
LSVT LOUD · Have you noticed any slurring or mumbling in your speech? ... What would you like to...
37
Copyright© 2012 LSVT Global, Inc. 5- 23 This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians LSVT ® LOUD Assessment Packet Initial Interview Evaluation Protocol Stimulability Protocol Follow-up Questions Perceptual Scales
-
Upload
vuongquynh -
Category
Documents
-
view
221 -
download
2
Transcript of LSVT LOUD · Have you noticed any slurring or mumbling in your speech? ... What would you like to...
Copyright© 2012 LSVT Global, Inc. 5- 23
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
LSVT®
LOUD
Assessment Packet Initial Interview
Evaluation Protocol Stimulability Protocol Follow-up Questions
Perceptual Scales

Copyright© 2012 LSVT Global, Inc. 5- 24
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
LSVT® LOUD Initial Interview
Identifying Information
Name: email address:
Address:
City: State: Zip: Phone:
Fax: Age: Date of Birth:
Date and Time of Day of Initial Interview:
Diagnosis/Stage: Date of Initial Diagnosis:
Time of Last Park med: Time of Next Park med:
Neurologist: Phone:
Address:
Neurosurgeon: Phone:
Address:
Otolaryngologist: Phone:
Address:
Physical Therapist: Phone:
Address:
Neurological and Other Medical Information
What were your initial symptoms of Parkinson disease?
Do you have any tremor? Yes No If yes, please describe:
Do you have any other medical problems? Yes No If yes, please describe:
Copyright© 2012 LSVT Global, Inc. 5- 25
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
Medication Information: Medication for Parkinson disease:
Other Medications:
How is it helpful?
Does your Parkinson medication affect your voice or speech? Yes No If yes, please describe:
Do you experience “on/off” symptoms? Yes No If yes, please describe:
Do you experience any dyskinesias: Yes No If yes, please describe:
Surgical Information:
Have you had neurosurgery or laryngeal surgery? If yes, what procedure, when, where, by whom?
Speech Symptoms:
Have you ever used your voice professionally (i.e., radio, television, acting, singing, etc.)? Yes No
If yes, please describe:
When did you first start to notice communication symptoms (i.e., changes in your speech and/or voice) that you
associate with Parkinson disease?
What are your current symptoms?
What is your most significant problem communicating today?
How do you typically use your voice during the day?

Copyright© 2012 LSVT Global, Inc. 5- 26
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
How many hours of speaking do you do in a day?
Right now does your voice sound like it usually does?
Do people ask you to repeat?
What do you do when you want to be as easy to understand as possible?
What percent of your speech do you think is intelligible (i.e., people can understand you)?
Has Parkinson disease caused you to talk less? How much less?
Why has Parkinson disease caused you to talk less?
Do you think you run out of breath during speech?
Is it difficult for you to take a deep breath?
Have you noticed if your voice is monotone in pitch?
Have you noticed if your speaking voice is higher or lower in pitch now compared to before you were diagnosed
with Parkinson disease?
Have you noticed pitch breaks in your voice?
Have you noticed changes in your singing voice?
Have you noticed changes in the quality of your voice?
If yes, please describe the changes you have noticed in quality. (Probe patient to determine if patient thinks voice
quality is hoarse, wet, breathy, rough, strained, etc.)
Have you noticed changes in the steadiness of your voice?
Does your voice feel fatigued at the end of the day?
Have you noticed if your voice is reduced in loudness?
Have you noticed any slurring or mumbling in your speech?
Has the rate of your speech changed?
If yes, please describe how your rate has changed. (Probe patient to determine if patient thinks rate is faster, slower,
variable, etc.)
Copyright© 2012 LSVT Global, Inc. 5- 27
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
Have you noticed any stuttering in your speech?
Do you experience food or liquid coming through your nose when you eat?
Do you think your voice sounds nasal (i.e., hyper or hyponasal)?
Have you previously had speech treatment?
If yes, how long ago and what did you do?
Was your previous speech treatment beneficial?
If yes, what changes did you notice? Describe
Swallowing Information:
Have you noticed any problems with eating, chewing, and/or swallowing?
If yes, please describe (types of foods, frequency of problem, etc.)
Have you noticed any change in taste or smell? If yes, what type of change?
Employment Information
Are you employed?
Type of employment?
Describe how you use your voice at your job.
Does Parkinson disease affect your employment?
How?

