LuisitoO. Llido’Professorial’Lecture’’. Llido’Professorial’Lecture’’ ’...
101
Luisito O. Llido Professorial Lecture Nutri&on and Recovery a1er Surgery Olle Ljungqvist MD PhD Professor Surgery Örebro University Hospital & Karolinska InsEtutet Sweden PHILSPEN Manilla, The Phillipines October 7, 2014
Transcript of LuisitoO. Llido’Professorial’Lecture’’. Llido’Professorial’Lecture’’ ’...
Luisito O. Llido Professorial Lecture
Nutri&on and Recovery a1er Surgery
Olle Ljungqvist MD PhD Professor Surgery
Örebro University Hospital & Karolinska InsEtutet Sweden
PHILSPEN Manilla, The Phillipines
October 7, 2014
Recovery AIer Surgery What are we trying to achieve?
Pa&ent back to preopera&ve func&on • Normal gastrointes&nal func&on
– Normal food intake – Bowel movement
• Pain control • Mobility
• No complica&on
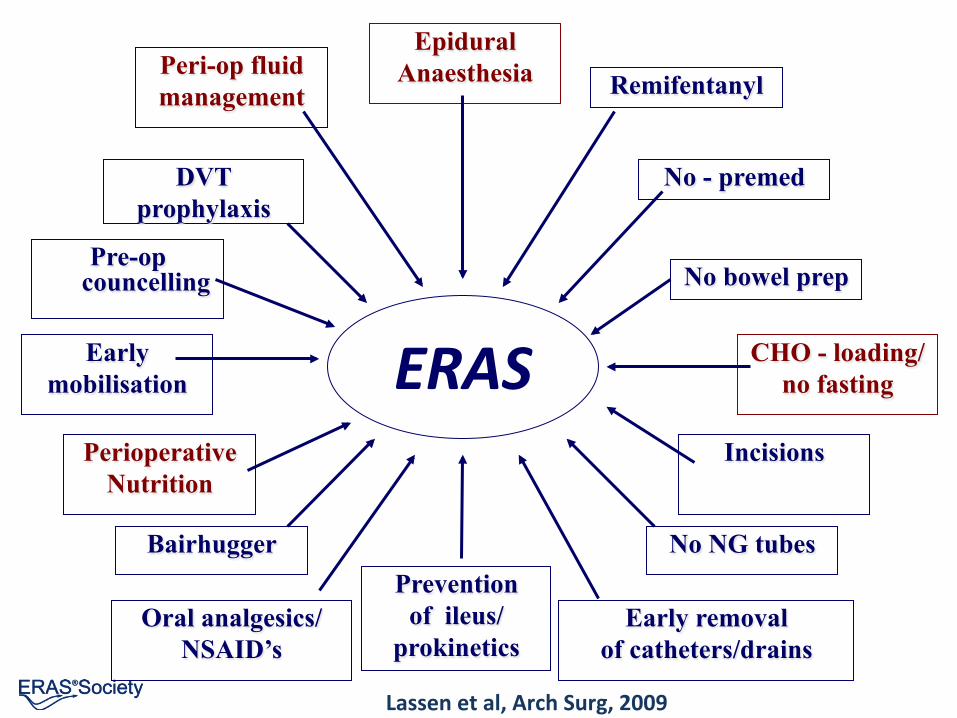
What is ERAS?
• ERAS = Enhanced Recovery AIer Surgery • Consensus on perioperaEve care* • InternaEonal network – ERAS Society • Team work – mulE professional & disciplinary • ImplementaEon:
– Audit – Control over care
*Fearon et al, Clin Nutr 2005, Lassen et al, Arch Surg, 2009, Guidelines 2012,2013,2014 www.erassociety.org

History

Ann Surg. 2002 Nov;236(5):643-8. From Cuthbertson to ERAS: 70 years of progress in reducing stress in surgical patients. Wilmore DW.
Sir David Cuthbertson, UK Francis Moore, USA

Henrik Kehlet: concepts
• Epidural anaesthesia
• Multimodal approach to recovery

Highlights: 2001: Initiation 2003: Database 2005: 1st protocol 2006: Implementation 2009: 2nd protocol
Tromsö: A Revhaug
Stockholm: O Ljungqvist
Copenhagen: H Kehlet
Maastricht: M v Meyenfeldt, C deJong
Edinburgh: KFC Fearon
Growth: St Marks: R Kennedy Nottingham: D Lobo Charité: C Spies, A Fledheiser
ERAS Study Group!
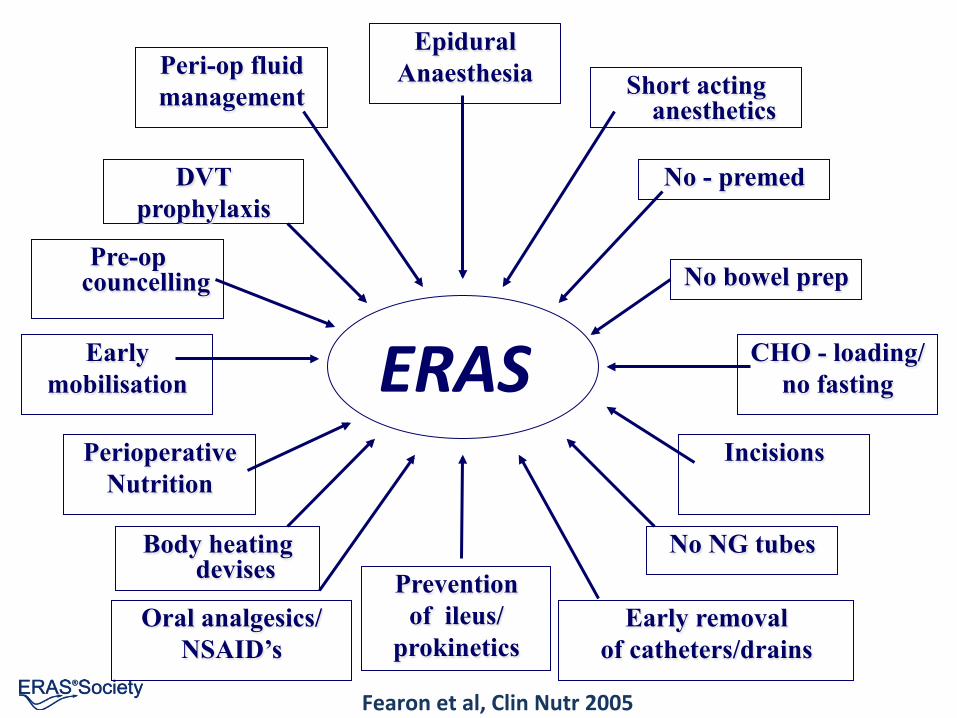
ERAS
Epidural Anaesthesia
Prevention of ileus/
prokinetics
CHO - loading/ no fasting
Early mobilisation
Peri-op fluid management
DVT prophylaxis
Pre-op councelling
Short acting anesthetics
No - premed
No bowel prep
Perioperative Nutrition
Body heating devises
Oral analgesics/ NSAID’s
Incisions
No NG tubes
Early removal of catheters/drains
Fearon et al, Clin Nutr 2005

A Non profit Multi-professional Multi-disciplinary Medical Society Founded in 2010
Mission statement: Enhancing Recovery After Surgery The mission of the Society is to develop perioperative care and to improve recovery through • Research, • Education, • Audit and • Implementation of evidence based practice.
The paradigm shi1:
Mul& modal Mul& professional Mul& disciplinary
EBM in prac&ce: Implementa&on
Interac&ve Team Audit Large network in collabora&on

Philosophy

ERAS Philosophy: The paEent’s journey
CLINIC PRE-‐OP
POST-‐OP WARD HOME
RECOVERY
SURGERY / ANESTHESIA
InteracEve Team audit of outcomes & compliance
PRE ADMISSION
FOL LOW UP 30 D AY
Integrated ERAS protocol
Ljungqvist JPEN 2014

ERAS team approach
• Surgeon • Anesthes&st • HDU specialist • Ward nurses • Anesthesia nurses • Physiotherapist • Die&&an
• Management
Team work: • Training • Implemen&ng • Planning • Audi&ng • Upda&ng • Repor&ng • Research

ERAS Securing modern care
Surgeon: No bowel prep Food a1er surgery No drains Early removal u-‐catheter No iv fluids, no lines Early discharge All evidence based!
Anesthe&st:
Carbohydrates no fas&ng
No premedica&on
Thoracic Epidural Anesthesia (open)
Balanced fluids
Vasopressors
No or short ac&ng opioids

ERAS works!

