
LTC - Part of the Solution in Community Preparednessarhealthcare.com/sites/default/files/2017-06/LTC...
57
Long Term Care: Part of the Solution in Community Preparedness
Transcript of LTC - Part of the Solution in Community Preparednessarhealthcare.com/sites/default/files/2017-06/LTC...
Long Term Care:Part of the Solution
in Community Preparedness

2017 Long Term Care Emergency Preparedness District Roundtable Training
Funding for this conference was made possible ( in part) by the Centers for Disease Control and Prevention. The views expressed in written conference materials or publications and by speakers and moderators do not necessarily reflect the official policies of the Department of Health and Human Services, nor does the mention of trade names, commercial practices, or organizations imply endorsement by the U.S. Government.

WhatisLongTermCare?

Long Term Care Facility• Refers to any of a range of institutions that
provide health care to people who are unable to manage independently in the community
• Facilities may provide short and long-term rehabilitative services as well as chronic health care management
www.longtermcareliving.com/glossary
Wide Range of Facilitiesin Long Term Care
• It can consist of:– Care in the home by family members who are
assisted with voluntary or employed help– Adult day health care– Care in assisted living facilities– Care in skilled nursing facilities– Care in other types of residential facilities
www.longtermcareliving.com/glossary

Wide Range of Recipients inLong Term Care
• It can include people who are: – Pediatric, elderly, in between– ambulatory – non ambulatory – cognitively intact– cognitively impaired– minimal assistance– completely dependant for all activities of daily livingAnd have special medical and/or behavioral needs

Skilled Nursing Facility Defined
“Skilled nursing facility" is defined as an institution (or a distinct part of an institution) which is primarily engaged in providing skilled nursing care and related services for residents who require medical or nursing care, or rehabilitation services for the rehabilitation of injured, disabled, or sick persons, and is not primarily for the care and treatment of mental diseases; …
§§1819(a) and 1919(a) of the Social Security Act

Snapshot of Nation’s SNFs• Approximately 16,000 SNFs • 1,730,000 licensed beds• 917,000 nursing staff• 122,400 RNs• 192,100 LPNs• 608,900 CNAs• 12,500 NAs/Orderlies
CDC National Center for Health Statistics 2006/2007 data
Snapshot of SNF Residents• 1,492,200 living in skilled nursing homes on
any given day.• The vast majority of these people are: • 75 or older• Female• White• Stay less than 3 months
Snapshot of SNF Residents
• Disease prevalence very high
• 61% have mental &/or cognitive conditions
• 41% do not walk• Only 18% walk without
help or supervision
Kaiser Commission on Medicaid and the Uninsured

LTC Disaster Capabilities• A critical component of the healthcare
system• Experts in caring for medically fragile
populations• Bed capacity• Back up power• Medications• Emergency Supplies

Federal Regulation Requirements
• CFR 483.75 (m) disaster and emergency preparedness
• F517 (1)the facility must have detailed written plans and procedures to meet all potential emergencies and disasters, such as fire, severe weather, and missing residents.
Federal Regulation Requirements
• CFR 483.75 (m) disaster and emergency preparedness– F518 (2) The facility must train
all employees in emergency procedures when they begin to work in the facility, periodically review the procedures with existing staff, and carry out unannounced staff drills using those procedures

Skilled Nursing Facilities as Resource?
YES…
BUT…

LTC Disaster Challenges• LTC facilities serve the medically fragile,
who may be more severely impacted by disasters
• Very little physician presence• High staff turnover• Scare resources for training or equipment• Typically not included in healthcare
preparedness community coalitions

LTC Disaster Needs• More involvement with local planning
efforts• Stronger facility emergency operation
plans, particularly from the “walls out”• Assistance to prepare as a partner in
response

LTC During Katrina
LTC During Katrina• All studied Gulf State nursing homes (20) met
the federal requirements on their most recent state survey
• All experienced problems, whether they evacuated or sheltered in place
• Plans were often missing several planning elements recommended by experts
• Plans were not up to date• Administrators not always familiar with plans