Copyright© 2012 LSVT Global, Inc. 5- 28
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
Neuropsychological Information
Have you noticed any difficulty with your memory?
What have you noticed?
Does your medication affect your memory?
If yes, how does it affect your memory?
What aspect of your Parkinson disease bothers you the most?
Other comments:
Questions to help determine/create “Magical Calibration Moments”
Communication Situations:
If you had one situation in which you wanted to communicate well, what would it be?
Describe your day in terms of speaking situations (i.e., elicit from the patient information about who the patient
communicates with, when the communication is done, and what may be said).
AM
PM
When do you find it most difficult to communicate?
Why is it difficult to communicate in these situations/times that you mentioned?
Copyright© 2012 LSVT Global, Inc. 5- 29
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
What would you like to improve about your ability to communicate?
What aspect of your Parkinson disease bothers you the most?
Other comments:
Are there things you stopped doing because of Parkinson disease (e.g., work activities, volunteer activities, leisure
activities, exercises, etc.?)
Why? Because of problems with Moving, Speaking, Motivation? Explain:
What are your interests and hobbies?:
_____________________________________________________________________________________
_____________________________________________________________________________________
Copyright© 2012 LSVT Global, Inc. 5- 30
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
LSVT® LOUD Evaluation Protocol (This protocol can be used both pre and post treatment)
Task 1: Maximum Duration of Sustained Vowel Phonation
Direction: “Say ‘ah’ for as long as you can at a comfortable pitch and loudness.”
Comment on: Loudness, quality and duration.
Record: Duration (seconds) and sound pressure level (SPL) throughout the vowel.
SPL Meter to Mouth Distance:
Duration (sec) dB SPL
1.
2.
3.
4.
5.
6.
Comments: ____________________________________________________________________
_______________________________________________________________________________
Average sec range sec Average dB range dB
Copyright© 2012 LSVT Global, Inc. 5- 31
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
Task 2: Maximum Fundamental Frequency Range
Direction: “Try to reach your highest pitch while saying ‘ah’.”
(clinician can model high “ah”)
Comment on: Pitch, loudness and quality
Record: Highest frequency (Hertz) reached, or musical note and octave from digital tuner
1. 4.
2. 5.
3. 6.
Highest pitch: Pitch range:
Comments: ____________________________________________________________
______________________________________________________________________
Direction: “Try to reach your lowest pitch while saying ‘ah’.”
(clinician can model low “ah”)
Comment on: Pitch, loudness and quality
Record: Lowest frequency (Hertz) reached
1. 4.
2. 5.
3. 6.
Lowest pitch: Pitch range:
Comments: ____________________________________________________________
______________________________________________________________________
Copyright© 2012 LSVT Global, Inc. 5- 32
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
Task 3: Reading of a passage (e.g., “Rainbow Passage”)
Direction: “Read this passage aloud in a comfortable pitch and loudness.”
Comment on: Pitch variability, loudness, voice quality, articulation, rate, prosody, stress.
Record: Sound pressure level (SPL) through the reading.
Sound Level Meter to Mouth Distance:
SPL
Comments:
Copyright© 2012 LSVT Global, Inc. 5- 33
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
Task 4: Conversation Monologue
Direction: ““I would like you to tell me about a time you felt extremely happy. I would
like you to recall a time that you felt this emotion with great intensity. Try to
remember and actually relive a time that you felt extremely happy. Put
yourself back into the situation and try to re-experience it with as much real
feeling and intensity as when it actually occurred. Take a moment and think
about such as situation and let me know when you are ready.”
When person is ready…
“Please speak for at least 90 seconds.”
Comment on: Pitch variability, loudness, voice quality, articulation, rate, prosody, stress.
Record: Sound pressure level (SPL) through the reading.
Sound Level Meter to Mouth Distance:
SPL
Comments:
Copyright© 2012 LSVT Global, Inc. 5- 34
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
Task 5: Generate Words
Direction: “In this next task, you will be asked to come up with words beginning with
certain letters. I will tell you a letter of the alphabet and I want you to think
of words that begin with that particular letter. You may say any words at all,
except proper names such as the names of people or places. For example if I
say M, you could say, ‘man’, ‘monkey’, or ‘milk’, but you would not say
Mary, Macy's or Minneapolis. Also, do not use the same word again with a
different ending, such as ‘eat’ and then ‘eating’.
