Lower 3rd molar impaction,its assessment and the buccal approach vz the lingual split technique of...
41
IMPACTED LOWER IIIrd MOLAR IMPACTED LOWER IIIrd MOLAR decision making, treatment planning and decision making, treatment planning and T T HE HE L L INGUAL INGUAL S S PLIT PLIT T T ECHNIQUE ECHNIQUE Dr. Waikhom Robindro Singh Assoc. Professor Assoc. Professor DENTAL COLLEGE, RIMS DENTAL COLLEGE, RIMS
-
Upload
waikhom-singh -
Category
Healthcare
-
view
2.749 -
download
1
Transcript of Lower 3rd molar impaction,its assessment and the buccal approach vz the lingual split technique of...

IMPACTED LOWER IIIrd MOLAR IMPACTED LOWER IIIrd MOLAR decision making, treatment planning and decision making, treatment planning and
TTHE HE L LINGUALINGUAL S SPLITPLIT T TECHNIQUEECHNIQUE
Dr. Waikhom Robindro SinghAssoc. ProfessorAssoc. Professor
DENTAL COLLEGE, RIMSDENTAL COLLEGE, RIMS

Impacted toothImpacted tooth
Causes of IIIrd molar impactionCauses of IIIrd molar impaction
i. i. failure of rotation of the tooth bud from horizontal to failure of rotation of the tooth bud from horizontal to vertical during developmentvertical during development ii. lack of space in the alveolar process anterior to theii. lack of space in the alveolar process anterior to the anterior border of the ramus 3anterior border of the ramus 3rdrd molars most molars most commonly to be impacted coz they are the last to eruptcommonly to be impacted coz they are the last to erupt
Failure to erupt to its correct Failure to erupt to its correct position in the dental arch within position in the dental arch within the specified time owing to some the specified time owing to some barrier in the pathway of eruption barrier in the pathway of eruption or due to some genetic reason or due to some genetic reason
Those that fail to erupt withoutany obvious reason are typed asembedded tooth by some authors

Periodontal pocketPericoronitisCariesRoot resorptionDenture irritationCyst and tumoursUnexplained painJaw fractureOrthodontic considerationInferior Alveolar Canal
the amount of bone on the distal aspect of 2nd molar
bone loss
What is the problem? Why remove it?What is the problem? Why remove it?

Periodontal pocketPericoronitisCariesRoot resorptionDenture irritationCyst and tumoursUnexplained painJaw fractureOrthodontic considerationInferior Alveolar Canal
What is the problem? Why remove it?
d/t entrapment of food, trauma from opposing tooth and infection in the operculum.
operculum
operculitis

Periodontal pocketPericoronitisCariesRoot resorptionDenture irritationCyst and tumoursUnexplained painJaw fractureOrthodontic considerationInferior Alveolar Canal
What is the problem? Why remove it?
Food entrapement and inaccessibility to toothbrush on the distal aspect of 2nd molar

Periodontal pocketPericoronitisCariesRoot resorptionDenture irritationCyst and tumoursUnexplained painJaw fractureOrthodontic considerationInferior Alveolar Canal
What is the problem? Why remove it?

Periodontal pocketPericoronitisCariesRoot resorptionDenture irritationCyst and tumoursUnexplained painJaw fractureOrthodontic considerationInferior Alveolar Canal
What is the problem? Why remove it?
Impacted tooth beneath an edentulous area gradually becomes superficial d/t resorption of the overlying bone irritate the soft tissue beneath the denture

Periodontal pocketPericoronitisCariesRoot resorptionDenture irritationCyst and tumoursUnexplained painJaw fractureOrthodontic considerationInferior Alveolar Canal
What is the problem? Why remove it?
Follicular sac cystic degeneration
The epithelium contained within the dental follicle leads to Odontogenic T.

Periodontal pocketPericoronitisCariesRoot resorptionDenture irritationCyst and tumoursUnexplained painJaw fractureOrthodontic considerationInferior Alveolar Canal
What is the problem? Why remove it?
Pain in the retromolar region without any apparent cause

Periodontal pocketPericoronitisCariesRoot resorptionDenture irritationCyst and tumoursUnexplained painJaw fractureOrthodontic considerationInferior Alveolar Canal
What is the problem? Why remove it?
Impacted tooth occupies space
weak point in the
mandible

Periodontal pocketPericoronitisCariesRoot resorptionDenture irritationCyst and tumoursUnexplained painJaw fractureOrthodontic considerationInferior Alveolar Canal
What is the problem? Why remove it?
Prevent distal retraction of the 1st and 2nd molar during ortho treatment.
Mesially inclined impacted molar
mesial force recurrence of crowding after ortho tt.

