Low-grade gliomas in adults
14
Low-Grade Gliomas in Adults Sandeep Mittal, MD, FRCSC Mark C. Szlaczky, PharmD Geoffrey R. Barger , MD Corresponding author Geoffrey R. Barger, MD Department of Neurology, Karmanos Cancer Institute, Wayne State University, 4201 St. Antoine, Suite 8D, Detroit, MI 48201, USA. E-mail: [email protected] Current Treatment Options in Neurology 2008, 10: 271–284 Current Medicine Group LLC ISSN 1092-8480 Copyright © 2008 by Current Medicine Group LLC Opinion statement Making treatment decisions for patients with infiltrating low-grade gliomas (LGGs) is challenging. Patients frequently present with seizures and usually have little or no neurologic deficit. In this younger and relatively well patient population, despite the potential for significant morbidity, we believe that surgical resection, radiation therapy, and chemotherapy each play an important role in the optimal manage- ment of these tumors. Randomized clinical trials have begun to address some of the many questions about prognosis, natural history, and treatment, but most questions have yet to be answered. We believe that, when possible, a maximal surgical resec- tion consistent with preservation of neurologic function should be performed, even though it is likely that no randomized clinical trial will ever be done to demonstrate a survival advantage for this approach. External beam radiation therapy is most often given to a total dose of 50.4 or 54 Gy in 1.8-Gy fractions. The role of chemotherapy is less certain, but a growing body of evidence suggests that temozolomide, a gen- erally well-tolerated drug, is active in the treatment of LGGs. In recent years, loss of heterozygosity of chromosome 1p and 19q, as well as silencing of the MGMT gene, have been identified as promising predictors of response to adjuvant therapy in gliomas. Although randomized trials have not yet shown a survival benefit for early radiation therapy or chemotherapy, one study by the European Organisation for Research and Treatment of Cancer did show an improvement in time to tumor progression with the earlier use of radiation therapy. In addition, a trial by the Radi- ation Therapy Oncology Group (soon to be analyzed and reported) is comparing radiation alone with radiation followed by a year (six cycles) of standard-dose PCV chemotherapy (procarbazine, CCNU, and vincristine); this trial may shed light on the use of chemotherapy in conjunction with radiation therapy for the initial treat- ment of LGGs. Because patients remain at risk for tumor progression for the re- mainder of their lives, we recommend lifelong follow-up with MRI scans, even for patients without documented tumor regrowth over long intervals. To give clinicians a more solid basis for guiding therapy recommendations, we encourage participa- tion in large cooperative group clinical trials. Introduction Tumors of the central nervous system (CNS) are grouped according to their cell of origin and are graded based on standard histopathologic features. Gliomas comprise a heterogeneous group of neuroectodermal tumors that arise from the glia, the supporting cells of the CNS, and have distinct clinical, histologic, and molecular charac- teristics. The World Health Organization (WHO) classi- fication, the most commonly accepted grading system for brain tumors, classifies tumors by predominant cell type and grade. The histologic grading of gliomas takes into account nuclear atypia, cellularity, mitotic activity, endo- thelial proliferation, necrosis, and proliferation index [1,
-
Upload
sandeep-mittal -
Category
Documents
-
view
224 -
download
2
Transcript of Low-grade gliomas in adults

Low-Grade Gliomas in Adults Sandeep Mittal , MD, FRCSC Mark C. Szlaczky , PharmD Geoffrey R. Barger , MD Corresponding author Geoffrey R. Barger, MD Department of Neurology, Karmanos Cancer Institute, Wayne State University, 4201 St. Antoine, Suite 8D, Detroit, MI 48201, USA.E-mail: [email protected]
Current Treatment Options in Neurology 2008, 10: 271– 284 Current Medicine Group LLC ISSN 1092-8480 Copyright © 2008 by Current Medicine Group LLC
Opinion statement Making treatment decisions for patients with infi ltrating low-grade gliomas (LGGs) is challenging. Patients frequently present with seizures and usually have little or no neurologic defi cit. In this younger and relatively well patient population, despite the potential for signifi cant morbidity, we believe that surgical resection, radiation therapy, and chemotherapy each play an important role in the optimal manage-ment of these tumors. Randomized clinical trials have begun to address some of the many questions about prognosis, natural history, and treatment, but most questions have yet to be answered. We believe that, when possible, a maximal surgical resec-tion consistent with preservation of neurologic function should be performed, even though it is likely that no randomized clinical trial will ever be done to demonstrate a survival advantage for this approach. External beam radiation therapy is most often given to a total dose of 50.4 or 54 Gy in 1.8-Gy fractions. The role of chemotherapy is less certain, but a growing body of evidence suggests that temozolomide, a gen-erally well-tolerated drug, is active in the treatment of LGGs. In recent years, loss of heterozygosity of chromosome 1p and 19q, as well as silencing of the MGMT gene, have been identifi ed as promising predictors of response to adjuvant therapy in gliomas. Although randomized trials have not yet shown a survival benefi t for early radiation therapy or chemotherapy, one study by the European Organisation for Research and Treatment of Cancer did show an improvement in time to tumor progression with the earlier use of radiation therapy. In addition, a trial by the Radi-ation Therapy Oncology Group (soon to be analyzed and reported) is comparing radiation alone with radiation followed by a year (six cycles) of standard-dose PCV chemo therapy (procarbazine, CCNU, and vincristine); this trial may shed light on the use of chemotherapy in conjunction with radiation therapy for the initial treat-ment of LGGs. Because patients remain at risk for tumor progression for the re-mainder of their lives, we recommend lifelong follow-up with MRI scans, even for patients without documented tumor regrowth over long intervals. To give clinicians a more solid basis for guiding therapy recommendations, we encourage participa-tion in large cooperative group clinical trials.
Introduction Tumors of the central nervous system (CNS) are grouped according to their cell of origin and are graded based on standard histopathologic features. Gliomas comprise a heterogeneous group of neuroectodermal tumors that arise from the glia, the supporting cells of the CNS, and have distinct clinical, histologic, and molecular charac-
teristics. The World Health Organization (WHO) classi-fi cation, the most commonly accepted grading system for brain tumors, classifi es tumors by predominant cell type and grade. The histologic grading of gliomas takes into account nuclear atypia, cellularity, mitotic activity, endo-thelial proliferation, necrosis, and proliferation index [ 1 ,

272 Neuro-oncology (Neoplasms)
Class III]. All WHO grade I and grade II gliomas are con-sidered to be low-grade tumors ( Table 1 ). However, the clinical presentation, location, natural history, histologic and molecular characteristics, and response to treatment of these low-grade glial tumors are very diverse. The most numerous (and perhaps most troublesome) of these neoplasms are the WHO grade II oligodendrogliomas, oligoastrocytomas, and astrocytomas. They are the only low-grade tumors that have been systematically studied in randomized clinical trials in adults. Unless otherwise specifi ed, the term low-grade glioma (LGG) in this article refers to these infi ltrating, WHO grade II, supratentorial oligodendrogliomas, oligoastrocytomas, and astrocyto-mas in adults. These supratentorial, non–optic pathway tumors have similar invasive and malignant potential and are the focus of this review. Most modern series report a longer median survival in patients with WHO grade II oli-godendrogliomas than in patients with low-grade astro-cytomas [ 2 , Class III]. The reported outcome of patients with mixed oligoastrocytomas falls between the outcomes with pure oligodendrogliomas and astrocytomas.