“I will now give you a letter. Say as many words that you can think of that
start with that letter. Remember no names of people or places, just ordinary
words. If you draw a blank it's OK, just sit quietly and wait until you think
of another word. You will have 60 seconds for each letter.
The first letter is F.”
Comment on: Loudness, voice quality and intelligibility
Record: SPL from sound level meter as they name words.
Sound Level Meter to Mouth Distance:
SPL
F.
A.
S.
Comments:
Copyright© 2012 LSVT Global, Inc. 5- 35
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
Task 6: Describe a Motor Task while completing a Dual Motor Activity
Direction: “Describe for me a motor task. Describe it as if I have never heard anything
about such a task or the tools involved. For example, tell me how you log
onto the Internet, swing a golf club, or make chocolate chip cookies.
Remember to tell me in very detailed terms how to complete this task.”
At the same time, have the patient simultaneously complete a motor task.
For example, 1) have the patient screw a nut on a bolt continuously while
speaking; or 2) have the patient continuously tap his or her leg while
speaking. Any distracting motor task is acceptable. The goal is to be sure
the patient does not stop the motor task or speaking; rather, he or she keeps
continuous dual activity (speaking and moving simultaneously).
Comment on: Loudness, voice quality and intelligibility
Record: SPL from sound level meter
Sound Level Meter to Mouth Distance:
SPL
Comments:

Copyright© 2012 LSVT Global, Inc. 5- 36
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
Task 7: Stimulability Testing
Direction: Have the patient produce the following voice and speech stimuli while cueing
increased loudness. Be sure to use a model, “Do what I do.”
Comment on: For all stimulability tasks, comment on the patient’s ability to increase phonatory effort,
loudness and any changes heard in voice quality, intelligibility, articulation, inflections.
Sustained Vowel Phonation “AH”
Direction: “Say ‘ah’, but make this ‘ah’ LOUD like me”
(Clinician models an “ah” with increased loudness and good quality. If
necessary, help patient shape voice, i.e., pushing, open mouth, etc)
Record: Sound pressure level (SPL),
Sound Level Meter to Mouth Distance:
Duration (sec) dB SPL
1.
2.
3.
Does the voice improve in loudness and quality? __________________
What technique works best for shaping a good quality loud AH voice? _____________________
Comments and/or Concerns:
Copyright© 2012 LSVT Global, Inc. 5- 37
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
Maximum High and Low Phonation
Directions: “Try to reach your highest pitch while saying ‘AH’ LOUD, like me”
(Clinician demonstrates. If necessary, help patient shape voice, i.e. pushing, open mouth)
Comment on: Pitch, loudness and quality
Record: Highest frequency (Hertz) reached or musical note and octave (if using
orchestral tuner)
1.
2.
3.
Directions: “Try to reach your lowest pitch while saying ‘AH’ LOUD, like me”
(Clinician demonstrates. If necessary, help patient shape voice, i.e. pushing, open mouth)
Comment on: Pitch, loudness and quality
Record: Highest frequency (Hertz) reached or musical note and octave (if using
orchestral tuner)
1.
2.
3.
Does the voice improve in loudness and quality? ____________________________________
What technique works best for shaping good quality loud High/Low pitches? _______________
Comments and/or Concerns:
Copyright© 2012 LSVT Global, Inc. 5- 38
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
Functional Phrases
Directions: “Repeat these words after me in a loud voice”
Comment on: Vocal loudness and quality, intelligibility
Record: Sound pressure level
(Clinician may choose additional words/phrases that are the most functional for the patient.)
Sound Level Meter to Mouth Distance:
1. Hello 5. Goodbye
2. Yes 6. No
3. I don’t know 7. How are you?
4. Thank you 8. You are welcome
Do voice and speech improve in loudness, intelligibility and voice quality?
Comments and/or Concerns?
ADDITIONAL INFORMATION
Laryngeal Exam Scheduled for:
Current communication situation and potential role of LSVT/LOUD?
Patient’s response to “LOUD” voice:
RECOMMENDATIONS:
Copyright© 2012 LSVT Global, Inc. 5- 39
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
LSVT® LOUD Follow-up Questions
(This protocol can be used post treatment)
Identifying Information
Name: email address:
Address:
City: State: Zip:
Phone: Fax: Age: Date of Birth:
Date and Time of Day of Initial Interview:
Diagnosis/Stage: Date of Initial Diagnosis:
Time of Last Park med: Time of Next Park med:
Neurologist: Phone:
Address:
Neurosurgeon: Phone:
Address:
Otolaryngologist: Phone:
Address:
Physical Therapist: Phone:
Address:
Copyright© 2012 LSVT Global, Inc. 5- 40
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
The following questions can be asked post-treatment and in follow-up sessions:
Voice and Speech Information
Since you completed treatment, have you noticed changes in your speech and/or voice?