Periodontal pocketPericoronitisCariesRoot resorptionDenture irritationCyst and tumoursUnexplained painJaw fractureOrthodontic considerationInferior Alveolar Canal
What is the problem? Why remove it?
Proximity to the nerve leading to symptoms

But why bother If surgical morbidity outweigh the benefits?
Aged
Medically compromised
Proximity to vital structure
probability of a lately discovered impacted tooth causing periodontal complications, caries, cyst n tumour is low
Highly calcified and less flexible bone
Increased surgical morbidity

But why bother If surgical morbidity outweigh the benefits?
Aged
Medically compromised
Proximity to vital structure
any medical condition which carries increased surgical risk

But why bother If surgical morbidity But why bother If surgical morbidity outweigh the benefits?outweigh the benefits?
Aged
Medically compromised
Proximity to vital structure
Too close to the Inferior Alveolar nerve

When to remove? … late teens When to remove? … late teens ideallyideally
more than 1/3 bt less than 2/3
less than 1/3
When one-third to two-third of the When one-third to two-third of the normal length of root is formed normal length of root is formed
Healthy period so less postoperative Healthy period so less postoperative morbiditymorbidity LLess chance of periodontal pocket d/t ess chance of periodontal pocket d/t more complete regeneration of bone and more complete regeneration of bone and reattachment of gingiva to adjacent toothreattachment of gingiva to adjacent tooth
Easier removal d/t flexible bone and wider Easier removal d/t flexible bone and wider periodontal ligament space in this age periodontal ligament space in this age groupgroup
Y in late teens?Y in late teens?

more than 20yrs mesial tilt positioned at the cervical level of 2nd molar covered with bone inadequate space LATE ERUPTION LIKELY less than20 yrs vertical positioned above the cervical level of the 2nd molar sufficient space covered with soft tissue/ thin layer of bone
Is it a case of impactionIs it a case of impaction or will it erupt late ?? or will it erupt late ?? LIKELY IMPACTION

Investigation n assessmentInvestigation n assessment radiographicradiographic
IOPA X-RAY
OCCLUSAL VIEW
TUBE - SHIFT TECHNIQUE
OPG
Lateral Oblique View
occlusal view
OPG
occlusal

DIFFICULTY ASSESSMENT for a systematic approach and for a proper surgical technique
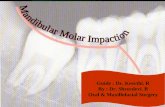
3 classification systems are correlated to determine the accessibility(ease of exposing tooth, pathway of delivery, purchase point) of the impacted tooth and hence calculate the difficulty score Winters classificationWinters classification
based on angulation of the impacted tooth
MESIOANGULAR
HORIZONTAL
VERTICAL
DISTOANGULAR
1.1.

DIFFICULTY ASSESSMENT DIFFICULTY ASSESSMENT for a systematic approach and for a proper surgical technique
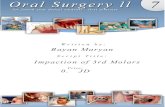
Pell & Gregory’s Class I, II & IIIPell & Gregory’s Class I, II & III
based on available space between the ant. border of ramus and distal side of 2nd molar
Pell & Gregory’s Type A, B & CPell & Gregory’s Type A, B & C based on the depth of the impacted molar with respect to the occlusal surface of the 2nd molar
2.2.
3.3.

calculatingcalculating the difficulty score: the difficulty score: impacted tooth is impacted tooth is
given a difficulty index valuegiven a difficulty index value Winter’sWinter’s Mesioangular - 1 Horizontal - 2 Vertical - 3 Distoangular - 4 Pell & Gregory’s Class I, II & IIIPell & Gregory’s Class I, II & III Class I - 1 Class II - 2 Class III - 3 Pell & Gregory’s A, B & CPell & Gregory’s A, B & C Level A - 1 Level B - 2 Level C - 3
Very difficult - 8 Very difficult - 8 to 10to 10Moderately difficult - 5 Moderately difficult - 5 to 7to 7Minimally difficult - 3 Minimally difficult - 3 to 4to 4
For eg. total difficulty score of an impacted molar with vertical angulation, at level B & under Class I category will be :
63+2+1 =

OTHER FACTORS for difficulty assessmentOTHER FACTORS for difficulty assessment
Contact with 2Contact with 2ndnd molar molar
Periodontal ligament spacePeriodontal ligament space
Size of follicular sacSize of follicular sac
Density of boneDensity of bone
Root morphologyRoot morphology
Relation with inf. Alveolar n.Relation with inf. Alveolar n.