EPIDEMIOLOGY LGGs constitute only a small subset of gliomas, the most common type of primary brain tumors. LGGs occur more commonly in men and whites and typically develop in patients at a younger age than high-grade gliomas. Cur-rently, no major risk factors for the development of LGGs have been identifi ed. A leading hypothesis is a yet-to-be identifi ed perturbation in the immune system [ 3 , Class III]. LGGs in adults are most commonly located along the cere-bral convexity in corticosubcortical areas. Compared with high-grade gliomas, LGGs have a predilection for eloquent and “secondary” functional areas including the sensorimo-
tor cortex, insula and subinsular region, and supplementary motor area [ 4 , Class III]. Adult patients infrequently pres-ent with LGGs originating in the cerebellum, brainstem, or spinal cord. Although these tumors are more common in patients with neurofi bromatosis and Li-Fraumeni syndrome, hereditary factors do not appear to play an important role in development of LGGs [ 5 , Class III].
CLINICAL PRESENTATION LGGs produce signs and symptoms through three main mechanisms: direct infi ltration and destruction of neuro-nal populations, local pressure from peritumoral edema, and intracranial hypertension from mass effect or ven-tricular obstruction. In many cases, the insidious onset of the presenting symptoms delays the diagnosis for months or years. The most common presenting symptom is sei-zures, which occur in up to 90% of patients [ 6 , Class III; 7 , Class I]. This high rate may be the result of frequent involvement of the cerebral cortex by these low-grade infi ltrative tumors. At the time of presentation, cognitive and behavioral changes are present in about 10% to 15% of patients, and 10% have signs of increased intracranial pressure, such as headache, nausea, and papilledema. Focal neurologic defi cits such as paresis or sensory loss are present in up to one third. The incidence of signifi -cant neurologic defi cits and raised intracranial pressure appears to be declining, however, as modern neuroimag-ing techniques allow diagnosis of the lesion at a much earlier stage. In fact, a normal neurologic examination is not uncommon in patients with LGGs [ 6 , Class III].
NEUROIMAGING FINDINGS Diagnostic neuroimaging assists in preoperative differ-ential diagnosis, localization for operative planning, and
Table 1. World Health Organization (WHO) classifi cation of low-grade gliomas
Grade Astrocytic Oligodendroglial Mixed Ependymal Other
neuroepithelial
Grade I Pilocytic astrocytoma,
subependymal giant-cell
astrocytoma (SEGA)
– Desmoplastic infan-tile astrocytoma (DIA) and gan-
glioglioma (DIG), ganglioglioma,
dysembryoplastic neuroepithelial tumor (DNT),
papillary glioneuronal tumor,
rosette-forming glioneuronal tumor of the
fourth ventricle
Subependymoma, myxopapillary ependymoma
Angiocentric glioma
Grade II Diffuse astrocytoma, pleomorphic
xanthoastrocy-toma, pilomyxoid
astrocytoma
Oligodendroglioma Oligoastrocytoma, cerebellar
liponeurocytoma
Ependymoma Chordoid glioma of the third ventricle

Low-Grade Gliomas in Adults Mittal et al. 273
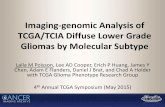
surveillance for response to therapy and tumor progres-sion. LGGs characteristically involve the white matter but also invade gray matter. On contrast-enhanced CT scans, LGGs typically appear as a heterogeneous region of low attenuation that generally does not enhance. Calcifi ca-tions are seen in up to 20% of oligodendrogliomas but are less common in astrocytomas. On MRI, LGGs com-monly cause mild expansion of the affected brain; they are usually nonenhancing, with low signal intensity on T1 and high signal intensity on T2 and fl uid-attenuated inversion recovery (FLAIR) sequences ( Fig. 1 ). There is generally little surrounding vasogenic edema and mass effect on adjacent structures. Areas of calcifi cations may appear as foci of high T1 and low T2 signals [ 8 , Class III]. FLAIR images frequently reveal the greatest contrast between the tumor margin and brain parenchyma. How-ever, these neoplasms are also highly infi ltrative, and there is invariably microscopic invasion into the surrounding “normal” brain beyond the radiographic border of the tumor. The presence of contrast enhancement on CT or MR imaging is not consistently associated with a higher incidence of tumor progression or a lower rate of patient survival [ 9 , Class III], but development of new contrast enhancement in a previously nonenhancing tumor should always raise suspicion of progression to a higher grade [ 10 , Class III]. Comparison of the most recent MRI scan with not only the most recent previous scan but also at least one remote scan can help with earlier discovery of subtle tumor progression.
Other neuroimaging techniques such as MR spectros-copy, diffusion tensor imaging, perfusion imaging, single-photon emission tomography (SPECT), and positron emission tomography (PET) can sometimes assist with the initial diagnosis, optimal management, and long-term follow-up and treatment of patients with LGGs [ 8 , 10 , 11 ,
Class III]. These advanced metabolic and molecular imag-ing modalities have improved the accuracy and sensitivity of imaging-based diagnosis and grading of gliomas [ 12 , Class III]. However, these techniques are still associated with signifi cant error rates and do not obviate the need for tumor sampling and histopathologic confi rmation. Histopathologic evaluation of tumor tissue by an expe-rienced neuropathologist continues to be the method of choice for diagnosing and classifying gliomas.
NEUROPATHOLOGIC EVALUATION A formal review of the patient’s tumor tissue histopathol-ogy by a neuropathologist skilled in grading gliomas is essential to optimal care. Equally important is access to a neuropathologist who can provide reliable interpretation of tumor samples during surgery. At times, critical deci-sions regarding the extent of surgical resection require accurately identifying tumoral versus nontumoral tissue and determining whether anaplastic features are present in the specimen. It is also important to recognize whether an oligodendroglial component is present because of the treatment-related survival advantage afforded to patients with oligodendrogliomas and oligoastrocytomas. We believe that when neuropathologists became aware that oligodendroglial tumors were more sensitive to treatment than astrocytomas, they became more diligent in assessing tumoral specimens for the presence of an oligodendrog-lial component. This diligence may partially explain the apparent rise in the incidence of oligodendroglial tumors over the past two decades [ 2 , Class III].
IMMUNOHISTOCHEMICAL MARKERS Astrocytomas are immunoreactive for glial fi brillary acidic protein (GFAP), vimentin, and S-100 protein. Oligo-dendrogliomas have a uniform population of cells with
Figure 1 . Typical MRI scan of a low-grade glioma (histopathologically, a WHO grade II oligodendroglioma). A, Preoperative T2-weighted image of a patient with a left temporal low-grade glioma presenting with complex partial seizures. There is T2 hyperintensity and gyral expansion. B, Preoperative contrast-enhanced T1-weighted image showing the hypointense, nonenhancing tumor. C, T2-weighted image after aggressive surgical resection.

274 Neuro-oncology (Neoplasms)
round nuclei and scant cytoplasm dispersed in a loose fi brillary matrix traversed by delicate, branching vessels that occasionally subdivide the tumor into pseudolobules. This distinctive vascular architecture is referred to as a “chicken-wire” pattern. Fixation artifact results in clear-ing of the cytoplasm and gives the cell a distinguishing “fried-egg” appearance. There are no reliable and con-sistently expressed immunocytochemical markers that distinguish neoplastic oligodendrocytes from developing or mature normal oligodendrocytes. Most oligodendro-gliomas do not express GFAP or vimentin. WHO grade II mixed oligoastrocytomas have histologic features of both astrocytoma and oligodendroglioma. The two glial com-ponents may be concentrated in distinct areas, producing a biphasic pattern; more commonly, they are dispersed in an intermingled pattern [ 1 , 2 , Class III]. Distinguishing pure oligodendrogliomas and astrocytomas from mixed oligoastrocytomas can be quite challenging at times, espe-cially because there are no stringent pathologic criteria for validating a diagnosis of oligoastrocytoma.