ERAS Meta analys
ERAS: shorter length of stay by 2.5 days
Varadhan et al, Clin Nutr 2010

ERAS Meta analys
ERAS: Reduce complicaEons by 50%
Varadhan et al, Clin Nutr 2010

How?
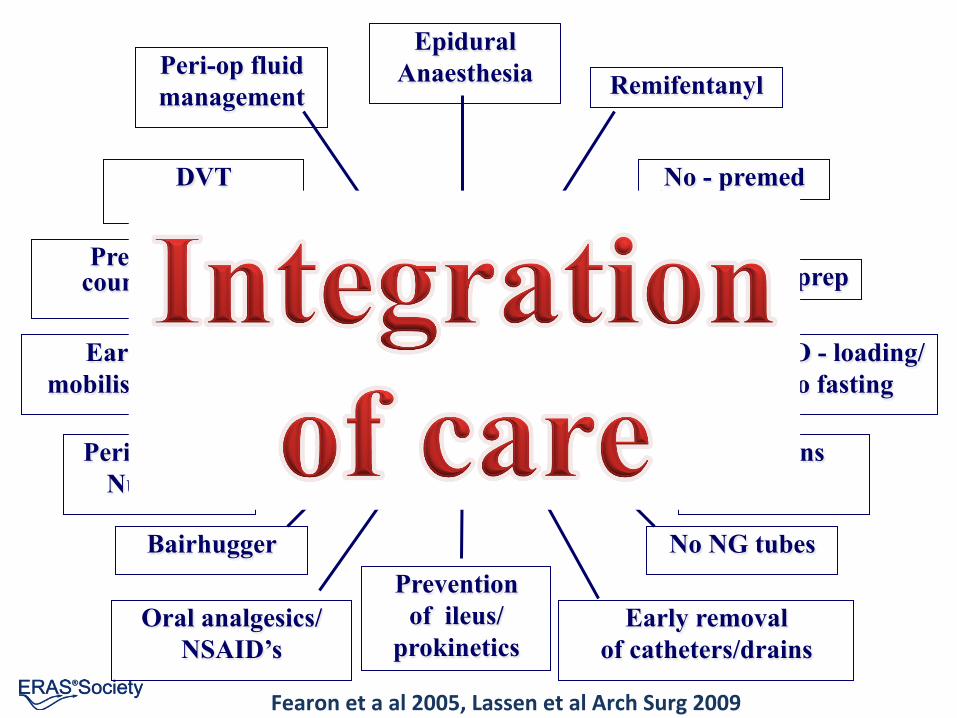
ERAS
Epidural Anaesthesia
Prevention of ileus/
prokinetics
CHO - loading/ no fasting
Early mobilisation
Peri-op fluid management
DVT prophylaxis
Pre-op councelling
Remifentanyl
No - premed
No bowel prep
Perioperative Nutrition
Bairhugger
Oral analgesics/ NSAID’s
Incisions
No NG tubes
Early removal of catheters/drains
Fearon et a al 2005, Lassen et al Arch Surg 2009

3 new guidelines 2012

ERAS in Theory

Goals Back to normal food Energy and protein
2 Key targets: Gut working
Metabolism ready

Goals Back to normal food Energy and protein
2 Key targets: Gut working
Metabolism ready ERAS does both!

Goals Back to normal food Energy and protein
2 Key targets: Gut working
Metabolism ready

The Metabolic Stress Response to Surgery and Trauma
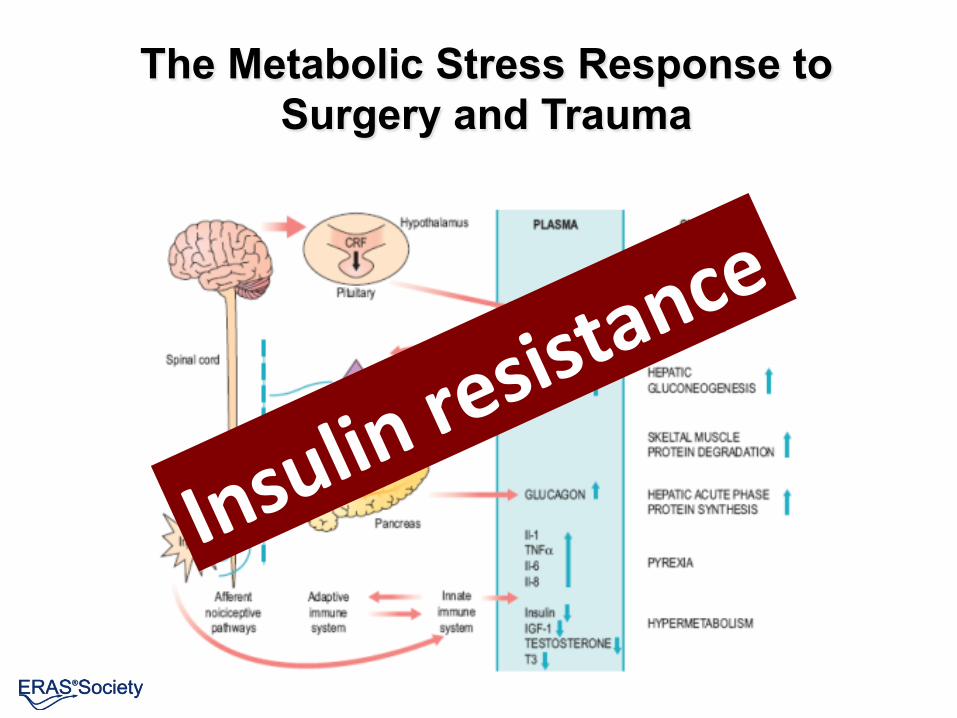
The Metabolic Stress Response to Surgery and Trauma

Insulin & Recovery Insulin: main anabolic hormone involved in • All parts of metabolism
– Glucose control – Fat metabolism – Protein
• Regulator of return of key func&ons • Central to development of complica&ons • Affected by many periopera&ve treatments
Insulin & Recovery Insulin: main anabolic hormone involved in • All parts of metabolism
– Glucose control – Fat metabolism – Protein
• Regulator of return of key func&ons • Central to development of complica&ons • Affected by many periopera&ve treatments
• Insulin resistance: a key for understanding and enhancing recovery
• Insulin func&on key for anabolism