TWO TECHNIQUES ARE PRACTISEDTWO TECHNIQUES ARE PRACTISED
BUCCAL TECHNIQUEBUCCAL TECHNIQUE
LINGUAL SPLIT TECHNIQUELINGUAL SPLIT TECHNIQUE

Flap design – similar for both the buccal and the lingual split technique
1.Triangular flap (L-shaped) Incision starts from the anterior
border of ramus the external oblique ridge distal aspect of IInd
molar Vertical release from the ant. end of
horizontal incision obliquely downwards and forward the vestibular sulcus
incision
bone
horizontal
vertical
BUCCAL TECHNIQUE
‘Depends upon the depth of the impacted tooth’

2.Variation of the triangular flap (bayonet) - Origin of incision same as triangular flap but continues as sulcular incision along
the cervical line of 2nd molar upto the 1st molar - vertical incision begin at distal aspect of 1st molar - for wider exposure in deep impaction
bone
horizontal
vertical

3. Envelope flap3. Envelope flap - begins at the ant. border of ramus distal begins at the ant. border of ramus distal aspect of 2aspect of 2ndnd molar, continue as sulcular incision molar, continue as sulcular incision along the cervical lines of last two teeth and along the cervical lines of last two teeth and ending at the mesial ending at the mesial aspect of 1aspect of 1stst molar molar -- no vertical release incisionno vertical release incision - superficial impaction- superficial impaction
bone
incision
no vertical incision

Removal of bone expose the crown expose the crown create pathway for removal. create pathway for removal. - bone is removed from the buccal n distal aspect - never lingually High speed-high torque bur High speed-high torque bur : no. 7/8 round
bur or straight fissure bur ; time consuming, bone necrosis, no need to support the mandible, may contaminate the room
Chisel - mallet Chisel - mallet : 3-5mm diam. chisel, less time consuming, no bone necrosis,
need to support the mandible for TMJ protection, inadvertent # of bone if undue force, clean technique
BONE
FROM
BUCCO
DISTAL
buccal bone
distal bone
distal bone

horizontal mesioangular distoangular
Tooth SectioningTooth Sectioning: : provides less bone removal small dead space; provides less bone removal small dead space; bur or chisel; only 1/2 the diam. sectioned n then fractured by elevatorbur or chisel; only 1/2 the diam. sectioned n then fractured by elevator
TOOTH SECTIONING USUALLY TOOTH SECTIONING USUALLY REQUIREDREQUIRED

Elevation of the toothElevatorsWinter Cryer’s elevator wedging action buccal elevation
Coupland St. elevator mesially at the base of the crown between the tooth and alveolar bone
luxation by distal rotation
elevating the tooth in a superior and distal direction
cryer elevation
coupland luxation
coupland elevation

Removal of follicular remnants
prevent cysts or tumours
follicle
peri-apical currette or
hemostat is used

After debridement , smoothening of bone margins and irrigation
with normal saline,
3 to 4 simple interrupted sutures given
3-0 black silk; reverse cutting needle used
Start at the distal aspect of 2nd molar to
provide watertight seal n prevent pocket
1st suture
SUTURESUTURE

TTHEHE L LINGUALINGUAL S SPLITPLIT T TECHNIQUEECHNIQUE Meant for removal of the impacted lower 3rd molar. most types but is usually suitable for lingually placed impaction; not in bucco-version 1st introduced by Sir William Kelsey FrySir William Kelsey Fry popularised by Terence WardTerence Ward Prof. R . Pradhan Prof. R . Pradhan is a major exponent of this technique in India. Purely a chisel - mallet technique
less surgical timeless surgical time PT. COMFORT LESS OEDEMA
To remove the portion of the lingual plate covering the impacted molar lingual pathway push the tooth lingually in toto Tooth sectioning not required The thin lingual cortical bone is chiseled in a piece instead of multiple chipping of the thick buccal plate
Rationale no. IRationale no. I

Rational no. II Rational no. II
Removal of lingual plate no socket close adaptation of vascular lingual flap
NO DEAD SPACE
PROPER HEALING [NO DRY SOCKET]
no socket

Muco-periosteal flap similar to buccal technique
1.Triangular (L-shaped) 2.Modified triangular (Bayonet) 3.Envelope flap
The techniqueThe technique
Fully covered toothFully covered tooth
Triangular incisionTriangular incision
Exposure of boneExposure of bone
Bone ExposureBone Exposure