LGGs are characterized by low to moderate cellu-larity and minimal cytonuclear atypia. They show no histologic features of anaplasia, such as microvascular proliferation or necrosis, and the mitotic activity is low [ 1 , Class III]. The proliferative index is assessed by labeling cells with an immunohistochemical stain for proliferation-related nuclear markers such as the prolif-erative cell nuclear antigen (PCNA) and Ki-67. The Ki-67 antigen is expressed in proliferative stages of the cell cycle (the G1, S, G2, and M phases) but not during the resting phase (G0). Both MIB-1 and Ki-67 are monoclo-nal antibodies directed against the Ki-67 nuclear antigen [ 13 , Class III]. Consequently, the MIB-1/Ki-67 labeling index, which refl ects only cells undergoing active divi-sion, is generally low (< 6%) in slow-growing neoplasms [ 14• , Class III]. As a general rule, higher proliferative rates, as assessed by Ki-67 and PCNA levels, are associ-ated with worse prognosis. MIB-1/Ki-67 labeling also appears to provide prognostic information that is inde-pendent of histopathologic grading. Emerging markers such as phosphohistone H3 (a specifi c marker of cells undergoing mitosis) and survivin (an inhibitory apopto-sis protein) may prove even more useful in determining the proliferative potential of gliomas [ 15 , 16 , Class III].
MOLECULAR GENETICS Over the past decade, several consistent molecular changes in LGGs have been discovered, permitting more precise subclassifi cation. The most prominent genetic anomaly observed has been the loss of heterozygosity of the 1p and 19q chromosomes (LOH 1p/19q). This event occurs in up to 80% of WHO grade II and grade III oligo dendrogliomas, suggesting that it may be an early oncogenic event in the development of these tumors [ 14• , Class III]. The chromosomal deletions are most frequent in oligo dendrogliomas (69%), followed by oligoastro-
cytomas (45%); they are rare in fi brillary astrocytomas (7%) and appear to be mediated by an unbalanced t(1;19)(q10;p10) translocation [ 2 , 17 , Class III]. Numer-ous studies have recognized that the presence of this codeletion in oligodendrogliomas suggests a considerably better prognosis [ 18 , 19 , 20•• , Class III]. In one study, median survival was 11.9 years in patients with the trans-location and 8.9 years in those without it [ 17 , Class III]. However, this association of LOH 1p/19q with a marked increase in treatment response has been noted primarily in anaplastic (WHO grade III) oligodendrogliomas and has not been studied extensively for grade II tumors.
Another genetic alteration commonly seen in LGGs is mutation of the p53 tumor suppressor gene. The TP53 gene functions to induce cell cycle arrest, apoptosis, and DNA repair; its mutation is associated with abnormal cell division and neoplastic transformation. It is observed in 88% of gemistocytic astrocytomas, 53% of fi brillary astro-cytomas, and 44% of oligoastrocytomas, but only 13% of oligodendrogliomas [ 21 , Class III]. There appears to be a mutually exclusive relationship between TP53 mutation and the presence of LOH 1p/19q [ 2 , Class III]. These fi nd-ings lend support to the notion that LOH 1p/19q leads toward oligodendroglioma formation, whereas TP53 mutations lead toward astrocytoma formation.
Several studies have identifi ed another potential bio-marker of clinical response of LGGs to chemotherapy. This biomarker is O 6 -methylguanine-DNA methyltrans-ferase (MGMT) [ 22• , Class III]. MGMT is a ubiquitous DNA repair protein that removes alkyl groups from the O 6 position of guanine, a critical site for production of DNA lesions by alkylating chemotherapeutic agents such as carmustine (BCNU), lomustine (CCNU), and temo-zolomide. Therefore, high levels of MGMT enzyme activ-ity in tumor cells result in chemoresistance. Conversely, MGMT silencing through hypermethylation of its pro-moter induces low expression of MGMT protein and decreases DNA repair activity, thereby increasing sensitiv-ity to alkylating agents. Oligodendrogliomas frequently have MGMT promoter methylation, which may partially explain their relative chemosensitivity [ 14• , Class III].
Advances in molecular biology are very promising. Evidence is mounting that LOH 1p/19q and MGMT inactivation are relevant prognostic markers and pre-dictors of chemosensitivity in gliomas, including LGGs. Although such genetic markers have not yet been for-mally validated by ongoing and planned prospective tri-als, it is anticipated that they will soon become essential for optimal treatment paradigms and individualized management decisions. Many other genetic alterations also have been identifi ed that, when present in LGGs, lead to dedifferentiation to a more malignant histology [ 23 , Class III]. The integration of such recent discoveries will allow gliomas to be classifi ed on the basis of molec-ular pathology and may permit more precise tailoring of therapy based on individual tumor biology.

Low-Grade Gliomas in Adults Mittal et al. 275
CLINICAL PROGNOSTIC FACTORS Despite their characteristic slow growth and indolent behavior, LGGs are not benign and are usually fatal. Our understanding of prognostic factors predicting survival in patients with LGGs has been greatly enhanced by three recently published prospective studies conducted by several large cooperative groups: the European Organisation for Research and Treatment of Cancer (EORTC), Medical Research Council (MRC), North Central Cancer Treatment Group (NCCTG), Radiation Therapy Oncology Group (RTOG), and Eastern Coop-erative Oncology Group (ECOG) [ 24 , 25 , 26•• , Class I]. They have completed three randomized trials (EORTC 22844, EORTC 22845, and the NCCTG/RTOG/ECOG study) that analyzed a total of 857 patients with LGG, providing vital insight and guidance for optimal care. Overall, 58% to 72% of patients in these studies were alive 5 years from the time of initial diagnosis.
The EORTC conducted a detailed analysis of prognos-tic factors for overall survival (OS) based on the 22844 and 22845 studies. That analysis excluded patients with WHO grade I astrocytomas and was conducted over a long er follow-up period than either of the original reports. On multivariate analysis of the data, Pignatti and colleagues [ 7 , Class I] determined that the fi ve factors listed in Table 2 were associated with unfavorable outcome. The number of unfavorable factors was directly correlated with survival of patients with LGGs: those with no poor prognostic factors had a median survival of 9 years, but the median survival of patients with all fi ve factors was 1 to 2 years. Similarly, the NCCTG/RTOG/ECOG study identifi ed age greater than 40 years, tumor size greater than 5 cm, and astrocytic histology as substantial negative prognostic factors [ 25 , Class I]. The median survival time for their entire cohort of 203 patients was 9.25 years. Based on these three random-
ized studies, patients can be separated into good and bad prognostic categories based on the presence of unfavorable prognostic variables.
