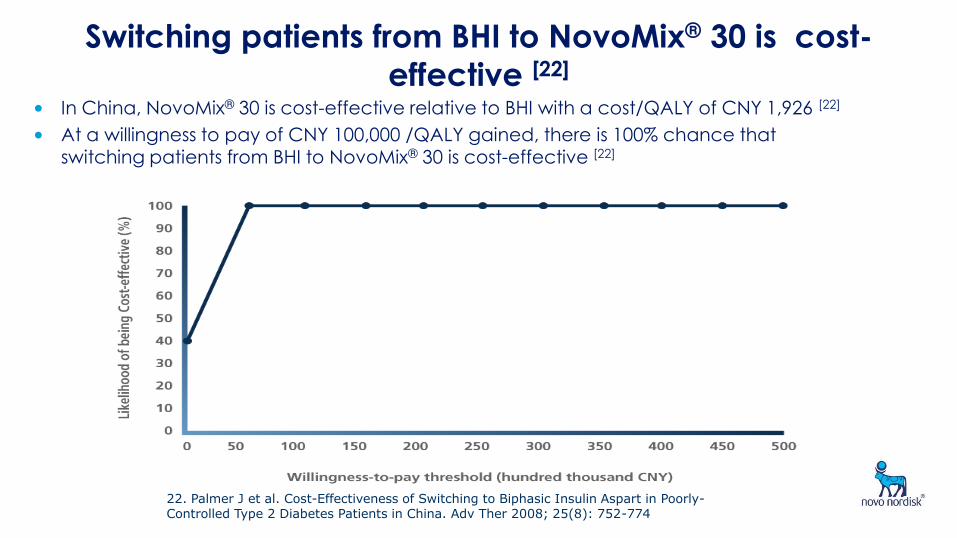
Switching patients from BHI to NovoMix® 30 is cost-
effective [22] • In China, NovoMix® 30 is cost-effective relative to BHI with a cost/QALY of CNY 1,926 [22]
• At a willingness to pay of CNY 100,000 /QALY gained, there is 100% chance that switching patients from BHI to NovoMix® 30 is cost-effective [22]
22. Palmer J et al. Cost-Effectiveness of Switching to Biphasic Insulin Aspart in Poorly-Controlled Type 2 Diabetes Patients in China. Adv Ther 2008; 25(8): 752-774
Conclusions
• As the prevalence of type 2 DM increases world wide the cost to manage the metabolic abnormalities and diabetic complications are also increased
• The total cost in managing these diabetic patients is not only in the treatment itself but as a whole including the management of complications
• In people in poor blood glucose control, starting a premix insulin analogue :
•Blood glucose control measured as HbA1c, FPG or PPPG improved markedly – clinically & statistically significantly
•This was not accompanied by an increase in reported hypoglycaemia, or in body weight
•Useful improvements in blood glucose control were seen both in insulin naïve people, and those already using insulin
Presentation title Slide no
50 Date












![NovoMix 30 PM-Eng Marketed [Feb 25-05] - Novo Nordisk Canada Home](https://static.fdocuments.us/doc/165x107/613d5153736caf36b75be63c/novomix-30-pm-eng-marketed-feb-25-05-novo-nordisk-canada-home.jpg)