1.1. Mandible support for Mandible support for TMJ protection TMJ protection
2. Vertical stop cut (5 to 6 mm ht.) placed 2. Vertical stop cut (5 to 6 mm ht.) placed distal to the 2distal to the 2ndnd molar - bevel of the molar - bevel of the chisel (3-5mm) facing posteriorly. chisel (3-5mm) facing posteriorly. 3. Oblique horizontal cut made backward 3. Oblique horizontal cut made backward from the lower end of the vertical limiting from the lower end of the vertical limiting cut – post. limit of the cut being distal cut – post. limit of the cut being distal aspect of the impacted crownaspect of the impacted crown 4. Buccal bone plate removed above the 4. Buccal bone plate removed above the horizontal cut to expose the crownhorizontal cut to expose the crown
5. Purchase point prepared by removing a 5. Purchase point prepared by removing a gular piece of bonegular piece of bone
Bone RemovalBone Removal : : to expose the crown and to remove to expose the crown and to remove
the obstruction to pathway for removalthe obstruction to pathway for removal
vertical stop cut
horizontal cut
Mandible support

The splitThe split
6. Fracture of the distolingual bone - the the lingual splitlingual split
Split lingual plate removed after detaching the periosteal attachment to expose the lingual aspect of the tooth
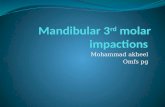
CHISEL POSITIONCHISEL POSITION Chisel placed at middle of the distal aspect of 2nd molar crown. Bevel of the chisel is upward.Cutting edge of chisel parallel to the external oblique ridge;Axis of the chisel at 45o the bone surface. Angulation of chisel depends upon the depth of the tooth; more depth require more angulation towards the vertical.
Chisel position4 ling. splitChisel position4 ling. split

Tooth Elevation:Tooth Elevation: The Coupland st. elevator is usedThe Coupland st. elevator is used Elevator placed between the mesial aspect Elevator placed between the mesial aspect of the impacted tooth and the alveolar bone of the impacted tooth and the alveolar bone and rotated distally for luxationand rotated distally for luxation
The tooth is pushed upward, backwards and The tooth is pushed upward, backwards and more lingually with minimum force. more lingually with minimum force. Tooth easily displaced lingually as Tooth easily displaced lingually as lingual plate is removedlingual plate is removed
DISTALLYDISTALLY
LINGUALLYLINGUALLY
SUPERIORLYSUPERIORLY

curette
stitchstitch
1. Socket eliminated
2. Peri-apical currete for debridement3. Normal saline irrigation for lavage n
decontamination4. Bone margins rounded5. Suturing by 3-0 black silk. Vertical
incision may be left unsutured for drainage
Post removalPost removalNo socketNo socket
curretecurrete
irrigationirrigation

ComplicationsComplications
PainPainSwellingSwelling - moderate swelling is part of normal responseTrismusTrismus - inflammatory inv. of m. of mastication ; multiple injections in Med. Ptygoid. M. ; damage to temporalis attachment.Dry socketDry socket - moderate to intense pain without swelling; pain increasing on 3rd or 4th dayParesthesiaParesthesia - in lower lip due to injury of the inf. alv n. ; in lingual split technique numbess of tongue d/t lingual n injury is a significant risk Jaw fractureJaw fracture - undue force of malletBone necrosisBone necrosis - bur techniqueLoss of vitality of adjacent toothLoss of vitality of adjacent tooth - injudicious bone cutting n use of elevatorTMJ affliction TMJ affliction - internal derangement meniscus athralgia n clicking

Lingual split Buccal technique
No dry socket
Dry socket
time consuming - thick buccal bone n tooth sectioning
Less time consuming no tooth sectioning
Lingual nerve
No bone necrosis
Less swelling
More pain d/t damage to lingual periosteum
Clean technique; no bur
Need practice
Bone necrosis
Chances nil
Bur may spray blood n bony particles
More swelling
Less pain
Easier

Bone belongs to the patient and tooth belongs to the surgeonBone belongs to the patient and tooth belongs to the surgeon
CONCLUSIONCONCLUSION
Prefer the technique most comfortable to youPrefer the technique most comfortable to you
Proper assessment of the case for Proper assessment of the case for tissue preservation and rapid removal tissue preservation and rapid removal of the tooth is empirical of the tooth is empirical
Lingual split technique requires Lingual split technique requires expertise but is an important expertise but is an important addition to our armamentariumaddition to our armamentarium