Bauman and coworkers [ 27 , Class III] performed a recursive partitioning analysis of potential prognostic factors on data from 401 patients with LGG from three different institutions. They assessed the following param-eters for prognostic signifi cance: gender, age at tissue diag-nosis (18–40 years vs > 40 years), presence of seizures at presentation, contrast enhancement on preoperative CT or MRI, extent of resection ( ≥ 90% vs < 90%), Karnof-sky performance status (KPS) ( ≥ 70 vs < 70), tumor type (astrocytoma vs oligodendroglioma/mixed oligoastrocy-toma), timing of radiotherapy (postoperative vs delayed), and treating institution. Of these variables, KPS, patient age, and presence of tumor enhancement defi ned four
Table 2. Clinical prognostic factors unfavorable for survival in adults with low-grade gliomas
Unfavorable prognostic factors
Age ≥ 40 y
Largest diameter of tumor ≥ 6 cm
Tumor crossing the midline
Astrocytoma histology
Presence of neurologic defi cit before surgery
Unfavorable prognostic factors, n
Median survival, y (EORTC 22844)
Median survival, y (EORTC 22845)
0 9.2 9.1
1 8.8 8.6
2 5.5 6.3
3 3.6 4.4
4 1.9 3.0
5 0.7 2.4
( Adapted from Pignatti et al. [7].)
Table 3. Potentially important favorable prognostic factors for survival in adults with low-grade gliomas
Extensive surgical resection
Isolated seizures as presenting symptom
Absence of preoperative corticosteroid dependency
Excellent postoperative performance status
Small residual tumor volume after surgery
Absence of contrast enhancement
Low proliferative rate (PCNA or MIB-1/Ki-67 labeling index)
Absence of TP53 mutation
Presence of LOH 1p/19q
Hypermethylation of MGMT promoter
LOH—loss of heterozygosity; MGMT—O 6 -methylguanine-DNA methyltransferase; PCNA—proliferative cell nuclear antigen.

276 Neuro-oncology (Neoplasms)
Treatment
• Low-grade glial tumors present a substantial challenge to neuro-oncolo-gists, neurosurgeons, and radiation oncologists. The optimal management of LGGs remains controversial. These patients are typically younger and have little if any neurologic defi cit. Because of the comparative rarity of these tumors, each clinician has a unique personal experience and bias re-garding treatment. In the past, because of the indolent character and vari-able behavior of LGGs, a common approach with young, healthy adults was to “wait and watch.” With time, greater awareness of the natural history of these infi ltrating tumors has increased interest in more proac-tive management. Few randomized trials have posed treatment questions. The recently completed randomized trials have lessened the controversy and provided some guidance for the care of patients with LGGs. However, important questions remain to be answered before the process of making treatment decisions becomes easier. In talking with patients and making treatment recommendations, the value of each therapy must be cautiously and objectively considered in light of the data available from the prospec-tive and selected retrospective studies performed to date. Clinicians must take into account not only the prognostic factors already discussed but also other clinical variables such as comorbid conditions, location and resectability of the tumor, and ultimately the patient’s preference.
Surgery • The optimal role of surgical resection in the long-term outcome of
patients with supratentorial non–optic pathway LGG remains contro-versial, and the debate about the effect on outcome of its timing and extent persists. Nevertheless, surgery continues to be indispensable to the establishment of tumor histology, pathologic grade, and genotype, all of which have important therapeutic and prognostic implications.
Simple biopsy or extensive resection? • Surgical options for patients with LGGs include stereotactic biopsy and
crani otomy with tumor resection. Simple biopsy is less invasive and is often preferred for deep-seated and widespread lesions extending across the midline. However, the biopsy specimen is only a small sample from what is frequently a heterogeneous mass; it is usually not suffi cient for molec ular or genetic testing. Through sampling error, the specimen may under estimate the true histologic grade of the tumor or may be nondiagnostic [ 28 , Class III]. Craniotomy with tumor resection generally provides ample tissue for histologic, molecular, and genetic studies, as well as tissue donation for research. Past recommendations were largely based on older retrospective studies and expert opinion. The decision to proceed with resection instead of a biopsy rests on the presumption that cytoreductive surgery will im-prove long-term survival or quality of life by delaying tumor regrowth, decreasing the risk of genetic transformation to a higher grade, and improv-ing the effectiveness of adjuvant radiation therapy and chemotherapy.
groups of patients with median survival ranging from 12 to 128 months [ 27 , Class III]. Table 3 lists these and other possibly important risk factors (independent of those identifi ed by the EORTC and NCCTG/RTOG/ECOG
randomized trials) that may provide additional prognos-tic information. Prospective studies on larger numbers of patients will be required to validate these clinical factors and defi ne their prognostic signifi cance.

Low-Grade Gliomas in Adults Mittal et al. 277
• However, the greater the resection of tumor, the greater the perceived risk of permanent neurologic defi cit. Tumor location frequently determines resectability of LGGs. Tumors situated in eloquent areas of the brain are often deemed unresectable. Even for tumors in noncritical regions, the question of whether the extent of resection alters long-term outcome re-mains contentious. Certainly, advances in diagnostic and functional neuro-imaging, preoperative and intraoperative brain mapping techniques [ 29 , Class III], intraoperative navigational tools and image guidance (includ-ing intraoperative MRI [ 30 , 31 , Class III]), and neurosurgical techniques have allowed radical tumor resection with reduced surgical morbidity. Nevertheless, because of the infi ltrating nature of these tumors, even imaging-complete gross total resections leave microscopic disease at the tumor margin. Therefore, the overall impact of cytoreductive surgery is uncertain. A number of large, retrospective studies have drawn some clear conclusions about the extent and timing of surgery.
• There is general agreement on the value of surgery in the treatment of infi ltrative LGGs in patients with raised intracranial pressure, neurologic defi cits related to mass effect, and medically refractory epilepsy [ 32• , 33 , Class III]. With the increasing availability of MRI, however, patients now typically present with minimal neurologic symptoms or signs, and some authors advocate continued observation of the less symptomatic LGGs and delay surgery until there is clinical or radiographic evidence of progression. The lack of prospective, randomized clinical trials ad-dressing the prognostic infl uence of aggressive surgical resection of LGGs has further fueled the debate. Over the past 15 years, however, a growing body of evidence has emerged that undoubtedly suggests that outcomes are signifi cantly better with more radical tumor removal than with simple biopsy or debulking alone.
• Berger et al. [ 34 , Class III] analyzed the effect of extent of resection of hemispheric LGGs (determined by tumor volumes based on preopera-tive and postoperative CT or MRI) on the incidence of tumor recur-rence, time to tumor progression, and histology of recurrent tumor in 53 patients. The 13 patients who underwent a gross total resection had a mean recurrence-free follow-up period of 54 months. In the remaining 40 patients, as the percentage of resection decreased, the rate of recur-rence increased and the time to tumor progression was shorter. Interest-ingly, the authors noted that in patients with the smallest preoperative tumor volumes (< 10 cm 3 ), no recurrence was detected over a mean follow-up period of 3.5 years, regardless of the percentage of surgical resection and volume of residual disease.
• Similarly, Leighton and coworkers [ 35 , Class III] retrospectively studied 167 LGG patients over a 16-year period and found (on both univariate and multivariate analysis) that minimal postoperative residual tumor was associated with signifi cantly improved OS at 5 years.
• Other retrospective studies have shown that extensive surgical excision may prolong time to tumor regrowth and reduce the incidence of tumor progression to a higher grade [ 32• , 34 , 36 , 37 , Class III]. Karim and col-leagues [ 24 , Class I] and Pignatti et al. [ 7 , Class I] both retrospectively analyzed data collected prospectively from the EORTC phase 3 trials 22844 and 22845. They observed that, on univariate analysis, extensive resection ( ≥ 90%) was associated with longer OS and progression-free survival (PFS). However, the degree of resection (defi ned by the neuro-surgeon’s impression rather than postoperative imaging) did not reach signifi cance when balanced for other risk factors in either the EORTC trials or the NCCTG/RTOG/ECOG study.