PostoperaEve Insulin resistance
Defin&on: Below normal metabolic effect of insulin • Glucose uptake • Reduc&on in glucose produc&on • Lipolysis • Protein breakdown / balance
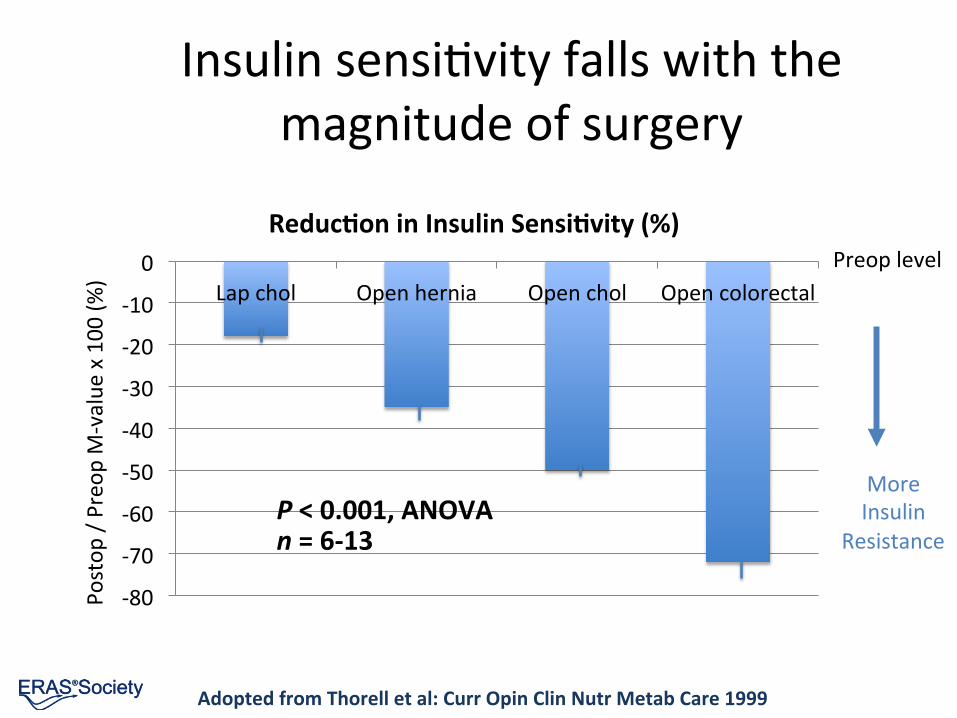
Insulin sensiEvity falls with the magnitude of surgery
Adopted from Thorell et al: Curr Opin Clin Nutr Metab Care 1999
-‐80
-‐70
-‐60
-‐50
-‐40
-‐30
-‐20
-‐10
0 Lap chol Open hernia Open chol Open colorectal
Reduc&on in Insulin Sensi&vity (%)
Postop
/ Preo
p M-‐value
x 100
(%)
P < 0.001, ANOVA n = 6-‐13
More Insulin
Resistance
Preop level

Postop Type 2 DM
Hyperglycemia + +
Insulin sensiEvity -‐ -‐
Glucose produc&on + +
Peripheral glucose uptake -‐ -‐
GLUT4 translocaEon -‐ -‐
Glycogen formaEon -‐ -‐
Adopted from Ljungqvist et al, Clin Nutr 2001
Driving forces for hyperglycemia aIer surgery similar to diabetes
Normalizing insulin acEon normalizes metabolism
Insulin infusion to normalize: • Blood glucose Also controlled: • FFA • Urea excre&on • Substrate u&liza&on a1er major surgery Insulin resistance the key to catabolism
Brandi LS et al: Clin Sci 1990

Independent factors predicEng length of stay
• Type of surgery
• Periopera&ve blood loss
• Postopera&ve insulin resistance
R2 = 0.71, p < 0.01
Thorell et al: Curr Opin Clin Nutr Metab Care 1999

Glucose uptake -‐ stress
Fat
Liver
Kidney
Blood cells
Endothel Neural &ssue
Insulin regulated Concentra&on regulated
[Glucose] Muscle
Too liqle
Too much

Insulin resistance muscle
• Reduced glucose uptake
• Reduced glycogen storage
• Increased protein catabolism

Insulin resistance muscle
• Reduced glucose uptake
• Reduced glycogen storage
• Increased protein catabolism
Lean body mass
Muscle func&on
Mobilisa&on
Energy supply

Impaired Recovery
Postop (days) Tissues/cells Muscle weakness muscle Infec&ons leukocytes Cardiovascular blood vessels Renal failure kidney Polyneuropathy nerve &ssue

Glucose uptake -‐ stress
Fat
Liver
Kidney
Blood cells
Endothel Neural &ssue
Insulin regulated Concentra&on regulated
[Glucose] Muscle
Too liqle
Too much

ComplicaEons
Postop (days) Tissues/cells Infec&ons leukocytes Cardiovascular blood vessels Renal failure kidney Polyneuropathy nerve &ssue Muscle weakness muscle

PostoperaEve insulin resistance increase the risk for complicaEons
The ORs were adjusted for potenEal confounders
Complica&on OR for every decrease by 1 mg/kg/min
(≈ 25% reduc&on in Insulin sensi&vity)
P value
Death 2.33 (0.94-‐5.78) 0.067
Major complicaEon 2.23 (1.30-‐3.85) 0.004
Severe infecEon 4.98 (1.48-‐16.8) 0.010
Minor infecEon 1.97 (1.27-‐3.06) 0.003
Sato et al, JCEM 2010; 95: 4338-‐44
273 paEents open cardiac surgery, insulin sensiEvity determined at the end of op

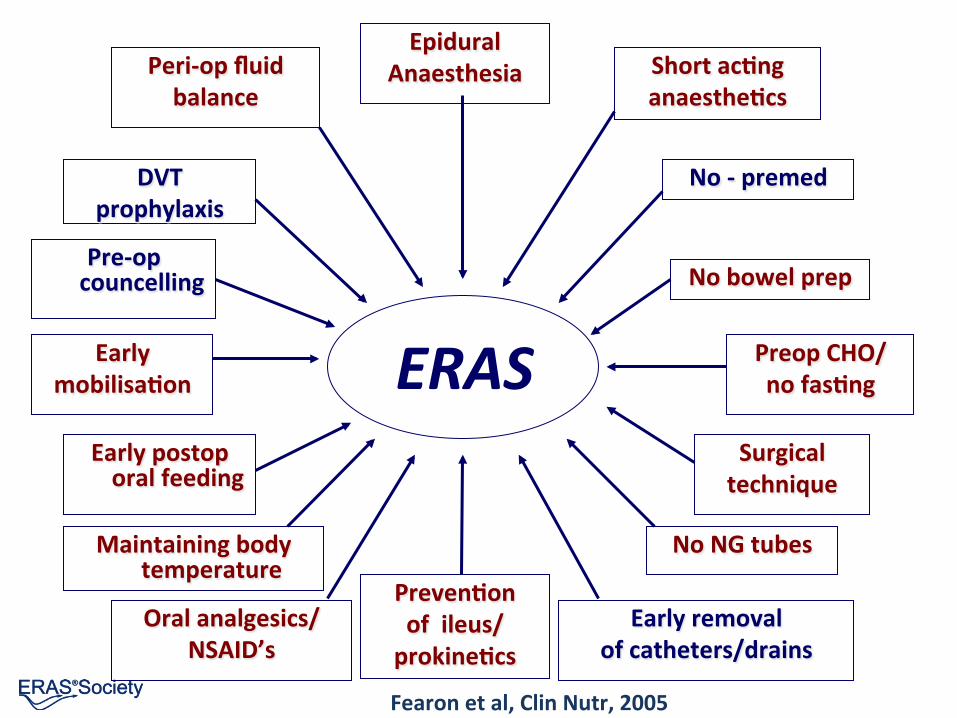
ERAS
Epidural Anaesthesia
Preven&on of ileus/ prokine&cs
Preop CHO/ no fas&ng
Early mobilisa&on
Peri-‐op fluid balance
DVT prophylaxis
Pre-‐op councelling
Short ac&ng anaesthe&cs
No -‐ premed
No bowel prep
Early postop oral feeding
Maintaining body temperature
Oral analgesics/ NSAID’s
Surgical technique
No NG tubes
Early removal of catheters/drains
Fearon et al, Clin Nutr, 2005
ERAS
Epidural Anaesthesia
Preven&on of ileus/ prokine&cs
Preop CHO/ no fas&ng
Early mobilisa&on
Peri-‐op fluid balance
DVT prophylaxis
Pre-‐op councelling
Short ac&ng anaesthe&cs
No -‐ premed
No bowel prep
Early postop oral feeding
Maintaining body temperature
Oral analgesics/ NSAID’s
Surgical technique
No NG tubes
Early removal of catheters/drains
Fearon et al, Clin Nutr, 2005