LTC During KatrinaEvacuation Issues:
– Instructions for evacuating to an alternate site– Guidance for deciding whether to evacuate or
shelter in place– Information about the specific needs of
residents (to allow staff to modify plans according to residents’ needs)
– Plans for reentry of facility

LTC During KatrinaSheltering in Place Issues:
– Problems with staffing– Uncertainty of access to community resources– Shortages of supplies narrowly averted – Power disruptions (2 hours—4 weeks)– Generators taxed (A/C in high temperatures;
generators only supported lights and fans)– Psychological stress on residents

LTC During KatrinaFindings:
• Lack of collaboration between state & local emergency entities and nursing homes– Review of plans and prior collaboration can
build better plans, and result in better emergency management & access to resources
HHS. Nursing Home Emergency Preparedness & Response During Recent Hurricanes.

Southern California 2007

Largest Evacuation (CA History)
• Approximately 515, 000 people evacuated• Over 2,200 medical patients evacuated• 14 Skilled Nursing Facilities• 5 Intermediate Care Facilities (MR)• 1 Acute Psychiatric Facility• 3 General Acute Care Hospitals

How Did LTC Do?• No structures lost
• No disaster – related deaths
• Displace residents received excellent care at other facilities and shelters
• Staff reported to work Many not knowing whether or not their house were standing
Lessons Learned During Fire StormNEED:• Centralized location to coordinate special needs
response operations, patient and bed tracking.
• Patient identification bands with critical medical information.
• Staff identification that enable them to return to facilities.
• LTC evacuation plans that adequately address transport of patients to other facilities.
• Criteria for approval to repatriate facility
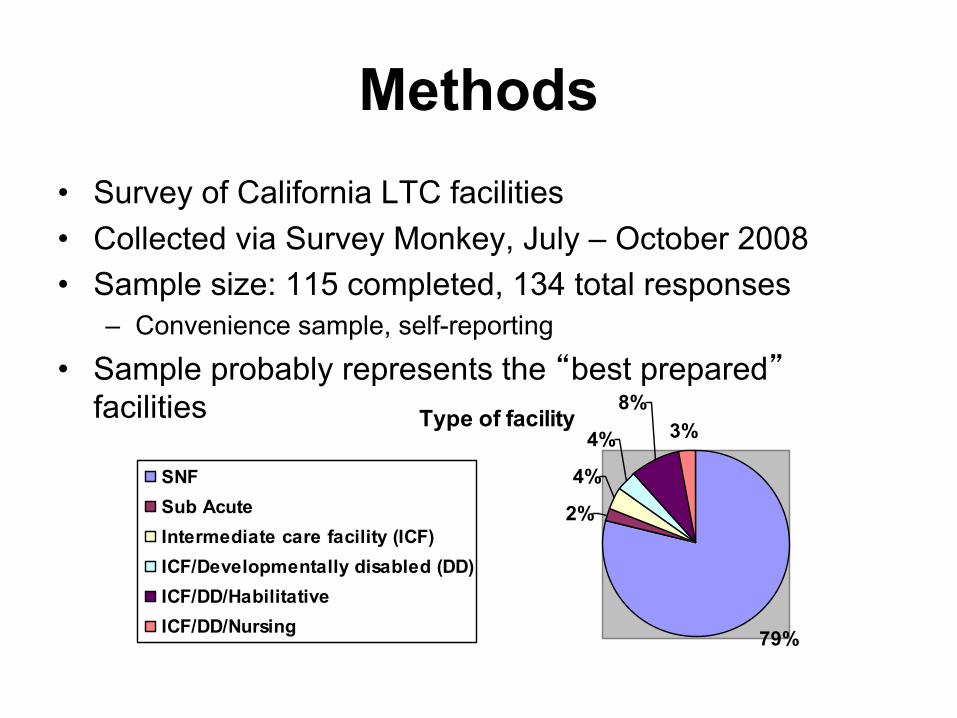
Methods• Survey of California LTC facilities• Collected via Survey Monkey, July – October 2008• Sample size: 115 completed, 134 total responses
– Convenience sample, self-reporting• Sample probably represents the “best prepared”
facilities Type of facility
79%
2%
4%
4%
8%3%
SNFSub AcuteIntermediate care facility (ICF)ICF/Developmentally disabled (DD)ICF/DD/HabilitativeICF/DD/Nursing
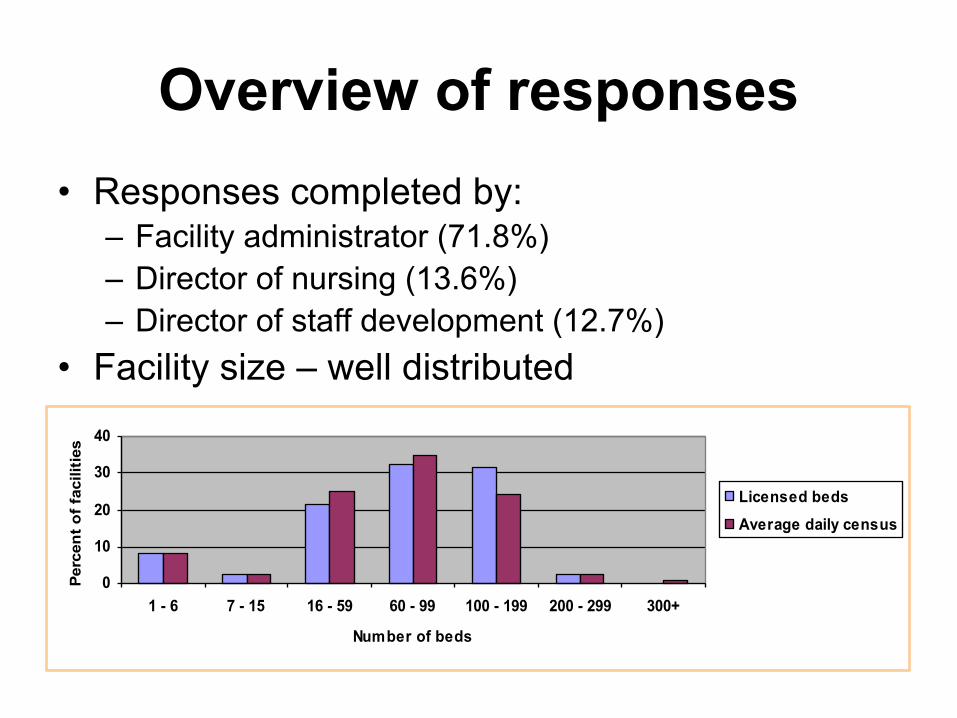
Overview of responses• Responses completed by:
– Facility administrator (71.8%)– Director of nursing (13.6%)– Director of staff development (12.7%)
• Facility size – well distributed
0
10
20
30
40
1 - 6 7 - 15 16 - 59 60 - 99 100 - 199 200 - 299 300+
Number of beds
Perc
ent o
f fac
ilitie
s
Licensed bedsAverage daily census