278 Neuro-oncology (Neoplasms)
• Keles et al. [ 38 , Class III] recently evaluated 30 studies (published be-tween 1970 and 2000) that included statistical analyses. Only fi ve met the methodologic criteria established by the authors. The extent of resec-tion was a statistically signifi cant prognostic factor in all fi ve studies by univariate analysis, and in four studies by multivariate analysis.
• In arguably the most rigorous retrospective study published thus far, Smith et al. [ 39•• , Class III], examined whether the extent of resection infl uenced long-term outcomes in 216 adults who underwent surgical resection of hemispheric LGGs. They assessed tumor volumes based on preoperative and postoperative axial FLAIR slices and reported that more aggressive resection clearly predicts signifi cantly improved OS.
• Between 1998 and 2002, the RTOG enrolled 111 adults (ages 18–39 years) with supratentorial WHO grade II glioma who underwent gross total resection (as determined by the neurosurgeon) in a phase 2 study [ 40 , Class III]. The primary end points were OS, PFS, and tumor recur-rence. Prognostic factors evaluated in the multivariate analysis included age, gender, KPS, Neurologic Function Score (NFS), histopathology, contrast enhancement on preoperative MRI, preoperative tumor size, postoperative size of residual disease, and baseline Mini-Mental State Examination. The OS rate was 99% at 2 years and 93% at 5 years. The PFS rate was 82% at 2 years and 48% at 5 years. Three factors predicted a signifi cantly poorer PFS on both univariate and multivariate analyses: preoperative tumor diameter ≥ 4 cm, astrocytoma or mixed oligoastrocytoma histology, and postoperative residual tumor ≥ 1 cm. Patients with residual tumor measuring less than 1 cm on postoperative MRI had a 26% recurrence rate, those with tumor measuring 1 to 2 cm had a 68% recurrence rate, and those with residual tumor larger than 2 cm had an 89% recurrence rate [ 40 , Class III]. The authors concluded that, excluding the favorable subset of LGG patients (preoperative tumor < 4 cm, postoperative residual < 1 cm, and oligodendroglioma histology), these patients are at signifi cant risk of tumor progression and therefore should be closely monitored and considered candidates for adjuvant treatment to reduce the likelihood of tumor recurrence.
Radiation therapy • Solid information about the dose of radiation that is appropriate for
treating LGGs in adults is available from two large, phase 3, prospec-tive, randomized clinical trials that have been completed and analyzed [ 24 , 25 , Class I] ( Table 4 ). The fi rst was EORTC 22844, in which pa-tients were enrolled between 1985 and 1991. Patients 16 to 65 years of age were randomized to receive focal radiation with either 45 Gy in 25 fractions of 1.8 Gy over 5 weeks or 59.4 Gy in 33 fractions of 1.8 Gy over 6.6 weeks. This study included patients who underwent resection or biopsy of supratentorial WHO grade II oligodendrogliomas, oligo-astrocytomas, or astrocytomas as well as incompletely resected pilocytic astrocytomas. Follow-up data on 343 eligible and evaluable patients were analyzed for PFS and OS. The 5-year PFS was 47% for the patients treated with 45 Gy and 50% for the patients treated with 59.4 Gy ( P = 0.94). The 5-year OS was 58% in the low-dose group and 59% in the high-dose group ( P = 0.73) [ 24 , Class I; 41 , Class III].
• The second trial to look for an improved outcome with a higher dose of radiation was the NCCTG/RTOG/ECOG intergroup trial, which enrolled patients between 1986 and 1994 [ 25 , Class I]. In this phase 3, prospective, randomized clinical trial, patients 18 years of age or older

Low-Grade Gliomas in Adults Mittal et al. 279
Tabl
e 4.
Out
com
e of
pro
spec
tive
ran
dom
ized
tri
als
of r
adia
tion
the
rapy
in a
dult
s w
ith
low
-gra
de g
liom
as
Tota
l dos
e, G
y Pa
tien
ts, n
Pa
tien
ts
< 4
0 y
Gro
ss t
otal
re
sect
ion
WH
O
grad
e I
WH
O g
rade
II
5-ye
ar
OS,
%
Med
ian
tim
e to
pr
ogre
ssio
n, y
5-
year
PF
S, %
O
ligod
endr
oglio
ma
Ast
rocy
tom
a O
ligoa
stro
cyto
ma
EOR
TC 2
2844
tri
al [
24]
(med
ian
follo
w-u
p, 7
4 m
o)
45
171
98 (5
7%)
40 (2
3%)
15 (9
%)
35 (2
0%)
105
(61%
) 16
(9%
) 58
N
A
47
59.4
17
2 87
(51%
) 44
(26%
) 17
(10%
) 38
(22%
) 10
1 (5
9%)
16 (9
%)
59
NA
50
NC
CTG
/RTO
G/E
CO
G t
rial
[25
] (m
edia
n fo
llow
-up,
77
mo)
50.4
10
1 49
(49%
) 12
(12%
) Ex
clud
ed
69 (6
8%) †
32 (3
2%) ‡
NA
72
5.
5 § N
A
64.8
10
2 51
(50%
) 17
(17%
) Ex
clud
ed
70 (6
9%) †
32 (3
1%) ‡
NA
65
5.
5 § N
A
EOR
TC 2
2485
tri
al [
26••
] (m
edia
n fo
llow
-up,
93
mo)
0 15
7 12
4 (7
9%)*
66
(42%
) 2
(1%
) 19
(12%
) 78
(50%
) 25
(16%
) 66
3.
4 35
54
154
125
(81%
)*
66 (4
3%)
2 (1
%)
23 (1
5%)
80 (5
2%)
15 (1
0%)
68
5.3
55
* A
ge <
50
y. † P
ure
olig
oden
drog
liom
as a
nd o
ligoa
stro
cyto
mas
with
olig
oden
drog
liom
a do
min
ance
. ‡ P
ure
astr
ocyt
omas
and
olig
oast
rocy
tom
as w
ith a
stro
cyto
ma
dom
inan
ce.
§ Med
ian
time
to p
rogr
essi
on fo
r al
l sub
ject
s. EC
OG
—Ea
ster
n C
oope
rativ
e O
ncol
ogy
Gro
up; E
OR
TC—
Euro
pean
Org
anis
atio
n fo
r R
esea
rch
and
Trea
tmen
t of C
ance
r; N
A—
data
not
ava
ilabl
e; N
CC
TG—
Nor
th C
entr
al C
ance
r Tr
eatm
ent
Gro
up; O
S—ov
eral
l sur
viva
l; PF
S—pr
ogre
ssio
n-fr
ee s
urvi
val;
RTO
G—
Rad
iatio
n Th
erap
y O
ncol
ogy
Gro
up; W
HO
—W
orld
Hea
lth O
rgan
izat
ion.

280 Neuro-oncology (Neoplasms)
were treated with focal radiation in dosages of either 50.4 Gy in 28 fractions of 1.8 Gy over 5.6 weeks, or 64.8 Gy in 36 fractions of 1.8 Gy over 7.2 weeks. Patients underwent resection or biopsy of supraten-torial Kernohan grade I or II oligodendrogliomas, oligoastrocytomas, or astrocytomas. Pilocytic astrocytomas and other LGG variants were excluded from the study. Among 203 eligible and analyzable patients, OS at 5 years was 72% with 50.4 Gy of radiation and 65% with 64.8 Gy of radiation ( P = 0.48). Of note was the 2-year actuarial incidence of severe (grade 3–5) radiation neurotoxicity: 2.5% with 50.4 Gy and 5% with 64.8 Gy of radiation ( P = 0.04).
