



Lumbar Assessment: Traditional vs. Contemporary Methods Scott D. Coon, DC, PCP-C, PSCP Adjunct...
38
Lumbar Assessment: Traditional vs. Contemporary Methods Scott D. Coon, DC, PCP- C, PSCP Adjunct Assistant Professor New York Chiropractic College
-
Upload
marlene-randall -
Category
Documents
-
view
214 -
download
0
Transcript of Lumbar Assessment: Traditional vs. Contemporary Methods Scott D. Coon, DC, PCP-C, PSCP Adjunct...
Lumbar Assessment:Traditional vs. Contemporary Methods
Scott D. Coon, DC, PCP-C, PSCPAdjunct Assistant Professor
New York Chiropractic College


Overview
Patient is diagnosed with lumbar segmental dysfunction (739.3) complicated by lumbar osteoarthritis (721.3) with symptoms associated with lumbar stenosis (721.42).

• Patient is diagnosed with lumbar segmental dysfunction (M99.13) complicated by lumbar osteoarthritis (M47.816) with symptoms associated with lumbar stenosis (M48.06).
• Under ICD-9 system about 14,000 codes are available, under the new ICD-10 system over 60,000 codes are available.
WHO Develops the ICD-10-CM
• Dr. K.S.J. Murkowski represented all chiropractors (ICA/ACA) to the World Health Organization on ICD-10.
• There were in excess of 500 codes suggested for vertebral subluxation complex (VSC and its eight physical and eight chemical components.
• This was a 5 year process with 2 of those years just having the ACA/ICA agree on the definition of VSC.

Recommended Texts

Recommended Texts

Recommended Texts

Shift in our Understanding of LBP
Pathoanatomical Model(Suffering can only be explained by tissue
injury/pathology)
Pathophysiological Model(Suffering results from complex processes of
dysfunction)
Shift in our Approach to LBP
Biomedical Model(The tissues involved are responsible for the pain)
Biopsychosocial Model(Other systems prevent the inhibitions of pain and
contribute to the magnification of pain)

NYCC’s Post-Graduate Seminar Series, “PRIMARY SPINE CARE PRACTITIONERS PROGRAM”
Module 1 - 12 Hours
Module 2 - 12 Hours
Module 3 - 12 Hours

Recommended TextsThe “CRISP” protocols as developed by Donald Murphy, DC, provides a blueprint for a new type of health care professional. The primary spine practitioner (PSP). There are 3 diagnostic questions to ask:
#1) Is the patient’s complaint life threatening or of visceral origin?
#2) Where is the pain coming from?
#3) What has happened to this person to cause the pain experience to develop and persist?
#1. Is the patient’s complaint life threatening or of visceral origin?
• Cancer• Benign Tumor• Infection• Fracture• Dissected or Ruptured AAA• GI Disease• GU Disease• Cauda Equina Syndrome

#2. Where is the pain coming from?
• Disc Derangement (Most Common)• Joint Dysfunction– Facet Joints– Sacroiliac Joints
• Radiculopathy• Myofascial Pain– Trigger Points– Sprain / Strain

Assessing Disc Derangement
• Antalgic?• Pain worse in the morning?• Pain increases during flexion?• Pain increases with sitting?• Pain increases with standing and stays with you for
several minutes but gradually gets better?
• Confirm disc derangement with End Range Loading (ERL) Exam.
Due to imbibition of fluid and increases in intradiscal pressure.

Disc Derangement – ERL Exam
• Loading in the “Direction of Detriment” causes further displacement of the intradiscal material during the arc of motion and at the end of range, thus causing peripheralization of symptoms.
• Loading in the “Direction of Benefit” is movement in the direction obstructed by the displacement of nuclear material.

Assessing Joint Dysfunction
• Lumbar Facet Joints– Extension-Rotation Test
• Sacroiliac Joints– Five SI Provocation Tests
Lumbar Extension-Rotation Test
• Patient starts in a neutral standing position with hands on their PSIS.
• Patient extends backward at the waist and asked if pain is present.
• The patient then extends backward with right or left torso rotation.
• If pain is provoked with the addition of the rotation then the test is positive.
Five SI Provocation Tests“Cluster of Laslett Tests”
• Distraction Test• Thigh Thrust Test• Gaenslen’s Test• Compression Test• Sacral Thrust Test
3 out of 5 tests must be positive in order to consider the SI joint as being the primary pain generator.
Clinical Pearl: Disc vs. SI
• Disc Derangement– When going from sitting to standing the patient
will be very slow to complete the process of standing up straight due to the obstruction of disc material.
• Sacroiliac Joint– Painful going from sitting to standing position but
the difficulty getting to a full upright position will not be present.

Assessing Radiculopathy
• Younger patient more often have disc herniation as the cause of radiculopathy while older patients with radiculopathy is caused by stenosis.
• The extremity pain is of neural origin and involves the nerve roots although piriformis syndrome can present very similar.
• Radiculopathy is assessed with “nerve root tension tests”.