ERAS elements to reduce insulin resistance
Preopera&ve • Preopera&ve carbohydrates • Epidural anesthesia
Postopera&ve • Pain control • Early postop feeding

Change from fasted to fed using a Carbohydrate load
Aims: Insulin response • 20% glucose iv • 12.5% carbohydrate drink 400 ml 2 h before anesthesia
– many studies combined with 800 ml in the evening before
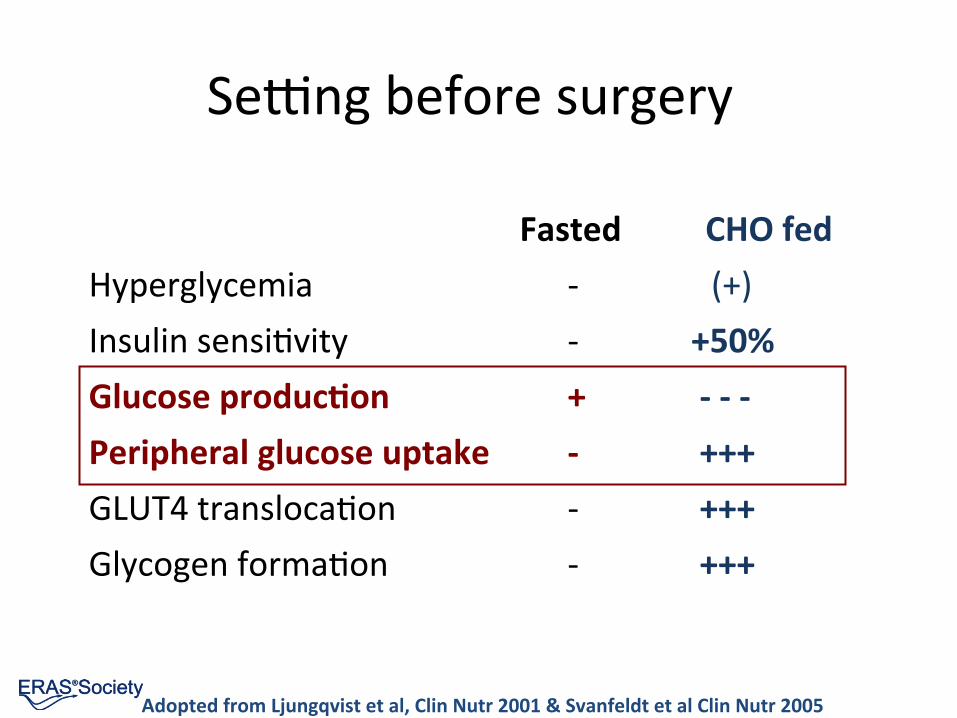
Semng before surgery
Fasted CHO fed Hyperglycemia -‐ (+) Insulin sensiEvity -‐ +50% Glucose produc&on + -‐ -‐ -‐ Peripheral glucose uptake -‐ +++ GLUT4 translocaEon -‐ +++ Glycogen formaEon -‐ +++
Adopted from Ljungqvist et al, Clin Nutr 2001 & Svanfeldt et al Clin Nutr 2005

Gastric emptying is complete in 90 minutes for CHO & water
Nygren et al, Ann Surg, 1995
Minutes a1er intake
Isotop
e ac&v
ity in
the stom
ach (%
)
120 90 60 30 0 0
20
40
60
80
100
120 **
*
*
*
CHO, n=6
Water, n=6

Safety data Preop CHO rich drink
• >5,000 pa&ents in clinical studies in surgical pa&ents
• 150 pa&ents before gastroscopy • >3,000,000 pa&ents in surgical prac&ce
• No adverse events reported

Why give preop carbohydrates?
• Effec&vely reduce insulin resistance
• Improves well being
• Improves postopera&ve muscle func&on
• Reduce lean body mass losses
• May result in faster recovery
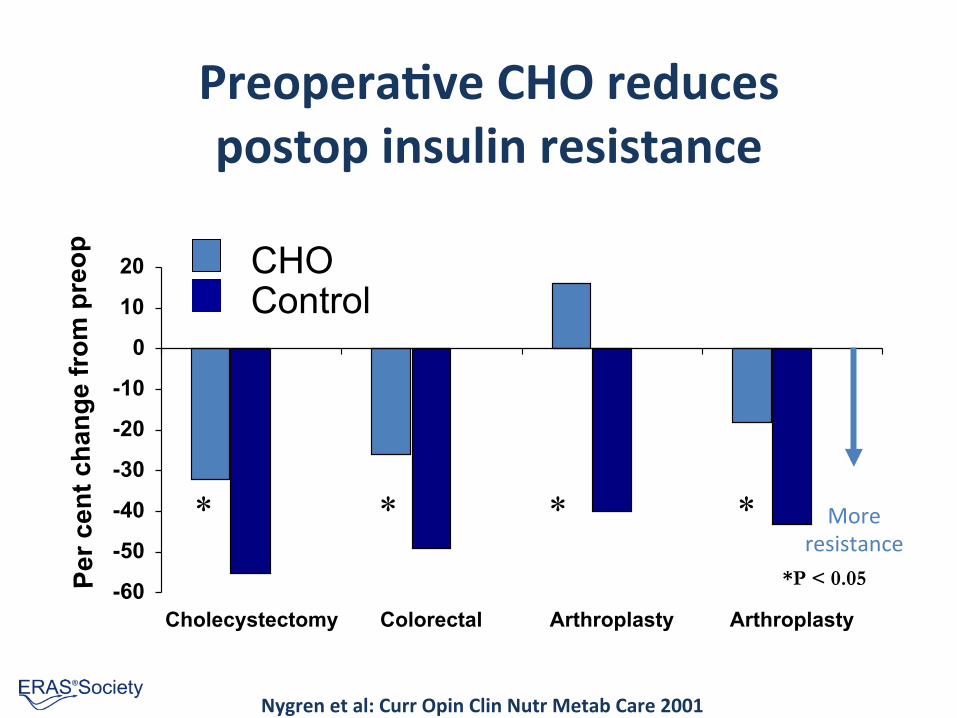
Preopera&ve CHO reduces postop insulin resistance
-60
-50
-40
-30
-20
-10
0
10
20
Cholecystectomy Colorectal Arthroplasty Arthroplasty
Per c
ent c
hang
e fr
om p
reop
* * * *
*P < 0.05
Nygren et al: Curr Opin Clin Nutr Metab Care 2001
CHO Control
More resistance
Confusing data No effect of preop carbs?