• Taken together, these two trials showed no detectable dose response be-tween 45 Gy and 64.8 Gy but a higher incidence of radiation necrosis at higher doses. Because of the lack of signifi cant benefi t from higher doses of radiation, the most common radiation dose currently prescribed for LGGs is 50.4 to 54 Gy in 1.8-Gy fractions.
• Only one phase 3, prospective trial has been completed that randomized patients to receive either early radiation or no radiation until after docu-mented tumor progression [ 26•• , Class I]. In this trial, EORTC 22845, patients 16 to 65 years of age were randomized between 1986 and 1997 to receive radiation starting within 8 weeks of surgery (54 Gy of focal radiation in 30 fractions of 1.8 Gy over 6 weeks) or no radiation until documented tumor progression. Patients with resected or biopsied supra-tentorial WHO grade II oligodendrogliomas, oligoastrocytomas, or astro-cytomas or incompletely resected pilocytic astrocytomas were included. In 303 eligible and assessable patients, the median PFS was 5.3 years in the early-radiation group and 3.4 years in the control group ( P < 0.0001). At 5 years, 55% of the early-radiation patients but only 35% of the control patients were free from progression. The median survival was 7.2 years in the early-radiotherapy group and 7.4 years in the control group. This trial shows a signifi cant prolongation of the time to tumor progression in the early-radiation group but no improvement in OS, presumably because of better effi cacy of treatment at tumor progression in the nonirradiated patients. The results suggest that radiation may have a comparable effect whether it is administered early or at subsequent tumor progression.
Pharmacologic treatment
Response to chemotherapy • Published fi nal results are available for only one phase 3, prospective,
randomized clinical trial. This small clinical trial was conducted by the Southwest Oncology Group (SWOG) between 1980 and 1985 [ 42 , Class I]. Patients with LGG were randomized to receive either 55 Gy of radia-tion in 32 fractions alone or with CCNU (100 mg/m 2 every 6 weeks for up to 2 years). This study hinted that CCNU may be active in LGG, although the difference between the two treatment arms in median survival was not statistically signifi cant. The patients who received radiation therapy plus CCNU had a median survival of 7.4 years, whereas the patients who re-ceived radiation therapy alone had a median survival of 4.5 years ( P = 0.7).
• Chemotherapy with the combination of procarbazine, CCNU, and vin-cristine (PCV) has also been found to be active in patients with LGGs, especially those with oligodendrogliomas or oligoastrocytomas [ 14• , Class III]. Because it was believed to be the most active chemotherapy available at that time, PCV was chosen as the chemotherapy to be given in the RTOG 98-02 phase 3, prospective, randomized LGG clinical trial, comparing 54 Gy of focal radiation alone with 54 Gy of focal radiation

Low-Grade Gliomas in Adults Mittal et al. 281
followed by six cycles of standard-dose PCV. The study accrued patients between 1998 and 2002. Preliminary results were reported in 2006, and more mature results are scheduled to be reported at the American Society of Clinical Oncology (ASCO) Annual Meeting in June 2008. The results of this trial will shed more light on the value of PCV in the initial management of patients with LGGs.
• More recently, single-agent temozolomide (TMZ) has also been found to be active in several small series and one large series of patients with LGGs. Response rates of 31% to 61% and 12-month PFS rates of 39% to more than 90% have been observed [ 14• , Class III]. In the largest series report-ed, Kaloshi and colleagues [ 20•• , Class III] retrospectively reviewed 149 patients with measurable, progressive, centrally reviewed, WHO grade II oligodendroglioma, oligoastrocytoma, or astrocytoma. These patients received up-front treatment with TMZ given in the conventional schedule of 200 mg/m 2 daily for 5 consecutive days, repeated every 28 days. The median number of TMZ cycles given was 14, with a range of 2 to 30. A partial response was seen in 15% of patients, minor response in 38%, stable disease in 37%, and progressive disease in 10%. The median time to reach maximum tumor response was 12 months, with a range of 3 to 30 months. The median PFS was 28 months. Tissue from 86 patients (in-cluding 60 with pure oligodendrogliomas) was checked for LOH 1p/19q, and codeletion of 1p/19q was detected in 36 cases: 30 (50%) of 60 oligo-dendrogliomas and 6 (23%) of 26 other LGGs ( P = 0.02). Codeletion of 1p/19q was associated with a higher response rate ( P = 0.02), a longer response to TMZ ( P = 0.017), longer PFS ( P = 0.00004), and longer OS ( P = 0.04). These results provide strong evidence that LGGs respond to TMZ. Besides LOH 1p/19q, another factor predicting a better response seems to be the methylation status of the MGMT promoter (MGMTP). Everhard et al. [ 22• , Class III] found that methylated MGMTP was as-sociated with better PFS when compared with unmethylated MGMTP in patients treated with TMZ ( P < 0.0001).
Choice and timing • The choice and timing of chemotherapy remain to be defi ned. TMZ is
less toxic than PCV, better tolerated, and more convenient to administer. Because of these favorable qualities and because of its demonstrated activity in treating LGGs both initially and at tumor progression, it has been chosen as the chemotherapeutic agent in two active clinical trials and one planned clinical trial. RTOG 0424 is a phase 2 trial investigat-ing the 3-year survival of high-risk (poor-prognosis) patients with LGG treated with 54 Gy of focal radiation with daily TMZ (75 mg/m 2 ) for 6 weeks, followed by 12 cycles of standard-dose TMZ [ 43 , Class III]. The EORTC 22033-26033 trial tackles the question of whether initial treatment with TMZ chemotherapy alone can replace initial radiation therapy. This trial randomizes patients to radiation therapy alone or to TMZ alone, after stratifi cation for genetic 1p loss. LGG patients are treated with either 50.4 Gy of focal radiation in 28 fractions or TMZ, 75 mg/m 2 daily for the fi rst 21 consecutive days of every 28-day cycle for 12 cycles [ 43 , Class III]. Lastly, ECOG and NCCTG are planning an intergroup randomized trial comparing combined radiation and TMZ with radiation alone [ 14• , Class III].
• At present, assessment of risk factors may guide patients and clinicians in choosing therapy. As indicated in Table 2 , patients with the most unfavorable prognostic factors usually live for a shorter time. An argu-ment for more aggressive treatment with radiation and chemotherapy

282 Neuro-oncology (Neoplasms)
may be made for such patients. For those with the fewest unfavorable prognostic factors (and the longest expected survival), consideration of long-term effects of therapy becomes more important, and a less aggres-sive approach may be more sensible. Whenever possible, however, we encourage participation in well-designed phase 2 and phase 3 clinical trials to better answer questions of effi cacy and optimal treatment. There is much to learn before we can take a more dogmatic approach to the treatment of adults with LGGs.
Pharmacologic agents Temozolomide
Classifi cation Nonclassic alkylating agent. Standard dosage 200 mg/m 2 per day orally for 5 consecutive days (days 1–5) every 28
days. If the absolute neutrophil count (ANC) falls below an acceptable level, reduce dose by 50 mg/m 2 daily. (Some clinicians prefer to start at 150 mg/m 2 for the fi rst cycle and escalate the dose to 200 mg/m 2 for subsequent cycles if there is no unacceptable toxicity).