If yes, please describe those changes.
Have other people commented that it is easier to understand you now?
What have they said?
Do people ask you to repeat?
Do people have a hard time understanding you?
When do you want to be as easy to understand as possible? What do you do?
How often do you do that?
Do you do more talking since you completed treatment?
How much more?
Why?
What percent of your speech do you think is intelligible (i.e., people can understand you)?
Have you been practicing?
How often?
Copyright© 2012 LSVT Global, Inc. 5- 41
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
What do you do when you practice?
Does it help?
Swallowing Information
Have you noticed any changes with eating, chewing and/or swallowing:
If yes, please describe:
Medical Information
Has your medication changed in any way in the last six months?
If yes, please describe how it has changed?
Has your Parkinson disease changed in any way in the last six months?
If yes, please describe what has changed?

Copyright© 2012 LSVT Global, Inc. 5- 42
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
Perceptual Rating Form
Client: Date: Relation to Client:
Please mark the place on the line that best represents the client’s typical speech:
Always loud enough Never loud enough
Never a “shaky” voice Always a “shaky” voice
Never a hoarse Always a hoarse
“scratchy” voice “scratchy” voice
Never monotone Always monotone
Never Slurs Always Slurs
Never a “strained” voice Always a “strained” voice
Never mumbles Always mumbles
Always Speaks so Never Speaks so
others can understand others can understand
Always Participates Never Participates
In a Conversation In a Conversation
Always Starts A Never Starts A
Conversation Conversation

Copyright© 2009 LSVT Global, LLC 5- 43
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
Voice Handicap Index (VHI) (Jacobson, Johnson, Grywalski, Silbergleit, Jacobson, Benninger, & Newman (1997). The Voice Handicap Index (VHI). American Journal of Speech Language
Pathology, 6, 66-70.)
Name:
Date: Session:
Instructions: These are statements that many people have used to describe their voices and the effects of their voices on their lives.
Check the response that indicates how frequently you have the same experience.
Never Almost
Never
Sometimes Almost
Always
Always
F1 My voice makes it difficult for people to hear me
P2 I run out of air when I talk
F3 People have difficulty understanding me in a noisy room
P4 The sound of my voice varies throughout the day
F5 My family has difficulty hearing me when I call them throughout the house
F6 I use the phone less often than I would like
E7 I’m tense when talking with others because of my voice
F8 I tend to avoid groups of people because of my voice
E9 People seem irritated with my voice
P10 People ask, “What’s wrong with your voice?”
F11 I speak with friends, neighbors or relatives less often because of my voice
F12 People ask me to repeat myself when speaking face-to-face
P13 My voice sounds creaky and dry