Clamp ≠ HOMA
Baban et al, Clin Nutr 2014 in press / on line
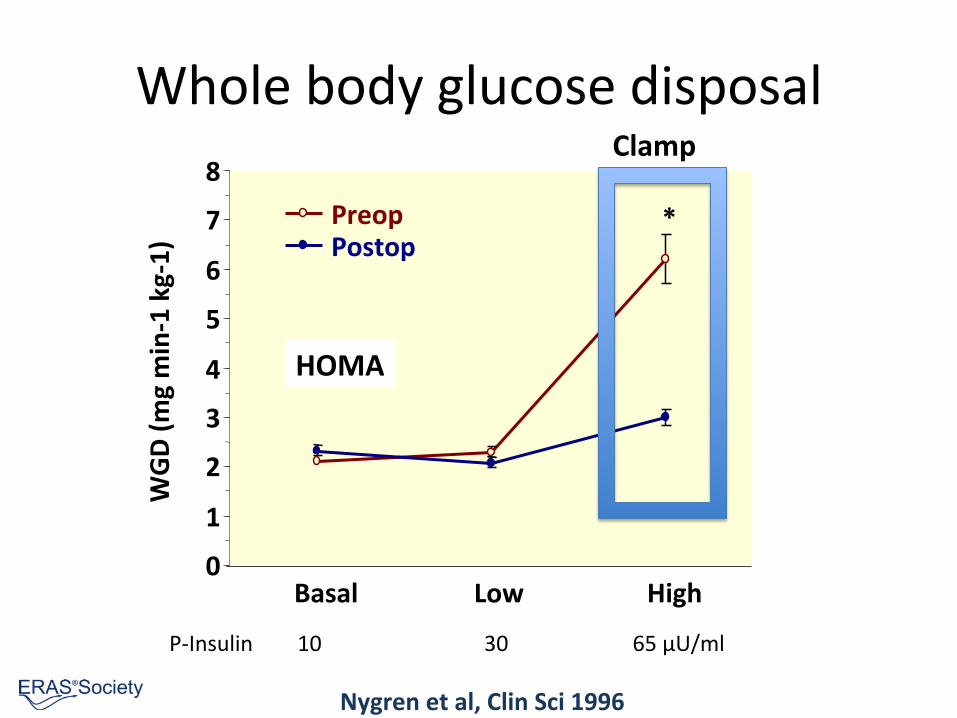
Whole body glucose disposal
0
1
2
3
4
5
6
7
8
Basal Low High
WGD (m
g min-‐1 kg-‐1) Preop
Postop *
Nygren et al, Clin Sci 1996
P-‐Insulin 10 30 65 µU/ml
HOMA
Clamp

Preop Carbohydrates acEvates muscle insulin signalling pathways
0
200
400
600
800
1000
1200
Control Placebo Carbohydrate
PI3Kinase (units) p=0.02
Wang et al, BJS 2010

Preop Carbohydrates maintains postop muscle anabolic pathways
P<0.001
Wang et al, BJS 2010
0
0.01
0.02
0.03
0.04
0.05
0.06
Carbohydrates Placebo Control
Protein Tyrosine Kinase Ac&vity

PreoperaEve carbohydrates retains lean body mass (MAC)
Yuill et al, Clin Nutr 2005
P <0.05
[cm]

0
1
2
3
4
5
6
Urea losses (m
mol/kg/d)
PreoperaEve carbohydrates reduces protein losses and improves muscle
strength
P<0.05
-‐16 -‐14 -‐12 -‐10 -‐8 -‐6 -‐4 -‐2 0
Postop
era&
ve m
uscle strength (%
)
Control CHO
P<0.05 Mean (SEM)
Crowe, BJS 1984; Henriksen Acta Anaesth Scand 2003
Urea losses Muscle strength

Breuer et al, Anesth Analg, 2006
Preop carbohydrate reduces requirements of inotropic support in cardiac surgery
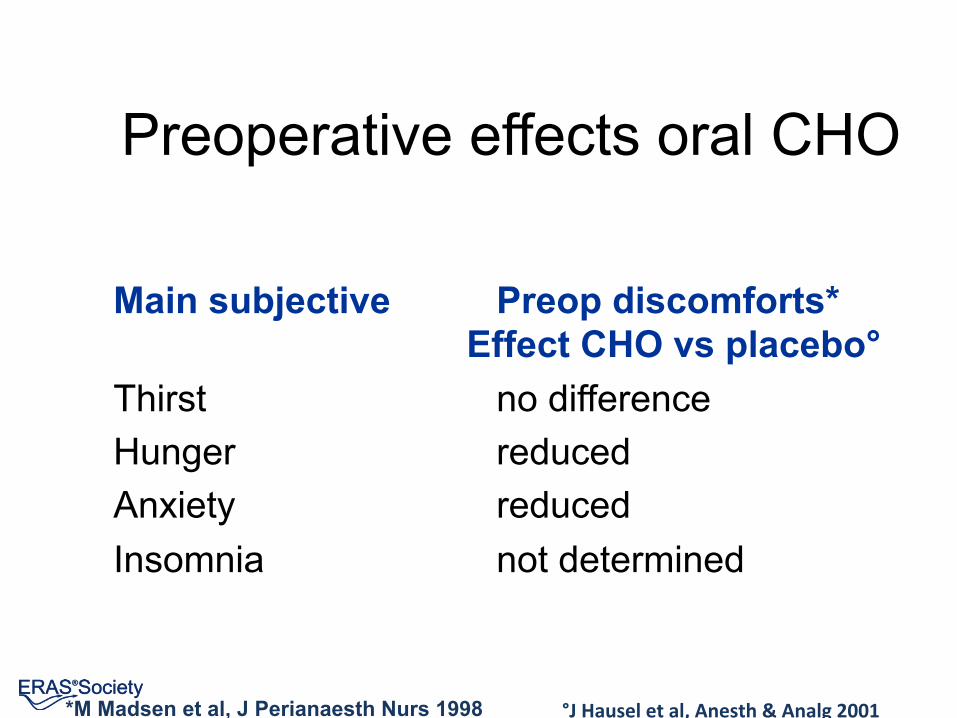
Preoperative effects oral CHO
Main subjective Preop discomforts* Effect CHO vs placebo°
Thirst no difference Hunger reduced Anxiety reduced Insomnia not determined
°J Hausel et al, Anesth & Analg 2001 *M Madsen et al, J Perianaesth Nurs 1998

All recent Guidelines recommend oral carbohydrate treatment Germany 2003: Major surgery Anaesthesist. 2003 Nov;52(11):1039-‐45.
Scandinavia 2005: Major surgery Acta Anaesthesiol Scand. 2005 Sep;49(8):1041-‐7
ESPEN 2005: Major surgery Clin Nutr. 2006 Apr;25(2):224-‐44
ESPEN 2009: Major surgery Clin Nutr. 2009 May 20
United Kingdom 2009: ElecEve surgery J Intensive Care Society. 2009;10(1):13-‐5
European Soc Anesthesiol 2011: ElecEve surgery Eur J Anaesthesiology. 2011;28:556-‐569
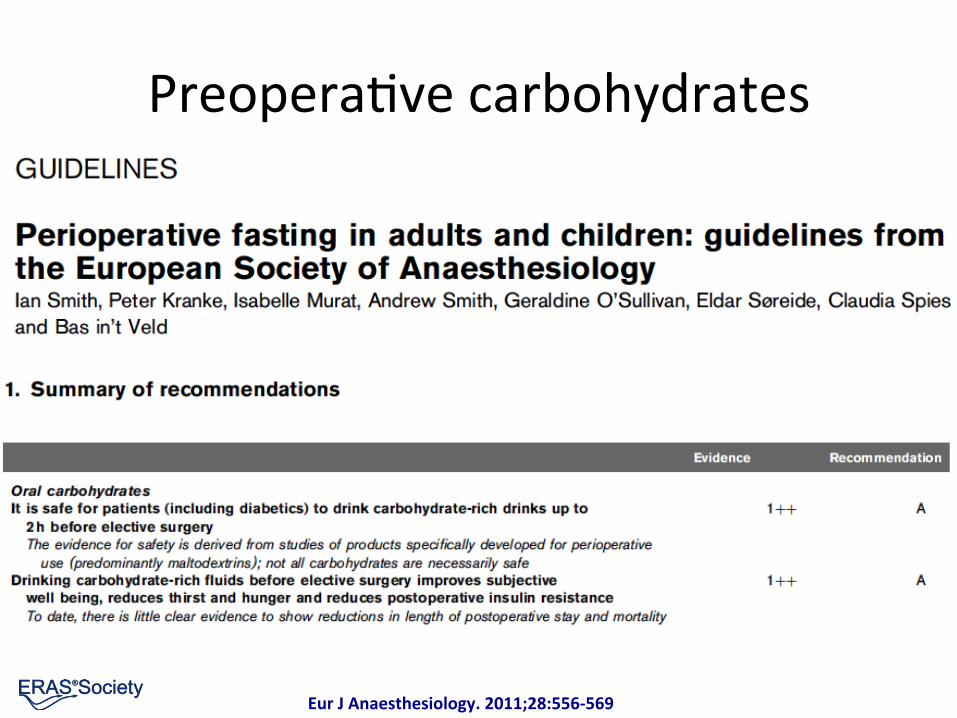
Eur J Anaesthesiology. 2011;28:556-‐569
PreoperaEve carbohydrates