Contraindications Hypersensitivity to the drug or its components. Also contraindicated in patients who have a history of hypersensitivity to dacarbazine (DTIC) and in patients with inadequate bone marrow reserve.
Main drug interactions No formal drug interactions have been characterized to date. Main side effects Myelosuppression is dose-limiting. Leukopenia and thrombocytopenia
are common. Mild to moderate nausea and vomiting may occur within 1 to 3 hours and last up to 12 hours. Headache, fatigue, mild elevation in hepatic transaminases. Increased photosensitivity.
Special points Myelosuppression, although generally mild, may be prolonged or severe in some patients.
Cost Actual Wholesale Price (AWP): $10 for each 5-mg capsule, $41 for each 20-mg capsule, $283 for each 140-mg capsule. Retail pharmacy prices vary widely and are generally less than AWP.
Procarbazine
Classifi cation Nonclassic alkylating agent. Standard dosage 60 mg/m 2 per day orally for 14 consecutive days (days 8–21); given in
combination with lomustine and vincristine. Contraindications Hypersensitivity to drug. Inadequate bone marrow reserve. Main drug interactions Alcohol or tyramine-containing foods taken concurrently with drug
can result in nausea, vomiting, increased CNS depression, hypertensive crisis, visual disturbances, and headache. Concurrent use of drug with antihistamines can result in CNS or respiratory depression. Concurrent use of procarbazine with levodopa or meperidine can result in hyperten-sion. Sympathomimetics and tricyclic antidepressants may result in CNS excitation manifesting as hypertension, tremors, and palpitations. Insulin and antidiabetic sulfonylurea drugs are potentiated when concurrently administered with this drug.
Main side effects Myelosuppression is the dose-limiting toxicity. Patients with glucose-6-phosphate dehydrogenase defi ciency may develop hemolytic anemia. Nausea and vomiting. Flulike symptoms of fever, chills, sweats, myalgias, and arthralgias. CNS toxicity can manifest as paresthesias, neuropathies, ataxia, lethargy, and headache. Hypersensitivity reactions with pruritus, urticaria, maculopapular rash, eosinophilia, and pulmonary infi ltrates. Skin rash usually responds to steroid therapy.
Special points Procarbazine-induced interstitial pneumonitis usually mandates discon-tinuation of therapy.
Cost AWP: $55 for each 50-mg capsule.

Low-Grade Gliomas in Adults Mittal et al. 283
Lomustine (CCNU)
Classifi cation Alkylating agent. Standard dosage 110 mg/m 2 administered orally on day 1 every 6 weeks in combination
with procarbazine and vincristine. The dose should be reduced in patients with bone marrow suppression.
Contraindications Hypersensitivity to the drug or its components. Inadequate bone marrow reserve.
Main drug interactions Cimetidine may enhance toxicity. Avoid alcohol ingestion 1 hour before and after administration.
Main side effects Myelosuppression is the dose-limiting toxicity. Nausea and vomiting may occur 2 to 6 hours after drug administration and may last up to 24 hours. Anorexia, pulmonary toxicity, and renal toxicity may also be dose-limiting.
Special points Should be taken on an empty stomach. Food may inhibit absorption. Cost AWP: $11 for each 10-mg capsule, $33 for each 40-mg capsule and $62
for each 100-mg capsule.
Vincristine
Classifi cation Vinca alkaloid, antimicrotubule agent. Standard dosage 1.4 mg/m 2 IV push (maximum 2 mg per dose) on days 8 and 29, given in
combination with procarbazine and lomustine. Contraindications Demyelinating form of Charcot-Marie-Tooth disease. Hypersensitivity to
the drug or its components. Main drug interactions The drug is metabolized by the liver cytochrome P450 3A4 system.
Cytochrome P450 3A4 inhibitors (eg, the azole class of antifungals) may increase vincristine serum concentrations; cytochrome P450 3A4 induc-ers (eg, phenytoin or phenobarbital) may decrease serum concentrations. Concurrent use with fi lgrastim may result in severe atypical neuropathy.
Main side effects Neurotoxicity is the most common dose-limiting toxicity. Neurotoxicity usually manifests as peripheral neuropathy or autonomic nervous system dysfunction. Constipation and abdominal pain are common. Paralytic ileus, alopecia, skin rash, and fever may also occur.
Special points Vincristine is a vesicant, and extravasation may cause local tissue injury, infl ammation, and necrosis. It should be administered via IV push in a free-fl owing intravenous line.
Cost AWP: $10 for each 1 mg.
Disclosures No potential confl icts of interest relevant to this article were reported.
References and Recommended Reading Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance 1. Louis DN, Ohgaki H, Wiestler OD, Cavenee WK (eds):
WHO Classifi cation of Tumours of the Central Nervous System. Lyon: IARC; 2007.
2. Ohgaki H, Kleihues P: Population-based studies on incidence, survival rates, and genetic alterations in astrocytic and oligoden-droglial gliomas. J Neuropathol Exp Neurol 2005, 64: 479– 489.
3. Schwartzbaum JA, Fisher JL, Aldape KD, Wrensch M: Epidemiology and molecular pathology of glioma. Nat Clin Pract Neurol 2006, 2: 494– 503.
4. Duffau H, Capelle L: Preferential brain locations of low-grade gliomas. Cancer 2004, 100: 2622– 2626.
5. Farrell CJ, Plotkin SR: Genetic causes of brain tumors: neurofi bromatosis, tuberous sclerosis, von Hippel-Lindau, and other syndromes. Neurol Clin 2007, 25: 925– 946.
6. Wessels PH, Weber WE, Raven G, et al. : Supratentorial grade II astrocytoma: biological features and clinical course. Lancet Neurol 2003, 2: 395– 403.

284 Neuro-oncology (Neoplasms)
7. Pignatti F, van den Bent M, Curran D, et al. : Prognostic fac-tors for survival in adult patients with cerebral low-grade glioma. J Clin Oncol 2002, 20: 2076– 2084.
8. Henson JW, Gaviani P, Gonzalez RG: MRI in treatment of adult gliomas. Lancet Oncol 2005, 6: 167– 175.
9. White ML, Zhang Y, Kirby P, Ryken TC: Can tumor contrast enhancement be used as a criterion for differen-tiating tumor grades of oligodendrogliomas? AJNR Am J Neuroradiol 2005, 26: 784– 790.
10. Danchaivijitr N, Waldman AD, Tozer DJ, et al. : Low-grade gliomas: do changes in rCBV measurements at longitu-dinal perfusion-weighted MR imaging predict malignant transformation? Radiology 2008, 247: 170– 178.
11. Guillevin R, Menuel C, Duffau H, et al. : Proton magnetic resonance spectroscopy predicts proliferative activity in diffuse low-grade gliomas. J Neurooncol 2008, 87: 181– 187.
12. Herholz K, Coope D, Jackson A: Metabolic and molecular imaging in neuro-oncology. Lancet Neurol 2007, 6: 711– 724.
13. Fisher BJ, Naumova E, Leighton CC, et al. : Ki-67: a prognostic factor for low-grade glioma? Int J Radiat Oncol Biol Phys 2002, 52: 996– 1001.
14.• Schiff D, Brown PD, Giannini C: Outcome in adult low-grade glioma: the impact of prognostic factors and treatment. Neurology 2007, 69: 1366– 1373.