P14 I feel as though I have to strain to produce voice
Copyright© 2009 LSVT Global, LLC 5- 44
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
Never Almost
Never
Sometimes Almost
Always
Always
E15 I find other people don’t understand my voice problem
F16 My voice difficulties restrict my personal and social life
P17 The clarity of my voice is unpredictable
P18 I try to change my voice to sound different
F19 I feel left out of conversations because of my voice
P20 I use a great deal of effort to speak
P21 My voice is worse in the evening
F22 My voice problem causes me to lose income
E23 My voice problem upsets me
E24 I am less out-going because of my voice problem
E25 My voice problem makes me feel handicapped
P26 My voice “gives out” on my in the middle of speaking
E27 I feel annoyed when people ask me to repeat
E28 I feel embarrassed when people ask me to repeat
E29 My voice makes me feel incompetent
E30 I’m ashamed of my voice problem
Please circle the word that matches how you feel your voice is today: Normal Mild Moderate Severe
P Scale __________ F Scale __________ E Scale __________ Total __________
Copyright© 2009 LSVT Global, LLC 5- 45
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
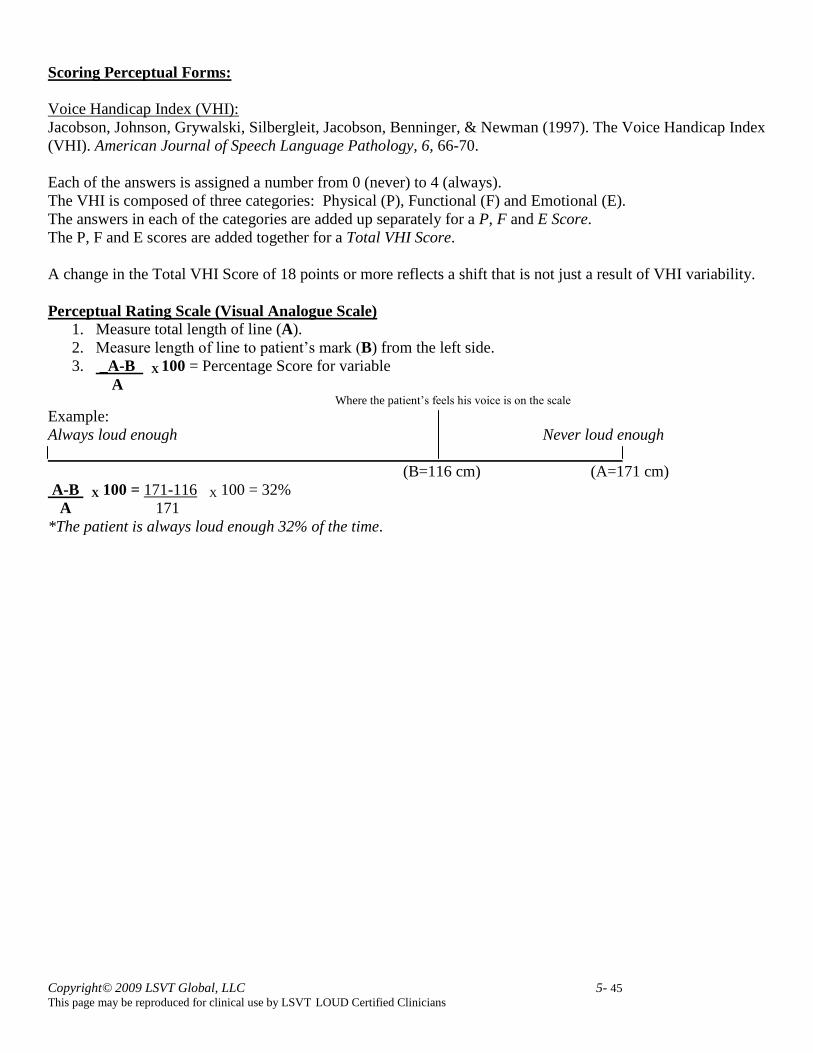
Scoring Perceptual Forms:
Voice Handicap Index (VHI):
Jacobson, Johnson, Grywalski, Silbergleit, Jacobson, Benninger, & Newman (1997). The Voice Handicap Index
(VHI). American Journal of Speech Language Pathology, 6, 66-70.
Each of the answers is assigned a number from 0 (never) to 4 (always).
The VHI is composed of three categories: Physical (P), Functional (F) and Emotional (E).
The answers in each of the categories are added up separately for a P, F and E Score.
The P, F and E scores are added together for a Total VHI Score.
A change in the Total VHI Score of 18 points or more reflects a shift that is not just a result of VHI variability.
Perceptual Rating Scale (Visual Analogue Scale)
1. Measure total length of line (A).
2. Measure length of line to patient’s mark (B) from the left side.
3. _A-B X 100 = Percentage Score for variable
A Where the patient’s feels his voice is on the scale
Example:
Always loud enough Never loud enough
(B=116 cm) (A=171 cm)
A-B X 100 = 171-116 X 100 = 32%
A 171
*The patient is always loud enough 32% of the time.
Copyright© 2009 LSVT Global, LLC 5- 46
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
LSVT
® LOUD
Treatment Packet Daily Treatment Forms
Functional Phrases Form Think LOUD sign Homework Forms
Homework Recommendations Sample functional words/phrases for hierarchy
practice
Copyright© 2009 LSVT Global, LLC 5- 47
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
LSVT® LOUD Voice Treatment Daily Tasks Treatment Forms
Name: Date: Session #:
Time: Time of Most Recent Meds: Next Meds:
Sound Level Meter Distance to Mouth:
Daily Task #1: Maximum duration of sustained “ah” phonation measured in seconds and decibels of sound
pressure level (dB SPL). Record SPL throughout the “ah” phonation.