Preop carbs shorter length of stay
*Awad et al, Clin Nutr 2012

Preop carbs shorter length of stay
Smith JD et al, Cochrane library 2014
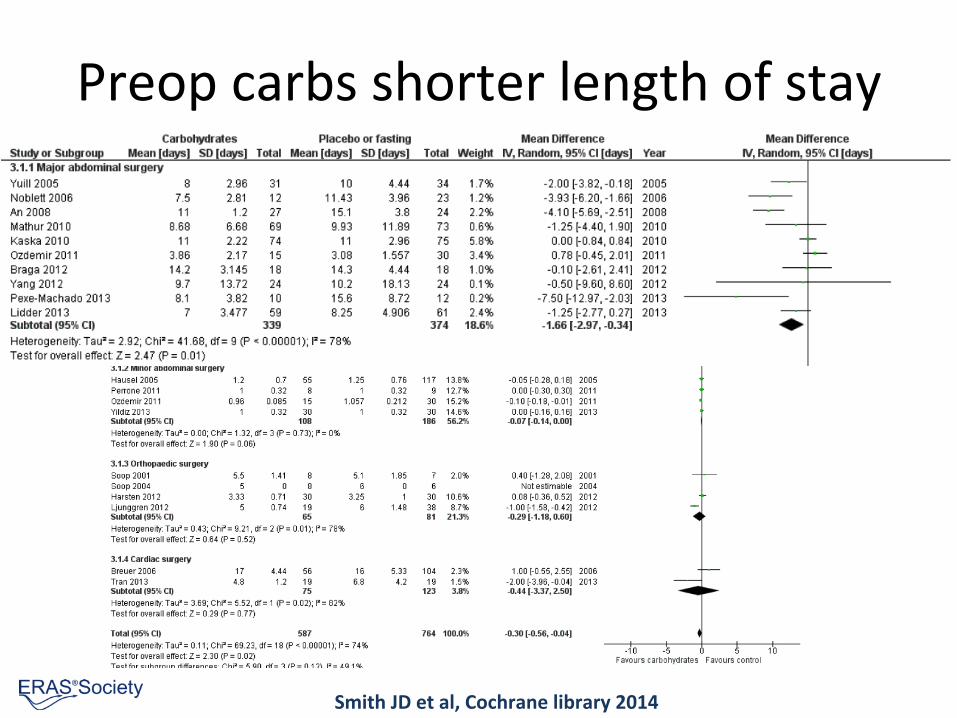
Preop carbs shorter length of stay
Smith JD et al, Cochrane library 2014

Combining carbohydrates with other stress reducing treatments
Combining carbohydrates with other stress reducing treatments
= Enhanced Recovery AIer Surgery
ERAS
Epidural Anaesthesia
Prevention of ileus/
prokinetics
CHO - loading/ no fasting
Early mobilisation
Peri-op fluid management
DVT prophylaxis
Pre-op councelling
Remifentanyl
No - premed
No bowel prep
Perioperative Nutrition
Bairhugger
Oral analgesics/ NSAID’s
Incisions
No NG tubes
Early removal of catheters/drains
Lassen et al, Arch Surg, 2009

EDA reduces postoperaEve insulin resistance
Uchida, Br J Surg 1988
-‐100
-‐50
0
50
100
150
200
250
300
350
Epinephrine Cor&sol Insulin sensi&vity
Postop
era&
ve cha
nge (%
)
IV Opiates EDA *p<0.05 **p<0.01
* * **

EDA + PreoperaEve CHO to control glucose during enteral feeding
Soop M et al, Br J Surg, 2004; *Harrison et al, JPEN 1997
0.0!
1.0!
2.0!
3.0!
4.0!
5.0!
6.0!
7.0!
8.0!
9.0!
10.0!Gl
ucos
e (m
mol
/l)!
Day!
complete!
hypocaloric!
Traditional*
No insulin required

Insulin sensiEvity improved with pre op Carb, EDA + post op feed
From Thorell et al: Curr Opin Clin Nutr Metab Care 1999, Soop M et al, Br J Surg, 2004
-‐80
-‐70
-‐60
-‐50
-‐40
-‐30
-‐20
-‐10
0 Lap chol Open hernia Open chol Open colorectal
Post op change in Insulin Sensi&vity (%)
Postop
/ Preo
p M-‐value
x 100
(%)
More Insulin
Resistance
Preop level
CHO EDA Postop Feed

Goals Back to normal food Energy and protein
2 Key targets: Gut working
Metabolism ready
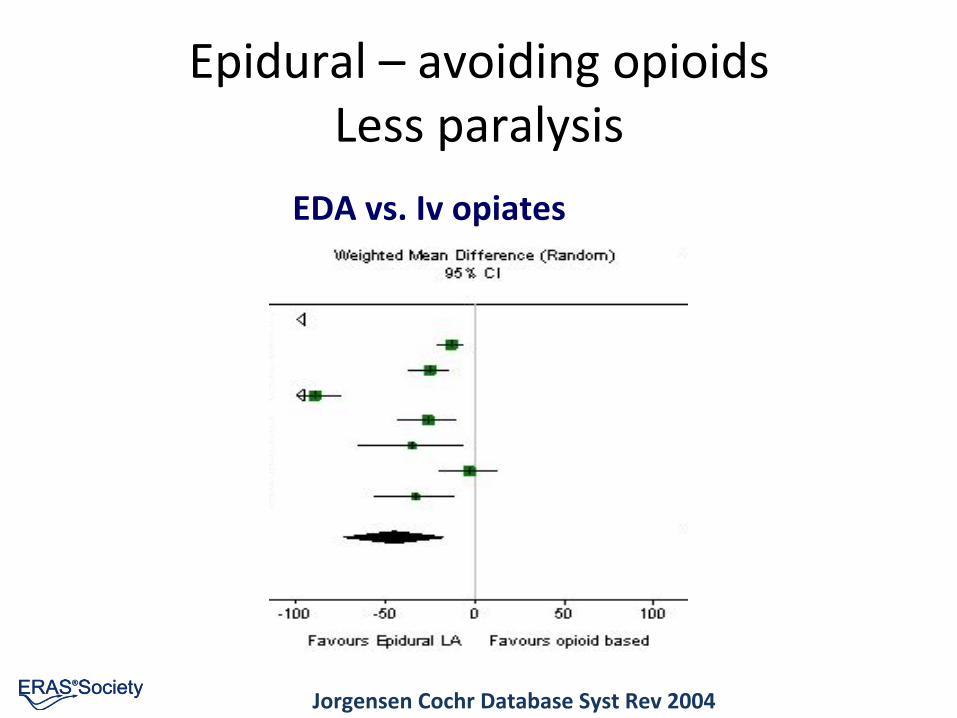
EDA vs. Iv opiates
Jorgensen Cochr Database Syst Rev 2004
Epidural – avoiding opioids Less paralysis

ERAS: oral intake development (mean intake postop day 1-‐4)