Readiness for evacuation• Evacuation includes:
– Receiving residents– Sending residents– Agreements with “like” facilities
• Within emergency operations plan (EOPs):– 99.1% facilities address evacuation– 87.9% address coordination with “like” facilities – 80.3% included processes for sharing residents’
information with other facilities and external/public agencies• Evacuation planning with local community partners
ranked second as a priority for next year
Sending residents/patients• Readiness of facilities to evacuate within 1 hour:
– Food ready to go: 87.4%– Water ready to go: 82.4% – Essential medical supplies/medication ready to go:
84.9%– Critical health info for residents ready to go: 87.4%
• Planned evacuation meals for residents: 74.6%• Planned meals for staff: 44.9%

Transportation preparedness • Facilities with transportation vendors or
ownership of vehicles for use in an evacuation: 47.9%– Of these, 44.7% have discussed their
vendors’ business continuity plan and priority of assistance
• 43.7% do not have readily available means to evacuate residents– And are dependent on external emergency
agencies

Receiving residents/patients• Does the EOP address receiving patients?
– 69.7% did– 19.7% did not – 10.6% didn’t know
• Specific procedures for accepting residents from like facilities:– 70.9% did– 20.5% did not (8.5% did not know)
Managing unsolicited clinical help
• Lack preparedness to handle clinical volunteers
• Most facilities did not have procedures to manage unsolicited clinical help
• Most facilities did not have procedures to request and receive volunteer health professionals from the county:

Readiness for sheltering in place• Performance target: > 72 hours’ supplies on hand• Most facilities in survey prepared – in some way – to SIP• However, adequate pharmaceuticals: only 76.7%• Facilities with no water stored: 6% either had no water
for staff or residents Days of potable water stored
020406080
None 1 2 3 4 5 > 5
Days
Perc
ent o
f fac
ilitie
s
Water for residentsWater for staff

Sheltering the staff in place• Adequate water (72+ hrs) for staff: 89.0% of facilities• Adequate food for staff: 88.1%• Extra bed linens for staff: 71.8% • Adequate extra cots, mattresses, or roll-away beds for staff: 25.4%• Most facilities have at least some supplies, even if they fall below the
72 hour target• But…this also means 11% don’t have adequate water, 12% don’t have
adequate food, etc.
Supplies for staff to shelter in place for 72 hours
020406080
100
Food Potablewater
Bedlinens
Cots
Type of supply
Perc
enta
ge YesNoSome, but not enoughDon't know