Seconds dB SPL
1.
________________________________________________________________________
2.
________________________________________________________________________
3.
________________________________________________________________________
4.
________________________________________________________________________
5.
________________________________________________________________________
6.
________________________________________________________________________
7.
________________________________________________________________________
8.
________________________________________________________________________
Copyright© 2009 LSVT Global, LLC 5- 48
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
9.
________________________________________________________________________
10.
_______________________________________________________________________
11.
_______________________________________________________________________
12.
_______________________________________________________________________
13.
_______________________________________________________________________
14.
_______________________________________________________________________
15.
_______________________________________________________________________
Daily Average in Seconds: Daily Average in dB SPL:
Range: Range:
Perceived level of effort:
Cues for Loudness: Maximum Moderate Minimal None
SPL in response to “off the cuff” questions: _________________________________________________
Copyright© 2009 LSVT Global, LLC 5- 49
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
Daily Task #2: Maximum fundamental frequency range measured in Hz, or musical note and octave.
Highest Pitch:
1. 2. 3. 4. 5. 6.
7. 8. 9. 10. 11. 12.
13. 14. 15.
Highest Pitch Daily Average:
Lowest Pitch:
1. 2. 3. 4. 5. 6.
7. 8. 9. 10. 11. 12.
13. 14. 15.
Lowest Pitch Daily Average:
Perceived level of effort:
Cues for Loudness: Maximum Moderate Minimal None
Cues for Pitch: Maximum Moderate Minimal None
SPL in response to “off the cuff” questions: ________________________________________
Copyright© 2009 LSVT Global, LLC 5- 50
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
Daily Task #3: Maximum speech loudness drill of functional phrases. Record SPL values.
1. 1. 1. 1. 1.
2. 2. 2. 2. 2.
3. 3. 3. 3. 3.
4. 4. 4. 4. 4.
5. 5. 5. 5. 5.
6. 6. 6. 6. 6.
7. 7. 7. 7. 7.
8. 8. 8. 8. 8.
9. 9. 9. 9. 9.
10. 10. 10. 10. 10.
Daily average of dB SPL: Range:
Perceived level of effort:
Cues for Loudness: Maximum Moderate Minimal None
SPL during “off the cuff” questions: ________________________________________________________
Copyright© 2009 LSVT Global, LLC 5- 51
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
Hierarchical Speech Loudness Drills: (Circle current level)
Single words/Phrases Sentences Paragraph Reading Conversation
Select reading material that is relevant and salient to the patient’s life. Periodically measure SPL during both reading
tasks and spontaneous questions.
SPL Meter to Mouth Distance:
SPL during “Reading”
_
_____________________________________________________________________________________
_____________________________________________________________________________________
Perceived level of effort:
Cues for Loudness: Maximum Moderate Minimal None
SPL during spontaneous “off the cuff” questions (when patient is not performing loudness)
Perceived level of effort:
Cues for Loudness: Maximum Moderate Minimal None
Copyright© 2009 LSVT Global, LLC 5- 52
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
COMMENTS FROM TREATMENT:
Intelligibility/Voice Quality:
Treatment:
Calibration:
Homework assignment:
Carryover assignment:
Copyright© 2009 LSVT Global, LLC 5- 53
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
LSVT® LOUD Functional Phrases Recording Form
Ten Commonly-Used Phrases/Sentences for
(1)
(2)
(3)
(4)
(5)
(6)
(7)
(8)
(9)
(10)

Copyright© 2009 LSVT Global, LLC 5- 54
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
THINK
LOUD!
Copyright© 2009 LSVT Global, LLC 5- 55
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
LSVT® LOUD Homework Recording Form
Schedule:
Complete only Set 1 on days when you have treatment in the clinic, 5-10 minutes
Complete Set 1 and Set 2 when you do not have treatment in the clinic. Complete each Set separately at
different times of the day, spending 10-15 minutes on each.
Materials:
A clock or watch with a second hand, or a digital counter
A pen or pencil
Optional: a sound level meter
Name: Date:
Time of Day: Time of last PD Medication:
DAILY TASKS:
1. Say “ah” with your loud, good quality voice for as long as you can. Try to feel the same level of effort you
did in treatment with your therapist. Record the times below or check off that you have completed the tasks.
Set 1: 1. 2. 3. 4. 5. 6.
Set 2: 1. 2. 3. 4. 5. 6.