Energy intake ± ONS aIer liver resecEon
Hendry et al, BJS 2010
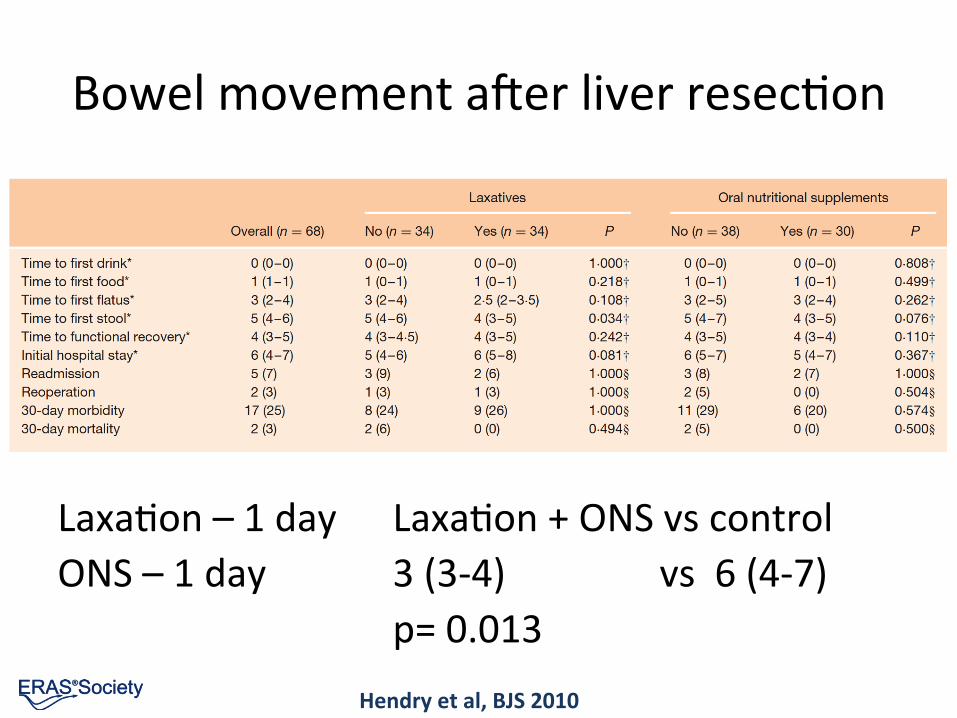
Bowel movement aIer liver resecEon
Hendry et al, BJS 2010
LaxaEon – 1 day LaxaEon + ONS vs control ONS – 1 day 3 (3-‐4) vs 6 (4-‐7) p= 0.013

ERAS in the old and co-‐morbid
Early ERAS / ERAS 2002-‐2004 / 2005-‐2006
< 75 years n= 160 / 164 > 74 years, ASA 1-‐2, n= 89 / 50 > 74 years, ASA 3-‐4 n = 34 / 33
Thus, 39% over 75 years Colonic resecEon J Nygren, Ersta hospital personal communicaEon
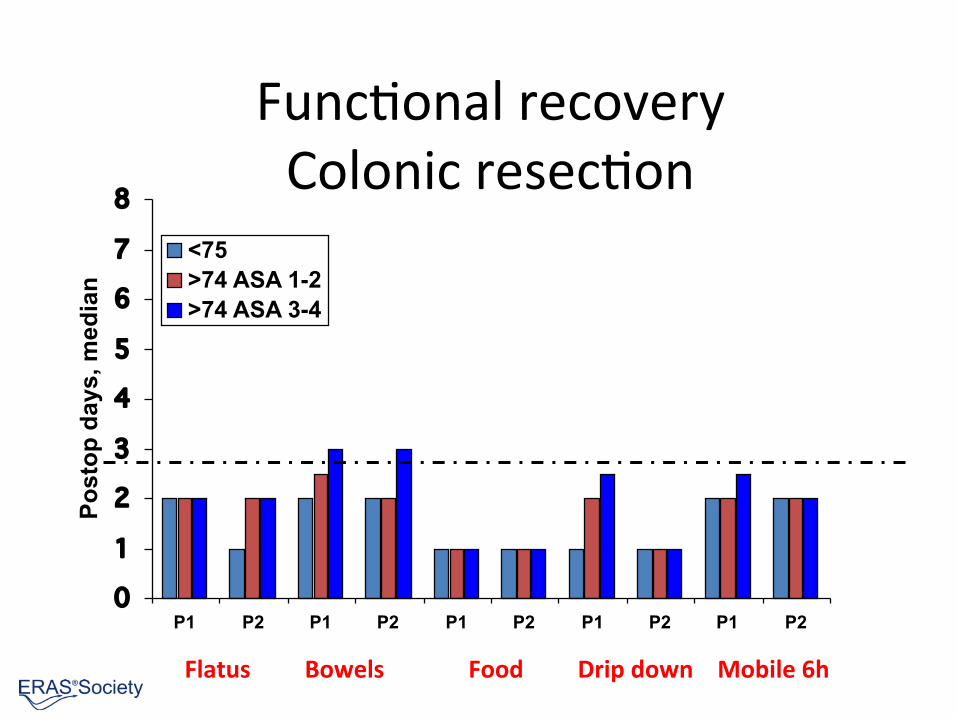
FuncEonal recovery Colonic resecEon
012345678
P1 P2 P1 P2 P1 P2 P1 P2 P1 P2
Pos
top
days
, med
ian
<75>74 ASA 1-2>74 ASA 3-4
Flatus Bowels Food Drip down Mobile 6h
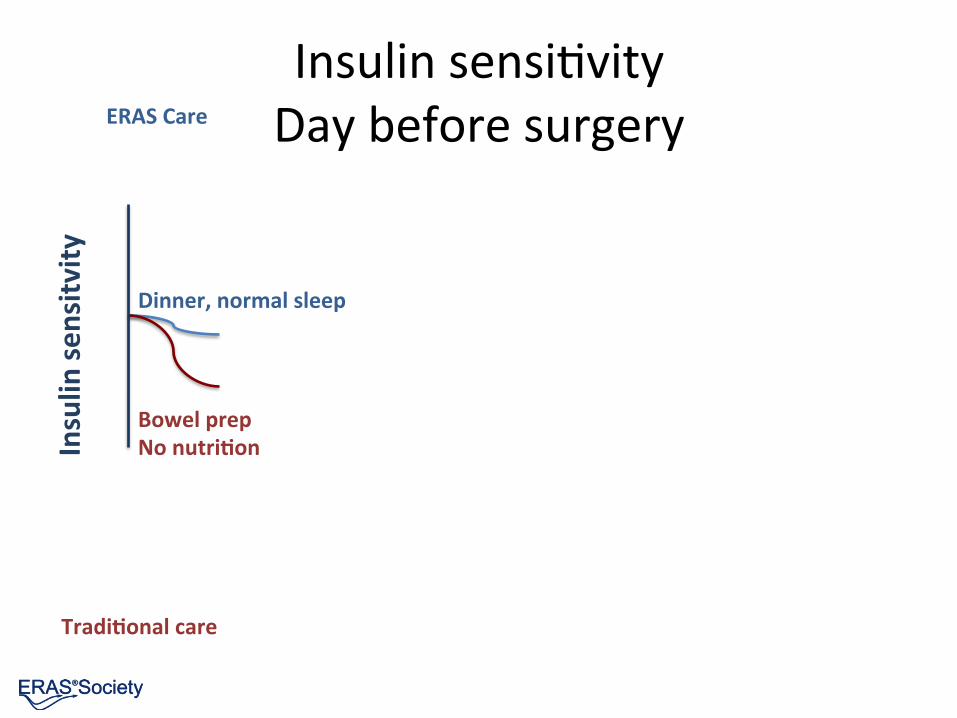
Insulin sensiEvity Day before surgery Insulin
sensitv
ity
Bowel prep No nutri&on
Dinner, normal sleep
ERAS Care
Tradi&onal care