Excellent review of recent studies outlining important clinical, histologic, and molecular prognostic factors. Also summarizes studies using PCV and TMZ in treating LGGs. 15. Colman H, Giannini C, Huang L, et al. : Assessment and prog-
nostic signifi cance of mitotic index using the mitosis marker phospho-histone H3 in low and intermediate-grade infi ltrating astrocytomas. Am J Surg Pathol 2006, 30: 657– 664.
16. Uematsu M, Ohsawa I, Aokage T, et al. : Prognostic signifi cance of the immunohistochemical index of survivin in glioma: a comparative study with the MIB-1 index. J Neurooncol 2005, 72: 231– 238.
17. Jenkins RB, Blair H, Ballman KV, et al. : A t(1;19)(q10;p10) mediates the combined deletions of 1p and 19q and predicts a better prognosis of patients with oligodendroglioma. Cancer Res 2006, 66: 9852– 9861.
18. Aldape K, Burger PC, Perry A: Clinicopathologic aspects of 1p/19q loss and the diagnosis of oligodendroglioma. Arch Pathol Lab Med 2007, 131: 242– 251.
19. Mariani L, Deiana G, Vassella E, et al. : Loss of hetero-zygosity 1p36 and 19q13 is a prognostic factor for overall survival in patients with diffuse WHO grade 2 gliomas treated without chemotherapy. J Clin Oncol 2006, 24: 4758– 4763.
20.•• Kaloshi G, Benouaich-Amiel A, Diakite F, et al. : Temo-zolomide for low-grade gliomas: predictive impact of 1p/19q loss on response and outcome. Neurology 2007, 68: 1831– 1836.
Retrospective, single-center study of 149 consecutive patients, revealing that LGGs respond to TMZ. Codeletion of 1p/19q in 36 of 86 patients tested predicted a better response to TMZ. 21. Okamoto Y, Di Patre PL, Burkhard C, et al. : Population-
based study on incidence, survival rates, and genetic alterations of low-grade diffuse astrocytomas and oligo-dendrogliomas. Acta Neuropathol 2004, 108: 49– 56.
22.• Everhard S, Kaloshi G, Criniere E, et al. : MGMT methyla-tion: a marker of response to temozolomide in low-grade gliomas. Ann Neurol 2006, 60: 740– 743.
Retrospective study examining the methylation status of the MGMT promoter in 68 patients with LGGs treated with TMZ. Methylated MGMTP was a favorable predictor of progression-free survival when compared with tumors with unmethylated MGMTP. 23. Hegi ME, Murat A, Lambiv WL, Stupp R: Brain tumors:
molecular biology and targeted therapies. Ann Oncol 2006, 17(Suppl 10): 191– 197.
24. Karim A, Maat B, Hatlevoll R, et al. : A randomized trial on dose-response in radiation therapy of low-grade cerebral glioma: European Organization for Research and Treat-ment of Cancer (EORTC) study 22844. Int J Radiat Oncol Biol Phys 1996, 36: 549– 556.
25. Shaw E, Arusell R, Scheithauer B, et al. : Prospective ran-domized trial of low- versus high-dose radiation therapy in adults with supratentorial low-grade glioma: initial report of a North Central Cancer Treatment Group/Radiation Therapy Oncology Group/Eastern Cooperative Oncology Group study. J Clin Oncol 2002, 20: 2267– 2276.
26.•• van den Bent MJ, Afra D, de Witte O, et al. : Long-term effi cacy of early versus delayed radiotherapy for low-grade astrocytoma and oligodendroglioma in adults: the EORTC 22845 randomised trial. Lancet 2005, 366: 985– 990.
Randomized trial of the long-term effi cacy of early versus delayed radiation for adults with LGGs, revealing that early radiation therapy after surgery prolongs the time to tumor progression but does not affect overall survival. 27. Bauman G, Lote K, Larson D, et al. : Pretreatment factors
predict overall survival for patients with low-grade glioma: a recursive partitioning analysis. Int J Radiat Oncol Biol Phys 1999, 45: 923– 929.
28. Jackson RJ, Fuller GN, Abi-Said D, et al. : Limitations of stereotactic biopsy in the initial management of gliomas. Neuro Oncol 2001, 3: 193– 200.
29. Sanai N, Mirzadeh Z, Berger MS: Functional outcome after language mapping for glioma resection. N Engl J Med 2008, 358: 18– 27.
30. Claus EB, Horlacher A, Hsu L, et al. : Survival rates in patients with low-grade glioma after intraoperative magnetic resonance image guidance. Cancer 2005, 103: 1227– 1233.
31. Nimsky C, Ganslandt O, Buchfelder M, Fahlbusch R: Intraoperative visualization for resection of gliomas: the role of functional neuronavigation and intraoperative 1.5 T MRI. Neurol Res 2006, 28: 482– 487.
32.• Pouratian N, Asthagiri A, Jagannathan J, et al. : Surgery Insight: the role of surgery in the management of low-grade gliomas. Nat Clin Pract Neurol 2007, 3: 628– 639.
Critical analysis of large retrospective studies investigating the effect of surgical resection on outcomes of patients with LGGs. 33. Chang E, Potts M, Keles G, et al. : Seizure characteristics
and control following resection in 332 patients with low-grade gliomas. J Neurosurg 2008, 108: 227– 235.
34. Berger M, Deliganis A, Dobbins J, Keles G: The effect of extent of resection on recurrence in patients with low grade cerebral hemisphere gliomas. Cancer 1994, 74: 1784– 1791.
35. Leighton C, Fisher B, Bauman G, et al. : Supratentorial low-grade glioma in adults: an analysis of prognostic factors and timing of radiation. J Clin Oncol 1997, 15: 1294– 1301.
36. Nakamura M, Konishi N, Tsunoda S, et al. : Analysis of prognostic and survival factors related to treatment of low-grade astrocytomas in adults. Oncology 2000, 58: 108– 116.
37. Scerrati M, Roselli R, Iacoangeli M, et al. : Prognostic factors in low-grade (WHO grade II) gliomas of the cerebral hemispheres: the role of surgery. J Neurol Neurosurg Psychiatry 1996, 61: 291– 296.
38. Keles G, Lamborn K, Berger M: Low-grade hemispheric gliomas in adults: a critical review of extent of resection as a factor infl uencing outcome. J Neurosurg 2001, 95: 735– 745.
39.•• Smith J, Chang E, Lamborn K, et al. : Role of extent of resection in the long-term outcome of low-grade hemi-spheric gliomas. J Clin Oncol 2008, 26: 1338– 1345.
Retrospective review revealing that improved outcome is predicted by greater extent of resection in adult patients with hemispheric LGGs. 40. Shaw EG, Berkey B, Coons MD, et al. : Recurrence follow-
ing neurosurgeon-determined gross total resection of adult supratentorial low-grade glioma: results of a prospective clinical trial. J Neurosurg (in press).
41. Papagikos MA, Shaw EG, Stieber VW: Lessons learned from randomised clinical trials in adult low grade glioma. Lancet Oncol 2005, 6: 240– 244.
42. Eyre H, Crowley J, Townsend J, et al. : A randomized trial of radiotherapy versus radiotherapy plus CCNU for incom-pletely resected low-grade gliomas. A Southwest Oncology Group study. J Neurosurg 1993, 78: 909– 914.
43. See SJ, Gilbert MR: Chemotherapy in adults with gliomas. Ann Acad Med Singapore 2007, 36: 364– 366.