2. Say “ah” with your loud, good quality voice and go as high as you can, hold it for 5 seconds. Try to feel
the same level of effort you did in treatment with your therapist. Place a check on each line as you complete
the task.
Set 1: 1. 2. 3. 4. 5. 6.
Set 2: 1. 2. 3. 4. 5. 6.
3. Say “ah” with your loud, good quality voice and go as low as you can, hold it for 5 seconds. Try to feel the
same level of effort you did in treatment with your therapist. Place a check on each line as you complete the
task.
Set 1: 1. 2. 3. 4. 5. 6.
Set 2: 1. 2. 3. 4. 5. 6.
Copyright© 2009 LSVT Global, LLC 5- 56
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
4. Read aloud from your list of 10 functional phrases and sentences using your loud, good quality voice that
you learned in treatment. Check each line as you complete the phrase or sentences.
Set 1: Set 2:
1. 1.
2. 2.
3. 3.
4. 4.
5. 5.
6. 6.
7. 7.
8. 8.
9. 9.
10. 10.
5. Complete practice at the level circled and check when completed. Use materials provided by your
therapist or favorite reading material you have at home.
Single words/Phrases Sentences Paragraph Reading Conversation
Do you feel like you used the same level of effort (e.g., LOUDNESS) as you do with your therapist?
What was your perceived effort level?
6. Carryover Assignment: Remember to feel AS LOUD as you do in the therapy room when you complete
this assignment.
Copyright© 2009 LSVT Global, LLC 5- 57
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
LSVT®/LOUD HOMEWORK RECOMMENDATIONS FOLLOWING THERAPY
Continue to do structured practice sessions 10-15 minutes everyday. Determine the time
and place that works well for you, and maintain that schedule. I will practice: .
It is important to keep practicing, this will keep your new strong voice in shape.
Materials:
a clock or watch with a digital second hand
a pen or pencil
optional: a sound level meter
Daily Tasks:
6 – 10 “AH’s”. Say “AH” using your LOUD, good quality voice as LONG as you can.
Think about being LOUD and try to feel the same level of energy and loudness you did in
treatment with your therapist. Record your times.
6 – 10 Highs. Start with your LOUD “AH” voice and then try to reach your highest pitch and
hold it for 5 seconds.
6 – 10 Lows. Start with your LOUD “AH” voice and then try to reach your lowest pitch and hold
it for 5 seconds.
Read aloud from your list of 10 functional phrases and sentences using the LOUD voice you
learned in treatment. Repeat the list 3-5 times.
Read aloud for 5-10 minutes. Any type of reading material will do.
Remember to THINK LOUD, using the same level of energy and loudness you put into
treatment each day.
The best practice is to continue to use the new strong voice
with family and friends in conversations, on the phone,
on the street, at the grocery store, etc.
This will keep your new strong voice in shape!
Good Luck!!!!!!!

Copyright© 2009 LSVT Global, LLC 5- 58
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
Words for Speech Exercises
Yes.
No.
Help!
Thank you.
You’re welcome.
What?
OK
Good.
Not bad.
Where?
Hello.
How are you?
I’m fine.
What’s next?
Excellent!
Oops!
Good morning.
See you later.
Ready?
Let’s go.
Good bye.
I don’t know.
Not now.
Who?
Oh no.
How long?
What’s new?
Congratulations!
I guess so.
Later.
Wow!
Ouch!
Why?
Not much.
Happy Birthday!
Really?
It’s bad.
Watch out!
Good night.
Did you get it?
No thanks.
Sure.
Great.
Can I help?
What happened?
Come here.
Not now.
Where is it?

Copyright© 2009 LSVT Global, LLC 5- 59
This page may be reproduced for clinical use by LSVT LOUD Certified Clinicians
Phrases for Speech Exercise
Who is calling?
Get the phone.
You’re kidding!
It’s over there.
See you later.
You are welcome
I’m not sure.
It’s time to go.
What is available?
Are we there yet?
It’s time to take my pills.
Come here please.
Where are you going?
What’s for dinner?
I don’t feel good.
Please pass the pepper.
Could you get that?
How was your day?
Anyone call for me?
I don’t need help.
Hello, this is .
Do you want some coffee?
Where are my shoes?
What’s the weather today?
Give me the remote.
Tell them I’m not home!
Excuse me, please.
I’m good for now.
We need to stop for gas.
Have a good day.


