Power and utilities• Automatic gas shutoff valves in 49.2%;
facilities without gas shutoff values 42.4% (7.6% didn’t know)
• Power failure addressed in EOP: 85.3% of facilities
• Facilities with stand-by/emergency generator capability 89.8%
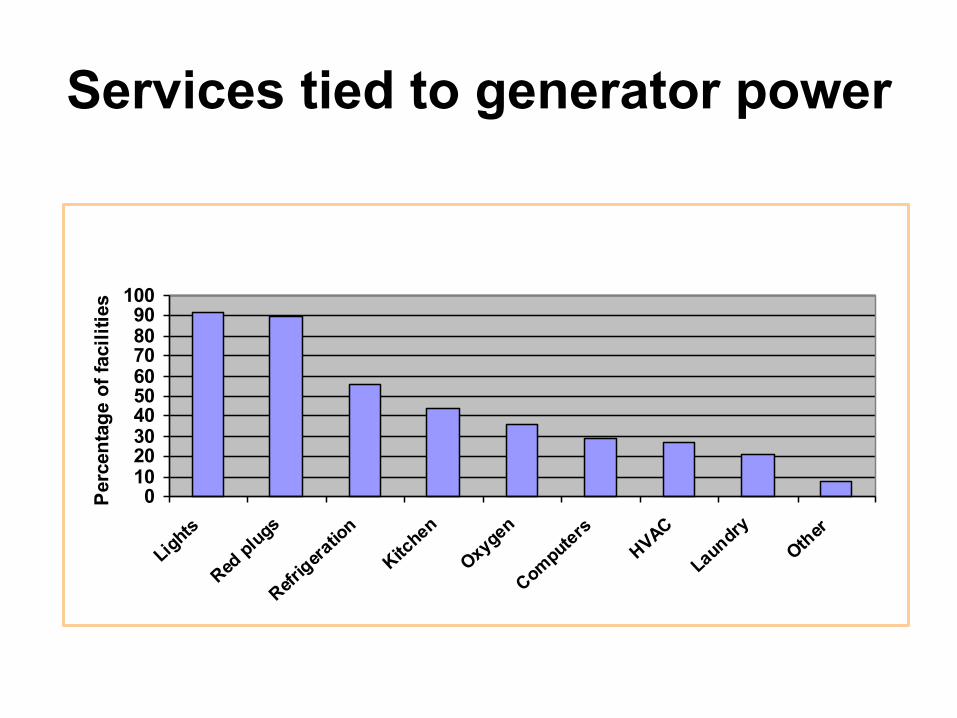
Services tied to generator power
0102030405060708090
100
Lights
Red plugs
Refrigera
tion
Kitchen
Oxygen
ComputersHVAC
LaundryOther
Perc
enta
ge o
f fac
ilitie
s
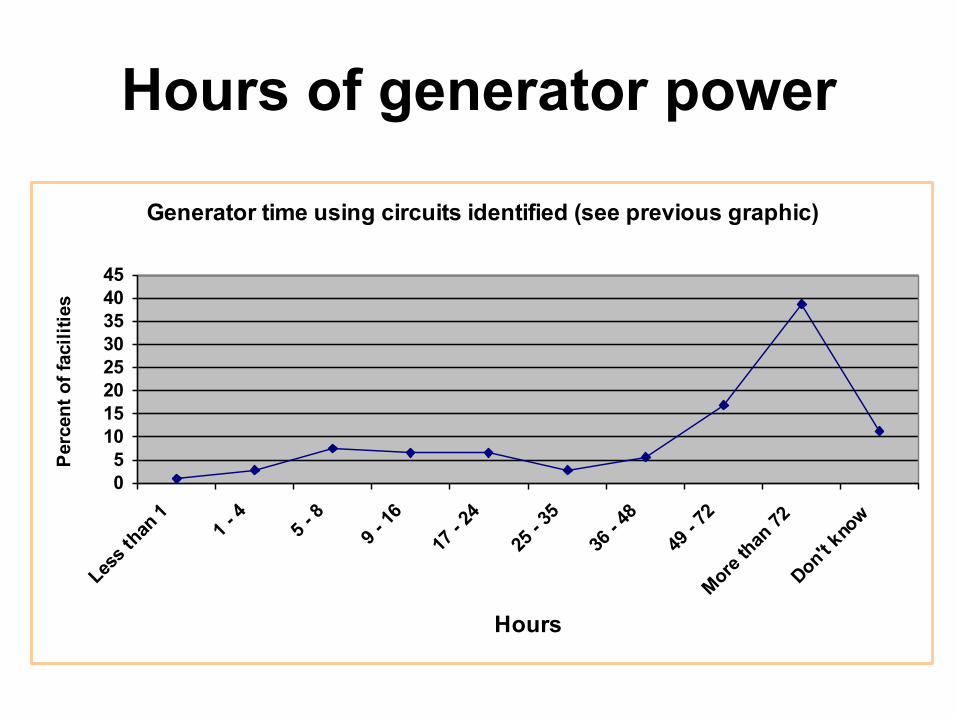