Insulin sensiEvity Morning of surgery Insulin
sensitv
ity
Bowel prep No nutriEon
Dinner, normal sleep
Carbohydrate treatment
Overnight fas&ng
ERAS Care
Tradi&onal care

Insulin sensiEvity Anesthesia start
Insulin
sensitv
ity
Bowel prep No nutriEon
Dinner, normal sleep Carbohydrate treatment
Overnight fasEng
Thoracic Epidural
Preopera&ve seda&on
ERAS Care
Tradi&onal care

Insulin sensiEvity ReacEon to surgery Insulin
sensitv
ity
Bowel prep No nutriEon
Dinner, normal sleep Carbohydrate treatment
Overnight fasEng
Thoracic Epidural
PreoperaEve sedaEon
Surgery
Greater drop without Epidural
ERAS Care
Tradi&onal care

Insulin sensiEvity AIernoon of surgery Insulin
sensitv
ity
Bowel prep No nutriEon
Dinner, normal sleep Carbohydrate treatment
Overnight fasEng
Thoracic Epidural
PreoperaEve sedaEon
Surgery
Immediate feeding & mobilisa&on
NPO iv low caloric fluids
ERAS Care
Tradi&onal care

Insulin sensiEvity Days aIer surgery
Insulin
sensitv
ity
Bowel prep No nutriEon
Dinner, normal sleep Carbohydrate treatment
Overnight fasEng
Thoracic Epidural
PreoperaEve sedaEon
Surgery
Immediate feeding & mobilisaEon
NPO iv low caloric fluids
Oral feeding & mobilisa&on
Slow return to feeding and mobilisa&on Days -‐ weeks
ERAS Care
Tradi&onal care

Insulin sensiEvity Days aIer surgery
Insu
lin s
ensi
tvity
Bowel prep No nutriEon
Dinner, normal sleep Carbohydrate treatment
Overnight fasEng
Thoracic Epidural
PreoperaEve sedaEon
Surgery
Immediate feeding & mobilisation
NPO iv low caloric fluids
Oral feeding & mobilisation
Slow return to feeding and mobilisa&on Days - weeks
ERAS Care
Traditional care
Ljungqvist JPEN 2012

Gut working
• Avoiding opioids
• Fluid balance
• Chewing gum 3 Emes daily
• LaxaEves

October 14, 2014 Olle Ljungqvist 85
Slower gastric emptying and bowel movements
Overloading with fluids and salt reduces GI motility
Lobo D, Lancet 2002: 359; 1812-‐1818
Passage of gas: 2 days faster; stools: 3 days faster
Body weight Gastric emptying

Chewing gum: flatus 8h sooner
Li S et al, J Gastroenterol Hepatol. 2013 Jul;28(7):1122-‐32

Chewing gum: bowels move 0,5d sooner
Li S et al, J Gastroenterol Hepatol. 2013 Jul;28(7):1122-‐32

Chewing gum: shorter length of stay
Li S et al, J Gastroenterol Hepatol. 2013 Jul;28(7):1122-‐32

Chewing gum in benign gynecology
Jerrigan AM et al Int J Gyn Obst, 2014 in press

LaxaEves in hysterectomy
Hansen CT et al, AJOB 2007; 196
Bowel movement laxaEves 45h, controls 69h, p<0.001, n= 53
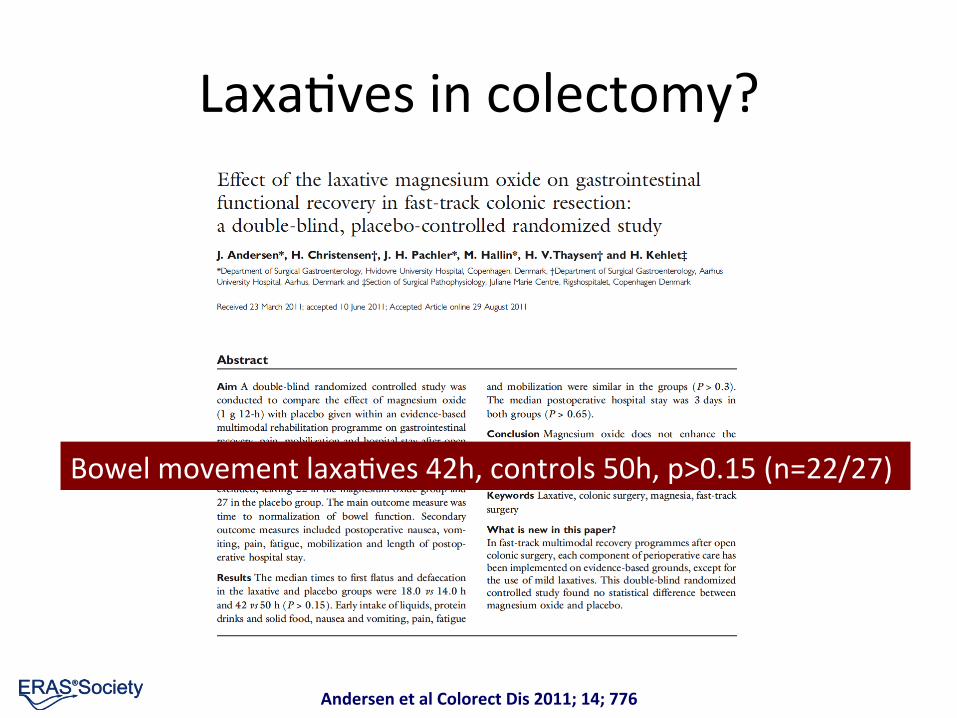
LaxaEves in colectomy?
Andersen et al Colorect Dis 2011; 14; 776
Bowel movement laxaEves 42h, controls 50h, p>0.15 (n=22/27)

ERAS guideline 2014: Gastrectomy
Colon
Pancreas
Rectal

ERAS compliance: Length of stay & Readmissions
Gustafsson et al, Arch Surg 2011
n = 953 p < 0.05
Compliance with ERAS protocol elements Single center study consecutive patients
Colorectal cancer

ERAS compliance: ComplicaEons
Gustafsson et al, Arch Surg, 2011
n = 953 p < 0.05
0"
5"
10"
15"
20"
25"
30"
35"
40"
45"
50"
<50%" >70%" >80%" >90%"
Complica6ons"
Compliance with ERAS protocol elements Single center study, consecutive patients
Per
cen
t pat
ient
s af
fect
ed
Colorectal cancer
n = 953 P < 0.05

Reduced mortality?
Savaridas et al, Acta Orthopedica 2013: 84, 40-‐43
Hip and Knee replacement TradiEonal AIer implementaEon of ERAS Causes of death Higher for Trad: Malignant disease

ERAS Compliance: LOS in open colonic resecEons
N= 57 own cases (green dot), compared to 934 total cases in 15 other centers

Recovery – what does it mean?
Lee et al, Surgery 2014

3rd World Congress of ERAS® Society with American Society for Enhanced Recovery Evidence Based PerioperaEve Medicine UK ERAS Society introductory course Henrik Kehlet lecture ERAS Society lecture ERAS Society guidelines ERAS for the surgeon
the anesthesiologist the nurse the manager
New findings – abstracts Debates Workshops
www.erassociety.org

Summary: NutriEon & ERAS
Gut working • Avoid opioid induced gut paralysis • Keep fluids in balance • Food, ONS combined for energy and protein • + laxa&ves for even faster gut recovery • Chewing gum Metabolism ready • Minimize insulin resistance Combining ERAS elements for best results

Summary: NutriEon & ERAS
Gut working • Avoid opioid induced gut paralysis • Keep fluids in balance • Food, ONS combined for energy and protein • + laxa&ves for even faster gut recovery • Chewing gum Metabolism ready • Minimize insulin resistance Combining ERAS elements for best results
Ge{ng metabolism and nutri&on right is key in ERAS

Stockholm winter
Stockholm winter