Nerve Root Tension Tests
• Straight Leg Raise• Slump Test• Femoral Nerve Stretch Test
• With all these tests, an increase in pain with tension of the neural structures and a decrease in pain with lessening of the tension indicates a neural structure cause of the pain.

Assessing Myofascial Pain
• Lumbar Erector Spinae• Lumbosacral Multifidis• Quadratus Lumborum• Glutues Medius• Piriformis

#3. What has happened to this person to cause the pain experience to develop and persist?
• Somatic Factors
• Psychological Factors
Somatic Factors
• Dynamic Instability• Passive Instability• Nociceptive System Sensitization

Psychological Factors
• Fear• Catastrophizing• Passive Coping• Poor Self- Efficacy• Depression• Perceived Injustice• Hypervigilance for Symptoms• Cognitive Fusion• Anxiety
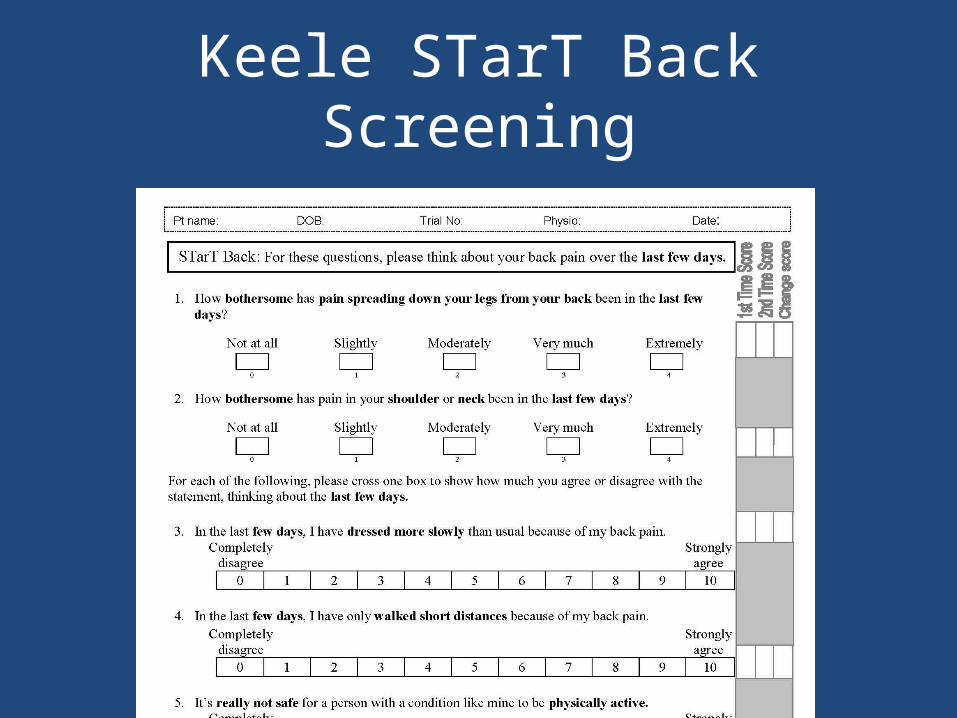
Keele STarT Back Screening

Keele STarT Recommendations• 1. Build rapport, validate and normalize the patient’s experiences.• 2. Conduct a comprehensive biopsychosocial assessment (physical examination, exploration
of the impact that pain is having on the patient’s physical and psychosocial functioning, identification of the patient’s beliefs and expectations regarding LBP and its management and structured identification of potential obstacles to recovery).
• 3. Address gaps in patients knowledge, correct possible misunderstandings and provide a credible explanation for their pain (e.g. cause, mechanisms, prognosis, role of investigations and treatments),
• 4. Create opportunities for patient’s to respond differently to difficult internal experiences (thoughts, feelings and bodily sensations) and to maintain or alter activity in keeping with their goals.
• 5. Provide guidance on a variety of pain rehabilitation techniques including pacing and graded activity.
• 6. Provide support in returning to usual activities, sleep and work.• 7. Specifically focus on the psychological prognostic indicators (catastrophizing, low mood,
anxiety and pain related fear) with the adoption of simple cognitive behavioral techniques.• 8. Encourage patients to put skills into practice between sessions, review and reinforce
progress and problem solve difficulties.• 9. Emphasize the role of active self-management of ongoing or future episodes.

Keele STarT Groups
CBT – Cognitive Behavioral Therapy

Patient-Specific Functional Scale

Shift in our Understanding of LBP
Pathoanatomical Model(Suffering can only be explained by tissue
injury/pathology)
Pathophysiological Model(Suffering results from complex processes of
dysfunction)

Shift in our Approach to LBP
Biomedical Model(The tissues involved are responsible for the pain)
Biopsychosocial Model(Other systems prevent the inhibitions of pain and
contribute to the magnification of pain)


Dr. Coon Contact Information
NYCC Adjunct Faculty Office2360 State Rte. 89Seneca Falls, NY 13148
[email protected](585) 425-9820


