Hours of generator power
Generator time using circuits identified (see previous graphic)
05
1015202530354045
Less th
an 1
1 - 4
5 - 8
9 - 16
17 - 2
425
- 35
36 - 4
849
- 72
More than
72
Don't kno
w
Hours
Perc
ent o
f fac
ilitie
s
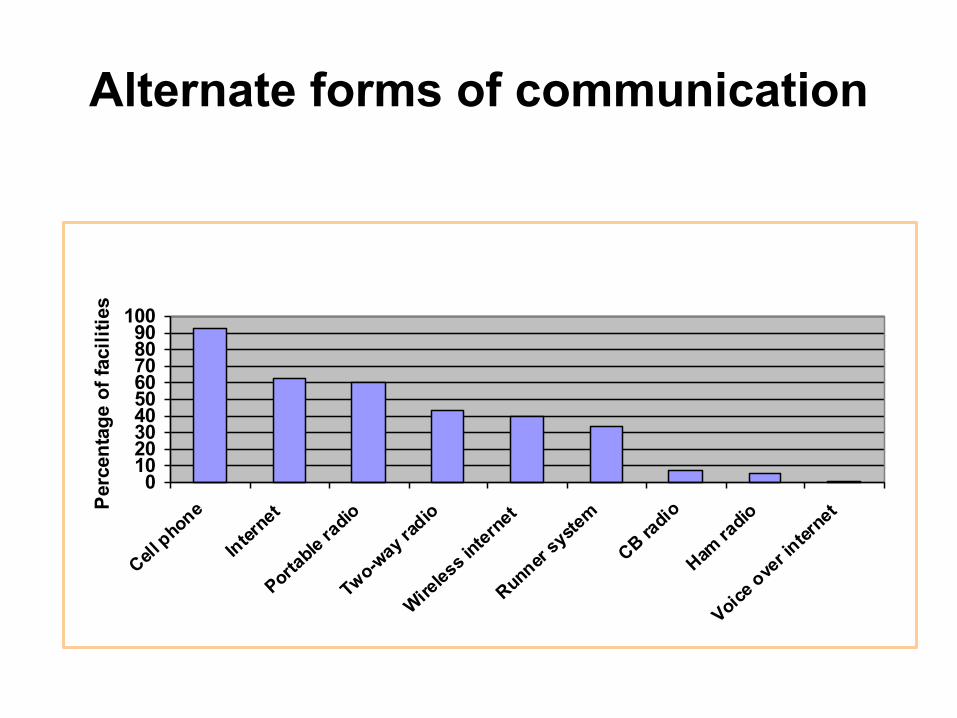
Alternate forms of communication
0102030405060708090
100
Cell phone
Internet
Portable ra
dio
Two-way ra
dio
Wireless i
nternet
Runner syste
m
CB radio
Ham ra
dio
Voice ove
r inter
netPerc
enta
ge o
f fac
ilitie
s

Internet-connected computers• Most facilities: at least 5 computers• Most facilities (> 94.6%) used their computers for web
access and email, facility computers played a key role in clinical care:
• Residents had internet access in 18.4% of facilities.
Internet-connected computers
0
10
20
30
40
None 1 - 5 6 - 10 11 - 20 21 - 30 > 30
Perc
ent o
f fac
ilitie
s
Computers withinternet access
Security• Lacking funding, lacking dedicated resources
• Most facilities’ staff not required to wear photo identification:
• Most facilities (69.9%) did not have security staff
• Facilities with procedures for locking down all exterior doors without help from external agencies: 54.7%
• Several facilities identified the use of surveillance systems (alarms) and/or security cameras as security mechanisms

Emergency operations plans (EOP)
• Hazard and Vulnerability Analysis • 22.2% completed HVA within last 5 years
– 41% had not – 36.8% didn’t know
• EOPs covered:– Evacuation planning - 99.1%– Sheltering in place - 96.6%– Command and control - 95.7%– Triage of casualties - 86.2%– Contingency of power failure - 85.3%

Local planning aspects addressed in EOPs
0102030405060708090
100
Hospitals Emergencyplanners
Community or faithbased groups
"Like" facilities
Coordination with local entities
Perc
ent o
f fac
ilitie
s
Yes No Don't know
Engagement in local planning• Local surge planning
– Facilities participating - 48.3% – Not participating - 34.7% – 16.9% didn’t know
• Receiving funds or supplies from local health/emergency services agency– Did receive funds/supplies - 6.8%– Did not - 82.9% – 10.3% didn’t know
• EOPs reviewed by local emergency planning officials: – 39.1% of facilities– 47% had not been reviewed locally– 13.9% didn’t know

Incident command systemsUse of HICS for emergency
operations
No42%
Don't know27%
Yes31%
Pandemic influenza preparedness
• A general lack of preparedness• Isolation/reverse ventilation rooms:
– Facilities with: 16%– With out: 82% did not (2% didn’t know)
• Infectious disease emergencies addressed in EOPs:– 38.3% addressed quarantine – 37.1% addressed configuration of facility space for
isolation or quarantine during an epidemic; and,– 27.4% addressed storage of remains following a
mass casualty event

Infectious disease preparedness as addressed in EOPs
0
10
20
30
40
50
60
Isolation of infectedpatients
Quarantine Reconfiguration ofspace for quarantine
Perc
ent o
f fac
ilitie
s
Yes No Don't know
Top 5 ranked priorities for the future
1. Development of risk assessments using an all-hazards approach
2. Evacuation planning, particularly with external partners
3. Implementing an incident command system for use during emergencies
4. Formalizing MOUs with like facilities; arrangements with vendors/service providers
5. Develop and maintain a communication plan that complies with Fed, State and local laws
Response Community Working with LTC Providers
• Understand the unique position that LTC is in, BOTH as a resource and as a group that may have needs
• Actively include LTC in your disaster-related workgroups and planning activities (example: pandemic planning)
• Accept invitations from the LTC community to work together (meetings, planning)
• Consider the challenges they face

Arkansas LTC Some Positive Practices

AHCA Disaster Preparedness Program
• Increase disaster readiness of individual long term care facilities (LTC)
• Promote integration and collaboration between LTC providers and– Other providers– Other healthcare partners– Emergency response
planners– State– Regional– Local levels

Sustainment Strategies• Broad impact over
geographies, ages, workforces
• Prolonged over weeks/months
• Resources will be decreased
• Demand for care will be increased
Annex to Disaster Plan• Build on the existing plan:
Disasters and Infectious Disease Outbreaks
• Add sustainability over weeks/months• Staffing strategies • Plan for higher acuity residents due to
an inability to transfer to acute care• Management of deceased
• Disaster supplies for all hazards (including food, water, etc.)
• Personal Protective Equipment (PPE)• Rehydration supplies• Infection control supplies• Respiratory care supplies• Mortuary supplies • OTC medications and Rx meds (antivirals) as
allowable under the regs
Start Stocking Up Now
Types of Supplies to Stockpile
Simple Oral Rehydration Solution1 TSP salt 4 TBSP sugar 8 Cups of clean drinking or boiled water and then cooled
Emergency Staffing Strategies
• Prepare for “worst case” 50 % absenteeism
• Cross Training in essential services– Resident Care– Food Service– Housekeeping– Laundry– Essential Administrative Procedures

Facility Security
• Protection of supplies may be important• Consider assigning security personnel
during high risk times• Control access to facility• Control access to supplies• Self protection training for staff• Deliveries of supplies be protected
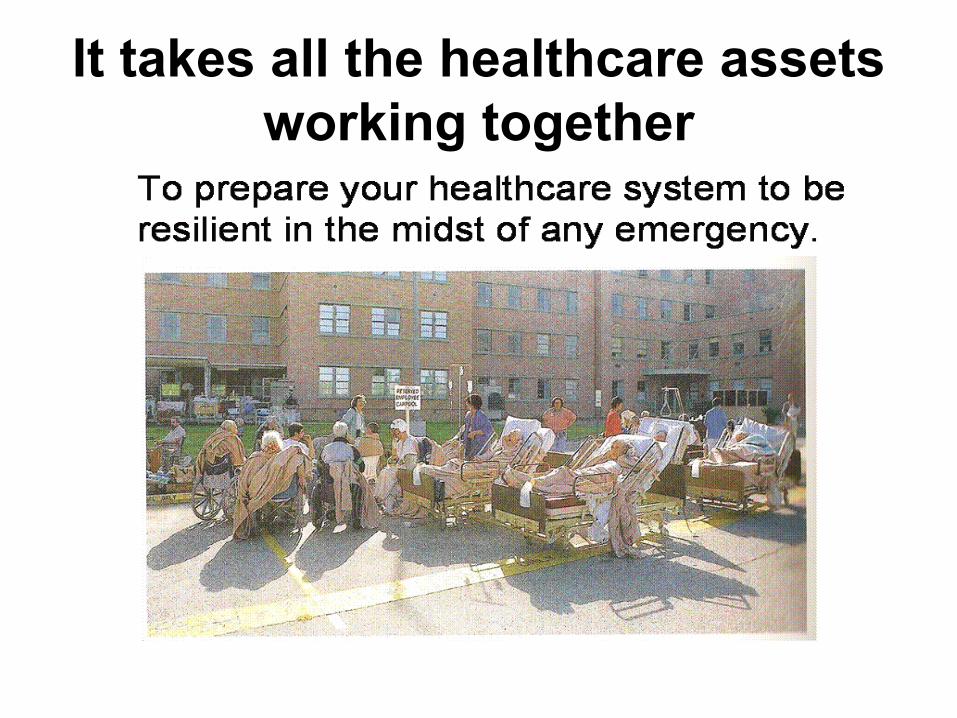
It takes all the healthcare assets working together
So Lets Work Together!


















